Cognitive-Communication Disorders An Overview Jody E. Rice, M.S., CCC- SLP

Cognitive-Communication Disorders An Overview Jody E. Rice, M.S., CCC-SLP.
Dec 29, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Cognitive-Communication Disorders
An OverviewJody E. Rice, M.S., CCC-SLP
Disorders Review
Introduction
• What do these have in common?– Traumatic brain injury– Right hemisphere syndrome/dysfunction– Dementia
Introduction
• Is a cognitive-communication disorder the same as an aphasia?
• Is a cognitive-communication the same as a dysarthria? – An apraxia?
Why is the SLP involved?• Cognition and communication are intrinsically and
reciprocally related in both development and function
• Cognitive-communication disorders encompass any aspect of communication affected by disruption of cognition
• Areas of function affected by cognitive impairments include behavioral self-regulation, social interaction, ADLs, learning and academic performance and vocational performance.
ASHA 2004 Knowledge and Skills Document
Narrative Discourse Sample
Bang, bang, twang, bang, as a bullet knocks the cup of hot coffee away from the lips of our trusty ol’ [Bill]. Yes, old and weak he was but, is always trying, and to no prevail. It wasn’t his real name, we think, but if people only knew, the horrifying secret of this calm yet not so docile old guy! The fact, that he had a few years on the others in the train was to be determined at some other event of event at hand. We think
Narrative Discourse Sample, cont.
Though it was always, [Bill] this, and [Bill] that, every time he turned around, the echo prevailed; [Bill] was a feeble old, chap though he had this seemingly strike one against him, he continued. Don’t worry; we wonder how, just the same as you. Great minds think alike, or not, or there about.
International Classification of Functioning, Disability, and Health 2001
• Functioning & Disability– Body structures and Functions– Activity and Participation
• Contextual Factors– Environmental Factors– Personal Factors
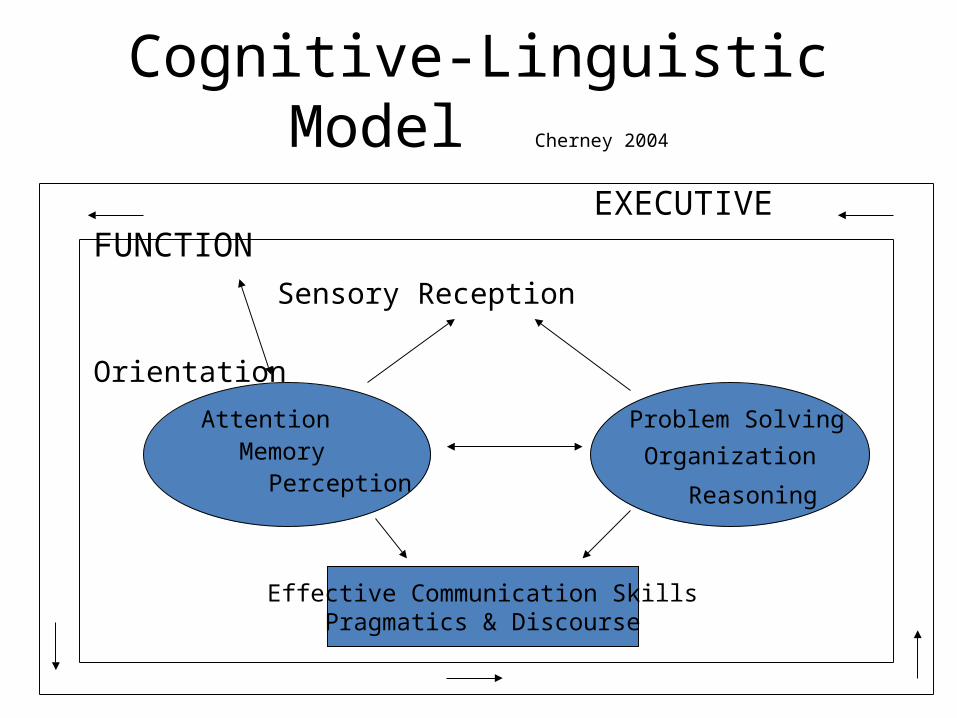
Cognitive-Linguistic Model Cherney 2004
EXECUTIVE FUNCTION Sensory Reception Orientation
Organization
Attention
PerceptionMemory
Problem Solving
Reasoning
Effective Communication SkillsPragmatics & Discourse
Sensory Reception
• Passive process
• Reception of tactile, olfactory, gustatory, visual, auditory, proprioceptive, and kinesthetic information
Attention
• Alertness and Arousal– Level of vigilance vs. active direction of attention
toward a target• Types of Attention (Sohlberg and Mateer)
– Focused (short focus)– Sustained (focus for a period of time)– Selective (Paying attention w/distractions– Alternating (switching activites back & fourth)– Divided (multitasking)
Perception
• Active process• Provides structure to the environment• Integrates sensory information; Detects
salient features and patterns in sensory stimuli
• Olfactory & gustatory information processes subcortically; other sensory information processed cortically
Memory• Encoding
– Linking information to the context– Phonological loop vs. visuospatial sketchpad
• Storage– Integrating new information with current store; requires
reorganization of memory• Retrieval
– Activating memory from storage for immediate use– Context during learning should be same during retrieval– Explicit (declarative)(ride bike or smell) vs. Implicit (procedural)
• Retrospective (past events) & prospective (future events)
Organization
• Sorting
• Categorizing
• Sequencing
• Prioritizing
• Analysis/Synthesis
Reasoning/Problem-Solving
• Abstract thinking; ability to draw inferences and conclusions
• Deductive/Inductive; divergent(central concept then branch off)/convergent(what does cat dog elaphant have in commen?)
• Problem-solving requires convergent and divergent thinking, especially divergent thinking
• Judgment: predicting consequences, forming opinions
Executive Functioning(mom of the brain)
• Associated with all aspects of cognitive functioning• “CEO”; Supervisory capacity to direct actions• More apparent in novel, unstructured situations• Setting goals; planning and directing goal-oriented activity• Awareness of strengths and limitations• Initiating and inhibiting behavior• Monitoring activity• Evaluating results• Taking another person’s perspective• Applying learned skills to context

TRAUMATIC BRAIN INJURY (TBI)
Head Injury
• A traumatic insult to the brain capable of producing physical, intellectual, emotional, social, and vocational changes (BIAA)– Acquired brain injury (ABI)– Examples of causes of head injury
• Closed vs. Open head injury
Statistics
• 1.4 million sustain BI each year• Leading causes: falls (28%); MVA (20%)• Males 1.5 times more likely to sustain BI• Age groups: 0-4 y.o.; 15-19 y.o.• At least 3.17 million Americans currently have
a long-term need to help to perform ADLsBIAA
Neuropathology
• Primary damage– Contusions(bruise on frontal or temporal lobe) vs.
diffuse axonal injury(not a focused area)
• Secondary damage– Occur as a result of primary damage (hemorrhage,
bleading on brain, preasure, adema(swelling))
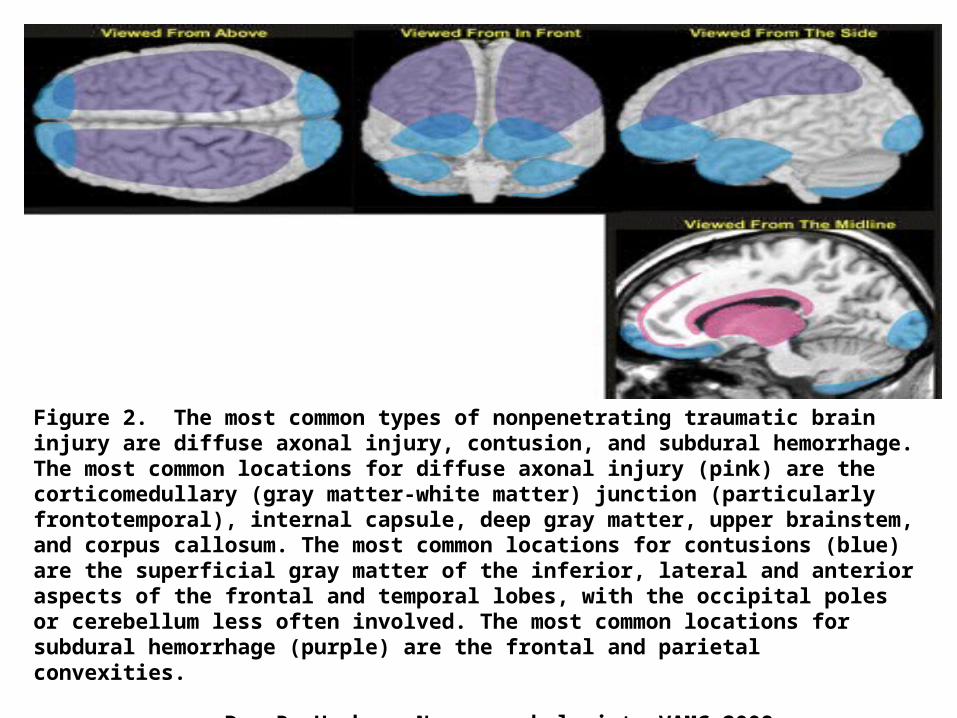
Figure 2. The most common types of nonpenetrating traumatic brain injury are diffuse axonal injury, contusion, and subdural hemorrhage. The most common locations for diffuse axonal injury (pink) are the corticomedullary (gray matter-white matter) junction (particularly frontotemporal), internal capsule, deep gray matter, upper brainstem, and corpus callosum. The most common locations for contusions (blue) are the superficial gray matter of the inferior, lateral and anterior aspects of the frontal and temporal lobes, with the occipital poles or cerebellum less often involved. The most common locations for subdural hemorrhage (purple) are the frontal and parietal convexities.
Dr. R. Hughes, Neuropsychologist, VAMC 2008 Presentation
Outcomes
• Depth and duration of coma – GCS 13-15 mild 9-12 moderate ≤ 8 severe
GCS score of 8 or less for 6 hours or more tend to have a poorer outcome• Age• Secondary medical complications• Behavioral & Psychological factors
(mild)mTBI
• Common Symptoms:– Fatigue– Headaches; Visual disturbances – Memory loss; Poor attention/concentration – Slowness in thinking– Irritability-emotional disturbances– Seizures– Getting lost or confused
BI in the Military
• Continuum of care from time of injury• Services at James H. Quillen Mountain Home
VAMC• Blasts/explosions as a primary source of BI
(IED, landmine, grenade)– Matter is literally transformed from a gas to a
solid wall of pressure traveling about 1300 mph.

• http://uk.truveo.com/IED-Attack-On-Humvee-In-Iraq-Humvee-Roll-Over/id/502692489
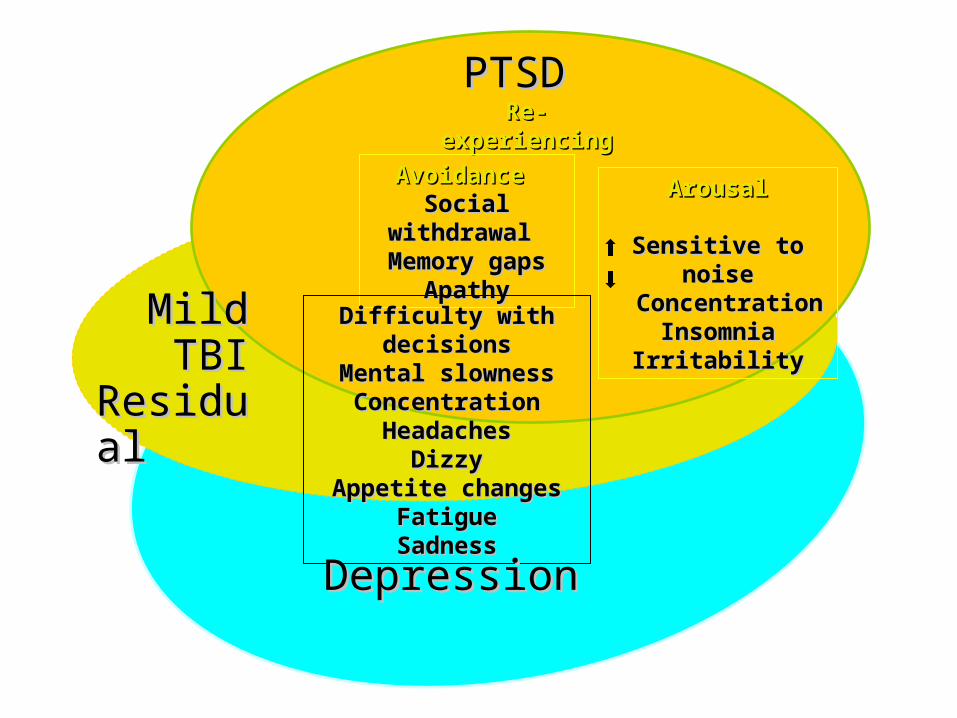
PTSDPTSD Re-experiencingRe-experiencing
AvoidanceAvoidance Social withdrawal Social withdrawal
Memory gapsMemory gapsApathyApathy
MildMild TBITBIResidualResidual
Difficulty with decisionsDifficulty with decisionsMental slownessMental slowness
ConcentrationConcentrationHeadachesHeadaches
DizzyDizzyAppetite changesAppetite changes
FatigueFatigueSadnessSadness
ArousalArousal
Sensitive to noiseSensitive to noise ConcentrationConcentration
InsomniaInsomniaIrritabilityIrritability
DepressionDepression
COGNITIVE-LINGUISTIC ASSESSMENT/ TREATMENT
Assessment• No single assessment battery effective• Review of records; thorough case history• Behavioral observations• Information from family/significant others• Standardized testing
– Component cognitive processes– Basic language function + verbal integration and reasoning
• Environmental Needs Assessment(what do they do on daily basis)
• Evaluation of Everyday Performance– Checklists/rating scales for cognitive-comm:– Discourse comprehension and production
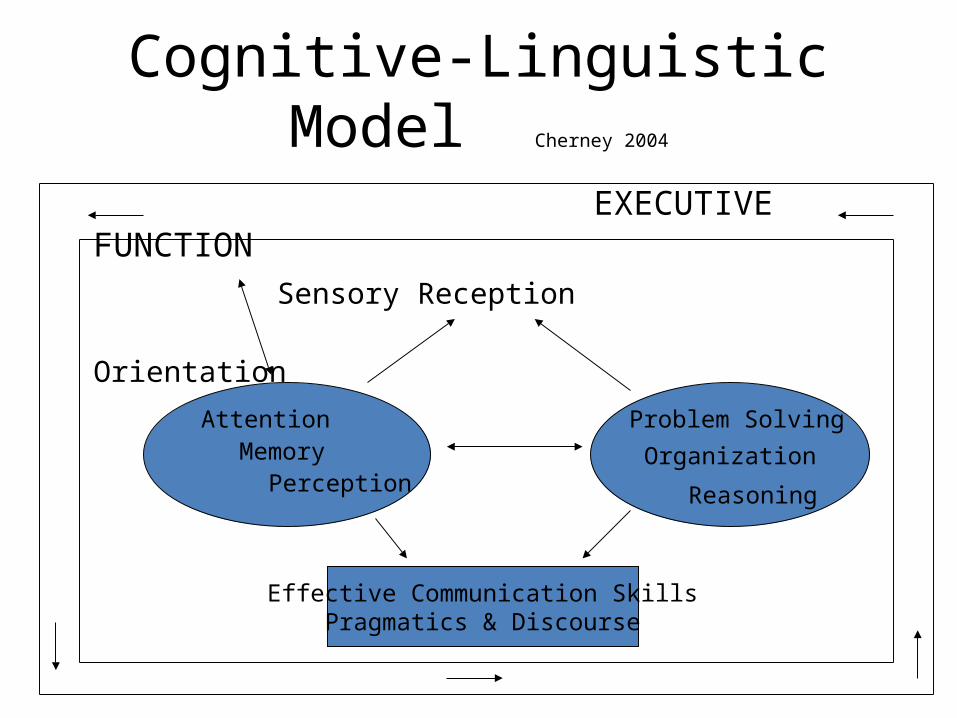
Cognitive-Linguistic Model Cherney 2004
EXECUTIVE FUNCTION Sensory Reception Orientation
Organization
Attention
PerceptionMemory
Problem Solving
Reasoning
Effective Communication SkillsPragmatics & Discourse
Testing Component Cognitive Processes
• Standardized Semi-Comprehensive Assessments– Brief Test of Head Injury– Scales of Cognitive Ability for Traumatic Brain
Injury– Cognitive Linguistic Quick Test– Ross Information Processing Assessment
• Tests of Specific Cognitive Processes(specific test like attention or memory)
Testing Basic Language Function & Verbal Integration/Reasoning
• Basic Language Function– Subtests of aphasia batteries
• Verbal Integration & Reasoning– Detroit Tests of Learning Aptitude– Right hemisphere language tasks– Other high-level language tasks

Evaluation of Everyday Performance
• Checklists/Rating scales
• Pragmatics/Discourse
• Environmental Needs Assessment/Ecological Inventory
Forms of Intervention
• Facilitation• Process-specific training• Functional approach• Skills training• Compensations(by pass)

INTERVENTION – A CONSIDERATION
• Tailor treatment approach to stage of recovery• Early
– Sensory stimulation
• Middle– Retraining of cognitive components
• Late– Functional integration of components; compensatory
strategies
Right Hemisphere Dysfunction
Dichotomies of Cerebral Hemispheres
LEFTVerbalLinguisticExpressionSymbolic/propositionalLogical/analyticFocal/discreteSegmental
RIGHTNonverbalVisual/kinestheticPerceptionVisual/imaginativeHolistic/syntheticDiffuseSpatial/global
• http://www.youtube.com/watch?v=ZVO2dcTUZRQ
Clinical Syndromes
• Visuoperceptual– Hemispatial neglect (attentional disorder)– Anosognosia (denial of illness)
• minimize deficit; attribute limbs to another; hatred of limb; exaggerate strength
– Environmental Agnosia (loss of environmental familiarity; inability to become topographically oriented)
– Prosopagnosia (failure to recognize familiar faces)
Clinical Syndromes, cont.
• Visuomotor– Constructional disability
• Neglect left half of model, errors in spatial relations, add extraneous material
– Dressing disturbances• Hemispatial neglect• Body-garment disorientation

Clinical Syndromes, cont.
• Affective and Emotional Alterations– Aprosody– Impaired affective auditory comprehension– Disturbances of emotional facial recognition– Altered emotional facial expression
• Memory Disorders– Retention of complex visual patterns/ faces– Nonverbal memory
Clinical Syndromes, cont.
• Neuropsychiatric Disorders– Visual hallucinations (r/t visual field defects)– Capgras’ Syndrome (loved ones replaced by
imposters)– Secondary mania (elated and/or irritable mood
lasting > 1 week)– Acute confusional states – Paranoid hallucinatory states
TREATMENT OF COGNITIVE-LINGUISTIC DISORDERS
Goal Setting
• Functional assessment• Identify long-term outcomes for life domains• Short-term objectives• Responses to be measured
– Consistency/accuracy– Efficiency/frequency– Duration– Response mode– Independence

Treatment
• Relation to ICF 2001 framework:– Treat underlying processes– Treat surface communication symptoms– Treat in appropriate contexts
• Integrative, collaborative approach
Treatment Principles
• Positive attitude – instill sense of ownership• Hierarchical organization – move from simple to the
complex; “error-free” environment• Concise, clear instructions and specific feedback• Use of strategies and problem-solving; task analysis• Self-talk; promote self-monitoring• Use natural consequences• Opportunity for generalization; role-play• Focus on functional routines
Attention Training• Process-Specific Training; Hierarchy• Environmental Adjustments
– Eliminate external distractions– Avoid clutter– One task at a time
• Compensatory Strategy Training– Self-talk: Am I paying attention? What am I supposed to
be doing?– Use of timer, alarm or watch– Other cognitive prosthetic devices– Breaks– Schedule more difficult tasks first
Memory Training
• Restoration vs. Compensation– Rehearsal– Focus on teaching of strategies– Internal vs. external strategies– Gear treatment to type of memory deficit
• External Memory Aids – Devices, notebooks
• Internal Retrieval Strategies
Dementia

Types of Dementia
• Primary (progressive & irreversible)– Alzheimer’s Disease: senile plaques and neurofibrillar tangles
• Secondary (progressive & irreversible)– Huntington’s Disease– Parkinson’s Disease
• Secondary (potentially reversible)– UTI– Stress/Fatigue
• Secondary (treatable but irreversible)– Alcoholic dementia

• http://www.alz.org/alzheimers_disease_4719.asp

Deficits Associated with AD• Cognition
• Language
• Perception– Figure ground, position in space, visuoconstructional skills,
facial agnosia• Psychomotor skills (apraxia)
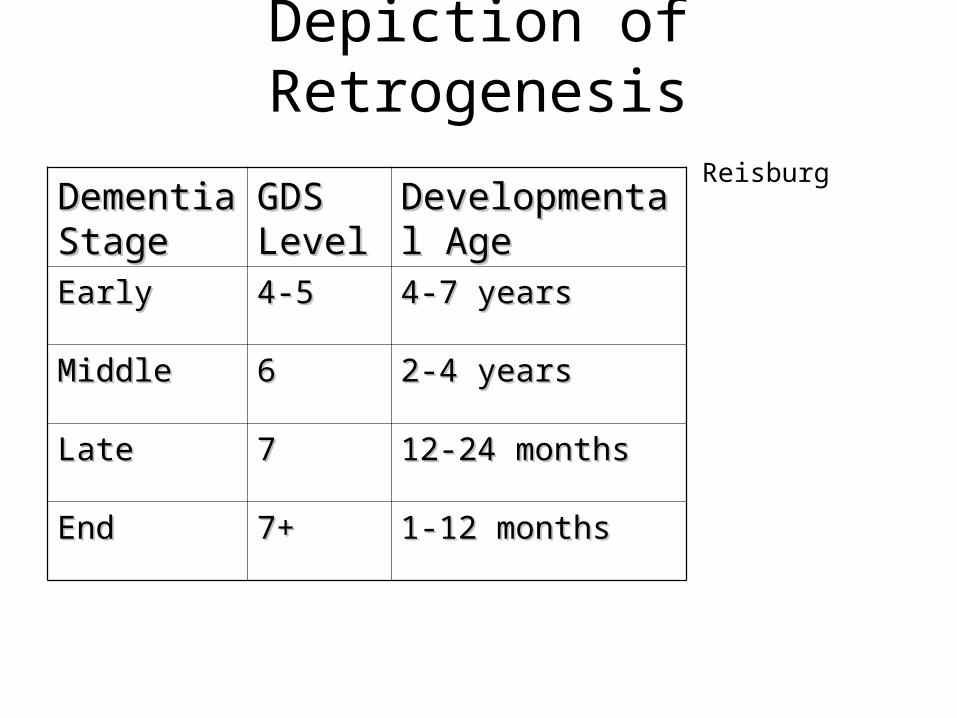
Depiction of RetrogenesisReisburg
Dementia Dementia StageStage
GDS GDS LevelLevel
Developmental Developmental AgeAge
EarlyEarly 4-54-5 4-7 years4-7 years
MiddleMiddle 66 2-4 years2-4 years
LateLate 77 12-24 months12-24 months
EndEnd 7+7+ 1-12 months1-12 months
WHAT IS BEHAVIOR?
Behavior is the action or reaction of persons or things in response to unmet physical, emotional, social, or environmental needs.
Behavior is language for late stages 6 & 7
Speech-Pathologist’s Role
• Evaluation/staging• Active tx (if appropriate)• Development and training in use of Functional
Maintenance Program
Assessment
• Brief Cognitive Rating Scale (BCRS); GDS• Arizona Battery for Communication Disorders
of Dementia (ABCD)• Functional Linguistic Communication
Inventory (FLCI)
Treatment
• Active treatment vs. functional maintenance plans
• Stage of dementia• Following directions• New learning
FMPs
• Developed by SLP• Support staff trained by SLP • Approx. 2-3 week duration of tx
Related Documents











