Open Forum Cognitive-Behavioral Couple’s Treatment for Posttraumatic Stress Disorder Candice M. Monson, Karen A. Guthrie, and Susan Stevens, White River Junction VA Regional Office and Medical Center C ognitive-behavioral theory and technique has been relatively underutilized in treat- ing individuals with posttraumatic stress disorder (PTSD) within a couple’s therapy con- text. This is despite the clinically recognized and empirically established association between PTSD and intimate relationship problems (e.g., Beckham, Lytle, & Feldman, 1996; Byrne & Riggs, 1996; Carroll, Rueger, Foy, & Donahoe, 1985; Jordan et al., 1992). Although existing cognitive-behavioral treatments for PTSD are ex- tremely beneficial for some clients (Rothbaum, Meadows, Resick, & Foy, 2000, for review), there are limitations to these existing treatments, in- cluding problems in delivery (i.e., attrition rates as high as 50% in some samples) and outcomes (e.g., variable success in treating avoidance/numbing symptoms; 25% to 60% still meet diagnostic cri- teria for PTSD at the end of treatment and at fol- low-up periods; see Zayfert, Becker, & Gillock, 2002, for discussion). Moreover, these treatments have not been specifically designed to address the complex interplay of intimate relationships and PTSD. In an effort to extend our treatment reper- toire for PTSD, we developed a Cognitive- Behavioral Couple’s Treatment (CBCT) for PTSD that addresses cognitive and behavioral mecha- nisms thought to contribute to both PTSD and intimate relationship discord. This article pro- vides an overview of the treatment protocol. the Behavior Therapist ISSN 0278-8403 Volume 26, No. 8, Winter, 2003 Winter 2003 393 c ontents Open Forum Candice M. Monson, Karen A. Guthrie, and Susan Stevens Cognitive-Behavioral Couples’Treatment for Posttraumatic Stress Disorder 393 William O’Donohue Rational Animals: Behavior Therapy’s Focus on Knowledge and Understanding of Human Behavior 402 Steven Reiss Epicurus: The First Rational-Emotive Therapist 405 Book Reviews Reviewed by Alan E. Kazdin Conditioned Reflex Therapy (50th-Anniversary printing), by Andrew Salter 408 Reviewed by Amy Przeworski and Michelle G. Newman Empirically Supported Cognitive Therapies: Current and Future Applications, by W. J. Lyddon and J. V. Jones, Jr. 411 Reviewed by Mariola Magovcevic and Michael E. Addis New Directions for Rational Emotive Behavior Therapy: Overcoming Destructive Beliefs, Feelings, and Behaviors, by Albert Ellis 412 ERRATUM 414 CLASSIFIEDS 414 At AABT • The Duties and Charges of the AABT President Elect and Representative-at-Large 415 • Nominate the Next Candidates for AABT Office back page Call for AABT Award Nominations: page 407

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Open Forum
Cognitive-BehavioralCouple’s Treatment forPosttraumatic StressDisorder
Candice M. Monson, Karen A. Guthrie, andSusan Stevens, White River Junction VARegional Office and Medical Center
Cognitive-behavioral theory and techniquehas been relatively underutilized in treat-ing individuals with posttraumatic stress
disorder (PTSD) within a couple’s therapy con-text. This is despite the clinically recognized andempirically established association between PTSDand intimate relationship problems (e.g.,Beckham, Lytle, & Feldman, 1996; Byrne &Riggs, 1996; Carroll, Rueger, Foy, & Donahoe,1985; Jordan et al., 1992). Although existingcognitive-behavioral treatments for PTSD are ex-tremely beneficial for some clients (Rothbaum,Meadows, Resick, & Foy, 2000, for review), thereare limitations to these existing treatments, in-cluding problems in delivery (i.e., attrition rates ashigh as 50% in some samples) and outcomes (e.g.,variable success in treating avoidance/numbingsymptoms; 25% to 60% still meet diagnostic cri-teria for PTSD at the end of treatment and at fol-low-up periods; see Zayfert, Becker, & Gillock,2002, for discussion). Moreover, these treatmentshave not been specifically designed to address thecomplex interplay of intimate relationships andPTSD. In an effort to extend our treatment reper-toire for PTSD, we developed a Cognitive-Behavioral Couple’s Treatment (CBCT) for PTSDthat addresses cognitive and behavioral mecha-nisms thought to contribute to both PTSD andintimate relationship discord. This article pro-vides an overview of the treatment protocol.
the Behavior Therapist
ISSN 0278-8403
Volume 26, No. 8, Winter, 2003
Winter 2003 393
contentsOpen Forum
Candice M. Monson, Karen A. Guthrie, and Susan Stevens
Cognitive-Behavioral Couples’Treatment for Posttraumatic
Stress Disorder 393
William O’Donohue Rational Animals: Behavior Therapy’s Focus
on Knowledge and Understanding of Human Behavior 402
Steven Reiss Epicurus: The First Rational-Emotive Therapist 405
Book Reviews
Reviewed by Alan E. Kazdin Conditioned Reflex Therapy
(50th-Anniversary printing), by Andrew Salter 408
Reviewed by Amy Przeworski and Michelle G. Newman
Empirically Supported Cognitive Therapies: Current and Future
Applications, by W. J. Lyddon and J. V. Jones, Jr. 411
Reviewed by Mariola Magovcevic and Michael E. Addis
New Directions for Rational Emotive Behavior Therapy: Overcoming
Destructive Beliefs, Feelings, and Behaviors, by Albert Ellis 412
ERRATUM 414
CLASSIFIEDS 414
At AABT
•The Duties and Charges of the AABT President Elect and
Representative-at-Large 415
•Nominate the Next Candidates for AABT Office back page
Call for AABT Award Nominations: page 407

394 the Behavior Therapist
the Behavior TherapistPublished by the Association for
Advancement of Behavior Therapy
305 Seventh Avenue - 16th Floor
New York, NY 10001-6008
(212) 647-1890 /Fax: (212) 647-1865
www.aabt.org
EDITOR · · · · · · · · · · · George F. Ronan
Editorial Assistant · · · · · · · · Jennifer Slezak
Behavior Assessment · · · · · · John P. Forsyth
Book Reviews · · · · · · · · · · Kurt H. Dermen
Clinical Forum · · · · · · · · · James D. Herbert
Dialogues · · · · · · · · Christine Maguth Nezu
Dissemination· · · · · · · Michael A. Tompkins
Institutional Settings · · · · · · · · · · · Tamara Penix Sbraga
International Scene · · · · Fugen A. Neziroglu
Lighter Side· · · · · · · · · · · Donna M. Ronan
Professional Issues · · · · · · · · · Saul D. Raw
Research-Practice Link · · · · · · · · · · · · · · · · · David J. Hansen
Research-Training Link · · · · · · · · · · · · · · · · Gayle Y. Iwamasa
Science Forum· · · · · · · · · · · Jeffrey M. Lohr
Special Interest Groups · · · · · · · · · · Andrea Seidner Burling
Student Forum· · · · · · · · · · · Kelly McClure
AABT
President · · · · · · · · · · · Jacqueline B. Persons
Executive Director · · · · · · Mary Jane Eimer
Director of Publications· · · · · David Teisler
Managing Editor · · · · · · Stephanie Schwartz
Projects Manager · · · · · · · Patience Newman
Copyright © 2003 by the Association for
Advancement of Behavior Therapy. All rights
reserved. No part of this publication may be
reproduced or transmitted in any form, or by
any means, electronic or mechanical, including
photocopy, recording, or any information stor-
age and retrieval system, without permission
in writing from the copyright owner.
Subscription information: the Behavior
Therapist is published in 8 issues per year. It
is provided free to AABT members.
Nonmember subscriptions are available at
$38.00 per year (+$17.00 surface postage or
+$32.00 airmail postage outside USA).
Change of address: 6 to 8 weeks are required
for address changes. Send both old and new
addresses to the AABT office.
All items published in the Behavior Therapist,
including advertisements, are for the informa-
tion of our readers, and publication does not
imply endorsement by the Association.
The Association for Advancement of BehaviorTherapy publishes the Behavior Therapist as a serviceto its membership. Eight issues are published annu-ally. The purpose is to provide a vehicle for the rapiddissemination of news, recent advances, and innova-tive applications in behavior therapy.
Feature articles that are approximately 16 dou-ble-spaced manuscript pages may be submitted. Brief
articles, approximately 6 to 12 double-spaced manu-script pages, are preferred. Feature articles andbrief articles should be accompanied by a 75- to100-word abstract. Letters to the Editor may beused to respond to articles published in the Behavior
Therapist or to voice a professional opinion. Lettersshould be limited to approximately 3 double-spacedmanuscript pages.
Please contact the Editor or any of the AssociateEditors for guidance prior to submitting series, specialissues, or other unique formats. All submissionsshould be in triplicate and formatted according to thePublication Manual of the American Psychological
Association, 5th edition. Prior to publication, authorswill be asked to provide a 3.5” diskette containing afile copy of the final version of their manuscript.Authors submitting materials to the Behavior
Therapist do so with the understanding that the copy-right of published materials shall be assigned exclu-sively to the Association for Advancement of BehaviorTherapy. Please submit materials to the attention ofthe Editor: George F. Ronan, Ph.D., Department ofPsychology, Central Michigan University, MountPleasant, MI 48859.
INSTRUCTIONS FOR AUTHORS
This approach evolved out of our work
with veterans suffering from military-
related PTSD—primarily men suffering
from combat-related trauma—within the
Family IMPACT (Family Integration in the
Management, Prevention, Assessment, and
Counseling of Trauma) Project at the White
River Junction VA Regional Office and
Medical Center, Mental Health/Behavioral
Science Service and National Center for
PTSD, Executive Division. However, the
interpersonal problems of men and women
suffering from PTSD caused by the expo-
sure to a wide variety of stressors appear to
be remarkably similar to those suffering
from combat-related trauma (e.g.,
Herman, 1992; Neumann, Houskamp,
Pollock, & Briere, 1996). In brief, individu-
als with PTSD report greater frequency and
severity of intimate relationship dysfunc-
tion, including intimate aggression. PTSD
is also associated with a higher rate of sepa-
rations and divorce. The avoidance/numb-
ing cluster of PTSD has been implicated in
relationship discord and intimacy prob-
lems, and there is some evidence of an asso-
ciation between hyperarousal symptoms
and the perpetration of physical and psy-
chological aggression in male veterans.
Most of the empirical research that has been
conducted with the significant others of
traumatized individuals has consisted of fe-
male partners of male combat veterans.
These partners report a wide range of men-
tal health and relationship problems that
have been found to be associated with their
partner’s PTSD symptomatology. Despite
the similarity of these relationship issues
caused by various forms of trauma, there are
also symptoms unique to specific types of
trauma.
Previous Studies of Conjoint
Therapy for PTSD
The identification of intimate relation-ship problems associated with PTSD anddiscussion of the role of traumatized indi-viduals’ partners in trauma treatment (e.g.,Byrne & Riggs, 1996; Carroll et al., 1985;Erickson, 1989; Figley, 1988, 1989;Johnson, Feldman, & Lubin, 1995; Johnson& Williams-Keeler, 1998; Matsakis, 1994;Riggs, 2000; Riggs, Byrne, Weathers, &Litz, 1998; Tarrier, Sommerfield, & Pil-grim, 1999) has not necessarily translatedinto treatment research efforts. To ourknowledge, there have been only two con-trolled and two uncontrolled studies thathave investigated conjoint treatment forPTSD. Treatments employed in these stud-ies consisted of generic forms of behavioralcouple’s/family therapy (i.e., no specificfocus on PTSD-related issues).
Randomized Clinical Trials
In a dissertation study of group behav-ioral couple’s therapy compared to wait list,Sweany (1987) found a significant decreasein self-reported PTSD symptoms for thosein treatment compared to the control con-dition. Furthermore, there were trends forimprovements in relationship satisfactionand the veteran’s depression. Also using aveteran sample, Glynn et al. (1999) com-pared individual exposure therapy alone toindividual exposure therapy followed by be-havioral family therapy (BFT; 89% wereconjugal partners) to a wait-list controlgroup. They found significant improve-ments in the positive symptoms of PTSD(i.e., reexperiencing and hyperarousal) forboth active treatments compared to thecontrol group, but no differences betweenthe two active treatments. There were nosignificant improvements found in the neg-ative symptoms of PTSD (i.e., avoidance

Winter 2003 395
and numbing) across the three conditions.It should be noted that there was a highdropout rate in the BFT condition (i.e.,35%), which the authors attributed to thedelay prior to receiving BFT and thefragility of these veterans’ relationships.Experiences with exposure therapy may alsoexplain this attrition, given the study’s se-quential design.
Uncontrolled Trials
Two uncontrolled treatment studies ofconjoint therapy have been reported. Usinggroup behavioral couple’s therapy withcombat veterans, Cahoon (1984) found sta-tistically significant improvements in PTSDsymptoms and coping ability (as rated bythe group leaders; effect sizes .47 and .72,respectively). While the veterans reportednonsignificant improvements in emotionaland problem-solving communication (ef-fect sizes .18 and .41, respectively), the vet-erans’ female significant others reportedsignificant improvements in marital distressand problem-solving communication (ef-fect sizes .34 and .56, respectively). Rabinand Nardi (1991) also provided a cognitive-behavioral group couple’s treatment withIsraeli combat veterans and their wives,which included psychoeducation aboutPTSD. Minimal objective outcome data areprovided from this study; however, 68% ofthe traumatized men and their wives re-ported relationship improvements. How-ever, this study did not show a decrease inthe veterans’ PTSD symptoms.
CBCT for PTSD
CBCT1 has received widespread valida-tion for treatment of couple’s distress anddysfunction (see Christensen & Heavey,1999, for review), and has been extendedand empirically tested in the treatment ofindividuals suffering from a variety of clinicalproblems. With regard to depression, do-mestic violence, alcohol and drug depen-dence/abuse, and agoraphobia, CBCT hasbeen found to be equally or more efficaciousthan individual or group therapy in treatingthe primary clinical problem. Moreover,CBCT has a variety of additional benefits,including increased relationship satisfac-tion, decreased intimate aggression, lesstime separated, fewer divorces, more effi-cient treatment (i.e., greater gains,quicker), less attrition from treatment, and
treatment-related cost savings (e.g.,Arrindell & Emmelkamp, 1986; Daiuto,Baucom, Epstein, & Dutton, 1998, formeta-analysis regarding agoraphobia; Fals-Stewart, Birchler, & O’Farrell, 1996;Jacobson, Dobson, Fruzzetti, Schmaling, &Salusky, 1991; McCrady, Stout, Noel,Abrams, & Nelson, 1991; O’Farrell et al.,1996; O’Leary & Beach, 1990; O’Leary,Heyman, & Neidig, 1999).
Taking into account the devastating andlargely untreated relationship problems as-sociated with PTSD, some preliminary evi-dence supporting the efficacy of behavioralcouple’s therapy for PTSD, and the estab-lished efficacy of CBCT for a variety of otherindividual problems, we have developed acognitive-behavioral couple’s treatmentspecific to PTSD. The treatment isgrounded in cognitive-behavioral concep-tualizations of intimate relationship discordand PTSD.
Cognitive and Behavioral Mechanisms
Behavioral conceptualizations have beenoffered to explain intimate relationship dis-cord and PTSD, respectively. In the case ofintimate relationship discord, nonreinforc-ing, conflictual, and/or abusive behaviorand communication are considered to causeand maintain couple distress and are pri-mary targets for intervention (Jacobson &Margolin, 1979). Mowrer’s (1960) two-fac-tor explanation of conditioned fears hasbeen used to explain the development andmaintenance of PTSD symptoms (e.g., Foa& Kozak, 1991; Keane, Zimering, &Caddell, 1985). Classical conditioningprocesses are postulated to explain the ori-gins of the anxiety response, while operantconditioning processes explain its mainte-nance (i.e., negative reinforcement of fearthrough behavioral avoidance). Experientialavoidance, or avoidance of private experi-ences (e.g., feelings, memories, behavioralpredispositions, thoughts; Hayes & Gifford,1997, for review) construed to be negative, isa particular form of avoidance that has re-cently been implicated in the developmentand maintenance of PTSD (Boeschen, Koss,Figueredo, & Coan, 2001). Behavioral in-terventions for PTSD are aimed at exposureto traumatic memories and trauma-relatedcues, with the goal of anxiety habituation.While the trauma exposure may differ withregard to the dimensions of exposure type
(i.e., imaginal versus in vivo), exposurelength (i.e., short versus long), and arousallevel during exposure (low versus high),they share the common feature of havingpatients confront their fears, and are generi-cally referred to as “exposure” treatmentsfor PTSD (Foa & Rothbaum, 1998).
Cognitive constructs have been incorpo-rated into these behavioral conceptualiza-tions of PTSD and relationship dysfunction.Selective attention to negative events, dis-tress-maintaining attributions, unrealisticand/or unshared expectancies, conflictingassumptions, and differing standards havebeen found to be associated with intimaterelationship discord (Baucom, Epstein, &Rankin, 1995). Similarly, information(Lang, 1977) and emotion (e.g., Foa &Kozak, 1991) processing theories have beenused to explain the processes through whichtraumatic memories and associated affectsare stored, maintained, and targeted intreatment. Schemas, or cognitive structuresof meaning, have also been used to explainhow trauma affects a person’s belief systemand the adjustments (i.e., schema accom-modation and assimilation) necessary toreconcile the traumatic event with existingbeliefs and expectations and to process asso-ciated emotions (e.g., Resick & Schnicke,1993). Cognitive interventions consist ofchallenging irrational and/or dysfunctionalthoughts and beliefs related to intimate re-lationship discord or PTSD.
Interplay of intimate relationship discord and
PTSD. Similar cognitive and behavioralmechanisms are postulated to underliePTSD and relationship discord, and can in-teract to maintain or exacerbate both prob-lem areas. If successfully targeted intreatment, this reciprocal association holdspotential to ameliorate both PTSD and inti-mate relationship dysfunction.
In CBCT for PTSD, avoidance is consid-ered to be a primary behavioral mechanismcontributing to PTSD and intimate rela-tionship problems, and is consequently tar-geted early on and throughout treatment.This notion is supported by empirical re-search that has revealed an association be-tween the avoidance/numbing PTSDsymptom cluster and diminished relation-ship satisfaction and intimacy. In this re-search, numbing symptoms were especiallyproblematic to relationship functioning(Riggs et al., 1998). Likewise, the avoidanceof affective expression and sharing in inti-mate relationships has long been associatedwith diminished relationship satisfactionand intimacy in couples in general (seeGottman & Levenson, 1986, for review).
1For this review, we use CBCT to describe the treatments to date that have been expanded to treat people suf-fering from a variety of individual problems. However, CBCT is part of a larger class of conjoint interventionswith varying emphases and interventions. These treatments are also referred to in the literature as behavioralcouple’s therapy, behavioral marital therapy, behavioral conjoint therapy, and integrative behavioral coupletherapy.

396 the Behavior Therapist
Monitoring for the various means bywhich an individual or couple may exhibitavoidance is considered integral to success-ful treatment. Avoidance may consist ofmore traditionally considered behavioralavoidance of trauma-related cues and re-minders. However, this avoidance may begeneralized to include experiential avoid-ance, as well as avoidance of certain individ-ual or couple’s issues. Experientialavoidance is considered to frustrate inti-macy because of the diminished ability foraffective expression and communication.“Avoiding avoidance” is accomplishedthrough psychoeducation and the couple’sdevelopment of conflict management andcommunication skills that can be used todiscuss and manage increasingly distressingissues previously avoided. The discussion ofthese topics, including trauma-relatedthoughts, feelings, and behaviors, providesopportunities to directly address the issuescontributing to PTSD. Moreover, specificemphasis is paid to emotion identification,sharing, and reflection in couple’s commu-nication, and the value of emotion expres-sion and tolerance in individual and couplefunctioning is underscored. Conflict-man-agement skills building is also postulated toimprove management of PTSD hyper-arousal symptoms such as anger and irri-tability, which have been found to beassociated with intimate aggression perpe-tration (Savarese, Suvak, King, & King,2001).
CBCT for PTSD is not considered to bean exposure treatment: Individuals are notconfronted with specific traumatic experi-ences with the goal of anxiety habituation.Rather, consistent with cognitive conceptu-alizations of PTSD, individuals are encour-aged to focus on the various emotionssurrounding their memories and remindersof the event(s), as well as the meaning of theevent(s) for the here-and-now. Thus, weargue that relaying the specific details is lessimportant than fully experiencing, express-ing, and processing the emotions attachedto them. In this cognitive vein, similar cog-nitive structural (i.e., schemas), content(i.e., irrational and/or dysfunctionalthoughts, beliefs, standards, assumptions,attributions), and process (i.e., accommoda-tion, assimilation) variables have been usedto explain the development and mainte-nance of intimate relationship discord andPTSD.
McCann and Pearlman’s (1990) work,also incorporated into Cognitive ProcessingTherapy (CPT; Resick & Schnicke, 1993),provides cognitive content relevant toPTSD and intimate relationships that is
specifically targeted for cognitive interven-tion. They outline five areas of functioningfrequently affected by traumatic experi-ences: safety, trust, power/control, esteem,and intimacy. Consistent with CPT,thoughts and beliefs held across these areasare explored and challenged as they relate tothe self and other, with the goal of schemaaccommodation and emotional processing.These themes, including their interpersonalfocus, fit nicely with the conjoint therapyframe.
Treatment Format
Routine pre- and posttreatment assess-ments are highly encouraged, regardless ofwhether the treatment is delivered in a re-search protocol or in nonresearch practice.Prior to initiating treatment, we provideclients with feedback about their PTSDsymptoms, relationship functioning, and as-sociated psychological issues. This feedbackis used as an aid to psychoeducation and intreatment goal setting, and supports thegoal-oriented focus of treatment. In our ex-perience, couples have been eager to receivetheir assessment results, and these resultshave enhanced treatment delivery. We useboth self-report (PTSD Checklist; Weathers,Litz, Herman, Huska, & Keane, 1993) andinterview (Clinician-Administered PTSDScale for DSM-IV; Blake et al., 1990) meth-ods for assessing PTSD. Relationship vari-ables assessed include relationship sat-isfaction (Dyadic Adjustment Scale; Spanier,1976), intimate aggression (Conflict TacticsScale–Second Edition; Straus, Hamby,McCoy, & Sugarman, 1996), communica-tion skills (10-minute communication sam-ple about a moderately distressing topic forbehavioral coding), and adult attachment(Experiences in Close Relationships;Brennan, Clark, & Shaver, 1998). De-pression (Beck Depression Inventory; Beck,Ward, Mendelsohn, Mock, & Erbaugh,1961), anxiety (State-Trait AnxietyInventory; Spielberger & Lushene, 1989),and affective control (Affective ControlScale; Berg, Shapiro, Chambless, Ahrens,1998) are associated features assessed.
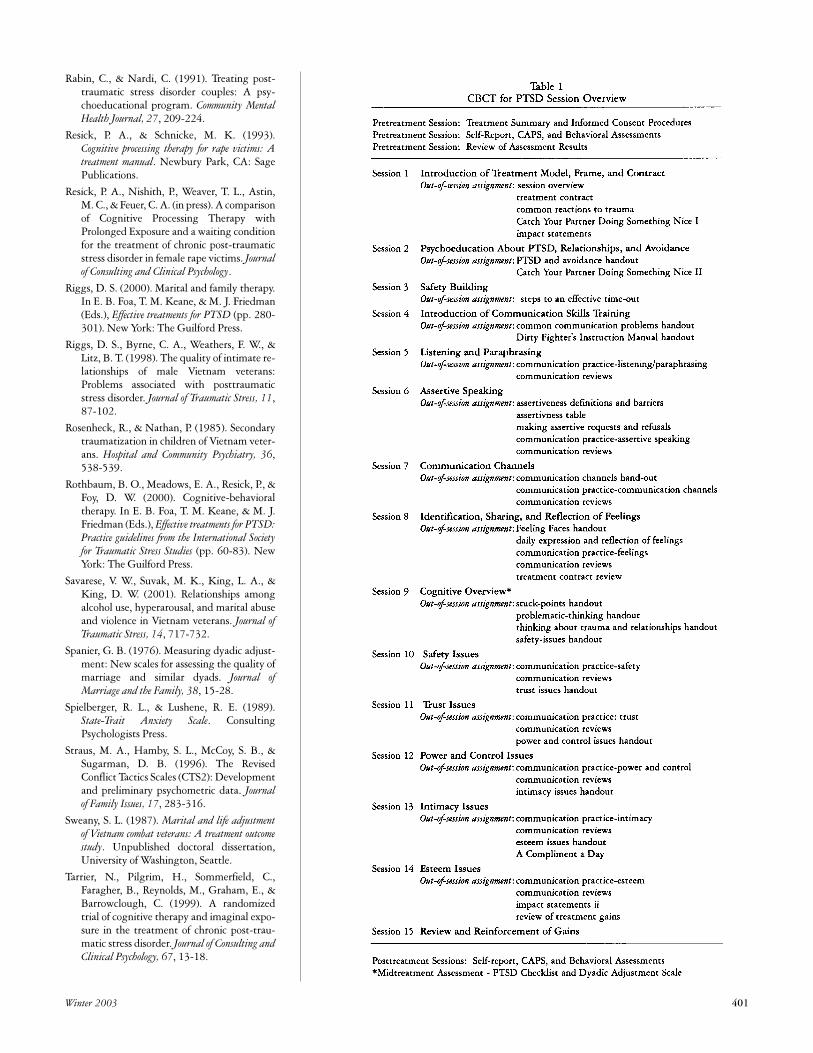
CBCT for PTSD consists of 15 weeklysessions comprising three primary treat-ment phases: (a) treatment orientation, psy-choeducation about PTSD and its relatedintimate relationship problems, and safetybuilding; (b) communication skills training;and (c) cognitive interventions. Each 75-minute session begins with an overview ofwhat is to be accomplished in the session,and includes didactic information to conveyto clients and skills for them to practice in
the session. Out-of-session assignmentsconclude each of the sessions (see Table 1).
The first three sessions of the treatmentare focused on orienting the couple to treat-ment, psychoeducation about PTSD, rela-tionships and avoidance, and establishingsafety within the couple and the therapeuticrelationship. The first session outlines treat-ment expectations and presents the phase-oriented, here-and-now, goal-oriented, andtime-limited nature of the treatment. Wecandidly discuss the issue of trauma disclo-sure and solicit possible concerns, desires,and prohibitions from each member of thecouple about this issue (see SpecialConsiderations section for more discussion).The expectation and rationale for out-of-session assignments (we are careful to usethe word “assignment” as opposed to“homework” based on feedback from ourclients) are also provided in this session.Treatment goals are mutually developed,and each member of the couple signs atreatment contract containing these goalsand the above treatment expectations.Session 1 also emphasizes the importance ofincreasing positive couple behavior whiledecreasing negative couple behavior. Thisleads to the first out-of-session assignment:daily attention to their partner’s positive be-havior.
Session 2 is devoted to understandingPTSD as an anxiety disorder as well as in-troducing a cognitive-behavioral conceptu-alization of PTSD. Couples receiveinformation about hallmark PTSD symp-toms and associated problems, for example,the maintenance of PTSD through avoid-ance strategies such as experiential avoid-ance. We also explore the hypothesizeddeleterious role of experiential avoidance inintimate relationships (i.e., avoidanceand/or numbing symptoms) and its mani-festation in the specific couple’s relation-ship. The notion of habituation is presentedto provide a rationale to support the couplein discussing uncomfortable and distressingtopics. The third session is spent exploringthe existence of very negative behavior (e.g.,intimate aggression, threats to leave the re-lationship, ongoing infidelity), and develop-ing conflict-management skills (e.g., time-outs).
Communication skills training. Sessions 4through 8 focus on traditional communica-tion skills building (e.g., listening/para-phrasing; assertiveness, emotional versusproblem-solving communication; emotionidentification, sharing, and reflection) usingincreasingly distressing topics (low to mod-erate range) based on the couple’s currentdifficulties. In the fourth session, the couple

Winter 2003 397

398 the Behavior Therapist
views their pretreatment communicationsample with the therapist. This supports therationale for communication skills trainingand allows the couple to observe their com-munication from a more objective perspec-tive. The couple is asked to audiotape 5 to10 minutes of communication each week intheir home setting during this treatmentphase, utilizing the communication skillsthey are building. These audiotapes are re-viewed with the couple in the next sessionto troubleshoot and to provide positivefeedback to the couple.
Cognitive interventions. In the final phaseof treatment, the couple more deeply con-solidates their knowledge about PTSD andintimate relationships using their newly de-veloped skills to address the effect of traumaon themselves and their relationship.Session 9 introduces the influence of traumaon how people perceive the world, them-selves, and others, and the role of dysfunc-tional thoughts and beliefs in maintainingdistress. The five themes outlined byMcCann and Pearlman (1990) presentedabove (i.e., safety, trust, power/control, inti-macy, and esteem) are introduced over fivesessions and used as communication topicsfor the couple’s out-of-session practice. Thecouple is encouraged to draw upon theircommunication skills and to assume a pos-ture of curiosity as they nonjudgmentallyexplore and gently mutually challenge orsupport their thoughts and beliefs held inthese areas. Each session concludes with anout-of-session assignment to discuss theidentified area presented in that session overthe subsequent week, audiotaping at leastone of the communications for review at thenext session.
The final session is spent reviewing andreinforcing gains made in therapy and an-ticipating future challenges.
Special Considerations
We recently completed an open trial ofCBCT for PTSD to fine-tune the treatmentmanual (available from the first author),train therapists, and provide initial evidenceregarding its safety, tolerability, and efficacy.From this initial, and other’s, work, we offerup the following considerations.
Dually Traumatized Couples
Dually traumatized couples may bemore the rule than the exception. This is es-pecially likely when working with coupleswherein the initially referred patient has afemale partner because of the two-to-oneprevalence of PTSD in women versus men(e.g., Kessler, Sonnega, Bromet, Hughs, &
Nelson, 1995). In addition, previous re-search suggests that people who have a psy-chological disorder are more likely to marryor cohabit with people who also have a psy-chological disorder (Du Fort, Kovess, &Boivin, 1994). The partner may have expe-rienced primary traumatization prior to orduring their intimate relationship as a resultof family-of-origin violence, exposure to do-mestic violence perpetrated by their partnerwith PTSD or previous partner, sexual as-sault, or some other type of trauma. In addi-tion, a number of authors have discussedvicarious or secondary traumatization ofthese partners as a result of strong emo-tional connections with the trauma victim(e.g., Figley, 1989; Nelson & Wright, 1996;Rosenheck & Nathan, 1985). Thus, we as-sume, and it has been the case thus far in ourwork, that partners are likely to presentwith PTSD and/or some other type of psy-chological problem.
The treatment principles and interven-tions of CBCT for PTSD are considered tobe sufficiently broad and flexible to meetthe challenges of couples with their respec-tive psychopathology. Evidence to supportthis assertion is that all of the female part-ners in our study had trauma historiesand/or clinical levels of depression, anxiety,and/or PTSD symptoms. Therapists shouldanticipate possible reactions to disclosuresand distressing topics, monitor for anychanges in risk factors (e.g., suicidality, ag-gression, substance abuse) for both mem-bers of the couple, and stress theimportance of emotional and physical safetythroughout therapy.
Trauma Disclosure
Another important point to highlightabout the treatment is that we explicitlydiscuss with the couple that there is no re-quirement that either of them disclose spe-cific information about their trauma history.In general, we encourage clients to talkabout their trauma histories as they relate tohere-and-now thoughts and feelings; wediscourage in-depth, gory, and/or gratu-itous retellings of their experiences. Wehave adopted this approach to avoid possi-ble vicarious traumatization of partners andbased on clinical trials supporting the effi-cacy of cognitively focused approaches toPTSD treatment (Marks, Lovell, Noshir-vani, Livanou, & Thrasher, 1998; Resick,Nishith, Weaver, Astin, & Feuer, in press;Tarrier et al., 1999). Even if clients do notshare details of their traumatic experiences,beliefs and emotions linked to their traumasare likely to be evoked, which provides op-
portunities for habituation, schema accom-modation, emotional processing, andgreater mastery and tolerance of these emo-tions.
Type of Trauma
As noted in the introduction, military-related trauma is clearly not the only formof trauma exposure that leads to significantinterpersonal difficulties. By their very na-ture, interpersonal traumas appear likely tolead to intimate relationship problems andmay be particularly well suited for CBCT.For example, Follette and Pistorello (1995)outlined various problems found in couplesin which the woman was a victim of child-hood sexual assault; they also suggest theuse of interventions to address experientialavoidance. Some specific problems relatedto sexual assault/abuse may include retrig-gering of traumatic memories and sensa-tions, dissociation, or flashbacks during thecouple’s sexual relations; hyper- or hyposex-uality; problems with libido; or generalnegative attitudes about sex. Revictim-ization is clearly of concern with victims ofinterpersonal violence (e.g., Messman-Moore & Long, 2000) and is an issue thatshould be specifically assessed and ad-dressed within the conjoint context (i.e.,history of, or current emotional, physical, orsexual abuse within the relationship).
Summary
Our challenge in advancing PTSD treat-ment is to offer innovative stand-alone oradjunctive treatments for those individualswho have not responded or fully benefitedfrom available empirically validated treat-ments. Given the established interpersonalcosts of PTSD and proven efficacy of con-joint therapy for other individual problems,we believe that CBCT for PTSD holdspromise as an efficient and efficacious treat-ment for individuals and their loved oneswith PTSD.
References
Arrindell, W. A., & Emmelkamp, P. M. G.(1986). Marital quality and general life ad-justment in relation to treatment outcome inagoraphobia. Advances in Behavior Research
and Therapy, 8, 139-185.
Baucom, D. H., Epstein, N., & Rankin, L. A.(1995). Cognitive aspects of Cognitive-Behavioral Marital Therapy. In N. S.Jacobson & A. S. Gurman (Eds.), Clinical
handbook of couple therapy (pp. 65-90). NewYork: The Guilford Press.
Beck, A. T., Ward, C. H., Mendelsohn, M.,Mock, J., & Erbaugh, J. (1961). An inventory

Winter 2003 399

400 the Behavior Therapist
for measuring depression. Archives of General
Psychiatry, 4, 561-571.
Beckham, J. C., Lytle, B. L., & Feldman, M. E.(1996). Caregiver burden in partners ofVietnam War veterans with posttraumaticstress disorder. Journal of Consulting and
Clinical Psychology, 64, 1068-1072.
Berg, C. Z., Shapiro, N., Chambless, D. L., &Ahrens, A. H. (1998). Are emotions fright-ening? II: An analogue study of fear of emo-tion, interpersonal conflict, and panic onset.Behaviour Research and Therapy, 36, 3-15.
Blake, D. D., Weathers, F. W., Nagy, L. M.,Kaloupek, D. G., Klauminizer, G., Charney,D. S., & Keane, T. M. (1990). A clinical ratingscale for assessing current and lifetimePTSD: The CAPS-1. the Behavior Therapist,
18, 187-188.
Boeschen, L. E., Koss, M. P., Figueredo, A. J., &Coan, J. A. (2001). Experiential avoidanceand post-traumatic stress disorder: A cogni-tive mediational model of rape recovery.Journal of Aggression, Maltreatment and
Trauma, 4, 211-245.
Brennan, K. A., Clark, C. L., & Shaver, P. R.(1998). Self-report measures of adult roman-tic attachment. An integrative overview. In J.A. Simpson & W. S. Rholes (Eds.), Attachment
theory and close relationships. New York: TheGuilford Press.
Byrne, C. A., & Riggs, D. S. (1996). The cycle oftrauma: Relationship aggression in maleVietnam veterans with symptoms of post-traumatic stress disorder. Violence and Victims,
11, 213-225
Cahoon, E. P. (1984). An examination of relation-
ships between post-traumatic stress disorder, marital
distress, and response to therapy by Vietnam veter-
ans. Unpublished doctoral dissertation,University of Connecticut, Storrs.
Carroll, E. M., Rueger, D. B., Foy, D. W., &Donahoe, C. P. (1985). Vietnam combat vet-erans with posttraumatic stress disorder:Analysis of marital and cohabitating adjust-ment. Journal of Abnormal Psychology, 94, 329-337.
Christensen, A., & Heavey, C. L. (1999).Interventions for couples. Annual Review of
Psychology, 50, 165-190.
Daiuto, A. D., Baucom, D. H., Epstein, N., &Dutton, S. S. (1998). The application of be-havioral couples therapy to the assessmentand treatment of agoraphobia: Implicationsof empirical research. Clinical Psychology
Review, 18, 663-687.
Du Fort, G. G., Kovess, V., & Boivin, J. F. (1994).Spouse similarity for psychological distressand well-being: A population study.Psychological Medicine, 24, 431-447.
Erickson, C. A. (1989). Rape and the family. InC. R. Figley (Ed.), Treating stress in families
(pp. 257-289). New York: Brunner/Mazel.
Fals-Stewart, W., Birchler, G. R., & O’Farrell, T.J. (1996). Behavioral couples therapy formale substance-abusing patients: Effects on
relationship adjustment and drug-using be-havior. Journal of Consulting and Clinical
Psychology, 64, 959-972.
Figley, C. R. (1988). A five-phase treatment ofpost-traumatic stress disorder in families.Journal of Traumatic Stress, 1, 127-141.
Figley, C. R. (1989). Helping traumatized families.San Francisco: Jossey-Bass.
Foa, E. B., & Kozak, M. J. (1991). Emotionalprocessing: Theory, research, and clinical im-plications for anxiety disorders. In J. D.Safran & L. S. Greenberg (Eds.), Emotion, psy-
chotherapy, and change (pp. 21-49). New York:The Guilford Press.
Foa, E. B., & Rothbaum, B. O. (1998). Treating
the trauma of rape: Cognitive-behavioral therapy
for PTSD. New York: The Guilford Press.
Follette, V. M., & Pistorello, J. (1995). Couplestherapy. In C. Classen & I. D. Yalom (Eds.),Treating women molested in childhood (pp. 129-161). San Francisco: Jossey-Bass.
Glynn, S. M., Eth, S., Randolph, E. T., Foy, D.W., Urbaitis, M., Boxer, L., Paz, G. G.,Leong, G. B., Firman, G., Salk, J. D.,Katzman, J. W., & Crothers, J. (1999). A testof behavioral family therapy to augment ex-posure for combat-related posttraumaticstress disorder. Journal of Consulting and
Clinical Psychology, 67, 243-251.
Gottman, J. M., & Levenson, R. W. (1986).Assessing the role of emotion in marriage.Behavioral Assessment, 8, 31-48.
Hayes, S. C., & Gifford, E. V. (1997). The troublewith language: Experiential avoidance, rules,and the nature of verbal events. Psychological
Science, 8, 170-173.
Herman, J. L. (1992). Trauma and recovery. NewYork: Basic Books.
Jacobson, N. S., Dobson, K., Fruzzetti, A. E.,Schmaling, K. B., & Salusky, S. (1991).Marital therapy as a treatment for depres-sion. Journal of Consulting and Clinical
Psychology, 59, 547-557.
Jacobson, N. S., & Margolin, G. (1979). Marital
therapy: Strategies based on social learning and be-
havior exchange principles. New York:Brunner/Mazel.
Johnson, D. R., Feldman, S. C., & Lubin, H.(1995). Critical interaction therapy: Couplestherapy in combat-related posttraumaticstress disorder. Family Process, 34, 401-412.
Johnson, S. M., & Williams-Keeler, L. (1998).Creating healing relationships for couplesdealing with trauma: The use of emotionallyfocused marital therapy. Journal of Marital
and Family Therapy, 24, 25-40.
Jordan, B. K., Marmar, C. R., Fairbank, J. A.,Schlenger, W. E., Kulka, R. A., Hough, R. L.,& Weiss, D. S. (1992). Problems in families ofmale Vietnam veterans with posttraumaticstress disorder. Journal of Consulting and
Clinical Psychology, 60, 916-926.
Keane, T. M., Zimering, R. T., & Caddell, J. M.(1985). A behavioral formulation of post-
traumatic stress disorder in Vietnam veter-ans. the Behavior Therapist, 8, 9-12.
Kessler, R. C., Sonnega, A., Bromet, E., Hughes,M., & Nelson, C. D. (1995). Posttraumaticstress disorder in the National ComorbiditySurvey. Archives of General Psychiatry, 52,1048-1060.
Lang, P. J. (1977). Imagery in therapy: An infor-mation processing analysis of fear. Behavior
Therapy, 8, 862-886.
Marks, I. M., Lovell, K., Noshirvani, H.,Livanou, M., & Thrasher, S. (1998).Treatment of post-traumatic stress disorderby exposure and/or cognitive restructuring:A controlled study. Archives of General
Psychiatry, 55, 317-325.
Matsakis, A. (1994). Dual, triple, and quadrupletrauma couples: Dynamics and treatment is-sues. In M. B. Williams & J. F. Sommers(Eds.), Handbook of post-traumatic therapy (pp.78-93). Westport, CT: Greenwood Press.
McCann, I. L., & Pearlman, L. A. (1990).Psychological trauma and the adult survivor:
Theory, therapy, and transformation. New York:Brunner/Mazel.
McCrady, B. S., Stout, R. L., Noel, N. E.,Abrams, D. B., & Nelson, H. F. (1991).Comparative effectiveness of three types ofspouse-involved behavioral alcoholism treat-ment: Outcome 18 months after treatment.British Journal of Addictions, 86, 1415-1424.
Messman-Moore, T. L., & Long, P. J. (2000).Child sexual abuse and revictimization in theform of adult sexual abuse, adult physicalabuse, and adult psychological maltreat-ment. Journal of Interpersonal Violence, 15, 489-502.
Mowrer, O. A. (1960). Learning theory and behav-
ior. New York: Wiley.
Nelson, B. S., & Wright, D. W. (1996).Understanding and treating post-traumaticstress disorder symptoms in female partnersof veterans with PTSD. Journal of Marital and
Family Therapy, 22, 455-467.
Neumann, D. A., Houskamp, B. M., Pollock, V.E., & Briere, J. (1996). The long-term seque-lae of childhood sexual abuse in women: Ameta-analytic review. Journal of the American
Professional Society on the Abuse of Children, 1, 6-16.
O’Farrell, T. J., Choquette, K. A., Cutter, H. S.G., Floyd, F. J., Bayog, R. D., Brown, E. D.,Lowe, J., Chan, A., & Deneault, P. (1996).Cost-benefit and cost-effectiveness analysesof behavioral marital therapy as an additionto outpatient alcoholism treatment. Journal of
Substance Abuse, 8, 145-166.
O’Leary, K. D., & Beach, S. R. H. (1990).Marital therapy: A viable treatment for de-pression and marital discord. American
Journal of Psychiatry, 147, 183-186.
O’Leary, K. D., Heyman, R. E., & Neidig, P. H.(1999). Treatment of wife abuse: A compari-son of gender-specific and couples ap-proaches. Behavior Therapy, 30, 475-505.
Winter 2003 401
Rabin, C., & Nardi, C. (1991). Treating post-traumatic stress disorder couples: A psy-choeducational program. Community Mental
Health Journal, 27, 209-224.
Resick, P. A., & Schnicke, M. K. (1993).Cognitive processing therapy for rape victims: A
treatment manual. Newbury Park, CA: SagePublications.
Resick, P. A., Nishith, P., Weaver, T. L., Astin,M. C., & Feuer, C. A. (in press). A comparisonof Cognitive Processing Therapy withProlonged Exposure and a waiting conditionfor the treatment of chronic post-traumaticstress disorder in female rape victims. Journal
of Consulting and Clinical Psychology.
Riggs, D. S. (2000). Marital and family therapy.In E. B. Foa, T. M. Keane, & M. J. Friedman(Eds.), Effective treatments for PTSD (pp. 280-301). New York: The Guilford Press.
Riggs, D. S., Byrne, C. A., Weathers, F. W., &Litz, B. T. (1998). The quality of intimate re-lationships of male Vietnam veterans:Problems associated with posttraumaticstress disorder. Journal of Traumatic Stress, 11,87-102.
Rosenheck, R., & Nathan, P. (1985). Secondarytraumatization in children of Vietnam veter-ans. Hospital and Community Psychiatry, 36,538-539.
Rothbaum, B. O., Meadows, E. A., Resick, P., &Foy, D. W. (2000). Cognitive-behavioraltherapy. In E. B. Foa, T. M. Keane, & M. J.Friedman (Eds.), Effective treatments for PTSD:
Practice guidelines from the International Society
for Traumatic Stress Studies (pp. 60-83). NewYork: The Guilford Press.
Savarese, V. W., Suvak, M. K., King, L. A., &King, D. W. (2001). Relationships amongalcohol use, hyperarousal, and marital abuseand violence in Vietnam veterans. Journal of
Traumatic Stress, 14, 717-732.
Spanier, G. B. (1976). Measuring dyadic adjust-ment: New scales for assessing the quality ofmarriage and similar dyads. Journal of
Marriage and the Family, 38, 15-28.
Spielberger, R. L., & Lushene, R. E. (1989).State-Trait Anxiety Scale. ConsultingPsychologists Press.
Straus, M. A., Hamby, S. L., McCoy, S. B., &Sugarman, D. B. (1996). The RevisedConflict Tactics Scales (CTS2): Developmentand preliminary psychometric data. Journal
of Family Issues, 17, 283-316.
Sweany, S. L. (1987). Marital and life adjustment
of Vietnam combat veterans: A treatment outcome
study. Unpublished doctoral dissertation,University of Washington, Seattle.
Tarrier, N., Pilgrim, H., Sommerfield, C.,Faragher, B., Reynolds, M., Graham, E., &Barrowclough, C. (1999). A randomizedtrial of cognitive therapy and imaginal expo-sure in the treatment of chronic post-trau-matic stress disorder. Journal of Consulting and
Clinical Psychology, 67, 13-18.

402 the Behavior Therapist
Tarrier, N., Sommerfield, C., & Pilgrim, H.(1999). Relatives’ expressed emotion (EE)and PTSD treatment outcome. Psychological
Medicine, 29, 801-811.
Weathers, F. W., Litz, B. T., Herman, J. A.,Huska, J. A., & Keane, T. M. (1993,November). The PTSD Checklist (PCL):
Reliability, validity and diagnostic utility. Paperpresented at the 9th Annual Conference ofthe ISTSS, San Antonio, TX.
Zayfert, C., Becker, C. B., & Gillock, K. G.(2002). Managing obstacles to the utiliza-tion of exposure therapy with PTSD pa-tients. In L. VandeCreek & T. L. Jackson(Eds.), Innovations in clinical practice: A source
book (pp. 201-222). Sarasota, FL:Professional Resource Press. �
Iwas trained as a cognitive-behavioralclinical psychologist with an emphasison research. My training was not too
atypical. There has been a trend over at leastthe last three decades for many of the topdoctoral programs to have a similar empha-sis. This trend looks like it will continue. Mythesis—my epiphany—is that the orienta-tion associated with this training is prob-lematic. This training produced what Ithink may be most aptly described as an ap-plied epistemologist—i.e., someone whohas excellent critical abilities regardingknowledge claims—but it produced a verylimited psychologist, someone who isskilled at understanding why people behaveas they do. Let me explain.
I was trained—well trained, I think—tohear knowledge claims and to evaluate theevidence and logic associated with these. Ifsomeone (a colleague or even a client) saidthat Person X was depressed, I was welltrained to evaluate and criticize the qualityof this claim, for example, by evaluating thepsychometrics of the assessment data, bythe degree of independent, convergentsources of information, and even to evaluateto what extent the construct of depressionmade sense, all in an effort to determine to
what level this inference was warranted.Similarly, if a colleague wanted to use a par-ticular therapy, I was well trained to evalu-ate the quality of the outcome research todetermine if some bar of acceptability waspassed. In fact, much of my “growth” aftergraduate school was learning how to beeven better at evaluating these claims. Ilearned about additional topics such as clin-ical significance, social validity, meta-analy-sis, path analyses—how to evaluateknowledge claims with even more tools andat times even higher standards. I could evenapply these generic critical skills to topicsoutside of psychology—the arguments forabortion or against school prayer. This iswhy I say I became what philosophers oftencall a critical rationalist; my focus was honingskills to critically evaluate beliefs andknowledge claims. I wasn’t unique (al-though I did have a somewhat unique pathas I studied philosophy and philosophy ofscience for 4 years at the graduate level). Mycolleagues also had these skills and this ori-entation.
This worldview—seeing humans asepistemic agents—has deep roots inWestern civilization. The ancient Greeksdefined humans as “rational animals” and a
key goal was to “know thyself.” Notice theterms “rational” and “know” (but don’t for-get the term “animal”!). TheEnlightenment and the rise of science em-phasized refinements and more emphasisupon more careful analysis of knowledgeclaims. Indeed, certain kinds of defects inrationality came to be the essence of defin-ing madness, insanity, or abnormality(Beck, Rush, Shaw, & Emery, 1979; Ellis &Grieger, 1977; but especially see Sass,1992). With this orientation, the epistemicemphasis in psychology followed: Look todefects in rationality to understand abnor-mal behavior and its cures.
But what happened to “the animal”?Taking a closer look at the Greeks and otherthinkers, we see that they had a very largeand important role for our animal, arationalnatures (see O’Donohue & Lloyd, 2003).Reason battled against the arational “pas-sions.” Even the medievals saw this battle,reason fought against the Seven DeadlySins: lust, gluttony, sloth, greed, etc. Muchlater in intellectual history, Nietzsche’s di-alectic involving the clean, orderly, rationalAppollian versus the chaotic, passionate,carnal Dionysian also superbly capturedthis contrast. What place do “the pas-sions”—lust, aggression, and greed—andthe Dionysian have in contemporary psy-chology, particularly contemporary cogni-tive behavior therapy? They seem to be inthe shadows, influencing the well-illumi-nated rationality. Why aren’t they exam-ined in the bright light?
My claim is that this epistemic emphasis(it can even be called rationalistic macho-ism) moved me away from being a betterpsychologist. When I listened to people orhad interactions, I listened to their knowl-
Open Forum
Rational Animals: Behavior Therapy’s Focuson Knowledge and the Understanding ofHuman Behavior
William O’Donohue, University of Nevada, Reno
ListserveReconnect with
the worldwide
membership
of AABT.
WWW.AABT.ORG
Click on the
bouncing ball.
is back
AABT

Winter 2003 403
edge claims (and even evaluated my knowl-edge claims about their knowledge claims)and evaluated the extent to which thesewere warranted. This was literally “my ex-perience.” I did not attend to the arational(e.g., the emotional motivations associatedwith the claim) or fully understand the ara-tional and thus I missed much of what wasactually happening. I missed, to be blunt,that people are much more than epistemicagents.
A first step along the path can be the re-alization that people have some of the be-liefs and make some of the knowledgeclaims they do for other than rational, evi-dential reasons. To be sure, some folks makethese claims because they fairly simply anddispassionately want to know, want to in-quire, and want to debate in the GrandConversation. But, at times, are there othermotivations? Are some people makingknowledge claims partly because they de-sire attention/recognition? Because theyseek power? Because they have aggressivedrives (e.g., Can criticism be aggressive?)Or do they make claims (perhaps at a lowfrequency and very qualified, and very“conservative”) because they fear being ex-posed as an imposter—as stupid or igno-rant? Are their claims doctrinaire becausethey need the security of group member-ship? Finally, are their arguments and evi-dence for their claims slippery and shoddybecause of psychopathic tendencies? I haverecently learned it is useful to look at thepsychology of the person making the claims—their fears, motivations, and needs insteadof simply focusing on the claim and its sup-porting argument. This is not an invitationto make ad hominem arguments—i.e., in-valid criticisms of reasoning that refer tosome characteristics of the person makingthe argument. It is a move away from thesimplistic notion that the only motivationfor a person to make Claim X is that theyare (perhaps) in an epistemic position to doso. And I believe it is a move toward one ofthe ultimate aims of both the scholar andthe therapist: to be persuasive. Being per-suasive involves understanding the psychol-ogy of the person as well as the evidentialbasis for the claim.
But this still does not go far enough. Thelesson I am claiming worth knowing is not,“When people make knowledge claims, un-derstand the person making the claim” (al-though this is part of it). What I am sayingis more like, “Understand people. Theirknowledge claim-making component (i.e.,what philosophers call their epistemic agency) isonly a part—sometimes only a smallpart—of such understanding.”
I believe I’ve made this error for fourprinciple reasons, three of which are com-mon to many of the readers and one ofwhich is somewhat unique. Psychologytraining has emphasized research method-ology. In some ways research methodologyis our core. Research methods are, inessence, applied epistemology. Their focusis on gaining knowledge and puttingknowledge claims to the test. One can seehow this core can lead to the basic orienta-tion I have described. Second, I was trainedas a cognitive-behavior therapist. Behaviortherapists tend to be hard-nosed, research-oriented folks—again, oriented to claimsand evidence. Cognitive therapy, on theother hand, is applied epistemology—eval-uating beliefs that lead to problems andteaching better belief formation(O’Donohue & Vass, 1996). Third, I won-der if this orientation comes from a personalneed, perhaps widely shared, to see life asorderly, rational, and knowable, and thatthe arational and irrational (to use Gellner’sfelicitous phrase, the “cunning of unrea-son”) is disturbing and anxiety provoking.
The unique reason (and this is more of ahopefully somewhat interesting side line) isthat during my training as a philosopher Ilearned much about the philosophy of sci-ence of Karl Popper and the neo-Popperians(e.g., Lakatos and Bartley). Popper’s ontol-ogy (on what there is) asserts the existenceof three worlds. Each world consists of dif-ferent kinds of existences. World 1 consistsof all physical objects. World 2 of all psy-chological events, including actual beliefs,thoughts, and emotions, experienced byreal people. World 3 contains intellectualproducts: arguments, books, claims, andevidence. World 3 objects can be evaluatedwithout reference to real people. Py-thagoras’ theorem can be evaluated withoutany reference to Pythagoras the person. Mypurpose here is not to argue for the sound-ness of this ontology but rather to point outhow this disposed me to forget the psychol-ogy involved in all of this. I lived in World 3and largely ignored World 2.
What are my positive proposals?
1. See people as (arational and rational)psychological entities (i.e., with motivations,fears, and guilt), not only as epistemic enti-ties. The question becomes, What are the
most useful noncognitive constructs to fill out this
picture?
2. Develop a research agenda into therational/arational model of human behav-ior, perhaps even drawing on other tradi-tions within psychology that have seen this.The goal is to provide useful assessments

404 the Behavior Therapist
and therapies that take into account thesefactors.
There are three (interrelated) general argu-ments against this “warmer” approach: (a)The ontic argument: These entities justdon’t exist. These constructs associatedwith the arational are in a similar state topoltergeists and devils. If one talks aboutthese, then one is talking about nothing. (b)The epistemic argument: Even if they exist,we can’t know them. This is an epistemicbar/detection-measurement issue (ontologyand epistemology are interconnected andthus so are 1 and 2. (c) Even if they exist andthey can be known, they aren’t useful in thedescription, prediction, and control ofhuman behavior. Let me briefly examineeach of these issues.
They Don’t Exist
This is phenomenologically false. Weknow directly that we have experiencessuch as felt motives, fears, guilt, needs, fan-tasies, conflicts. We directly experience ouranimal/emotional/instinctual/Dionysian na-tures (at least part of this). We don’t per-haps know all of it, may perhaps haveunrecognized components of this, and mayneed a good taxonomy to organize it, but toany reasonably observant person this claimis obviously false.
Second, science is ultimately pragmatic,and if talk of these constructs results in bet-ter outcomes, then this conceptualizationwins and these entities are construed as “ex-isting” (see Quine’s 1980 work on what ex-ists—bound variables in the best scientifictheories).
We Can’t Measure These
Reliably and Validly
Basically we won’t know until we try.Some progress has been made, but this ar-gument is too general. If we look at thetotal number of constructs psychologists ofall persuasions use and the actual evidencethat they can measure these well, we’d findthat the vast majority of constructs are notmeasured well. Some of the hard scientificpsychology folks have similar problems(show me a person’s “reinforcement his-tory”). Second, some progress has beenmade in measuring these constructs.Admittedly more work needs to be done.This does not mean I think something likethe Rorschach is what is needed. But it is anargument to understand and attempt to as-sess that rational but still cognitive andemotional forces influence human behavior.This argument is basically an epistemic one:
The issue is that they cannot be known. Letme spend a bit of time on a meta-issue.
Epistemic Bars, What ConstitutesKnowledge, and What Might Need to Bein Our Net
This is a direct relationship betweenwhat epistemic criteria we hold and whatgets into our net. The philosophy of RenéDescartes shows this lesson clearly.Descartes wanted to make sure he did nothold a false belief and so he set the epistemicbar very high. Basically he said that a claimcould not count as knowledge unless it was“clear and distinct” and “indubitable”—lit-erally not capable of being doubted. Heeven used an “evil genius” as a heuristic tooperationalize the second criterion.
This evil genius was omnipotent and in-tent on doing all in his power to deceivepoor Descartes. Thus, for example,Descartes concluded that none of his sen-sory data could count as knowledge becausethe evil genius could simply be tricking hissenses. The only belief that passed both cri-teria was “I think.” (Deception, Descartespointed out, implied a thinking entitybeing deceived.) From “I think” Descartesargued that “I exist” could be indubitablyinferred. And that was about it. This episte-mological bar admitted only Descartes’cogito, “I think, therefore I exist.”
Descartes was in a pickle. He didn’twant to stop there. Solipsism isn’t all thatinteresting, particularly in the historicalcontext of the early Enlightenment.Descartes admitted other beliefs, such asthe existence of the world through an (in-valid) ontological argument for the exis-tence of God. (Basically this argument goes,“I have a thought of God, a perfect being.The only way I can have a thought of such aperfect being is for such a perfect being toactually exist because only a perfect beingcan cause the thought of its existence.”)Because this perfect being is all good, hedoes not want to deceive, and thereforeDescartes could believe in the verdicalnessof his senses and consequently the existenceof the world.
Descartes’ epistemic bar is too high. Notenough passes to say much of interest aboutthe world. Bars, obviously, can be too low—and as a field we’ve paid a lot of attention tothis problem. But have we paid insufficientattention to the other problem? Have webeen too concerned with epistemology andset our epistemic bar too high? Is there a di-alectic here—between epistemic standardsand admitting the “right stuff ” of what ittakes to understand humans? Note also
that this happens commonly in the sciences.If astronomy were held to an experimentalbar (that is, astronomers had to manipulateindependent variables before they couldmake a knowledge claim), astronomerswould be able to make only a small fractionof their current knowledge claims.
Let me ask my new style question: Howmuch have we ignored the irrational andarational because of our needs (associatedwith being a researcher and intellectual) tosee the world in dispassionate, rationalterms?
What is it to see a person as a complexpsychological entity rather than simply asan epistemic agent? These are the kinds ofentities I think might need more attention.Here’s a quick list:
arational needs (e.g., sex and aggression; recognized and unrecognized)
ambivalence
core interpersonal styles and conflict patterns
image of self
secrets and shame
implicit agendas
narcissistic and power drives
developmental blocks/issues
blind spots (motivated and unmotivated),and the processes that create these
The person with these constructs is seenas an epistemic agent but also as a needy,emotional, somewhat confused, somewhatambivalent, somewhat deceptive, some-what fearful, somewhat proud, somewhataggressive, somewhat ashamed, somewhatharmed by past difficulties individual con-structing façades to self and others to hidesome of these irrationalities and embarrass-ments. And of course there are huge indi-vidual differences in the valences andmagnitudes of each of these dimensions.This, I think, is a more interesting and fruit-ful conceptualization of human behavior. Ahuman being is seen as much more than anepistemic agent. How do we balance epis-temic standards and not make the Cartesianmistake to gain some of the content ofthese, while at the same time not becomingcareless epistemically?
We can have reasonable epistemic stan-dards and still adopt this basic view of a per-son. After all, even the behavioral positionsees arational mechanisms as its two majordeterminants of human behavior. The “con-tingencies of survival” are not rational, theysimply determine the probability of surviv-ing and reproducing. The same thing is trueabout the “contingencies of reinforcement,”except the stuff acted on is behavior instead

Winter 2003 405
of people (or gene pools). Some of theabove-listed entities can be translated intoother systems’ vernaculars.
We have two orthogonal dimensions:humans as rational agents versus arationalbeings. We also have epistemic standards(say, high or low) to know these. Note that acomfortable place for some people—andstill a more broad view—is high epistemicstandards applied to understanding the ara-tional elements of human behavior. Thehighest risk and scariest category is lower(although still “acceptable”) standards ap-plied to the arational.
They Are Not Scientifically Useful
There is an important distinction tomake in this claim. First is the case in whichthey have been tried and found to be notuseful. The second is the case in which theyhave largely been untried and the issue isthat we really don’t know how useful theywill prove to be. My claim is that we are in
the second case, not the first. And then itcan be useful (depending perhaps on whatindividual researchers see as most plausible)to place bets on these horses.
Conclusion
Let me close by saying there is no doubtthat this is somewhat controversial. Pleasedon’t counterargue by using a slippery slopeargument—that is, “If we lower our epis-temic standard, then we accept all kinds ofgobbledygook.” This is a red herring. Onecan lower epistemic standards (and I couldargue we actually do this in our day-to-daylives to function). We don’t have to becomedogmatists or irrationalists, we just need totitrate to let into our nets some interestingand potentially useful constructs. We needto have epistemic standards that connectwith and illuminate our problems. If as-tronomers had epistemic standards that al-lowed beliefs to be counted as knowledgeonly if these beliefs were evaluated by ex-
perimental evidence, we’d know nothingabout the planets.
References
Beck, A. T., Rush, A. J., Shaw, B. R., & Emery, G.(1979). Cognitive therapy of depression. NewYork: The Guilford Press.
Ellis, A., & Grieger, R. (1977). Handbook of ratio-
nal-emotive therapy. New York: Springer.
O’Donohue, W., & Lloyd, A. (2003). Enhanced
cognitive therapy. Manuscript in preparation.
O’Donohue, W., & Vass, J. (1996). What is an ir-rational belief? Rational-emotive therapyand accounts of rationality. In W.O’Donohue & R. Kitchener (Eds.), The phi-
losophy of psychology. London: Sage.
Sass, L. (1992). Madness and civilization. NewYork: Basic Books.
Quine, W.V.O. (1980). From a logical point of view
(pp. 20-46). Cambridge, MA: HarvardUniversity Press. �
Epicurus (341–270 B.C.E.) was a Greekphilosopher who advocated ideassimilar to those embraced in rational-
emotive theory (Ellis, 1962; Lazarus, 1971).His history shows the extraordinary appealof the rational-emotive approach. For 700years Epicurus’ teachings were popularamong Greeks, Romans, barbarians,Syrians, Jews, Egyptians, Africans, andGaulists (Inwood & Gerson, 1994; Russell,1977). Followers wore his likeness on ringsand created statues in his honor. His mosteminent disciple was Lucretius (99–55B.C.E.), the great Roman poet.
Epicurus is one of history’s most influ-ential hedonists. Hedonists hold that theroad to a good life comes from maximizingpleasure and minimizing pain. This mayseem straightforward, but there are prob-lems with hedonism that are not immedi-ately apparent. The advice to maximizepositive feelings leads to a lifestyle of plea-sure seeking, but pleasure seeking often in-creases risk of future pain and suffering.Feasting, for example, increases the risk ofindigestion. Thrill seeking is fun but dan-
gerous. Alcohol consumption feels good atfirst but leads to hangover. Nearly every he-donist of historical significance advocatedthat it is more important to minimize painand suffering than to maximize pleasure.Epicurus was no exception: He taught thatthe pain of indigestion outweighs the plea-sures of a feast.
Epicurus’ philosophy is not what psy-chologists think it is. Although remem-bered for advocating the pleasure-seekingphilosophy of “eat, drink, and be merry,”Epicurus actually advocated the opposite,advising only to eat what was necessary be-cause one does not want indigestion, todrink as little as possible because one doesnot want hangover, and to keep the merri-ment to a minimum to avoid exhaustion.He was no connoisseur of gourmet food,and he did not have a highly refined sense oftaste. The man for whom the word “epi-cure” was coined taught that a meal of bar-ley cakes and water will taste good whenyou are sufficiently hungry.
Epicurus thought that the best strategyin life is to minimize anxiety and pain. He
was quoted as having said that we should doeverything for the sake of being neither inpain nor in fear. He believed that the ab-sence of pain and anxiety was an essential el-ement of the good life. For example, headvised his followers to keep romance to aminimum. Although sex is enjoyable, manyrelationships deteriorate toward disillusion-ment, argument, and boredom. How can aperson maintain a tranquil lifestyle goingthrough the frustrations of love? Romanceis often not worth it because “the thingswhich produce certain pleasures bring trou-bles many times greater than the plea-sures.”
How could a resident of the ancientworld reduce worry and stress when war,famine, disease, and economic depressionswere common? According to Epicurus, thekey to reducing worry is to control ourthoughts. People need to embrace the fol-lowing four beliefs (“points of rational em-phasis”):
God does not judge us. Death is not unpleasant.What is good is easy to get.What is terrible is easy to endure.
We will consider each of these pointsseparately.
1. Epicurus taught that the fear of divinejudgment is irrational. Because God is astate of bliss—a state of maximum possiblehappiness—he will not interrupt the blissto pay attention to us. Since He is not payingattention, God will not bother to judge usafter we die. Once we embrace this rational
Open Forum
Epicurus: The First Rational-EmotiveTherapist
Steven Reiss, The Ohio State University

406 the Behavior Therapist
analysis of divinity, we will stop worryingabout the afterlife.
2. Because we will not experience anxi-ety and pain after we die, we should neitherworry nor fear death. “Death is nothing tous,” Epicurus taught. “For what has beendissolved has no sensory experience, andwhat has no sensory experience is nothingto us” (Hutchinson, 1994, p. 7).
3. We can avoid worrying about moneyby embracing a simple and inexpensivelifestyle. Only if we desire more than whatis necessary to sustain life do we risk disap-pointment. Rather than strive to bewealthy, which is difficult to do, we shouldlower our expectations, which is easy to do.After our expectations are adjusted, thebasic necessities will bring as much joy to usas luxury brings to the wealthy.
4. We can endure any tragedy and mini-mize pain by controlling how we think. It isbest to be optimistic, expecting that anypain in our lives will be brief, bearable, andnot intense. We should not exaggerate anytragedy in our mind (do not catastrophize).We should focus on the positive aspects ofexperience and forget the negative aspects.When faced with inescapable disaster, wecan minimize the pain and suffering by re-maining calm. Worry and emotional dis-tress only make the experience moreunpleasant than it already is. Dying is lesspainful if one does not whimper about it.(Epicurus allowed, however, that even peo-ple who embrace his philosophy moan andgroan when being tortured on the rack.)
Epicurus’ ideas, and the basic assump-tions of rational-emotive theory, are similarin a number of significant ways. Bothschools hold that cognitions are the key tocontrolling emotions. Whereas Epicurustaught people to reduce stress and worry bychanging their beliefs, expectations, and in-terpretations, rational-emotive theoristshold that changing irrational ideas is thekey to improvement in anxiety and stressdisorders (Ellis, 1962; Lazarus, 1973).Under both approaches, the ultimate rea-son to embrace cognitions is to reduce anxi-ety and worry or improve symptoms ofpsychopathology. The alternative idea—that we should embrace cognitions basedon their validity, not based on how theymake us feel—was deemphasized in theworks of both Epicurean and rational-emo-tive theorists.
In certain key respects, Epicurus washistory’s first influential rational-emotivetheorist. His focus, not unlike that of a ra-tional-emotive therapist, was to make peo-ple worry less and feel better. His techniquewas to change cognitions by arguing ratio-
nally. In his system, a “rational” person em-braces stress-reducing thoughts and rejectsstress-enhancing thoughts. Arguing thatbelieving in a nonjudgmental God is a lessstressful idea than believing in a judgmentalgod, Epicurus concluded that the rationalperson should embrace the nonjudgmentaldeity.
The extraordinary appeal of Epicurus’ideas had much to do with the promise ofcontrol over the emotional consequences oflife in an unpredictable, violent, and chaoticworld. Although we cannot control events,we have the potential to control our emo-tional reaction to those events and the con-sequences of events for our personalhappiness. During the Hellenistic period ofhistory, there was little individuals could doto control their fate. Wars and natural disas-ters were common, resulting in famine.Diseases were poorly understood and medi-cine was primitive. Poverty was a reality;there were no government safety nets.
In a frightening and uncontrollableworld, Epicurus’ philosophy offered peoplea measure of control. The key to happinessis our feelings, our feelings are determinedby our interpretations of events (not somuch the events themselves), and we cancontrol how we interpret things.
In conclusion, Epicurus expressed ideassimilar to those that underlie rational-emo-tive theory. His work had extraordinary ap-peal, partially because it offered people ameasure of control in an unpredictableworld. The conclusion that Epicurean phi-losophy and rational-emotive theory aresimilar does not have implications for thevalidity of rational-emotive theory, but itdoes provide an interesting context for ra-tional-emotive theory. These ideas had a700-year run the last time they surfaced,and I suspect they will remain a focus ofpsychology for quite some time.
References
Ellis, A. (1962/1973). Reason and emotion in psy-
chotherapy. New York: Lyle Stuart.
Hutchinson, D. S. (1994). Introduction. In B.Inwood & L. P. Gerson (Eds.), The Epicurus
reader. Indianapolis: Hackett Publishing.
Inwood, B., & Gerson, L. P. (1994). The Epicurus
reader. Indianapolis: Hackett Publishing.
Lazarus, A. A. (1971). Behavior therapy and be-
yond. New York: McGraw-Hill.
Russell, B. (1977). A history of Western philosophy.New York: Simon & Schuster. �
International
Association of
Cognitive
Psychotherapy
(IACP)
The Journal of Cognitive
Psychotherapy
Join the IACP and receive the
Journal, The International News-
letter, the IACP Listserve, informa-
tion on workshops, conferences and
jobs, discounts on auto rental,
hotels, journals, and conferences.
Get the Journal with the
leaders in the field—
. . . all for $55 per year!
Contact our Webpage for the
membership application:
http://iacp.asu.edu
or
http://jcp.asu.edu
L. Abramson
L. Alloy
A. T. Beck
J. Beck
D. Burns
D. M. Clark
F. Dattilio
R. DiGiuseppe
E. T. Dowd
A. Ellis
N. Epstein
A. Freeman
R. L. Leahy
M. Mahoney
C. Padesky
J. Persons
J. Safran
P. Salkovskis
Z. Segal

Winter 2003 407
CallDistinguished/Outstanding Contribution by an Individual for Research Activities
On a rotating annual basis, one of the following three types ofdistinguished contributions by an individual member of AABTwill be recognized at the Annual Convention: research, clinical,or educational/training. For 2004, we seek nominations fromAABT members concerning outstanding research contributions.Eligible candidates for this award should be members of AABTin good standing who have provided significant contributions tothe literature advancing our knowledge of behavior therapy.Applications should include a letter of nomination, at least threeletters of support, and a curriculum vitae of the nominee.Please send an e-mail version as well as a hard copy of all nom-ination material to the program chair at the address below, plus,send 1 duplicate copy of your submission to AABT, OutstandingResearch Award, 305 Seventh Ave., New York, NY 10001. Pastrecipients of this award are Alan E. Kazdin in 1998 and DavidH. Barlow in 2001.
Outstanding Training Program This award will be given to a training program (not an indi-
vidual) that has made a significant contribution to trainingbehavior therapists and/or promoting behavior therapy. Trainingprograms can include graduate (doctoral or master’s), predoc-toral internship, postdoctoral programs, institutes, or continuingeducation initiatives. Nominations for outstanding education-al/training programs should be accompanied by a brief sum-mary of information in support of the nomination, as well as anyother supporting materials deemed essential for review of theprogram.
Please send an e-mail version as well as a hard copy of allnomination material to the program chair at the address below,plus, send 1 duplicate copy of your submission to AABT,Outstanding Training Program Award, 305 Seventh Ave., NewYork, NY 10001. Past recipients of this award include Universityof Georgia’s Clinical Psychology program; the ClinicalPsychology Training Programs at Rutgers, the State University ofNew Jersey; the Clinical Psychology Training Program at WestVirginia University; the Psychology Internship and PostdoctoralPrograms at Wilford Hall Medical Center; and University ofWashington Clinical Ph.D. Program.
Virginia A. Roswell Student Dissertation AwardThis award will be given to a student based upon his or herapproved doctoral dissertation proposal. The research shouldbe relevant to behavior therapy. Accompanying this honor will
be a $1,000 award to be used in support of research (e.g., payparticipants, purchase testing equipment) and/or to facilitatetravel to the AABT convention. Eligible candidates for thisaward should be student members, have already had their dis-sertation proposal approved, and be investigating an area ofdirect relevance to behavior therapy, broadly defined. A stu-dent’s dissertation mentor should send a letter of nominationand provide a 3- to 5-page summary of the proposal. Anythinglonger than 3 to 5 pages will not be considered. The summaryshould minimally include a brief introduction to the area ofresearch, methodological design, and a description of the par-ticipants. Please send an e-mail version as well as a hard copyof all materials to the program chair at the address below, plus,send 1 duplicate copy of your submission to AABT, StudentDissertation Award, 305 Seventh Ave., New York, NY 10001.
Three additional awards will be presented annually.
CCaarreeeerr//LLiiffeettiimmee AAcchhiieevveemmeennttDDiissttiinngguuiisshheedd FFrriieenndd ttoo BBeehhaavviioorr TThheerraappyyOOuuttssttaannddiinngg SSeerrvviiccee ttoo AAAABBTT
Nominations for these awards are solicited from the mem-bers of AABT governance. (This award program does notreplace those awards offered by certain segments within AABTsuch as the President’s New Researcher Award, Elsie RamosStudent Poster Award, or those awards offered by individualSIGs. Attempts are made to avoid duplication in a given year.)
To make this a successful program, we need your help.Please e-mail and regular mail nominations to:
JJoohhnn CC.. GGuutthhmmaann,, PPhh..DD..,, CChhaaiirrAAAABBTT AAwwaarrddss aanndd RReeccooggnniittiioonn CCoommmmiitttteeee113311 HHooffssttrraa UUnniivveerrssiittyyHHeemmppsstteeaadd,, NNYY 1111554499TTeell..:: 551166--446633--66779911ee--mmaaiill:: ccccccjjccgg@@hhooffssttrraa..eedduu
General suggestions about the annual AABT awards pro-gram are appreciated. Please forward your suggestions toAABT, 305 Seventh Ave., New York, NY 10001.
DEADLINE FOR ALL NOMINATIONS:
THURSDAY, APRIL 1, 2004
fo r Award Nominat ions
TThhiiss iiss aann ooppeenn ccaallll ttoo tthhee AAAABBTT mmeemmbbeerrsshhiipp ttoo
pprroovviiddee nnoommiinnaattiioonnss ffoorr tthhee ffoolllloowwiinngg aawwaarrddss,,
ttoo bbee pprreesseenntteedd aatt tthhee 22000044 CCoonnvveennttiioonn iinn
NNeeww OOrrlleeaannss..
10th Annual AABT Awards

408 the Behavior Therapist
Andrew Salter (1914–1996) was aclinical psychologist in private prac-tice who made enormous contribu-
tions to behavior therapy. Conditioned Reflex
Therapy, only one of his books, was firstpublished in 1949. The book was reissuedto celebrate the 50th anniversary of its pub-lication. With some minor condensation,the book retains the richness, innovative-ness, and wisdom of the original. In addi-tion, the reissued version includes aforeword by Gerald Davison and an ex-tended introduction by William Salter, apsychologist and one of Andrew Salter’stwo sons.
Leaving aside the historical significanceof the work, the book stands on its own asan excellent account of a novel set of behav-ioral treatments applicable to diverse disor-ders. The book is remarkably engaging,clinically astute, and of great practicalvalue. However, it is the historical signifi-cance that deserves special attention. Thisfacet requires comment on the context andtime in which the book was published andhow the book and Salter’s work contributeddirectly to and anticipated much of contem-porary behavior therapy. I highlight thecontext as a way to convey why we are in-debted to Salter. At the same time, formany who knew him, I shall convey as wellsome of those features that made him amost unforgettable person in one’s life.
Salter received his undergraduate degreein 1937 (New York University). Among hismany interests was hypnosis. He drew uponthe work of the learning theorist ClarkHull, who had provided a learning-basedinterpretation of hypnosis. This view reliedon classical conditioning in which speechbecame conditioned stimuli that evoked re-actions in clients. Salter expanded on thisconcept and developed techniques of auto-hypnosis as a self-control technique (Salter,1941, 1944).
Salter continued his private practice anddeveloped therapy techniques based explic-itly on conditioning. The treatment, called
conditioned reflex therapy, drew directlyfrom the writings of Sechenov, Pavlov, andBechterev, but other learning theorists andresearchers as well. The reader may recallthat Sechenov, sometimes referred to as “thefather of Russian physiology,” discussed andexperimentally investigated “reflexes of thebrain” (i.e., inhibition and excitation in ani-mal research). Pavlov and Bechterev weredirectly influenced by this work and inmany ways continued the conceptual viewand research focus begun by Sechenov.Pavlov elaborated on the notions of excita-tion, inhibition, and disinhibition, conveyedthat they were processes within the brain,and could explain maladaptive (and other)behavior. Salter drew on these concepts ex-plicitly. He believed that excessive inhibi-tion in particular was responsible formaladjustment, and that the task was toachieve a balance between inhibition andexcitation. In most cases, the task of thetherapist was to increase excitation.Concretely, this meant encouraging expres-sion of emotions and positive actions ineveryday life. Expression of emotion wasnot based on a cathartic view. Rather, actionin everyday life and expression of how onefeels and thinks were critical.
Salter noted that the words of the thera-pist served as conditioned stimuli and couldinfluence the client’s nervous system inways to encourage behavior change. Thebehavior changes would influence the ner-vous system further, and this in turn wouldfoster further behavior change. This is cer-tainly an early version of bidirectionalchanges and reciprocal causality. However,the key to the contribution was in viewingmaladjustment and therapy from the stand-point of learning and then generating andapplying concrete techniques for therapy.Salter made the case with unequivocal clar-ity: “Maladjustment is malconditioning,and psychotherapy is reconditioning”(Salter, 1949, p. 316).
Context Highlights
Permit me to merely identify a fewpoints to situate Salter’s work and to conveywhy the writings and this book in particularconstitute formidable contributions. Thecontext includes early stirrings of behaviortherapy, conceived at the time as applica-tion of learning theory and research totreatment. It is useful to highlight the his-torical time line with familiar points merely.I have discussed a broader set of influenceselsewhere (Kazdin, 1978).
The context within psychology moregenerally in the early 1900s was the bur-geoning influence of learning theory and re-search. Psychology was moving to moreobjective methods of study than had beenemphasized (e.g., away from introspectionas a method of study and mentalistic de-scriptions and interpretations). Learningtheory and research and comparative psy-chology developed in earnest, as evident inthe first few decades of the 1900s in theworks of Thorndike, Guthrie, Hull,Skinner, and others. Watson’s (1919) for-malization of the movement of behaviorismat this time emphasized both objectivemethods of research (conditioning para-digms) and the importance of the work ofPavlov and Bechterev. Conditioning meth-ods and models were viewed as generalways of moving psychology forward. Forexample, in 1915, Watson’s presidential ad-dress at the American PsychologicalAssociation was titled, “The Place of theConditioned Reflex in Psychology.”
Conditioning was evident in researchand in the air but not much in therapy.Watson and his case studies to induce fear inLittle Albert (Watson & Rayner, 1920) andto eliminate fear in Peter (Jones, 1924a)were influential in advancing a behavioristview of psychology in general and in thecontext of psychopathology and psy-chotherapy more specifically. Jones, whowas one of Watson’s students and involvedin the case of Peter, completed a dissertationthat compared several methods of treatingfear in children, and that study alone pio-neered many innovations (e.g., demonstra-tion of graduated exposure and modeling aseffective therapy techniques; Jones, 1924b).
Isolated outcroppings of conditioning-based treatments emerged in which learn-ing research was drawn on directly toexplain existing treatments or to developnew treatments. For example, in 1938,Mowrer and Mowrer described the bell-and-pad method for controlling enuresis.The method was developed already but theMowrers cast this as classical conditioning.
Book Review
Salter, Andrew (1949; 2002— 50th-anniversary printing)
Conditioned Reflex Therapy: The Direct Approach to the
Reconstruction of Personality
Gretna, LA: Wellness Institute. (232 pp., ISBN 1-58741-048-6)
Reviewed by Alan E. Kazdin, Yale University School of Medicine

Winter 2003 409
The fact that the procedure was effectiveadded empirical frosting to the cake. In thelate 1930s and early 1940s, aversion ther-apy was used as a treatment for voluntarilyhospitalized individuals (Shadel Sanato-rium, Washington) who abused alcohol, in atreatment referred to as conditioned reflextherapy (Voegtlin, Lemere, & Broz, 1940).This work drew directly from Russian re-search on conditioning to develop aversivereactions to alcohol. Treatment was evalu-ated in several reports encompassing over4,000 patients and follow-up evaluation upto 13 years after treatment. This work wassophisticated (e.g., evaluation of abstinence,comparisons of multiple treatments, studyof moderators) and exerted its own influ-ence on behavior therapy.
The examples illustrate a few of manylargely independent efforts to apply condi-tioning concepts for therapeutic ends. I notethey are independent in the sense that theinnovators did not draw on each other, usu-ally did not know of each other’s work, andwere not wildly interested in beginning alarger movement of behavior therapy. Salteris a key figure in this history. In 1949, Salterdeveloped conditioned reflex therapy, quiteseparate from the use of the term associatedwith the treatment developed of individualswith alcohol abuse in the program men-tioned previously. Salter applied condition-ing much more broadly to therapy andtherapeutic problems than had been thecase previously.
At the time of Salter’s book, other im-portant writings helped launch the move-ment toward learning-based therapies.From the 1930s through the 1950s, severalauthors provided accounts of “normal” andabnormal behavior, personality, and psy-chotherapy in terms of learning (e.g.,Masserman, 1943; Mowrer, 1950). Thebest known of these is the book Personality
and Psychotherapy: An Analysis in Terms of
Learning, Thinking, and Culture, by Dollardand Miller (1950). This book provided acomprehensive theory of behavior andunited learning, psychopathology, and psy-chotherapy. Of special note, psychoanalyticconcepts related to symptom formation,conflict, transference, and others were ex-plained in terms of learning concepts.
Treatises on learning, psychopathology,and therapy provided the groundwork formany later developments. However, theyleft open a great need, namely, to movefrom the concepts of conditioning to newtreatment that could be used in clinicalwork. Salter explained therapy in learningterms too but also made the next criticalnext step, i.e., development of treatment
techniques that could be used in the contextof therapy. A few years later, Wolpe (1958)made a similar leap in the development ofsystematic desensitization.
The beginning of behavior therapy in-cluded many writings on conditioning andtheir application to treatment. A relatedbut distinguishable genre was a literaturecritically evaluating the prevailing concep-tualization of psychopathology and itstreatment (e.g., psychiatric diagnosis, med-ical models). Key writers whose names arefamiliar within behavior therapy (e.g.,Eysenck, Rachman) criticized the sub-stance, methods, unscientific nature, andplausibility of psychoanalysis, the dominantmodel at the time. Salter contributed to thisgenre as well with his inimitable vitality andstyle. For example, in lamenting the unsci-entific nature of key psychoanalytic con-cepts, he noted, “It is as easy to nail acustard pie to the wall as to pin down theFreudian speculations about the ‘death in-stinct’ and ‘aggression’” (Salter, 1962, p. 8;first published in 1952). Salter criticized therole of insight as a basis of therapeuticchange and continued his persuasive style inmaking the case by noting that “insight isnot necessarily accompanied by importantsymptom improvement. Often individualswith insight might as well be saying, ‘Mydentist is marvelous. My teeth still ache butI know all about my roots and root canals. Ican even read my own X-rays. . . . Really,you should try my dentist.’ “ (1962, p. 146).In this book, The Case Against Psychoanalysis,Salter drew heavily on quotes of Freud andthe writings of others to make the case and tohelp set a context from which new therapiesemerged.
As behavior therapy developed, therewas a move away from criticizing psycho-analysis and traditional models of psy-chopathology and therapy in general. Bythe mid-1960s behavior therapy was devel-oping its own literature that included con-ceptual views, scores of case studies, and thebeginnings of an empirical literature thatcould stand on its own (Bandura, 1969;Krasner & Ullmann, 1965; Ullmann &Krasner, 1965). The task remained to spec-ify the treatments and to conduct researchto evaluate their effects and generalityacross problem domains and populations.
Conditioned Reflex Therapy andSalter’s Contributions
Salter’s leap from learning theory and re-search to treatments for clinical practice wasnovel and groundbreaking. He drew on abroad range of learning theorists and their
findings to explain the emergence of mal-adaptive behavior and the treatmentprocess. He made a critical distinction oftenneglected today, namely, between a theoryabout the onset of a problem (e.g., etiology)and a theory of change (how treatmentworks). They may or may not be related.For example, Salter noted that “finding andexploring the situations that have causedthe psychological difficulty does nothing tofacilitate the cure” (1949, p. 38). For practi-cal purposes, “how the individual ‘gets thatway’ is of little therapeutic importance” (p.143). Actually, in any given instance, how aperson developed the problem might be im-portant. Even so, Salter’s views underscorethe critical task of developing a theory oftherapeutic change, generating techniquesthat follow from that, and then applyingand testing the techniques in laboratoryand treatment contexts. These were novelviews.
In treatment, Salter focused primarilyon behavior as a way of achieving therapeu-tic change. “To change the way a personfeels and thinks about himself, we mustchange the way he acts toward others”(Salter, 1949, p. 100). The reader familiarwith early musings of cognitive therapy andcognitively based interpretations of therapywill recognize the position of later writers(e.g., Bandura, 1977), who noted that cog-nition is a key to sources of clinical problemsand/or therapeutic change. However, one ofthe best ways to modify cognitions isthrough action.
Salter did not believe improvementswould be gained if treatment were re-stricted to the therapist’s office. Clientswere instructed on how to perform in every-day life situations and were given extra-therapeutic tasks (i.e., homeworkassignments). In the treatment sessions,Salter used many adjunctive therapy tech-niques. For example, individuals who expe-rienced anxiety learned to relax to reducetension in stressful settings. They weretrained to relax in therapy and to apply thisskill to problematic situations in everydaylife, a procedure very closely resemblingwhat came to be known years later as invivo desensitization. Similarly, imagery con-nected with positive experiences or eventswere evoked to overcome other problems.For example, calmness would be inducedwith pleasant imagery to overcome anxietyor insomnia or to foster desired behaviorsuch as appropriate sexual functioning.These applications anticipated diverseforms of systematic desensitization as wellas covert conditioning.

410 the Behavior Therapist
In Salter’s Conditioned Reflex Therapy,several treatments are explicitly describedand applied to many cases. I mentioned sys-tematic desensitization and covert condi-tioning, but these cases illustrate othertechniques as well, including self-controltherapy and assertion training (later blend-ing into social skills training). These treat-ments all played a part in behaviormodification in the 1960s. Assertion train-ing in particular deserves special mentionbecause it is evident, without the term,quite explicitly in the book and did not takehold in research until 20 to 25 years later.
Salter’s work was carried out in a veryactive private practice. With a baccalaure-ate degree and novel experience and creden-tials, he was grand-fathered officially as aclinical psychologist. He did not have theacademic affiliations that may have givenhim an even more visible historical placethat I believe he unequivocally deserves.One only has to brush the surface of hiswritings to find many treatments and in-sights that characterize early behavior ther-apy and contemporary cognitive behaviortherapy. In terms of professional develop-ment, Salter organized the first conferenceon behavior modification in 1962 in collab-oration with Wolpe and Reyna. The pro-ceedings of this conference were laterpublished in book form (Wolpe, Salter, &Reyna, 1964), a time that preceded thetsunami of books on behavior therapy thatbegan in the 1970s.
Salter’s clinical work was not just an-other private practice. He routinely treatedwell-placed figures from diverse areas of lifeincluding the arts and movies. This was notminor; many outside of academia were in-fluenced by Salter and were vocal in his sup-port. His ideas in various degrees ofexplicitness found their ways into moviesand books outside of psychology because ofthe circles in which he provided treatment.
The Person
The scholarship, merit, prescience, andinsightfulness of Salter’s ideas stand on theirown and are critically important. Some-thing must be said about the man and hischaracter, although they can be readily sep-arated from his intellectual contributions.To facilitate this, permit me to switch fromreferring to him as Salter to Andy.
Andy was perhaps the most unforget-table character I ever knew. I met and be-friended Andy and Rhoda, his wife, in themid-1970s; Andy was in his 60s at thetime. He was a wonderful mix of boyishmischief and wisdom, plainly a young man
in the body of the older person. He was dy-
namic (although he would mock me gently
for using a word that in mixed company
might be interpreted as psychodynamic).
He sparkled in a room, was warm, engag-
ing, witty, and a raconteur without peer. He
was the kind of person to whom we gravi-
tated in a room. He was a constant per-
former but a willing audience. He and
Rhoda invariably were together, and if there
is another unforgettable character to com-
pete with this title, she would be the other
person. In ordinary social interaction, it is
often said that the opposite of speaking is
not listening but rather waiting to speak.
This would be quite untrue of Andy and
Rhoda. They had so much to say but lis-
tened, heard, and cared with equal intensity
and focus. If one were on a debating team,
an infinitely long voyage, or in need of com-
fort from a horrible personal loss, Andy and
Rhoda would be the choice partners.
A facet of history that may be relatively
superficial is to identify who was first in rela-
tion to an invention, device, or discovery.
Scholars often debate these details but those
of us who are merely lay persons in relation
to the issue are relatively indifferent. For ex-
ample, not many of us are concerned with
the fact that Pavlov was not the first to dis-
cover classical conditioning any more than
Columbus was the first to discover America.
We love or at least respect Ivan and Chris
because their contributions do not depend
on whether they were first. Similarly, cogni-
tive therapy has so many historical an-
tecedents before contemporary work,
including those by Salter, as to make any
reader clinically depressed. These an-
tecedents too do not distract from contem-
porary advances. Salter could arguably be
credited with firsts on several fronts in be-
havior therapy, including a handful of tech-
niques, a stable full of ideas, and a look
toward the future about what treatment
ought to be. He had, in my view, something
much better than a positive posthumous
crediting of his accomplishments, namely, a
rather amazing family, a set of friends who
loved and adored him, and patients who
were grateful to him for having changed
their lives. I expect that during his life the
present was amply rewarded, even though I
expect due credit was not provided fully in
the domains I have highlighted here. It is a
privilege to have the opportunity to men-
tion some of his major accomplishments,
even if only briefly here.
References
Bandura, A. (1969). Principles of behavior modifica-
tion. New York: Holt, Rinehart & Winston.
Bandura, A. (1977). Social learning theory.Englewood Cliffs, NJ: Prentice Hall.
Dollard, J., & Miller, N. E. (1950). Personality and
psychotherapy: An analysis in terms of learning,
thinking, and culture. New York: McGraw-Hill.
Jones, M. C. (1924a). A laboratory study of fear:The case of Peter. Pedagogical Seminary and
Journal of Genetic Psychology, 31, 308-315.
Jones, M. C. (1924b). The elimination of chil-dren’s fears. Journal of Experimental Psychology,
7, 382-390.
Kazdin, A. E. (1978). History of behavior modifica-
tion: Experimental foundations of contemporary
research. Baltimore: University Park Press.(Masochists Book of the Month, 1978-92.)
Krasner, L. A., & Ullmann, L. P. (Eds.). (1965).Research in behavior modification: New develop-
ments and implications. New York: Holt,Rinehart & Winston.
Masserman, J. H. (1943). Behavior and neurosis:
An experimental psycho-analytic approach to psy-
chobiologic principles. Chicago: University ofChicago Press.
Mowrer, O. H. (1950). Learning theory and person-
ality dynamics: Selected papers. New York:Ronald.
Mowrer, O. H., & Mowrer, W. M. (1938).Enuresis: A method for its study and treat-ment. American Journal of Orthopsychiatry, 8,436-459.
Salter, A. (1941). Three techniques of autohypno-sis. Journal of General Psychology, 24, 423-438.
Salter, A. (1944). What is hypnosis. New York:Richard R. Smith.
Salter, A. (1949). Conditioned reflex therapy: The
direct approach to the reconstruction of personality.New York: Capricorn.
Salter, A. (1952). The case against psychoanalysis.New York: Holt.
Ullmann, L. P., & Krasner, L. A. (Eds.). (1965).Case studies in behavior modification. New York:Holt, Rinehart & Winston.
Voegtlin, W. L., Lemere, F., & Broz, W. R.(1940). Conditioned reflex therapy of alco-holic addiction. III. An evaluation of presentresults in the light of previous experienceswith this method. Quarterly Journal of Studies
on Alcohol, 2, 501-516.
Watson, J. B. (1919). Psychology, from the stand-
point of a behaviorist. Philadelphia: Lippincott.
Watson, J. B., & Rayner, R. (1920). Conditionedemotional reactions. Journal of Experimental
Psychology 3, 1-14.
Wolpe, J. (1958). Psychotherapy by reciprocal inhibi-
tion. Stanford, CA: Stanford University Press.
Wolpe, J., Salter, A., & Reyna, L. J. (Eds.).(1964). The conditioning therapies: The challenge
in psychotherapy. New York: Holt, Rinehart &Winston. �

Winter 2003 411
Cognitive-behavioral therapy (CBT) isone of the most widely used and re-searched treatments for psychologi-
cal disorders (Barlow, 1988; Chambless &Gillis, 1993; Zinbarg, Barlow, Brown, &Hertz, 1992). In fact, in the past 30 yearswell over 1,000 studies have examined theefficacy of CBT for psychological disorders.
William Lyddon and John V. Jones, Jr.’sEmpirically Supported Cognitive Therapies:
Current and Future Applications unites thiswide body of research in a comprehensiveyet concise review of the theory, empiricalsupport, and implementation of cognitiveand cognitive-behavioral therapies for psy-chological disorders. Each chapter in thebook is devoted to a different psychologicaldisorder and includes a description of thetheory underlying the etiology and treat-ment of the disorder, a review of the empiri-cal support for the treatment, and a casestudy that illustrates the implementation ofthe cognitive-behavioral techniques.
Chapter 1 introduces the debate sur-rounding empirically supported treat-ments. The chapter begins with a historicalreview of psychotherapy research, begin-ning with Eysenck’s (1952) assertion thatthere is no evidence to support the effective-ness of psychotherapy. The chapter goes onto describe criticism of and support for theempirical evaluation of psychotherapy aswell as the importance of disseminatingsuch information to clinicians and studentsin training.
Chapter 2 provides a systematic reviewof empirically validated treatments forunipolar depression and includes a discus-sion of the process variables that have beenexamined as well as moderators, such as theworking alliance, homework compliance,and therapist contact. The authors also de-scribe mediators of change, such as hope-lessness and the effect that specifictreatment techniques can have on thesevariables. This chapter also demonstratesthe evolution of the cognitive theory of de-
pression, starting with Beck’s (1963) theoryand ending with more contemporary theo-ries emphasizing interpersonal schema andmetacognition. Finally, the authors illus-trate the implementation of cognitive ther-apy for depression in a complex case studyof an individual with comorbid unipolar de-pression and personality disorders.
In chapter 3, the authors describe a newand innovative CBT approach for individualswith bipolar disorder. The treatment pack-age helps clients to increase medicationcompliance, recognize patterns of moodfluctuation, decrease insomnia, and use cog-nitive restructuring to intervene on subsyn-dromal mood fluctuations. The chapter alsodescribes the implementation of this cut-ting-edge treatment in a clinical setting andillustrates each step of the process using acase study of an individual with bipolar dis-order and medication noncompliance.
Chapter 4 describes CBT for phobias, awell-documented and empirically validatedtreatment. The chapter provides step-by-step guidelines for the methods of treatingphobias and a case study demonstrating theuse of these guidelines.
Chapter 5 covers CBT for panic disorderand provides a well-documented table re-viewing the empirical support for CBT inpanic disorder. The chapter describes theimplementation and efficacy of the coretreatment components, psychoeducation,cognitive restructuring, relaxation, intero-ceptive exposure, and visualization as wellas research examining the efficacy of theseinterventions. Finally, the case study illus-trates these techniques as well as the impor-tance of utilizing a variety of means ofassessing outcome, including behavioralavoidance and cognitive change.
Chapter 6 approaches obsessive-com-pulsive disorder (OCD) from a purely cog-nitive perspective. It first cites researchdemonstrating that cognitive therapy is asefficacious as exposure and response preven-tion in the treatment of OCD. The authors
then describe the cognitive domains ofOCD targeted in cognitive therapy, includ-ing overestimation of danger, intolerance ofuncertainty, perfectionism, excessive re-sponsibility, overimportance of thoughts,and the need to control thoughts. The casestudy describes an 8-week brief cognitivetherapy which was effective in treatingOCD despite the restricted number of ther-apy hours, further lending support for theefficacy of this intervention. Finally, the au-thors provide a detailed description of vari-ous assessment methods that were utilizedin the case, including commonly used OCDmeasures such as the Yale-BrownObsessive-Compulsive Scale (YBOCS;Goodman et al., 1989) and measures ofoverall disability and functional improve-ment.
Chapter 7 discusses the efficacy of CBTfor PTSD and highlights the additive effectthat comorbid disorders can have on im-pairment associated with PTSD. The chapterfirst reviews the treatment outcome re-search supporting the use of cognitive be-havioral alternatives for PTSD treatment,such as cognitive processing therapy, pro-longed exposure, and stress inoculationtraining. The authors then describe a newand innovative treatment called MultipleChannel Exposure Therapy (MCET; Falsetti& Resnick, 1997), which targets comorbidPTSD and panic disorder symptoms. Theimplementation of this treatment is illus-trated through a complex case study of anindividual with a primary diagnosis ofPTSD resulting from multiple traumas, anda secondary diagnosis of panic disorder.
The final section of this book elaborateson new directions and developments in cog-nitive-behavioral treatments. These includeinterventions for such common but oftenunderresearched difficulties as anger man-agement and antisocial behaviors. For ex-ample, chapter 8 examines cognitivebehavioral techniques for addressing prob-lematic levels of anger. It reviews classic lit-erature on the treatment of anger andillustrates these well-supported techniquesthrough a description of therapy with an in-dividual with road rage. The case study alsohighlights the importance of assessingphysiological arousal, signs of physical ten-sion, and cognitive and behavioral symp-toms of anger when treating someone withanger management problems.
Another new direction, described inchapter 9, is the CBT of antisocial behaviorsin children and adolescents. The chapteraims to integrate a cognitive model of anti-social behavior with a family systems modelthrough the use of cognitive techniques tar-
Book Review
Lyddon, W. J., & Jones, J. V., Jr. (2001). Empirically
Supported Cognitive Therapies: Current and Future
Applications
New York: Springer Publishing Company
Reviewed by Amy Przeworski and Michelle G. Newman, The Pennsylvania StateUniversity

412 the Behavior Therapist
geting not only problematic behaviors in
the child or adolescent, but also the contri-
butions of parents, peers, communities, and
teachers. Consistent with this approach, the
case study describes therapeutic techniques
targeting both the child’s delinquent be-
haviors and the parent’s inconsistent and in-
effective disciplinary strategies. The treat-
ment also targets the parent’s coercive and
hostile interactive style.
Chapter 10 integrates a cognitive model
of eating disorders and a feminist perspec-
tive that emphasizes the importance of soci-
etal and cultural contributions to eating
disorders. This innovative approach is theo-
rized to improve upon existing treatments
for eating disorders by teaching clients to
explore their own core beliefs, as well as im-
plicit cultural and societal beliefs that are
communicated through such media as ad-
vertisements. Similar to a family systems
approach, this therapy aims to treat the
client within the context of his or her envi-
ronment in order to fully change the mal-
adaptive core belief structure and prevent
relapse. The chapter also provides client
handouts that may be helpful in teaching
clients to attend to personal reactions to ad-
vertising, identify cultural directives, and
critique core cultural beliefs in advertising.
The final chapter of the book describeslimitations of and future directions for psy-chotherapy research. The chapter high-lights the importance of empiricallysupported treatments in ensuring that thepsychotherapies administered to clients aresound. Nonetheless, it points to the need fora greater focus on ecological validity andpsychotherapy effectiveness research in clin-ical settings.
This well-written and organized book is afantastic resource for practitioners, teachers,and graduate students uniting 30-plusyears worth of research into a single smallvolume. The book integrates empirical re-search with illustrations of the implementa-tion of therapy techniques in clinicalsettings. Further, it includes complex casestudies in which comorbid diagnoses, med-ication noncompliance, and maintainingcontextual factors further complicate theimplementation of the techniques. Thus,we recommend this book as a means to be-come acquainted with recent research andthe application of empirically supportedtreatments.
References
Barlow, D. H. (1988). Anxiety and its disorders:
The nature and treatment of anxiety and panic.New York: The Guilford Press.
Beck, A. T. (1963). Thinking and depression. I.Idiosyncratic content and cognitive distor-tions. Archives of General Psychiatry, 9, 324-333.
Chambless, D. L., & Gillis, M. M. (1993).Cognitive therapy of anxiety disorders.Journal of Consulting and Clinical Psychology,
61, 248-260.
Eysenck, H. J. (1952). The effects of psychother-apy: An evaluation. Journal of Consulting
Psychology, 16, 319-324.
Falsetti, S. A., & Resnick, H. S. (1997). Multiple
channel exposure therapy: Patient and therapist’s
manuals. Unpublished manuscript, NationalCrime Victims Research and TreatmentCenter, Charleston, SC.
Goodman, W. K., Price, L. H., Rasmussen, S. A.,Mazure, C., Fleischman, R. L., Hill, C. L.,Heninger, G. R., & Charney, D. S. (1989).The Yale-Brown Obsessive-CompulsiveScale: Development, use, and reliability.Archives of General Psychiatry, 46, 1006-1011.
Zinbarg, R. E., Barlow, D. H., Brown, T. A., &Hertz, R. M. (1992). Cognitive-behavioralapproaches to the nature and treatment ofanxiety disorder. Annual Review of Psychology,
43, 235-267. �
The therapeutic techniques and con-cepts of rational emotive behaviortherapy (REBT) have been highly in-
fluential in professional and lay circles forclose to half a century. Since 1955, AlbertEllis has consistently developed the theoryand techniques of what was first termed ra-
tional therapy, then later renamed rational-
emotive therapy, and finally, in the early 90s,retitled rational emotive behavior therapy.
In his most recent book, Ellis providesan overview of the theoretical and practicaldevelopment of REBT, discusses the newesttheoretical developments, and provides
multiple examples of the application ofREBT techniques in clinical practice. Thebook is divided into two parts; the first partmostly focuses on the theoretical premisesof REBT, and the second part provides ex-amples of the practical application of REBTin the treatment of multiple disorders.
Ellis begins by discussing the major the-oretical premises of REBT, and develops histheory further by incorporating some as-pects of postmodernist theory. Ellis not onlyclearly explains the relationship between ac-tivating events (A), irrational beliefs (B),and behavioral consequences (C), but also
develops the concept of irrational beliefsfurther by conceptualizing them as irra-tional believing-emoting-behaving. Viewing ir-rational believing as an ongoing action,which in itself incorporates both emotionsand behaviors, makes salient one’s constantinteraction with the environment and inthis way speaks to the way people createtheir own realities. This view, according toEllis, together with the idea that peopleconstantly make choices about their behav-ior, emotions, and beliefs, is the major argu-ment for why REBT represents aconstructivist approach. The importance ofthe interplay of beliefs, emotions, and be-haviors in conceptualizing a client is clearlystressed throughout the book, and is one ofthe most salient factors in distinguishingREBT from other cognitive behavioral ther-apies. Ellis’ major theoretical focus is on theimportance of viewing people as creators oftheir own realities, as agents of their ownbehavioral, emotional, and cognitive distur-bances, and as agents of their own change.
Ellis stresses his advocacy of a socio-political stance in therapy by comparingREBT to Rigazio-DiGilio, Ivey, and Locke’s(1997; as cited in Ellis, 2001, pp. 51–58)
Book Review
Ellis, A. (2001). New Directions for Rational Emotive
Behavior Therapy: Overcoming Destructive Beliefs,
Feelings, and Behaviors
Amherst, NY: Prometheus Books
Reviewed by Mariola Magovcevic and Michael E. Addis, Clark University

Winter 2003 413
Theory of Developmental Counseling andTherapy (DCT) and Systematic Cognitive-Developmental Theory (SCDT). The hu-manistic aspects of REBT are highlightedby comparison to, among others, CarlRogers’ person-centered approach. Themultimodal and comprehensive aspects ofREBT are explained by describing REBT’sapplication in brief, family, and group ther-apy, and the incorporating of behavioral,emotive, and cognitive techniques in thepractice of REBT.
Although Ellis discusses his ideas in de-tail, and often provides case examples andtherapy excerpts as illustrations of his ideas,the first part of the book can be difficult tofollow at points. For example, some chap-ters cover similar complex theoretical con-cepts without providing the reader with aclear idea of how the ideas are distinct. Forinstance, Ellis in one chapter states thatREBT is in essence a postmodernist theory,but in a later chapter compares the theoret-ical premises of REBT to Alfred Korzybski’stheory of general semantics (as cited in Ellis,2001, pp. 99-113). Ellis draws on both ofthese theories in his theoretical elaborationof REBT; yet, these two theories providecontradictory explanations of the humancondition.
In the second part of the book, Ellis pro-vides numerous examples of the applicationof REBT in the treatment of specific disor-ders and problems. Ellis discusses the appli-
cation of REBT in the treatment of depres-sion, anxiety, low frustration tolerance,morbid jealousy, perfectionism, addictivebehaviors, borderline personality disorder,obsessive-compulsive disorder, and post-traumatic stress disorder. The theoreticalideas discussed in the first part of the bookare made concrete through case examples.The REBT techniques Ellis employs differsomewhat from techniques applied by othercognitive-behavioral practitioners. For in-stance, in addition to rational coping tech-niques common to many cognitive-behavioral therapies, Ellis favors the use ofrational-emotive imagery and forcefultaped disputing as emotive techniques, andshaming exercises as behavioral interven-tions.
A strength of the REBT techniques pro-vided is that they are discussed clearly andin detail, and could be applied as usefultools even by those practitioners who do notnecessarily adhere to the theory underlyingthe treatment. However, although there is abody of empirical support for the efficacy ofREBT techniques (Engels, Garnefski, &Diekstra, 1993), Ellis provides little empiri-cal evidence for the efficacy of the therapeu-tic techniques he presents for many of thedisorders and problems.
Ellis’ directive and uncompromisingclinical style is evident throughout the ther-apy excerpts. The directive style and theteacher-student quality of the therapeutic
relationship are clearly implicated in the
theory underlying REBT. However, this
style may not come naturally to many ther-
apists and may be uncomfortable for some
clients. For example, the song that Ellis cites
as a technique to help clients not take them-
selves too seriously is entitled “I Wish I
Were Not Crazy” and includes the follow-
ing verse:
I could agree to really be less crazy,
but I, alas, am just too goddamned
lazy! (p. 180)
Ellis intends this book as a tool for both
therapists and lay people. Although it may
function well as a tool for facilitating thera-
pists’ application of REBT, its usefulness as
a self-help book may be somewhat con-
strained. Many of the chapters are laden
with psychological jargon and difficult theo-
retical concepts. These sections may be per-
ceived as too intricate by some psych-
ologically nonsavvy individuals who are
looking for a concise and clear how-to guide
in dealing with their life problems.
Reference
Engels, G. I, Granefski, N., & Diekstra, R. F. W.
(1993). Efficacy of rational-emotive therapy:
A quantitative analysis. Journal of Consulting
and Clinical Psychology, 61, 1083-1090. �
Stay Connected | Renew* Your Membership *LATE FEE if you do not renew by Dec. 31, 2003!
..
.
..
..
.. .... . ...... . . ....
.. ......
..................
...... .
......
.1
2
3
5
6
7
89
10
11
12
13 1415
16
171819
20 21 22 23
242526
2728
293031
32
3334
35
3637
383940414243
444546
4748
4950
515253
54
55565758
5960
616263
6465
6667
4
begin
end
MMeemmbbeerrsshhiipp iinncclluuddeess* the Behavior Therapist
* listserve
* on-line directory of members
* ability to promote your practice
on AABT’s Web site
* Cognitive and Behavioral
Practice journal
* or Behavior Therapy journal
* Annual Convention discount
* special interest groups
* discounts on training tapes,
archive videos, and other
educational resources
* leadership and networking
opportunities
* involvement in an enduring group
whose members share your mission

414 the Behavior Therapist
Classifieds
Classified ads are charged at $4.00 per line. Classified ads
can be e-mailed directly to Stephanie Schwartz, Advertising
Manager, at [email protected]; otherwise, please fax or
mail hard copy to AABT, 305 Seventh Ave., New York,
NY 10001 (fax: 212-647-1865).
Positions Available
UNIQUE CAREER OPPORTUNITY! Weare looking for a behavioral clinician interested inintegrating behavioral health services within ourmulti-site primary care system. Duties includedeveloping an integrated care program andtraining/supervising other clinicians working onmedical teams. Looking for a team-orientedmental health clinician with master’s degree orPh.D. Experience with behavioral medicine,health psychology and health and wellness pro-grams a plus. Salary negotiable depending upondegree and qualifications. Must be licensed or li-cense eligible in Michigan. Contact (preferablyvia email) Pamela L. Silva; Director, MarketServices and Operations; Grand Valley HealthPlan; [email protected]; 829 Forest HillAvenue, SE, Grand Rapids, MI 49546.
CAMBRIDGE HEALTH ALLIANCE, affili-ated with Harvard Medical School, seeks appli-cations for a 32 hour staff position in child andadolescent Cognitive-Behavioral Therapy in theDepartment of Psychiatry. Academic appoint-ment at a rank determined by criteria of HarvardMedical School. Requirements include doctoratewith specialization in cognitive-behavioral ther-
apy, experience with children and adolescentsfrom diverse backgrounds, and state license.Send letter of interest, CV, and three letters ofreference to: Deborah Weidner, MD, Division ofChild and Adolescent Psychiatry, 1493Cambridge Street, Cambridge, MA 02139. Fax:617-665-1973. Email: [email protected]. CHA is an equal opportunity employer, andwomen and minority candidates are especiallyencouraged to apply.
CLINICAL FELLOWSHIPS IN COGNI-TIVE BEHAVIOR THERAPY AND REBT.A limited number of part-time two-year post-graduate Fellowships are being offered at theAlbert Ellis Institute beginning July 2004.Featuring supervision of individual, couples, andgroup therapy by Ray DiGiuseppe, Albert Ellis,Kristene Doyle, and Michael Broder. Trainingprograms involve 16 hours a week. Candidatescarry a diverse caseload of clients, co-lead ther-apy groups, participate in special seminars andongoing clinical research, and co-lead publicworkshops. Send requests for applications to:Kristene Doyle, Albert Ellis Institute, 45 East65th St., New York, NY 10021. Deadline forapplications is February 15, 2004.
HUDSON RIVER REGIONAL PREDOC-TORAL INTERNSHIP PROGRAM INPROFESSIONAL PSYCHOLOGY, NEWYORK STATE OFFICE OF MENTALHEALTH: offers full time pre-doctoral intern-ship positions in professional psychology for2004-2005 in its APA accredited program.Weekly seminars in a variety of clinical and pro-fessional areas supplement extensive supervision.Clinical assignments are to inpatient and com-munity services programs at facilities of the New
York State Office of Mental Health. Preference isgiven to students enrolled in APA-accreditedclinical or counseling psychology programs. Forfurther information and application materialscontact: Paul Margolies, Ph.D., TrainingDirector, Hudson River Regional PsychologyInternship Program, Hudson River PsychiatricCenter, 10 Ross Circle, Poughkeepsie, NewYork, 12601-1078; e-mail [email protected]; phone: (845) 483-3310.
EXCELLENT OPPORTUNITY FOR APART-TIME BEHAVIORAL PSYCHOLO-GIST to work in a well-established private prac-tice. Applicants must have a doctorate inpsychology and be on at least two major insur-ance panels (i.e., BC/BS, Tufts, Magellan,Harvard Pilgrim). Send resume to: JacobAzerrad, Ph.D., P.O. Box 353, Lexington, MA02420 or fax to 781-861-8637.
POSTDOCTORAL POSITION IN COG-NITIVE THERAPY. Beginning August 2004.Commitment to the CBT model is essential.Applications will be accepted until a suitablecandidate is found. Send a Vita, statement of ex-perience and interest, and three letters of refer-ence to Dr. Robert Leahy, Search Committee,American Institute for Cognitive Therapy, 136East 57th St., Suite 1101, New York, NY10022. www.CognitiveTherapyNYC.com oremail to [email protected].
BEHAVIORAL PSYCHOLOGIST. Multi-disciplinary practice in suburban Philadelphiaseeks licensed psychologist for full or part time.Must have strong training in CBT and desire topractice free of managed care. Fax vita toMargaret Sayers, Ph.D. 215/396-1886. �
Erratum
tBT 26(7), p. 338
Michel Hersen was a postdoctoral
fellow at Yale from 1965 to 1966,
not from 1965 to 1996.
Stefan Hofmann, incoming editor in
2005, is now accepting manuscripts.
Please send all new submissions to
Stefan Hofmann at this address:
Stefan Hofmann, Ph.D.
Boston University
Center for Anxiety & Related
Disorders
648 Beacon Street,
6th Floor
Boston, MA 02215-2015
s u b • m i s s i o n s
Cognitive and
Behavioral
Practice
Volume 11 #1 2004
Association for Advancement of
Behavior Therapy
ISSN 1077-7229
Anne Marie
Albano
Editor
Barbara Stetson
Eric Wagner
Association
Editors
Although Anne Marie Albano remains
editor of the journal Cognitive and
Behavioral Practice until the end of
2004, note this change:

The duties and charges of the AABT
President-Elect & Rep-at-Large
This individual serves as liaison to an AABT
Coordinator, working to review, develop, and/or main-
tain activities that service and support the members of
AABT in that respective area of the governing struc-
ture and serving as the “big picture” person to assist
the coordinator in knowing who to keep informed of
activities that have an effect on other areas of the gov-
erning structure.
The Representative-at-Large should be familiar
with the AABT mission statement, bylaws, and the
most recent strategic long-range planning report, and
is expected to attend the annual fall Board of
Directors meeting and monthly conference calls;
maintain contact with the coordinator, and to serve as
a facilitator if required to move projects and/or activi-
ties along; encourage members’ involvement in AABT
and encourage prospective members to join; and
attend the annual convention, including all relevant
meetings (i.e., with your coordinator and committee
chairs).
The person elected as President-Elect (2004–
2005) will serve as President (2005–2006) and Past
President (2006–2007) and on the Board of Directors
for 3 years. The Board meets once a year the Thursday
of the convention and conducts monthly conference
calls the other 11 months of the year.
The President-Elect works closely with the
President on all executive matters. In the President’s
absence at any meeting except the Board meeting
during the annual convention, the President-Elect
presides. In case of absence, disability, or resignation
of the President, the President-Elect will perform the
duties of the President.
The President presides at, schedules, and prepares
the agendas of meetings of the Board, the annual
meeting of the Association, and any special meetings
that may be called. The President may make nomina-
tions for approval by the Board for any appointive posi-
tion which must be filled except as otherwise stated.
The President of AABT is responsible in all matters,
stated or implied, that are related to the welfare,
stature and proper operation of the Association.
REPRESENTATIVE-AT-LARGEPRESIDENT-ELECT
AABT’s Bylaws are accessible on-line:
www.aabt.org/Bylaws.html
To cast your nomination, turn the page.
Winter 2003 415

I nominate
the following individuals
for the positions indicated:
P R E S I D E N T- E L E C T ( 2 0 0 4 – 2 0 0 5 )
R E P R E S E N TAT I V E -AT- L A R G E ( 2 0 0 4 – 2 0 0 7 )
N A M E ( p r i n t e d )
S I G N AT U R E ( r e q u i r e d )
2004 Call for Nominations NOMINATE the Next Candidates for AABT Office
The first phase of AABT’s 2004 election process is under
way: the nomination of qualified full members for the posi-
tions of President-Elect (2004-2005) and Representative-
at-Large (2004-2007).
Run for President-Elect or Representative-at-Large!
You can make a difference in the future of AABT.
Nominate yourself and one of your colleagues. You must
be a full member of AABT to be nominated. Only those
nomination forms bearing a signature and postmark on
or before February 2, 2004, will be counted.
Nomination acknowledges an individual’s leadership
abilities and dedication to behavior therapy and/or cogni-
tive therapy, empirically supported science, and to AABT.
When completing the nomination form, please take into
consideration that these individuals will be entrusted to
represent the interests of AABT members in important pol-
icy decisions in the coming years. Contact the
Nominations and Elections Chair for more information
about serving AABT or to get more information on the
positions. Please complete, sign, and send this nomina-
tion form to Carrie Winterowd, Ph.D., Associate
Professor, School of Applied Health and Educational
Psychology, 434 Willard Hall, Oklahoma State University,
Stillwater, OK 74078.
�
See page 415 for descriptions of President-Elect and
Representative-at-Large.
PRSRT STD
U.S. POSTAGE
PAID
Hanover, PA
Permit No. 4
the Behavior TherapistAssociation for Advancement of Behavior Therapy
305 Seventh Avenue, 16th floor
New York, NY 10001-6008
Tel.: 212-647-1890
Fax: 212-647-1865
e-mail: [email protected]
www.aabt.org
ADDRESS SERV ICE REQUESTED
�
�
�
�
�
�
�
�
�
h a p p yh o l i d a y s !
Related Documents











