Accepted Manuscript Title: Cognitive Behavior Therapy versus Interpersonal Psychotherapy for social anxiety disorder delivered via smartphone and computer: a randomized controlled trial Author: Jesper Dag¨ o¨ o Robert Persson Asplund Helene Andersson Bsenko Sofia Hjerling Anna Holmberg Susanne Westh Louise ¨ Oberg Brj´ ann Lj ´ otsson Per Carlbring Tomas Furmark Gerhard Andersson PII: S0887-6185(14)00031-0 DOI: http://dx.doi.org/doi:10.1016/j.janxdis.2014.02.003 Reference: ANXDIS 1584 To appear in: Journal of Anxiety Disorders Received date: 30-8-2013 Revised date: 26-1-2014 Accepted date: 18-2-2014 Please cite this article as: Dag¨ o¨ o, J., Asplund, R. P., Bsenko, H. A., Hjerling, S., Holmberg, A., Westh, S., ¨ Oberg, L., Lj´ otsson, B., Carlbring, P., Furmark, T., & Andersson, G.,Cognitive Behavior Therapy versus Interpersonal Psychotherapy for social anxiety disorder delivered via smartphone and computer: a randomized controlled trial, Journal of Anxiety Disorders (2014), http://dx.doi.org/10.1016/j.janxdis.2014.02.003 This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Accepted Manuscript
Title: Cognitive Behavior Therapy versus InterpersonalPsychotherapy for social anxiety disorder delivered viasmartphone and computer: a randomized controlled trial
Author: Jesper Dagoo Robert Persson Asplund HeleneAndersson Bsenko Sofia Hjerling Anna Holmberg SusanneWesth Louise Oberg Brjann Ljotsson Per Carlbring TomasFurmark Gerhard Andersson
PII: S0887-6185(14)00031-0DOI: http://dx.doi.org/doi:10.1016/j.janxdis.2014.02.003Reference: ANXDIS 1584
To appear in: Journal of Anxiety Disorders
Received date: 30-8-2013Revised date: 26-1-2014Accepted date: 18-2-2014
Please cite this article as: Dagoo, J., Asplund, R. P., Bsenko, H. A., Hjerling,S., Holmberg, A., Westh, S., Oberg, L., Ljotsson, B., Carlbring, P., Furmark,T., & Andersson, G.,Cognitive Behavior Therapy versus InterpersonalPsychotherapy for social anxiety disorder delivered via smartphone andcomputer: a randomized controlled trial, Journal of Anxiety Disorders (2014),http://dx.doi.org/10.1016/j.janxdis.2014.02.003
This is a PDF file of an unedited manuscript that has been accepted for publication.As a service to our customers we are providing this early version of the manuscript.The manuscript will undergo copyediting, typesetting, and review of the resulting proofbefore it is published in its final form. Please note that during the production processerrors may be discovered which could affect the content, and all legal disclaimers thatapply to the journal pertain.

Page 1 of 34
Accep
ted
Man
uscr
ipt
1.
Cognitive Behavior Therapy versus Interpersonal Psychotherapy for social anxiety
disorder delivered via smartphone and computer: a randomized controlled trial
Jesper Dagöö1, Robert Persson Asplund1, Helene Andersson Bsenko2, Sofia Hjerling3, Anna
Holmberg4, Susanne Westh4, Louise Öberg5, Brjánn Ljótsson6, Per Carlbring7, Tomas
Furmark3, Gerhard Andersson1,8 *
1 Department of Behavioural Sciences and Learning, Linköping University, Linköping,
Sweden.
2 Department of Psychology, Umeå University, Umeå, Sweden.
3 Department of Psychology, Uppsala University, Uppsala, Sweden.
4 Department of Social Sciences, Division of Psychology, Mid Sweden University, Östersund,
Sweden.
5 Department of Psychology, Lund University, Lund, Sweden.
6 Department of Clinical Neuroscience, Division of Psychology, Karolinska Institute,
Stockholm, Sweden.
7 Department of Psychology, Stockholm University, Stockholm, Sweden.
8 Department of Clinical Neuroscience, Section of Psychiatry, Karolinska Institute,
Stockholm, Sweden.
* Corresponding author. Tel.: +46-(0)13-28 58 40. E-mail address: [email protected]
(G. Andersson).
Abstract
In this study, a previously evaluated guided Internet-based cognitive behavior therapy for
social anxiety disorder (SAD) was adapted for mobile phone administration (mCBT). The
treatment was compared with a guided self-help treatment based on interpersonal

Page 2 of 34
Accep
ted
Man
uscr
ipt
2.
psychotherapy (mIPT). The treatment platform could be accessed through smartphones,
tablet computers, and standard computers. A total of 52 participants were diagnosed with
SAD and randomized to either mCBT (n=27) or mIPT (n=25). Measures were collected at
pre-treatment, during the treatment, post-treatment and 3 month follow-up. On the primary
outcome measure, the Liebowitz Social Anxiety Scale – self rated, both groups showed
statistically significant improvements. However, mCBT performed significantly better than
mIPT (between group Cohen’s d =0.64 in favor of mCBT). A larger proportion of the
mCBT group was classified as responders at post-treatment (55.6 % versus 8.0 % in the
mIPT group). We conclude that CBT for SAD can be delivered using modern information
technology. IPT delivered as a guided self-help treatment may be less effective in this
format.
Keywords: Cognitive behavior therapy; Interpersonal psychotherapy; Social
anxiety disorder; Smartphone; Internet
1. Introduction
Social anxiety disorder (SAD) is characterized by a fear of being scrutinized and negatively
evaluated by others and is associated with a substantial impairment in quality of life
(American Psychiatric Association, 2000). It is a costly disorder for society at large in terms
of direct costs in the form of pharmacotherapy and psychotherapy and indirect costs in terms

Page 3 of 34
Accep
ted
Man
uscr
ipt
3.
of productivity loss (Acarturk, Cuijpers, van Straten, & de Graaf, 2009; Smit, et al., 2006).
SAD is a highly prevalent condition, although prevalence estimates differ between countries
(Furmark, 2002). Several treatments have been investigated for SAD, and the two major
evidence-based treatments are cognitive behavior therapy (CBT) (Ponniah & Hollon, 2008)
and pharmacotherapy (Stein, Ipser, & Balkom, 2004).
Since the late 1990’s guided Internet-delivered cognitive behavior therapy
(ICBT) has been developed and evaluated (Andersson, 2009), and has been found to have
large effect sizes for a range of psychiatric and health-related problems such as depression,
anxiety disorders, severe health anxiety, irritable bowel syndrome, eating disorders, and
pathological gambling (Hedman, Ljótsson, & Lindefors, 2012). ICBT for SAD has been
evaluated in several studies by independent research groups with studies from Sweden
(Andersson, et al., 2006; Carlbring, et al., 2007), Australia (Titov, Andrews, Schwencke,
Drobny, & Einstein, 2008; Titov, et al., 2010), Switzerland (Berger, et al., 2011; Berger,
Hohl, & Caspar, 2009), and Spain (Botella, et al., 2010). In addition, the research has been
summarized in reviews (Andersson, Carlbring, & Furmark, in press; Tulbure, 2011). Guided
ICBT has also been found to be cost-effective (Hedman, Andersson, Ljótsson, Andersson,
Rück, & Lindefors, 2011), and to be as effective as group-based CBT (Hedman, Andersson,
Ljótsson, Andersson, Rück, Mörtberg, et al., 2011). The common elements of ICBT for SAD
have been a structured self-help CBT program combined with therapist guidance from an
online therapist (Andersson, 2009). The ICBT treatment manual that has been used in the
Swedish studies on ICBT for SAD (Furmark, Holmström, Sparthan, Carlbring, &
Andersson, 2013) is inspired by Clark and Well’s cognitive model of SAD (Clark & Wells,
1995).
Interpersonal psychotherapy (IPT) was originally developed to provide an
effective short-term treatment for depression (Klerman, Dimascio, Weissman, Prusoff, &

Page 4 of 34
Accep
ted
Man
uscr
ipt
4.
Paykel, 1974), and is recommended by numerous practice guidelines as a treatment of
choice for unipolar depressive disorder (Cuijpers, et al., 2011). IPT for SAD has been
studied less often, but has been compared with CBT in previous studies performed in
clinical, residential, and academic outpatient treatment settings (Borge, et al., 2008; Lipsitz,
Markowitz, Cherry, & Fyer, 1999; Stangier, Schramm, Heidenreich, Berger, & Clark, 2011).
As IPT focuses on how problems in interpersonal relations predispose, precipitate and
perpetuate a patient’s distress (Weissman, Markowitz, & Klerman, 2000) it is plausible to
assume that it can be helpful for persons with SAD. Several theories have been considered
influential in the development of IPT including attachment theory (Weissman, et al., 2000).
Lipsitz and Markowitz developed an IPT manual for SAD in the 1990’s in which they
incorporated content and techniques relevant for this disorder (Lipsitz, et al., 1999). They
argued that IPT had an intuitive appeal as a treatment for SAD because of the prominent
interpersonal features of the condition (Lipsitz, et al., 1999). The manual was tested in a 14
week open trial (Lipsitz, et al., 1999). Seven out of nine participants were independently
rated as much or very much improved on overall social phobia symptoms (Lipsitz, et al.,
1999). IPT was compared to CBT for SAD in a larger randomized trial conducted in a
residential setting (n=80) (Borge, et al., 2008). Effect sizes for the IPT group were medium
to large and no significant differences were found between the groups (Borge, et al., 2008).
More recently, Stangier and coworkers compared the efficacy of CBT (n=38), IPT (n=38),
and a waiting-list control condition (n=41) in two academic outpatient treatment sites. In this
randomized controlled trial both treatments were superior to a waiting-list control condition.
However, CBT performed significantly better than IPT (Stangier, et al., 2011).
Smartphone technology has the potential to make psychological and behavioral
health interventions more accessible, efficient, and interactive for patients (Boschen &
Casey, 2008). The smartphone is in essence a combined telephone and portable computer

Page 5 of 34
Accep
ted
Man
uscr
ipt
5.
connected to the Internet and is increasingly used as a way to access information on the
internet (Klasnja & Pratt, 2012). Moreover, smartphone users tend to carry their phones with
them everywhere (Klasnja & Pratt, 2012), and some features of a smartphone might prove
useful and add new possibilities in psychological treatments. For example, the small
smartphone programs or applications commonly referred to as “apps”, might be used as a
platform for in vivo exposure exercises, self-assessments, monitoring of progress in real
time, visual feedback, and evaluation of treatment outcome (Ly, Dahl, Carlbring, &
Andersson, 2012). In addition, psychoeducation can be presented via video and audio
material, homework can be scheduled in the built-in calendar, and the camera can be used to
record exposure sessions (Luxton, McCann, Bush, Mishkind, & Reger, 2011). However,
there are few evidence-based behavioral and psychological smartphone applications and
there is a need for controlled studies (Luxton, et al., 2011).
In the present study, we adapted our previously tested guided Internet
treatment for SAD to a mobile format (mCBT). mCBT can be seen as an expansion of the
reach of our Internet treatments for SAD, since the principal contents were preserved even if
the format was modified to better fit the screen size and interface of a smartphone. With the
exception of applied relaxation (Furmark, et al., 2009), guided ICBT has not been compared
to an active psychological treatment. We developed a guided self-help treatment based on
IPT, which we regarded as a credible control condition. This treatment shared many
technical features of the mCBT program (e.g., administration over the Internet and a mainly
text-based format), but was distinctly different in terms of contents. The reason for
comparing mCBT against mIPT was that we wanted a control condition that was principally
different from CBT while having been tested in previous controlled trials. We expected that
the mCBT condition would lead to improvements in symptoms of SAD in line with previous
ICBT studies. Based on the low number of studies of regular face-to-face IPT for SAD and

Page 6 of 34
Accep
ted
Man
uscr
ipt
6.
the absence of any web-based studies of IPT for SAD, we did not formulate any hypothesis
regarding the effects of mIPT. The novel aspects of this controlled trial are the
administration format and that to our knowledge neither CBT nor IPT has been delivered via
smartphone previously.
2. Method
2.1 Trial design
This was a randomized controlled trial within the context of a between groups repeated
measures design.
2.2 Sample and recruitment
2.2.1 Inclusion criteria
To be eligible for inclusion potential participants had to meet the following criteria; (a)
fulfilling the DSM-IV criteria for social anxiety disorder as assessed using the Structured
Clinical Interview for DSM-IV axis I disorders (SCID-I) (First, Gibbon, Spitzer, &
Williams, 1997), (b) being 18 years old or older, (c) having SAD as primary diagnosis (d)
scoring <25 on the Montgomery Åsberg Depression Rating Scale-self report (MADRS-S)
(Svanborg & Åsberg, 1994), (e) having a score of less than 4 of 6 on the suicide ideation
item 9 on MADRS-S, (f) no ongoing alcohol abuse or dependence as measured by the self-
report questionnaire Alcohol Use Disorder Identification Test (AUDIT) (Bergman &
Källmen, 2002), (g) no history of psychosis or bipolar disorder, (h) not meeting criteria for
any personality disorders within clusters A or B, (i) no ongoing other form of psychological
treatment, (j) no history of CBT the preceding four years, (k) if on medication have constant
dosage of any prescribed psychotropic medication three months prior to treatment, (l) not
having a psychiatric problem where a treatment provided by psychiatric outpatient care

Page 7 of 34
Accep
ted
Man
uscr
ipt
7.
would be more appropriate, (m) having access to smartphone and computer with Internet
connection, and (n) being able to read and write in Swedish.
2.2.2 Recruitment
Recruitment for the study took place during 2011 and 2012. Participants were recruited
nation-wide via the project’s home page and advertisement in Swedish press, Google
Adwords, and Facebook. Information about the study was presented on the project’s
homepage. After application, potential participants completed the following online electronic
screening questionnaires; the Liebowitz Social Anxiety Scale – self-report (LSAS-SR)
(Baker, Heinrichs, Kim, & Hofmann, 2002), the Social Interaction Anxiety Scale (SIAS)
(Mattick & Clarke, 1998), the Social Phobia Scale (SPS) (Mattick & Clarke, 1998), the Beck
Anxiety Inventory (BAI) (Beck, Epstein, Brown, & Steer, 1988), the MADRS-S (Svanborg &
Åsberg, 1994), the Quality Of Life Inventory (QOLI) (Frisch, Cornell, Villanueva, &
Retzlaff, 1992), and the AUDIT (Bergman & Källmen, 2002; Selin, 2003). Applicants
fulfilling the initial screening criteria were invited to a diagnostic interview via telephone.
2.2.3 Diagnostic assessment and participants
Diagnoses were established using the Mini International Neuropsychiatric Interview
(Sheehan, et al., 1998), and the SAD section of the research version of the semi-structured
interview the Structured Clinical Interview for DSM-IV (SCID-I-RV; (First, Spitzer, Gibbon
M, & Williams, 2002). The SCID-I-RV was used because it can provide more detailed
information about SAD and has high inter-rater reliability (Zanarini & Frankenburg, 2001).
An evaluation of in-person and telephone interviews for the assessment of SAD patients via
the SCID has indicated excellent agreement (Crippa, et al., 2008). The AUDIT was used to
assess potential alcohol dependence or abuse and solely used as a screening instrument. In a

Page 8 of 34
Accep
ted
Man
uscr
ipt
8.
study of the psychometric properties of the Swedish version of the AUDIT, both the internal
and test-retest reliabilities were satisfactory (Selin, 2003). The diagnostic interviews were
conducted by a psychologist or by psychologist students supervised by licensed
psychologists.
In total, 235 applied to participate out of which 76 were invited to a diagnostic
interview. Following the interview, 52 participants were included in the trial (see Table 1 for
demographic description of the participants, Table 2 for medication data of the participants,
and Figure 1 for Flowchart participant flow). Of the 52 participants, 20 (38,5%) fulfilled the
criteria for social anxiety disorder in a specific form and 32 (61.5%) in a generalized form.
For comorbid diagnoses, 1 (1.9%) fulfilled the criteria for depression and 1 (1.9%) the
criteria for generalized anxiety disorder (GAD). Five potential participants were referred to a
psychologist with clinical experience from outpatient psychiatric care for further assessment
of differential diagnostic issues, prior experience of cognitive behavior therapy, suicide risk
and potential alcohol dependence or abuse.
2.3 Procedure
Once potential participants were included they were informed when they would get access to
the first treatment module, which could be accessed via smartphone, computer or tablet
computer. Each treatment lasted nine weeks. Participants had to send in feedback regarding
treatment and homework progression before a new module was activated. Each week the
participants were encouraged to log in via a computer to fill in an electronic version of the
LSAS-SR questionnaire. Therapists were instructed to set aside 15 minutes per week and
participant to deliver feedback on reflections, homework, and questions from participants.
Post-treatment measurements were collected via the web-based questionnaire system.

Page 9 of 34
Accep
ted
Man
uscr
ipt
9.
Randomization was performed by an independent person within the research
team who had no contact with the participants and based upon a list of anonymous
participant identification numbers. Applicants were divided into two groups using a net-
based randomization tool, “Research Randomizer” (http://randomizer.org/form.htm). The
randomization process was conducted in two steps; first applicants were randomized in 1:1
proportion to each treatment group, and then they were randomized to four Internet
therapists who were last-year students at the 5-year Swedish psychology program. Because
of a duplication of a participant code the treatment randomization of participants was not
exactly in a 1:1 proportion. The study was approved by the regional ethics committee at
Linköping University, Sweden.
2.4 Treatments
2.4.1 Cognitive behavior therapy via mobile computer solutions (mCBT)
The mCBT manual used in this study was based on a previous guided self-help ICBT for
SAD developed by our research group (Andersson, et al., 2006). It is primarily a text-based
treatment, and exercises are given as homework between each module. Both of the ICBT
and mCBT manuals consist of nine weekly modules. The mCBT modules comprised one
introduction module, three modules focusing on cognitive interventions (challenging
automatic thoughts, behavioral experiments and a video feedback exercise), three modules
focusing primarily on exposure, one module focusing on social skills and one maintenance
module. The mCBT manual was shortened as we assumed that long texts would be difficult
to read on a smartphone. Entries of anxiety levels were made in an exposure module in
which anxiety levels pre, during and post exposure were presented graphically. Other forms
of homework were entered into electronic forms as well. The anxiety hierarchy and
idiosyncratic information that had been entered into the modules during the treatment (e.g.
previous exposure exercises and safety behaviors of the participant) were automatically

Page 10 of 34
Accep
ted
Man
uscr
ipt
10.
presented throughout the treatment at relevant points and were included in the maintenance
plan of the participant.
2.4.2 Interpersonal psychotherapy via mobile computer solutions (mIPT)
The mIPT treatment was modeled to resemble the mCBT treatment in terms of format and
length. The manual, which was not based on any previous self-help manual, was inspired by
texts on interpersonal psychotherapy for depression (Klerman, Weissman, Rounsaville, &
Chevron, 1984; Weissman, Markowitz, & Klerman, 2007), and treatment descriptions in the
existing trials on IPT for SAD (Stangier, et al., 2011). Unlike other IPT treatments, with the
exception of one Internet study (Donker, et al., 2013), the IPT group participants in this
study worked with all four problem areas of an IPT treatment; grief, interpersonal disputes,
role transitions, and interpersonal sensitivity (Markowitz, et al., 2000). The first module
covered psychoeducation and a short presentation of interpersonal psychotherapy. Module 2
had a focus on attachment theory and interaction patterns and number 3 on social phobia in
an interpersonal context. Modules 4 and 5 depicted role transitions (participants were
encouraged to role play problematic situations with a friend), and module 6 interpersonal
disputes. Then module 7 covered the area of grief, module 8 social skills, and module 9 a
maintenance program. Between each weekly contact with the therapists participants were
encouraged to reflect upon their work and the material that had been presented in the
modules.
2.5 Material
The treatment material of both mIPT and mCBT was presented in text format. A video
greeting and presentation by the principal investigator (G.A.) introduced and ended both
programs. Registration forms and rating scales used in the program were converted into
electronic modules designed to suit the format of a website adapted for mobile devices, but

Page 11 of 34
Accep
ted
Man
uscr
ipt
11.
these could also be accessed via computers and tablet computers in an interface adapted for
these platforms. The smartphone interface layout was essentially in black/white and the
combined layout for computers and computer tablets also included some colors.
In comparison to our previous ICBT programs for SAD, mCBT differs in the
aforementioned text mass reduction, layout differences (“book-like” vs. “smart phone web
app-like”), a development from paper-and-pencil entries to entries directly into the
smartphone/computer interface system, automatic presentation at relevant points throughout
the program of previously entered information, and a continual graphic presentation of the
anxiety level development during in-vivo exposure exercises. The last two of these were
designed to enable direct and possibly more reliable entries of anxiety levels in real time and
to provide monitoring of potential progress in real time through direct visual feedback.
Participants had to use an access code to log into the treatment platform in a secure manner.
2.6 Method of delivery
An Internet application, used in previous studies e.g., (Carlbring, et al., 2013), was used to
administer outcome measures at pre- and post-treatment. Weekly measurements with the
LSAS-SR were collected within the same Internet application. In a study of psychometric
properties of Internet administration of self-report measures commonly used in research on
SAD, paper-and-pencil and versions were found to possess equivalent psychometric
properties (Hedman, et al., 2010).
2.7 Outcome measures
2.7.1 Primary outcome measure

Page 12 of 34
Accep
ted
Man
uscr
ipt
12.
The LSAS-SR was used as the primary outcome measure. The LSAS-SR measures the
degree of avoidance and fear in 24 social situations (13 performance and 11 interaction
situations). Fear and avoidance are rated separately for each situation on a scale from 0 (no
fear/never avoid) to 3 (severe fear/usually avoid). The clinician-administered version of the
LSAS has good psychometric properties (Heimberg, et al., 1999). In a comparison of the
psychometric properties of the self-report and clinician-administered formats of the LSAS
there was little difference between the two versions on any scale or subscale score (Fresco,
et al., 2001). They were both internally consistent and had essentially identical subscale
intercorrelations. The discriminant validity of the two forms of the LSAS was shown to be
strong (Fresco, et al., 2001).
2.7.2 Secondary outcome measures
The SIAS and SPS were used to assess social anxiety symptoms, the BAI was used to assess
general anxiety, the MADRS-S was used to assess depressive symptoms and the QOLI was
used to assess perceived quality of life. The SPS, SIAS, BAI, MADRS-S, and the QOLI
have all demonstrated good psychometric properties for online administration for patients
with SAD (Hedman, et al., 2010).
2.8 Statistical analysis
Statistical analyses were conducted using SPSS 21. For primary and secondary outcome
measures, intention-to-treat (ITT) analyses were performed based on data from all
randomized participants, which is a more conservative approach compared to only including
those who completed the treatment. The multiple imputation module in SPSS was used to
create 5 sets of missing data imputations. In a simulation study in which several
statistical approaches to data missing data were tested the use of multiple imputation was

Page 13 of 34
Accep
ted
Man
uscr
ipt
13.
shown to improve the validity of the results when analyzing datasets
with missing observations (Blankers, Koeter, & Schippers, 2010). The effects of group on
primary and secondary outcome measures were analyzed in the imputed data sets using
analysis of covariance (ANCOVA), with pre-treatment values as covariate (Vickers &
Altman, 2001). Means, standard deviations, and standard errors of effect sizes were pooled
from the 5 imputations using “Rubin’s rules” (Rubin & Schenker, 1991), and the small
sample correction for pooled degrees of freedom (Barnard & Rubin, 1999). Paired samples t-
tests were used to evaluate improvement from pre- to post-treatment for within-group
calculations and for a comparison between post-treatment and follow-up on the primary
outcome the LSAS-SR. Clinical significant improvement, using Jacobson’s procedures
(Jacobson & Truax, 1991), was used to estimate rates of responders on the primary outcome
measure (e.g., both a reliable change and a reduction to a specified level). Following the
approach used in a recent Swedish study on ICBT for SAD (Hedman, Andersson, Ljótsson,
Andersson, Rück, Mörtberg, et al., 2011), a cutoff value of a score below 43.3 on the LSAS-
SR was used. The reliable change index was established using observed data of the study
and the test-retest value used in Hedman’s study (r=.97).
3. Results
3.1 Attrition, user information, and technique
In total, 30 participants (57.7 %) completed all treatment modules within the 9-week time
frame. Corresponding figures for each group separately were 17 (63.0 %) for the mCBT
group and 13 (52.0 %) for the mIPT group. For attrition see Figure 1. When accessing the
treatment platform, participants used smartphone 42.81 % , computer 50.05 %, and tablet
computer 7.14 % of the time. 21 participants of the mCBT program logged into both the
anxiety exposure and anxiety hierarchy modules. Out of these 15 worked with both the

Page 14 of 34
Accep
ted
Man
uscr
ipt
14.
exposure modules and created anxiety hierarchies. In average these participants entered data
from 8.20 exposure exercises (SD=4.95, min=1, max=21) into the platform and put 8.73
items on their anxiety hierarchies (SD=5.61, min=4, max=25). Overall, the instruction to
therapists of 15 minutes of feedback to participants delivered once a week was followed.
There were technical problems related to using the new smartphone platform and interface;
problems to enter estimated anxiety levels during exposure, complicated log-in codes and the
necessity to log out of the smartphone to enter weekly measurements on the primary
outcome measure.
3.2 Treatment effects
3.2.1 Primary outcome measure (LSAS-SR)
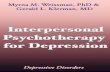
Results for the primary outcome measure are presented in Table 3. The two groups did not
differ significantly on the LSAS-SR at pre-treatment, M=60.19 (SD=18.95) for mCBT and
M=65.72 (SD=27.15) for the mIPT group: t(50) = -0.86, n.s. On the LSAS-SR pre/post, both
treatment groups showed significant improvements at the p < .05 level; mCBT: t(24) = 6.18,
p=.001; mIPT: t(21) = 2.75, p =.01. Within-group Cohen’s d effect sizes were large for
mCBT (d= 0.99), and small for mIPT (d = 0.43). The between group effect size was
moderate (d= 0.64). Results for the weekly measurements on the LSAS-SR are presented in
Figure 2 for illustration.
3.2.2 Secondary outcome measures
Results for the secondary self-report inventories are presented in Table 3. Within group
effect sizes on SIAS and SPS were moderate in the mCBT group and small in the mIPT
group. Between groups effect sizes for these inventories were moderate, for the SIAS and for

Page 15 of 34
Accep
ted
Man
uscr
ipt
15.
the SPS. The inventories for the measurement of general anxiety (BAI) and quality of life
(QOLI) revealed small between group effect sizes. The between groups effect size for the
measurement of depression, the MADRS-S, was large (in favor of the mCBT group, but
within group effects were small for both groups (Table 3)).
3.2.3 Three-months follow-up
In addition to the pre/post analysis a post/follow-up analysis was conducted using paired
samples t-tests on the basis of the results on the primary outcome measure at the three-month
follow-up (N=39; with n=24 in the mCBT group and 15 in the mIPT group). We did not
impute the missing data at this stage and focused only on completers of the follow-up. The
results were stable for both groups: mCBT, Post M=38.21 (SD=24.50), Follow-up M=39.75
(SD =24.87), t(21) = -0.74, p=.47; mIPT, Post M=57.21 (SD =28.24), Follow-up M=59.00
(SD =28.84), t(14) = 1.27, p=.23.
3.2.4 Clinical significance
The number of participants meeting the criteria for clinically significant improvement was
calculated for the LSAS-SR. In the mCBT group there were 55.6 % (n=15) who were
classified as responders at post-treatment compared to 8.0 % (n=2) in the mIPT group, and
this difference was statistically significant χ2(1)= 9.07, p=.04.
4. Discussion
The aim of this study was to compare mCBT, a CBT treatment adapted for mobile phone
administration, with mIPT, a newly developed self-help treatment based on interpersonal
psychotherapy. On the primary outcome measure LSAS-SR both groups showed statistically
significant improvements. However, mCBT performed significantly better than mIPT on the

Page 16 of 34
Accep
ted
Man
uscr
ipt
16.
social phobia measures. Moreover, a larger portion of the mCBT group was classified as
clinically improved at post-treatment (55.6 %) when compared with the mIPT group (8 %).
The within-group effect size for mCBT (Cohen’s d = 0.99) is in line with effect sizes of
both CBT and ICBT in previous SAD studies (Acarturk, et al., 2009; Tulbure, 2011). For
example, the average within group effect size in a meta-analysis of CBT treatments entailing
exposure and cognitive restructuring was Cohens’s d = 0.83 (Fedoroff & Taylor, 2001). In
five previous Swedish ICBT trials on SAD using the longer version of the self-help manual
and with the LSAS-SR as primary outcome measure the between-group effect sizes have
ranged between d= 0.82 to 1.35 (Andersson, Carlbring, Furmark, & on behalf of the SOFIE
Research Group, 2012; Andersson, et al., 2006; Carlbring, et al., 2007; Furmark, et al., 2009;
Tillfors, et al., 2008).
There are to our knowledge no previous studies on mIPT. While it is less likely that
mCBT would differ much from the previous Internet studies on SAD, the effects of mIPT
are more difficult to understand and should be interpreted with caution. A comparison with
Stangier et al.’s (2011) results from a clinical outpatient care setting is also difficult since
our study did not include a waiting list control group. However, in both studies both active
treatments produced significant results. Our material does not lend itself easily to any further
comparisons with Stangier et al.’s study given the administration format. However, as CBT
performed better than IPT in both studies it may be that the superiority of CBT is present in
other administration formats. This is probably in contrast to IPT for depression, which is as
effective as CBT (Cuijpers, et al., 2011), and may also be so when delivered via the Internet
as an unguided treatment (Donker, et al., 2013). We interpret our results as an indication that
CBT treatment delivered via smartphones might work well when the technical problems that
hampered this trial are dealt with as indicated by the fact that participants also used
computers to access the treatment. Then the unique contributions of a smartphone interface

Page 17 of 34
Accep
ted
Man
uscr
ipt
17.
to a CBT treatment should be investigated further, but it is also likely that clients prefer to
have the option to choose which platform to use. However, for scientific reasons it would
have been preferable if participants had used their smartphones to a greater extent only.
The results of the mIPT treatment in our study are more difficult to interpret.
The mIPT group had initially a mean score on the LSAS-SR, that was somewhat greater than
that of the mCBT group (albeit not statistically significant). Up until the fourth week there is
limited progress in the mCBT group and no progression in the mIPT group. The fifth week
there is a sudden drop in the mean of the mIPT group and the mIPT group is this week on
par with the mCBT group on the primary outcome measure. After week five the progression
of the mCBT group gains momentum and the distance between the means of the two groups
finally reaches a point where there is a significant difference between the means at the post
level. It is hard to draw any conclusions on the basis of our material but probably could this
effect be attributed to several factors. There is a shift in content midway through the mCBT
treatment. Week five is the first of three weeks of exposure treatment modules and one
social skills module in the mCBT treatment program.
It is interesting to note that we included all problem areas as described in IPT
for depression, and that a focus of one or two would have lead to even fewer treatment
components. It is possible that IPT is a treatment that requires therapist-patient interaction
(Weissman, et al., 2000), as there arguably is less psychoeducation than in CBT for SAD.
The fact that mCBT was superior to mIPT, being an active treatment control, support that
there are components inherent in the CBT program that contribute specifically to
improvement.
There are limitations of our study that require comment. The technical
problems related to using the new smartphone platform and interface possibly made it more
favorable to access the treatment platform via a computer interface, which might explain the

Page 18 of 34
Accep
ted
Man
uscr
ipt
18.
relatively large proportion of computer use of the treatment program. However, as
participants could use the different platforms as they liked we have no means to estimate if
one format differs from the other. All participants were however smartphone users and there
are no empirical strong reasons to assume that it would be much different to access a
treatment via different platforms, even if this remains to be tested for SAD as it has been
tested for depression (Watts, et al., 2013). There was no untreated or placebo-treated control
condition, as two active treatments were tested. The small sample sizes resulted in low
statistical power for comparing two active treatments. In spite of this, mCBT performed
significantly better than mIPT. A substantially larger sample size would however been better
suited to test differences between two active treatments if not large differences were
expected. The fact that we recruited patients for this study plus the relatively conservative
exclusion criteria for suicidality, secondary depression and alcohol abuse/dependence might
have resulted in a sample, which is not representative of a clinical population. The
generalizability to regular clinical patients might thus be limited. However, for ethical
reasons the groups we excluded (with secondary depression as an exception) are usually
considered too risky to include in studies similar to ours. This also applies to previous ICBT
studies on SAD. However, ICBT for SAD has been tested with regular routine care patients
and with similar results as in efficacy trials (Aydos, Titov, & Andrews, 2009; Hedman,
Andersson, Ljótsson, Andersson, Rück, Mörtberg, et al., 2011). Finally, no conclusions can
be drawn regarding treatment credibility since there was no measurement of treatment
credibility included in the trial and measurement could have been improved if diagnostic
interviews were also conducted post treatment.
In spite of these limitations we conclude that a smartphone-based mCBT
treatment interface for SAD is feasible as an alternative option for accessing online
treatment. Further studies are needed to compare mCBT and mIPT as there may be patients

Page 19 of 34
Accep
ted
Man
uscr
ipt
19.
who prefer one treatment over the other. Moreover the possible advantages and client
experiences of using smartphones in treatment for SAD and other conditions should be
explored further.
Conflicts of Interest
The authors report no conflicts of interest.
Acknowledgement
This study was sponsored in part by a grant from the Swedish Science Council, Swedish
Council for Working and Life research and Linköping University.
References
Acarturk, C., Cuijpers, P., van Straten, A., & de Graaf, R. (2009). Psychological treatment of
social anxiety disorder: a meta-analysis. Psychological Medicine, 39, 241-254.
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental
disorders (4th ed., text revision ed.). Washington, DC: American Psychiatric Press.
Andersson, G. (2009). Using the internet to provide cognitive behaviour therapy. Behaviour
Research and Therapy, 47, 175-180.
Andersson, G., Carlbring, P., & Furmark, T. (in press). Internet-delivered treatments for
social anxiety disorder In J. Weeks (Ed.), Handbook of Social Anxiety Disorder. New
York: Wiley-Blackwell.
Andersson, G., Carlbring, P., Furmark, T., & on behalf of the SOFIE Research Group. (2012).
Therapist experience and knowledge acquisition in Internet-delivered CBT for social
anxiety disorder: A randomized controlled trial. PloS ONE, 7(5), e37411.

Page 20 of 34
Accep
ted
Man
uscr
ipt
20.
Andersson, G., Carlbring, P., Holmström, A., Sparthan, E., Furmark, T., Nilsson-Ihrfelt, E.,
Buhrman, M., & Ekselius, L. (2006). Internet-based self-help with therapist feedback
and in-vivo group exposure for social phobia: a randomized controlled trial. Journal of
Consulting and Clinical Psychology, 74, 677-686.
Aydos, L., Titov, N., & Andrews, G. (2009). Shyness 5: the clinical effectiveness of Internet-
based clinician-assisted treatment of social phobia. Australasian Psychiatry, 17, 488-
492.
Baker, S. L., Heinrichs, N., Kim, H. J., & Hofmann, S. G. (2002). The Liebowitz Social
Anxiety Scale as a self-report instrument: a preliminary psychometric analysis.
Behaviour Research and Therapy, 40, 701-715.
Barnard, J., & Rubin, D. (1999). Miscellanea. Small-sample degrees of freedom with multiple
imputation. Biometrika, 86, 948-955.
Beck, A. T., Epstein, N., Brown, G., & Steer, R. (1988). An inventory for measuring clinical
anxiety. Psychometric properties. Journal of Consulting and Clinical Psychology, 56,
893-897.
Berger, T., Caspar, F., Richardson, R., Kneubühler, B., Sutter, D., & Andersson, G. (2011).
Internet-based treatment of social phobia: A randomized controlled trial comparing
unguided with two types of guided self-help. Behaviour Research and Therapy, 48,
158-169.
Berger, T., Hohl, E., & Caspar, F. (2009). Internet-based treatment for social phobia: A
randomized controlled trial. Journal of Clinical Psychology, 65, 1021-1035.
Bergman, H., & Källmen, H. (2002). Alcohol use among Swedes and a psychometric
evaluation of the Alcohol Use Disorders Identification Test. Alcohol and Alcoholism,
37, 245-251.

Page 21 of 34
Accep
ted
Man
uscr
ipt
21.
Blankers, M., Koeter, M. W., & Schippers, G. M. (2010). Missing data approaches in eHealth
research: simulation study and a tutorial for nonmathematically inclined researchers.
Journal of Medical Internet Research, 12, e54.
Borge, F. M., Hoffart, A., Sexton, H., Clark, D. M., Markowitz, J. C., & McManus, F. (2008).
Residential cognitive therapy versus residential interpersonal therapy for social
phobia: a randomized clinical trial. Journal of Anxiety Disorders, 22, 991-1010.
Boschen, M. J., & Casey, L. M. (2008). The use of mobile telephones as adjuncts to cognitive
behavioral psychotherapy. Professional Psychology: Research and Practice, 39, 546-
552.
Botella, C., Gallego, M. J., Garcia-Palacios, A., Guillen, V., Banos, R. M., Quero, S., &
Alcaniz, M. (2010). An Internet-based self-help treatment for fear of public speaking:
a controlled trial. Cyberpsychology, Behavior and Social Networking, 13, 407-421.
Carlbring, P., Gunnarsdóttir, M., Hedensjö, L., Andersson, G., Ekselius, L., & Furmark, T.
(2007). Treatment of social phobia: randomized trial of internet delivered cognitive
behaviour therapy and telephone support. British Journal of Psychiatry, 190, 123-128.
Carlbring, P., Hägglund, M., Luthström, A., Dahlin, M., Kadowaki, Å., Vernmark, K., &
Andersson, G. (2013). Internet-based behavioral activation and acceptance-based
treatment for depression: A randomized controlled trial. Journal of Affective
Disorders, 148, 331-337.
Clark, D. M., & Wells, A. (1995). A cognitive model of social phobia. In R. G. Heimberg, M.
Leibowitz, D. A. Hope & F. R. Schneider (Eds.), Social phobia: Diagnosis,
assessment and treatment (pp. 63-93). New York: Guilford press.
Crippa, J. A., de Lima Osorio, F., Del-Ben, C. M., Filho, A. S., da Silva Freitas, M. C., &
Loureiro, S. R. (2008). Comparability between telephone and face-to-face structured

Page 22 of 34
Accep
ted
Man
uscr
ipt
22.
clinical interview for DSM-IV in assessing social anxiety disorder. Perspectives in
Psychiatric Care, 44, 241-247.
Cuijpers, P., Geraedts, A. S., van Oppen, P., Andersson, G., Markowitz, J. C., & van Straten,
A. (2011). Interpersonal psychotherapy of depression: A meta-analysis. American
Journal of Psychiatry, 168, 581-592.
Donker, T., Bennett, K., Bennett, A., Mackinnon, A., van Straten, A., Cuijpers, P.,
Christensen, H., & Griffiths, K. M. (2013). Internet-delivered interpersonal
psychotherapy versus internet-delivered cognitive behavioral therapy for adults with
depressive symptoms: randomized controlled noninferiority trial. Journal of Medical
Internet Research, 15, e82.
Fedoroff, I. C., & Taylor, S. (2001). Psychological and pharmacological treatments of social
phobia: a meta-analysis. Journal of Clinical Psychopharmacology, 21, 311-324.
First, M. B., Gibbon, M., Spitzer, R. L., & Williams, J. B. W. (1997). Structured clinical
interview for DSM-IV Axis I Disorders (SCID-I). Washington, D.C: American
Psychiatric Press.
First, M. B., Spitzer, R. L., Gibbon M, & Williams, J. B. W. (2002). Structured Clinical
Interview for DSM-IV-TR Axis I Disorders, Research Version, Patient Edition. (SCID-
I/P). New York: Biometrics Research, New York State Psychiatric Institute.
Fresco, D. M., Coles, M. E., Heimberg, R. G., Liebowitz, M. R., Hami, S., Stein, M. B., &
Goetz, D. (2001). The Liebowitz Social Anxiety Scale: a comparison of the
psychometric properties of self-report and clinician-administered formats.
Psychological Medicine, 31, 1025-1035.
Frisch, M. B., Cornell, J., Villanueva, M., & Retzlaff, P. J. (1992). Clinical validation of the
Quality Of Life Inventory: A measure of life satisfaction for use in treatment planning
and outcome assessment. Psychological Assessment, 4, 92-101.

Page 23 of 34
Accep
ted
Man
uscr
ipt
23.
Furmark, T. (2002). Social phobia: overview of community surveys. Acta Psychiatrica
Scandinavica, 105, 84-93.
Furmark, T., Carlbring, P., Hedman, E., Sonnenstein, A., Clevberger, P., Bohman, B.,
Eriksson, A., Hållén, A., Frykman, M., Holmström, A., Sparthan, E., Tillfors, M.,
Nilsson Ihrfelt, E., Spak, M., Eriksson, A., Ekselius, L., & Andersson, G. (2009).
Guided and unguided self-help for social anxiety disorder: randomised controlled trial.
British Journal of Psychiatry, 195, 440-447.
Furmark, T., Holmström, A., Sparthan, E., Carlbring, P., & Andersson, G. (2013). Social fobi
- Effektiv hjälp med kognitiv beteendeterapi [Social phobia - effective help via CBT]
(2 ed.). Stockholm: Liber.
Hedman, E., Andersson, E., Ljótsson, B., Andersson, G., Rück, C., & Lindefors, N. (2011).
Cost-effectiveness of Internet-based cognitive behavior therapy vs. cognitive
behavioral group therapy for social anxiety disorder: results from a randomized
controlled trial. Behaviour Research and Therapy, 49, 729-736.
Hedman, E., Andersson, G., Ljótsson, B., Andersson, E., Rück, C., Mörtberg, E., &
Lindefors, N. (2011). Internet-based cognitive behavior therapy vs. cognitive
behavioral group therapy for social anxiety disorder: A randomized controlled non-
inferiority trial. PloS ONE, 6(3), e18001.
Hedman, E., Ljótsson, B., & Lindefors, N. (2012). Cognitive behavior therapy via the
Internet: a systematic review of applications, clinical efficacy and cost-effectiveness.
Expert Review of Pharmacoeconomics and Outcomes Research, 12, 745-764.
Hedman, E., Ljótsson, B., Rück, C., Furmark, T., Carlbring, P., Lindefors, N., & Andersson,
G. (2010). Internet administration of self-report measures commonly used in research
on social anxiety disorder: a psychometric evaluation Computers in Human Behavior,
26, 736-740.

Page 24 of 34
Accep
ted
Man
uscr
ipt
24.
Heimberg, R. G., Horner, K. J., Juster, H. R., Safren, S. A., Brown, E. J., Schneier, F. R., &
Liebowitz, M. R. (1999). Psychometric properties of the Liebowitz Social Anxiety
Scale. Psychological Medicine, 29, 199-212.
Jacobson, N. S., & Truax, P. (1991). Clinical significance: A statistical approach to defining
meaningful change in psychotherapy research. Journal of Consulting and Clinical
Psychology, 59, 12-19.
Klasnja, P., & Pratt, W. (2012). Healthcare in the pocket: mapping the space of mobile-phone
health interventions. Journal of Biomedical Informatics, 45, 184-198.
Klerman, G. L., Dimascio, A., Weissman, M., Prusoff, B., & Paykel, E. S. (1974). Treatment
of depression by drugs and psychotherapy. American Journal of Psychiatry, 131, 186-
191.
Klerman, G. L., Weissman, M. M., Rounsaville, B. J., & Chevron, E. S. (1984). Interpersonal
psychotherapy of depression. New York: Basic Books.
Lipsitz, J. D., Markowitz, J. C., Cherry, S., & Fyer, A. J. (1999). Open trial of interpersonal
psychotherapy for the treatment of social phobia. American Journal of Psychiatry,
156, 1814-1816.
Luxton, D. D., McCann, R. A., Bush, N. E., Mishkind, M. C., & Reger, G. M. (2011).
mHealth for mental health: Integrating smartphone technology in behavioral
healthcare. Professional Psychology: Research and Practice, 42, 505-512.
Ly, K. H., Dahl, J., Carlbring, P., & Andersson, G. (2012). Development and initial
evaluation of a smartphone application based on acceptance and commitment therapy.
SpringerPlus, 1, 11.
Markowitz, J. C., Leon, A. C., Miller, N. L., Cherry, S., Clougherty, K. F., & Villalobos, L.
(2000). Rater agreement on interpersonal psychotherapy problem areas. Journal of
Psychotherapy Practice and Research, 9, 131-135.

Page 25 of 34
Accep
ted
Man
uscr
ipt
25.
Mattick, R. P., & Clarke, J. C. (1998). Development and validation of measures of social
phobia scrutiny fear and social interaction anxiety. Behaviour Research and Therapy,
36, 455-470.
Ponniah, K., & Hollon, S. D. (2008). Empirically supported psychological interventions for
social phobia in adults: a qualitative review of randomized controlled trials.
Psychological Medicine, 38, 3-14.
Rubin, D. B., & Schenker, N. (1991). Multiple imputation in health-care databases: An
overview and some applications. Statistics in Medicine, 10, 585-598.
Selin, K. H. (2003). Test-retest reliability of the alcohol use disorder identification test in a
general population sample. Alcoholism: Clinical and Experimental Research, 27,
1428-1435.
Sheehan, D. V., Lecrubier, Y., Sheehan, K. H., Amorim, P., Janavs, J., Weiller, E., Hergueta,
T., Baker, R., & Dunbar, G. C. (1998). The Mini-International Neuropsychiatric
Interview (M.I.N.I.): the development and validation of a structured diagnostic
psychiatric interview for DSM-IV and ICD-10. The Journal of Clinical Psychiatry, 59
Suppl 20, 22-33.
Smit, F., Cuijpers, P., Oostenbrink, J., Batelaan, N., de Graaf, R., & Beekman, A. (2006).
Costs of nine common mental disorders: implications for curative and preventive
psychiatry. Journal of Mental Health Policy and Economy, 9, 193-200.
Stangier, U., Schramm, E., Heidenreich, T., Berger, M., & Clark, D. M. (2011). Cognitive
therapy vs interpersonal psychotherapy in social anxiety disorder: a randomized
controlled trial. Archieves of General Psychiatry, 68, 692-700.
Stein, D. J., Ipser, J. C., & Balkom, A. J. (2004). Pharmacotherapy for social phobia.
Cochrane database of systematic reviews (Online)(4), CD001206.

Page 26 of 34
Accep
ted
Man
uscr
ipt
26.
Svanborg, P., & Åsberg, M. (1994). A new self-rating scale for depression and anxiety states
based on the Comprehensive Psychopathological Rating Scale. Acta Psychiatrica
Scandinavica, 89, 21-28.
Tillfors, M., Carlbring, P., Furmark, T., Lewenhaupt, S., Spak, M., Eriksson, A., Ekselius, L.,
Westling, B., & Andersson, G. (2008). Treating university students with social phobia
and public speaking fears: Internet delivered self-help with or without live group
exposure sessions. Depression and Anxiety, 25, 708-717.
Titov, N., Andrews, G., Schwencke, G., Drobny, J., & Einstein, D. (2008). Shyness 1:
distance treatment of social phobia over the Internet. The Australian and New Zealand
Journal of Psychiatry, 42, 585-594.
Titov, N., Andrews, G., Schwencke, G., Robinson, E., Peters, L., & Spence, J. (2010).
Randomized controlled trial of Internet cognitive behavioural treatment for social
phobia with and without motivational enhancement strategies. Australian and New
Zealand Journal of Psychiatry, 44, 938-945.
Tulbure, B. T. (2011). The efficacy of Internet-supported intervention for social anxiety
disorder: A brief meta-analytic review. Procedia - Social and Behavioral Sciences, 30,
552-557.
Watts, S., Mackenzie, A., Thomas, C., Griskaitis, A., Mewton, L., Williams, A., & Andrews,
G. (2013). CBT for depression: a pilot RCT comparing mobile phone vs. computer.
BMC Psychiatry, 13, 49.
Weissman, M. M., Markowitz, J. C., & Klerman, G. L. (2000). Comprehensive guide to
interpersonal psychotherapy. New York: Basic Books.
Weissman, M. M., Markowitz, J. C., & Klerman, G. L. (2007). Clinician's quick guide to
interpersonal psychotherapy. Oxford: Oxford University Press.

Page 27 of 34
Accep
ted
Man
uscr
ipt
27.
Vickers, A. J., & Altman, D. G. (2001). Statistics notes: Analysing controlled trials with
baseline and follow up measurements. British Medical Journal, 323, 1123-1124.
Zanarini, M. C., & Frankenburg, F. R. (2001). Attainment and maintenance of reliability of
axis I and II disorders over the course of a longitudinal study. Comprehensive
Psychiatry, 42, 369-374.
�

Page 28 of 34
Accep
ted
Man
uscr
ipt
28.
Captions
Figure 1. Flowchart participant flow. Abbreviations: mIPT, mobile-based
Interpersonal Psychotherapy, mCBT, mobile-based Cognitive Behavior Therapy,
SAD, Social Anxiety Disorder.
Figure 2. Weekly change on LSAS-SR. Scores for both groups at each assessment
point; pre-treatment, treatment and post-treatment. Vertical bars denote 95% CI,
confidence interval.
Table 1. Demographic description of the participants.
Variable mIPT, n = 25 mCBT, n = 27 Total, N = 52

Page 29 of 34
Accep
ted
Man
uscr
ipt
29.
Gender Women (%) 14 (56) 13 (48.1) 27 (51.9)
Men (%) 11 (44) 14 (51.9) 25 (48.1)
Age Mean age (SD) 39.08 (11.3) 34.70 (11.2) 36.81 (11.4)
Min-Max 20-65 21-60 20-65
Highest
completed
educational
level
Nine-year
compulsory
school (%)
0 (0) 2 (7.4) 2 (3.8)
Senior high
school /
Secondary
school (%)
13 (52) 13 (48.1) 26 (50)
University (%) 12 (48) 12 (44.4) 24 (46.2)
Years at
university
Mean years
(SD)
1.78 (2.1) 2.07 (2.6) 1.93 (2.3)
Min – max 0-6 0-8 0-8
Table 2. Medication data of the participants.
mIPT, n = 25 mCBT, n = 27 Total, N=52
Psycho-tropic
SSRI (%)
Beta antagonists
3 (12)
0 (0)
0 (0)
3 (11.1)
3 (5.8)
3 (5.8)

Page 30 of 34
Accep
ted
Man
uscr
ipt
30.
Other
medication
(%)
NaSSA (%)
Sedative-
hypnotic (%)
Thyroid
hormones (%)
ACE inhibitors
(%)
1 (4)
1 (4)
0 (0)
1 (4)
0 (0)
0 (0)
2 (7.4)
0 (0)
1 (1.9)
1 (1.9)
2 (3.8)
1 (1.9)
Abbreviations: SSRI, Selective Serotonin Reuptake Inhibitor, NaSSA, Noradrenergic and Specific Serotonergic
Antidepressant, ACE inhibitor, Angiotensin-Converting-Enzyme inhibitor.
Table 3. Means, SD’s, within and between group effect sizes (Cohen’s d), confidence
intervals,
F-values and significance levels for primary and secondary outcome variables.
Measure Group Pre Post – est. values Within group ES Between group ES F-values
n=52 n=52 (1, 49)
M (SD) M (SD) d CI lo CI hi d CI lo CI hi
LSAS-SR mCBT 60.19 (18.95) 38.93 (23.18) 0.99 0.58 1.39
0.64 0.06 1.22 5.18 *
mIPT 65.72 (27.15) 54.41 (25.19) 0.43 0.09 0.77

Page 31 of 34
Accep
ted
Man
uscr
ipt
31.
SIAS mCBT 45.15 (15.81) 34.30 (14.76) 0.71 0.35 1.07
0.72 0.14 1.30
5.83 *
mIPT 50.12 (14.06) 44.54 (13.76) 0.40 0.11 0.70
SPS mCBT 32.59 (11.31) 23.42 (12.15) 0.78 0.30 1.27
0.63 0.05 1.22 2.97
mIPT 37.64 (15.07) 31.30 (12.81) 0.45 0.12 0.77
BAI mCBT 17.30 (9.25) 14.79 (10.97) 0.25 -0.31 0.81
0.46 -0.10 1.03 2.09
mIPT 19.80 (12.12) 20.02 (11.56) -0.02 -0.41 0.37
MADRS-S mCBT 11.70 (5.09) 10.44 (4.77) 0.26 -0.16 0.67
0.88 0.28 1.47 7.25 **
mIPT 14.08 (6.30) 14.62 (4.77) -0.10 -0.61 0.42
QOLI mCBT 1.09 (1.58) 1.41 (1.66) -0.20 -0.55 0.16
0.37 -0.25 0.99 0.12
mIPT 0.37 (1.59) 0.82 (1.51) -0.29 -0.72 0.13
Abbreviations: mCBT, mobile-based Cognitive Behavior Therapy; mIPT, mobile-based Interpersonal Therapy; Pre, pre- treatment; Post, post-
treatment; LSAS-SR, Liebowitz Social Anxiety Scale – Self Report; SIAS, Social Interaction Scale; SPS, Social Phobia Scale; MADRS-S,
Montgomery-Åsberg Depression Rating Scale-Self Report; BAI, Beck Anxiety Inventory; QOLI, Quality of Life Inventory.
*p < .05, ** p < .01 = significance level for effect of group (ANCOVA).

Page 32 of 34
Accep
ted
Man
uscr
ipt
mCBT
Allocated to intervention, n= 27 Dropouts, n=3
mIPT
Allocated to intervention, n=25 Dropouts, n=6
Included in ITT analysis, n= 27 Included in Completers analysis, n=24
Included in ITT analysis,n=25
Included in Completers analysis, n= 19
Diagnostic interview. Assessed for eligibility, n=68
235 individuals in total applied to participate via the project´s homepage
52 subjects were included in the study and randomized
Excluded, n= 142 Did not complete online screening forms at all, did not fully complete online
screening forms or applied to late.
Excluded, n= 16
Did not meet inclusion criteria for SAD, n=4 Suicide risk, n=1
History of CBT during the last four years, n=1 No access to smartphone, n=1
Referred to outpatient psychiatric care; n=3 Alcohol abuse/dependence, n=1
Declined to participate, n=1 Screened and interviewed, met inclusion criteria, but could not commence
treament in time, n= 4
Invited to participate in diagnostic interview (contacted via telephone or e-mail), n= 76
Fully completed online screening forms, n= 93
Excluded, n= 17 Did not meet inclusion criteria as judged via screening forms.
Excluded, n= 8
Could not be reached via e-mail or telephone or declined to participate.
Figure

Page 33 of 34
Accep
ted
Man
uscr
ipt
0
10
20
30
40
50
60
70
80
90
Pre W1 W2 W3 W4 W5 W6 W7 W8 W9 Post
mCBT
mIPT
Figure

Page 34 of 34
Accep
ted
Man
uscr
ipt
Highlights The effects of CBT using mobile phone administration (mCBT) for social anxiety disorder was compared interpersonal psychotherapy (mIPT) Guided mCBT was found to be superior to mIPT. The finding add to the growing literature on guided self-help for social anxiety disorder
Related Documents