
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript


Dr. Mohammad Kurniawan, MSc (stroke med.), FICADept. Neurology Faculty of Medicine, Universitas Indonesia
Cipto Mangunkusumo National Hospital
Code Stroke in Pandemic Era

STROKE An episode of neurological dysfunction caused by focal cerebral, spinal, or retinal infarction/ischemia, based on pathological, imaging, or other objective evidence in a defined vascular distribution; and/or clinical evidence of cerebral, spinal cord, or retinal focal ischemic injury based on symptoms persisting ≥24 hours or until death, and other etiologies excluded
(AHA/ASA Expert Consensus 2013)

EPIDEMIOLOGY
1 in 4 of uswill have a stroke
Every 2 second, there will be 1 person suffered from stroke
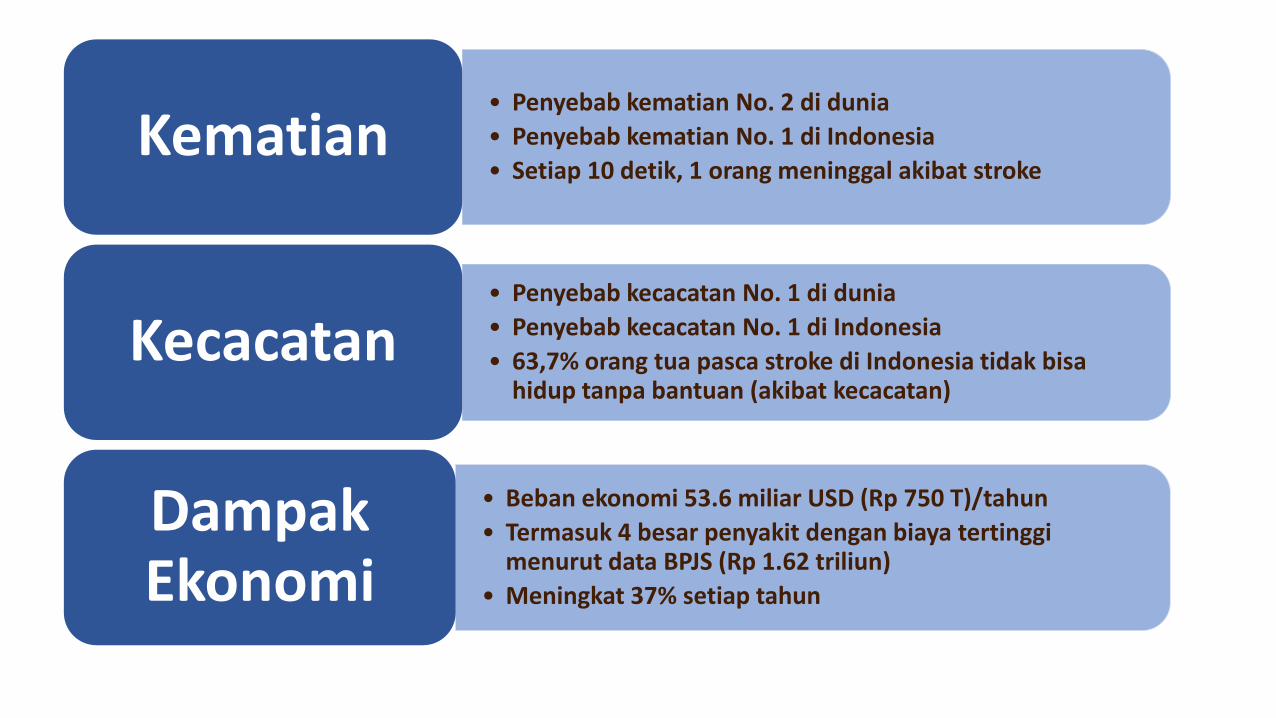
• Penyebab kematian No. 2 di dunia
• Penyebab kematian No. 1 di Indonesia
• Setiap 10 detik, 1 orang meninggal akibat strokeKematian
• Penyebab kecacatan No. 1 di dunia
• Penyebab kecacatan No. 1 di Indonesia
• 63,7% orang tua pasca stroke di Indonesia tidak bisahidup tanpa bantuan (akibat kecacatan)
Kecacatan
• Beban ekonomi 53.6 miliar USD (Rp 750 T)/tahun
• Termasuk 4 besar penyakit dengan biaya tertinggimenurut data BPJS (Rp 1.62 triliun)
• Meningkat 37% setiap tahun
DampakEkonomi

Time is Brain, every minute counts
Blockage of one blood vessel will cause ischemia
Saver JL, Stroke 2006
STROKE
Time lost is Brain lost
TimeNeurons
LostSynapses
LostMyelinated Fibers Lost
Premature Aging
1 second 32,000 230 million 200 m 8.7 hours
1 minute 1.9 million 14 billion 12 km 3.1 weeks
1 hour 120 million 830 billion 714 km 3.6 years
Complete 1.2 billion 8.3 trillion 7140 km 36 years


Stroke is Emergency Time is Brain Tissue
Saver. Stroke 2006;37:263-266.González. Am J Neuroradiol 2006;27:728-735.
Donnan. Lancet Neurol 2002;1:417-425.
An untreated patient
loses approximately 1.9
million neurons every
minute in the ischaemic
area
Revascularization /
reperfusion offers the
potential to reduce the
extent of ischaemic injury
Ischaemic core
(brain tissue
destined to die)
Penumbra
(salvageable
brain area)
FAILED TO UNDERSTAND…

Intravenous thrombolysis (NNT : 3.6 to 5.9)Mechanical thrombectomy (NNT : 2.6/5)Intra-arterial thrombolysis (NNT : 7.7)
Goal : Recanalization - Reperfusion

Code Stroke
A term used to prioritize the hyperacute assessment and care of a patient presenting
with signs and symptoms concerning for stroke.
The word code brings forward a sense of nuance with measured urgency without
compromising precision in diagnosing and treating patients with stroke.
Intravenous Thrombolysis
Endovascular treatment with Mechanical Thrombectomy

Intravenous Thrombolysis (IVT)

Stroke Thrombolysis Evidences
NINDS TPA Stroke Trial
Global outcome statistic: OR=1.7, 50% v. 38%= 12% benefit
Excellent outcome at 3 months on all scales
52%
38%43%
26%
45%
31%34%
21%
0%
10%
20%
30%
40%
50%
60%
Barthel
Index
Rankin
Scale
Glasgow
Outcome
NIHSS
score
TPA
Placebo
N Engl J Med 1995;333:1581-7

ECASS 3 - EndpointsDay 90: NINDS global endpoint statistic
(mRS 0-1; BI ≥95; NIHSS ≤1 or >8 point improvement; GOS 1)
Hacke et al; the ECASS 3 Investigators. N Engl J Med 2008;359:1317-1329.
rt-PA
(N=418)
Placebo
(N=403)
OR
(95% CI)
p
Global outcome n/a n/a 1.28
(1.00–1.65)
0.05
mRS score ≤1 219 (52.4%) 182 (45.2%) 1.34
(1.02–1.76)
0.04‡
BI score ≥95 265 (63.4%) 236 (58.6%) 1.23
(0.93–1.62)
0.16‡
NIHSS score ≤1 210 (50.2%) 174 (43.2%) 1.33
(1.01–1.75)
0.04‡
GOS score 1 213 ( 51.0%) 183 (45.4%) 1.25
(0.95–1.64)
0.11‡
0.5 1 1.5
Favours placebo Favours rt-PAITT, intent-to-treat; ‡ p value was obtained by
the Pearson chi-square test of proportions

NNT to Reach Optimal Benefit from IV TPA
(mRS 0-1)
Hacke W et al. Lancet 2004 ; Lees KR et al. Lancet 2010

Evidence - Based Guidelines of StrokeThrombolysis
I.V. rt-PA (0.9 mg/kg body weight, max. 90 mg), with 10% of the dose given as a
bolus followed by a 60-minute infusion, is recommended within 4.5 hours of
onset of ischaemic stroke (Class I, Level A)
ESO Guidelines 2021
Intravenous rt-PA is recommended for selected patients who may be treated
within 3 hours of onset of ischemic stroke (Class I Level A)
rt-PA should be administered to eligible patients who can be treated in the time
period of 3 to 4.5 hours after stroke (Class I Level B)
AHA/ASA Guideline 2019
Alteplase direkomendasikan pada Stroke iskemik, onset pemberian trombolisis
direkomedasikan ialah ≤4,5 jam atau ≤6 jam (bukan wake up stroke) pada jalur
intravena dengan sirkulasi anterior
(PNPK Stroke 2019)

Recommendation Regarding Thrombolytic Treatment in Acute Ischemic Stroke
▪ An organized protocol for the emergency evaluation of patient with suspected stroke is reccommended (I/B)
▪ It is recommended that DTN time goals be established. A primary goal of achieving DTN times within 60 minutes in ≥50% of AIS patients treated with IV alteplase should be established (I/B)
▪ It may be reasonable to establish a secondary DTN time goal of achieving DTN times within 45 minutes in ≥50% of patients with AIS who were treated with IV alteplase (Iib/C)
▪ Designation of an acute stroke team that includes physicians, nurses, and laboratory/radiology personnel is recommended. Patients with stroke should have a careful clinical assessment, including neurological examination (I/A)
▪ Multicomponent quality improvement initiatives, which include ED education and multidisciplinary teams with access to neurological expertise, are recommended to safely increase IV thrombolytic treatment (I/B)
AHA/ASA Guideline Guidelines for the Early Management of Patients With Acute Ischemic Stroke 2019
Early Management of Patients With Acute Ischemic Stroke HOSPITAL STROKE TEAMS

NIH-Recommended ED Response Time
NINDS NIH website. Stroke proceedings. Latest update 2008
DTN ≤60 min : the “golden hour” for evaluating & treating acute stroke
T=0
Suspected
stroke patient
arrives at
stroke unit
≤10 min
Initial MD evaluation
(including patient
history, lab work
initiation, & NIHSS)
≤ 15 min
Stroke team
notified
(including
neurologic
expertise)
≤ 25 min
CT scan
initiated
≤ 45 min
CT & labs
interpreted
≤ 60 min
rt-PA
given if
patient
is eligible

THROMBOLYSIS PATHWAY
➊ Arrival to ED
➋ A&PE assessment
➌ Stroke team notified
➍ Order priority CT Brain
➎ Lab & ECG exams
➏ CT scan performed
➐ CT report obtained
➑ Patient informed and consent
obtained
➒ Reconstitution and drawing up of
Alteplase
➓ Thrombolysis is initiated
INCLUSION CRITERIA
1. Clinical signs and symptoms of definite acute stroke
2. Clear time of onset
3. Presentation within 3 hrs of acute onset
4. Haemorrhage excluded by CT scan
5. Age 18 - 80 years old
6. Consent to treat (every effort must be made to contact next of kin)
EXCLUSION CRITERIA1. Rapidly improving or minor stroke symptoms (NIHSS 1-4)
2. NIHSS < 5 or >25
3. Stroke or serious head injury within 3 months
4. Major surgery, obstetrical delivery, external heart massage in last 14 days
5. Seizure at onset of stroke
6. Prior stroke and concomitant diabetes
7. Severe haemorrhage in last 21 days
8. Increase bleeding risk
9. History of central nervous damage (neoplasm, haemorrhage, aneurysm, spinal or intracranial surgery or haemorrhagic retinopathy)
10. Blood pressure above 185 mmHg systolic or 110 mmHg diastolic
11. Symptoms suggestive of SAH (even if CT is normal)
12. Known clotting disorder
13. APTT abnormal, INR>1.5
14. Suspected iron deficient anaemia
15. Thrombocytopenia <100,000
16. Hypoglycaemia or hyper glycaemia <50 mg/dL >400 mg/dL
17. Bacterial endocarditis, pericarditis
18. Acute pancreatitis
19. Ulcerative GI disease in last 3 months, oesophageal varices, arterial-aneurysm, arterial/venous malformation.
20. Severe liver disease including cirrhosis, acute hepatitis
DTN
The Golden Hour

Pasien dicurigaiStroke
DOKTER EMERGENSICURIGA STROKE AKUT < 4.5 jam)
Gejala FAST : (Lihat Ceklis)
-Face (mulut mencong)-Arm (lemah separuh badan)-Speech (pelo/afasia)-Time last normal (< 4.5 jam)
Dalam 10 menit :1. EKG2. GDS (stick)3. Lab (bila perlu)
(Warfarin → INR ; NOAC → APTT)4. Order Urgent CT/MRI Brain 5. Nilai NIHSS6. Pasang iv-line7. Call Neurologist
DPJP NEUROLOGI
Konsul / Refer cito ! Neurologi
• IGD (Triage)• Ruang Rawat
ACTIVATE CODE STROKE
DPJP Neurologi• Konfirmasi Stroke Iskemik• Klarifikasi onset gejala• NIHSS• Order Obat Alteplase
UrgentCT/MRI Brain
ELIGIBILITAS TROMBOLISISLihat Ceklis
START TROMBOLISIS
TRANSFER KE RUANGAN (STROKE UNIT/HCU/ICU)
•Dosis Alteplase 0.6-0.9 mg/kgBB• Berikan bolus 10% dosis• Sisanya di drip dalam 1 jam
CO
DE
STR
OK
E R
SCM
/FK
UI
DN
T: 6
0 M
inu
tes
TROMBEKTOMI @CATHLAB

Mechanical Thrombectomy(Endovascular Thrombectomy/EVT) in Acute Ischemic Stroke

History of EVT in Hyperacute Ischemic Stroke
Local intra-arterial thrombolysis1988 - 1998



Terapi intervensi endovaskular
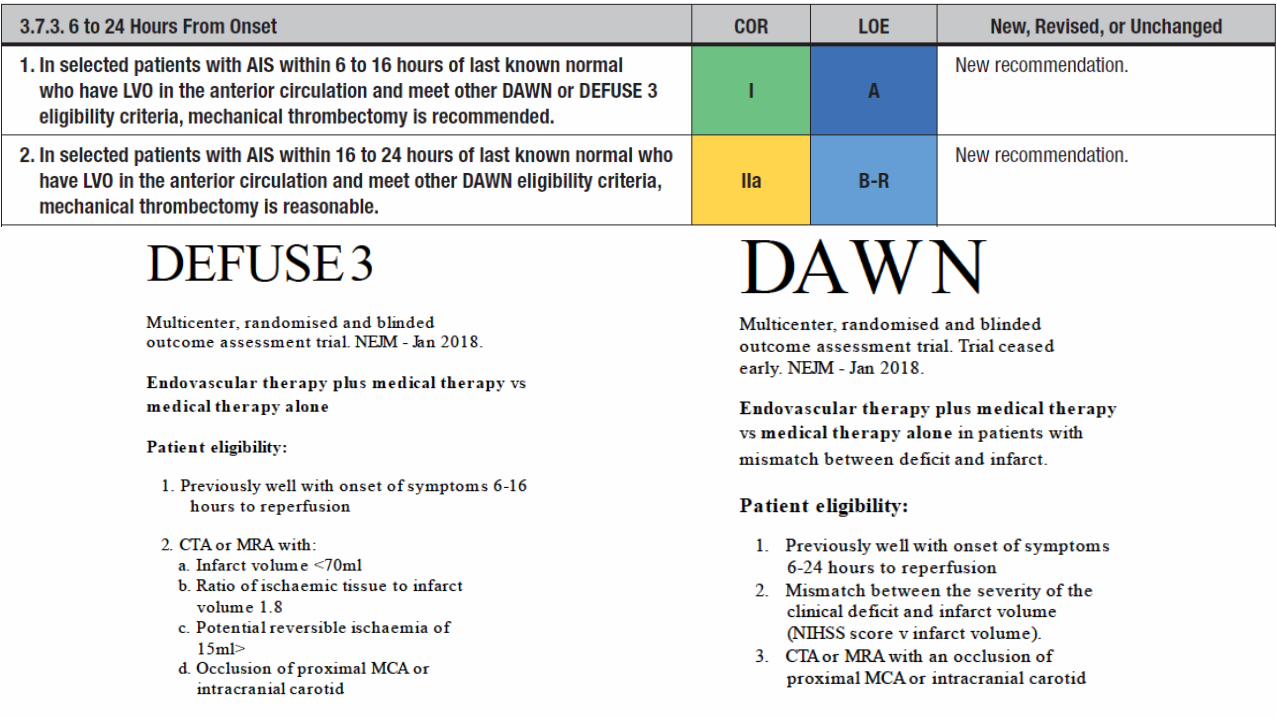
• Pemberian rtPA (Alteplase) harus dilakukan secepatnya pada pasien yang memenuhi kriteria (kelas I, peringkat bukti A).
• Pasien sebaiknya mendapatkan terapi endovaskular dengan menggunakanstent retriever jika memenuhi kriteria sebagai berikut (kelas I, peringkatbukti A):
a) Skor mRS prestroke 0 sampai 1b) Stroke disebabkan karena oklusi pada arteri karotis interna atau arteri serebri media
cabang proksimal.c) Usia ≥18 tahun.d) Terapi dapat dimulai (puncture) dalam 6 jam setelah onset stroke.e) Skor NIHSS ≥6.f) Skor ASPECTS ≥6.


Sharing our experience…
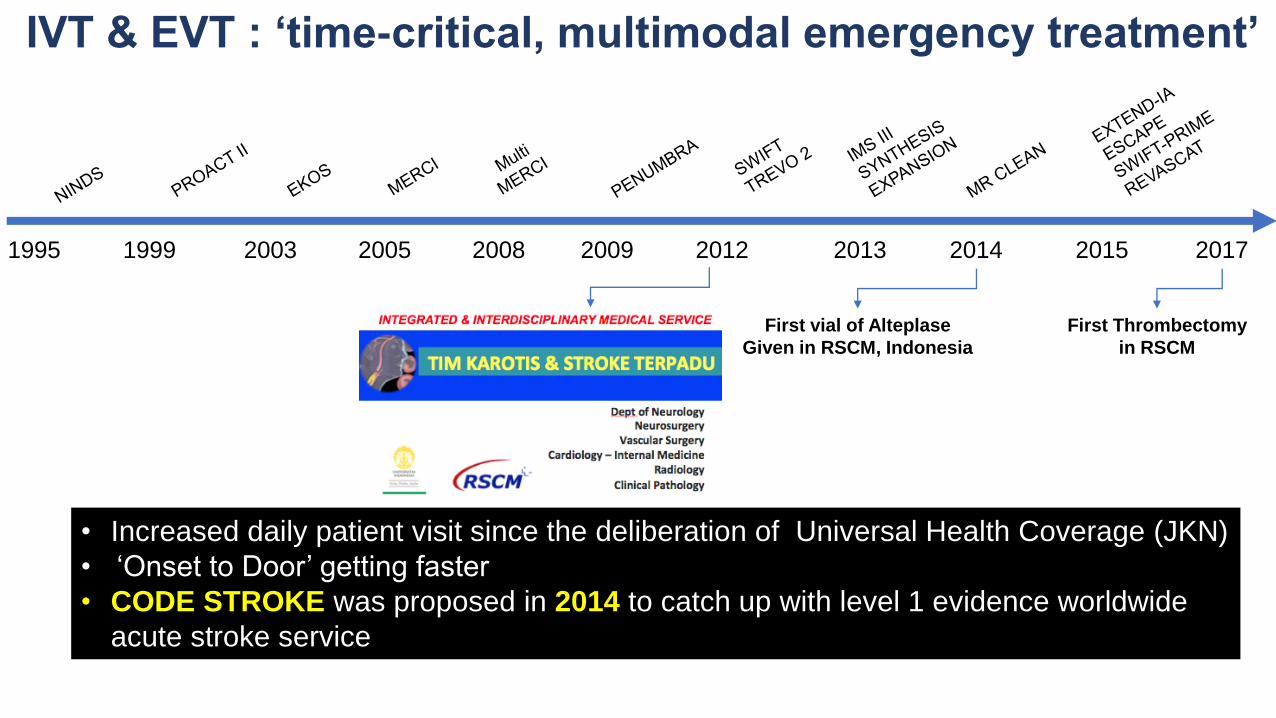
IVT & EVT : ‘time-critical, multimodal emergency treatment’
First vial of Alteplase
Given in RSCM, Indonesia
1995 1999 2003 2005 2008 2009 2012 2013 2014 2015 2017
First Thrombectomy
in RSCM
• Increased daily patient visit since the deliberation of Universal Health Coverage (JKN)
• ‘Onset to Door’ getting faster
• CODE STROKE was proposed in 2014 to catch up with level 1 evidence worldwide
acute stroke service

What we have achieved…
≤ 60 mins
Door to Needle≤ 25 mins
Door to CT
>40 casesThrombectomy
since Jan 2017
≤420
minsOnset to Puncture
CODE STROKEWarning system for integrated-team trained residents, fellows, nurses,
pharmacy, administration, & stroke team (neurologist, neurosurgeon,
neurointerventionist & radiologist). ‘Messenger App’ based communication
>300 cases Thrombolysissince Nov 2014
>500Code Stroke Activation
10 min 30 min
9.7% of all ischemic stroke cases ; 90% of candidate

CASE• Male, 38 yo• Sudden right side weakness, aphasia• Onset 1 hours


Result
•Good recanalization, TICI III
•After 24 hours, the symptom improved (motoric power from 0/5 become 4/5)
•Fully recover after 5 days (no paresis, no aphasia)
•Currently, active as physician

During pandemic era..• Patients with stroke who require hospitalization during pandemic are at increased
risk of suboptimal outcomes.
• Currently, in the setting of COVID-19 pandemic, similar medical emergencies such as cardiopulmonary arrest (code blue) are being modified to the protected designation to provide an additional layer of protection for healthcare professionals and patients.
• These measures include the use of personal protective equipment (PPE) andmodifications to human performance factors in relation to triage processes, team member role designation, and dynamics while caring for patients during a protected code.
Protected Code Stroke

SCREENING• Travel history ≤ 14 days (travel abroad or local transmission)
• Risk of infectious contact
• Infectious symptoms
• Neurological symptoms
• For patients being transferred from other health facilities, an infection control screen and travel history screen should be completed and communicated before transfer.
Protected Code Stroke
Activated

Protected Code Stroke• The appropriate use of PPE by all team members → full-sleeved gown,
surgical mask, eye protection (face shield and/or goggles), head covering and gloves.
• A fitested N95 respirator when there is an aerosolizing procedure →oropharyngeal/nasal (open) suctioning, bag-valve-mask ventilation, and intubation
• Recommend placement of a surgical mask on the nonintubated patient →should remain on the patient during transportation to, during, and back from imaging if the patient is able to tolerate.
• Avoid exam maneuvers that increase repeat contact between provider and patient such as figer-nosefinger and repeat assessments such as for motor and speech.



TAKE HOME MESSAGE• Clinical assessment and intervention during the hyperacute stroke
phase have unique challenges during the COVID-19 pandemic
• There are challenges to maintaining high quality care and promoting the best chance for recovery, while at the same time preventing transmission of pathogens to team members or other patients.
• Vigilant screening processes, proper adherence to established infection prevention and control measures, and a coordinated team response all contribute to a safe and resilient clinical stroke team during these challenging times.
TIME IS STILL BRAIN

Related Documents











