Cochlear Cochlear Implants Implants Glen T. Porter, MD Glen T. Porter, MD Arun K. Gadre, MD Arun K. Gadre, MD Department of Otolaryngology, Head & Neck Department of Otolaryngology, Head & Neck Surgery Surgery Galveston, TX Galveston, TX

Cochlear Implants Glen T. Porter, MD Arun K. Gadre, MD Department of Otolaryngology, Head & Neck Surgery Galveston, TX.
Dec 23, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Cochlear ImplantsCochlear Implants
Glen T. Porter, MDGlen T. Porter, MDArun K. Gadre, MDArun K. Gadre, MD
Department of Otolaryngology, Head & Neck SurgeryDepartment of Otolaryngology, Head & Neck SurgeryGalveston, TXGalveston, TX

History of Cochlear ImplantsHistory of Cochlear Implants
VoltaVolta
Djourno and EyriesDjourno and Eyries
House, Doyle, House, Doyle, SimmonsSimmons
1972 Single-channel 1972 Single-channel implantimplant
1984 FDA approval1984 FDA approval
1990’s1990’s
BeyondBeyond
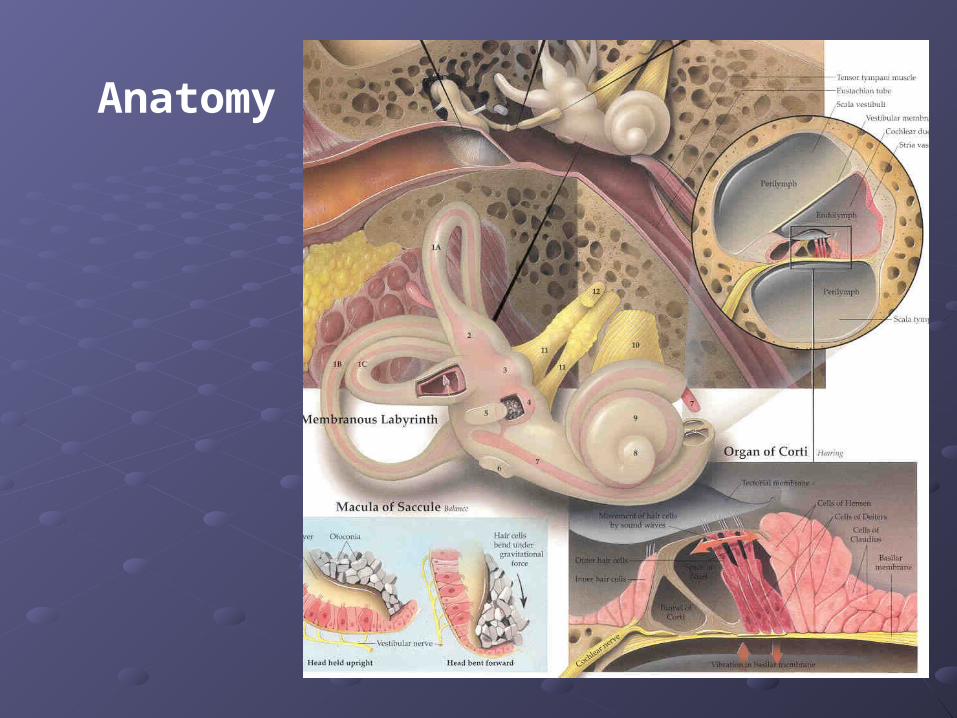
AnatomyAnatomyAnatomy

AnatomyAnatomyScala tympani
Scala vestibuli
Cochlear duct
Basilar membrane
Vestibular membrane
Tectoral membrane
Hair cells (outer/inner)
Cochlear nerve fibers
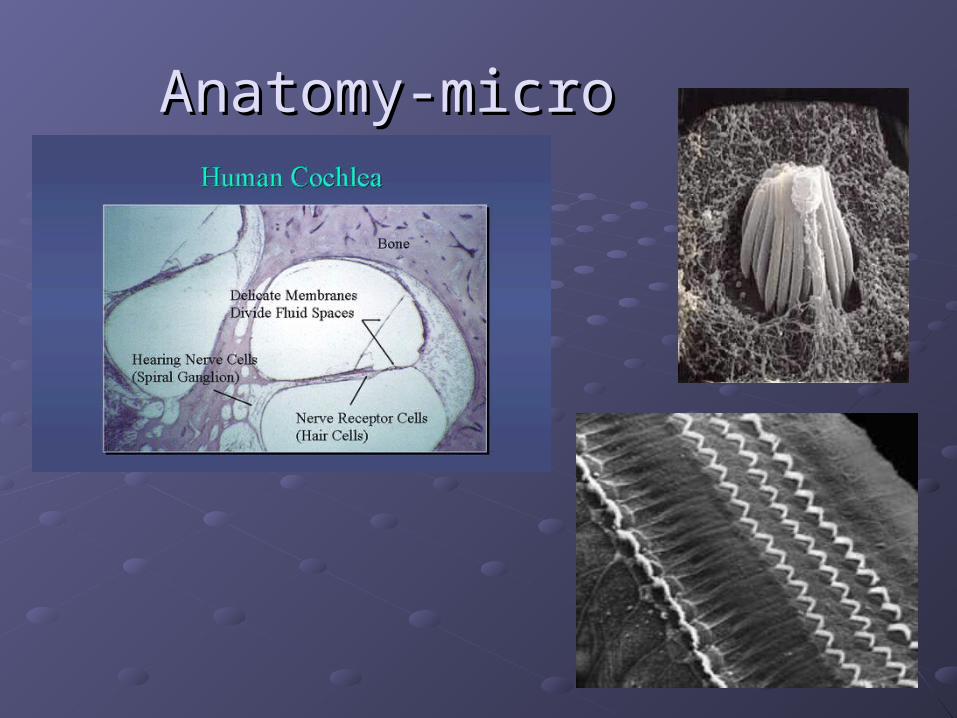
Anatomy-microAnatomy-micro

Physiology of Hearing

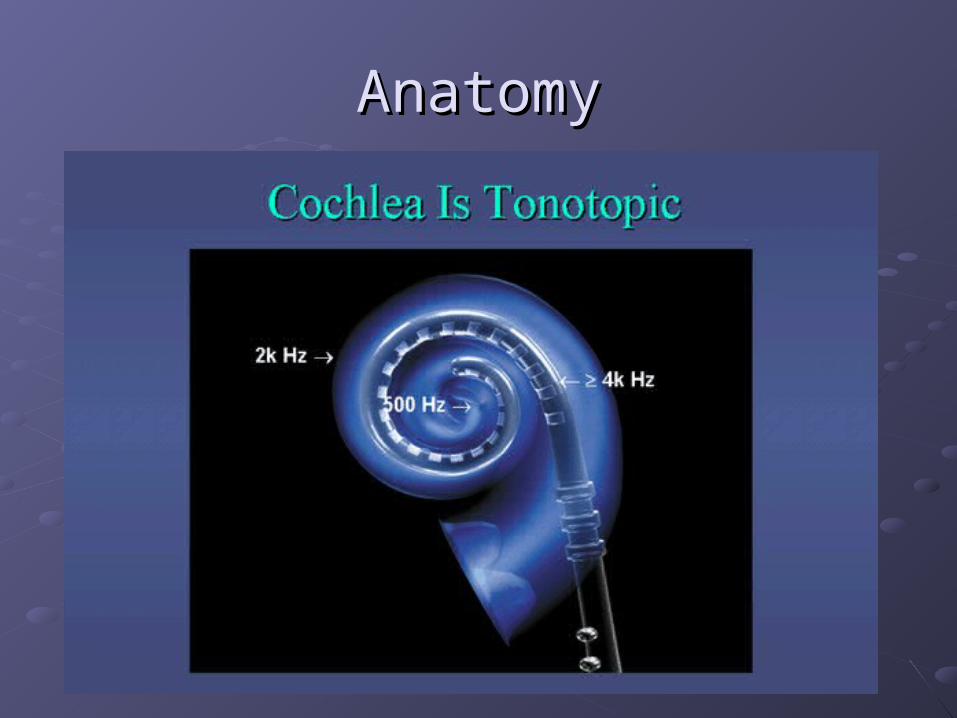
AnatomyAnatomy
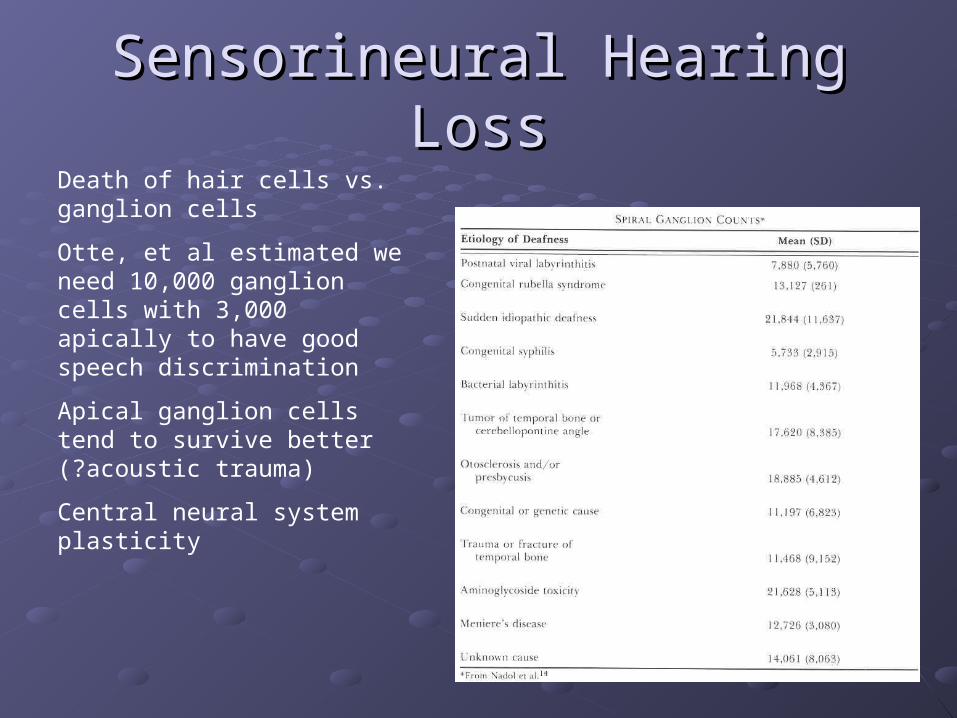
Sensorineural Hearing LossSensorineural Hearing LossDeath of hair cells vs. ganglion cells
Otte, et al estimated we need 10,000 ganglion cells with 3,000 apically to have good speech discrimination
Apical ganglion cells tend to survive better (?acoustic trauma)
Central neural system plasticity

Pathologic AnatomyPathologic Anatomy

Anatomy of Sound
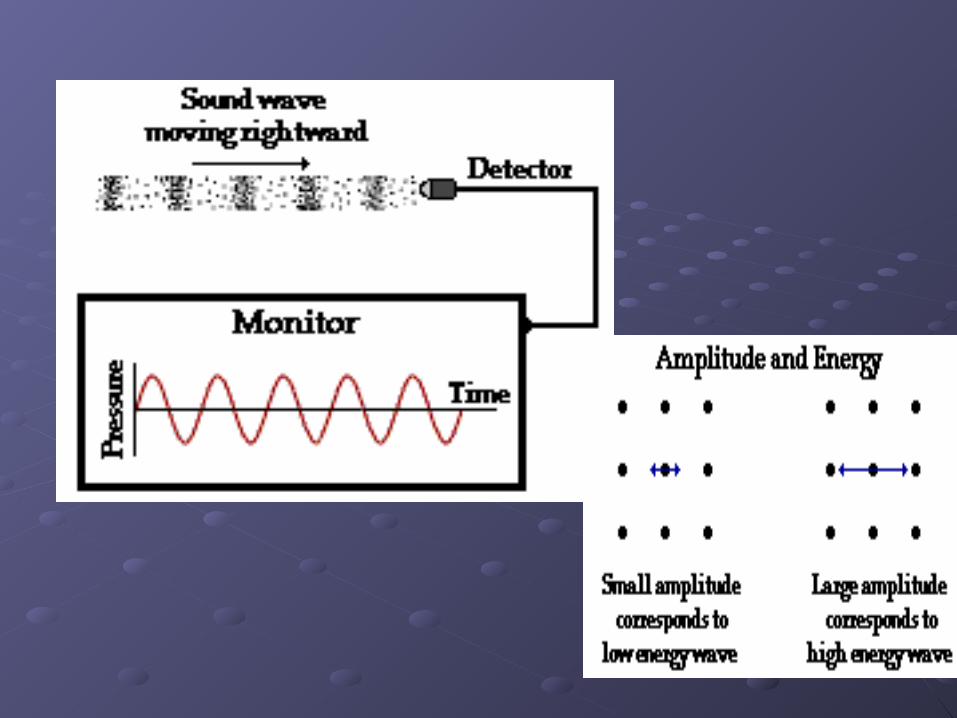


Anatomy of SpeechAnatomy of Speech
Mix of frequenciesMix of frequenciesSpeech recognition is “top-down” process Speech recognition is “top-down” process Formant frequencies: frequency maximum Formant frequencies: frequency maximum based on vocal tractbased on vocal tractF0 is fundamental frequencyF0 is fundamental frequencyF1 & F2—contribute to vowel identificationF1 & F2—contribute to vowel identificationF3—l,r (lateral and retroflex glides)F3—l,r (lateral and retroflex glides)F4 & F5—higher frequency speech soundsF4 & F5—higher frequency speech soundsSome speech based on amplitude—k, f, l, sSome speech based on amplitude—k, f, l, s

Components of Cochlear Implant

Implant ComponentsImplant Components
MicrophoneMicrophone amplificationamplification
External speech External speech processorprocessor
CompressionCompression FilteringFiltering ShapingShaping
Transmitter (outer coil)Transmitter (outer coil)
ReceiverReceiver
Electrode arrayElectrode array
Neural pathwaysNeural pathways

Types of Cochlear ImplantsTypes of Cochlear Implants
Single vs. Multiple channelsSingle vs. Multiple channels Audio example of how a cochlear implant sounds with Audio example of how a cochlear implant sounds with
varying number of channelsvarying number of channels
Monopolar vs. BipolarMonopolar vs. Bipolar
Speech processing strategiesSpeech processing strategies Spectral peak (Nucleus)Spectral peak (Nucleus) Continuous interleaved sampling (Med-El, Nucleus, Continuous interleaved sampling (Med-El, Nucleus,
Clarion)Clarion) Advanced combined encoder (Nucleus)Advanced combined encoder (Nucleus) Simultaneous analog strategy (Clarion)Simultaneous analog strategy (Clarion)
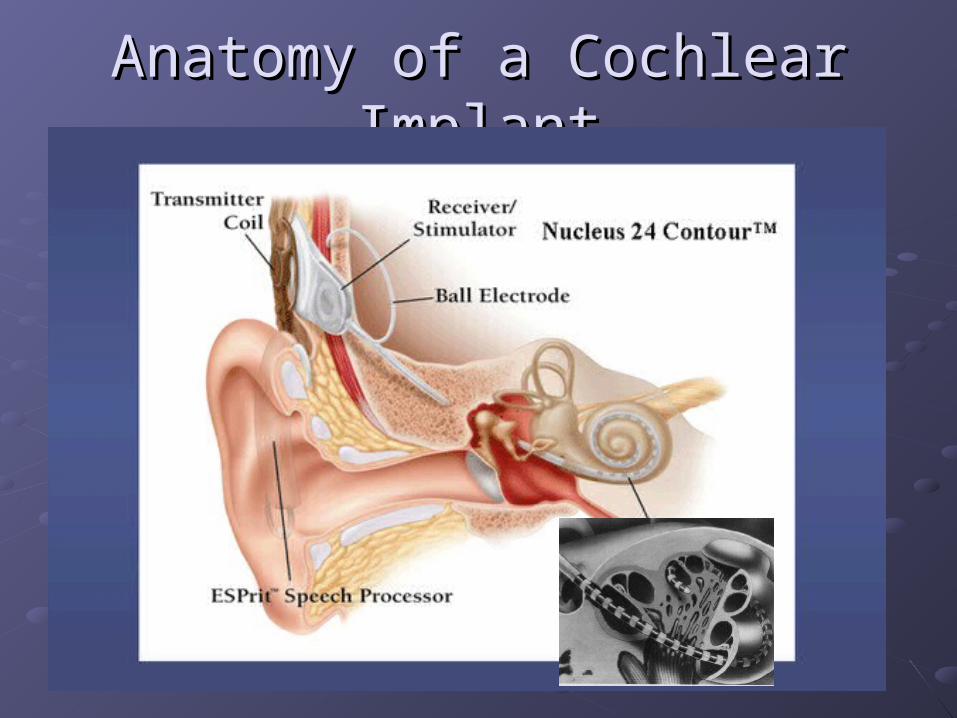
Anatomy of a Cochlear ImplantAnatomy of a Cochlear Implant

Indication for Cochlear ImplantIndication for Cochlear Implant
AdultsAdults 18 years old and older (no limitation by age)18 years old and older (no limitation by age) Bilateral severe-to-profound sensorineural Bilateral severe-to-profound sensorineural
hearing loss (70 dB hearing loss or greater hearing loss (70 dB hearing loss or greater with with littlelittle or no benefit from hearing aids for 6 or no benefit from hearing aids for 6 months)months)
Psychologically suitablePsychologically suitable No anatomic contraindicationsNo anatomic contraindications Medically not contraindicatedMedically not contraindicated

Indications for Cochlear Indications for Cochlear Implantation -- ChildrenImplantation -- Children
12 months or older12 months or older
Bilateral severe-to-profound sensorineural hearing loss Bilateral severe-to-profound sensorineural hearing loss with PTA of 90 dB or greater in better earwith PTA of 90 dB or greater in better ear
No appreciable benefit with hearing aids (parent survey No appreciable benefit with hearing aids (parent survey when <5 yo or 30% or less on sentence recognition when <5 yo or 30% or less on sentence recognition when >5 yo)when >5 yo)
Must be able to tolerate wearing hearing aids and show Must be able to tolerate wearing hearing aids and show some aided abilitysome aided ability
Enrolled in aural/oral education programEnrolled in aural/oral education program
No medical or anatomic contraindicationsNo medical or anatomic contraindications
Motivated parentsMotivated parents
ContraindicationsContraindications
Incomplete hearing lossIncomplete hearing lossNeurofibromatosis II, mental retardation, psychosis, Neurofibromatosis II, mental retardation, psychosis, organic brain dysfunction, unrealistic expectationsorganic brain dysfunction, unrealistic expectationsActive middle ear diseaseActive middle ear diseaseCT findings of cochlear agenesis (Michel deformity) or CT findings of cochlear agenesis (Michel deformity) or small IAC (CN8 atresia)small IAC (CN8 atresia)Dysplasia not necessarily a contraindication, but Dysplasia not necessarily a contraindication, but informed consent is a mustinformed consent is a mustH/O CWD mastoidectomyH/O CWD mastoidectomyLabyrinthitis ossificans—follow scansLabyrinthitis ossificans—follow scansAdvanced otosclerosisAdvanced otosclerosis

CT FindingsCT Findings
General WorkupGeneral Workup
Audiologic exam with binaural Audiologic exam with binaural amplificationamplification
CT scan/MRI of temporal bonesCT scan/MRI of temporal bones
Trial of high-powered hearing aidsTrial of high-powered hearing aids
Psychological evaluationPsychological evaluation
Medical evaluationMedical evaluation
Any necessary tests to discover etiology of Any necessary tests to discover etiology of hearing losshearing loss

Surgical techniqueSurgical technique
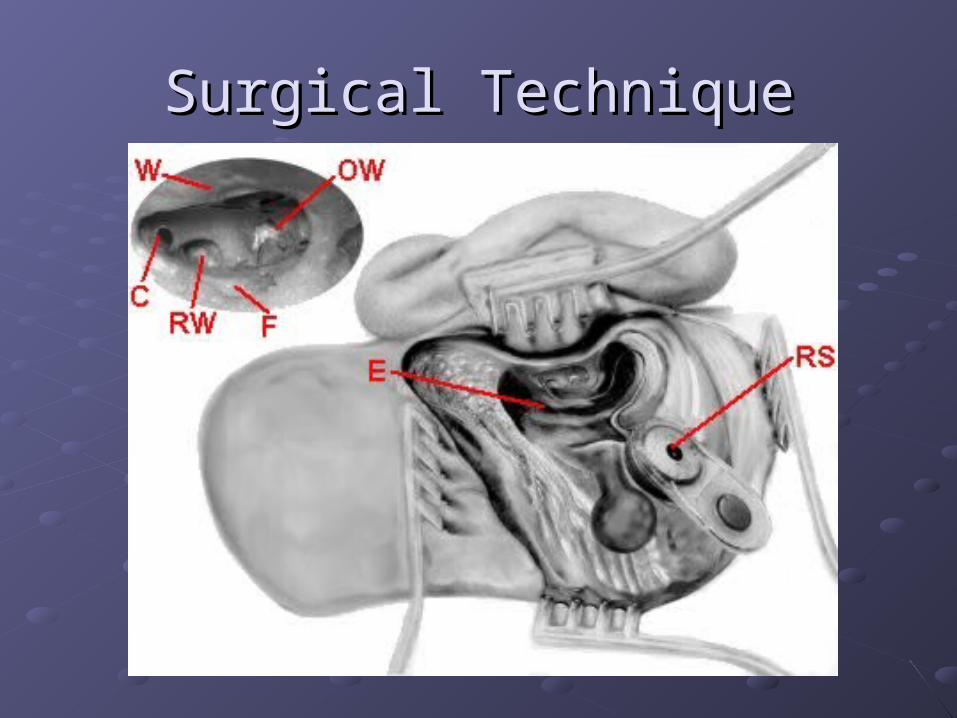
Surgical TechniqueSurgical Technique

Surgical TechniqueSurgical Technique

Postoperative ManagementPostoperative Management
Complication rate only 5%Complication rate only 5%Wound infection/breakdownWound infection/breakdown Yu, et al showed good response to Abx, I&DYu, et al showed good response to Abx, I&D
Facial nerve injury/stimulation, CSF leak, Facial nerve injury/stimulation, CSF leak, MeningitisMeningitis CDC recommendationsCDC recommendations
Vertigo (Steenerson reported 75%)Vertigo (Steenerson reported 75%)Device failure—re-implantation usually Device failure—re-implantation usually successfulsuccessfulAvoid MRIAvoid MRI

Postoperative RehabilitationPostoperative Rehabilitation
Necessary part of implantationNecessary part of implantationDifferent focus depends on patient’s Different focus depends on patient’s previous experience with soundprevious experience with soundGoal is to enable children to be able to Goal is to enable children to be able to learn passively from the environmentlearn passively from the environmentProgram addresses receptive as well as Program addresses receptive as well as expressive language skillsexpressive language skillsMultidisciplinary, dedicated group Multidisciplinary, dedicated group necessarynecessary
Results of ImplantationResults of Implantation
Wide range of outcomesWide range of outcomesImprovement is long-term (Waltzman, et al. 5-15 yr f/u)Improvement is long-term (Waltzman, et al. 5-15 yr f/u)Implantation is cost effective—even in the elderly Implantation is cost effective—even in the elderly (Francis, et al)(Francis, et al)Research indicates recipe for success includes:Research indicates recipe for success includes:
Short length of time from deafness to implantationShort length of time from deafness to implantation (Sharma (Sharma showed <3.5 years regain normal latencies within 6 mos. After 7 showed <3.5 years regain normal latencies within 6 mos. After 7 years, little plasticity remains)years, little plasticity remains)
Experience with language before onset of deafnessExperience with language before onset of deafness Implantation before age sixImplantation before age six for prelingually deafened children for prelingually deafened children
(Govaerts, et al showed 90% of children implanted <2yo were (Govaerts, et al showed 90% of children implanted <2yo were integrated into mainstream vs. only 20-30% if implanted after integrated into mainstream vs. only 20-30% if implanted after age 4)age 4)
Aural/oral educationAural/oral education Highly motivated patients/parentsHighly motivated patients/parents

A Look to the FutureA Look to the Future
Partial implants with hearing aidPartial implants with hearing aid Those with residual low-frequency hearingThose with residual low-frequency hearing
Intraoperative mappingIntraoperative mapping
Bilateral implantation Bilateral implantation One vs. two speech processorsOne vs. two speech processors
Implantation for asymmetric SNHLImplantation for asymmetric SNHL
““Softip” array Softip” array
Minimally invasive implantationMinimally invasive implantation

Related Documents











