Comorbidities in acute heart failure- pulmonary disease Frans H. Rutten, MD, PhD, general practitioner Frans H. Rutten, MD, PhD, general practitioner Julius Center, University Medical Center Utrecht, Netherlands

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Comorbidities in acute heart failure- pulmonary disease
Frans H. Rutten, MD, PhD, general practitionerFrans H. Rutten, MD, PhD, general practitioner
Julius Center, University Medical Center Utrecht, Netherlands
No conflict of interest on this topic
40% ‘COPD’ aged 65 yrs or over: NO COPD1
78% ‘COPD’ hospitalized acute systolic HF: NO COPD 2
20.5% ‘COPD’: unrecognized HF 120.5% real COPD: unrecognized HF 1
1. Rutten FH et al. EHJ 2005;26:1887-942. Brenner S et al. Int J Card 2013;168:1910-6.
Doubt diagnosis of COPD!!
cardiologists afraid to overdiagnose HF..pulmonologist/GPs are not afraid to overdiagnose COPD..
Background heart and lungs ‘tandem’ in providing oxygen saturated blood
both share tobacco smoking as important risk factor: - lung destruction (Western world >90% COPD by smoking) - endothelial dysfunction atherosclerosis and IHD - first/second/third hand smoke plaque rupture/erosion
risk of acute MI , also in non-smokers
- cause of death in COPD patients often cardiovascular
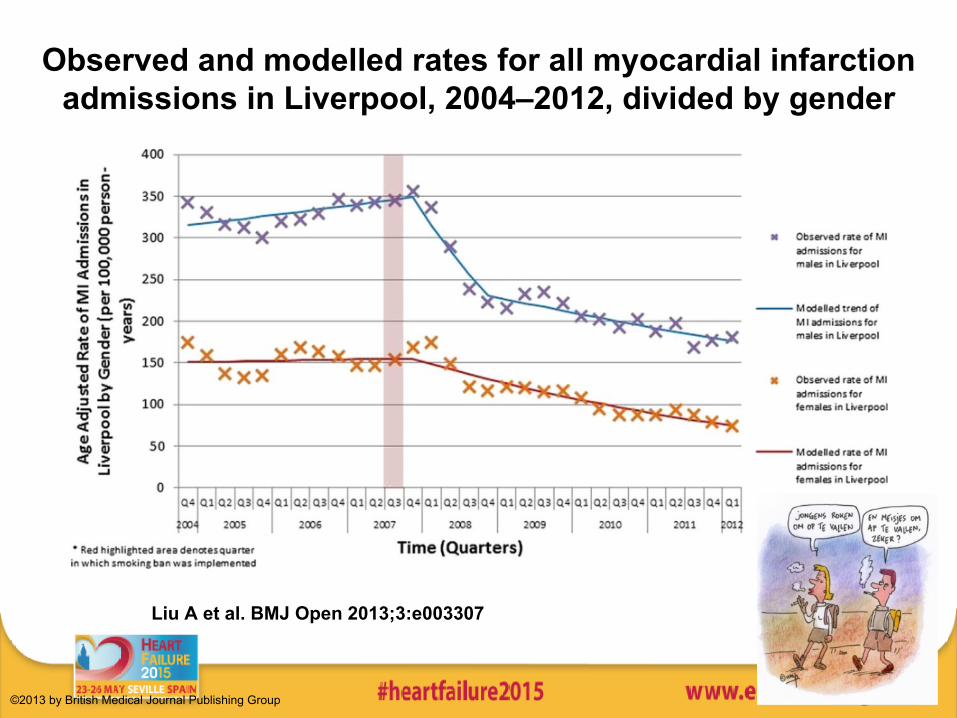
Observed and modelled rates for all myocardial infarction admissions in Liverpool, 2004–2012, divided by gender
Liu A et al. BMJ Open 2013;3:e003307
©2013 by British Medical Journal Publishing Group
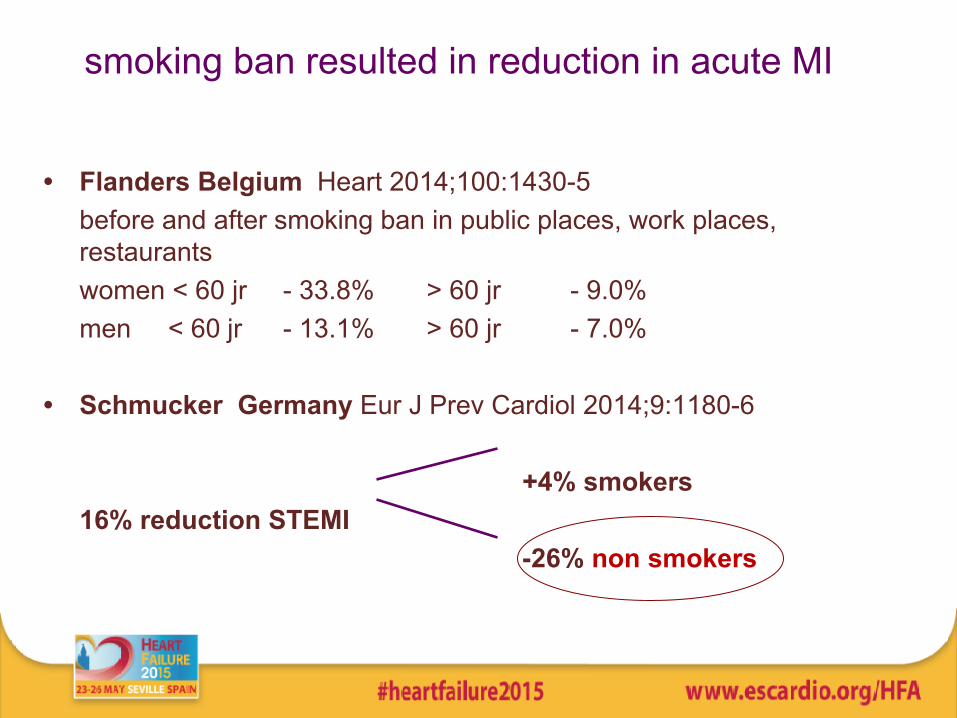
smoking ban resulted in reduction in acute MI
• Flanders Belgium Heart 2014;100:1430-5before and after smoking ban in public places, work places, restaurantswomen < 60 jr - 33.8% > 60 jr - 9.0%men < 60 jr - 13.1% > 60 jr - 7.0%
• Schmucker Germany Eur J Prev Cardiol 2014;9:1180-6
+4% smokers16% reduction STEMI
-26% non smokers
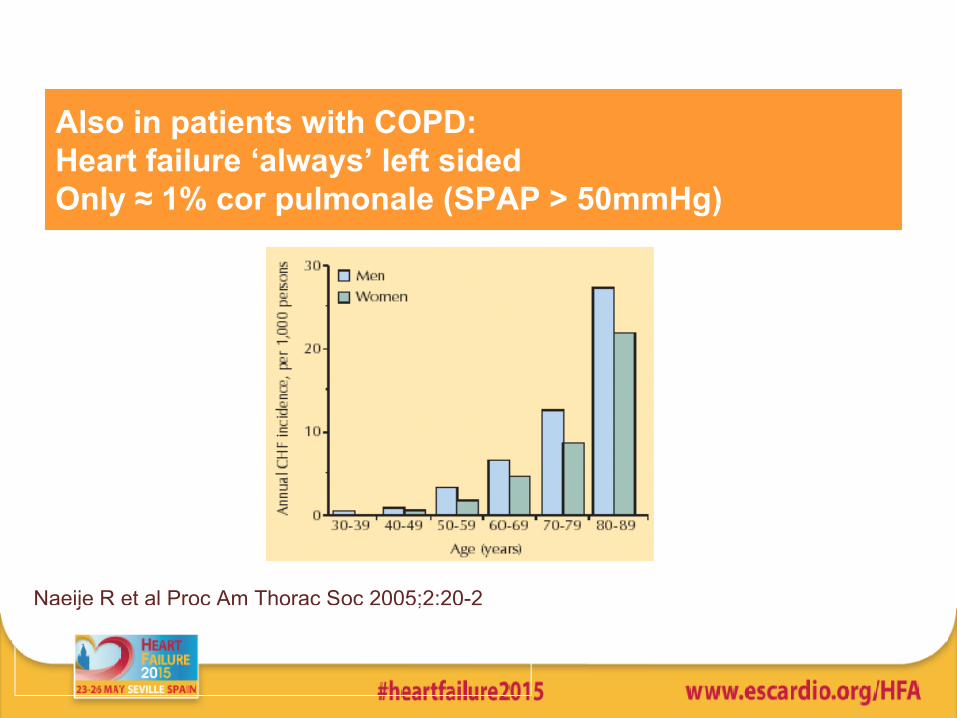
Also in patients with COPD: Heart failure ‘always’ left sidedOnly ≈ 1% cor pulmonale (SPAP > 50mmHg)
Naeije R et al Proc Am Thorac Soc 2005;2:20-2
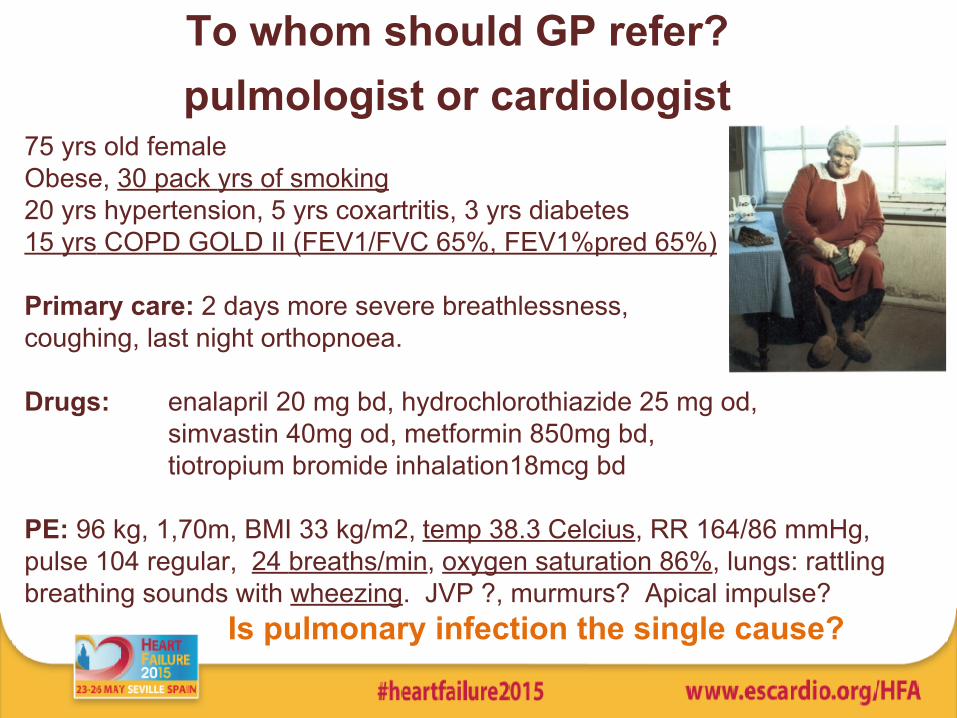
To whom should GP refer? pulmologist or cardiologist
75 yrs old femaleObese, 30 pack yrs of smoking20 yrs hypertension, 5 yrs coxartritis, 3 yrs diabetes 15 yrs COPD GOLD II (FEV1/FVC 65%, FEV1%pred 65%) Primary care: 2 days more severe breathlessness, coughing, last night orthopnoea.
Drugs: enalapril 20 mg bd, hydrochlorothiazide 25 mg od, simvastin 40mg od, metformin 850mg bd,
tiotropium bromide inhalation18mcg bd
PE: 96 kg, 1,70m, BMI 33 kg/m2, temp 38.3 Celcius, RR 164/86 mmHg, pulse 104 regular, 24 breaths/min, oxygen saturation 86%, lungs: rattling breathing sounds with wheezing. JVP ?, murmurs? Apical impulse?
Is pulmonary infection the single cause?
respiratory symptoms ≠ pulmonary disease Does wheezing fit with asthma or COPD?
35% of elderly with AHF wheeze at initial presentation
Risk of overdiagnosing COPD
Jorge S et al. BMC Cardiovasc Disord 2007;7:16
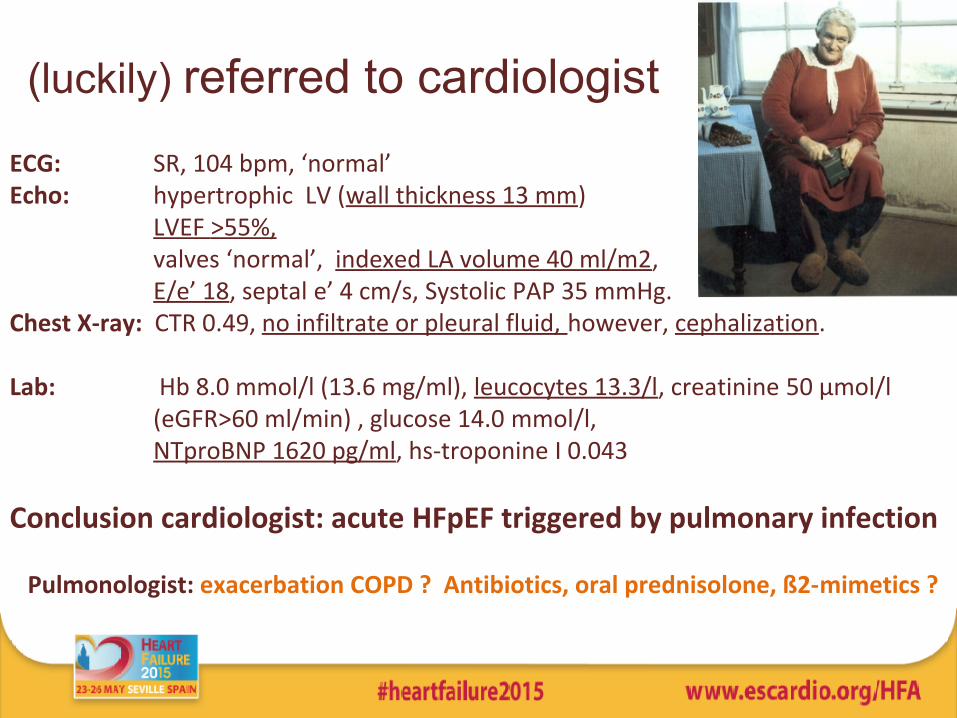
(luckily) referred to cardiologistECG: SR, 104 bpm, ‘normal’ Echo: hypertrophic LV (wall thickness 13 mm)
LVEF >55%, valves ‘normal’, indexed LA volume 40 ml/m2, E/e’ 18, septal e’ 4 cm/s, Systolic PAP 35 mmHg. Chest X-ray: CTR 0.49, no infiltrate or pleural fluid, however, cephalization.
Lab: Hb 8.0 mmol/l (13.6 mg/ml), leucocytes 13.3/l, creatinine 50 μmol/l (eGFR>60 ml/min) , glucose 14.0 mmol/l,
NTproBNP 1620 pg/ml, hs-troponine I 0.043
Conclusion cardiologist: acute HFpEF triggered by pulmonary infection
Pulmonologist: exacerbation COPD ? Antibiotics, oral prednisolone, ß2-mimetics ?
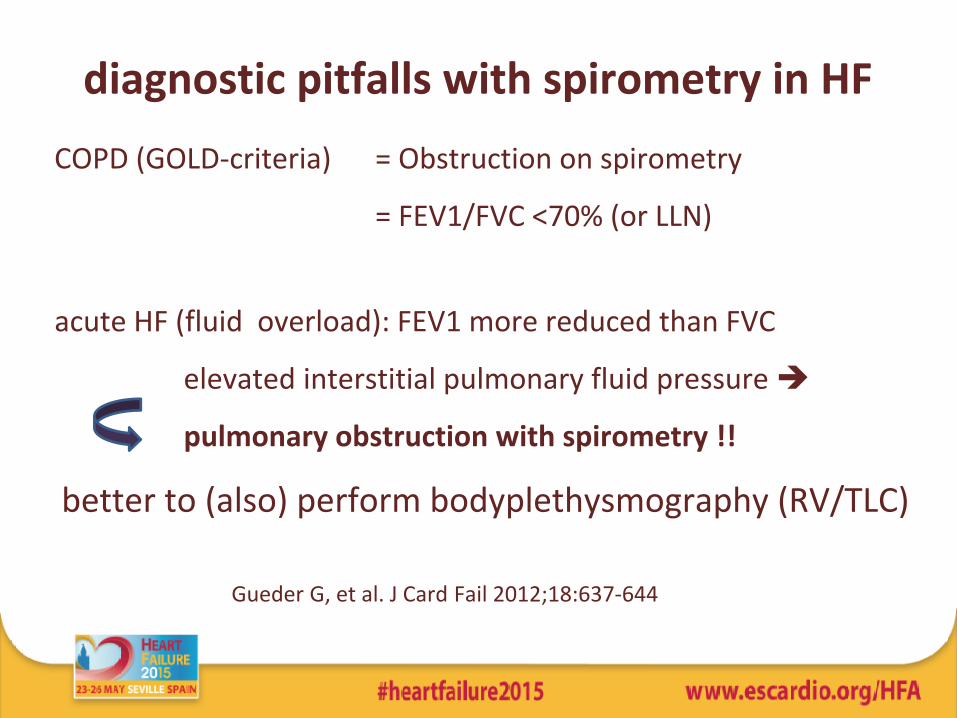
diagnostic pitfalls with spirometry in HF COPD (GOLD-criteria) = Obstruction on spirometry
= FEV1/FVC <70% (or LLN)
acute HF (fluid overload): FEV1 more reduced than FVC
elevated interstitial pulmonary fluid pressure
pulmonary obstruction with spirometry !!
better to (also) perform bodyplethysmography (RV/TLC)
Gueder G, et al. J Card Fail 2012;18:637-644
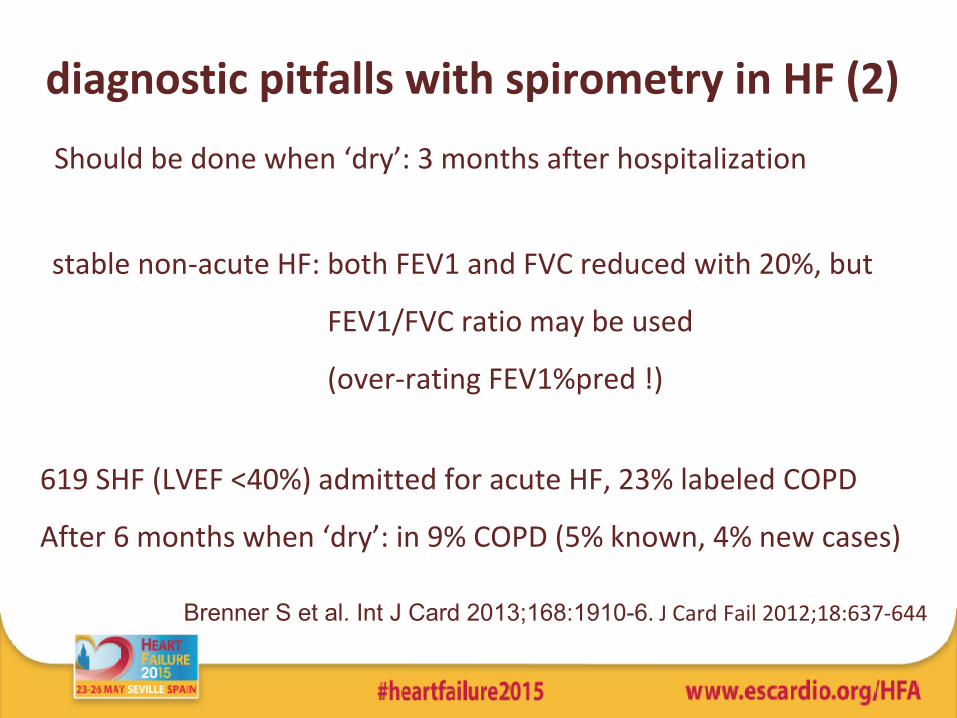
diagnostic pitfalls with spirometry in HF (2) Should be done when ‘dry’: 3 months after hospitalization
stable non-acute HF: both FEV1 and FVC reduced with 20%, but
FEV1/FVC ratio may be used
(over-rating FEV1%pred !)
619 SHF (LVEF <40%) admitted for acute HF, 23% labeled COPD
After 6 months when ‘dry’: in 9% COPD (5% known, 4% new cases)
Brenner S et al. Int J Card 2013;168:1910-6. J Card Fail 2012;18:637-644

Therapeutic challenges in our case
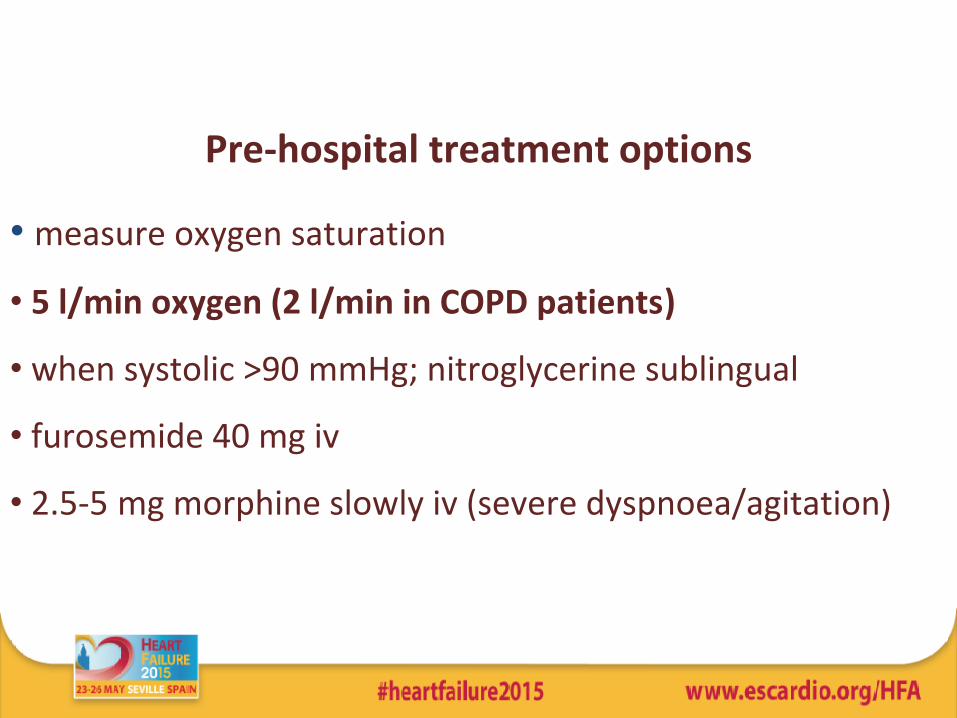
Pre-hospital treatment options
• measure oxygen saturation
• 5 l/min oxygen (2 l/min in COPD patients)
• when systolic >90 mmHg; nitroglycerine sublingual
• furosemide 40 mg iv
• 2.5-5 mg morphine slowly iv (severe dyspnoea/agitation)
Other options for our case?
–
Any other options in our case? - antibiotics for pulmonary infection
- Short acting beta2 mimetic inhalation for the first minutes???
• …on the short run…it may reduce pulmonary congestion by increasing transepithelial sodium and chloride transport (shown in animal models)!
• …on the short run.. in small sized studies increased FEV1, improved peripheral oxygen delivery, increased cardiac index, and decreased systemic vascular resistance
• On the other hand: positive chronotropic effects; increased heart rates and decreased potassium levels; facilitating hypo-potassemia -induced arrhythmias and tachycardias.
Maak CA, et al. J Emerg Med 2013;40:135-145, Mutlu GM. Crit Care Med 2004;32:1607-1608,Singer AJ et al ADHERE-EM Ann Emerg Med 2008
When stable again; beta-blockers allowed?
practice study UK: >80% of HFrEF patients with COPD managed in HF outpatient clinic tolerated beta-blockers Shelton RJ, et al. Heart 2006;92:331-36.
But,
Beta-blockers might slightly reduce FEV1
- clinically irrelevan, but ….
another risk of overdiagnosing COPDGueder G et al EJHF 2014
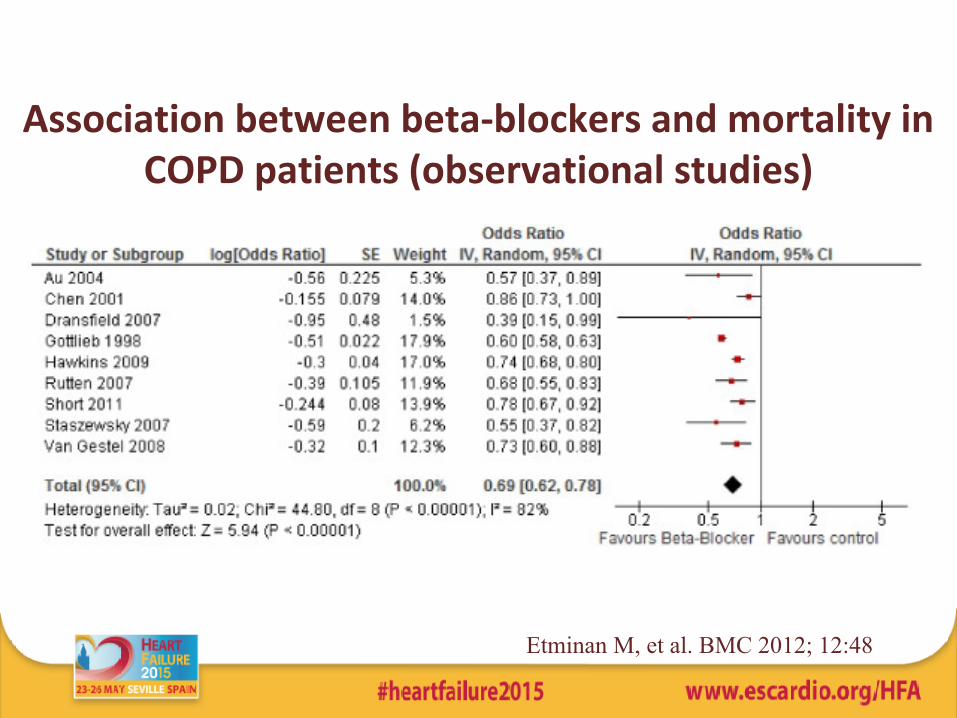
Association between beta-blockers and mortality in COPD patients (observational studies)
Etminan M, et al. BMC 2012; 12:48
Other cardiovascular drugs in COPD
Same story as for beta-blockers.
Also statins and ACEi and ARBs may reduce all-cause mortality
But, observational studies !!
Risk of (residual) confounding
1. Mancini GBJ et al. JACC 2006;47:2554-60 (ACE-i/ARBs, statins)
2. Soyeth V et al. Eur Resp J 2007;29:279-83 (statins)
Conclusions
• a label of COPD ≠ true COPD
• HF treatment on the first place before inhalers
• spirometry should be done when stable/euvolemic
• shortacting beta2-mimetics in acute HF (those wheezing)??
• near future; RCTs with CV drugs in COPD??
• when stabilised: not withhold HF patients from beta-blockers

Thank you for your attention
Related Documents