Closed-Heart Technique for Wolff-Parkinson-White Syndrome: Further Experience and Potential Limitations Gerard M. Guiraudon, M.D., F.R.C.S.(C), George J. Klein, M.D., F.R.C.P.(C), Arjun D. Sharma, M.D., F.R.C.P.(C), Simon Milstein, M.D., and Douglas G. McLellan, B.Sc., M.A. ABSTRACT We have described a closed-heart technique for division of atrioventricular (AV) pathways in Wolff- Parkinson-White (WPW) syndrome. The technique in- volves dissection and mobilization of the AV fat pad with exposure and cryoablation of the AV junction at the site of the AV pathways. One hundred five consecutive patients with WPW syn- drome with left ventricular free wall (741, posterior septal (231, and right ventricular free wall AV pathways (11) were operated on between July, 1982, and September, 1985. Three patients had multiple accessory pathways, and 9 had associated cardiac disease. Electrophysiological testing to determine the presence and site of the AV pathway was performed before and after dissection of the fat pad and again after cryoablation of the AV junction. All AV pathways but 1 were successfully ablated. There were no deaths and no incident of AV block. One hundred four patients remain free from arrhythmia in the absence of drugs after a mean follow-up of 18 months (range, 2 to 42 months). Four patients required a second operation within the first few weeks for recurrence of AV pathway conduction, and 1 patient required a third operation. In 3 of these patients, AV pathway conduction persisted after extensive dissection and exposure of the AV junction and disappeared only after cryoablation. Recurrence of AV pathway conduction in the latter patients suggests the presence of a subendocardial pathway protected from cryo- ablation by the warm, circulating blood pool. The closed-heart technique appears safe and efficacious. A potential limitation may be the presence of subendocar- dial AV pathways, which may require an alternative surgi- cal approach at the site of the pathway to attain uniform primary success. A successful surgical approach to Wolff-Parkinson- White (WPW) syndrome was achieved by Sealy and col- leagues [l, 21 in 1968. Since then, the operation has been perfected using an endocardial approach necessitating cold cardioplegic arrest [3]. The endocardial approach From the Departments of Surgery and Medicine, University of Western Ontario, University Hospital, London, Ont, Canada. Presented at the Twenty-second Annual Meeting of The Society of Tho- racic Surgeons, Washington, DC, Jan 27-29, 1986. Address reprint requests to Dr. Guiraudon, University Hospital, PO Box 5339, Terminal "A," London, Ont, Canada N6A 5A5. currently yields excellent results, although surgical risk in terms of mortality has not significantly improved [3]. It is probable that some of the deaths associated with this approach are related to cardioplegic arrest [4, 51. Consequently, we developed an epicardial approach for ablation of atrioventricular (AV) accessory pathways that does not require cold cardioplegic arrest and can be carried out on the beating heart with or without the cover of normothermic cardiopulmonary bypass [6]. The rationale for the epicardial approach is based on pathological evidence that the vast majority of accessory pathways course within the AV groove (epicardialacces- sory pathway) [7] and that a minority course across the AV junction within the subendocardium (subendocar- dial accessory pathway) [8, 91. The epicardial approach involves two steps: (1) dissection and mobilization of the AV fat pad and exposure of the AV junction and (2) cryoablation of the AV junction (Fig 1). This approach was used first for left ventricular free wall and right ven- tricular free wall accessory pathways and subsequently for posterior septal accessory pathways. Anterior septal accessory pathways are generally para-Hisian and necessitate an elective open-heart approach to the sep- tum [lo]. We report here our experience with 105 consecutive patients with WPW syndrome operated on using the epicardial approach between July, 1982, and September, 1985. Material and Methods There were 70 men (67%) and 35 women (33%). The ages ranged from 6 to 66 years with a mean of 32.8 years. A total of 108 accessory pathways were identified. Three patients had multiple accessory pathways. The accessory pathways were classified according to the lo- cation of their ventricular insertion: left ventricular free wall, 74; posterior septal (posterosuperior process of the left ventricle), 23, and right ventricular free wall, 11. Eighty-four patients were seen with "manifest" and 21 with "concealed' WPW syndrome associated with accessory pathways that conducted only retrograde. All patients complained of recurrent cardiac palpitation. Twenty-seven patients had at least one episode of syn- cope, and 16 patients had undergone cardioversion at least once. One patient had incessant reciprocating tachycardia complicated by cardiomyopathy. Nine patients had associated disease: aortic insuffi- ciency associated with a bicuspid aortic valve (l), atrial septal defect (l), forme fruste of Ebstein's anomaly (2), 651 Ann Thorac Surg 42651-657, Dec 1986

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Closed-Heart Technique for Wolff-Parkinson-White Syndrome: Further Experience and Potential Limitations Gerard M. Guiraudon, M.D., F.R.C.S.(C), George J. Klein, M.D., F.R.C.P.(C), Arjun D. Sharma, M.D., F.R.C.P.(C), Simon Milstein, M.D., and Douglas G. McLellan, B.Sc., M.A.
ABSTRACT We have described a closed-heart technique for division of atrioventricular (AV) pathways in Wolff- Parkinson-White (WPW) syndrome. The technique in- volves dissection and mobilization of the AV fat pad with exposure and cryoablation of the AV junction at the site of the AV pathways.
One hundred five consecutive patients with WPW syn- drome with left ventricular free wall (741, posterior septal (231, and right ventricular free wall AV pathways (11) were operated on between July, 1982, and September, 1985. Three patients had multiple accessory pathways, and 9 had associated cardiac disease. Electrophysiological testing to determine the presence and site of the AV pathway was performed before and after dissection of the fat pad and again after cryoablation of the AV junction.
All AV pathways but 1 were successfully ablated. There were no deaths and no incident of AV block. One hundred four patients remain free from arrhythmia in the absence of drugs after a mean follow-up of 18 months (range, 2 to 42 months). Four patients required a second operation within the first few weeks for recurrence of AV pathway conduction, and 1 patient required a third operation. In 3 of these patients, AV pathway conduction persisted after extensive dissection and exposure of the AV junction and disappeared only after cryoablation. Recurrence of AV pathway conduction in the latter patients suggests the presence of a subendocardial pathway protected from cryo- ablation by the warm, circulating blood pool.
The closed-heart technique appears safe and efficacious. A potential limitation may be the presence of subendocar- dial AV pathways, which may require an alternative surgi- cal approach at the site of the pathway to attain uniform primary success.
A successful surgical approach to Wolff-Parkinson- White (WPW) syndrome was achieved by Sealy and col- leagues [l, 21 in 1968. Since then, the operation has been perfected using an endocardial approach necessitating cold cardioplegic arrest [3]. The endocardial approach
From the Departments of Surgery and Medicine, University of Western Ontario, University Hospital, London, Ont, Canada.
Presented at the Twenty-second Annual Meeting of The Society of Tho- racic Surgeons, Washington, DC, Jan 27-29, 1986.
Address reprint requests to Dr. Guiraudon, University Hospital, PO Box 5339, Terminal "A," London, Ont, Canada N6A 5A5.
currently yields excellent results, although surgical risk in terms of mortality has not significantly improved [3]. It is probable that some of the deaths associated with this approach are related to cardioplegic arrest [4, 51. Consequently, we developed an epicardial approach for ablation of atrioventricular (AV) accessory pathways that does not require cold cardioplegic arrest and can be carried out on the beating heart with or without the cover of normothermic cardiopulmonary bypass [6].
The rationale for the epicardial approach is based on pathological evidence that the vast majority of accessory pathways course within the AV groove (epicardial acces- sory pathway) [7] and that a minority course across the AV junction within the subendocardium (subendocar- dial accessory pathway) [8, 91. The epicardial approach involves two steps: (1) dissection and mobilization of the AV fat pad and exposure of the AV junction and (2) cryoablation of the AV junction (Fig 1). This approach was used first for left ventricular free wall and right ven- tricular free wall accessory pathways and subsequently for posterior septal accessory pathways. Anterior septal accessory pathways are generally para-Hisian and necessitate an elective open-heart approach to the sep- tum [lo].
We report here our experience with 105 consecutive patients with WPW syndrome operated on using the epicardial approach between July, 1982, and September, 1985.
Material and Methods There were 70 men (67%) and 35 women (33%). The ages ranged from 6 to 66 years with a mean of 32.8 years.
A total of 108 accessory pathways were identified. Three patients had multiple accessory pathways. The accessory pathways were classified according to the lo- cation of their ventricular insertion: left ventricular free wall, 74; posterior septal (posterosuperior process of the left ventricle), 23, and right ventricular free wall, 11.
Eighty-four patients were seen with "manifest" and 21 with "concealed' WPW syndrome associated with accessory pathways that conducted only retrograde. All patients complained of recurrent cardiac palpitation. Twenty-seven patients had at least one episode of syn- cope, and 16 patients had undergone cardioversion at least once. One patient had incessant reciprocating tachycardia complicated by cardiomyopathy.
Nine patients had associated disease: aortic insuffi- ciency associated with a bicuspid aortic valve (l), atrial septal defect (l), forme fruste of Ebstein's anomaly (2),
651 Ann Thorac Surg 42651-657, Dec 1986

652 The Annals of Thoracic Surgery Vol 42 No 6 December 1986
A
& . - B Fig I . Surgical rationale. (A) Cross section of the left coronary sul- cus. The small arrow indicates the subendocardial accessory pathway and the large arrow, the “epicardiul” accessory pathway coursing within the groove. ( B ) The operation in progress. The atrioventricular fat pad has been mobilized, and the mitral valve annulus has been exposed. The absence of the large arrow suggests that the epicardial accessory pathway is likely ablated. The endocardial accessory path- way is depicted within the cyoublative hemisphere of the cryoprobe (CRYO). (V = left ventricle; A = left atrium.)
coronary artery disease (2), cardiomyopathy (l), pericar- ditis (l), and mitral valve prolapse (1). Some of these associated abnormalities necessitated concomitant surgi- cal correction. Two patients had previously had an un- successful operation elsewhere for WPW syndrome by the endocardial approach.
Preoperative Evaluation All patients underwent preoperative electrophysiolog- ical study. Eight patients had associated AV node reen- trant tachycardia or AV node echo beats. One patient had primary atrial fibrillation with a rapid ventricular response without inducible reciprocating tachycardia. During reciprocating supraventricular tachycardia, the cycle length ranged from 225 to 460 msec with a mean of 333.0 2 58.4 msec (k standard deviation).
Atrial fibrillation was induced in all patients. In pa- tients with manifest WPW syndrome, the shortest R-R interval during atrial fibrillation ranged from 140 to 400 msec with a mean of 241.0 2 68.6 msec.
All patients had a preoperative echocardiographic ex- amination. Those with an associated cardiac structural abnormality underwent standard right and left ventricle catheterization, and all patients older than 40 years had left ventricle catheterization with coronary angiography.
Surgical M i c a t ions The surgical indications have evolved over time. The most frequent indication was reciprocating supraven- tricular tachycardia resistant to medical drug therapy, or potential life-threatening atrial fibrillation [ll]. More re- cently, operation was offered as an alternative to lifelong
medical therapy in young patients (less than 40 years old).
Surgical Exposure The heart was exposed through a median stemotomy in 104 patients. In 1 patient with a left ventricular free wall accessory pathway, the heart was exposed through a left lateral thoracotomy and the accessory pathway was ab- lated without cardiopulmonary bypass.
Normothermic cardiopulmonary bypass was not used in patients with right ventricular free wall accessory pathways except in 1 patient with a forme fruste of Eb- stein’s anomaly. Cardiopulmonary bypass was used in 15 patients with posterior septal accessory pathways and was not used in 8 of them. Cardiopulmonary bypass was used essentially for left posterior septal accessory path- ways and posterior septal accessory pathways associ- ated with a coronary sinus diverticulum, and for all left ventricular accessory pathways approached through a median sternotomy. Normothermic cardiopulmonary bypass was also used during intraoperative electrophys- iological studies before or after ablation of the accessory pathway. The mean normothermic cardiopulmonary by- pass time was 77 minutes.
lntraoperative Electrophysiological Study Intraoperative electrophysiological mapping was carried out using a handheld exploring electrode. Ventricular mapping during normal sinus rhythm or atrial pacing was confined to the base of the ventricles over seventeen predetermined sites (Fig 2). Retrograde atrial mapping during reciprocating tachycardia or ventricular pacing was confined to the juxtaannular atrial wall at the same seventeen sites. The delta wave was continuously moni-
Fig 2. Epicardial map showing an inferior view of the heart. The anterior wall of both the left (LV) and right ventricle (RV) has been mobilized around the obtuse and acute margin, respectively. The closed triangles represent the sites of left ventricular free wall acces- sory pathways and the closed squares, the sites of posterior septal accessory pathways. The open triangles represent the sites of right ventricular free wall accessory pathways. The closed circle represents the site ofpreexcitation of anterior septal accessory pathways. (CS = coronary sinus.)
653 Guiraudon, Klein, Sharma, et al: Closed-Heart Technique for WPW Syndrome
tored. Electrophysiological study was camed out after dissection of the AV fat pad was completed, as well as after cryoablation. The persistence of accessory pathway conduction after exposure of the AV junction was con- sidered evidence of a subendocardial location of the ac- cessory pathway.
Surgical Technique Pathological data and surgical experience have sug- gested that to attain consistent success at the first opera- tion, a complete, extensive dissection in depth and in width of all potential insertions of the accessory path- way onto either the ventricle or atrium must be achieved.
The accessory pathways were located in the region of the obtuse margin in all patients except 1. The entire left AV fat pad was dissected and mobilized from the left fibrous trigone to the posterior septa1 region.
The operation was carried out in the following manner (Fig 3).
(1) The dissection was started over the left atrial inferior wall posterior to the coronary sinus. The left atrial oblique vein was present and identified in all but 1 patient. Its division allowed the coronary sinus to be mobilized.
(2) Dissection of the anterior part of the fat pad in the region of the left appendage was started. The epicar- dium was carefully incised along its atrial insertion. The great cardiac vein could be seen coursing toward the ventricular wall. The circumflex coronary artery was sought in the event that it was intramural or entwined in a myocardial loop. If this was the case, the circumflex was unroofed and mobilized. Care
LEFT VENTRICULAR FREE WALL ACCESSORY PATHWAYS.
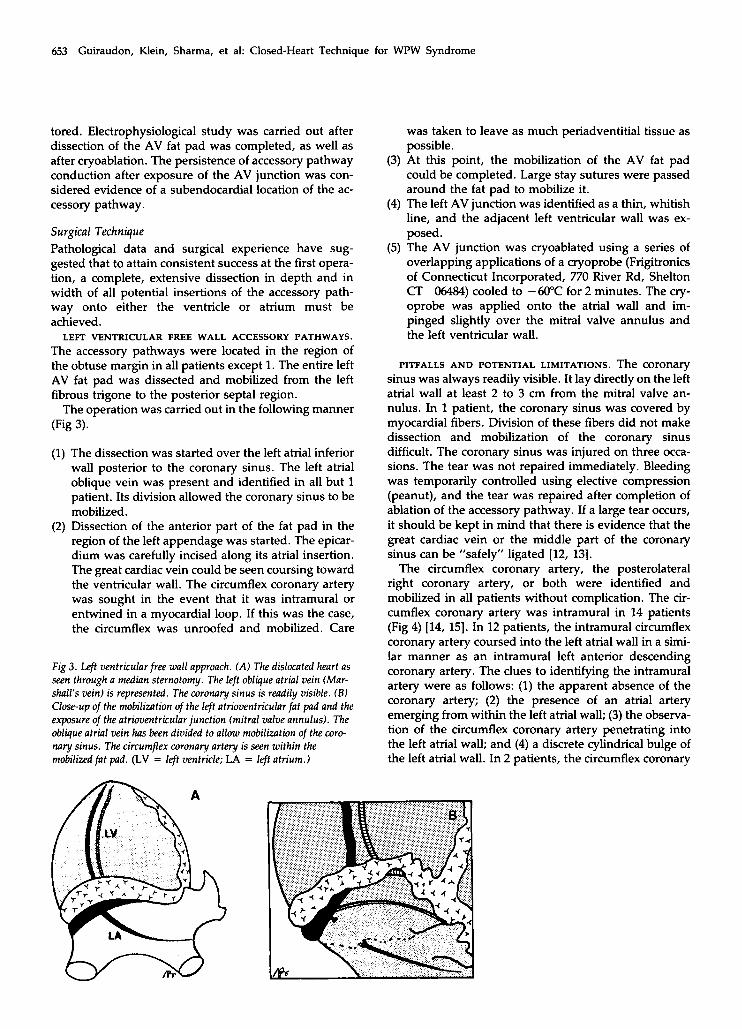
Fig 3 . Left ventricularfree wall approach. (A) The dislocated heart as seen through a mediun sternotomy. The left oblique atrial vein (Mar- shall's vein) is represented. The coronary sinus is readily visible. ( B ) Close-up of the mobilization of the left atrioventricular fat pad and the exposure of the atrioventricular junction (mitral valve annulus). The oblique atrial vein has been divided to allow mobilization of the coro- m r y sinus. The circumflex coronary artery is seen within the mobilizedfat pad. (LV = left ventricle; LA = left atrium.)
was taken to leave as much periadventitial tissue as possible.
(3) At this point, the mobilization of the AV fat pad could be completed. Large stay sutures were passed around the fat pad to mobilize it.
(4) The left AV junction was identified as a thin, whitish line, and the adjacent left ventricular wall was ex- posed.
(5) The AV junction was cryoablated using a series of overlapping applications of a cryoprobe (Frigitronics of Connecticut Incorporated, 770 River Rd, Shelton CT 06484) cooled to -60°C for 2 minutes. The cry- oprobe was applied onto the atrial wall and im- pinged slightly over the mitral valve annulus and the left ventricular wall.
PITFALLS AND POTENTIAL LIMITATIONS. The coronary sinus was always readily visible. It lay directly on the left atrial wall at least 2 to 3 cm from the mitral valve an- nulus. In 1 patient, the coronary sinus was covered by myocardial fibers. Division of these fibers did not make dissection and mobilization of the coronary sinus difficult. The coronary sinus was injured on three occa- sions. The tear was not repaired immediately. Bleeding was temporarily controlled using elective compression (peanut), and the tear was repaired after completion of ablation of the accessory pathway. If a large tear occurs, it should be kept in mind that there is evidence that the great cardiac vein or the middle part of the coronary sinus can be "safely" ligated [12, 131.
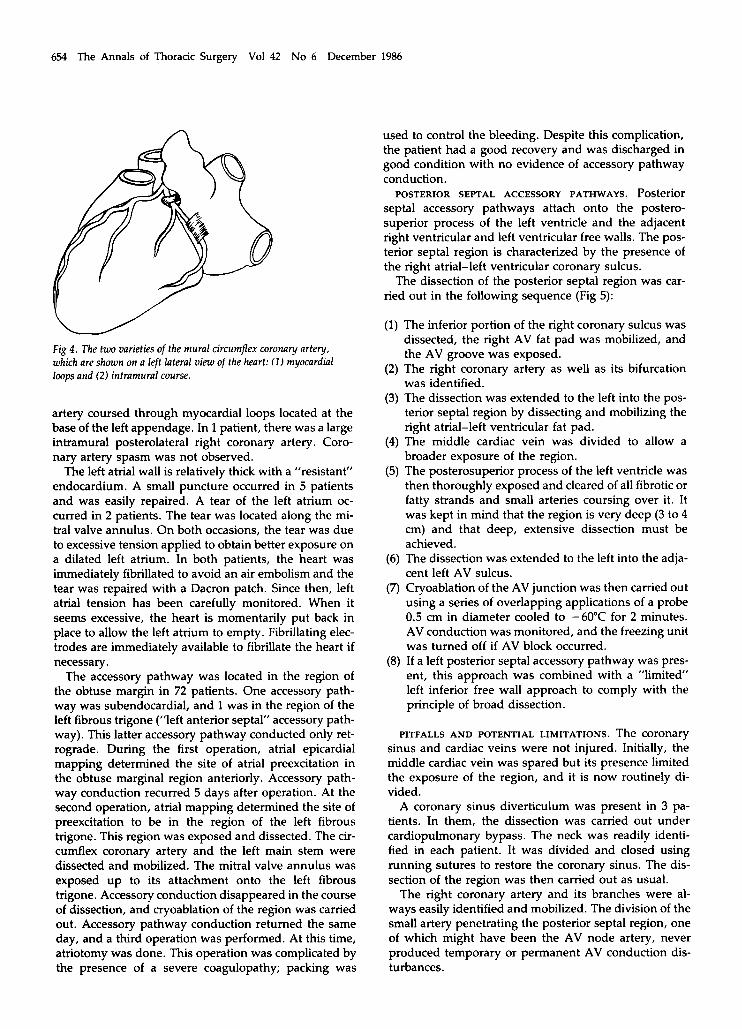
The circumflex coronary artery, the posterolateral right coronary artery, or both were identified and mobilized in all patients without complication. The cir- cumflex coronary artery was intramural in 14 patients (Fig 4) (14, 151. In 12 patients, the intramural circumflex coronary artery coursed into the left atrial wall in a simi- lar manner as an intramural left anterior descending coronary artery. The clues to identifying the intramural artery were as follows: (1) the apparent absence of the coronary artery; (2) the presence of an atrial artery emerging from within the left atrial wall; (3) the observa- tion of the circumflex coronary artery penetrating into the left atrial wall; and (4) a discrete cylindrical bulge of the left atrial wall. In 2 patients, the circumflex coronary
654 The Annals of Thoracic Surgery Vol 42 No 6 December 1986
W Fig 4 . The two varieties of the mural circumflex coronary artery, which are shown on a left lateral view of the heart: ( 1 ) myocardiul lwps and (2) intramural course.
artery coursed through myocardial loops located at the base of the left appendage. In 1 patient, there was a large intramural posterolateral right coronary artery. Coro- nary artery spasm was not observed.
The left atrial wall is relatively thick with a ”resistant” endocardium. A small puncture occurred in 5 patients and was easily repaired. A tear of the left atrium oc- curred in 2 patients. The tear was located along the mi- tral valve annulus. On both occasions, the tear was due to excessive tension applied to obtain better exposure on a dilated left atrium. In both patients, the heart was immediately fibrillated to avoid an air embolism and the tear was repaired with a Dacron patch. Since then, left atrial tension has been carefully monitored. When it seems excessive, the heart is momentarily put back in place to allow the left atrium to empty. Fibrillating elec- trodes are immediately available to fibrillate the heart if necessary.
The accessory pathway was located in the region of the obtuse margin in 72 patients. One accessory path- way was subendocardial, and 1 was in the region of the left fibrous trigone (”left anterior septal” accessory path- way). This latter accessory pathway conducted only ret- rograde. During the first operation, atrial epicardial mapping determined the site of atrial preexcitation in the obtuse marginal region anteriorly. Accessory path- way conduction recurred 5 days after operation. At the second operation, atrial mapping determined the site of preexcitation to be in the region of the left fibrous trigone. This region was exposed and dissected. The cir- cumflex coronary artery and the left main stem were dissected and mobilized. The mitral valve annulus was exposed up to its attachment onto the left fibrous trigone. Accessory conduction disappeared in the course of dissection, and cryoablation of the region was carried out. Accessory pathway conduction returned the same day, and a third operation was performed. At this time, atriotomy was done. This operation was complicated by the presence of a severe coagulopathy; packing was
used to control the bleeding. Despite this complication, the patient had a good recovery and was discharged in good condition with no evidence of accessory pathway conduction.
POSTERIOR SEPTAL ACCESSORY PATHWAYS. Posterior septal accessory pathways attach onto the postero- superior process of the left ventricle and the adjacent right ventricular and left ventricular free walls. The pos- terior septal region is characterized by the presence of the right atrial-left ventricular coronary sulcus.
The dissection of the posterior septal region was car- ried out in the following sequence (Fig 5):
(1) The inferior portion of the right coronary sulcus was dissected, the right AV fat pad was mobilized, and the AV groove was exposed.
(2) The right coronary artery as well as its bifurcation was identified.
(3) The dissection was extended to the left into the pos- terior septal region by dissecting and mobilizing the right atrial-left ventricular fat pad.
(4) The middle cardiac vein was divided to allow a broader exposure of the region.
(5) The posterosuperior process of the left ventricle was then thoroughly exposed and cleared of all fibrotic or fatty strands and small arteries coursing over it. It was kept in mind that the region is very deep (3 to 4 cm) and that deep, extensive dissection must be achieved.
(6) The dissection was extended to the left into the adja- cent left AV sulcus.
(7) Cryoablation of the AV junction was then carried out using a series of overlapping applications of a probe 0.5 cm in diameter cooled to -60°C for 2 minutes. AV conduction was monitored, and the freezing unit was turned off if AV block occurred.
(8) If a left posterior septal accessory pathway was pres- ent, this approach was combined with a “limited’ left inferior free wall approach to comply with the principle of broad dissection.
PITFALLS AND POTENTIAL LIMITATIONS. The coronary sinus and cardiac veins were not injured. Initially, the middle cardiac vein was spared but its presence limited the exposure of the region, and it is now routinely di- vided.
A coronary sinus diverticulum was present in 3 pa- tients. In them, the dissection was carried out under cardiopulmonary bypass. The neck was readily identi- fied in each patient. It was divided and closed using running sutures to restore the coronary sinus. The dis- section of the region was then carried out as usual.
The right coronary artery and its branches were al- ways easily identified and mobilized. The division of the small artery penetrating the posterior septal region, one of which might have been the AV node artery, never produced temporary or permanent AV conduction dis- turbances.

655 Guiraudon, Klein, Sharma, et al: Closed-Heart Technique for WPW Syndrome
Fig 5. Posterior septal approach. (A) Exposure of the posterior septal region through a median sternotomy. The inferior wall of the heart is exposed by deflecting the right ventricular inferior wall using a U- shaped stay suture pledgeted by a thick piece of cardboard. (B) Poste- rior septal region. The right atrial-left ventricular (RA-LV) sulcus has been exposed. The middle cardiac vein has been divided, and the right atrioventricular fat pad and the RA-LV fat pad have been mobilized. The right coronary artery is seen within the fat pad. (A0 = aorta; RV = right ventricle; RA = right atrium; PSP = pos- terosuperior process; LV = l q t ventricle; CS = corona y sinus; LA = left atrium; IVC = inferior vena cava.)
The accessory pathway was subendocardial in 1 pa- tient.
The dissection was not different in principle from the left ventricular free wall dissection. (1) The plane of dissec- tion was not as neat as on the left side because of the opening of the right ventricular veins into the right atrium. (2) Also, patches of the fat pad adhered tightly to the thin right atrial wall, and (3) the right ventricular wall frequently overlapped the tricuspid annulus and “adhered’ to the right atrial wall. These adhesions were freed to expose the tricuspid annulus.
PITFALLS AND POTENTIAL LIMITATIONS. No specific pit- falls were encountered. Three of these patients had sub- endocardial accessory pathways.
Results There were no deaths. No permanent or temporary AV block occurred, and no pacemakers were implanted. Four patients had two operations; 1 had three.
RIGHT VENTRICULAR FREE WALL ACCESSORY PATHWAYS.
Complications The patient with a left fibrous trigone accessory pathway had postoperative low cardiac output secondary to perioperative coagulopathy and packing. He left the hospital in good condition without further problems. Two patients were reoperated on for postoperative bleeding. One patient had postpericardiotomy syn- drome. Three weeks after operation, 1 patient had chy- lopericardium, which resolved after pericardial drain- age.
Efficacy A total of 106 of the 107 accessory pathways were ab- lated. Only 1 pathway was obtunded; the condition of the patient is well controlled with a regimen of pro- cainamide hydrochloride, which was previously ineffec- tive. There were no late recurrences after a mean follow- up of 18 months (range, 2 to 42 months).
Comment The Subendocardial Accessory Pathway Evidence strongly suggested that accessory pathways could course in an endocardial (91 or even intracavitary fashion [8], particularly in the right ventricular free wall region. Based on experimental studies using the dog [16], it was assumed that transmural cryonecrosis could be achieved on the normothermic beating heart. Conse- quently, it was hypothesized that the epicardial acces- sory pathway would be ablated by the dissection and exposure of the sulcus and that cryoablation would ab- late the subendocardial pathways. The presence of ac- cessory pathway conduction after exposure of the sulcus suggests an endocardial accessory pathway. The precise location of the endocardial accessory pathway was de- termined using ice mapping: interruption of accessory pathway conduction by applying a cryoprobe cooled to -5°C suggested that the accessory pathway was near the probe and in the ”kill” zone of the freeze when the probe was subsequently cooled to - 60°C.
Five patients had a “subendocardial” accessory path- way. Three pathways were right ventricular free wall, 1 was posterior septal, and 1 was left ventricular free wall. Ice mapping at - 5°C stopped pathway conduction in all instances, and cryoablation to -60°C was carried out. Successful interruption was achieved in 2 right ventricu- lar free wall accessory pathways, but accessory conduc- tion returned in the remaining 3 patients. Conduction returned the same day in the posterior septal pathway, and the accessory pathway was ablated at a second oper- ation using a septal right atriotomy. Conduction re- turned after two to three weeks in the left ventricular free wall accessory pathway, which was ablated at a sec- ond operation using an elective juxtaannular left at- riotomy under normothermic cardiopulmonary bypass on the fibrillating heart. The right ventricular free wall accessory pathway conduction recurred. The same tech- nique used at the first operation was used again because it was thought that the exposure of the tricuspid annulus
656 The Annals of Thoracic Surgery Vol 42 No 6 December 1986
could have been incomplete initially. The second opera- tion produced permanent modification of the accessory pathway.
Based on this experience, we suggest that the pres- ence of accessory pathway conduction after dissection necessitates an alternative surgical technique: an elective atriotomy for accessory pathways in the posterior septal region to avoid injury to the His bundle, a n d elective endocardial cryoablation for free wall accessory path- ways. The cryoprobe can be introduced through the left o r right appendage.
Mortality There were no deaths i n this series of 105 patients. Death d u e to postoperative low-output failure persists even in patients without associated structural disease [3] when the endocardial approach, which requires aortic cross-clamping and cold cardioplegic myocardial preser- vation, is used. More patients are needed, however, to verify that the epicardial approach carries a significantly lower surgical mortality.
Morbidity Except for the patient in w h o m three interventions were necessary a n d in w h o m a severe coagulopathy associ- ated with hemodynamic impairment requiring inotropic support developed, we observed no myocardial dys- function postoperatively and no patient required ino- tropic support. No patient had postoperative atrial fibrillation (171. These results suggest a trend toward a decrease in postoperative morbidity compared with the open-heart approach [3]. However, this remains to be confirmed by further experience.
Efficacy One hundred six accessory pathways were ablated, a n d 1 was obtunded. Five patients had more than one opera- tion. With the knowledge gained from this learning series, we may expect to attain uniform ablation of the accessory pathway during the first operation.
There are other potential advantages of the epicardial approach. Continuous monitoring of preexcitation dur- ing the dissection allows recognition of the moment of accessory pathway interruption a n d facilitates avoidance of inadvertent AV block with septal accessory pathways. The absence of cardioplegia allows immediate assess- ment of accessory pathway ablation a n d sequential map- ping for multiple accessory pathways. Ablation of acces- sory pathways in the closed heart without cardioplegic arrest allows the subsequent performance of concomi- tant procedures without adding to aortic cross-clamping and cardioplegic arrest times.
We conclude that the results of the epicardial ap- proach for ablation of the accessory pathway i n WPW syndrome demonstrate low morbidity and mortality without jeopardizing efficacy. These results justify the continued use and development of this epicardial ap- proach.
References 1. Sealy WC, Hattler BG Jr, Blumenschein SD, Cobb FR: Sur-
gical treatment of Wolff-Parkinson-White syndrome. Ann Thorac Surg 8:1, 1969
2. Sealy WC, Gallagher JJ, Wallace AG: The surgical treatment of Wolff-Parkinson-White syndrome: evolution of im-
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
proved methods for identification and interruption of the Kent bundle. Ann Thorac Surg 22443, 1976 Cox JL, Gallagher JJ, Cain ME: Experience with 118 con- secutive patients undergoing operation for the Wolff- Parkinson-White syndrome. J Thorac Cardiovasc Surg 90:490, 1985 Buckberg GD: A proposed "solution" to the cardioplegic controversy. J Thorac Cardiovasc Surg 77:803, 1979 Roberts AJ: Perioperative myocardial infarction and changes in left ventricular performance related to coronary artery bypass graft surgery (collective review). Ann Thorac Surg 35208, 1983 Guiraudon GM, Klein GJ, Gulamhusein S, et al: Surgical repair of Wolff-Parkinson-White syndrome: a new closed- heart technique. Ann Thorac Surg 37:67, 1984 Anderson RH, Becker AE: Stanley Kent and accessory atrio- ventricular connections. J Thorac Cardiovasc Surg 81649, 1981 Lev M, Sodi-Pallares D, Friedland C: A histopathologic study of the atrioventricular communications in a case of WPW with incomplete left bundle branch block. Am Heart J 66399,1963 Lev M, Kennamer R, Prinzmetal M, de Mesquita QH: A histopathologic study of the atrioventricular communica- tions in two hearts with the Wolff-Parkinson-White syn- drome. Circulation 24:41, 1961 Guiraudon GM, Klein GJ, Sharma AD, Jones DL: An- teroseptal AV pathways are true septal, para-hisian struc- tures: verification by ice mapping. Circulation 70:338, 1984 Gallagher JJ, Gilbert M, Svenson F W , et al: Wolff- Parkinson-White syndrome: the problem, evaluation, and surgical correction. Circulation 51:767, 1975 Parsonnet V: The anatomy of the veins of the human heart with special reference to normal anastomotic channels. J Med SOC NJ 50:446, 1953
13. Bates RJ, Toscano M, Balderman SC, Anagnostopoulos CE: The cardiac veins and retrograde coronary venous perfu- sion. Ann Thorac Surg 23:83, 1977
14. Polacek P, Kralove H: Relation of myocardial bridges and loops on the coronary arteries to coronary occlusions. Am Heart J 61:44, 1961
15. Geiringer E: The mural coronary. Am Heart J 41:359, 1951 16. Klein GJ, Guiraudon GM, Perkins DG, et al: Surgical correc-
tion of the Wolff-Parkinson-White syndrome in the closed heart using cryosurgery: a simplified approach. J Am Coll Cardiol 3:405, 1984
17. Tchervenkov CI, Wynands JE, Symes JF, et al: Persistent atrial activity during cardioplegic arrest: a possible factor in the etiology of postoperative supraventricular tachyar- rhythmias. Ann Thorac Surg 36:437, 1983
Discussion DR. WILL c. SEALY (Macon, GA): Dr. Guiraudon's results are excellent, although I disagree with the methods used to achieve them. For posterior septal pathways, I open the right atrium, enter the pyramidal space, and then open the epicardium over the crux. Pathways can course from the right atrium to the

657 Guiraudon, Klein, Sharma, et al: Closed-Heart Technique for WPW Syndrome
muscular ventricular septum. Dr. Guiraudon's one initial fail- ure is evidence of this.
His finding that 3 of 23 patients had aneurysms of the coro- nary sinus that were the atrial connections of a Kent bundle is of great clinical importance. Jay Selle and I have found this once.
I disagree with his approach to left free wall pathways. I gave it up for the less difficult endocardial approach, as did Dr. Iwa in Japan. The approach used by Dr. Guiraudon and his group required a bypass time of 77 minutes, the same as for an at- riotomy. Recently I have participated in more than 100 success- ful open-chest operations involving the left free wall. Most of the operations were done with Jay Selle in Charlotte, NC.
Pathways adjacent to the left fibrous trigone can be divided only by the endocardial approach. Here cryothermia could damage the left main coronary artery and also might alter a large segment of the aortic annulus.
Dr. Guiraudon believes that some left free wall pathways take an endocardial course. I do not agree. The two references he gives are descriptions of right free wall pathways.
I have two questions. Are all patients connected to the heart- lung machine? Would the destruction by cryothermia of a large segment of the mitral annulus result later in malfunction of the mitral valve?
Again, I compliment Dr. Guiraudon on his excellent results. In Paris, he taught both surgery and anatomy. His technical skills and anatomical knowledge make it possible for him to successfully perform these very complicated procedures.
DR. JOHN w. BROWN (Indianapolis, IN): I congratulate Dr. Guiraudon on this very clear presentation and his superb re- sults with this technique. I defend his technique. My colleagues and I thank him for sharing its salient features with us when we visited him in London, Ont, and watched him perform his pro- cedure.
We adopted his technique and began our series in May, 1985. To date, we have operated on 13 patients with WPW syndrome. Their ages ranged from 16 to 67 years. We used the Guiraudon technique, supplementing the AV fat pad dissection with cryo- ablation. The location of the accessory pathways was left lateral in 7, right lateral in 3, and posterior paraseptal in 3. Our results have been gratifymg in that there have been no deaths, no recurrences, and no necessity to prescribe drugs for postopera-
tive arrhythmias. One patient each underwent mitral valve and aortic valve replacement at the same time as accessory pathway ablation. Those 2 patients are on a regimen of maintenance digoxin.
We believe the Guiraudon technique is simple, straightfor- ward, and reproducible. It is quite gratifying to be operating and know precisely when you have interrupted the accessory pathway because the electrophysiologist monitoring the ECG can tell you exactly when you have accomplished this goal. As Dr. Guiraudon mentioned, the surgical dissection most often interrupts the pathway; it has in each of our 13 patients. Cryo- ablation is done for insurance in case there is an associated subendocardial accessory pathway.
DR. GUIRAUDON: I give special thanks to Dr. Will Sealy. He is the man who pioneered this whole field. Since 1974, when he wel- comed me in his office in Durham, he has always been a mas- ter, a mentor, and a friend, and he has continually supported my efforts to improve techniques for cardiac arrhythmias. Thank you very much, Dr. Sealy.
I will answer the two questions posed by Dr. Sealy. First, cardiopulmonary bypass is not necessary for posterior septal accessory pathways, and we are using it less and less frequently for that location. In this series, cardiopulmonary bypass was utilized in 15 of the 23 patients with posterior septal pathways. We don't have to use cardiopulmonary bypass for the right free wall accessory pathway. If a left thoracotomy approach is se- lected, cardiopulmonary bypass is not needed to ablate the left free wall accessory pathway. In conclusion, in some instances not only can we eliminate cross-clamping of the aorta but also the need for cardiopulmonary bypass.
As far as the mitral valve annulus and mitral valve injury are concerned, we observed no mitral valve lesions in our dog study. All of our patients have undergone two-dimensional echocardiography, and we have seen no mitral valve dysfunc- tion after operation, even after one year.
In regard to the anatomy of the left and right AV junction, it is true that most of the subendocardial pathways were de- scribed in the right ventricular free wall and we did not expect any in the left ventricular free wall. However, this pathological finding is based on only 45 specimens; it is much less of a surgical experience.
I thank Dr. Brown very much for his support. I hope that he will continue to have success with this technique.
Related Documents