clinicaloptions.com/hepatitis Seizing the Opportunity Management of Chronic Hepatitis C in 2013 John M. Vierling, M.D., F.A.C.P. Professor of Medicine and Surgery Chief of Hepatology Director of Advanced Liver Therapies Baylor College of Medicine St. Luke’s Medical Center Houston, Texas

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

clinicaloptions.com/hepatitis
Seizing the Opportunity
Management of Chronic Hepatitis C in 2013
John M. Vierling, M.D., F.A.C.P.
Professor of Medicine and Surgery
Chief of Hepatology
Director of Advanced Liver Therapies
Baylor College of Medicine
St. Luke’s Medical Center
Houston, Texas
clinicaloptions.com/hepatitis
Seizing the Opportunity
Management of Chronic Hepatitis C in 2013
I would rather donate all of my organs right now than hear another talk about currently approved therapies for chronic hepatitis C.
A. True
B. False
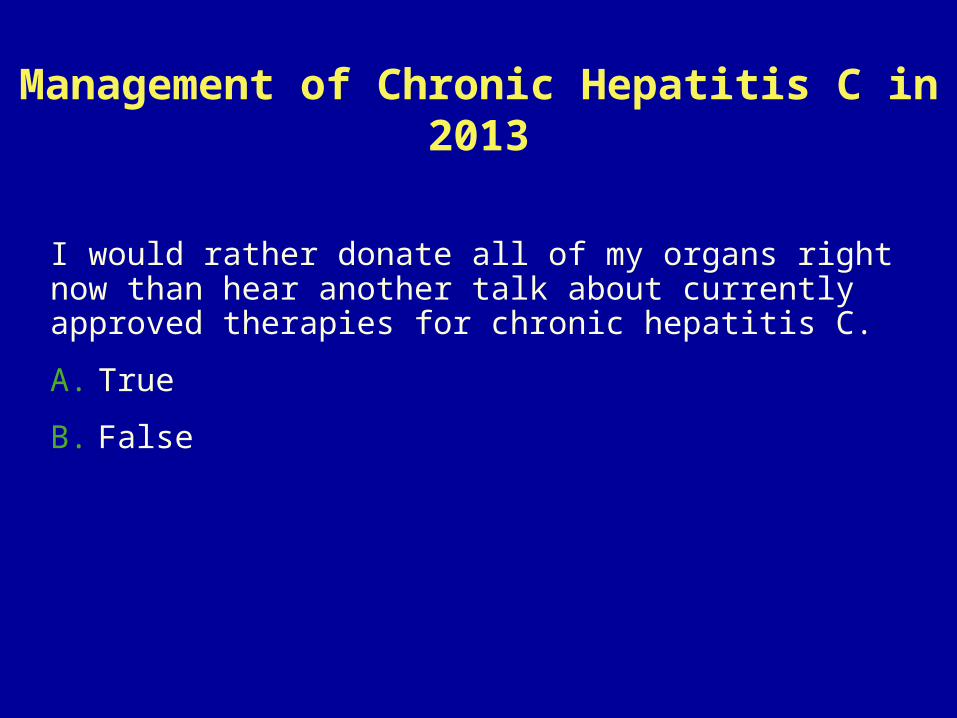
HCV Infection a Global Problem: 170 M PersonsHepatitis C Death Rates Per 100,000
www.worldlifeexpectancy.com

clinicaloptions.com/hepatitis
Seizing the Opportunity
Chronic Hepatitis C: A Treatable Disease
HCV infection Chronic in 70-85% and progressive in substantial proportion
Complications increasingly common[1,2]
Decompensated cirrhosis
Hepatic failure
HCC 3-7% per year in cirrhotics
Treatment resulting in SVR Eradication of HCV infection (cure)
Results in histologic improvement and regression of fibrosis[3]
Reduces risk of hepatic failure and HCC
Improves survival[4,5]
1. Kanwal F, et al. Gastroenterology. 2011;140:1182-1188. 2. Shaw JJ, et al. Expert Rev Gastroenterol Hepatol. 2011;5:365-370. 3. Poynard T, et al. Gastroenterology. 2002;122:1303-1313. 4. Craxi A, et al. Clin Liver Dis. 2005;9:329-346. 5. Shiratori Y, et al. Ann Intern Med. 2005;142:105-114.
clinicaloptions.com/hepatitis
Seizing the Opportunity
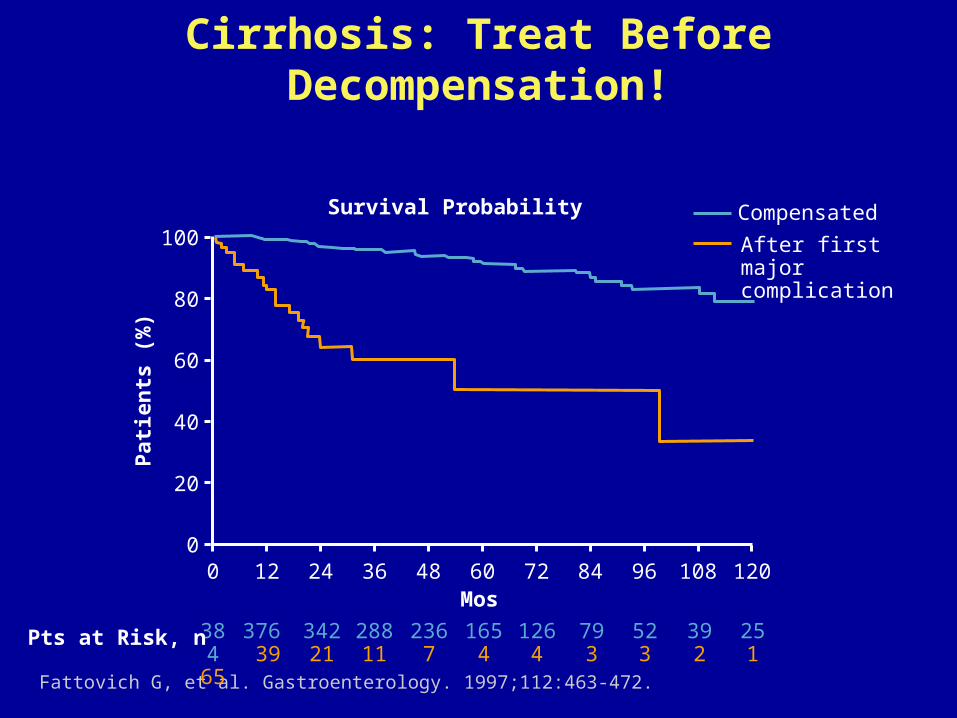
Cirrhosis: Treat Before Decompensation!
Fattovich G, et al. Gastroenterology. 1997;112:463-472.
Compensated
After first major complication
Survival Probability
100
Pat
ien
ts (
%)
80
60
40
20
01200 12 24 36 48 60 72 84 96 108
Mos
384 65
Pts at Risk, n 376 39
34221
28811
2367
1654
1264
793
523
392
251

clinicaloptions.com/hepatitis
Seizing the Opportunity
No SVR
SVR100
Pat
ien
ts W
ith
Liv
er
Co
mp
licat
ion
s (%
) 80
60
40
20
01680 24 48 72 96 120 144
Mos
759 124
702119
634116
527108
34570
20741
3412
Liver-Related Complications Decrease Following SVR in Cirrhotic Patients
Bruno S, et al. Hepatology. 2007;45:579-587.
Pts at Risk, n
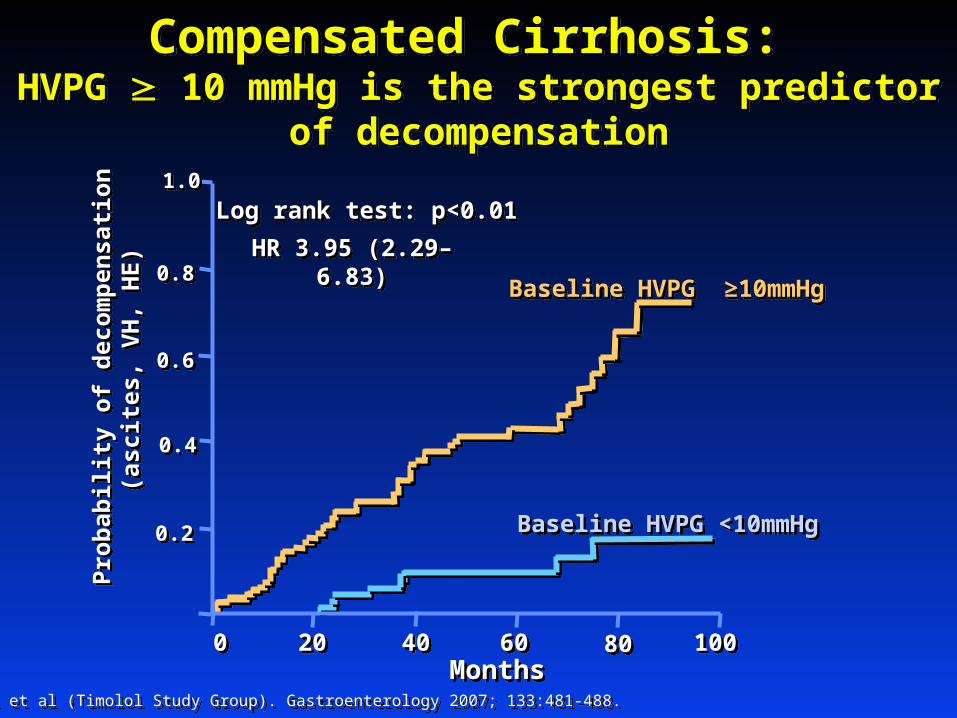
Compensated Cirrhosis: HVPG 10 mmHg is the strongest predictor of
decompensation
Compensated Cirrhosis: HVPG 10 mmHg is the strongest predictor of
decompensation
Ripoll et al (Timolol Study Group). Gastroenterology 2007; 133:481-488. Ripoll et al (Timolol Study Group). Gastroenterology 2007; 133:481-488.
0.20.2
0.40.4
0.60.6
0.80.8
1.01.0
Pro
bab
ilit
y o
f d
eco
mp
ensa
tio
n
(asc
ites
, V
H,
HE
)P
rob
abil
ity
of
dec
om
pen
sati
on
(a
scit
es,
VH
, H
E)
00 80802020 1001004040 6060MonthsMonths
Baseline HVPG ≥10mmHgBaseline HVPG ≥10mmHg
Baseline HVPG <10mmHg Baseline HVPG <10mmHg
Log rank test: p<0.01Log rank test: p<0.01
HR 3.95 (2.29–6.83)HR 3.95 (2.29–6.83)

HCV Antiviral Therapy Decreases HVPG in Patients with Advanced Fibrosis or Cirrhosis
with Portal Hypertension (n=20)
Rincon et al. Am J Gastroenterol 2006;101:2269–2274.Rincon et al. Am J Gastroenterol 2006;101:2269–2274.
9/11 patients with HVPG ≥ 12 mmHg had a reduction >20% or to <12 mmHg
HVPG reduction superior in virological and biochemical
responders at EOT
*
* Almost immediately after completing AVT

121200 60602424 7272
HVPG > 10% HVPG > 10%
HVPG 10% HVPG 10%
% F
ree
of
var
ice
s%
Fre
e o
f v
aric
es
MonthsMonths
100100
8080
6060
4040
2020
003636 4848
p=0.014p=0.014
Groszmann, Garcia-Tsao, Bosch et al. N Engl J Med 2005, 353:2254-2261.Groszmann, Garcia-Tsao, Bosch et al. N Engl J Med 2005, 353:2254-2261.
Compensated Cirrhosis:
Reduction in HVPG >10% at one-year prevents development of varices
clinicaloptions.com/hepatitisUse of Boceprevir and Telaprevir for the Treatment of Hepatitis C
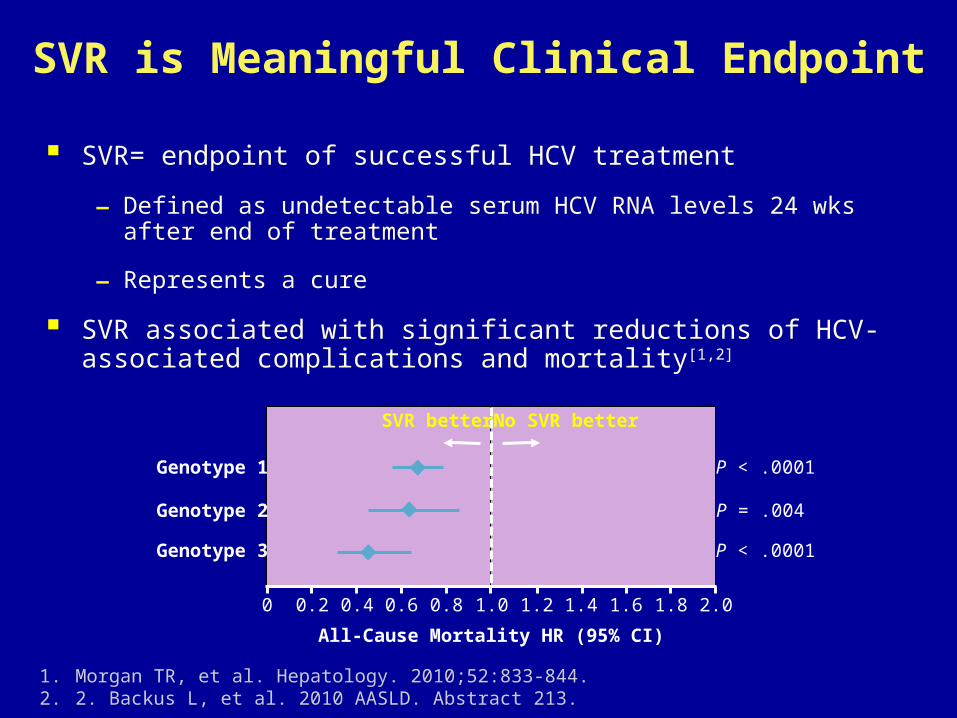
SVR is Meaningful Clinical Endpoint
SVR= endpoint of successful HCV treatment
– Defined as undetectable serum HCV RNA levels 24 wks after end of treatment
– Represents a cure
SVR associated with significant reductions of HCV-associated complications and mortality[1,2]
1. Morgan TR, et al. Hepatology. 2010;52:833-844. 2. 2. Backus L, et al. 2010 AASLD. Abstract 213.
SVR better No SVR better
Genotype 1
Genotype 2
Genotype 3
P < .0001
P = .004
P < .0001
All-Cause Mortality HR (95% CI)
0 0.2 0.4 0.6 0.8 1.0 1.2 1.4 1.6 1.8 2.0
clinicaloptions.com/hepatitis
Seizing the Opportunity
Management of Chronic Hepatitis C in 2013
SVR after antiviral therapy for HCV infection:
A. Represents a cure
B. Reduces liver-related mortality
C. Reduces all-cause mortality
D. Needs to be better understood by Dr. Goss
E. All of the above
clinicaloptions.com/hepatitis
Seizing the OpportunityFor HCV Genotype 2 or 3, PegIFN/RBV Current Standard of Care
Higher SVR rates than genotype 1
24 wks of therapy recommended[1,2]
Patients with RVR and low baseline HCV RNA can be treated for 16 wks
Relapse rates may be higher[2]
Future regimens may offer further improvements, such as
Shorter durations
All-oral therapy
Fewer adverse events
1. Ghany MG, et al. Hepatology. 2011;54:1433-1444. 2. EASL. J Hepatol. 2011;55:245-264.
clinicaloptions.com/hepatitis
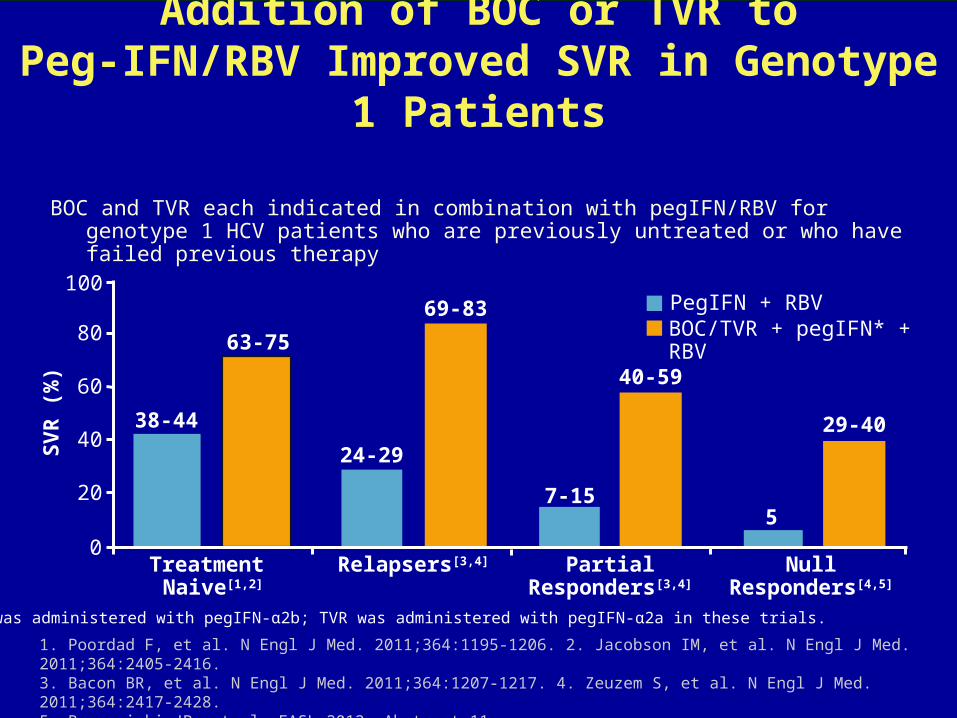
Seizing the OpportunityAddition of BOC or TVR to Peg-IFN/RBV Improved SVR in Genotype 1 Patients
BOC and TVR each indicated in combination with pegIFN/RBV for genotype 1 HCV patients who are previously untreated or who have failed previous therapy
1. Poordad F, et al. N Engl J Med. 2011;364:1195-1206. 2. Jacobson IM, et al. N Engl J Med. 2011;364:2405-2416. 3. Bacon BR, et al. N Engl J Med. 2011;364:1207-1217. 4. Zeuzem S, et al. N Engl J Med. 2011;364:2417-2428. 5. Bronowicki JP, et al. EASL 2012. Abstract 11.
0
20
40
60
80
100
SV
R (
%)
Relapsers[3,4] Partial Responders[3,4]
PegIFN + RBV
NullResponders[4,5]
BOC/TVR + pegIFN* + RBV
24-29
7-15
29-40
5
69-83
40-59
63-75
38-44
Treatment Naive[1,2]
*BOC was administered with pegIFN-α2b; TVR was administered with pegIFN-α2a in these trials.
clinicaloptions.com/hepatitis
Seizing the Opportunity
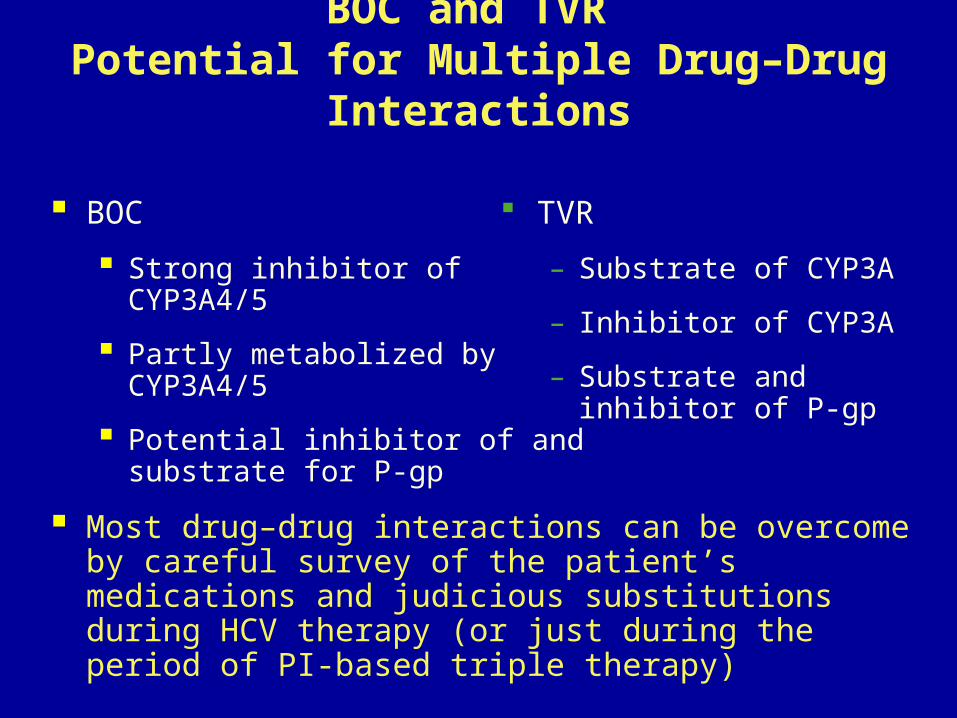
TVR
– Substrate of CYP3A
– Inhibitor of CYP3A
– Substrate and inhibitor of P-gp
BOC and TVR Potential for Multiple Drug–Drug Interactions
BOC
Strong inhibitor of CYP3A4/5
Partly metabolized by CYP3A4/5
Potential inhibitor of and substrate for P-gp
Most drug–drug interactions can be overcome by careful survey of the patient’s medications and judicious substitutions during HCV therapy (or just during the period of PI-based triple therapy)
clinicaloptions.com/hepatitis
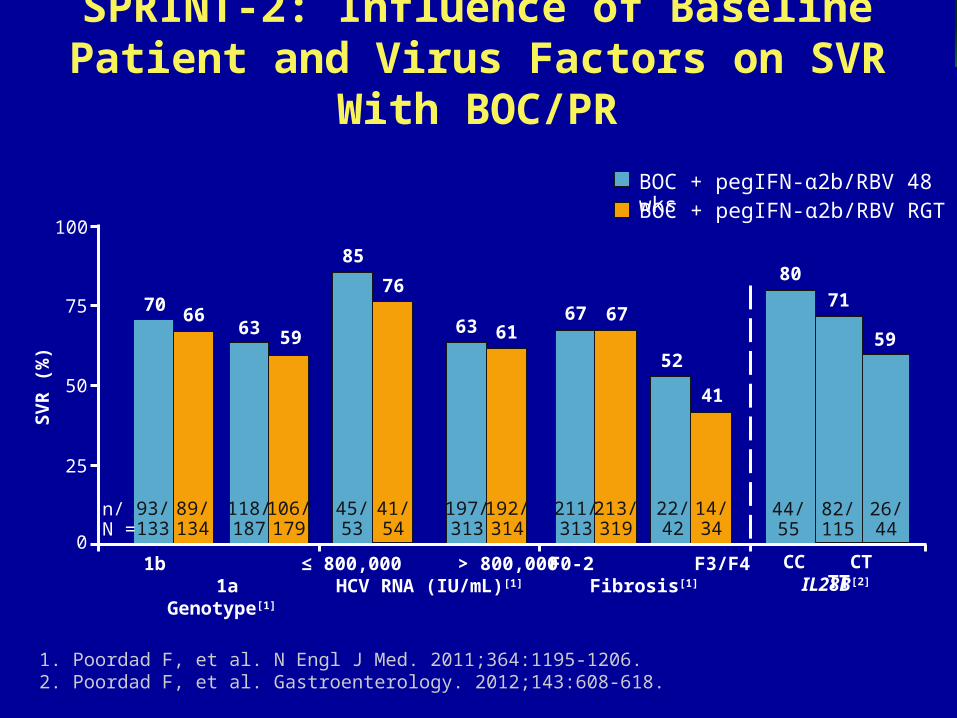
Seizing the OpportunitySPRINT-2: Influence of Baseline Patient and Virus Factors on SVR With BOC/PR
1. Poordad F, et al. N Engl J Med. 2011;364:1195-1206. 2. Poordad F, et al. Gastroenterology. 2012;143:608-618.
BOC + pegIFN-α2b/RBV RGTBOC + pegIFN-α2b/RBV 48 wks
93/133
89/134
100
0
50
1b 1aGenotype[1]
70 66
≤ 800,000 > 800,000 HCV RNA (IU/mL)[1]
85
76
F0-2 F3/F4Fibrosis[1]
6767
SV
R (
%)
75
25
41/54
45/53
213/319
211/313
n/N =
63 5963 61
41
52
118/187
106/179
14/34
22/42
192/314
197/313
44/55
82/115
26/44
CC CT TT
80
71
59
IL28B[2]

clinicaloptions.com/hepatitis
Seizing the Opportunity
1b 1aGenotype[1]
< 800,000 ≥ 800,000HCV RNA (IU/mL)[1]
F0-2 F3/F4Fibrosis[1]
ADVANCE: Influence of Baseline Patient and Virus Factors on SVR With TVR
Data from TVR12 + pegIFN-α2a/RBV arm only
1. Jacobson IM, et al. N Engl J Med. 2011;364:2405-2416. 2. Jacobson IM, et al. EASL 2011. Abstract 1369.
CC CT TT
IL28B*[2]
152/213
118/149
100
0
50
7971
7874
62
78
SV
R (
%)
75
25
207/281
64/82
45/73
226/290
n/N =
45/50
48/68
16/22
90
71 73
*IL28B testing was in whites only.

clinicaloptions.com/hepatitis
Seizing the Opportunity
Challenging Patients with Suboptimal Current Treatment Options
Cirrhosis (all genotypes)
Decompensated cirrhosis
Null responders
Pre-transplantation
Post-transplantation
Chronic Renal failure
Impaired renal function
Dialysis
Renal transplantation recipients
Injection-drug users
Methadone substitution
Thalassemics
Children
IFN contraindicated
IFN intolerant
Those with poor social support
Psychiatric comorbidities

HCV AntiviralsNew Studies Using Current Therapies

clinicaloptions.com/hepatitisHCV Phase III Studies and Approved Agents
CONCISE: Telaprevir + P/R for Patients with HCV GT 1 and IL28B CC
Interim analysis of ongoing, multicenter, randomized, active-controlled, exploratory phase IIIb study
Treatment-naive patients or previous relapsers with GT 1
HCV, IL28B CC genotype,
and no cirrhosis(N = 239)
T12/PR24Continue P/R alone
(n = 52)
2:1 randomization*
Wk 12 Wk 24
T12/PR12Stop all treatment
(n = 107)
*Patients with RVR randomly assigned 2:1 to T12/PR12 or T12/PR24.
Nelson DR, et al. EASL 2013. Abstract 881.
Telaprevir + P/R
clinicaloptions.com/hepatitisHCV Phase III Studies and Approved Agents
0
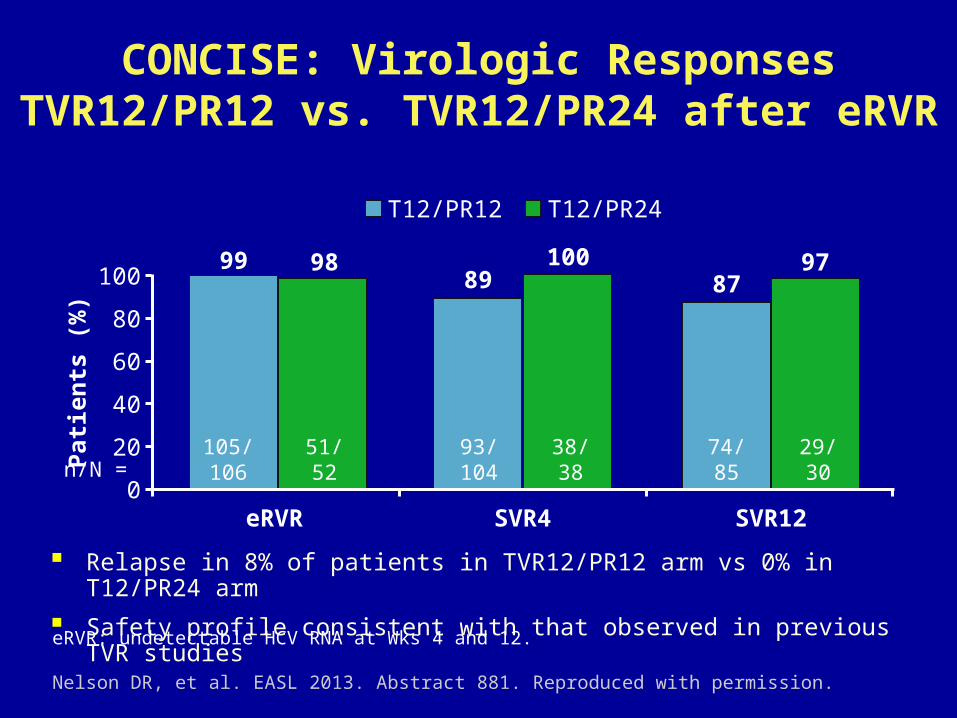
CONCISE: Virologic ResponsesTVR12/PR12 vs. TVR12/PR24 after eRVR
Relapse in 8% of patients in TVR12/PR12 arm vs 0% in T12/PR24 arm
Safety profile consistent with that observed in previous TVR studies
eRVR: undetectable HCV RNA at Wks 4 and 12. Nelson DR, et al. EASL 2013. Abstract 881. Reproduced with permission.
n/N =105/106
51/52
93/104
38/38
74/85
29/30
100
80
60
40
20Pat
ien
ts (
%)
99 9889
10087
97
eRVR SVR4 SVR12
T12/PR12 T12/PR24

clinicaloptions.com/hepatitisHCV Phase III Studies and Approved Agents
TARGET-C: TVR With Reduced RBV + Peg-IFN in HCV-Infected Hemodialysis Patients
Increased incidence of select AEs in TVR arms vs P/R
Anemia (54% vs 33%)
Neutropenia (50% vs 33%)
Thrombocytopenia (37% vs 25%)
Rash (42% vs 17%)
Anorectal dysfunction (33% vs 0%)
Dysgeusia (42% vs 17%)Basu P, et al. EASL 2013. Abstract 67.
n/N =
8/12
6/12
3/12
7/12
6/12
3/12
80
60
40
20
0
HC
V R
NA
U
nd
etec
tab
le (
%)
EOT SVR
67
50
25
63
50
25
TVR + PegIFN/RBV 200 mg
Wk 12
Pts with GT 1 HCV; on hemodialysis
(N = 36)
PegIFN/RBV 400 mg
TVR + PegIFN + Placebo PegIFN/RBV 400 mg
Placebo + PegIFN/RBV 400 mg
Wk 24 Wk 36 Wk 48
n = 12
n = 12
n = 12
100 PegIFN alfa-2a dosed at 135 µg/wk

HCV Antiviral Therapyfor Genotype 1 Cirrhotics
clinicaloptions.com/hepatitisHCV Phase III Studies and Approved Agents
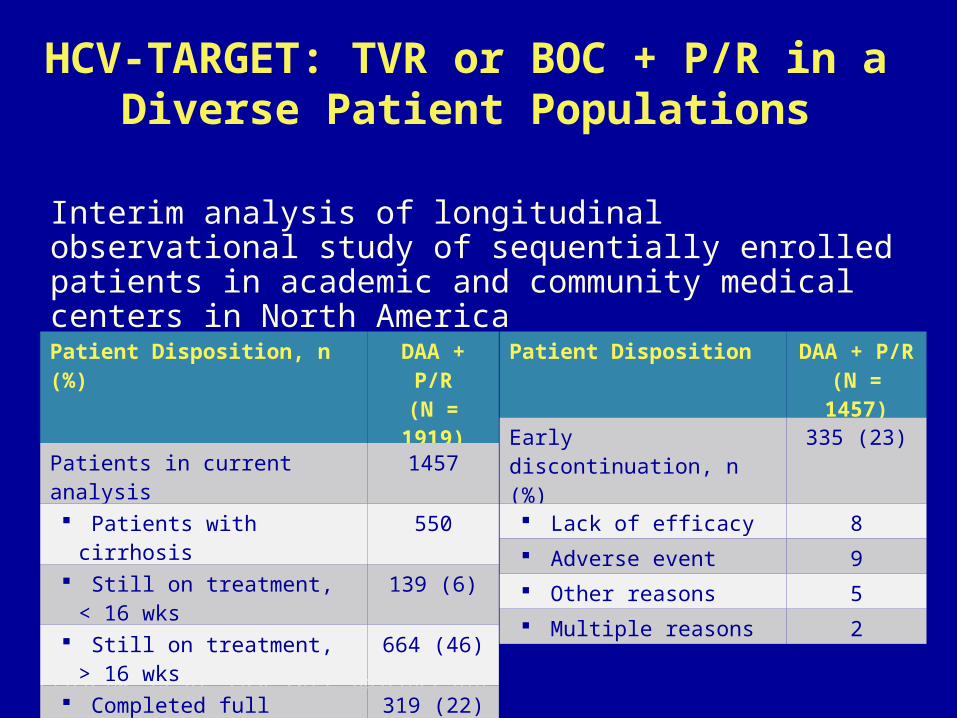
HCV-TARGET: TVR or BOC + P/R in a Diverse Patient Populations
Interim analysis of longitudinal observational study of sequentially enrolled patients in academic and community medical centers in North America
Fried MW, et al. EASL 2013. Abstract 818.
Patient Disposition, n (%) DAA + P/R(N = 1919)
Patients in current analysis 1457
Patients with cirrhosis 550
Still on treatment, < 16 wks 139 (6)
Still on treatment, > 16 wks 664 (46)
Completed full course 319 (22)
Patient Disposition DAA + P/R(N = 1457)
Early discontinuation, n (%) 335 (23)
Lack of efficacy 8
Adverse event 9
Other reasons 5
Multiple reasons 2

clinicaloptions.com/hepatitisHCV Phase III Studies and Approved Agents
HCV-TARGET: Baseline Characteristics
Fried MW, et al. EASL 2013. Abstract 818.
Patient Characteristic Cirrhotic(n = 550)
Noncirrhotic(n = 787)
40-64 yrs of age, % 84 80
Male, % 69 55
White, % 78 70
Genotype, % 1a 1b Not otherwise specified
581919
582213
Treatment naive, % 41 52
Mean hemoglobin > 12 g/dL 94 84
Mean platelets, cells/mm3 126,000 203,000
Mean total bilirubin, mg/dL (range) 1.0 (0.2-5.0) 0.63 (0.2-2.5)
Mean albumin, g/dL (range) 3.9 (1.4-5.0) 4.2 (1.9-5.4)
Mean Meld score (range) 8 (6-22) N/A
Presence of varices, % 33 1

clinicaloptions.com/hepatitisHCV Phase III Studies and Approved Agents
HCV-TARGET: Virologic Response by Previous Treatment Category
In interim analysis, on-treatment efficacy of telaprevir and boceprevir in real-world setting comparable to registration trials
Fried MW, et al. EASL 2013. Abstract 818. Reproduced with permission.
n = 400 247 101 79 133 92 28 25 119 74 21 16 149 76 37 32
100
80
60
40
20
0
TVR Wk 4TVR Wk 12
BOC Wk 8BOC Wk 12
Treatment Naive
Previous Relapser
Previous Partial or Null Response
UnknownResponse
54
86
61
78
54
78
25
48 43
73
15
44 45
80
43
63
Un
det
ecta
ble
HC
V R
NA
(%
)
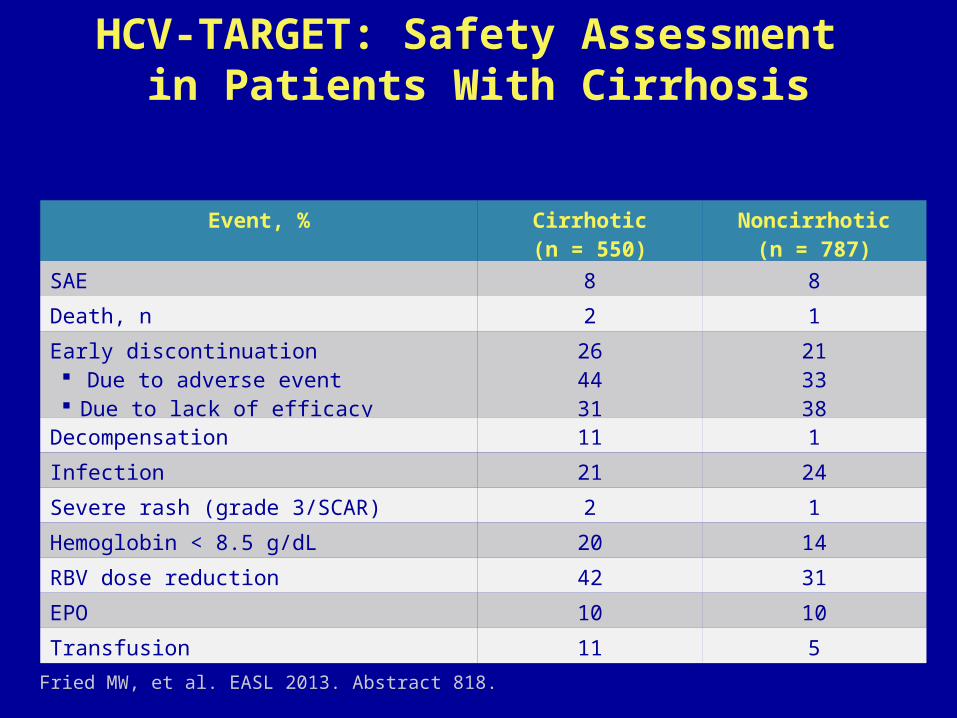
clinicaloptions.com/hepatitisHCV Phase III Studies and Approved AgentsHCV-TARGET: Safety Assessment
in Patients With Cirrhosis
Fried MW, et al. EASL 2013. Abstract 818.
Event, % Cirrhotic(n = 550)
Noncirrhotic(n = 787)
SAE 8 8
Death, n 2 1
Early discontinuation Due to adverse event Due to lack of efficacy
264431
213338
Decompensation 11 1
Infection 21 24
Severe rash (grade 3/SCAR) 2 1
Hemoglobin < 8.5 g/dL 20 14
RBV dose reduction 42 31
EPO 10 10
Transfusion 11 5

CUPICBoceprevir and Telaprevir Treatment Regimens
Fontaine H, et al. 48th EASL; Amsterdam, Netherlands; April 24-28, 2013. Abst. 60Hezode, C, et al. 63rd AASLD; Boston, MA; November 9-13, 2012. Abst. 51.
Peg-IFN α-2a + RBVTVR + Peg-IFN α-2a + RBV Follow-up
484 160 128Weeks
72SVR12
BOC + Peg-IFN α-2b + RBV Follow-upPeg-IFN + RBV
36
BOC: 800 mg/8h; Peg-IFNα-2b: 1.5 µg/kg/week; RBV: 800 to 1400 mg/day
TVR: 750 mg/8h; Peg-IFNα-2a: 180 µg/week; RBV: 1000 to 1200 mg/day
SVR24
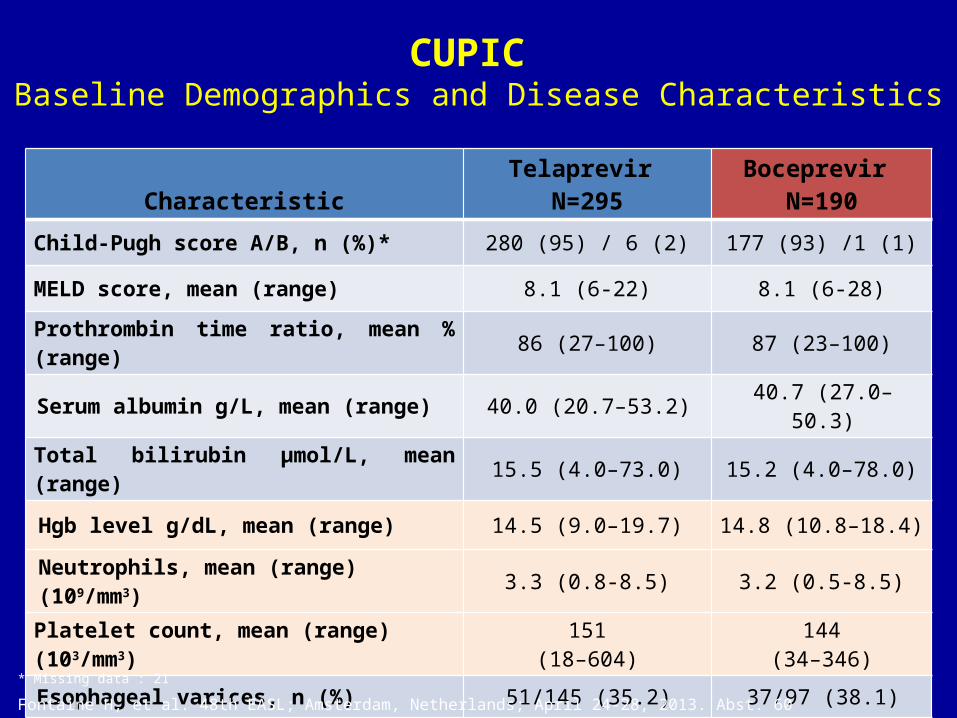
CUPIC Baseline Demographics and Disease Characteristics
CharacteristicTelaprevir
N=295Boceprevir
N=190
Child-Pugh score A/B, n (%)* 280 (95) / 6 (2) 177 (93) /1 (1)
MELD score, mean (range) 8.1 (6-22) 8.1 (6-28)
Prothrombin time ratio, mean % (range) 86 (27–100) 87 (23–100)
Serum albumin g/L, mean (range) 40.0 (20.7–53.2) 40.7 (27.0–50.3)
Total bilirubin μmol/L, mean (range) 15.5 (4.0–73.0) 15.2 (4.0–78.0)
Hgb level g/dL, mean (range) 14.5 (9.0–19.7) 14.8 (10.8–18.4)
Neutrophils, mean (range) (109/mm3) 3.3 (0.8-8.5) 3.2 (0.5-8.5)
Platelet count, mean (range) (103/mm3) 151(18–604)
144(34–346)
Esophageal varices, n (%) 51/145 (35.2) 37/97 (38.1)
Fontaine H, et al. 48th EASL; Amsterdam, Netherlands; April 24-28, 2013. Abst. 60
* Missing data : 21
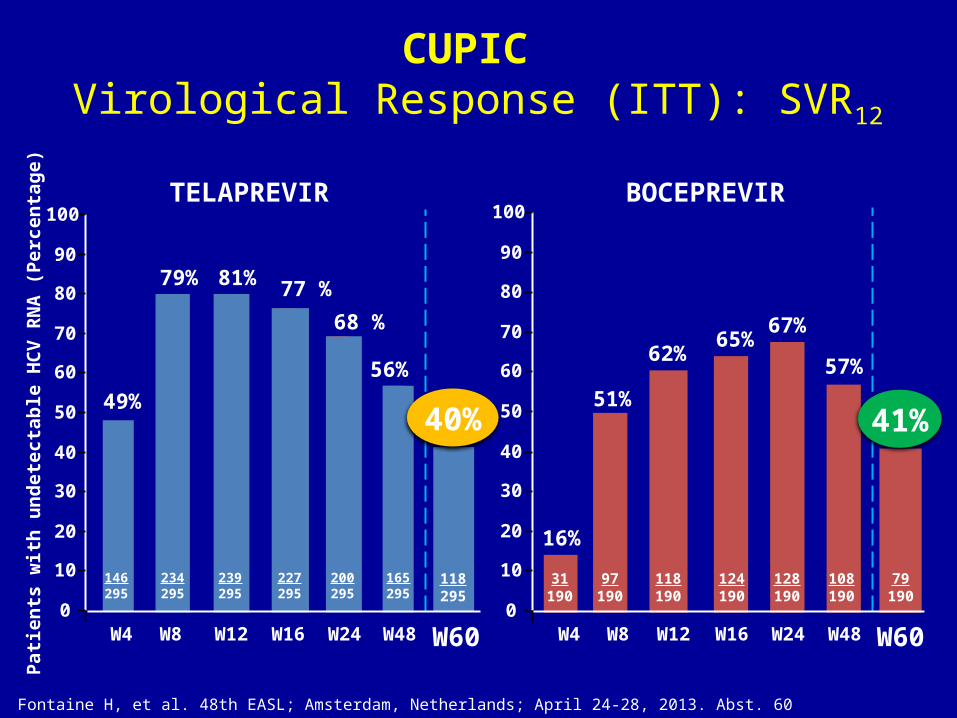
CUPIC Virological Response (ITT): SVR12
Fontaine H, et al. 48th EASL; Amsterdam, Netherlands; April 24-28, 2013. Abst. 60
TELAPREVIR BOCEPREVIR
0
10
20
30
40
50
60
70
80
90
100
49%
Pat
ien
ts w
ith
un
det
ecta
ble
HC
V R
NA
(P
erce
nta
ge
)
79% 81%
56%
W4 W8 W12 W24 W48 W60W16
77 %
68 %
146295
234295
239295
227295
200295
165295
118295
0
10
20
30
40
50
60
70
80
90
100
16%
51%
62%65%
67%
W4 W8 W12 W16 W24 W48 W60
31190
97190
118190
124190
128190
108190
57%
79190
40% 41%

CUPICSVR12 According to HCV G1 Subtype
Fontaine H, et al. 48th EASL; Amsterdam, Netherlands; April 24-28, 2013. Abst. 60
Genotype 1a
Genotype 1b
Undeterminedgenotype 1
33/98 75/162 9/33
34%46%
27%
P=0.004
0
10
20
30
40
50
60
70
80
90
100
SV
R 1
2 (I
TT
) (
Pe
rcen
tag
e)
TELAPREVIR
Genotype 1a
Genotype 1b
Undeterminedgenotype 1
0
10
20
30
40
50
60
70
80
90
100
6/16
P=0.03
31%
51%
37%
49/9624/77
BOCEPREVIR
SV
R 1
2 (I
TT
) (
Pe
rcen
tag
e)

CUPIC: SVR12 Safety FindingsPatients, n
(% patients with at least one event) Telaprevir n=295 Boceprevir n=190
Serious adverse events (SAEs)* 535 in 160 patients (54.2%)
321 in 97 patients(51.0%)
Premature discontinuation / due to SAEs
139 (47.1%) / 63 (21.3%)
80 (42.1%)/27 (14.2%)
Death 7 (2.4 %) 3 (1.6%)
Infection (Grade 3/4) 27 (9.1 %) 8 (4.2%)
Hepatic decompensation (Grade ¾ ) 15 (5.1 %) 9 (4.7%)
Anemia (Grade ¾ : Hb < 8 g/dL) 38 (12.9 %) 19 (10%)
Rash (grade 3/SCAR) 16 (5.4 %)/ 2 (0.6 %) 2 (1.0%)/
EPO use / blood transfusion
168 (57 %) / 53 (18 %)
119 (62.6%) /26 (13.7%)
GCSF use 8 (2.7 %) 13 (6.8%)
TPO use 6 (2 %) 3 (1.6%)
Fontaine H, et al. 48th EASL; Amsterdam, Netherlands; April 24-28, 2013. Abst. 60
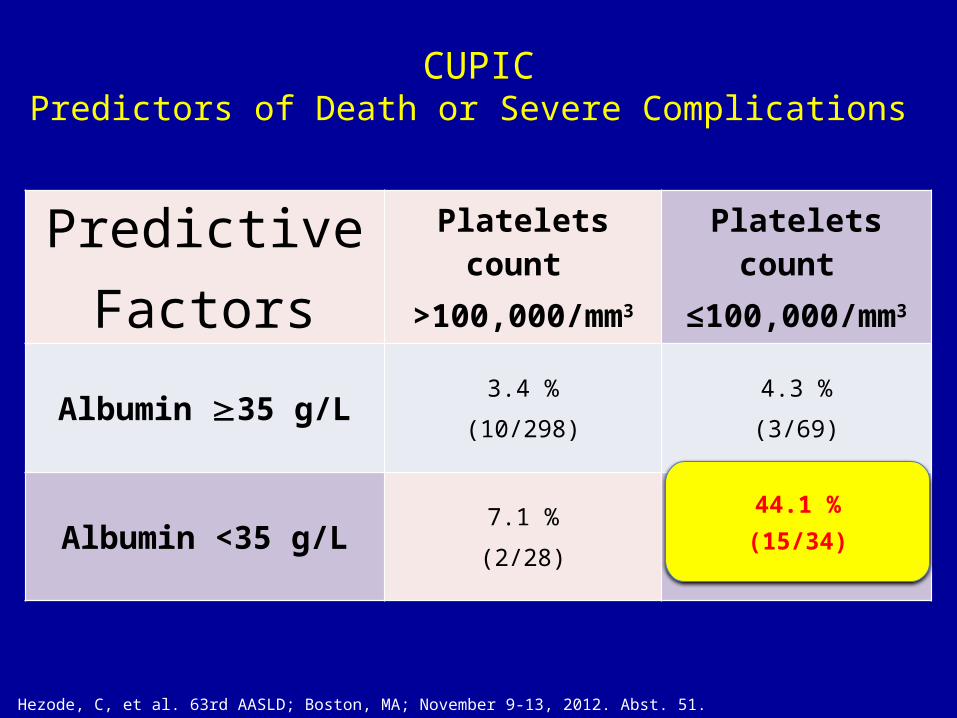
CUPICPredictors of Death or Severe Complications
Hezode, C, et al. 63rd AASLD; Boston, MA; November 9-13, 2012. Abst. 51.
PredictiveFactors
Platelets count >100,000/mm3
Platelets count ≤100,000/mm3
Albumin 35 g/L 3.4 %(10/298)
4.3 %(3/69)
Albumin <35 g/L 7.1 %(2/28)
44.1 %
(15/34)
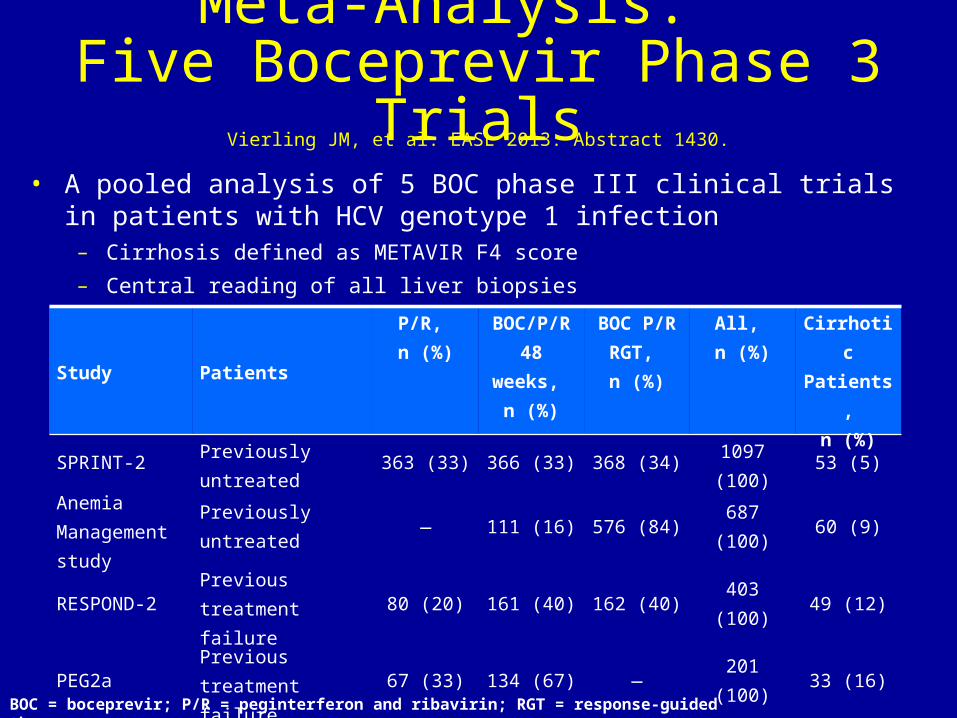
Meta-Analysis: Five Boceprevir Phase 3 Trials
• A pooled analysis of 5 BOC phase III clinical trials in patients with HCV genotype 1 infection
– Cirrhosis defined as METAVIR F4 score – Central reading of all liver biopsies
BOC = boceprevir; P/R = peginterferon and ribavirin; RGT = response-guided therapy
Study PatientsP/R, n (%)
BOC/P/R 48 weeks,
n (%)
BOC P/RRGT, n (%)
All, n (%)
Cirrhotic Patients,
n (%)
SPRINT-2 Previously untreated 363 (33) 366 (33) 368 (34) 1097 (100) 53 (5)
Anemia Management study
Previously untreated — 111 (16) 576 (84) 687 (100) 60 (9)
RESPOND-2 Previous treatment failure 80 (20) 161 (40) 162 (40) 403 (100) 49 (12)
PEG2a Previous treatment failure 67 (33) 134 (67) — 201 (100) 33 (16)
PROVIDE Previous treatment failure — 134 (100) — 134 (100) 17 (13)
Total 510 (20) 906 (36) 1106 (44) 2522 (100) 212 (8)
Vierling JM, et al. EASL 2013. Abstract 1430.
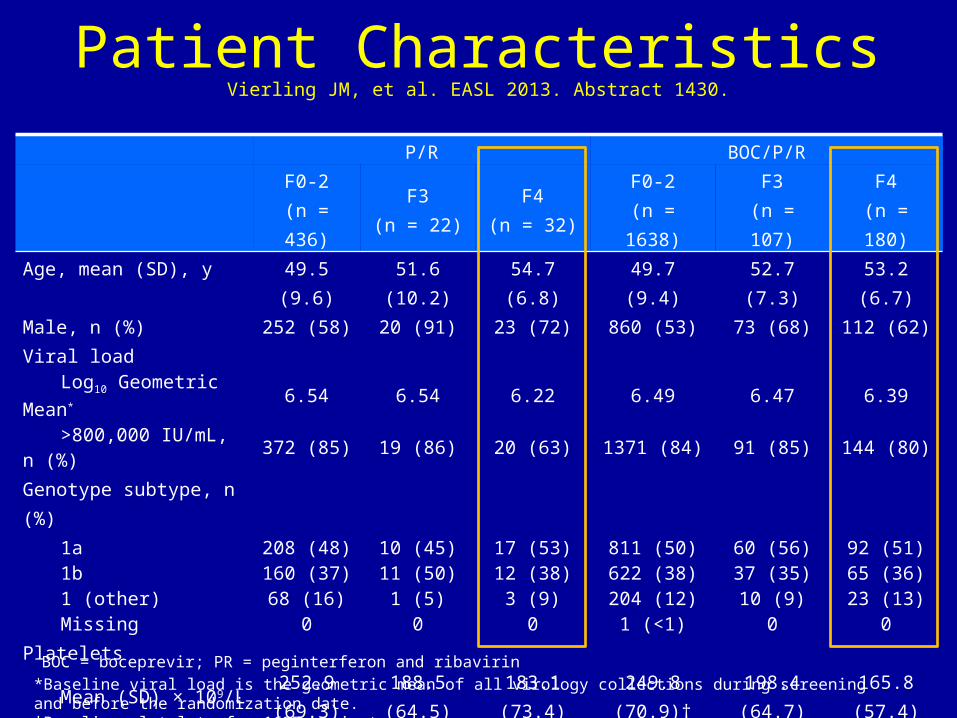
Patient CharacteristicsP/R BOC/P/R
F0-2(n = 436)
F3(n = 22)
F4(n = 32)
F0-2(n = 1638)
F3(n = 107)
F4(n = 180)
Age, mean (SD), y 49.5 (9.6) 51.6 (10.2) 54.7 (6.8) 49.7 (9.4) 52.7 (7.3) 53.2 (6.7)Male, n (%) 252 (58) 20 (91) 23 (72) 860 (53) 73 (68) 112 (62)Viral load
Log10 Geometric Mean* 6.54 6.54 6.22 6.49 6.47 6.39>800,000 IU/mL, n (%) 372 (85) 19 (86) 20 (63) 1371 (84) 91 (85) 144 (80)
Genotype subtype, n (%) 1a 208 (48) 10 (45) 17 (53) 811 (50) 60 (56) 92 (51)1b 160 (37) 11 (50) 12 (38) 622 (38) 37 (35) 65 (36)1 (other) 68 (16) 1 (5) 3 (9) 204 (12) 10 (9) 23 (13)Missing 0 0 0 1 (<1) 0 0
Platelets Mean (SD) × 109/L 252.9 (69.3) 188.5 (64.5) 183.1 (73.4) 249.8 (70.9)† 198.4 (64.7) 165.8 (57.4)<150 × 109 cells/L, n (%) 26 (6) 8 (36) 10 (31) 99 (6) 27 (25) 78 (43)
Baseline haemoglobin (g/dL), mean (SD) 14.7 (1.3) 15.7 (1.3) 15.2 (1.1) 14.6 (1.3) 15.1 (1.4) 14.6 (1.2)
Baseline serum albumin Mean (range), g/L 40.7 (32-49) 40.1 (34-46) 39.1 (34-44) 40.9 (30-51) 39.9 (30-49) 38.8 (31-49)<35 g/dL, n (%) 6 (<1) 1 (5) 3 (9) 38 (2) 5 (5) 21 (12)
*Baseline viral load is the geometric mean of all virology collections during screening and before the randomization date.†Baseline platelets for 1637 patients.
BOC = boceprevir; PR = peginterferon and ribavirin
Vierling JM, et al. EASL 2013. Abstract 1430.

F0-2 F3 F4METAVIR Fibrosis Score
0%
25%
50%
75%
100%
66%54% 55%
28% 26% 17%
Boceprevir + PR PR
SVR
(%, 9
5 CI
%)
Sustained Virologic Response
• SVR rates were substantially higher with BOC/P/R compared with P/R alone, regardless of fibrosis score
• In patients receiving BOC/P/R, SVR rates were similar in patients with bridging fibrosis (F3) and cirrhosis (F4)
*Treatment-naive patients and those with previous treatment failure combined. The analyses of the pooled studies were homogeneous for the SVR rates for F0-2 and F3 patients treated with BOC/P/R, and for F3 patients treated with P/R. Therefore, the fixed-effect estimates for the SVR rates were used for these patients. The analysis of the studies for the SVR rates was heterogeneous for F4 patients treated with BOC/P/R or P/R, and for F0-2 patients treated with P/R; therefore, the random-effect estimate for the SVR rate was used for these patientsBOC = boceprevir; CI = confidence interval; P/R = peginterferon and ribavirin; SVR = sustained virologic response.
n=1638 n=436 n=107 n=22 n=180 n=32
Vierling JM, et al. EASL 2013. Abstract 1430.

F0-2 F3 F4METAVIR Fibrosis Score
0%
25%
50%
75%
100%
77% 67% 66%40% 29% 21%
≥1 log HCV RNA decline at TW4 <1 log HCV RNA decline at TW 4
SVR
(%, 9
5% C
I)
SVR According to TW4 Virologic Response
• Regardless of METAVIR fibrosis score, SVR rates were higher in patients with ≥1 log10 decline in HCV RNA at TW4 than those with <1 log10 decline
• Among patients with ≥1 log10 decline in HCV RNA, SVR rates with BOC/P/R were similar in patients with METAVIR F3 and F4 fibrosis
• SVR rate was 21% in cirrhotic patients receiving BOC/P/R with <1 log10 decline in HCV RNA at TW4
*Treatment-naive patients and those with previous treatment failure combined (total treatment duration = 8 weeks).CI = confidence interval; HCV = hepatitis C virus; SVR = sustained virologic response; TW = treatment week.
895/1155 168/415 47/70 10/35 85/128 10/48
Vierling JM, et al. EASL 2013. Abstract 1430.
F0-2 F3 F4METAVIR Fibrosis Score
0%
25%
50%
75%
100%
86% 85% 89%
54%34% 35%
6%0% 0%
Undetectable ≥3 log HCV RNA decline and detectable <3 log HCV RNA decline and detectable
SVR
(%, 9
5% C
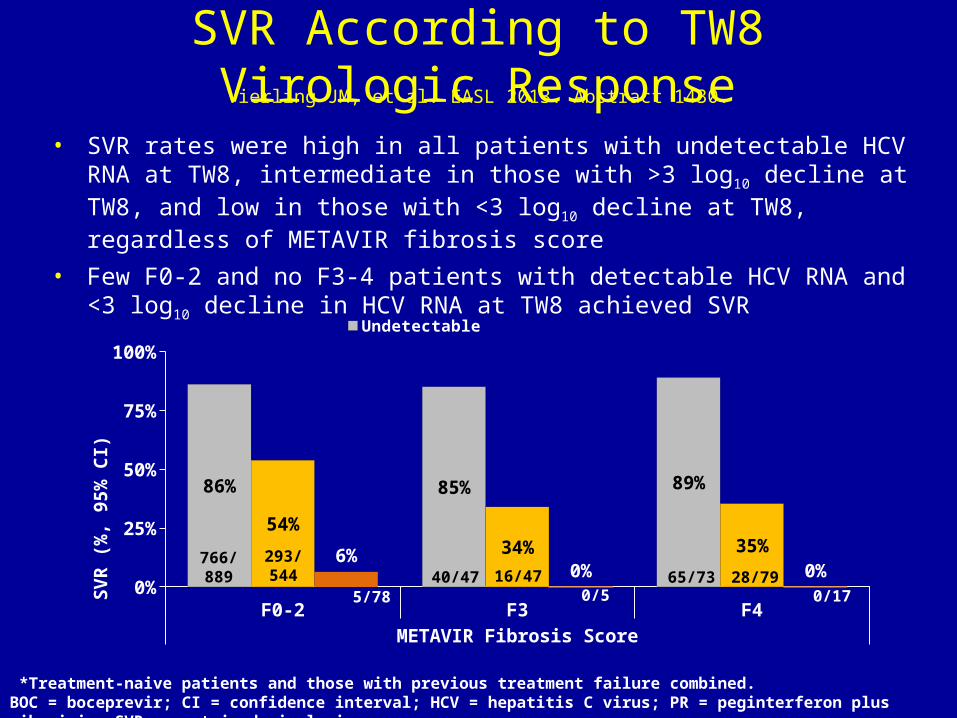
I)SVR According to TW8 Virologic Response
• SVR rates were high in all patients with undetectable HCV RNA at TW8, intermediate in those with >3 log10 decline at TW8, and low in those with <3 log10 decline at TW8, regardless of METAVIR fibrosis score
• Few F0-2 and no F3-4 patients with detectable HCV RNA and <3 log10 decline in HCV RNA at TW8 achieved SVR
*Treatment-naive patients and those with previous treatment failure combined. BOC = boceprevir; CI = confidence interval; HCV = hepatitis C virus; PR = peginterferon plus ribavirin; SVR = sustained virologic response.
766/889
293/544 40/47 16/47 65/73 28/79
0/170/55/78
Vierling JM, et al. EASL 2013. Abstract 1430.

Predictors of SVR in F3/F4 Patients Receiving BOC/PR
1 2 3 4 5 6 7 8
10.57 (5.23 – 21.36); P<0.0001
2.64 (1.33 – 5.21); P=0.0053
2.23 (1.18 – 4.24); P=0.0141
2.55 (1.05 – 6.20); P=0.0383
1.76 (0.90 – 3.44); P=0.0971
1.08 (0.43 – 2.72); P=0.8636
9 10Odds Ratio (95% CI)
TW8: undetectable vs. detectable HCV-RNA
TW4: ≥1log decline vs. <1 log decline
Male vs. female
Baseline viral load ≤800,000 IU/mL vs. >800,000 IU/mL
G1b vs. G1a
Non-black vs. black
CI = confidence interval; G = genotype; TW = treatment week.
Vierling JM, et al. EASL 2013. Abstract 1430.

SVR According to Treatment Duration in Patients with Undetectable HCV RNA at TW8 receiving BOC/PR*
*Treatment-naive patients and those with previous treatment failure combined. BOC = boceprevir; CI = confidence interval; HCV = hepatitis C virus; PR = peginterferon plus ribavirin; SVR = sustained virologic response.
58/132 4/6279/306 15/18 78/84 6/6 8/916/183/7
351/367 17/18 38/39
Vierling JM, et al. EASL 2013. Abstract 1430.

Significant Medical EventsPatients with Potential Hepatic Decompensation or Sepsis
Patient ID(Study)
Baseline Data Event Treatment regimen (weeks of treatment)
Outcome
Cirrhotic Patients016301(PROVIDE)
Male, 64 yo; F4.History of ascitesPlatelets, 108KAlbumin, 3.7 g/L
Decompensated cirrhosis with ascites and encephalopathy (confusion)
BOC/P/R(TW6)
Discontinued treatment; events resolved
012072(RESPOND-2)
Female, 51 yo; F4Platelets, 170KAlbumin, 3.5 g/L
Bleeding esophageal varices and portal hypertension
P/R(TW2)
Discontinued treatment; events resolved
000603(PEG2a study)
Male, 48 yo; F4Diabetic, IVDUPlatelets, 135KAlbumin, 3.8 g/L
Multi-organ failure with total bilirubin peak 17.4 mg/dL(Staphylococcus pneumonia, resulting in multi-organ failure)
BOC/P/R(TW12)
Died of multi-organ failure
Non-Cirrhotic Patients000005(PEG2a study)
Male, 52 yo; F2Platelets, 280KAlbumin, 4.2 g/L
Possible urosepsis(negative blood and urine cultures)
P/R(TW3)
Discontinued treatment; event resolved
001868(SPRINT-2)
Male, 58 yo; F2Platelets, 192KAlbumin, 3.5 g/L
Ascites(Hospitalized with severe epiglottitis and neutropenia; developed acute renal failure; treatment discontinued; ascites and oedema noted 12 days later)
12 days after discontinuing BOC/P/R (TW12)
Discontinued treatment for other AEs; ascites resolved
BOC = boceprevir; IVDU = intravenous drug user; P/R = peginterferon and ribavirin; TW = treatment week; yo = years old.
Vierling JM, et al. EASL 2013. Abstract 1430.

clinicaloptions.com/hepatitis
Seizing the OpportunityLimitations of Current Regimens and Prospects for Future Regimens
Current
Must be eligible for pegIFN/ RBV
High pill burden, TID dosing of PIs (at present); parenteral IFN
Multiple adverse events
Selection of resistance –associtaed variants with treatment failure
Only effective for genotype 1
Risk of resistance with poor adherence
Future
Increasingly IFN free
Lower pill burden, daily dosing;
Better tolerated
Limited resistance-associated variants
Pangenotypic
Higher barrier to resistance with some classes

clinicaloptions.com/hepatitis
Seizing the Opportunity
Investigational Agents for HCV in 2013
Interferons Antiviral agents
Therapeuticvaccines
Hosttarget
Replication, polyprotein processing and/or assembly
Entry
NS5Bpolymerase inhibitors
NS3/4Aprotease inhibitors
NS5Areplication complex inhibitors
miRNA-122 Cyclophilin
CypA
inhibitors
clinicaloptions.com/hepatitis
Seizing the Opportunity
Management of Chronic Hepatitis C in 2013
Regimens containing Peg-IFN are contraindicated for patients with cirrhosis who have all but one of the following:
A. Compensated cirrhosis
B. Decompensated cirrhosis
C. Albumin <3.5 mg/dL and Platelets <100,000 mm3
D. ESRD
Related Documents



![Hepatitis B virus and hepatitis C virus play different ... · alcoholic cirrhosis, hepatitis viruses, tobacco and metabolic diseases[4]. Hepatitis viruses, including hepatitis B virus](https://static.cupdf.com/doc/110x72/60e46cab5bd9101a6f539e91/hepatitis-b-virus-and-hepatitis-c-virus-play-different-alcoholic-cirrhosis.jpg)