Accepted Manuscript Clinical tests to diagnose lumbar spondylolysis and spondylolisthesis: A systematic review Abdullah M. Alqarni, MPhty, Anthony G. Schneiders, PhD, Chad E. Cook, PhD, Doctor of Physical Therapy Program, Paul A. Hendrick, PhD PII: S1466-853X(15)00002-4 DOI: 10.1016/j.ptsp.2014.12.005 Reference: YPTSP 648 To appear in: Physical Therapy in Sport Received Date: 10 June 2014 Revised Date: 14 December 2014 Accepted Date: 31 December 2014 Please cite this article as: Alqarni, A.M., Schneiders, A.G., Cook, C.E., Hendrick, P.A., Clinical tests to diagnose lumbar spondylolysis and spondylolisthesis: A systematic review, Physical Therapy in Sports (2015), doi: 10.1016/j.ptsp.2014.12.005. This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Accepted Manuscript
Clinical tests to diagnose lumbar spondylolysis and spondylolisthesis: A systematicreview
Abdullah M. Alqarni, MPhty, Anthony G. Schneiders, PhD, Chad E. Cook, PhD,Doctor of Physical Therapy Program, Paul A. Hendrick, PhD
PII: S1466-853X(15)00002-4
DOI: 10.1016/j.ptsp.2014.12.005
Reference: YPTSP 648
To appear in: Physical Therapy in Sport
Received Date: 10 June 2014
Revised Date: 14 December 2014
Accepted Date: 31 December 2014
Please cite this article as: Alqarni, A.M., Schneiders, A.G., Cook, C.E., Hendrick, P.A., Clinical tests todiagnose lumbar spondylolysis and spondylolisthesis: A systematic review, Physical Therapy in Sports(2015), doi: 10.1016/j.ptsp.2014.12.005.
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service toour customers we are providing this early version of the manuscript. The manuscript will undergocopyediting, typesetting, and review of the resulting proof before it is published in its final form. Pleasenote that during the production process errors may be discovered which could affect the content, and alllegal disclaimers that apply to the journal pertain.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Clinical tests to diagnose lumbar spondylolysis and spondylolisthesis: A systematic review
Abdullah M. Alqarni (MPhty)
Department of Physiotherapy, King Abdul-Aziz University Hospital, Jeddah, Saudi Arabia.
Anthony G. Schneiders (PhD)
School of Human, Health and Social Sciences, Central Queensland University, Branyan,
Australia.
Chad E. Cook (PhD) Doctor of Physical Therapy Program, Duke University, Durham, USA.
Paul A. Hendrick (PhD) Division of Physiotherapy Education, University of Nottingham,
Nottingham, UK.
Corresponding author: A.G. Schneiders, Central Queensland University, University Drive,
Branyan, Queensland, Australia, 4670.
Tel: +61 7 41507007; fax: +61 7 41507080
E-mail address: [email protected]
Keywords: Systematic review, Diagnosis, Lumbar spine, Validity
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
1
Clinical tests to diagnose lumbar spondylolysis and spondylolisthesis: A systematic
review
ABSTRACT
The aim of this paper was to systematically review the diagnostic ability of clinical
tests to detect lumbar spondylolysis and spondylolisthesis.
A systematic literature search of six databases, with no language restrictions, from
1950 to 2014 was concluded on February 1, 2014. Clinical tests were required to be
compared against imaging reference standards and report, or allow computation, of
common diagnostic values.
The systematic search yielded a total of 5164 articles with 57 retained for full-text
examination, from which 4 met the full inclusion criteria for the review. Study
heterogeneity precluded a meta-analysis of included studies. Fifteen different clinical
tests were evaluated for their ability to diagnose lumbar spondylolisthesis and one
test for its ability to diagnose lumbar spondylolysis. The one-legged hyperextension
test demonstrated low to moderate sensitivity (50-73) and low specificity (17-32) to
diagnose lumbar spondylolysis, while the lumbar spinous process palpation test was
the optimal diagnostic test for lumbar spondylolisthesis; returning high specificity (87-
100) and mixed sensitivity (60-88) values.
Lumbar spondylolysis and spondylolisthesis are identifiable causes of LBP in athletes.
There appears to be utility to lumbar spinous process palpation for the diagnosis of
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
2
lumbar spondylolisthesis, however the one-legged hyperextension test has virtually no
value in diagnosing patients with spondylolysis.
1. INTRODUCTION
Lumbar spondylolysis and spondylolisthesis are established conditions in both
adolescent and adult populations and an identifiable cause of low back pain (LBP) in
athletes (Garet et al., 2013). The prevalence of lumbar spondylolysis differs in the
literature but has been estimated to be approximately 6–8% in the general
population by some authors (Wiltse and Rothman, 1989; Brooks et al., 2010), and
as high as 63% in those engaging in specific sporting activities (Rossi, 1988);
while the reported incidence of spondylolisthesis is suggested to comprise
between 2% to 6% of LBP populations (Magora 1976; Osterman et al., 1993).
Spondylolysis is characterised by a defect in the pars interarticularis which is
proposed to be either developmental or an acquired stress fracture secondary to
chronic low-grade trauma or repetitive loading (Leone et al., 2011) such as that can
occur in sport. Over time, stress concentration and accumulation can lead to a physis
stress fracture at the vertebral body diminishing the stabilising ability of the posterior
elements in the spinal segment and can progress to an isthmic spondylolisthesis
(Sairyo et al., 2006). A spondylolisthesis occurs when there is a bilateral pars
interarticularis defect and is often hallmarked by a forward slip of the superior
vertebrae on the inferior vertebrae (McNeely et al., 2003;Cavalier et al., 2006).
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
3
The Wiltse classification system (Wiltse et al., 1976) subdivides
spondylolisthesis into five aetiological categories; isthmic, dysplastic, degenerative,
traumatic, and pathological (Huijbregts, 2001). Of these categories, the degenerative
form is the most prevalent with isthmic spondylolisthesis more common in individuals
aged less than 50 years (Logroscino et al., 2001). Whereas the majority of individuals
with spondylolysis remain asymptomatic (Haun and Kettner, 2005), symptomatic
cases may present with considerable morbidity and result in focal low back pain.
Symptoms may radiate into the buttock or lower limb following incidental trauma or
intense athletic activities; most often associated with repeated extension and/or
rotation of the lumbar spine (Morita et al., 1994; Ralston, 1998; Standaert and
Herring, 2000; Standaert, 2002).
Other classification systems for spondylolisthesis define the grade of severity,
such as the commonly used Meyerding system (Ganju, 2002), which categorizes the
degree of vertebral slip using static lateral radiographs. Similar approaches, such as
the Boxall and Taillard method, use comparable slip assessment criteria (Taillard,
1954; Boxall et al, 1979). Each of these measures quantifies the severity of
spondylolisthesis and each implies the potential presence of instability.
A recent systematic review assessed the accuracy of tests to diagnose lumbar
instability and included tests utilised with both spondylolysis and spondylolisthesis
(Alqarni et al., 2011), however, these conditions do not always lead to lumbar
structural instability and current evidence suggests that translational instability
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
4
(structural instability) and spondylolisthesis represent differing and separate
aetiologies (Axelsson et al., 2000; McGregor et al., 2002). Translational instability is
defined as abnormal translation and/or rotation around the x-, y-, and z-axes of the
three-dimensional coordinates of the spine (Panjabi and White, 1978). The reported
cutoff values for vertebral translatory motion employed to diagnose the presence of
translational instability (structural instability) also remain somewhat contentious and
very between 3 to 5 mm in the literature (Knutsson, 1944; Shaffer et al., 1990; Hayes
at al., 1989).
A variety of diagnostic imaging methods are used to identify the presence of
spondylolysis, including plain-film imaging, computed tomography (CT), magnetic
resonance imaging (MRI), single photon emission computed tomography (SPECT) and
bone scintigraphy. SPECT has demonstrated the greatest sensitivity of the measures
with 10-12 times more contrast than bone scintigraphy (Harvey et al., 1998; Standaert
and Herring, 2000). Further estimates of the incidence of spondylolysis in the general
population range from 5.9% in the general population to 30% in select populations
(Sakai et al., 2010) with a reported prevalence of 11.5% in populations with CLBP
(Leonid et al., 2009). Since imaging is an imperfect science, linking the symptom
severity and the degree of anatomical or radiographic changes is challenging (Gibson
and Waddell, 2005). We cannot yet therefore determine the link between the levels of
morbidity and radiographic features.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
5
Spondylolisthesis is diagnosed radiographically through bone scintigraphy,
computed tomography (CT), magnetic resonance imaging (MRI), and lateral
radiographs in order to demonstrate a pars interarticularis defect and establish the
percentage of vertebral slippage in the absence of translation instability (Standaert
and Herring, 2000; Campbell et al.,2005). The North American Spine Society Clinical
Guidelines for Multidisciplinary Spine Care report (2008) designated lateral plain-film
radiographs and MRI as the most effective tools for diagnosis of spondylolisthesis with
stenosis, with CT-scan demonstrating effectiveness for patients in which MRI is
contraindicated. However, as with diagnosis of other low back-related conditions, a
high degree of false positives (imaging findings with poor correlation to clinical
symptoms) are present (Lurie, 2005).
Clinical examination findings, including specific orthopaedic tests offer
advantages as initial diagnostic indicators as they may expedite diagnosis and guide
initial management, while limiting the exposure of patients to the associated risks and
further costs of radiology (Alqarni et al., 2011). At present, there are few pre-clinical
indications that are specific to degenerative and asymptomatic lumbar
spondylolisthesis, whereas patients who are symptomatic complain primarily of
radiculopathy or neurogenic intermittent claudication with or without concomitant
back pain. While seminal signs and symptoms that are suggested to be associated with
spondylolysis and spondylolisthesis have been described in the literature (Barash et
al., 1970), it is important to note that these are not unique to spondylolysis and
spondylolisthesis and therefore the clinical diagnosis of these conditions based on
these signs and symptoms currently remains challenging.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
6
To our knowledge there have been no systematic reviews to date that have
investigated the accuracy of clinical tests to diagnose spondylolysis and
spondylolisthesis. Therefore, the aim of this paper was to systematically search and
review the literature relating to clinical tests specifically for the detection of
spondylolysis and spondylolisthesis in order to establish which tests have the best
accuracy and utility to diagnose these conditions. We planned to qualitatively report
the diagnostic accuracy of the clinical tests and describe the risk of bias of each
included study.
2. METHODS
2.1 Study Design
This systematic review used the Preferred Reporting Items for Systematic
Reviews and Meta-Analyses (PRISMA) guidelines throughout the research and
reporting process (Moher et al., 2009). The study was exempt from Human Ethics
Committee review.
2.2 Study Inclusion Criteria
Type of Studies: Prospective and retrospective case control and case-based study
designs were included in this review.
Type of Participants: For inclusion, at least one group of participants in the studies was
required to have been diagnosed with either spondylolisthesis or spondylolysis with
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
7
an acceptable reference standard. There were no restrictions with regards to age for
patients included in the studies.
Index Tests: The diagnostic accuracy of clinical tests associated with spondylolisthesis
or spondylolysis were required to be reported for inclusion in this review.
Targeted Conditions: At least one group of subjects in each study required a diagnosis
of the targeted conditions of spondylolisthesis or spondylolysis.
Reference Standard: The following reference standards were considered acceptable
for diagnosis of spondylolysis and/or spondylolisthesis; plain-film imaging, computed
tomography (CT), magnetic resonance imaging (MRI), single photon emission
computed tomography (SPECT) and bone scintigraphy.
Diagnostic Accuracy Measures: Each study was required to report or allow
computation of diagnostic values (sensitivity, specificity, positive & negative likelihood
ratios) for all clinical tests.
2.3 Search Strategy
Electronic Search: A comprehensive electronic search of the relevant literature was
concluded on February 1, 2014 in the following databases: CINHAL, PubMed,
MEDLINE, Scopus, AMED, and SPORTDiscus from 1950 to 2014. The following key
words/mesh terms were used in various combinations; lumbar spine,
spondylolisthesis, anterolisthesis, posterolisthesis, spondylolysis, validity, sensitivety,
specificity, diagnosis, clinical tests, provocation tests, and physical examination (Figure
1). No language restrictions were applied.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
8
Other Searches: The reference lists of all included articles were hand searched for
additional relevant references. Relevant grey literature was also accessed where
available as were references through review of the authors’ personal literature.
Selection of Studies: The first reviewer (A.M.A) evaluated the retrieved articles’ title
and abstract from the initial search, for possible inclusion. Two independent reviewers
(A.M.A & P.A.H) then assessed the retrieved titles for potential inclusion and retrieval
of the full text article. Full text articles were scrutinised independently for inclusion by
two reviewers (A.M.A & P.A.H). A third reviewer (A.G.S) was consulted if consensus
was unable to be reached. The reviewers were experienced Orthopaedic Manipulative
Physical Therapists, and as active researchers, were familiar with the literature and
therefore it was not possible to blind reviewers to the; authors, date of publication or,
journals in which the articles were published.
2.4 Data Extraction and Management
Data were extracted by one author (A.M.A) and was either placed in a 2 X 2
contingency table or, if the sensitivity, specificity and positive and negative likelihood
ratios (± LRs) were reported, the values were tabulated.
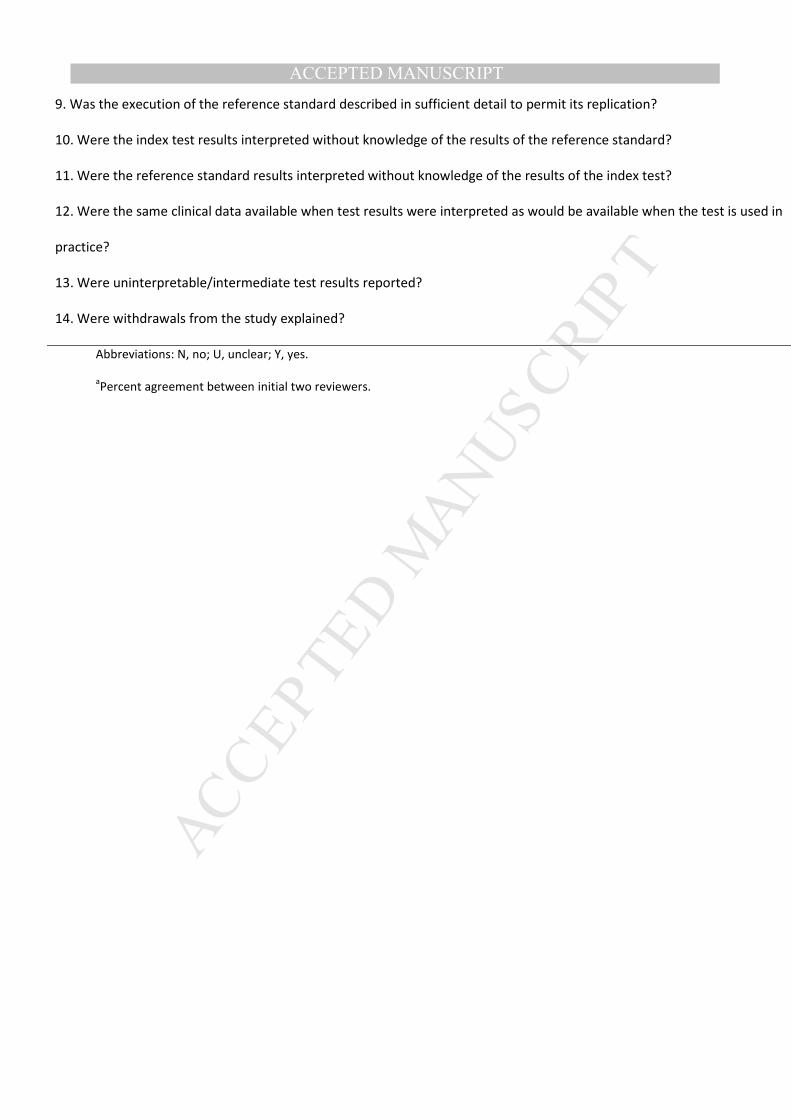
2.5 Quality Assessment
The Quality Assessment of Diagnostic Accuracy Studies (QUADAS) tool,
developed by Whiting et al. (2003) was used to assess the methodological quality of
included articles. The QUADAS tool consists of 14 items which are scored as either yes,
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
9
no or, unclear. Nine items specifically relate to bias, three items to the quality of
reporting, and two items relate to variability. To provide uniform interpretation of
each study and avoid quality assessment bias, the reviewers re-familiarised
themselves with the QUADAS prior to the evaluation, as all reviewers had
considerable experience in using the QUADAS, and a priori pre-piloting of the form for
calibration of assessors was not deemed necessary.Each of the 14 items were
independently scored either “yes”, “no” or, "unclear" by two reviewers (A.M.A &
A.G.S). In the case of any disagreement, a third reviewer (P.A.H) was consulted.
The original QUADAS tool did not initially incorporate a quality scoring system.
For this review, we used the methods proposed by the original developers (Whiting et
al.,2003). Quality was scored using item-weightings based and scaled for potential bias
or variation. Items 1, 5, 10, 11, and 12 were scored three points for “yes”, while items
3 and 6 were scored two for yes, and all other items (2, 4, 7, 8, 9, 13, and 14) scored
one point for yes. All items were scored zero if the response was “no”, or unable to be
determined (unclear); with a total possible score of 26. Studies were not stratified into
“high or low quality” using the QUADAS quality score, since it was estimated that the
number of articles retrieved during the review would be low, and as it is also
recognised that rating scores can potentially bias conclusions based on the quality of
diagnosis accuracy estimates and the weighting attributed to each item (Whiting et
al., 2005).
2.6 Statistical Analysis and Data Synthesis
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
10
To determine the accuracy with which each physical examination test
identifies each pathology and subsequently its clinical usefulness, sensitivity and
specificity and positive and negative likelihood ratios were calculated. Sensitivity is the
probability of a positive test result in someone with the pathology, whereas specificity
is the probability of a negative test result in someone without the pathology. The
taxonomy for descriptively characterizing magnitudes of sensitivity and specificity as
described by Schneiders et al., (2012) was used for this study and were classified as;
low if 50% or less, low to moderate if between 51% and 64%, moderate if between
65% and 74%, moderate to high if between 75% and 84%, and high if 85% or greater.
Both positive likelihood ratios (LR+) and negative likelihood ratios (LR-) were
calculated from the data provided from the sensitivity and specificity findings.
Positive likelihood ratios (LR+) greater than one (1) increase the post-test probability
that the target condition is present, and the higher the positive likelihood ratio the
greater this increase. Negative likelihood ratios (LR-) closer to 0 decreases the
probability of the target disorder with a negative finding, and the smaller the negative
likelihood ratio, the greater the decrease in probability (McCarthy et al., 2008). A
positive finding with a test that has a LR+ >10 generates a large change in post-test
probability, whereas a LR+ of 5-10 moderately influences post-test probability. A
negative finding with a test that has a LR- <0.1 generates a large shift in post-test
probability, whereas a LR- of 0.1-0.2 moderately shifts the pre to post-test probability
(Jaeschke et al., 1994). This study did not endeavour to perform a meta-analysis.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
11
3. RESULTS
3.1 Study Selection Results
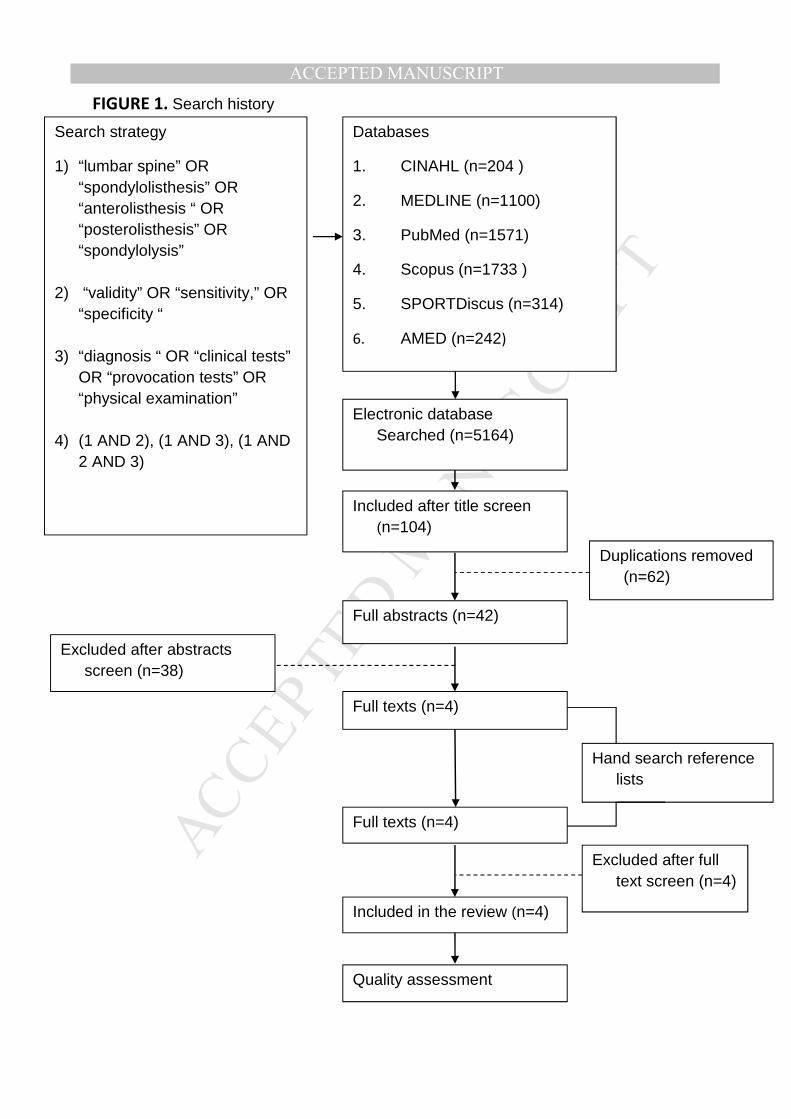
A total of 5164 articles resulted from the initial systematic literature search.
After title screening, 42 articles were selected for possible inclusion in the review and
after full text examination (Figure 1), 4 articles fulfilled all eligibility criteria.
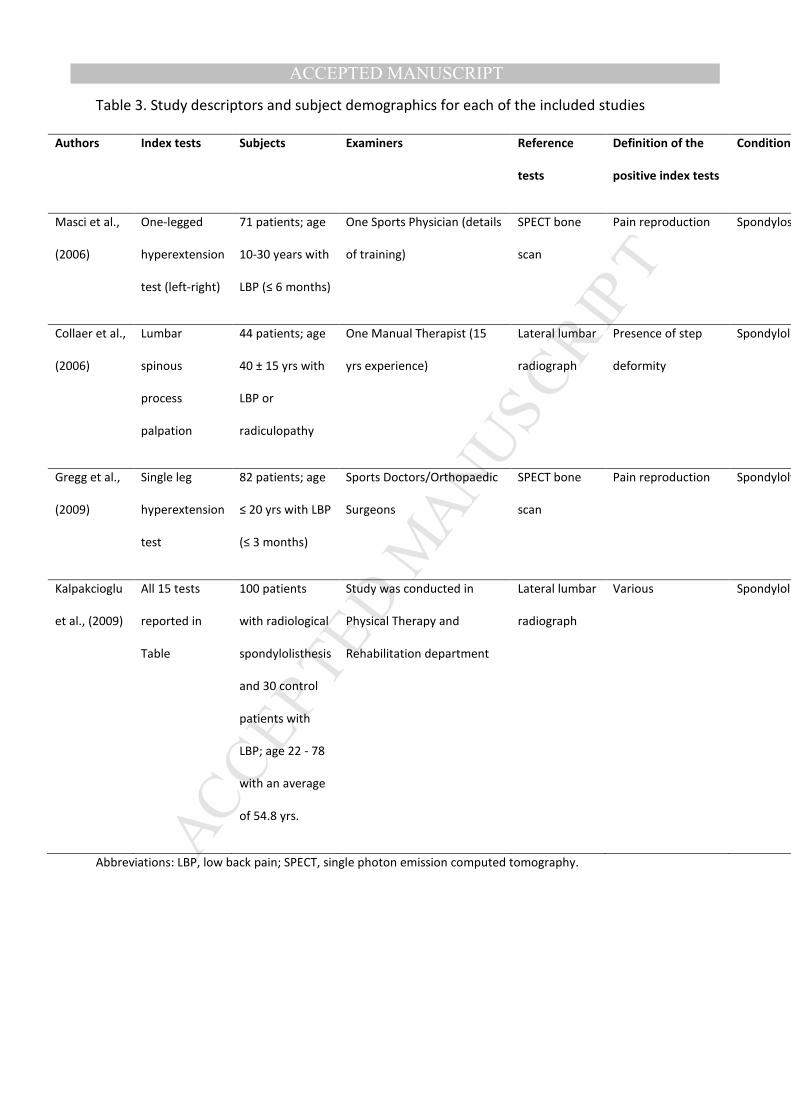
3.2 Study Characteristics
Two studies (Collaer et al., 2006; Kalpakcioglu et al., 2009) used lateral
radiographs as the reference standard for the differential diagnosis of a
spondylolisthesis and two studies (Masci et al.,2006; Gregg et al., 2009) used MRI and
SPECT to diagnose the presence of spondylolysis. A total of 15 different clinical tests
were evaluated for their ability to diagnose lumbar spondylolisthesis, and 1 test for its
ability to diagnose lumbar spondylolysis.
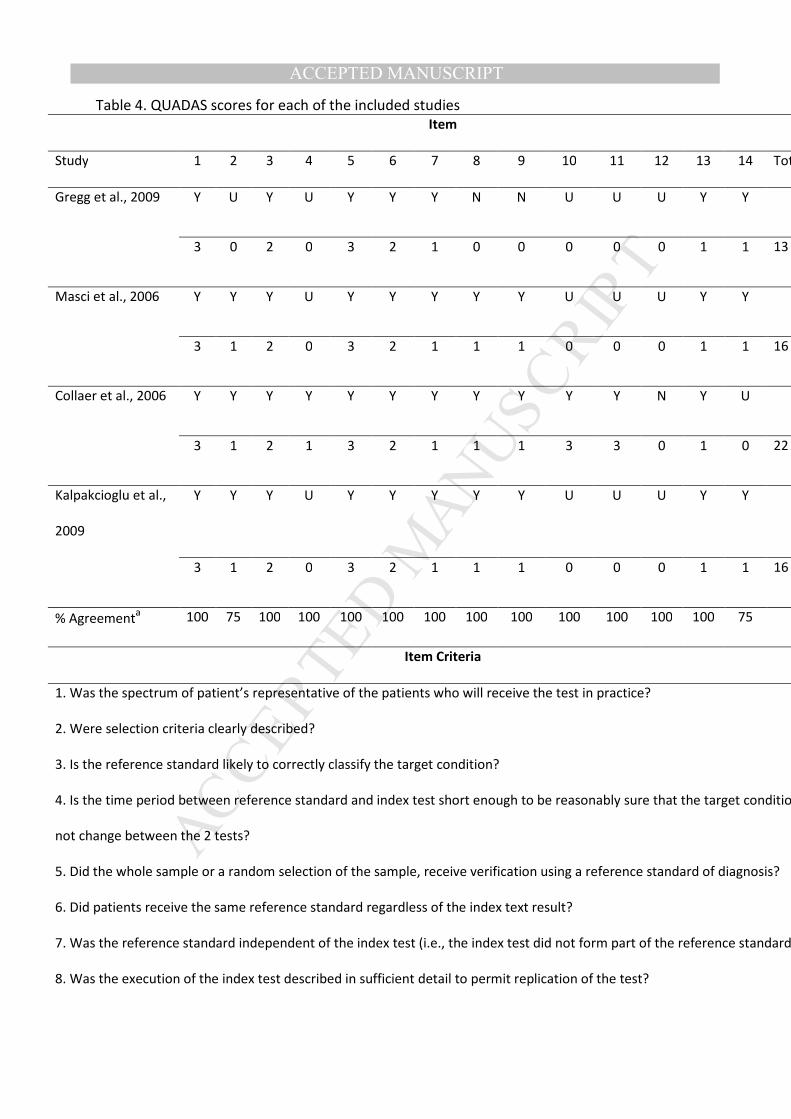
3.3 Risk of Bias Scores
The quality scores using the QUADAS tool for each item, total score, and the
percentage agreement between the two reviewers are presented in Table 4. All items
had an initial reviewer agreement of 100%, except clarity of selection criteria and
patient withdrawal from studies, where agreement was 75%. A third reviewer (P.A.H)
was consulted where agreement was not initially reached, resulting in the final scores
reported in Table 4. All articles satisfied the criterion that subjects in the studies
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
12
included the complete spectrum of patients representative of those whom would
normally be expected to receive the test in clinical practice (Whiting et al., 2003).
None of the included studies clarified whether the time period between the
performance of the reference standard and clinical test was short enough to be sure
that the target condition had not changed between the two tests (Whiting et al.,
2003). Subjects in all studies received the same diagnostic test regardless of the
clinical test result, and the diagnostic test was performed independent of the clinical
test results in all cases. Diagnostic and clinical tests were sufficiently described in all
included studies, except the study by Gregg et al. (2009) and all studies reported
uninterruptible test results. Blinding of assessors for the clinical testing procedures
and radiographic diagnosis of lumbar spondylolysis and spondylolisthesis was unclear
in all studies except the study by Collaer et al. (2006). None of the studies reported
whether interpretation of the radiological examination occurred without prior
knowledge of the clinical test results. Only one study (Collaer et al., 2006) did not
report on the reasons for patients’ withdrawal.
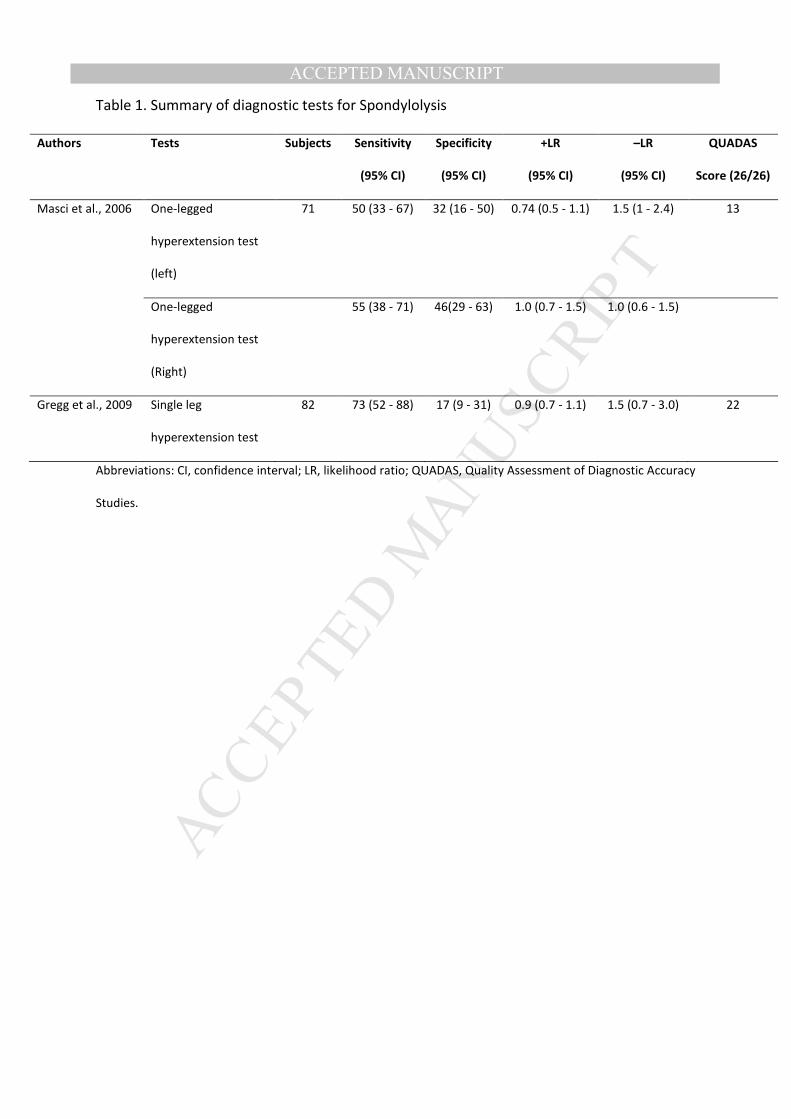
3.4 Tests for Spondylolysis
The one-legged hyperextension test was employed to diagnose lumbar
spondylolysis in a prospective cohort study of 71 patients with symptoms of recent
onset non-specific LBP recruited from a sports medicine clinic (Masci et al., 2006) and
a retrospective cohort of 82 patients with suspected spondylolysis recruited from a
medical facility that included a sports medicine centre and radiology clinic (Gregg et
al., 2009). The test was performed, as previously described by Jackson et al. (1981),
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
13
with the patient standing, facing away from the tester and each subject was then
asked to stand on his/her left leg and to raise his/her right leg with right hip slightly
flexed and right knee flexed to 80 degrees. Subjects were then asked to actively
extend their lumbar spine. Subjects repeated the test on the opposite side to compare
and record the symptom response. A positive result occurred when the patient
reported pain during this procedure. Masci and colleagues (2006) reported low
sensitivity, specificity, and +LR values for both sided tests; left leg (50%, 32%, 0.7),
right leg (55%, 46%, 1.0) for the diagnosis of spondylolysis confirmed by scintigraphy
(SPECT). Gregg et al. (2009) reported a sensitivity of 73% and specificity of 17% with a
+LR of 0.9, however it is unclear from this study which leg was used. Full study results
are presented in Table 1.
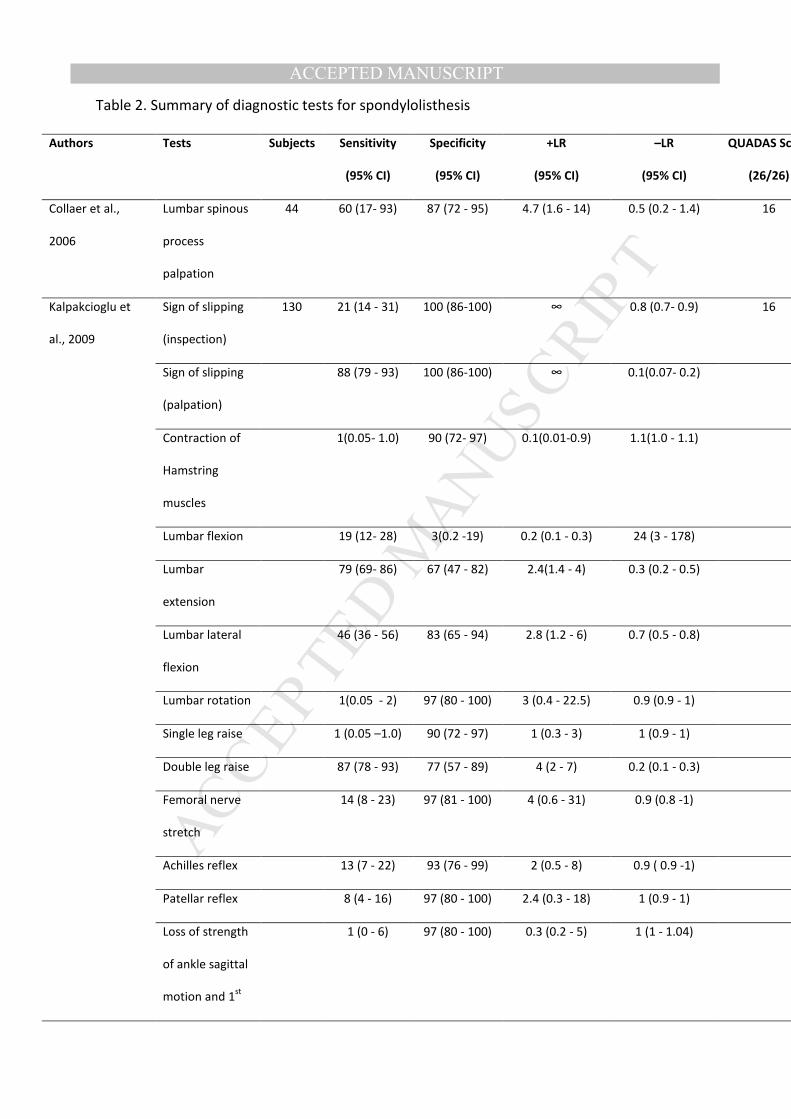
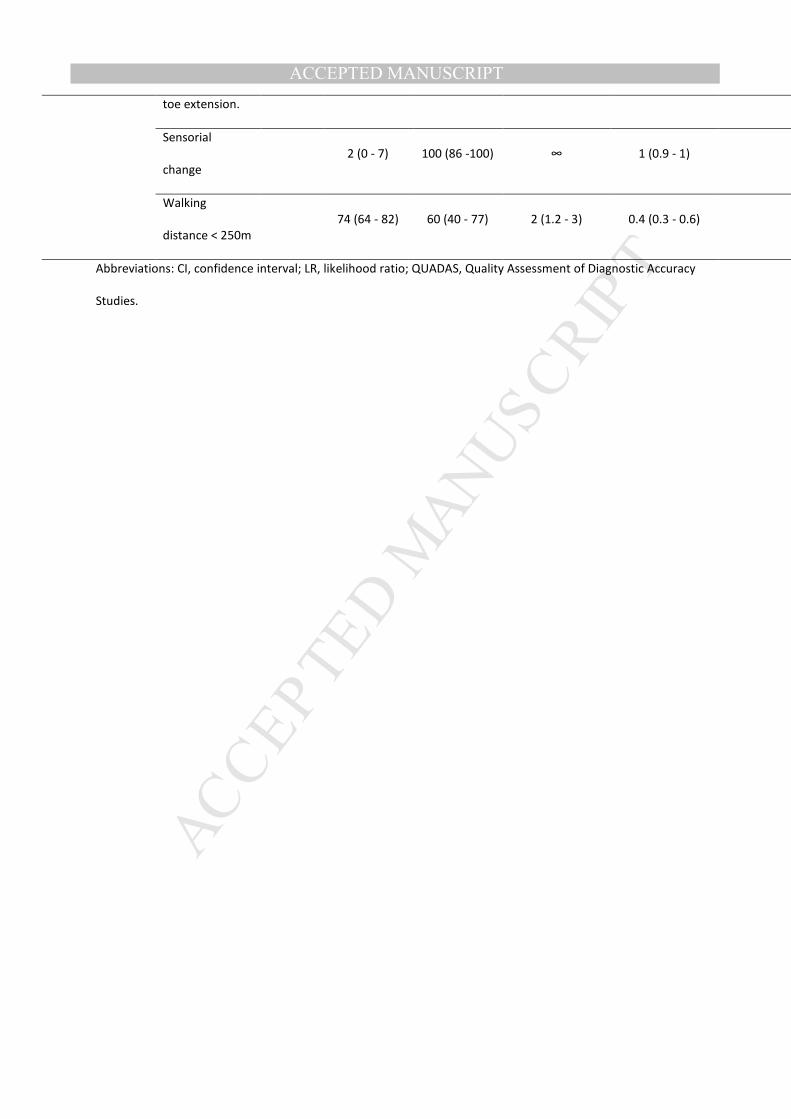
3.5 Tests for Spondylolisthesis
Table 2 outlines the 15 tests evaluated for their association with lumbar
spondylolisthesis. Lumbar spinous process palpation was investigated by Collaer et al.
(2006) in 44 patients with LBP and/or radiculopathy (mean age 40 yrs). The palpation
was performed with the examiner seated whilst maintaining a lateral view of the
patient’s lumbar spine. The palpation examination consisted of applying and
maintaining firm contact on the lumbosacral spinous processes, while sliding the
examining finger tips from the upper lumbar region to the sacrum for the presence or
absence of a lumbar spinous process “step”. Sensitivity, specificity, and +LR were
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
14
reported as 60%, 87%, and 4.6 respectively, for the diagnosis of lumbar
spondylolisthesis as confirmed on lateral radiographs.
Kalpakcioglu et al. (2009) compared the findings of lateral radiography and 15
clinical tests/signs within a cohort of 100 patients (mean age 54.8 yrs) with
radiologically confirmed lumbar spondylolisthesis and 30 patients (Table 3) without
radiological diagnosis of translational spondylolisthesis. The 15 tests (Table 2)
comprised; sign of slipping (inspection and palpation), contraction of the hamstring
muscles, lumbar flexion, extension, lateral flexion, and rotation, single and double leg
raise, femoral nerve stretch, Achilles and patellar reflexes, loss of strength of ankle
sagittal motion and first toe extension, sensorial change, and a walking distance <250
meters. Sensitivity values ranged from 1% for active lumbar rotation, active single leg
raise, lumbar spasm or pain on contraction of the hamstring muscles and, loss of
strength of ankle sagittal motion with first toe extension to 88% for a sign of slipping
on palpation. Specificity values ranged from 3% for active lumbar flexion to 100% for a
sign of slipping on inspection, a sign of slipping on palpation, and sensorial change.
Positive LRs were unable to be calculated from tests with 100% specificity (+LR = ∞).
4. DISCUSSION
The goals of this study were to investigate the diagnostic accuracy of clinical
tests to detect spondylolysis and spondylolisthesis. We evaluated studies that
investigated the clinical test’s diagnostic ability when compared to imaging reference
standards of bone scintigraphy (SPECT), computed tomography (CT), magnetic
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
15
resonance imaging (MRI), and lateral radiographs which are capable of demonstrating
the presence of a pars interarticularis defect or establishing the percentage of
vertebra slippage in the absence of translational instability. The majority of clinical
tests (n = 16) reviewed were utilised to diagnose lumbar spondylolisthesis, with only
one test found that had been evaluated for its specific ability to diagnose lumbar
spondylolysis. The large number of clinical tests associated with the assessment of
spondylolisthesis is due to Kalpakcioglu et al. (2009) investigating the diagnostic ability
of common assessment procedures which are often evaluated in LBP patients but are
not necessarily specific to pathology associated with spondylolisthesis. Our findings
suggest there is utility to lumbar spinous process palpation for the diagnosis of lumbar
spondylolisthesis whereas there are no tests that demonstrate clinical value when
diagnosing spondylolysis.
This review differs from the previous review by Alqarni et al. (2011), which
focused purely on a reference standard of radiographic translational instability.
Despite this separate focus, it is worth noting that there is strong evidence that
spondylolysis can induce spinal instability (Leone et al., 2011) and that some of the
individuals included in this review might have also have been diagnosed with lumbar
instability based on current clinical criteria. Although current evidence suggests that
translational instability and spondylolisthesis represent differing conditions (Axelsson
et al., 2000; McGregor et al., 2002), there is potential for these conditions to co-exist
and/or represent a progression on a clinical spectrum, thus affecting the utility and
diagnostic ability of the testing procedures for each of these conditions. The relatively
low diagnostic ability of the clinical tests from the review may also reflect the fact that
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
16
these conditions sit on a clinical spectrum with potential for a number of co-existing
pathologies dependent upon the aetiology of the condition and the age range of the
participants (Logroscino et al., 2001).
The one-legged hyperextension test was the single clinical test found which
was evaluated for its diagnostic ability to detect spondylolysis. The premise behind the
one-legged hyperextension test is that unilateral standing on the affected side and
hyperextension loads and stresses the posterior structures resulting in pain elicitation.
Based on low to high grading criteria for sensitivity and specificity conceived by
Schneiders et al. (2012); Gregg et al. (2009) reported moderate sensitivity but low
specificity, whereas, Masci et al. (2006) demonstrated low specificity, while sensitivity
for this test was low for the left leg, and low to moderate for the right leg. Differences
in selection criteria might have affected the sensitivity value in the study by Gregg et
al. (2009) which included patients who were already suspected of having lumbar
spondylolysis. Another possible factor for the higher sensitivity in the study by Gregg
et al. (2009) is the higher age range of participants. Masci and colleagues (2006)
included an age range of 10-30 years, excluding the potential for elderly patients with
possible degenerative lumbar spondylolysis. Despite these differences, and the
retrospective nature of Gregg et al.’s (2009) study, both studies reported similar and
very small +LRs (1.0), which suggests that one-legged hyperextension test has virtually
no value in diagnosing patients with spondylolysis.
Two studies evaluated a combined total of 16 clinical tests to diagnose lumbar
spondylolisthesis between them. Collaer et al. (2006) demonstrated the lowest risk of
bias of all the studies in this review and reported that the lumbar spinous process
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
17
palpation test (with the presence of step) had high specificity (87%), low to moderate
sensitivity (60%), and a moderate +LR (4.7) for the diagnosis of lumbar
spondylolisthesis. It is however important to note that these authors reported poor
inter-rater reliability (K: 0.18, 0.39, 0.31) for the lumbar spinous process palpation test
among the three pairs of examiners. Kalpakcioglu et al. (2009) examined the palpation
test’s ability to detect spondylolisthesis in a cohort of 100 patients with confirmed
radiological lumbar spondylolisthesis and compared them to 30 controls. They
reported high specificity (100%) and sensitivity (88%), however, the inclusion of
patients with confirmed spondylolisthesis would have inflated the sensitivity value
and such spectrum bias would inflate other diagnostic accuracy values. Despite these
potential methodological reservations, the authors of both studies indicated that
lumbar spinous process palpation might be an effective clinical test to diagnose
lumbar spondylolisthesis. Further study in wider spectrums of LBP populations is
required to validate these findings.
Other tests evaluated by Kalpakcioglu et al. (2009) also demonstrated potential
utility. A visual sign of slipping on inspection and the presence of sensory changes
(sciatalgia) demonstrated low sensitivity (21% & 2% respectively) but high specificity
(100%) to diagnose spondylolisthesis. The active double leg raise test also provided
high sensitivity (87%), and moderate to high specificity (77%), and a small but
sometimes important +LR value (4) to diagnose lumbar spondylolisthesis.The femoral
nerve stretch test demonstrated low sensitivity (14%), but high specificity (97%), with
a +LR of 4, and this could be due to the movement of the femoral nerve and/or the
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
18
movement in the spine during the testing procedure which stresses the lumbar spine
in extension.
Kalpakcioglu et al. (2009) also investigated a number of other active and
passive clinical tests that yielded poor utility in diagnosis of lumbar spondylolisthesis.
The lumbar extension test, lumbar lateral flexion test, and a test of walking distance
(<250m) all had respectively low to moderate/high sensitivities and specificities,
however, +LRs were small. The other common clinical tests (Table 2) had low
sensitivity, but high specificity and consequently small +LRs. Lumbar flexion also
showed no ability to diagnose lumbar spondylolisthesis with low sensitivity and
specificity, and very small +LR values.
It is acknowledged that the clinical tests evaluated in this review are routinely
performed in combination in clinical practice and also in conjunction with a thorough
subjective examination. However, the diagnostic capacity of combined clinical tests
has yet to be comprehensively evaluated and reported in the literature. It is also the
case that lumbar spondylolisthesis and spondylolysis often represent differing stages
of a progressive disorder and therefore symptomology and clinical signs may vary
dependent on where the patient sits on the clinical spectrum at a said point in time.
Further prospective research into the diagnostic ability of the clinical tests within
mixed cohorts of LBP patients is therefore warranted.
4.1 Limitations
The findings of this review are primarily limited by the small number of articles
that have reported on the accuracy of clinical tests to diagnose lumbar spondylolysis
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
19
and spondylolisthesis. The study sample sizes were also relatively small ranging from
44 to 130 patients (Table 3) which also may have affected the internal validity and
diagnostic accuracy of included studies. For this review the weighted QUADAS
assessment tool was used to assess the quality of included articles; however, the
QUADAS tool is suggested to have a number of associated limitations. These include
the possibility that even well-conducted studies may score poorly if the methods and
results of the study are not reported in sufficient detail, and that the tool does not
include items that assess statistical power which can subsequently affect a study’s
internal validity. In our assessment of quality, only 1 of the 4 papers evaluated yielded
a low risk of bias score. The reference standards used for both targeted diagnoses
demonstrate weaknesses in that findings are not always corrected with clinical
symptoms. Additionally, as stated, we targeted papers that did not use a translational
instability measure for a reference standard for spondylolysis and spondylolisthesis.
Despite this, and as stated previously, there is a chance that patients could
demonstrate instability that was not captured in the study.
This review is also limited due to a meta-analysis not being performed due to
the clinical heterogeneity of the studies. While Masci et al. (2006) and Gregg et al.
(2009) did appear to perform the same test (one-legged hyperextension test), one
study was prospective and the other retrospective and although Masci et al. reported
adequate raw data (true/false-positive/negatives) to allow a meta-analysis, Gregg et
al. did not. Additionally Gregg et al. was working with a limited data set for the one-
legged hyperextension test with only 44 of the 82 patient reports having sufficient
detail to determine the outcome of this test. Additionally, Masci et al. reported data
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
20
from both legs while Gregg reported only one set of data and it is therefore unclear
which leg contributed to the data set.
Limitations in test detail also retrospectively precluded meta-analysis of the
data for diagnosis of lumbar spondylolisthesis. While both Kalpakcioglu et al. (2009)
and Collaer et al. (2006) appeared to perform similar lumbar palpation techniques, the
test was not explained in sufficient detail in Kapakcioglu’s study to determine a
definite association. For instance, it is not clear if the test was performed in standing
or lying and what the outcome variable was (pain or displacement). An additional
problem when performing a metaanaylsis on these studies is that Kapakcioglu
reported 100% specificity as there were no true-negatives (0) in their cohort, which
meant a positive likelihood ratio approaching infinity. The resulting empty cell for
true-negatives poses additional problems for a meta-analysis where calculation is
impossible without inserting dummy variables into the equation. These clinical and
statistical heterogenity issues are suggested to limit the ability to confidently combine
the data of both tests in a meta-analysis. Future studies should be adequately
powered incorporating a broad spectrum of patients with and without the disorder
and a standardised and well-described clinical testing procedure. Additionally, a clear
and defined valid reference standard for diagnosis should be correlated independently
to the results of the clinical test. This would allow meta-synthesis of the results.
5. CONCLUSION
Spondylolysis and spondylolisthesis has a high prevalence in sporting and
athletic populations. This is the first systematic review to evaluate the accuracy of
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
21
clinical tests to diagnose patients with lumbar spondylolysis and spondylolisthesis that
used reference standard mechanisms that were not associated with translational
instability. There appears to be utility to lumbar spinous process palpation for the
diagnosis of lumbar spondylolisthesis, however the one-legged hyperextension test
has virtually no value in diagnosing patients with spondylolysis. To ensure the
reliability, validity and diagnostic accuracy of included clinical tests, further studies are
required, which have larger sample sizes, lower risks of bias, differing age ranges, and
different examiners.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
22
REFERENCES
Alqarni AM, Schneiders AG, Hendrick PA. Clinical Tests to Diagnose Lumbar Segmental
Instability: A Systematic Review. Journal of Orthopaedic & Sports Physical
Therapy 2011; 3(41): 130-40.
Axelsson P, Johnsson R, Strömqvist B. Is there increased intervertebral mobility in
Isthmic adult spondylolisthesis? A matched comparative study using roentgen
stereophotogrammetry. Spine 2000; 25(13):1701-3.
Barash HL, Galante JO, Lambert CN, Ray RD. Spondylolisthesis and tight hamstrings.
The Journal of Bone & Joint Surgery 1970; 52(7): 1319-28.
Boxall D, Bradford DS, Winter RB, Moe JH. Management of severe spondylolisthesis in
children and adolescents. The Journal of Bone & Joint Surgery 1979; 61: 479-
95.
Brooks BK, Southam SL, Mlady GW, Logan J, Rosett M. Lumbar spine spondylolysis
in the adult population: using computed tomography to evaluate the
possibility of adult onset lumbar spondylosis as a cause of back pain. Skeletal
Radiology 2010; 39(7): 669-73.
Campbell RS, Grainger AJ, Hide IG, Papastefanou S, Greenough CG. Juvenile
spondylolysis: a comparative analysis of CT, SPECT, and MRI. Skeletal Radiology
2005; 34: 63-73.
Cavalier R, Herman MJ, Cheung EV, Pizzutillo PD. Spondylolysis and
spondylolisthesis in children and adolescents: I. Diagnosis, natural history, and
nonsurgical management. Journal of the American Academy of Orthopaedic
Surgeons 2006; 14(7): 417-24.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
23
Collaer JW, McKeough DM, Boissonnault WC. Lumbar isthmic spondylolisthesis
detection with palpation: Interrater reliability and concurrent criterion-related
validity. The Journal of Manual & Manipulative Therapy 2006; 14(1): 22-9.
Fritz JM, Erhard RE, Hagen BF.Segmental instability of the lumbar spine. Physical
Therapy 1998; 78(8): 889-96.
Ganju A. Isthmic spondylolisthesis. Neurosurgical Focus 2002; 13(1):E1.
Garet, M., Reiman, M. P., Mathers, J., & Sylvain, J. (2013). Nonoperative Treatment in
Lumbar Spondylolysis and Spondylolisthesis A Systematic Review. Sports
Health: A Multidisciplinary Approach, 5(3), 225-232.
Gibson JN, Waddell G. Review Surgery for degenerative lumbar spondylosis: updated
Cochrane Review. Spine 2005; 30(20):2312-20.
Gregg CD, Dean S, Schneiders AG. Variables associated with active spondylolysis.
Physical Therapy in Sport 2009; 10: 121-4
Harvey C, Richenberg J, Saifuddin A, Wolman R: Pictoral review: The radiological
investigation of lumbar spondylolysis. Clinical Radiology 1998; 53: 723-8.
Haun D.W., Kettner N.W. Spondylolysis and spondylolisthesis: A narrative review of
etiology, diagnosis, and conservative management. Journal of Chiropractic
Medicine 2005; 4(4):206-17.
Hayes MA, Howard TC, Gruel CR, Kopta JA. Roentgenographic evaluation of lumbar
spine flexion-extension in asymptomatic individuals. Spine (Phila Pa 1976).
1989;14:327-331.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
24
Huijbregts PA. HSC 11.2.4. Lumbopelvic region: Aging, disease, examination,
diagnosis, and treatment. In: Wadsworth C, editor. HSC 11.2.Current Concepts
of Orthopaedic Physical Therapy. LaCrosse, Wl: Orthopaedic Section APTA;
2001.
Jackson D, Wiltse L, Dingeman R, Hayes M. Stress reactions involving the pars
interarticularis in young athletes. The American Journal of Sports Medicine
1981; 9:304-12.
Jaeschke R, Guyatt GH, Sackett DL. Users’ guides to the medical literature. III. How to
use an article about a diagnostic test. The Evidence-Based Medicine Working
Group. JAMA 1994;7(271):703-707.
Johnson R. Low back pain in sports: managing spondylolysis in young patients.
Physician and Sports Medicine 1993; 21: 53-9.
Kalpakcioglu B, Altinbilek T, Senel K. Determination of spondylolisthesis in low back
pain by clinical evaluation. Journal of Back and Musculoskeletal Rehabilitation
2009; 22(1):27-32.
Knutsson F. The instability associated with disk degeneration in the lumbar spine. Acta
Radiol. 1944;25:593-609
Leone A, Cianfoni A, Cerase A, Magarelli N, Bonomo L. Lumbar spondylolysis: a review.
Skeletal Radiology 2011; 40(6): 683-700.
Leonid K, Kim DH, Li L, Guermazi A, Berkin V, Hunter DJ. Spondylolysis and
spondylolisthesis: prevalence and association with low back pain in the adult
community-based population. Spine 2009; 34(2):199-205.
Logroscino G, Mazza O, Aulisa G, Pitta L, Pola E, Aulisa L. Spondylolysis and
spondylolisthesis in the pediatric and adolescent population. Childs Nervous
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
25
System 2001; 17(11):644-55.
Lurie JD. What diagnostic tests are useful for low back pain? Best Pract Res Clin
Rheumatol. 2005;19(4):557-75.
Magora A. Conservative treatment in spondylolithesis. Clinical Orthopaedics 1976;
117:74-79
Masci L, Pike L, Malara F, Phillips B, Bennell K, Brukner P. Use of the one-legged
hyperextension test and magnetic resonance image in the diagnosis of active
spondylolysis. British Journal of Sports Medicine 2006; 40: 940-6.
McCarthy CL, Wilson DJ, Coltman TP. Anterolateral ankle impingement: findings and
diagnostic accuracy with ultrasound imaging. Skeletal Radiol. 2008;37:209–
216.
McGregor AH, Anderton L, Gedroyc WM, Johnson J, Hughes SP. The use of
interventional open MRI to assess the kinematics of the lumbar spine in
patients with spondylolisthesis. Spine 2002; 27(14): 1582-6.
McNeely ML, Torrance G, Magee DJ. A systematic review of physiotherapy for
spondylolysis and spondylolisthesis. Manual Therapy 2003; 8: 80-91.
Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items
for systematic reviews and meta-analyses: The PRISMA statement. Physical
Therapy 2009; 89(9): 873-80.
Morita T, Ikata T, Katoh S. Pathogenesis of spondylolysis and spondylolisthesis in
young athletes based on a radiological and MRI study. North American Spine
Society/Japanese Spine Research Society Spine across the Sea meeting, Maui,
Hawai; 1994.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
26
North American Spine Society. Clinical Guidelines for Multidisciplinary Spine Care
Diagnosis and Treatment of Degenerative Lumbar Spondylolisthesis. 7075
Veterans Boulevard, Burr Ridge, IL 60527 USA: 2008.
Osterman K, Schlenzka D, Poussa M, Seitsalo S, Virta L. Isthmic spondylolisthesis in
symptomatic and asymptomatic subjects, epidemiology, and natural history
with special reference to disk abnormality and mode of treatment. Clinical
Orthopaedics and Related Research 1993; 297: 65-70.
Panjabi MM, White AA III. Physical properties and functional mechanics of the spine.
In: White AA III, Panjabi MM, editors. Clinical biomechanics of the spine.
Philadelphia, Pa: Lippincott; 1978. p. 1-60.
Ralston S. Suspecting lumbar spondylolysis in adolescent lumbar back pain.
Clinical Paediatrics 1998; 37:287-93.
Rossi F. Spondylolysis, spondylolisthesis and sports. Journal of Sports Medicine and
Physical Fitness 1988; 18:317-40.
Sairyo K, Goel VK, Masuda A, Vishnubhotla S, Faizan A, Biyani A, Ebraheim N, Yonekura
D, Murakami R, Terai T. Three dimensional finite element analysis of the
pediatric lumbar spine. II. Biomechanical change as the initiating factor for
pediatric isthmic spondylolisthesis at the growth plate. European Spine Journal
2006; 15(6): 930-5.
Sakai T, Sairyo K, Suzue N, Kosaka H, Yasui N. Incidence and etiology of lumbar
spondylolysis: review of the literature. Journal of orthopaedic science 2010;
15(3): 281-88.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
27
Schneiders AG, Sullivan SJ, Hendrick PA, Hones BD, McMaster AR, Sugden BA,
Tomlinson C. The ability of clinical tests to diagnose stress fractures: a
systematic review and meta-analysis. Journal of Orthopaedic & Sports Physical
Therapy 2012; 42(9):760-71.
Shaffer WO, Spratt KF, Weinstein J, Lehmann TR, Goel V. 1990 Volvo Award in clinical
sciences. The consistency and accuracy of roentgenograms for measuring
sagittal translation in the lumbar vertebral motion segment. An experimental
model. Spine (Phila Pa 1976). 1990;15:741-750.
Standaert DC, Herring S. Spondylolysis: A critical review. British Journal of Sports
Medicine 2000; 34:415-22.
Standaert DC. Practical management: Spondylolysis in the adolescent athlete. Clinical
Journal of Sports Medicine 2002; 12: 119-22.
Taillard W. Le spondylolisthesis chez l’enfant et l’adolescent. ActaOrthopaedica
Scandinavia 1954; 24: 115-44.
Whiting P, Harbord R, Kleijnen J. No role for quality scores in systematic reviews of
diagnostic accuracy studies. BMC Medical Research Methodology 2005; 5:19.
Whiting P, Rutjes AW, Reitsma JB, Bossuyt PM, Kleijnen J. The development of
QUADAS: A tool for the quality assessment of studies of diagnostic accuracy
included in systematic reviews. BMC Medical Research Methodology 2003;
3:25.
Wiltse LL, Newman PH, Macnab I. Classification of Spondylolysis and
Spondylolisthesis. Clinical Orthopaedics and Related Research 1976; 117: 23-9.
Wiltse LL, Rothman SLG. Spondylolisthesis: Classification, diagnosis and natural
history. Seminar in Spine Surgery 1989; 1: 78-94.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
28
FIGURE 1. Search history
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
29
Table 1. Summary of diagnostic tests for Spondylolysis

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
30
Table 2. Summary of diagnostic tests for spondylolisthesis

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
31
Table 3. Study descriptors and subject demographics for each of the included studies

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
32
Table 4. QUADAS scores for each of the included studies
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Table 1. Summary of diagnostic tests for Spondylolysis
Authors Tests Subjects Sensitivity
(95% CI)
Specificity
(95% CI)
+LR
(95% CI)
–LR
(95% CI)
QUADAS
Score (26/26)
Masci et al., 2006 One-legged
hyperextension test
(left)
71 50 (33 - 67) 32 (16 - 50) 0.74 (0.5 - 1.1) 1.5 (1 - 2.4) 13
One-legged
hyperextension test
(Right)
55 (38 - 71) 46(29 - 63) 1.0 (0.7 - 1.5) 1.0 (0.6 - 1.5)
Gregg et al., 2009 Single leg
hyperextension test
82 73 (52 - 88) 17 (9 - 31) 0.9 (0.7 - 1.1) 1.5 (0.7 - 3.0) 22
Abbreviations: CI, confidence interval; LR, likelihood ratio; QUADAS, Quality Assessment of Diagnostic Accuracy
Studies.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Table 2. Summary of diagnostic tests for spondylolisthesis
Authors Tests Subjects Sensitivity
(95% CI)
Specificity
(95% CI)
+LR
(95% CI)
–LR
(95% CI)
QUADAS Score
(26/26)
Collaer et al.,
2006
Lumbar spinous
process
palpation
44 60 (17- 93) 87 (72 - 95) 4.7 (1.6 - 14) 0.5 (0.2 - 1.4) 16
Kalpakcioglu et
al., 2009
Sign of slipping
(inspection)
130 21 (14 - 31) 100 (86-100) ∞ 0.8 (0.7- 0.9) 16
Sign of slipping
(palpation)
88 (79 - 93) 100 (86-100) ∞ 0.1(0.07- 0.2)
Contraction of
Hamstring
muscles
1(0.05- 1.0) 90 (72- 97) 0.1(0.01-0.9) 1.1(1.0 - 1.1)
Lumbar flexion 19 (12- 28) 3(0.2 -19) 0.2 (0.1 - 0.3) 24 (3 - 178)
Lumbar
extension
79 (69- 86) 67 (47 - 82) 2.4(1.4 - 4) 0.3 (0.2 - 0.5)
Lumbar lateral
flexion
46 (36 - 56) 83 (65 - 94) 2.8 (1.2 - 6) 0.7 (0.5 - 0.8)
Lumbar rotation 1(0.05 - 2) 97 (80 - 100) 3 (0.4 - 22.5) 0.9 (0.9 - 1)
Single leg raise 1 (0.05 –1.0) 90 (72 - 97) 1 (0.3 - 3) 1 (0.9 - 1)
Double leg raise 87 (78 - 93) 77 (57 - 89) 4 (2 - 7) 0.2 (0.1 - 0.3)
Femoral nerve
stretch
14 (8 - 23) 97 (81 - 100) 4 (0.6 - 31) 0.9 (0.8 -1)
Achilles reflex 13 (7 - 22) 93 (76 - 99) 2 (0.5 - 8) 0.9 ( 0.9 -1)
Patellar reflex 8 (4 - 16) 97 (80 - 100) 2.4 (0.3 - 18) 1 (0.9 - 1)
Loss of strength
of ankle sagittal
motion and 1st
1 (0 - 6) 97 (80 - 100) 0.3 (0.2 - 5) 1 (1 - 1.04)
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTtoe extension.
Sensorial
change
2 (0 - 7) 100 (86 -100) ∞ 1 (0.9 - 1)
Walking
distance < 250m
74 (64 - 82) 60 (40 - 77) 2 (1.2 - 3) 0.4 (0.3 - 0.6)
Abbreviations: CI, confidence interval; LR, likelihood ratio; QUADAS, Quality Assessment of Diagnostic Accuracy
Studies.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Table 3. Study descriptors and subject demographics for each of the included studies
Authors Index tests Subjects Examiners Reference
tests
Definition of the
positive index tests
Condition
Masci et al.,
(2006)
One-legged
hyperextension
test (left-right)
71 patients; age
10-30 years with
LBP (≤ 6 months)
One Sports Physician (details
of training)
SPECT bone
scan
Pain reproduction Spondylosis
Collaer et al.,
(2006)
Lumbar
spinous
process
palpation
44 patients; age
40 ± 15 yrs with
LBP or
radiculopathy
One Manual Therapist (15
yrs experience)
Lateral lumbar
radiograph
Presence of step
deformity
Spondylolisthesis
Gregg et al.,
(2009)
Single leg
hyperextension
test
82 patients; age
≤ 20 yrs with LBP
(≤ 3 months)
Sports Doctors/Orthopaedic
Surgeons
SPECT bone
scan
Pain reproduction Spondylolysis
Kalpakcioglu
et al., (2009)
All 15 tests
reported in
Table
100 patients
with radiological
spondylolisthesis
and 30 control
patients with
LBP; age 22 - 78
with an average
of 54.8 yrs.
Study was conducted in
Physical Therapy and
Rehabilitation department
Lateral lumbar
radiograph
Various Spondylolisthesis
Abbreviations: LBP, low back pain; SPECT, single photon emission computed tomography.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Table 4. QUADAS scores for each of the included studies
Item
Study 1 2 3 4 5 6 7 8 9 10 11 12 13 14 Total
Gregg et al., 2009 Y U Y U Y Y Y N N U U U Y Y
3 0 2 0 3 2 1 0 0 0 0 0 1 1 13
Masci et al., 2006 Y Y Y U Y Y Y Y Y U U U Y Y
3 1 2 0 3 2 1 1 1 0 0 0 1 1 16
Collaer et al., 2006 Y Y Y Y Y Y Y Y Y Y Y N Y U
3 1 2 1 3 2 1 1 1 3 3 0 1 0 22
Kalpakcioglu et al.,
2009
Y Y Y U Y Y Y Y Y U U U Y Y
3 1 2 0 3 2 1 1 1 0 0 0 1 1 16
% Agreementa 100 75 100 100 100 100 100 100 100 100 100 100 100 75
Item Criteria
1. Was the spectrum of patient’s representative of the patients who will receive the test in practice?
2. Were selection criteria clearly described?
3. Is the reference standard likely to correctly classify the target condition?
4. Is the time period between reference standard and index test short enough to be reasonably sure that the target condition did
not change between the 2 tests?
5. Did the whole sample or a random selection of the sample, receive verification using a reference standard of diagnosis?
6. Did patients receive the same reference standard regardless of the index text result?
7. Was the reference standard independent of the index test (i.e., the index test did not form part of the reference standard
8. Was the execution of the index test described in sufficient detail to permit replication of the test?
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
9. Was the execution of the reference standard described in sufficient detail to permit its replication?
10. Were the index test results interpreted without knowledge of the results of the reference standard?
11. Were the reference standard results interpreted without knowledge of the results of the index test?
12. Were the same clinical data available when test results were interpreted as would be available when the test is used in
practice?
13. Were uninterpretable/intermediate test results reported?
14. Were withdrawals from the study explained?
Abbreviations: N, no; U, unclear; Y, yes.
aPercent agreement between initial two reviewers.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
FIGURE 1. Search history
Search strategy
1) “lumbar spine” OR “spondylolisthesis” OR “anterolisthesis “ OR “posterolisthesis” OR “spondylolysis”
2) “validity” OR “sensitivity,” OR
“specificity “ 3) “diagnosis “ OR “clinical tests”
OR “provocation tests” OR “physical examination”
4) (1 AND 2), (1 AND 3), (1 AND
2 AND 3)
Databases
1. CINAHL (n=204 )
2. MEDLINE (n=1100)
3. PubMed (n=1571)
4. Scopus (n=1733 )
5. SPORTDiscus (n=314)
6. AMED (n=242)
7. EMBASE (n=2427)
Electronic database Searched (n=5164)
Included after title screen (n=104)
Full abstracts (n=42)
Full texts (n=4)
Full texts (n=4)
Included in the review (n=4)
Quality assessment
Excluded after abstracts screen (n=38)
Hand search reference lists
Excluded after full text screen (n=4)
Duplications removed (n=62)
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
• Lumbar spondylolysis and spondylolisthesis are identifiable causes of LBP in athletes
• This paper is the first to systematically review clinical tests to diagnose lumbar
spondylolysis and spondylolisthesis
• Fifteen clinical tests were retrieved that had been studied to diagnose lumbar
spondylolisthesis and lumbar spondylolysis
• The one-legged hyperextension test demonstrated low to moderate sensitivity and
low specificity to diagnose spondylolysis
• Lumbar spinous process palpation had high specificity and was the optimal
diagnostic test for lumbar spondylolisthesis
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Source of Support: No specific and/or direct funding was received for this study
Conflict of Interest: Dr A.G Schneiders, the second and corresponding author, is an associate
editor of the journal, Physical Therapy in Sport.
Related Documents











