“CLINICAL STUDY ON ORBITAL SPACE OCCUPYING LESIONS” DISSERTATION SUBMITTED TO THE TAMILNADU DR.M.G.R. MEDICAL UNIVERSITY CHENNAI in partial fulfillment of the requirements for the degree of M.S (OPHTHALMOLOGY) Registration No.: 221713253 (BRANCH-III) TIRUNELVELI MEDICAL COLLEGE TIRUNELVELI MAY - 2020

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
“CLINICAL STUDY ON ORBITAL SPACE OCCUPYING LESIONS”
DISSERTATION SUBMITTED TO
THE TAMILNADU DR.M.G.R. MEDICAL UNIVERSITY
CHENNAI
in partial fulfillment of
the requirements for the degree of
M.S (OPHTHALMOLOGY)
Registration No.: 221713253
(BRANCH-III)
TIRUNELVELI MEDICAL COLLEGE
TIRUNELVELI
MAY - 2020
CERTIFICATE BY THE GUIDE
This is to certify that this dissertation titled “CLINICAL STUDY ON ORBITAL
SPACE OCCUPYING LESIONS” submitted by DR.V.THENDRAL to the
Tamilnadu Dr.M.G.R Medical university, Chennai, in partial fulfilment of the
requirement for the award of the MS degree (Branch III) in ophthalmology during the
academic period of 2017-2020 is an original bonafide research work carried out by her
under my direct supervision and guidance. I forward this to the Tamil Nadu
Dr.M.G.R. Medical University, Chennai, Tamil Nadu, India
Place: Tirunelveli
Date:
DR.M.RITA HEPSI RANI M.S., D.N.B., FAICO.,Assistant Professor
Department of Ophthalmology,Tirunelveli Medical College
Tirunelveli
CERTIFICATE BY THE HEAD OF THE DEPARTMENT
This is to certify that the dissertation entitled “CLINICAL STUDY ON ORBITAL
SPACE OCCUPYING LESIONS” is a bonafide and genuine research work carried
out by Dr.V.THENDRAL under the guidance and supervision of DR.M.RITA
HEPSI RANI M.S., D.N.B., FAICO., Assistant professor, Department of
Ophthalmology, Tirunelveli Medical College, Tirunelveli in the Department of
Ophthalmology, Tirunelveli Medical college, Tirunelveli, in partial fulfilment of the
requirements for the degree of M.S in Ophthalmology.
Date:
Place: Tirunelveli
DR.V.RAMALAKSHMI, M.S.,Professor & Head of the Department
Department of Ophthalmology,Tirunelveli Medical College
Tirunelveli
CERTIFICATE BY THE DEAN
I hereby certify that the dissertation entitled “A STUDY OF BEHAVIOURAL
PROBLEMS IN CHILDREN WITH HISTORY OF FEBRILE CONVULSION”
is a bonafide and genuine research work carried out by Dr.V.THENDRAL under the
guidance and supervision of DR.M.RITA HEPSI RANI M.S., D.N.B., FAICO.,
Assistant professor, Department of Ophthalmology, Tirunelveli Medical College,
Tirunelveli in the Department of Ophthalmology, Tirunelveli Medical college,
Tirunelveli, during his postgraduate degree course period from 2017-2020 in partial
fulfilment of the requirements for the degree of M.S in Ophthalmology. This work has
not formed the basis for previous award of any degree.
Date :
Place : TIRUNELVELI
Prof.Dr. S. M.KANNAN,M.S., MCh.,(Uro)The DEAN
Tirunelveli Medical College,Tirunelveli - 627011.
DECLARATION BY THE CANDIDATE
I solemnly declare that this dissertation titled “CLINICAL STUDY ON
ORBITAL SPACE OCCUPYING LESIONS” is a bonafide and genuine research
work carried out by me under the guidance and supervision of DR.M.RITA HEPSI
RANI M.S., D.N.B., FAICO., Assistant Professor, Department of ophthalmology,
Tirunelveli medical college, Tirunelveli.
Place : Tirunelveli
Date :
Dr. V.THENDRAL,Registration No.: 221713253
Post Graduate Student,Department of OphthalmologyTirunelveli Medical College,
Tirunelveli.
ACKNOWLEDGEMENT
I express my sincere gratitude and thanks to The Dean, Tirunelveli Medical
college, Tirunelveli, for providing all the facilities to conduct this study.
I sincerely thank Dr.V.Ramalakshmi, M.S., professor and HOD, For her
valuable advice, comments and constant encouragement for the completion of
this study.
I am highly thankful to Dr.M.Rita Hepsi Rani M.S., D.N.B., FAICO., Assistant
professor, Department of ophthalmology, TVMCH, for her valuable guidance
throughout the study.
I am thankful to Dr. Anandhi. D, M.S., D.O., F.I.C.O., Assistant professors,
Department of ophthalmology, TVMCH who helped me by offering their
valuable suggestions and for being with me throughout the study.
My special thanks to my Co-postgraduate colleagues Dr.M.Chandralekha,
Dr.V.C. Gitanjali, Dr. S. Tinustefi for their help and immense support.
I thank Dr.V.Arumugam M.D., DM., HOD of Oncology, Dr.R.Deivanaygam
MD., DM., HOD of Radiotherapy, Dr.K.Santharaman M.D., HOD of
Pathology, DR. S.Suresh Kumar MS., DLO., HOD of ENT., for their
immense support.
I thank all those patients who participated in the study, who made this study
possible.
I am also thankful to my beloved family and friends for giving me constant
support and encouragement.
CERTIFICATE – II
This is certify that this dissertation work title “CLINICAL STUDY ON
ORBITAL SPACE OCCUPYING LESIONS” of the candidate
Dr.V.THENDRAL with registration Number 221713253 is for the award of
M.S. Degree in the branch of OPHTHALMOLOGY (III). I personally verified
the urkund.com website for the purpose of plagiarism check. I found that the
uploaded thesis file contains from introduction to conclusion page and result
shows 16 percentage of plagiarism in the dissertation.
Guide & Supervisor sign with Seal.
CONTENTS
S.NO TITLE PAGE NO
1 INTRODUCTION 1
2 AIM OF THE STUDY 56
3 MATERIALS AND METHODS 57
4 REVIEW OF LITERATURE 58
5 RESULTS 62
6 DISCUSSION 74
7 CONCLUSION 78
BIBILIOGRAPHY
PROFORMA
MASTER CHART
List of Charts
Figure 1 Age wise sex distribution
Figure 2 Laterality
Figure 3 Involvement of Right eye and Left eye
Figure 4 Presenting complaints
Figure 5 visual acuity
Figure 6 Origin of IOSOL
Figure 7 Location of IOSOL
Figure 8 Age distribution in benign and malignant tumour
Figure 9 Type of proptosis
Figure 10 Nature of tumour
Figure 11 Type of IOSOL
Figure 12 Diagnosis of benign tumour
Figure 13 Diagnosis of malignant tumour
Figure 14 Treatment Modality
Figure 15 Kaplan – Meier Survival Analysis
ABBREVATIONS
RE-Right eye
LE- Left eye
IOSOL- Intra orbital space occupying lesions
SOF-Superior orbital fissure
DLCL – Diffuse large cell lymphoma
CLL- Chronic lymphoid leukemia
CT- Computed tomography
MRI-Magnetic resonance imaging
EBRT-External beam radiotherapy
R-CHOP- Rituximab , Cyclophosphamide , Oncovin , Prednisolone
VEC- Vincristine , Etoposide , Carboplatin
1
1.INTRODUCTION
Space-occupying lesions, both benign and malignant, cause significant functional
and anatomical problems. Intra orbital space occupying lesions can result in
double vision, exophthalmos, ptosis, loss of vision, limited action of extraocular
movements and even permanent visual loss. Orbital lesions can be diagnosed by
radiological examinations such as Magnetic Resonance Imaging (MRI) and
Computed Tomography (CT) but definite diagnosis is mostly obtained by
histopathological examination of the removed mass . CT provides useful
information about the relationship of the mass with the orbital bones, intralesional
calcifications and other orbital structures . MRI provides more detailed
information about the morphology of the soft tissue masses, their relationship to
the orbital tissues and their borders .
2.ANATOMY OF THE ORBIT AND PARANASAL SINUS
Dimension of the orbit
Orbital wall
Apertures
Soft Tissues
Periorbital Structures- paranasal sinuses
2
Orbit resembles a quadrilateral pyramid . The capacity of orbit is 30 ml of
which eye ball constitutes 6.5ml[1] .It has medial wall , lateral wall , roof and
floor .
DIMENSIONS[1]
Volume 30cm3
Entrance Width 40-45mm
Entrance height 35mm
Medial wall length 40-45mm
Distance between the posterior globe
to optic foramen
18mm
Length of optic nerve in orbital portion 25-30mm
3
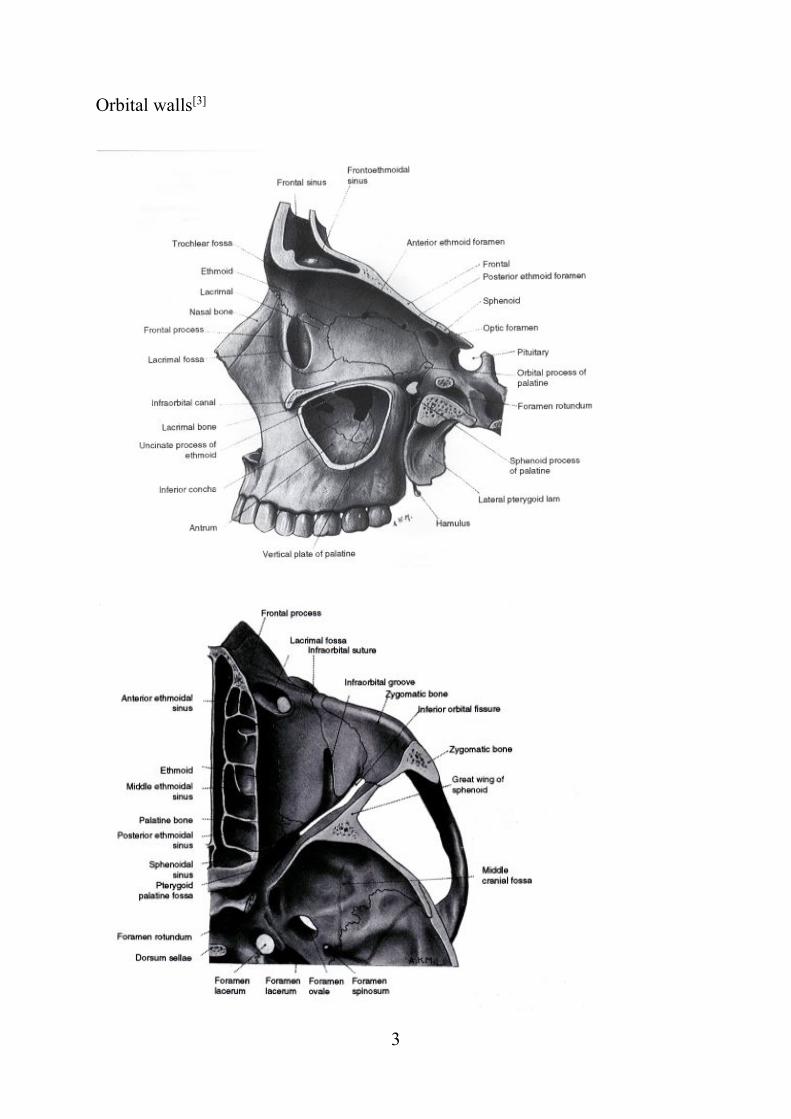
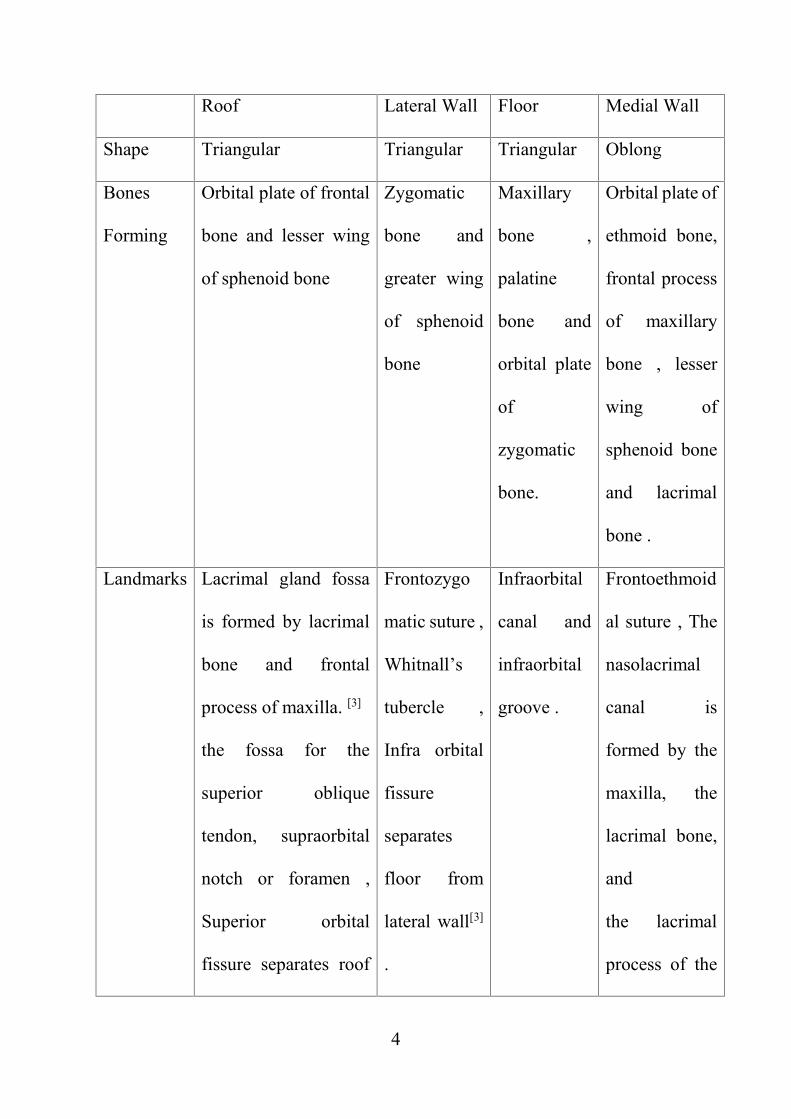
Orbital walls[3]
4
Roof Lateral Wall Floor Medial Wall
Shape Triangular Triangular Triangular Oblong
Bones
Forming
Orbital plate of frontal
bone and lesser wing
of sphenoid bone
Zygomatic
bone and
greater wing
of sphenoid
bone
Maxillary
bone ,
palatine
bone and
orbital plate
of
zygomatic
bone.
Orbital plate of
ethmoid bone,
frontal process
of maxillary
bone , lesser
wing of
sphenoid bone
and lacrimal
bone .
Landmarks Lacrimal gland fossa
is formed by lacrimal
bone and frontal
process of maxilla. [3]
the fossa for the
superior oblique
tendon, supraorbital
notch or foramen ,
Superior orbital
fissure separates roof
Frontozygo
matic suture ,
Whitnall’s
tubercle ,
Infra orbital
fissure
separates
floor from
lateral wall[3]
.
Infraorbital
canal and
infraorbital
groove .
Frontoethmoid
al suture , The
nasolacrimal
canal is
formed by the
maxilla, the
lacrimal bone,
and
the lacrimal
process of the
5
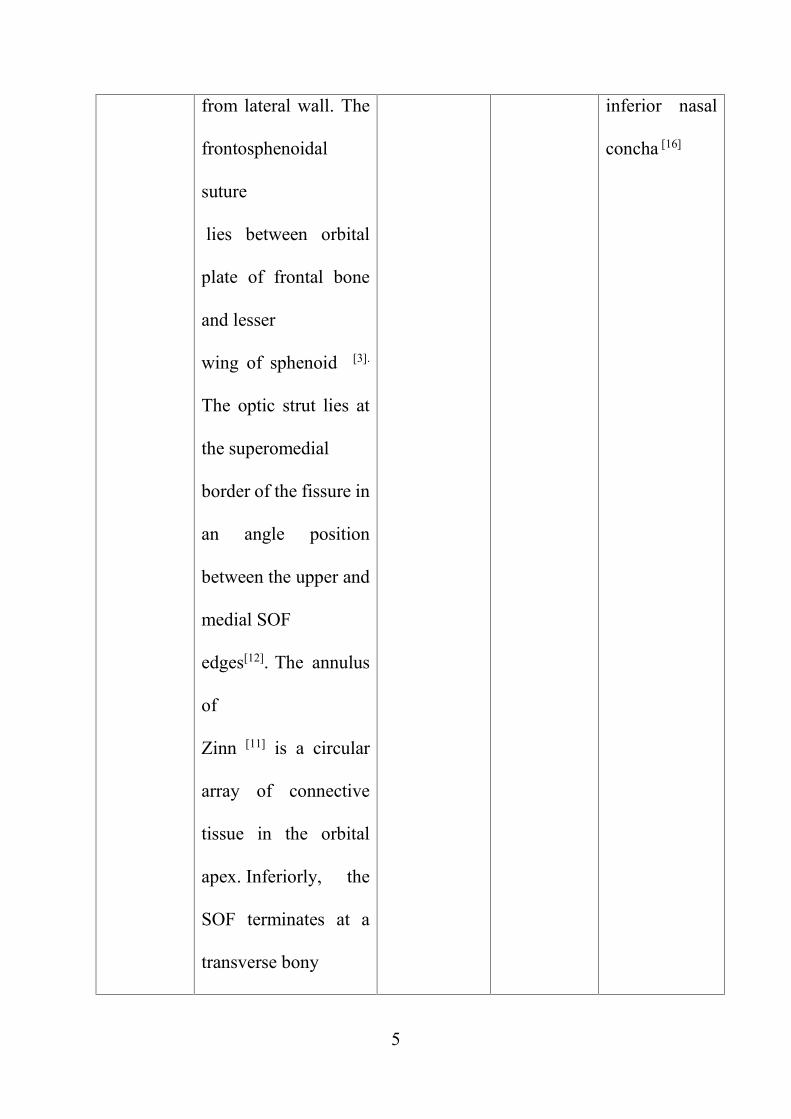
from lateral wall. The
frontosphenoidal
suture
lies between orbital
plate of frontal bone
and lesser
wing of sphenoid [3].
The optic strut lies at
the superomedial
border of the fissure in
an angle position
between the upper and
medial SOF
edges[12]. The annulus
of
Zinn [11] is a circular
array of connective
tissue in the orbital
apex. Inferiorly, the
SOF terminates at a
transverse bony
inferior nasal
concha [16]
6
confluence above the
foramen rotundum,
which is referred to as
maxillary
strut. [13][14][15]
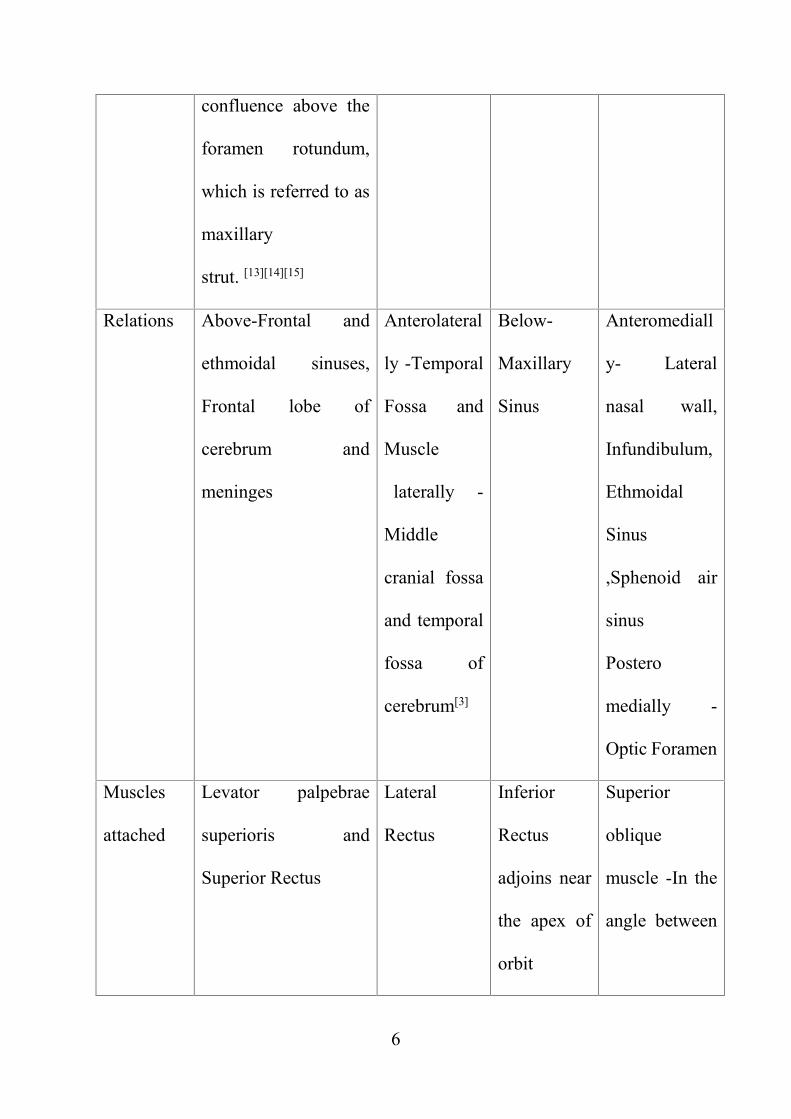
Relations Above-Frontal and
ethmoidal sinuses,
Frontal lobe of
cerebrum and
meninges
Anterolateral
ly -Temporal
Fossa and
Muscle
laterally -
Middle
cranial fossa
and temporal
fossa of
cerebrum[3]
Below-
Maxillary
Sinus
Anteromediall
y- Lateral
nasal wall,
Infundibulum,
Ethmoidal
Sinus
,Sphenoid air
sinus
Postero
medially -
Optic Foramen
Muscles
attached
Levator palpebrae
superioris and
Superior Rectus
Lateral
Rectus
Inferior
Rectus
adjoins near
the apex of
orbit
Superior
oblique
muscle -In the
angle between
7
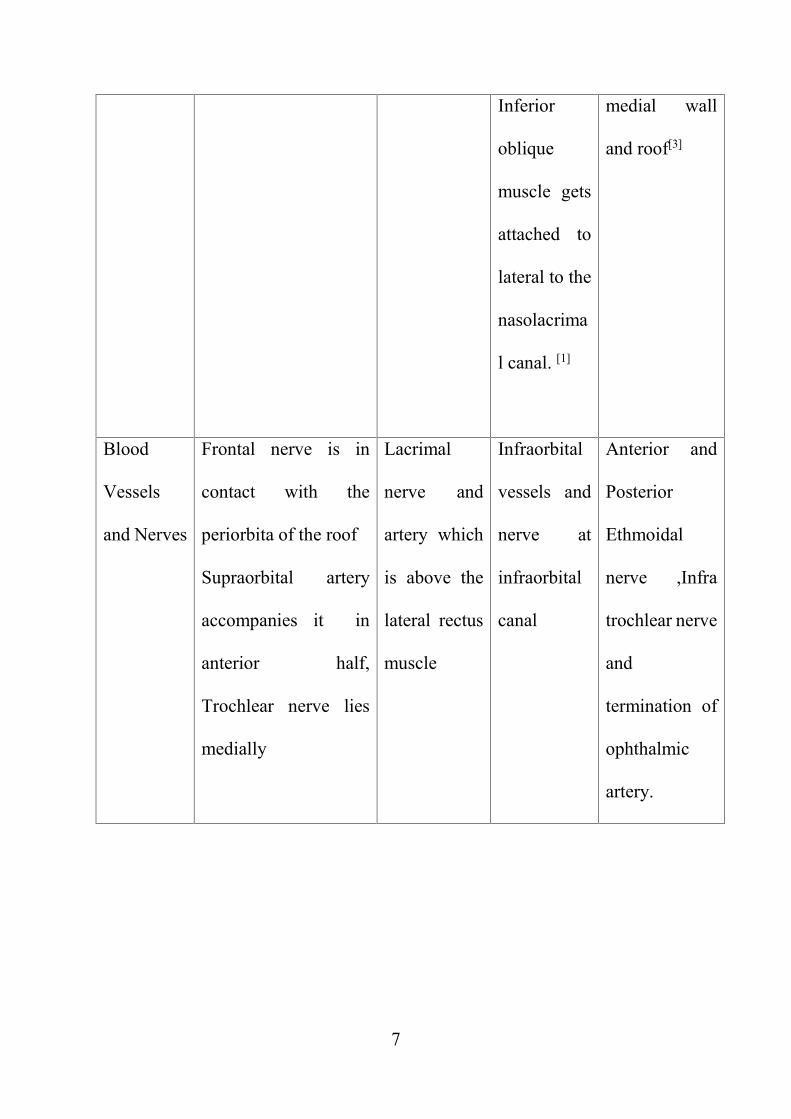
Inferior
oblique
muscle gets
attached to
lateral to the
nasolacrima
l canal. [1]
medial wall
and roof[3]
Blood
Vessels
and Nerves
Frontal nerve is in
contact with the
periorbita of the roof
Supraorbital artery
accompanies it in
anterior half,
Trochlear nerve lies
medially
Lacrimal
nerve and
artery which
is above the
lateral rectus
muscle
Infraorbital
vessels and
nerve at
infraorbital
canal
Anterior and
Posterior
Ethmoidal
nerve ,Infra
trochlear nerve
and
termination of
ophthalmic
artery.
8
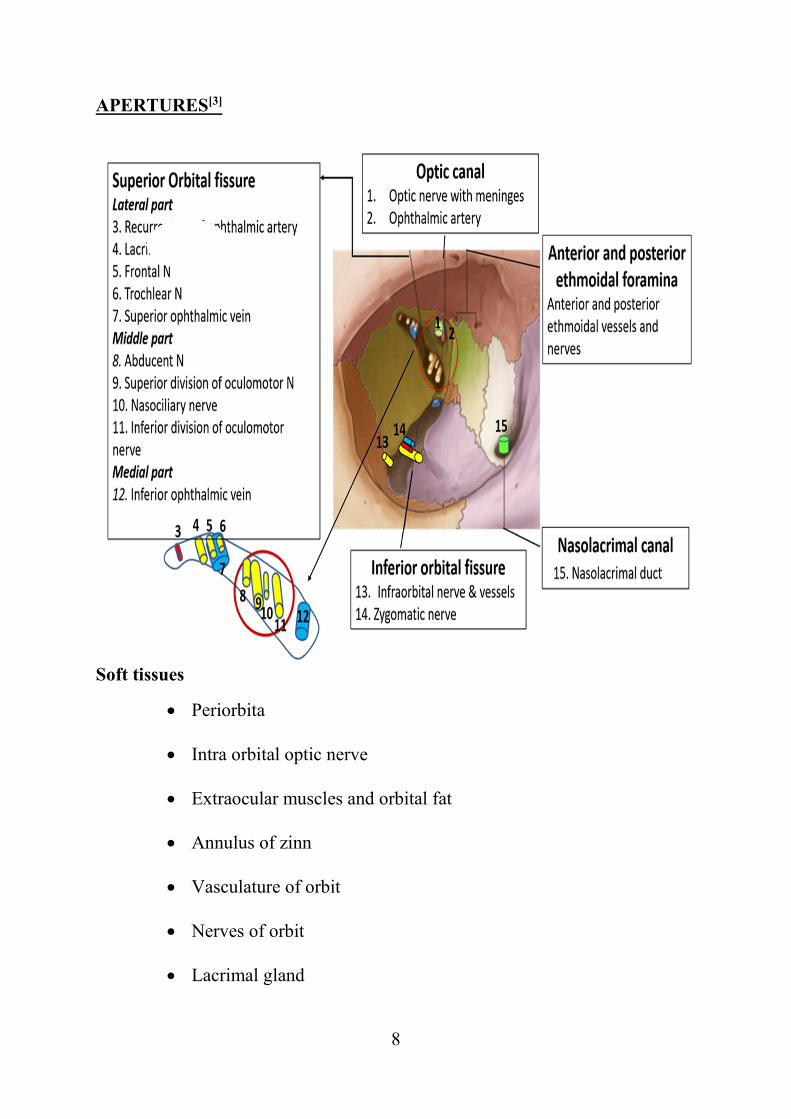
APERTURES[3]
Soft tissues
Periorbita
Intra orbital optic nerve
Extraocular muscles and orbital fat
Annulus of zinn
Vasculature of orbit
Nerves of orbit
Lacrimal gland
9
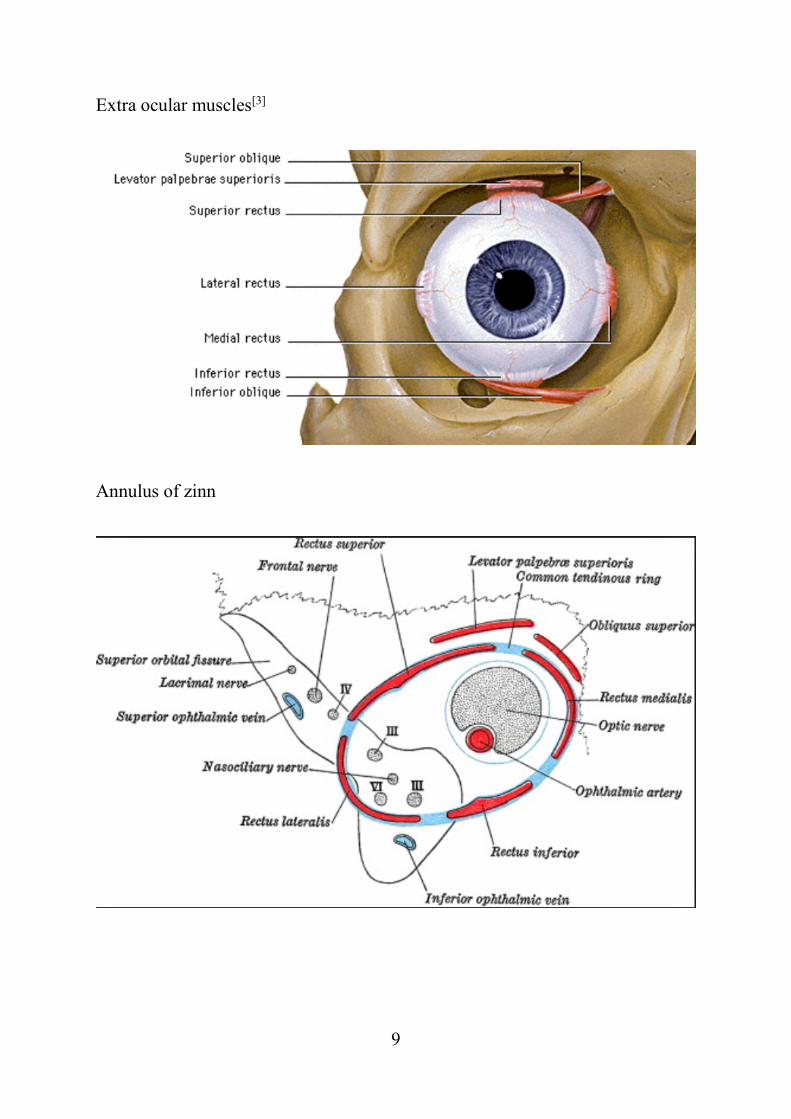
Extra ocular muscles[3]
Annulus of zinn
10
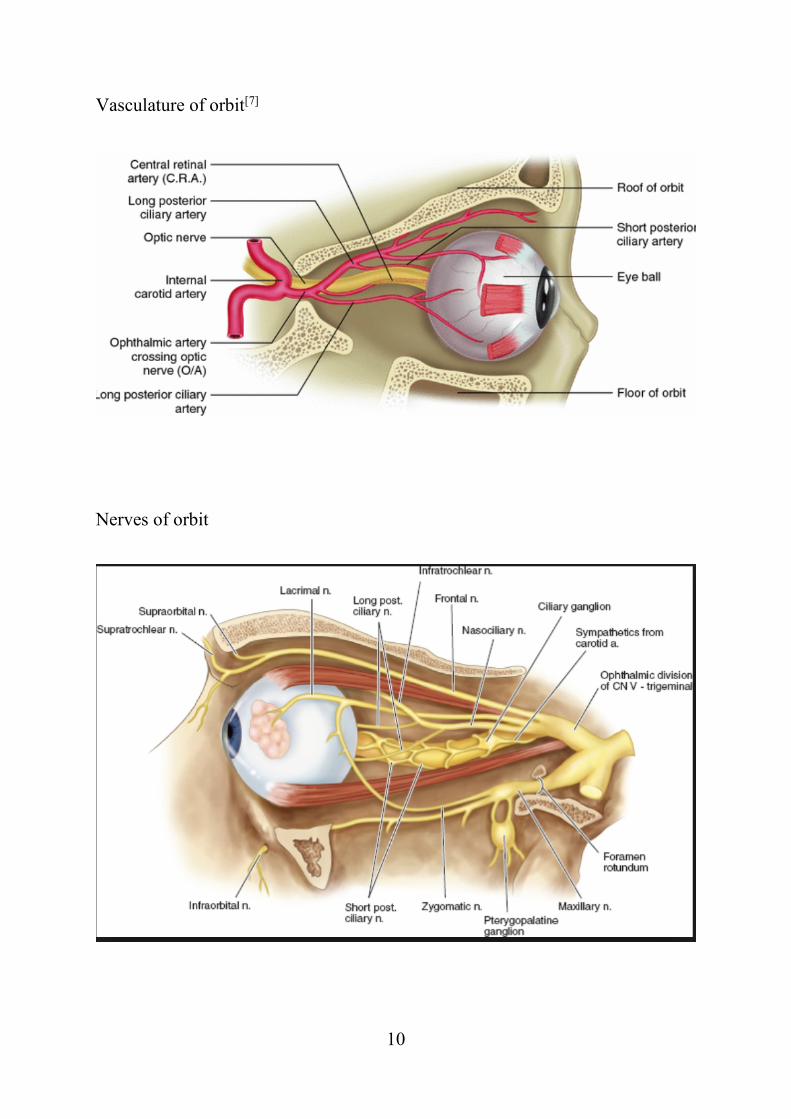
Vasculature of orbit[7]
Nerves of orbit
11
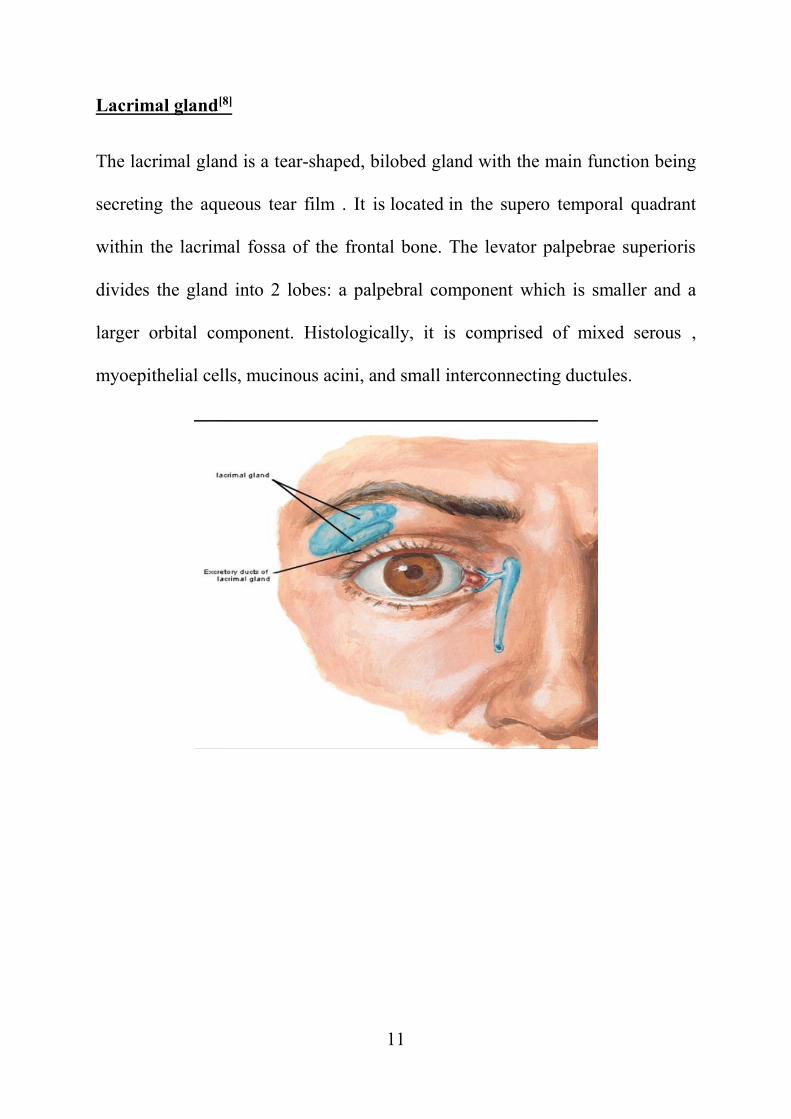
Lacrimal gland[8]
The lacrimal gland is a tear-shaped, bilobed gland with the main function being
secreting the aqueous tear film . It is located in the supero temporal quadrant
within the lacrimal fossa of the frontal bone. The levator palpebrae superioris
divides the gland into 2 lobes: a palpebral component which is smaller and a
larger orbital component. Histologically, it is comprised of mixed serous ,
myoepithelial cells, mucinous acini, and small interconnecting ductules.
12
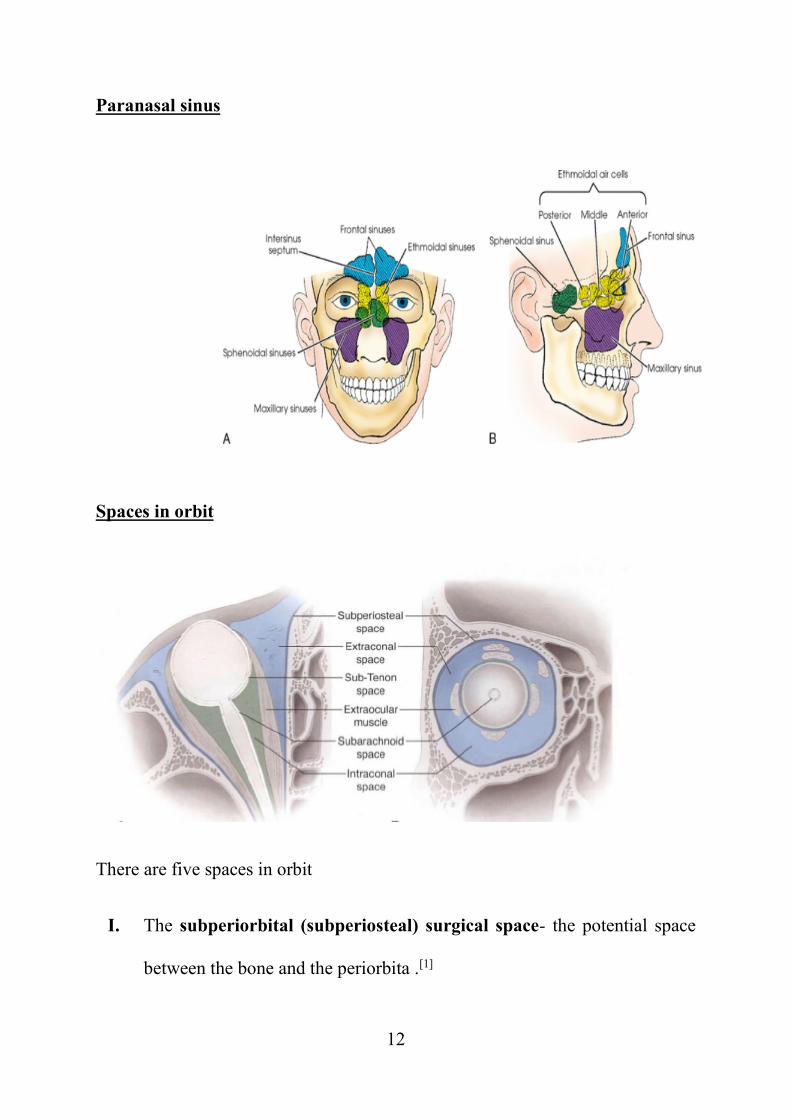
Paranasal sinus
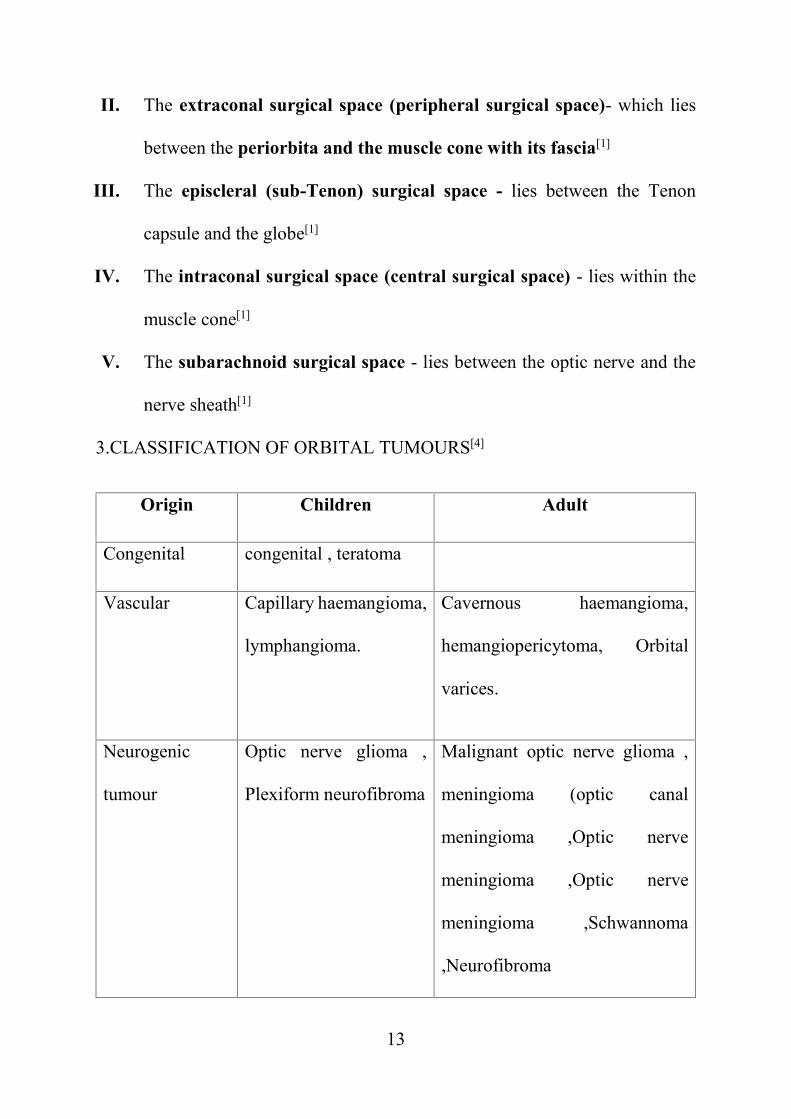
Spaces in orbit
There are five spaces in orbit
I. The subperiorbital (subperiosteal) surgical space- the potential space
between the bone and the periorbita .[1]
13
II. The extraconal surgical space (peripheral surgical space)- which lies
between the periorbita and the muscle cone with its fascia[1]
III. The episcleral (sub-Tenon) surgical space - lies between the Tenon
capsule and the globe[1]
IV. The intraconal surgical space (central surgical space) - lies within the
muscle cone[1]
V. The subarachnoid surgical space - lies between the optic nerve and the
nerve sheath[1]
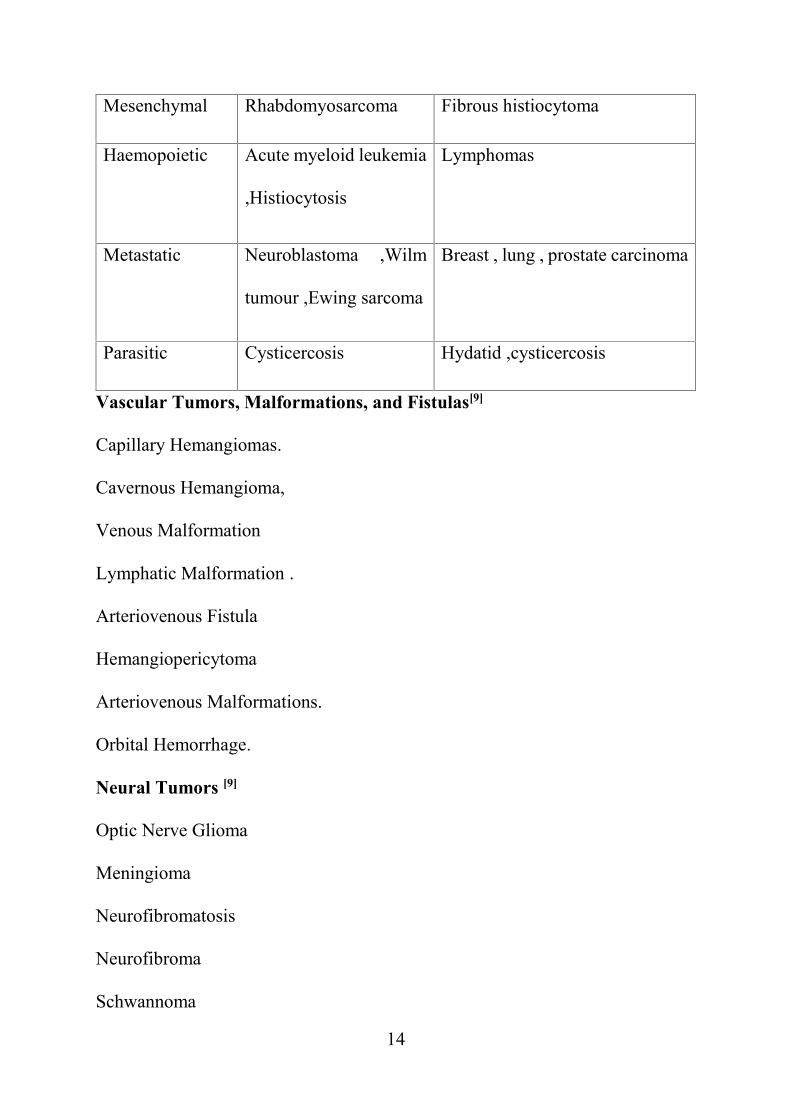
3.CLASSIFICATION OF ORBITAL TUMOURS[4]
Origin Children Adult
Congenital congenital , teratoma
Vascular Capillary haemangioma,
lymphangioma.
Cavernous haemangioma,
hemangiopericytoma, Orbital
varices.
Neurogenic
tumour
Optic nerve glioma ,
Plexiform neurofibroma
Malignant optic nerve glioma ,
meningioma (optic canal
meningioma ,Optic nerve
meningioma ,Optic nerve
meningioma ,Schwannoma
,Neurofibroma
14
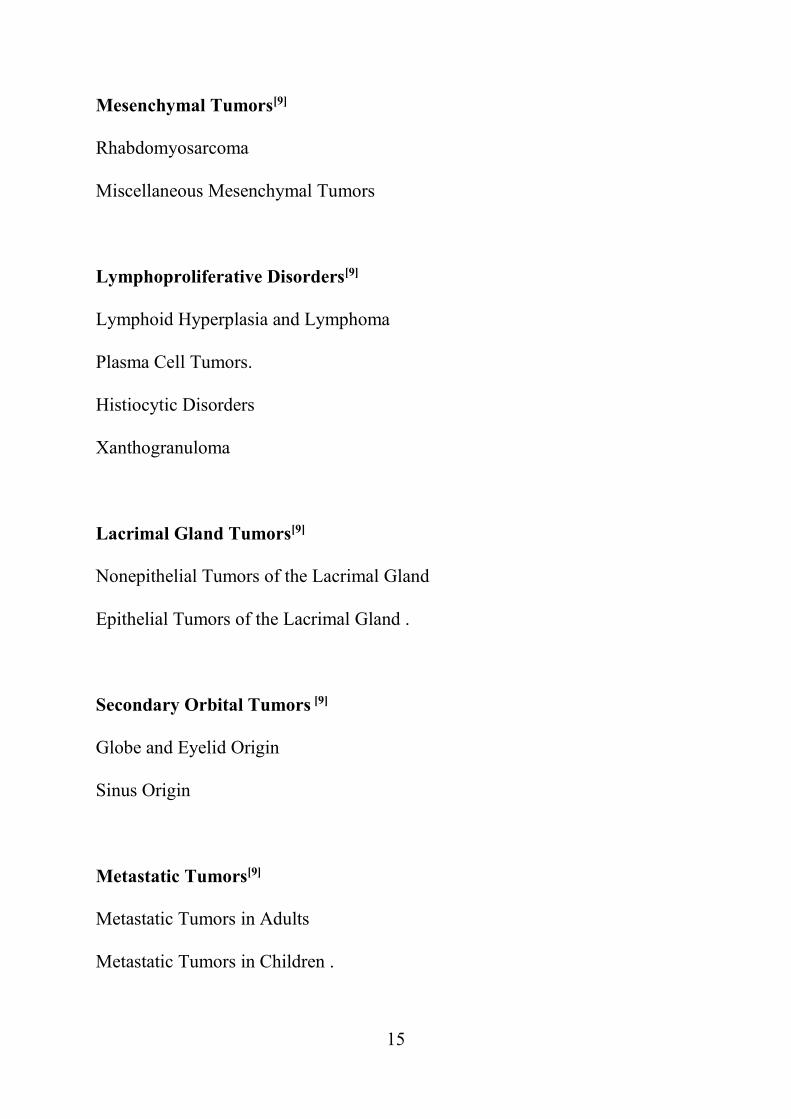
Mesenchymal Rhabdomyosarcoma Fibrous histiocytoma
Haemopoietic Acute myeloid leukemia
,Histiocytosis
Lymphomas
Metastatic Neuroblastoma ,Wilm
tumour ,Ewing sarcoma
Breast , lung , prostate carcinoma
Parasitic Cysticercosis Hydatid ,cysticercosis
Vascular Tumors, Malformations, and Fistulas[9]
Capillary Hemangiomas.
Cavernous Hemangioma,
Venous Malformation
Lymphatic Malformation .
Arteriovenous Fistula
Hemangiopericytoma
Arteriovenous Malformations.
Orbital Hemorrhage.
Neural Tumors [9]
Optic Nerve Glioma
Meningioma
Neurofibromatosis
Neurofibroma
Schwannoma
15
Mesenchymal Tumors[9]
Rhabdomyosarcoma
Miscellaneous Mesenchymal Tumors
Lymphoproliferative Disorders[9]
Lymphoid Hyperplasia and Lymphoma
Plasma Cell Tumors.
Histiocytic Disorders
Xanthogranuloma
Lacrimal Gland Tumors[9]
Nonepithelial Tumors of the Lacrimal Gland
Epithelial Tumors of the Lacrimal Gland .
Secondary Orbital Tumors [9]
Globe and Eyelid Origin
Sinus Origin
Metastatic Tumors[9]
Metastatic Tumors in Adults
Metastatic Tumors in Children .
16
Congenital tumour
Dermoid cyst
A dermoid cyst is a congenital choristoma of the orbit. A choristoma is a
benign tumour consisting histologically normal cells occurring in an abnormal
location. Dermoid cysts consist of keratinized epithelium and adnexal structures
like hair follicles, sebaceous glands and sweat glands. Dermoid cysts are the most
common orbital tumours in children, accounting for 46% of childhood orbital
neoplasms [5]. It constitute 3-9 % of all orbital tumours [6]. Dermoid cysts are
consists of keratinized stratified squamous epithelium with dermal appendages
and adnexal structures, including hair follicles, sebaceous glands, sweat glands,
smooth muscle, and fibro adipose tissue. The lumen contains keratin and hair.
CAPILLARY HEMANGIOMA (HEMANGIOENDOTHELIOMA)
Capillary hemangioma is also called hemangioendothelioma , a congenital
tumour which consists of tightly packed capillaries that usually presents during
the first 6 months of life .
It is mostly unilateral and visible on the surface, but it may lie deep in the orbit -
more common quadrant being the superonasal quadrant .
Superficial Lesions
Also called as the ‘strawberry nevus,’ capillary hemangioma is confined to
the dermis. It may be single or multiple and is generally elevated.
Symptoms include ptosis, sometimes associated with astigmatism and amblyopia.
17
Treatment
Observation is warranted in most cases, since involution usually occurs.
Recently, systemic propranolol for 8-12 months has been shown to achieve
dramatic resolution for lesions in the proliferative phase. Intralesional steroids,
radiotherapy, and, more recently, topical corticosteroids also have been tried.
Topical Timolol maleate oinment has also been tried .
Deep Lesions
Deep lesions occur most commonly in the lids or posterior to orbital
septum and the most common quadrant involved being supero nasal quadrant.
Symptoms are proptosis, increasing size with the Valsalva maneuver or crying
displacement of the globe, subtle pulsations due to high vascular flow . Secondary
amblyopia may result from distortion of the globe.
Orbital imaging
Orbital imaging shows a well-defined intraconal or extraconal lesion , with
moderate to intense enhancement. On MRI the signals can be homogeneous to
heterogeneous, being hypointense on T1 and hyperintense on T2 images .
Pathology
A proliferation of capillary endothelial cells and small capillaries
is seen, with few spaces . Mitoses are commonly observed .
Treatment
18
Treatment consists of mainly observation, since many lesion will involute
.If the lesion is large or amblyopia is present, local radiotherapy (500 cGy) or
corticosteroids (systemic or local) may be given. Recently, propranolol has been
shown to cause significant involution for tumors .
Orbital Lesions Frequency
Cavernous hemangioma 50 %
Capillary hemangioma 18 %
Hemangiopericytoma 13 %
Lymphangioma 10 %
Orbital varices 5 %
Other 5 %
Cavernous Hemangioma[9]
It is the commonly occuring benign neoplasm of the orbit in adult age
group.
Age-Adults (20-40 years)
Sex predilection -Women more than men.
Pattern of growth- Slowly progressive proptosis which accelerates during
pregnancy.
19
Histopathology-Encapsulated tumour wih larege cavernous spaces containing
red blood cells and the walls contain smooth muscles.
Echography- Shows well circumscribed round to oval lesions with high internal
reflectivity and regular acoustic structure.
CT Scan -Homogenous soft tissue density and may show small phleboliths [10]
.MRI- Isointense T1 signal and bright T2 signal, Dark internal septations ,daek
circumferential rims which represent pseudocapsule.
Lymphatic Malformations (Lymphangiomas) [9]
Age- 1st or 2nd decade of life.
Sex Predilection – No sex predilection
Histopathology -Large serum filled channels lined by flat endothelial cells .
Scattered follicles of lymphoid tissues are found in the interstitium . They are not
encapsulated.
Echography -Shows orbital lesion with poor outline and irregular shape and low
internal reflectivity and highly reflective internal septa.
CT- Shows phleboliths[23] in the venous component and it may also have bony
abnormalities. [22] Venous or solid components of the tumours are hyperdense
compared to brain tissue in non contrast CT .
MRI - Grape like cystic lesions with fluid filled layers of RBCs and serum.
20
Orbital Varices[9]
They are low flow vascular lesions resulting from vascular dysgenesis.
Age- can occur in any age group
Sex Predilection – no sex prediliction
Clinical Presentations – Patient may have enophthalmos at rest and proptosis
increases Valsalva Maneuver.
Echography- Poorly defined margins with Calcifications seen.
CT- Contrast enhanced CT during Valsalva Maneuver shows enlargement of the
engorged veins .Phleboliths may be seen
Arteriovenous Fistula [9]
Age-Traumatic Fistula (15-30 years ) ,Spontaneous Fistula (30-60 years )
Sex Predilection– Traumatic Fistula is more common in men , Sponatneous
Fistula is more common in women .
Echography-Shows a dilated superior ophtalmic vein amd mikd thickness of
extraocular muscles with medium to highinternal reflectivity.
CT-Shows diffuse enlagement of some or all of the extraocular muscles reulting
from venous engorgement and a characterstically enlarged superior ophthalmic
vein.
21
Neural Tumours [9]
Optic nerve glioma
Age-1st decade
Sex Predilection-No sex predilection
Clinical Presentations- Gradual painless unilateral axial proptosis associated with
vision loss and RAPD.It affect 28% in optic nerve alone 72% chiasma and 43%
involve chiasma and midbrain.
Histopathology-Smooth fusiform intradural lesion,cystic spaces that contain
mucoid material with pial septae which are separated by well differentiated
astrocytes,eosinopholic Rosnthal fibres will be present which represents
degenerated astrocytic process,Immunohistochemistry reveals positive for
neuron specifis enolase .
Echography-Fusiform enlargement of the optic nerve, low to medium regular
internal reflectivity will be present .
CT-Fusiform enlargement of the optic nerve with kinking of the nerve.
MRI- [33] The hallmark of optic nerve glioma is circumscribed tortuosity and
fusiform thickening of the optic nerve. Optic gliomas are T2 hyperintense .
[34] Diffuse thickening of the substance of the nerve , differentiates optic nerve
22
glioma from optic nerve sheath meningioma which shows tram track appearance
Optic nerve sheath meningioma[9]
It is a benign neoplasm of meningo endothelial cells. Age-Middle aged adults
Sex Predilection -Women (3:2) Clinical Presentation-Slowly progressive
proptosis with disc edema and optico ciliary shunt vessels.
Histopathology-1. Meningoepithelial type- Lobules of meningothelial cells
2.Psammous type - Psamoma bodies or Calcified concretions .
3.Angioblastic type-Vascular elements resembling hemangiopericytoma.
Echography-Medium to high internal reflectivity and calcification
Orbital Imaging.
CT -Tubular enlargement of the optic nerve with characteristic Tram -track
pattern enhancing nerve sheath with Radiolucent central portion of the nerve
MRI- T1 is hypointense and T2 is hyperintense .Optic nerve sheath meningioma
may produce a thin sheet around the optic nerve, termed “en plaque
meningioma”, producing the ‘tram track’ sign. [24]
Plexiform Neurofibroma
It is the most common benign peripheral nerve tumour in eyelid and orbit .
Age - 1st Decade
Sex Predilection -No sex predilection
23
Clinical Presentation - palpable “bag of worms” and an S shaped eye . 50% may
be associated with uveal neurofibromatosis and 77% associated with Lish nodule
25% associated with prominent corneal nerves 15%associted with optic nerve
glioma . The patient may have pulsatile proptosis due to the absence of greater
wing of sphenoid.
Histopathology - Bundles of axon , Schwann cells and endoneural fibroblast in
mucoid matrix. It has a characteristic cellular perineural sheath.
Immunohistochemistry is positive for S100 stain.
Echography- It has a irregular contour with high internal reflectivity and irregular
internal structure.
Orbital Imaging -A diffuse irregular mass with variable contrast enhancement
which may involve extraocular muscles ,orbital fat and Cavernous sinus .
MRI -T1 is hypointense and T2 is hyperintense to muscle .
Mesenchymal Tumours[9]
Fibrous Histiocytoma
It is a benign or malignant tumour which arises from fascia , muscle or other soft
tissues .
Age – Children and middle aged (40-60 years )
Sex Predilection- No sex predilection
24
Clinical Presentation-The most common orbital site is upper nasal quadrant .
Decreased vision, diplopia, exophthalmos , ptosis and epiphora are the presenting
symptoms .
Histopathology-A mixture of spindle shaped fibroblasts and histocytes arranged
in a storiform pattern around a central focus . Benign form – Well circumscribed
slowly growing lesion . Malignant – Rapidly growing , more infiltrative.
Echography – Well outlined lesion with low to medium internal reflectivity and
regular internal structure .
Orbital Imaging
MRI -Isointense with T1 and variable intense with T2 with respect to muscle .
Rhabdomyosarcoma
It is the most common soft tissue mesenchymal tumour in children .
Age-1st decade of life (7-8 years)
Sex Predilection -Males (Boys :Girls – 5:3)
Clinical Presentation- The onset will be Sudden and it progresses rapidly ,
discoloration of lids, edema , strabismus and ptosis .It can be divide into four
types :
1.Embryonal – Most common type . Represents more than 80% of cases. It mostly
affects the superior nasal quadrant.
25
2.Alveolar- – This is the most malignant form of rhabdomyosarcoma. It has a
predilection for inferior orbit which accounts for 9% of orbital
rhabdomyosarcoma.
3.Pleomorphic-It is the least common ad most differentiated form .
4.Botryoid- It is the rare variant of rhabdomyosarcoma which appears grape like.
It appears as a secondary invader from the paranasal sinus or conjunctiva
Histopathology-Myoglobulin is a specific immunohistochemical marker .
Embryonal – It consists of loose fascicles of undifferentiated spindle cells and
some may show cross striations on trichrome staining in immature
rhabdomyosarcoma
Alveolar –It has regular compartments which are composed of fibrovascular
strands in which rounded rhabdomyoblasts line up the connective tissues and float
in the alveolar spaces
Pleomorphic-It has strap like or round cells with cross striations which can be
visualised with trichrome stain.
Echography- They are usually well circumscribed, occasionally there may be
bony defects, low to medium reflectivity, moderate sound attenuation.
Orbital imaging
26
It represents a irregular well defined mass. Bony erosion is seenT1 is
isointense to hyperintense, T2 is hyperintense with respect to muscle. Globe
distortion [28] and extension to the paranasal sinuses [29] is seen. Calcification is
rare in untreated tumours. MRI shows bright T2 signal, which distinguishes
rhabdomyosarcoma from tumours such as chloroma or granulocytic sarcoma,
lymphoma and metastatic neuroblastoma . MR may delineate the true extent of
disease for surgical resection . [30] On occasion, a pyogenic abscess may mimic a
necrotic rhabdomyosarcoma clinically and by imaging. [31] In such cases, MRI
with DWI is important in distinguishing, through demonstration of restricted
diffusion of pus in an abscess cavity, [32] as opposed to elevated diffusion in the
necrotic portion of a tumour.
Staging -There are four stages :
I. Localised tumour, completely resected
II Regional spread ,with or without positive nodes, grossly resected
III Gross residual tumour remaining after incomplete resection
IV Distant metastases
Miscellaneous Mesenchymal Tumours
Solitary fibrous tumour – Composed of spindle shaped cells which are positive
for CD34 on immunohistochemical studies
27
Fibrous dysplasia -Benign developmental disorder. MRI shows the lack of dural
enhancement (which distinguishes it from meningioma) and CT shows
hyperostotic bone .
Osteoma- Benign tumours which involves any of the periorbital sinuses. CT scans
show dense hyperostosis with well defined margins. They are slow growing
lesions that can produce proptosis, compressive optic neuropathy.
Lymphoproliferative disorder [9]
Lymphoid hyperplasia and lymphoma
Lymphoid tumours mold around normal structures without deforming them, and
they are homogenous which does not erode the adjacent bone. They may be
well defined, or infiltrative.
Based on the REAL classification, types of orbital lymphomas are
I. Mucosa associated Lymphoid tissue (MALT) lymphoma-It accounts for
40-60% of orbital lymphomas. MALT lymphoma occurring in ocular
adnexa are not associated with mucosal tissues . Some conjunctival MALT
lymphomas are associated with chronic chlamydial infection .They have a
low grade malignancy. Long term follow up shows half of the patients
developed systemic disease in 10 years .
28
II. Chronic lymphocytic lymphoma (CLL) represents a low grade lesion with
small and mature -appearing lymphocytes.
III. Follicular Centre Lymphomas – Represents low grade lesion with
follicular centre.
IV. High grade lymphomas which includes lymphoblastic lymphoma, Large
cell lymphoma , Burkitt’s Lymphoma
It can also be classified as lymphocytic, plasmacytic and leukemic lesions .
Lymphocytic lesions are again classified into
Idiopathic inflammation (Pseudotumour)
Lymphoproliferative reactive and atypical disease
Lymphomas
Benign reactive lymphoid hyperplasia
It constitutes a benign proliferation of lymphoid follicles.
Clinical Presentation- Patient will present with painless and normal vision . A firm
rubbery mass is palpable and there may be subconjunctival “salmon patch”.
Histopathology-It has a polymorphic array of small lymphocytes and plasma cells.
It has mitotically active germinal centres.
Echography – A-scan shows low to medium internal reflectivity with regular
structure .
Orbital Imaging -It moulds to the globe and other adjacent structures. On MRI it
shows T1 hypointense and T2 hyperintense to muscle.
29
Atypical Lymphoid Hyperplasia
It represents an intermediate between Benign reactive lymphoid hyperplasia and
malignant lymphoma.
Clinical Presentations- Patient may present with painless exophthalmos and
normal vision .A firm rubbery mass is palpable and there may be subconjunctival
“salmon patch” . It may involve other systemic organs.
Histopathology – Monomorphous sheets of lymphocytes which have larger nuclei
than Benign reactive lymphoid hyperplasia
Echography – A-scan shows low to medium internal reflectivity
With regular acoustic structure .
Orbital Imaging -It moulds to the globe and other adjacent structures. MR imaging
shows T1 hypointense and T2 hyperintense .
Malignant orbital lymphoma (Lymphosarcoma )
It is characterised by proliferation of monoclonal B-cells (Non-Hodgkins) which
arises in lymph node or in extra nodal site (orbit)
Age-Older age group (50-70 years )
Sex Predilection- No sex predilection
Clinical presentation –Palpable mass in the anterior orbit. symptoms like lid
oedema, exophthalmos, ptosis and diplopia. Most lesions are located in the
anterior, superior and the lateral orbit and frequently involve the lacrimal gland.
75% of cases – Unilateral involvement
25% of cases – Bilateral involvement
30
40% of cases – Systemic Involvement.
Histopathology-It has an anaplastic , infiltrative lymphocytes with large cleaved
nucleus with no follicles .
Echography-It shows with low to medium internal reflectivity with regular
acoustic shadow.
Orbital Imaging – Well defined mass which moulds to the adjacent structures.
Lymphoma
CT density is similar to skeletal muscle. MRI demonstrates homogenous,
intermediate T1 and T2 signals, and homogeneous contrast enhancement. [25][26][27]
Lymphomas most commonly involve the superolateral aspect of the orbit, [26] and
bilateral disease is common.
Histiocytic tumours
They are rare proliferative disorders of histiocytes which range from a solitary
benign lesion to a malignant lesion.
Eosinophilic Granuloma ( Histiocytosis X)
Age-5-10 years of age
Sex Predilection-No sex predilection
Clinical Presentation –Rapid onset of eccentric displacement of globe with
painful superolateral swelling. Overlying skin shows erythema and inflammatory
signs .
31
Histopathology- It is a soft friable tan yellow tumour which has sheets of
binuclear histiocytes, giant cells and eosinophils. In the cytoplasm , characteristic
Langerhan cells are seen.
Echography – Shows a well circumscribed mass with low internal reflectivity.
Orbital imaging -It shows an osteolytic lesion near the supratemporal bony rim
with marginal hyperostosis .Occasionally the lesion may extend into the canial
fossa.
Xanthogranuloma
Adult Xanthogranuloma of the orbit and the adnexa is often associated with
systemic manifestations . They are classified into four syndromes in their order
of frequency of occurrence :
1.Necrobiotic-xanthogranuloma(NBX)
2.Adult onset asthma with periocular xanthogranuloma (AAPOX)
3.Erdhiemm -Chaster disease(ECD)
4.Adult onset xanthogranuloma (AOX)
1. Necrobiotic-xanthogranuloma(NBX)- It is characterised by presence of
subcutaneous lesion in the lids and the anterior orbit. It has the propensity
to ulcerate and fibrose. Systemically it is associated with paraproteinemia
and multiple myeloma .
32
2. Adult onset asthma with periocular xanthogranuloma (AAPOX)- It is a
syndrome which includes periocular xanthogranuloma, lymphadenopathy,
asthma and increase in IgG levels .
3. Erdhiemm -Chaster disease(ECD)-It is the most severe of the adult
xanthogranulma, is characterised by dense progressive , recalcitrant
fibrosclerosis of the orbit and internal organs, including the retroperitoneal
,pleural ,perinephric spaces, mediastinum and the pericardium .In ECD ,
the involvement of the orbit is diffuse , which is in contrast to the NBX and
the AAPOX and AOX where there is an anterior orbit invovlvement which
leads to severe visual loss.
4. Adult onset xanthogranuloma (AOX)- It is an isolated xamthogranuloma
without any systemic involvement.
Metastatic tumour [9]
Metastatic tumour in children -Neuroblastoma, Leukemia
Metastatic tumour in adults – From breast carcinoma, From bronchogenic
carcinoma, From prostate carcinoma
Metastatic tumour in children
Neuroblastoma
It is the second most common orbital tumour in children. It arises from primitive
neuroblast which may be metastatic to the orbit . Orbital neuroblastoma in
33
children commonly occurs due to metastasis with primary in the abdomen.
[17] 40% of orbital metastases are bilateral. Primary orbital neuroblastoma arises
from the ciliary ganglion, [20][21] derived from neural crest cells.
Differentiated neuroblastoma is made of mature ganglion cells, Schwann
cells, and nerve bundles [19].
Age-Mean age at presentation is 2 years . 75% of cases occur before 4 years .
Sex Predilection-No sex predilection
Clinical Presentation-Rapid progression of exophthalmos over several weeks ,lid
ecchymosis ,lid edema, Ptosis is and Horner’s Syndrome
Histopathology-soft friable bluish mass with small round cells, with calcium and
areas of necrosis. Orbital Imaging -Irregular and poorly defined mass associated
with bone destruction and separation of suture .
Leukemia
Acute lymphoblastic leukaemia (ALL) is the most common type of leukaemia
which metastases to the orbit. Granulocytic sarcoma or chloroma - It is a primary
leukemic orbital mass and a rare variant of mylogenic leukaemia .
Metastatic tumours in adult
The most common metastatic tumours to the orbit are the breast, lung , prostate,
gastrointestinal tract, kidney . Owing to its abundant blood supply , the
34
extraocular muscles are commonly involved. Because of the relatively high
volume of low blood flow ,the second most common site is the bone marrow of
the sphenoid bone.
Breast Carcinoma – It is the most common primary source of orbital metastasis
in women . After 3-5 years of primary diagnosis it metastasis to orbit . It may
elicit a fibrous response which causes enophthalmos and restriction of ocular
motility .
Bronchogenic Carcinoma – It is the most common primary source of orbital
metastasis in men . It occurs most commonly in smoking males aged 45-60 years.
Prostate Carcinoma – It occurs most commonly in elderly man which can produce
a clinical picture resembling that of acute non specific orbital inflammation .They
mostly present with pain due to bony involvement .Imaging shows a lytic bone
lesion.
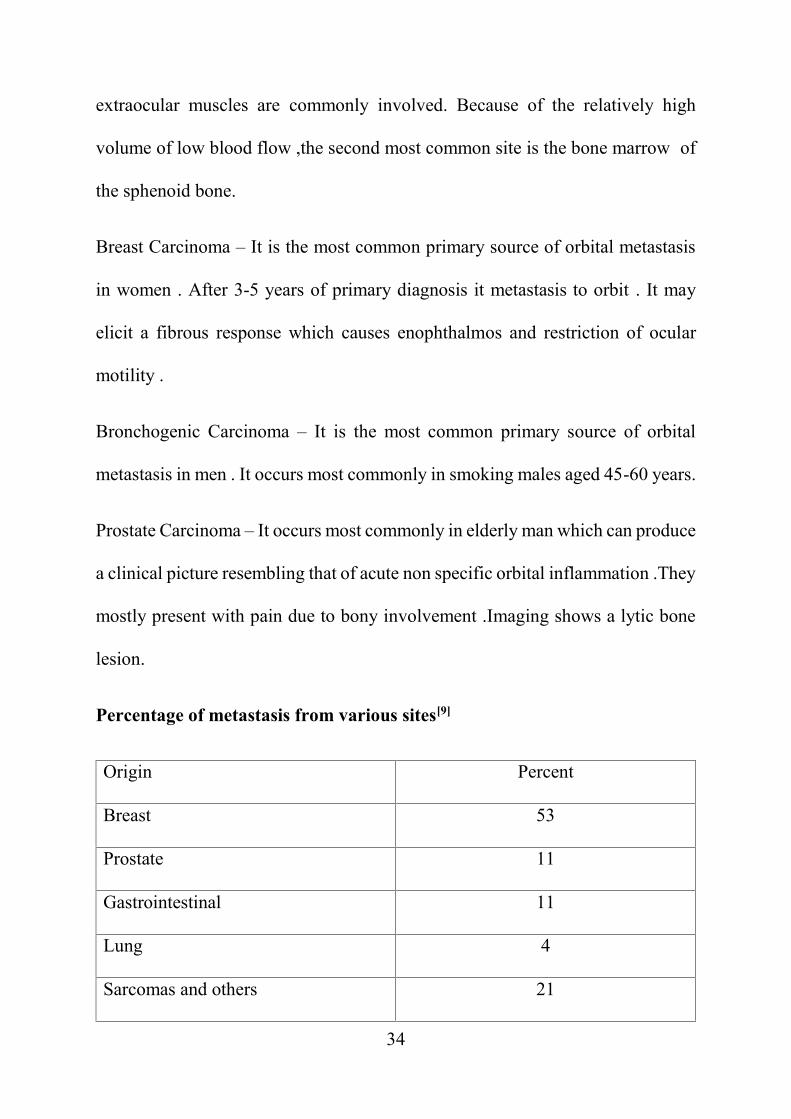
Percentage of metastasis from various sites[9]
Origin Percent
Breast 53
Prostate 11
Gastrointestinal 11
Lung 4
Sarcomas and others 21
35
Other solid tumors that metastasize to orbit are Ewings sarcoma, Wilms'
tumor, and testicular sarcoma. [20] These tumors rarely metastasize to the eye
itself.
4.Diagnosis and investigations of orbital disorders
o History
o onset, course, and duration of symptoms (pain, changes in vision
altered sensation and diplopia,)
o signs (globe displacement , erythema, palpable mass,)
o prior disease (such as thyroid eye disease [TED] or sinus disease)
and therapy
o injury (especially head or facial trauma)
o systemic disease (especially cancer)
o family history
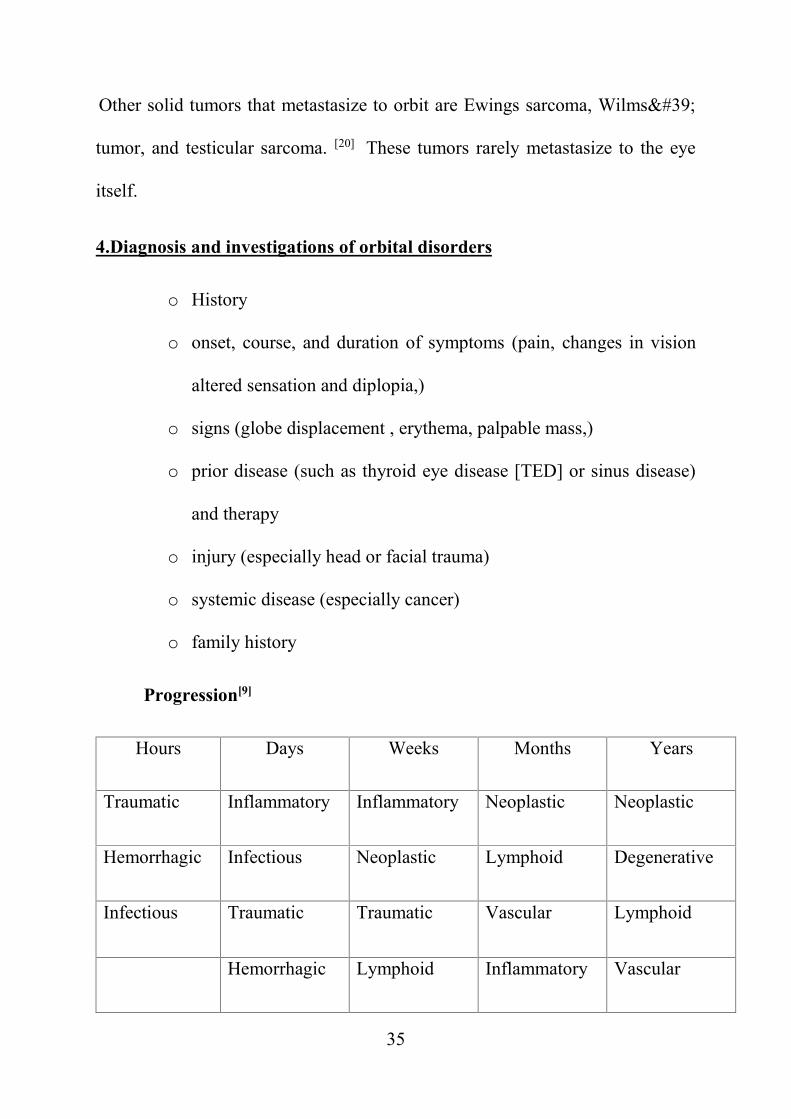
Progression[9]
Hours Days Weeks Months Years
Traumatic Inflammatory Inflammatory Neoplastic Neoplastic
Hemorrhagic Infectious Neoplastic Lymphoid Degenerative
Infectious Traumatic Traumatic Vascular Lymphoid
Hemorrhagic Lymphoid Inflammatory Vascular
36
Vascular Vascular Degenerative Inflammatory
CAUSES FOR ABAXIAL GLOBE DISPLACEMENT
DOWNWARD DISPALCEMENT
Fibrous dysplasia
Schwannoma
Frontal mucocele
Subperiosteal hamartoma
thyroid orbitopathy
Lymphoma
Neuroblastoma
UPWARD DISPLACEMENT
Maxillary sinus tumour
Lymphoma
Metastatic tumour
LATERAL DISPLACEMENT
Ethmoid mucocele
Lacrimal sac tumour
37
Nasopharyngeal tumours
Lethal midline granuloma
Metastatic tumours
Rhabdomyosarcoma
MEDIAL DISPLACEMENT
Lacrimal fossa tumours
Sphenoid wing meningioma
Periorbital changes[1]
Salmon patch in cul-de-sac Lymphoma
Corkscrew conjunctival vessels Arteriovenous fistula
S-shaped eyelid Plexiform neurofibroma
Lid lag and eye lid retraction Thyroid eye disease
Eczematous lesions over eyelids Mycosis fungoides (Tcell lymphoma)
Edematous swelling of lower id Meningioma , Inflammatory tumour ,
metastasis
Frozen globe Metastasis or Zygomycosis
38
Ecchymosis of eyelid Sign of metastatic neuroblastoma ,
Leukemia or amyloidosis
Opticociliary shunt (Retinociliary
venous collaterals )
Meningioma
Prominent temple Sphenoid wing meningioma and
metastatic neuroblastoma
Vascular anomaly of eyelid skin varix , Lymphatic malformation and
hemangioma .
Black crusted lesions in nasopharynx Phycomycosis
Facial asymmetry Fibrous dysplasia and
neurofibromatosis
Inspection
Enophthalmos, may occur as a result of volume expansion of the orbit (fracture),
in association with orbital varix, or secondary to sclerosing orbital tumors (eg,
metastatic breast carcinoma) . Proptosis often indicates the location of a mass
because the globe is usually displaced away from the site of the mass.
Exophthalmometry- is a measurement of the anterior-posterior position of the
globe. Commonly used are hertels and leuddes exophthalmometry .
It usually measures from the lateral orbital rim to the anterior corneal surface .
39
An asymmetry of greater than 2 mm between an individual patient's eyes suggests
proptosis or enophthalmos.
Proptosis can be tested clinically by asking the patient to sit and extend the neck
and the examiner has to stand behind the patient -Naffziger test .
Proptosis appreciated clinically when the examiner looks up from below with the
patient's head tilted back – WORMS EYE VIEW
Asymmetric orbital size- asymmetric palpebral fissures (usually caused by
ipsilateral eyelid retraction or facial nerve paralysis or contralateral ptosis)
Ocular movements- may be limited in a specific direction of gaze by neoplasm
or inflammation. In TED, the inferior rectus is the muscle most commonly
affected, followed by medial rectus, superior rectus and inferior rectus .
Palpation
Palpation around the globe may disclose the presence of a mass in the anterior
orbit.
Resistance to retrodisplacement - result either from a retrobulbar tumor
or from diffuse inflammation such as TED.
Pulsations of the eye -It may result from either abnormal vascular flow or
transmission of normal intracranial pulsations through a bony wall defect in the
orbit. Abnormal vascular flow may be caused by arteriovenous communications,
40
such as dural cavernous fistulas or carotid cavernous . Defects in the bony orbital
walls may result from sphenoid wing dysplasia in neurofibromatosis , trauma
sinus mucoceles, surgical removal of bone, or developmental abnormalities,
including encephalocele and meningocele .
Finger insinuation – If this is positive it indicates finger can be insinuated
between mass and bony orbital rim , hence there is no tumour infiltration .
Auscultation
Auscultation with a stethoscope over the globe may detect bruits in cases of
carotid cavernous fistula. The patient may also subjectively describe an audible
bruit.
Primary studies
CT
MRI
Ultrasonography
Secondary studies
Arteriography
Venography
CT and MR Angiography
41
5.Treatment modalities
A) Orbital surgery[2]
Anterior Routes
Anterior routes include the superior, inferior, medial, and transconjunctival
approaches. In this area are the orbital tumors that are palpated through the eyelids
or conjunctival fornices.
Tumors frequently managed by these approaches are the
carcinomas secondarily invading the orbit from a sinonasal source
the frontal mucocele extending into the superonasal orbit
some lymphangiomas, capillary hemangiomas, and rhabdomyosarcomas
and
the non-Hodgkin lymphomas clustered around the trochlea or protruding
into the conjunctival fornix
the inflammatory tumor extending along the back of the orbital septum
the orbitofrontal organizing hematoma without intracranial extension.
Excluded from this list are the palpable lacrimal gland tumor because these
lesions should be approached through a wider exposure through lateral or
superolateral orbitotomy because their size is often larger than expected. The
lacrimal gland tumours should be biopsied without rupturing its capsule . In all
the anterior approaches other the transconjunctival route, the location and length
42
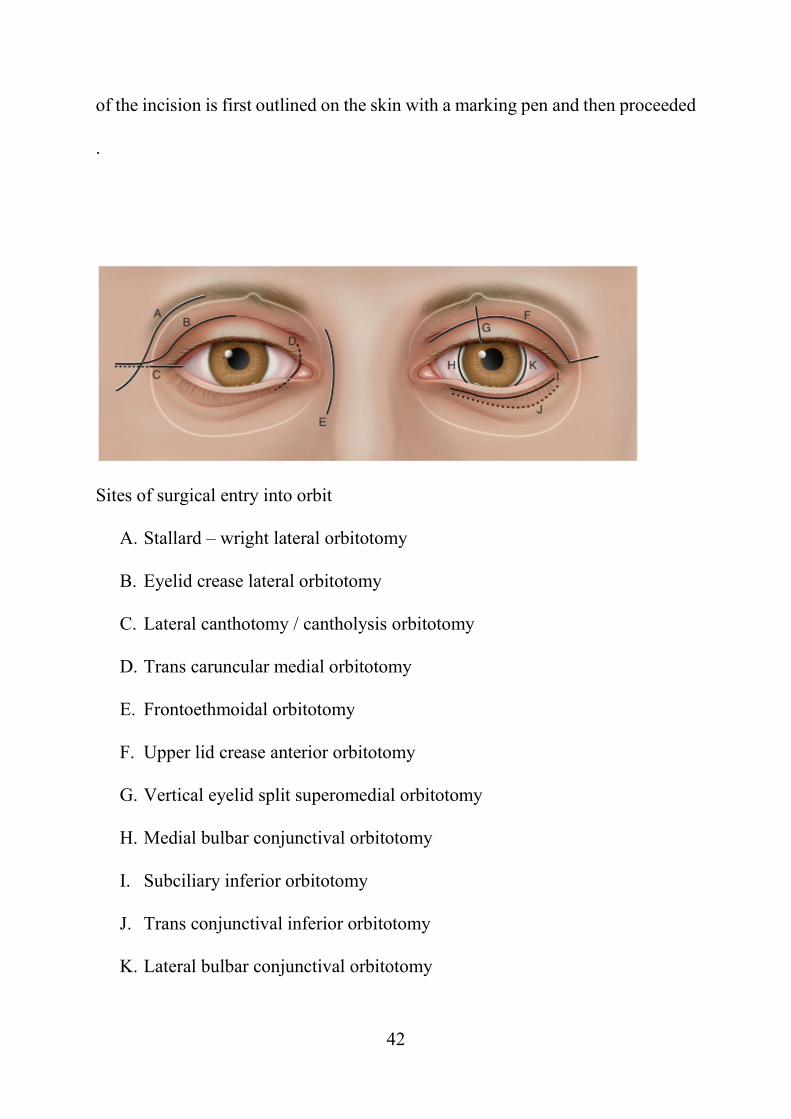
of the incision is first outlined on the skin with a marking pen and then proceeded
.
Sites of surgical entry into orbit
A. Stallard – wright lateral orbitotomy
B. Eyelid crease lateral orbitotomy
C. Lateral canthotomy / cantholysis orbitotomy
D. Trans caruncular medial orbitotomy
E. Frontoethmoidal orbitotomy
F. Upper lid crease anterior orbitotomy
G. Vertical eyelid split superomedial orbitotomy
H. Medial bulbar conjunctival orbitotomy
I. Subciliary inferior orbitotomy
J. Trans conjunctival inferior orbitotomy
K. Lateral bulbar conjunctival orbitotomy
43
Inferior Approach
Since there is a less number of primary orbital tumours in inferior orbit,
inferior orbitotomy is less frequently done . For the management of secondary
tumors that invade from a source in either the nasal cavity or maxillary antrum,
the inferior orbitotomy is combined with some sino nasal procedure.
The objective of the inferior orbitotomy is to gain access to the junction of the
periosteum of the maxillary bone with the periorbita covering the floor of the
orbit and the fascia separating the tissues of the eyelid from the orbital space. The
skin overlying the inferior orbital rim also is very thin. This feature, combined
with the tendency of healing skin to adhere directly to the underlying periosteum,
creates a visible scar. So skin incision is placed somewhere in the lower eyelid
superior to the orbital rim. The incision is generally a millimeter or two below the
lashes in a subciliary position .
Once the inferior orbital space is entered, the orbital fat will prolapse into the
space and visibility is adequate and it may be retracted with cotton-tipped
applicators . The location of the inferior oblique muscle should be noted when
dealing with orbital fat during this approach to avoid postoperative diplopia.
There are no major sources of hemorrhage in the infero anterior orbital space.
Medial Approach
The curved contour of the supero nasal orbital rim is the landmark for the
medial approach . The incision is gull-wing shaped over the medial canthal
44
tendon. This is the standard external ethmoidectomy incision. Other options
include a trans marginal, lid-splitting procedure and medial lid crease.
The external ethmoidectomy incision is 25 to 30 mm in length and is roughly
equal to one-fourth the circumference of the orbital rim.
In the supero nasal quadrant the bleeding vessels are the terminal branches of the
frontal and dorsal nasal arteries in the area of the trochlea and the angular vein .
The foramen of the anterior ethmoidal artery is an important topographic
landmark. It is located at the level of the cribriform plate and the junction between
the ethmoid labyrinth and the frontal bone. The diplopia occurs as a complication
of surgery results from the postoperative malposition of the trochlea of superior
oblique and also because of the secondary malfunction of the superior oblique
muscle of the affected eye . The complication is secondary to disengagement of
the periosteal base of trochlea during the course of the elevation of the periosteum
from supero nasal orbital rim.
The most recent description of a medial orbitotomy is the trans caruncular
approach. Mainly used for biopsy of the medial rectus muscle belly or for lesions
within the medial extraconal or peripheral space. The incision should be just
immediately lateral to the caruncle itself and the dissection should continue down
to the posterior lacrimal crest.
45
Lateral Route
The incision is carried through the skin and subcutaneous tissue to the
periosteum, which covers the temporal orbital rim (anteriorly) and the temporalis
fascia (posteriorly). The subcutaneous tissue along these planes is undermined
with a sharp dissection augmented by mobilization of soft tissues by blunt
dissection, which is accomplished by a gauze that is wrap around the tip of the
index finger, which results in a nearly bloodless surgical field. Next an incision
is made in the periosteum directly over the lateral orbital rim starting above from
the zygomatic-frontal suture extending upto the level of the zygomatic arch, 2 to
3 mm posterior to the bony rim. The periosteum is removed away from the bony
rim along the length of the incision .Edges of the periosteal incision are sutured
with silk for the anatomic closure. This will prevent the malposition of the
lateral canthal tendon. When the periosteum is lifted from the anterior portion of
the zygomatic arch and the periorbita is reflected from the inner face of the lateral
orbital wall, terminal branches of the lacrimal artery are noted . These can then
be coagulated with a bipolar cautery. The temporalis muscle is released from its
attachment to the posterior lip of the orbital rim after which the muscle is pealed
posteriorly from the surface of the lateral orbital wall .
46
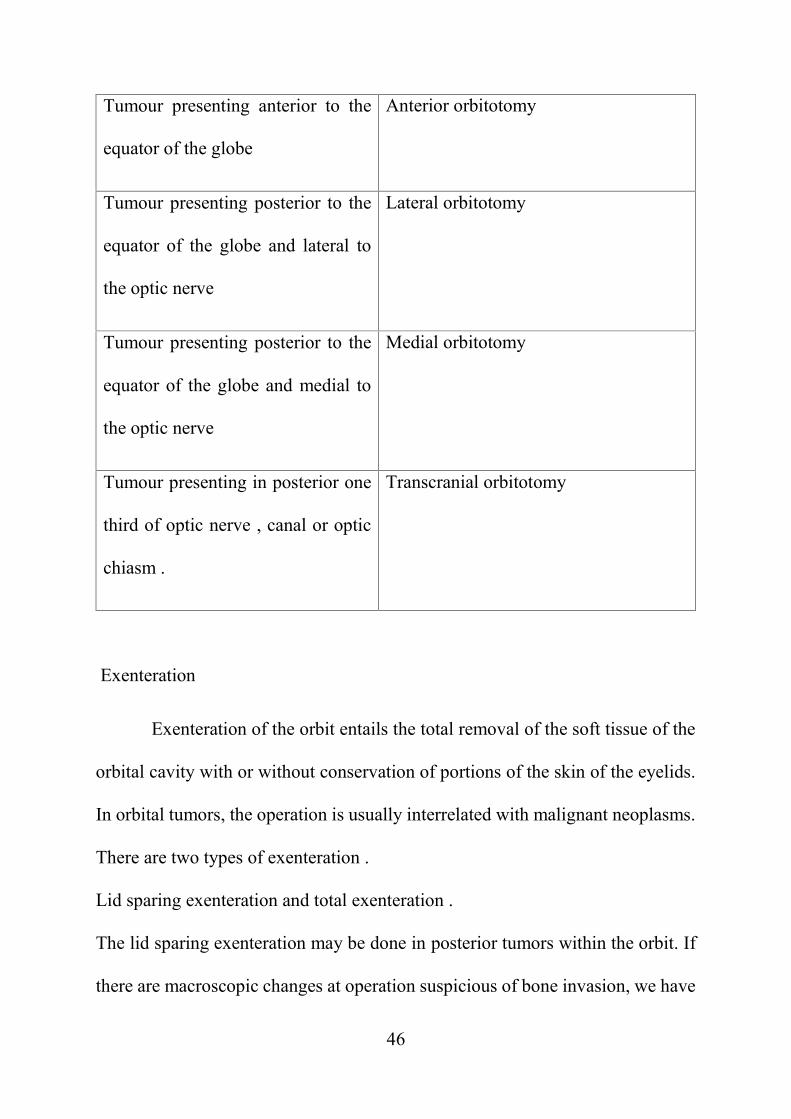
Tumour presenting anterior to the
equator of the globe
Anterior orbitotomy
Tumour presenting posterior to the
equator of the globe and lateral to
the optic nerve
Lateral orbitotomy
Tumour presenting posterior to the
equator of the globe and medial to
the optic nerve
Medial orbitotomy
Tumour presenting in posterior one
third of optic nerve , canal or optic
chiasm .
Transcranial orbitotomy
Exenteration
Exenteration of the orbit entails the total removal of the soft tissue of the
orbital cavity with or without conservation of portions of the skin of the eyelids.
In orbital tumors, the operation is usually interrelated with malignant neoplasms.
There are two types of exenteration .
Lid sparing exenteration and total exenteration .
The lid sparing exenteration may be done in posterior tumors within the orbit. If
there are macroscopic changes at operation suspicious of bone invasion, we have
47
to do a frozen section examination of the periorbita. If it is positive, bone should
be removed and sent for pathological analysis [35].
B) Chemotherapy
Lymphoma- High-grade tumors should be treated with standard
combination chemotherapy, cyclophosphamide, adriamycin, vincristine and
prednisone (CHOP). The current treatment of choice for elderly patients with
DLCL (Diffuse large cell lymphoma ) is that of CHOP chemotherapy with
rituximab (an anti CD-20 monoclonal antibody) , cyclophosphamide
,doxorubicin, (vincristine) oncovin prednisolone (R-CHOP) regimen. This is
based on a European study which studied CHOP vs R-CHOP in patients with
DLCL and showed prolongation of survival and overall survival in the group that
was treated with R-CHOP without additional toxicity.
Maxillary carcinoma- Induction chemotherapy (ICT) and concurrent
chemoradiation therapy (CCRT) are the common multimodality treatments for
stages III and IV locally advanced maxillary sinus carcinoma.
Cisplatin (100 mg/m2) was administered via a microcatheter into internal
maxillary artery over two hours on day 1, and 5-FU (1000 mg/m2/day) was
continuously infused from day 1 to day 5 over 120 hours through the IV line. A
standard hydration and mannitol diuresis regimen were applied. The entire
procedure was repeated 2–3 times for every 3–4 weeks.
48
C) Radiotherapy
Methods of Radiation Delivery
A. EXTERNAL BEAM RADIATION THERAPY
External beam radiation therapy (EBRT) is currently delivered utilizing photons
(gamma rays or X ray) or particles (protons or neutrons), with linear accelerators
(LINACs) doing the bulk of the work.
B. INTENSITY-MODULATED RADIATION THERAPY
Intensity-modulated radiation therapy (IMRT) utilizes controlled X-ray
accelerators to create a three-dimensional (3-D)--shaped conformal
treatment zone.
IMRT allows for a higher and more effective radiation dose to be delivered to the
tumor, with fewer normal-tissue side effects .
49
C.VOLUMETRIC MODULATED ARC RADIATION THERAPY
It is a volumetric arc therapy that delivers a precisely sculpted 3-D dose
distribution with a single 360degree rotation of the LINAC( linear particle
accelerator ).
D.STEREOTACTIC RADIOSURGERY
There are three basic types of SRS:
The gamma knife
The LINAC is preferred to deliver high-energy X rays, photons, or electrons
to larger tumors.
Charged-particle (e.g., proton) irradiation
E. PARTICLE RADIATION THERAPY
1. Proton
2.Neutron
F. BRACHYTHERAPY
Brachytherapy involves surgically placing a radio- active material (typically
seeds or wires) directly inside the body. It is commonly used to overlap with a
50
larger field of EBRT. Brachytherapy implants can be either temporary or
permanent.[36]For example, plaque radiation therapy for choroidal melanoma .
1. Brachytherapy Techniques
a.Finger’s Indications for the Brachytherapy Boost Technique
1 When the standard external beam radiotherapy dose would likely result in a
blind and painful eye due to radiation retinopathy, ulcerative keratopathy, and/or
neovascular glaucoma.
2 When exenteration of the orbit is the only option, but offers historically poor
local control rates (e.g., adenoid cystic carcinoma).
3 When a recurrent tumor has already received maximal external beam radiation
therapy.
4 When a patient refuses or is a poor medical candidate for exenteration surgery,
preferentially use brachytherapy to address residual microscopic orbital disease
in treatment of extra scleral extension of uveal melanoma.
51
Irradiation of Specific Orbital Tumors
A.OPTIC NERVE GLIOMA
Multiport beam arrangements are typically used to minimize the entry dose and
concentrate the radiation within the targeted zone. Orbital tumors are typically
treated with a wedged-pair external (photon beam) technique. Doses of 45 to 54
Gy (in 1.8 to 2.0 Gy daily fractions) are typically employed.
B.RHABDOMYOSARCOMA
The minimum tumor dose should be 45 to 50 Gy over 5 to 7 weeks.[37][38] Lens
blocks are typically placed to protect the anterior segment (when possible).
Although patient survival has been excellent, doses in this range are typically
associated with severe, late ocular, and orbital side effects.
Intraocular Tumors that Require Orbital Radiation Therapy
A.. METASTASIS
In most cases, prompt ocular and therefore orbital EBRT(External beam
radiotherapy) at 25 to 40 Gy (in 2-3 Gy daily fractions) makes the preservation
of vision likely.
52
Both breast and lung cancers are radiosensitive, and so most patients with uveal
metastasis can be treated with relatively low-dose EBRT(External beam
radiotherapy) .
B.RETINOBLASTOMA
In treatment of retinoblastoma and using schedules of 2 Gy daily fractions with
long-term follow-up, radiation retinopathy has been reported to occur in as many
as 10% of eyes dosed to 35 Gy (EBRT), in 66% of eyes treated to 45 Gy, and in
100% of eyes given 80 Gy or more. Radiation optic neuropathy has been reported
after high-dose EBRT and ophthalmic plaque radiation therapy[39][40][41][42].
Side Effects of Orbital Radiation Therapy
A.EYELIDS AND LASHES
Skin changes associated with radiation therapy
acute erythema,
atrophy,
hair loss,
ectropion or entropion of the eyelid .
depigmentation,
telangiectasias,
53
Most desquamation is more common after doses of 50-60 Gy (in 1.8 to 2.2 Gy
daily fractions) over 5-6 weeks.
Eyelash loss may occur depending on the dose and dose rate. It may occur with
as little as 10 Gy, and it is permanent with dose of 30 Gy. At more than 50 Gy,
radiation can produce permanent alopecia.
B. LACRIMAL APPARATUS AND DRY EYE
Doses in the range of 30--40 Gy can be safely delivered to the entire orbit without
long- term keratitis sicca and it can be treated with Puntal occlusion , tear
supplementation and lid tarsorrhaphy .
C.CORNEA
Temporary limbal stem cell dysfunction has been described.
Acute corneal toxicity results from a loss of the tear film with secondary
keratitis sicca .
D.LENS
As little as 2 Gy in a single fraction or 8 Gy in multiple fractions can induce
cataract.[43][44]
The most common cataract after EBRT is posterior subcapsular cataracts , donut
cataracts have also been reported .
54
E.SCLERA
Beta-emitting strontium-90 (90Sr) and ruthenium-106 (106Ru) episcleral
applicators are more likely to deliver much higher ‘‘sclera-thinning’’ doses as
compared with low-energy iodine-125 (125I) or palladium-103 (103Pd) . No
scleral radiation damage has been reported in external beam radiation doses of 60
Gy.
F.IRIS
Iritis can occur with a single dose of 10-20 Gy, but severe anterior uveitis has
been observed with doses of 30-40 Gy (in 10 Gy fractions) and after 70--80 Gy
(over 6--8 weeks).
Radiation therapy can also lead to iris neovascularization and neovascular
glaucoma.
G.RETINA, CHOROID, AND OPTIC NERVE
Radiation-related retinal and choroid vascular changes can occur to external beam
radiation doses in a range of 45-60 Gy .
Patients receiving 35- 50 Gy has a moderate risk of developing vasculopathy, and
those receiving ocular doses of more than 50 Gy will all finally develop radiation-
related ocular vasculopathy.
Also , radiation can occlude the blood vessels within the optic nerve (radiation
optic neuropathy) .
55
H.ORBIT
Orbital irradiation of children can decrease with bone development.[45]This leads
to hypoplasia and orbital asymmetry. secondary sarcoma can develop [46][47]
I.HYPOTHALAMUS AND PITUITARY DYSFUNCTION
pituitary and hypothalamic dysfunction is most commonly seen in children
irradiated for optic nerve glioma.
56
AIM
To study the clinical & histopathological Etiology of orbital space
occupying lesions.
Objective:
1.To study the Etiology
2. To study the Radiological features (CT/MRI/B scan)
3. To study the Treatment modalities & Prognosis over one year follow up period.
Study Design:
Observational prospective cohort study.
Inclusion Criteria:
All age group including both males and females presenting with unilateral
and bilateral orbital swelling.
Exclusion Criteria:
Patient with History of trauma
Patient with Orbital infections / Inflammation
Patient who are not willing to participate in the study.
Eyelid swellings/tumours not extending into orbit .
57
MATERIALS AND METHODS
Sample size 35
The study will include patients of all age groups who are presenting in the
Department of Ophthalmology, Tirunelveli Medical College , and they will be
subjected to ,
I. Informed written consent
II. Detailed history regarding age, sex , duration of complaints , including
history of trauma ,infection ,ocular co morbidities .
III. Previous treatment history and systemic illness .
IV. Visual acuity assessment , slit lamp examination, fundus examination ,
extra ocular movement assessment, Intraocular pressure measurement
using Goldman applanation tonometry and differential tonometry .
V. CT, MRI, & B scan will be taken if necessary.
VI. Histopathological examination and immunohistochemistry will be
checked if needed .
VII. Treatment options like surgery , chemotherapy , Radiotherapy , surgery
with chemotherapy , surgery with radiotherapy will be done depending
upon the diagnosis .
VIII. Patients will be followed up on 3months, 6months, 1year and their
visual acuity , colour vision , extraocular movements , anterior segment
and fundus examination prognosis will be assessed.
58
REVIEW OF LITERATURE
Neto et al[48] described that in 11 year study period our of 181 tumours studied
70% were primary , 23% secondary , 6% metastatic and lymphomas, and 1%
was not classified .
Bajaj et al[49] described the profile of orbital lesions histopathologically and
found 63 malignancies among 119 cases, with malignancy rate of 53%. Among
children , Orbital rhabdomyosarcoma and retinoblastoma with orbital spread
were the most common causes of proptosis .
Bonavolonta et al[50] analysed that the most common benign tumour is dermoid
cyst (14%) and cavernous hemangioma (9%) . Non-Hodgkin lymphoma was the
most common malignant neoplasm (12%). And among lacrimal tumours , 64 %
were benign and among malignant tumours adenoid cystic carcinoma .
Mathew et al [51] described that 68% were benign and 32 % were malignant .
Benign tumors were more common in patients less than 60 years and malignant
tumors were more common in patients older than 60 years. Benign tumors were
most common in the superior temporal quadrant .
Tailor et al[52] cavernous hemangiomas appear as a well-circumscribed, ovoid
intraconal mass on cross-sectional images. Breast cancer is the most common
malignancy to metastasize to the orbit, followed by prostate cancer, melanoma,
and lung cancer. At imaging, gliomas often cause fusiform expansion of the optic
59
nerve, in which the nerve itself cannot be delineated from the lesion. In contrast,
meningiomas classically have a "tram-track" configuration .
Sarah et al [53] described the radiological features of Orbital space occupying
lesions classic finding of optic nerve glioma , which are T2 hyperintense and
involves substance of optic nerve . MRI of rhabdomyosarcoma shows bright T2
signals , which distinguish it from chloroma ,metastatic neuroblastoma and
lymphoma .
Sim et al [54] described that due to the lack of lymphatics in the orbit,
haematogenous spread is the mode of development of metastasis . Orbital breast
metastases tend to preferentially localize within orbital fat or extraocular muscles.
Mohammed Jaber Al-Mamoori [55] described presenting clinical
manifestations of patients proptosis (94.7%), visual acuity impairment (49.5%),
diplopia (18.9%), strabismus (10.5%), ptosis (4.2%), ocular/orbital pain (26.3%),
conjunctival edema (12.6%), subconjunctival hemorrhage (5.3%),
lacrimation (21.1%), tinnitus (2.1%), epistaxis (2.1%), vertigo (2.1%) .
McNab et al[56] studied the anatomical location and laterality of Orbital
cavernous hemangioma and found that it occurs in the intraconal space (87%) and
lateral to the optic nerve (47%), a distribution which is similar to the distribution
of small arteries and arterioles in the orbit.
60
Gensheimer et al[57] studied the survival index of patients using Kaplan-Meier
analysis which showed 5-year local tumor control was 80%, disease-free survival
was 61%, and total overall survival was 90%.
Isaacson PG et al[58] described that the majority of non-Hodgkin’s lymphomas
of the orbit and orbital adnexa are extra nodal marginal-zone B-cell lymphomas
of mucosa-associated lymphoid tissue (MALT)-type lymphomas .
Gill et al[59] studied the response and complications of 150 mg oral vismodegib
in 7 patients with locally advanced BCC. The mean treatment duration is 11
weeks (range, 4 to 16 weeks), 58% had 80-100% regression, 29% had less than
35% partial regression, and there was progression in 1 patient (14%). The most
common side effects of oral vismodegib are muscle spasm (100%) and weight
loss (83%) .
Tuncer et al[60] evaluated the therapeutic efficacy of rituximab in 10 patients with
Orbital adnexal lymphoma .Complete response was achieved in 36% and the
remainder required adjuvant radiotherapy for recurrence.
Raksha rao and Santosh honaver [61] described the use of intra-arterial
chemotherapy (IAC), periocular chemotherapy (POC), and intravitreal
chemotherapy (IVitC) has enabled to focus direct drug delivery to the tumor.
Unlike intravenous chemotherapy (IVC) which can be used in the primary
management of all retinoblastomas, IAC, POC and IVitC have specific

61
indications. The prognosis for life salvage is now around 98%, with 90% eye
salvage and 80% vision salvage.
62
RESULTS
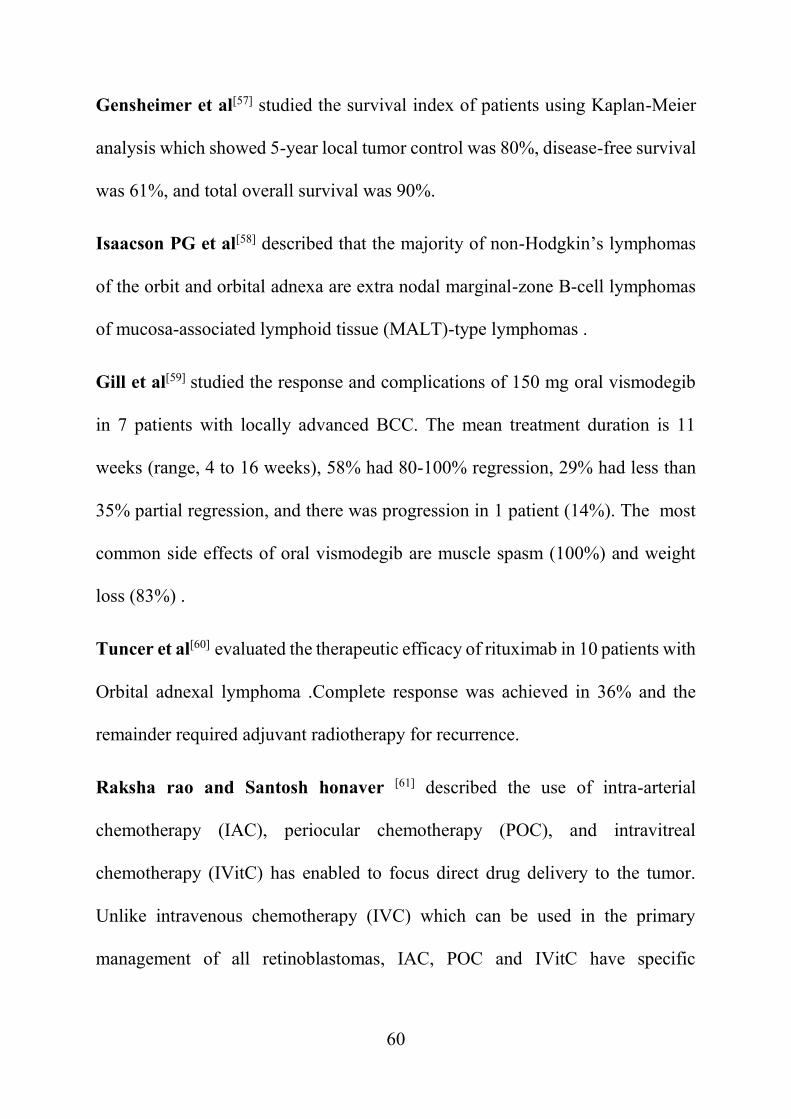
Figure 1: Age wise sex distribution
Figure 1 represents age wise sex distribution of study population. In less than one
year 1 male and no female . In the 1-10 years age group 5 were male and 1 female.
In the 11-20 years age group 1 was male and no female. In the 21-40 years age
group 3 were male and 5 female. In the 40-60 years age group 6 were male and 6
female . In the more than 60 years age group 7 were male and 2 female .
0
1
2
3
4
5
6
7
LESS THAN 1 1 TO 10 11 TO 20 21 TO 40 40 TO 60 60 PLUS
Sex and age Distribution
Female
Male
63
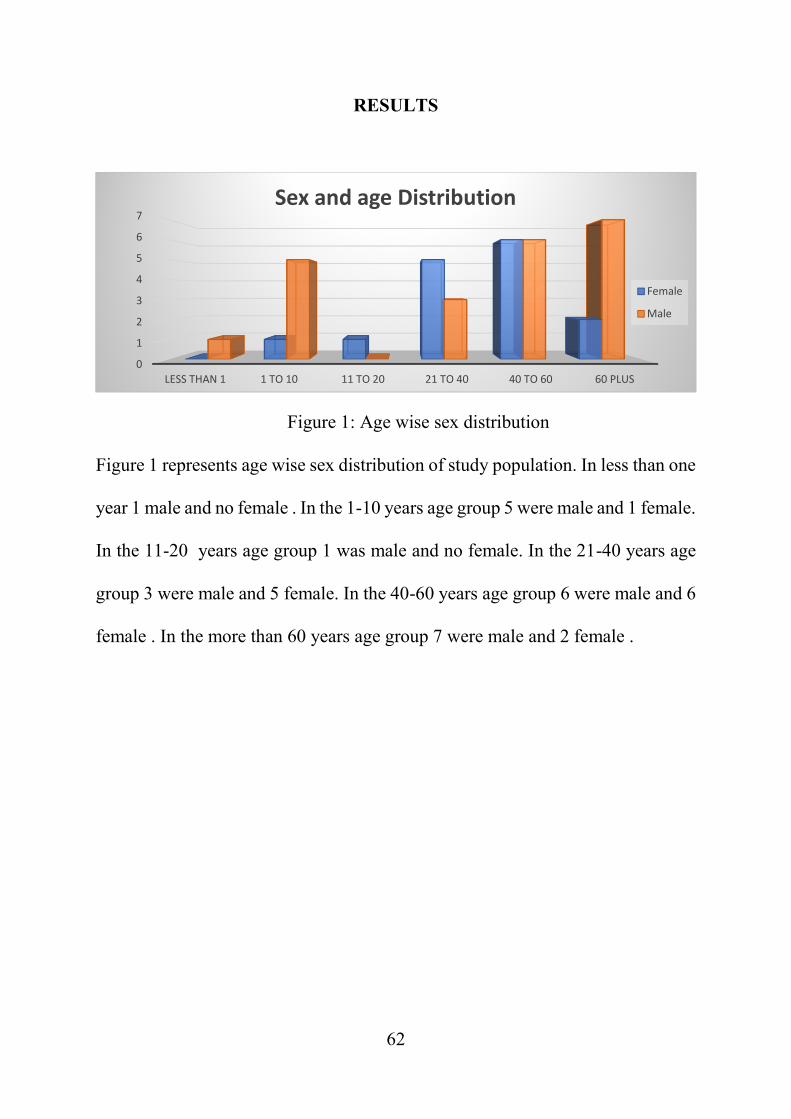
Figure 2: Laterality
Figure 2 represents laterality of the involved eye . In 36 patients there was
unilateral involvement and 1 bilateral involvement .
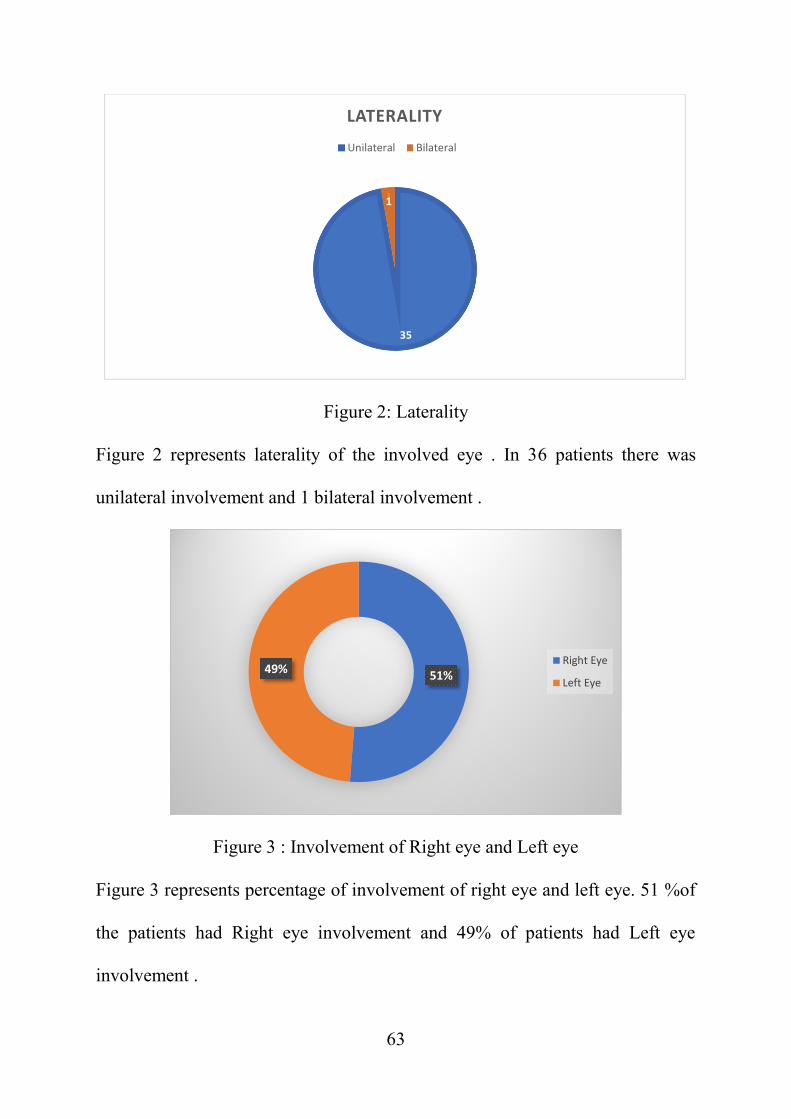
Figure 3 : Involvement of Right eye and Left eye
Figure 3 represents percentage of involvement of right eye and left eye. 51 %of
the patients had Right eye involvement and 49% of patients had Left eye
involvement .
35
1
LATERALITYUnilateral Bilateral
51%49%Right Eye
Left Eye
64
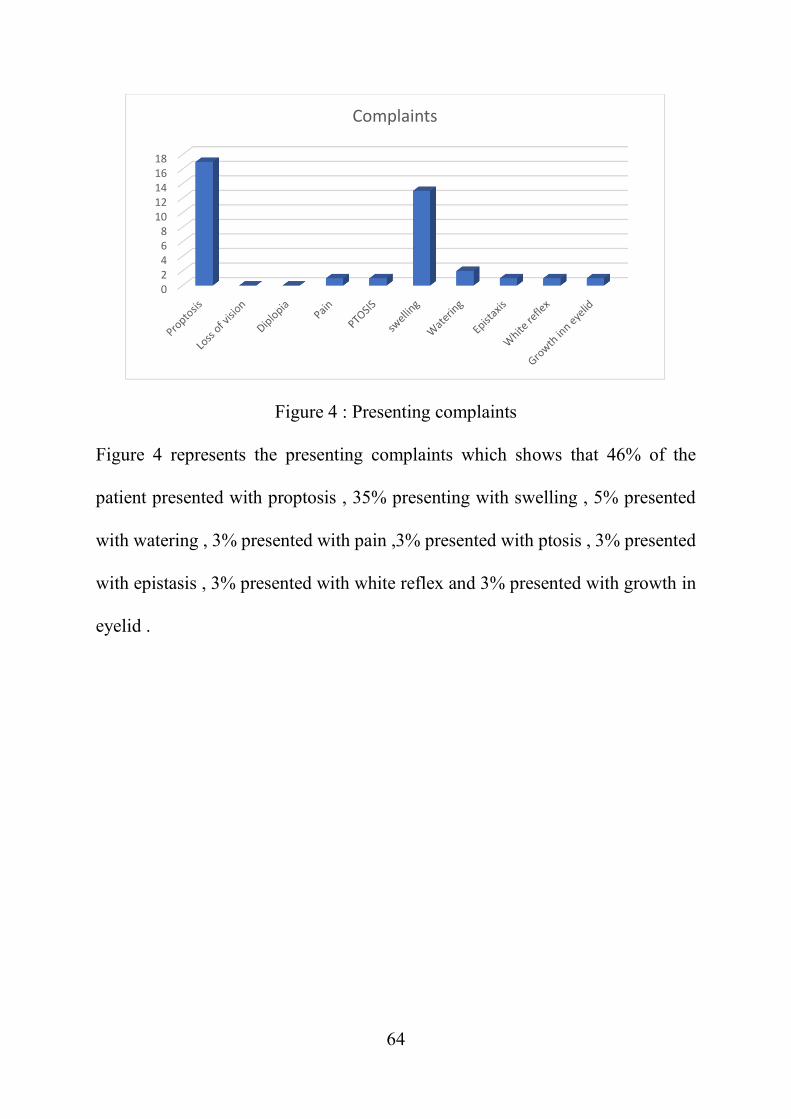
Figure 4 : Presenting complaints
Figure 4 represents the presenting complaints which shows that 46% of the
patient presented with proptosis , 35% presenting with swelling , 5% presented
with watering , 3% presented with pain ,3% presented with ptosis , 3% presented
with epistasis , 3% presented with white reflex and 3% presented with growth in
eyelid .
02468
1012141618
Complaints
65
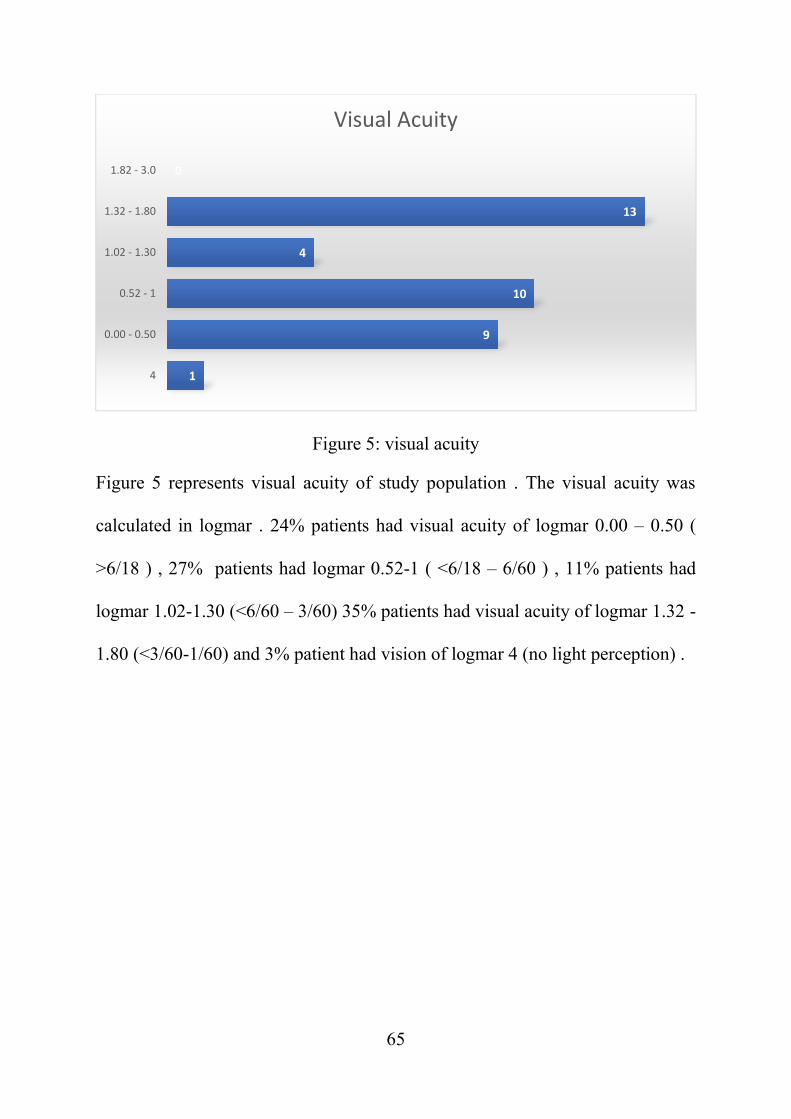
Figure 5: visual acuity
Figure 5 represents visual acuity of study population . The visual acuity was
calculated in logmar . 24% patients had visual acuity of logmar 0.00 – 0.50 (
>6/18 ) , 27% patients had logmar 0.52-1 ( <6/18 – 6/60 ) , 11% patients had
logmar 1.02-1.30 (<6/60 – 3/60) 35% patients had visual acuity of logmar 1.32 -
1.80 (<3/60-1/60) and 3% patient had vision of logmar 4 (no light perception) .
1
9
10
4
13
0
4
0.00 - 0.50
0.52 - 1
1.02 - 1.30
1.32 - 1.80
1.82 - 3.0
Visual Acuity
66
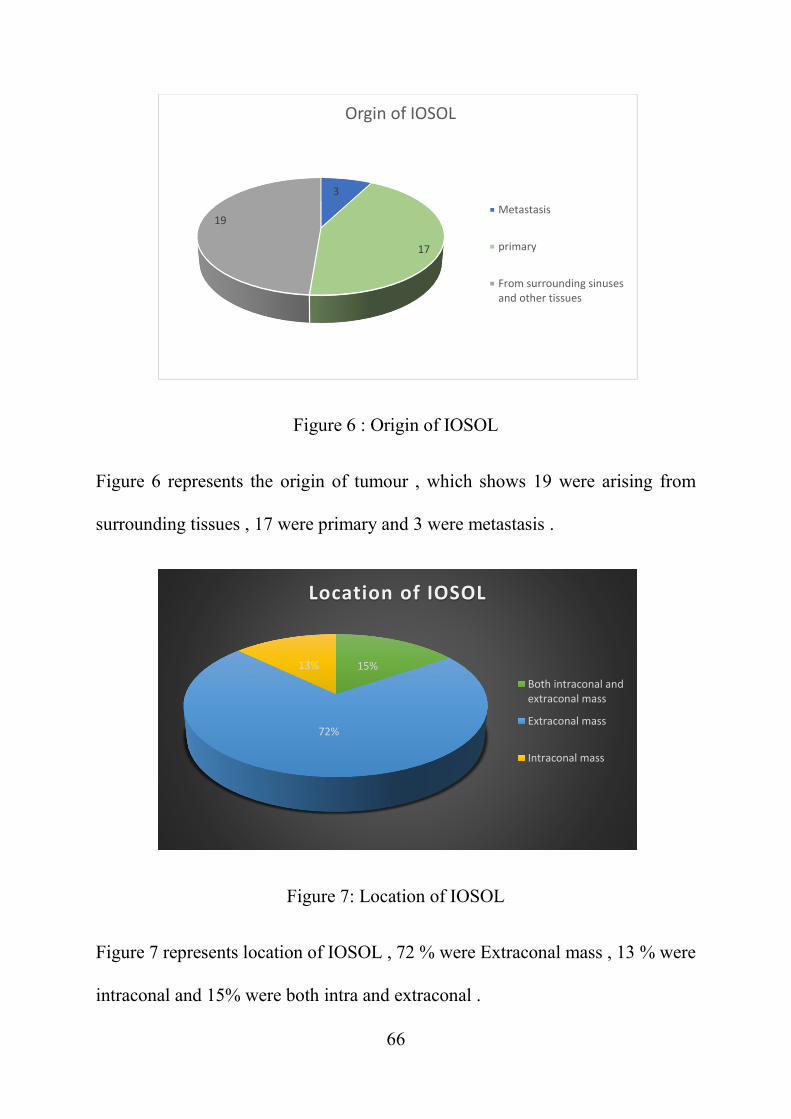
Figure 6 : Origin of IOSOL
Figure 6 represents the origin of tumour , which shows 19 were arising from
surrounding tissues , 17 were primary and 3 were metastasis .
Figure 7: Location of IOSOL
Figure 7 represents location of IOSOL , 72 % were Extraconal mass , 13 % were
intraconal and 15% were both intra and extraconal .
3
17
19
Orgin of IOSOL
Metastasis
primary
From surrounding sinusesand other tissues
15%
72%
13%
Location of IOSOL
Both intraconal andextraconal mass
Extraconal mass
Intraconal mass
67
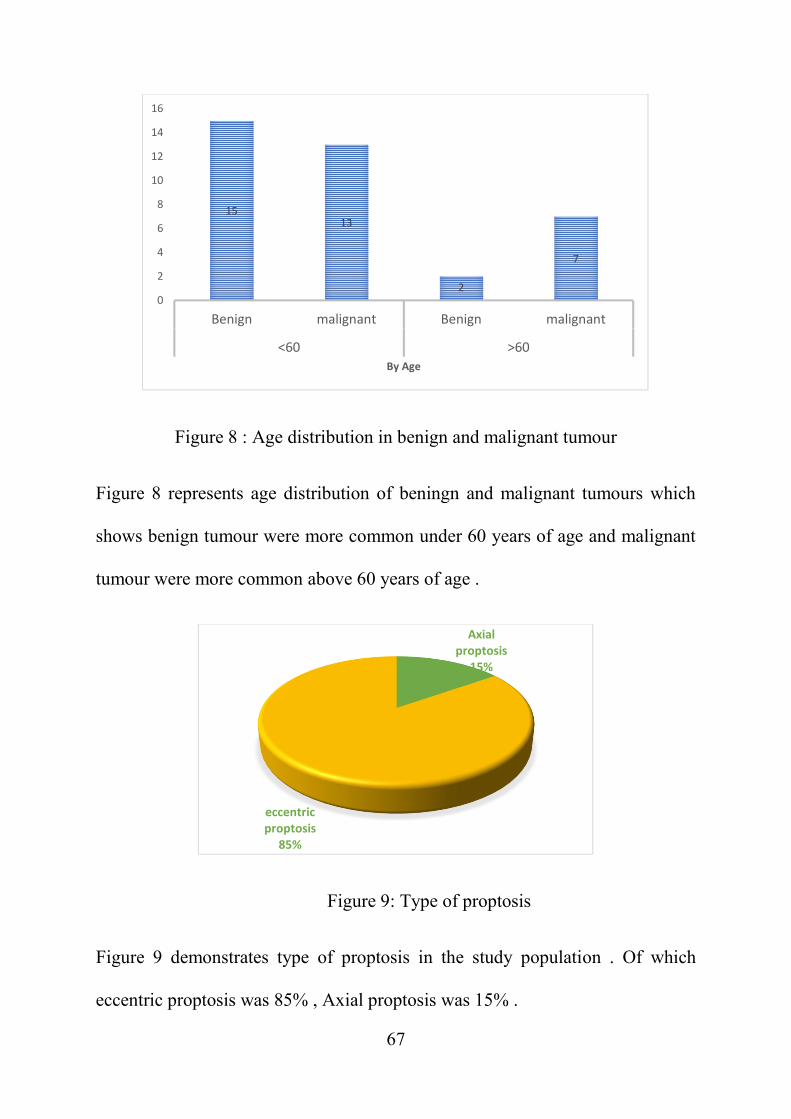
Figure 8 : Age distribution in benign and malignant tumour
Figure 8 represents age distribution of beningn and malignant tumours which
shows benign tumour were more common under 60 years of age and malignant
tumour were more common above 60 years of age .
Figure 9: Type of proptosis
Figure 9 demonstrates type of proptosis in the study population . Of which
eccentric proptosis was 85% , Axial proptosis was 15% .
1513
2
7
0
2
4
6
8
10
12
14
16
Benign malignant Benign malignant
<60 >60By Age
Axialproptosis
15%
eccentricproptosis
85%
68
Axial
proptosis
eccentric
proptosis
Column
totalP value
Both
intraconal and
extraconal
mass
3 3 6
P<0.05Extraconal
mass0 27 27
Intraconal
mass4 0 4
Row total 7 30 37
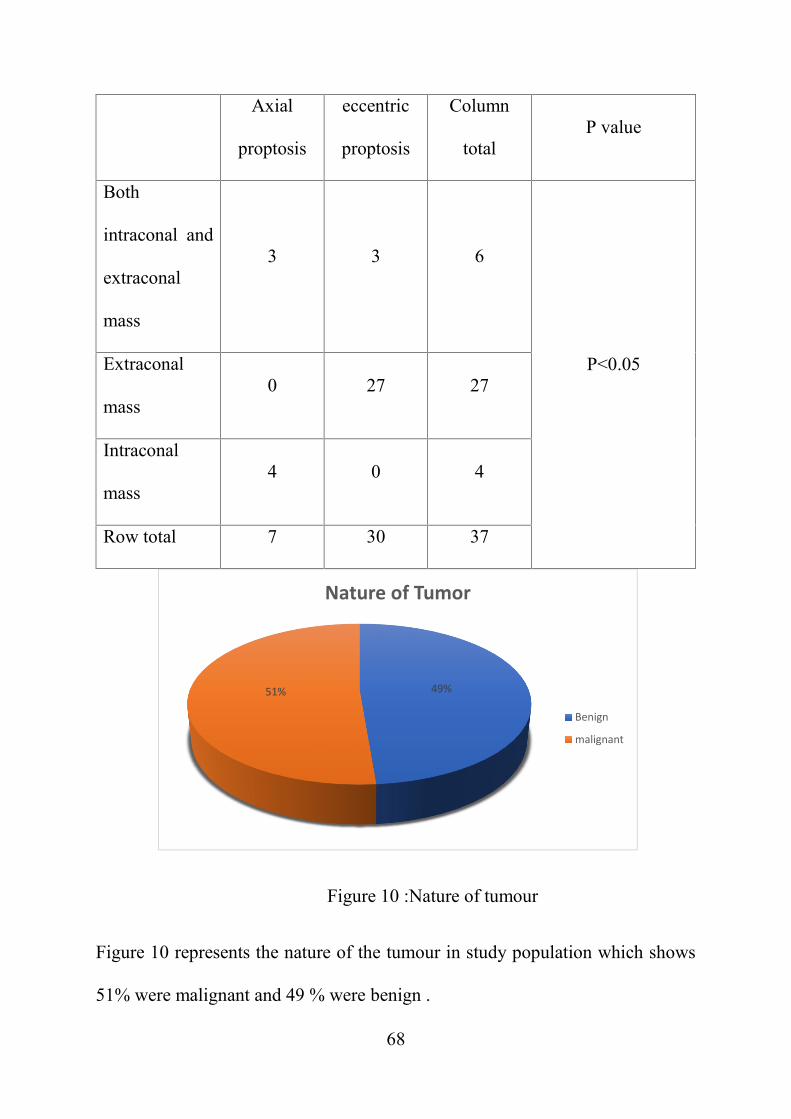
Figure 10 :Nature of tumour
Figure 10 represents the nature of the tumour in study population which shows
51% were malignant and 49 % were benign .
49%51%
Nature of Tumor
Benign
malignant
69
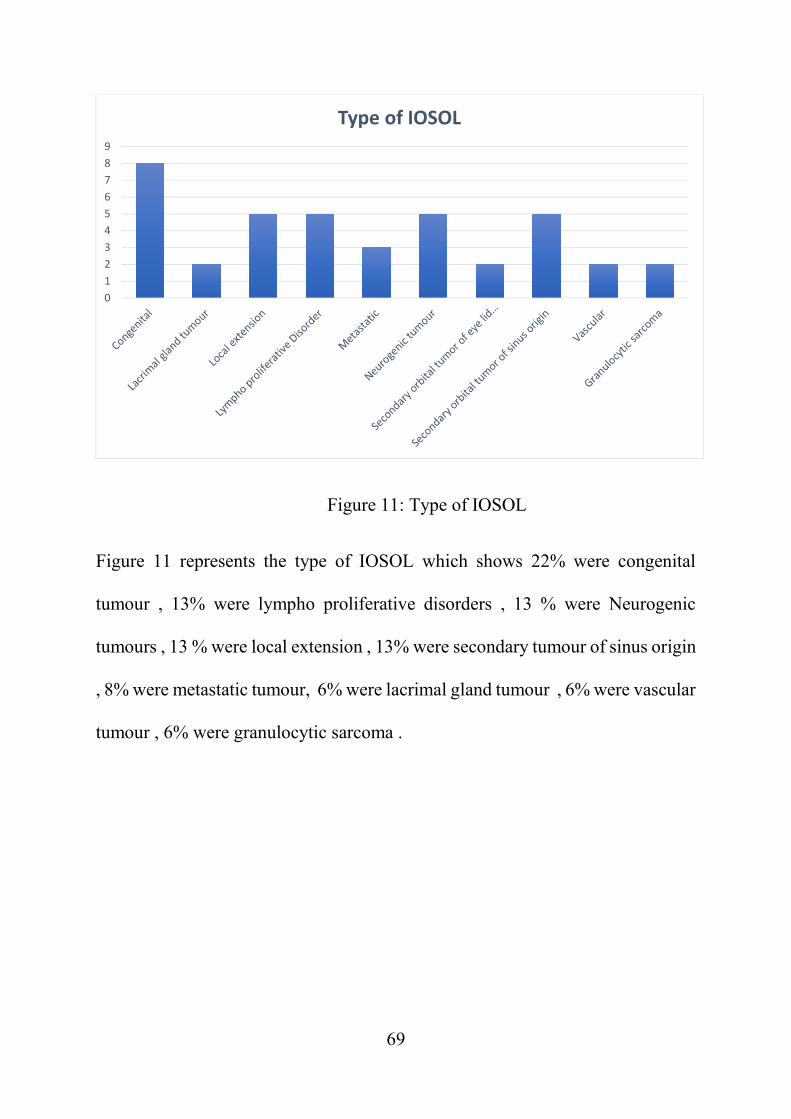
Figure 11: Type of IOSOL
Figure 11 represents the type of IOSOL which shows 22% were congenital
tumour , 13% were lympho proliferative disorders , 13 % were Neurogenic
tumours , 13 % were local extension , 13% were secondary tumour of sinus origin
, 8% were metastatic tumour, 6% were lacrimal gland tumour , 6% were vascular
tumour , 6% were granulocytic sarcoma .
0123456789
Type of IOSOL
70
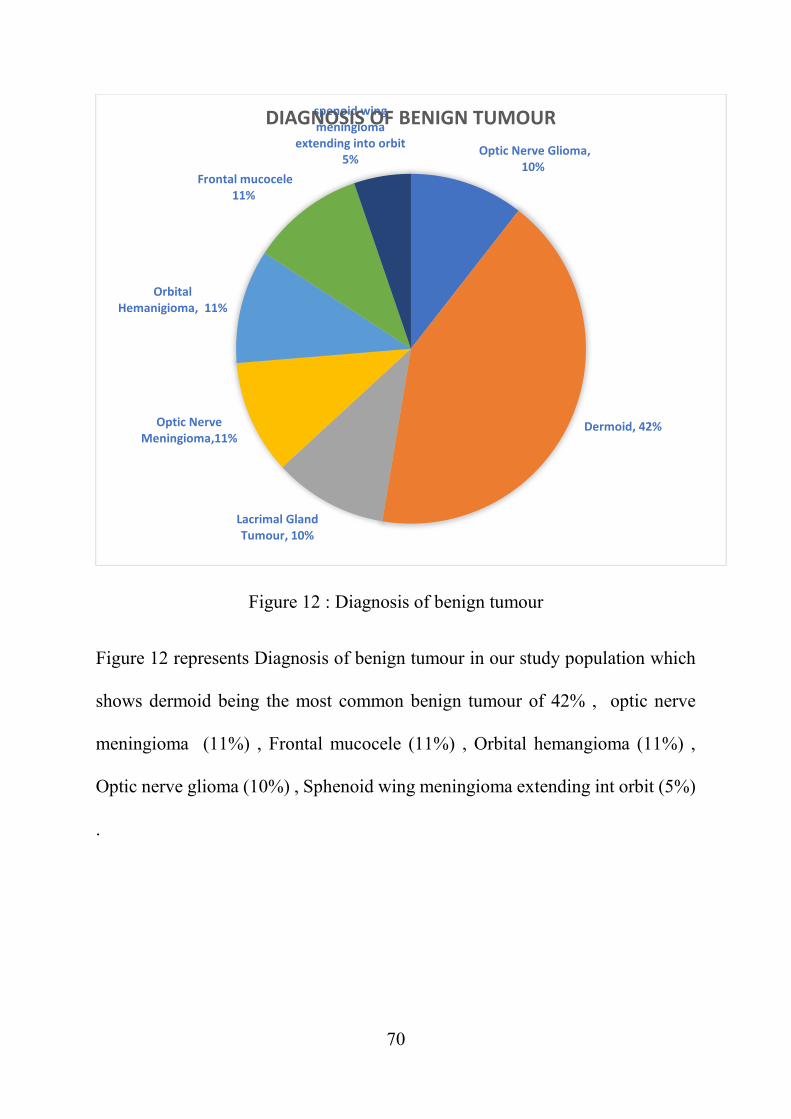
Figure 12 : Diagnosis of benign tumour
Figure 12 represents Diagnosis of benign tumour in our study population which
shows dermoid being the most common benign tumour of 42% , optic nerve
meningioma (11%) , Frontal mucocele (11%) , Orbital hemangioma (11%) ,
Optic nerve glioma (10%) , Sphenoid wing meningioma extending int orbit (5%)
.
Optic Nerve Glioma,10%
Dermoid, 42%
Lacrimal GlandTumour, 10%
Optic NerveMeningioma,11%
OrbitalHemanigioma, 11%
Frontal mucocele11%
spenoid wingmeningioma
extending into orbit5%
DIAGNOSIS OF BENIGN TUMOUR
71
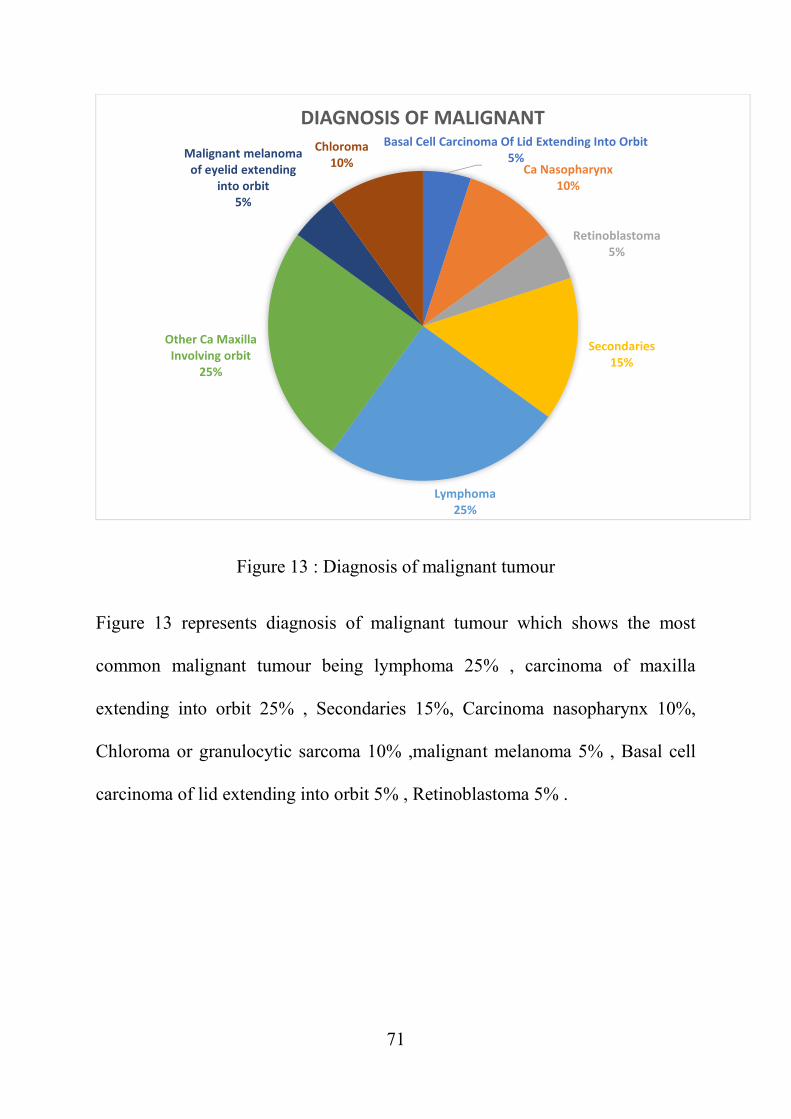
Figure 13 : Diagnosis of malignant tumour
Figure 13 represents diagnosis of malignant tumour which shows the most
common malignant tumour being lymphoma 25% , carcinoma of maxilla
extending into orbit 25% , Secondaries 15%, Carcinoma nasopharynx 10%,
Chloroma or granulocytic sarcoma 10% ,malignant melanoma 5% , Basal cell
carcinoma of lid extending into orbit 5% , Retinoblastoma 5% .
Basal Cell Carcinoma Of Lid Extending Into Orbit5%
Ca Nasopharynx10%
Retinoblastoma5%
Secondaries15%
Lymphoma25%
Other Ca MaxillaInvolving orbit
25%
Malignant melanomaof eyelid extending
into orbit5%
Chloroma10%
DIAGNOSIS OF MALIGNANT
72
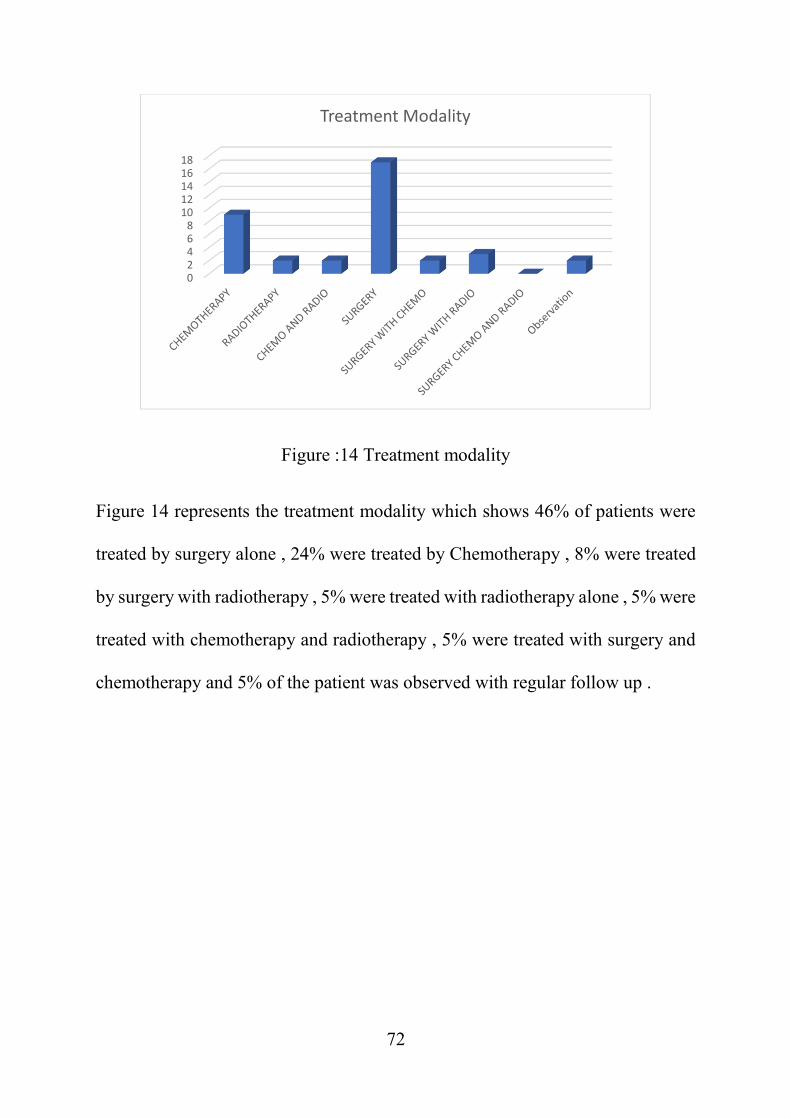
Figure :14 Treatment modality
Figure 14 represents the treatment modality which shows 46% of patients were
treated by surgery alone , 24% were treated by Chemotherapy , 8% were treated
by surgery with radiotherapy , 5% were treated with radiotherapy alone , 5% were
treated with chemotherapy and radiotherapy , 5% were treated with surgery and
chemotherapy and 5% of the patient was observed with regular follow up .
02468
1012141618
Treatment Modality
73
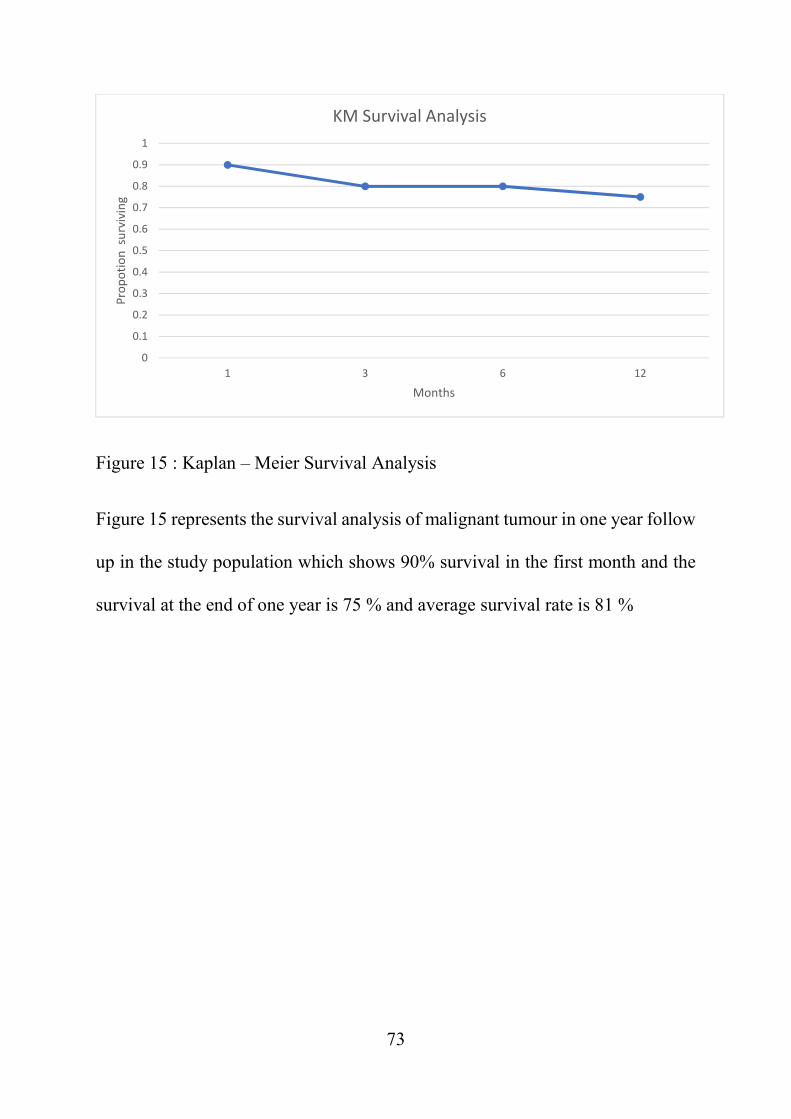
Figure 15 : Kaplan – Meier Survival Analysis
Figure 15 represents the survival analysis of malignant tumour in one year follow
up in the study population which shows 90% survival in the first month and the
survival at the end of one year is 75 % and average survival rate is 81 %
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
1 3 6 12
Prop
otio
n su
rviv
ing
Months
KM Survival Analysis
74
DISCUSSION
In my study the most common age group involved was 40-60 years. Females were
40% and males were 59% which is similar with study of Ralene et al[54] in which
53% were male .
In my study benign tumours were more common in patients less than 60 years of
age and malignant tumours were more common in patients above 60,
Out of the total IOSOL (Intraorbital space occupying lesions) 97.3% were
unilateral and only 2.7% were bilateral. In bilateral tumour, the neurofibromatosis
patient presented with bilateral optic nerve glioma.
In my study Right eye involvement was 51% and left eye involvement was 49%.
In my study , the most common clinical presentation was proptosis 46% followed
by orbital swelling 36% and the other presentation included watering (5%) , pain
(5%) , ptosis (5%) ,epistaxis (5%) , white reflex (5%) and growth in eyelid (5%)
which is similar to Mohammed Jaber Al-Mamoori et al[55] study in which the
most common clinical features at presentation was proptosis .
In my study most common (27%) presenting visual acuity is logmar 0.52-1 (<6/18
– 6/60) and the least common presenting visual acuity is no light perception.
Orbital retinoblastoma presented with visual acuity of no light perception.
The origin of tumour showed 49 % of tumours were arising from surrounding
tissues , 43% of tumours were primary and 8% were metastasis , from invasive
75
ductal carcinoma breast , Papillary carcinoma thyroid and small round cell
tumour of lung . Old age with history of lump in breast , visible thyroid swelling
, history of chronic cough with haemoptysis was present in patients with orbital
metastasis in my study .
Out of IOSOL (Intra orbital space occupying lesions) 72 % of tumours were
Extraconal mass , 13 % of tumours were intraconal and 15% of the tumours were
both intra and extraconal .Of which eccentric proptosis was 85% , axial proptosis
was 15% . Most of the extraconal lesions caused eccentric proptosis and
intraconal lesions caused axial proptosis with statistically significant p value of
<0.05.
Histopathology showed that 51% of the tumours were malignant and 49 % of
tumours were benign which is in accordance with the study by Geeta et al
[63]which showed 48% to be malignant and 52 % benign .
Of the benign tumour the most common tumour is dermoid (42%). Most of the
Dermoids are located in supero temporal quadrant which is same as the study
described by Mathew et al in which the most common occurrence of benign
tumour is supero temporal . In my study 50% of the patients with dermoid tumour
presented to us in the age group of 1- 10 years.
Of the malignant tumours the most common tumour is non-Hodgkins lymphoma
(25%) , which is similar to the Bonavolonta et al[50] study which showed the most
common malignant tumour being to be non-Hodgkin lymphoma of diffuse large
76
B cell type . PET scan was done to rule out systemic lymphoma. By
immunohistochemical marker study all the 4 non-Hodgkins lymphomas were
CD20 positive. patients treated with chemotherapy R-CHOP (Rituximab,
Cyclophosphamide, Hydroxydaunorubicin, Oncovin ,Prednisolone)regimen .
One patient recovered completely, two of them recovered with additional
radiotherapy and one patient died of systemic disease.
The only patient with orbital Retinoblastoma was presented with history of
swelling for 2 years duration and took native treatment and presented to us with
visual acuity of no light perception, we have treated the patient with 4 cycles of
chemotherapy of VEC (Vincristine, Etoposide and Carboplatin) regimen in the
interval of 21 days. The complications of chemotherapy like Hair loss, decreased
appetite has been observed. As per the suggested protocol in managing orbital
lymphoma by Santosh honavar et al[64] , the patient has been treated with 4 cycles
of neo adjuvant chemotherapy , followed by enucleation and there was no residual
tumour present .
The complications of Radiotherapy like Keratitis, Skin discolouration was
observed in 50% of the patients.
Survival analysis of malignant tumour in one year follow up was calculated using
Kaplan – meier survival index which showed 90% survival at the end of one
month and 75 % at the end of one yea . which differs from the study of devron et
al[65] which shows mean survival of patients was 1.3 years; the 2 year survival
77
rate was 27% . The good survival index in my study is possibly because of short
follow up period of one year and also the survival index was calculated for all the
malignant tumour in my study whereas in devron et al study only patients with
orbital metastasis was included.
78
CONCLUSION
In my study the most common age group involved is 40-60 years .
In my study males were more than females.
Most of the benign tumours presented under 60 years of age and most of the
malignant tumours above 60 years of age .
Most of the IOSOL (Intraorbital space occupying lesions ) are unilateral in
presentation .
There was no statistical significance in involvement of right eye or left eye .
In my study , the most common presenting complaint is proptosis . Rarely they
may also presented with epistaxis , Ptosis and white reflex as the only
presenting complaint .
Most of the patients presented with visual acuity of logmar 0.52-1 ( <6/18 –
6/60 ) and the least common is no light perception . The most common cause
for poor visual acuity of <6/60 is Optic nerve involvement and exposure
keratopathy .
Of the location of IOSOL , majority of the tumour are located in extraconal
space compared with intraconal space.
Both benign and malignant tumour were almost equal in number .
Most common benign tumour is Dermoid followed by optic nerve
meningioma .
Most common malignant tumour is lymphoma and maxillary carcinoma
extending into orbit .
79
Though Retinoblastoma is a rare tumour , timely diagnosis and management
is important to prevent distant metastasis.
Most of the patients were treated by surgery alone followed by chemotherapy
. The other treatment modalities were Radiotherapy , Chemotherapy with
radiotherapy , surgery with radiotherapy , surgery with chemotherapy , surgery
with chemotherapy and radiotherapy .
A multimodal workup protocol for IOSOL would ensure early definitive
diagnosis . The choice of appropriate treatment is the key to a good survival
rate as in our study .
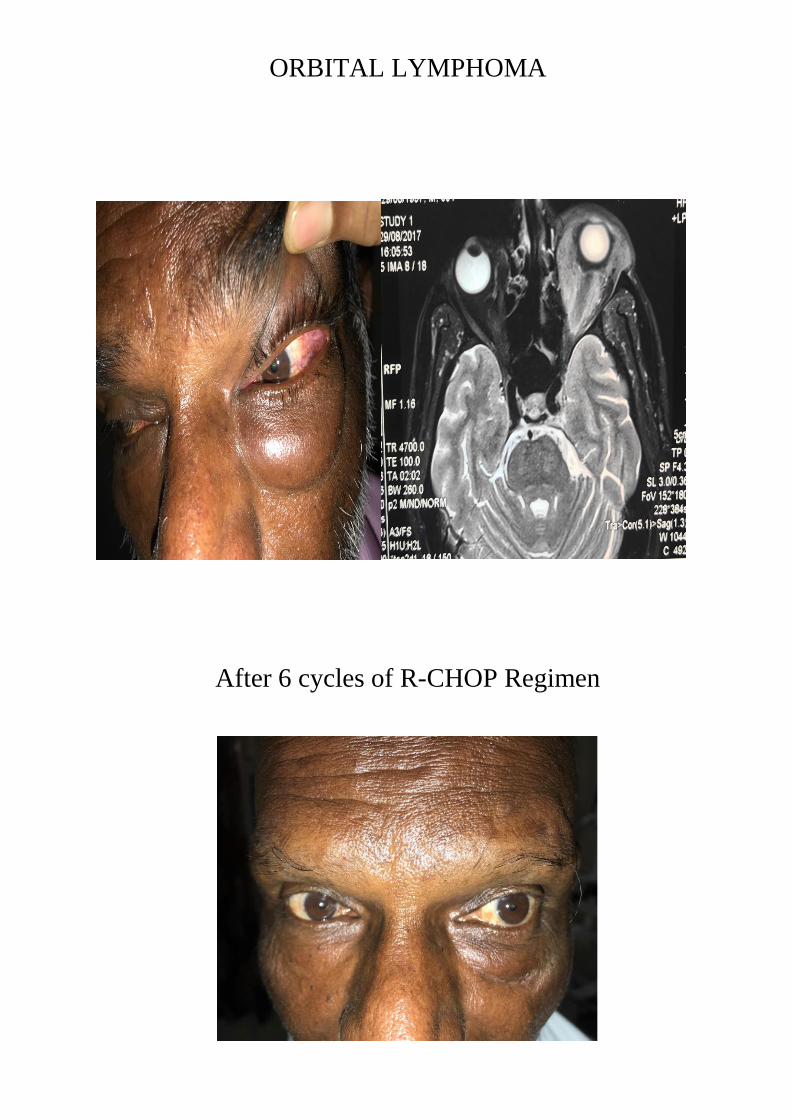
ORBITAL LYMPHOMA
After 6 cycles of R-CHOP Regimen
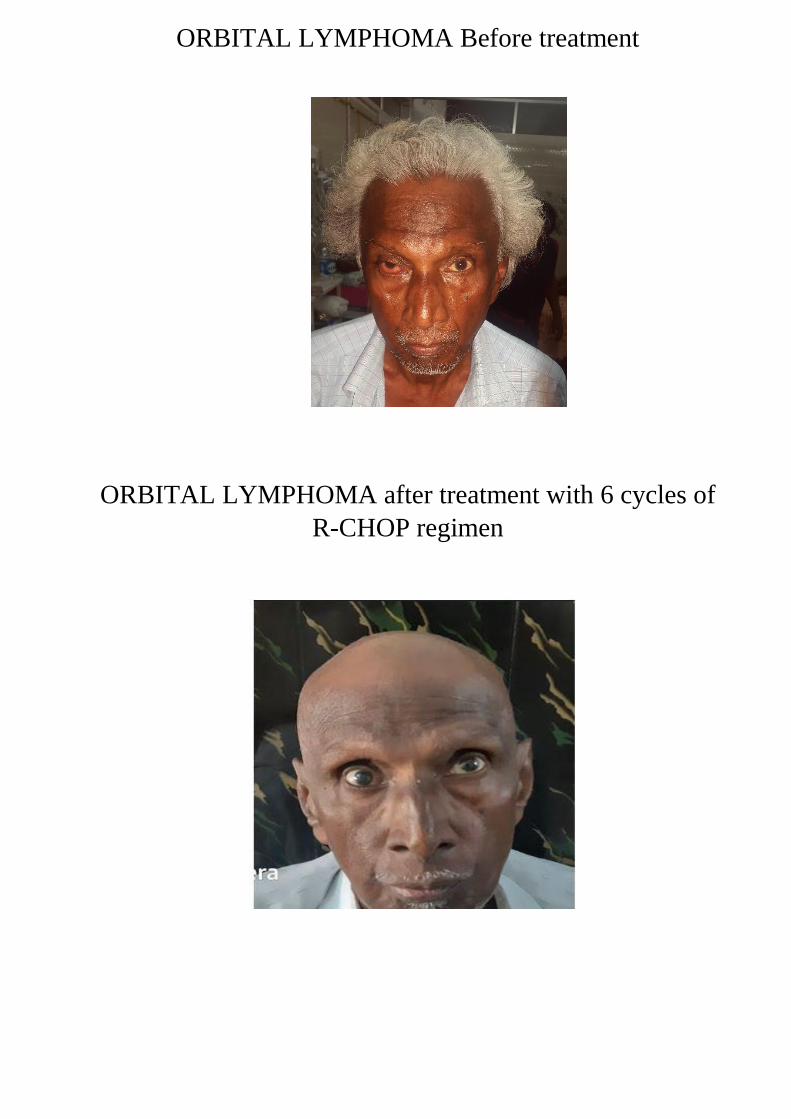
ORBITAL LYMPHOMA Before treatment
ORBITAL LYMPHOMA after treatment with 6 cycles of
R-CHOP regimen
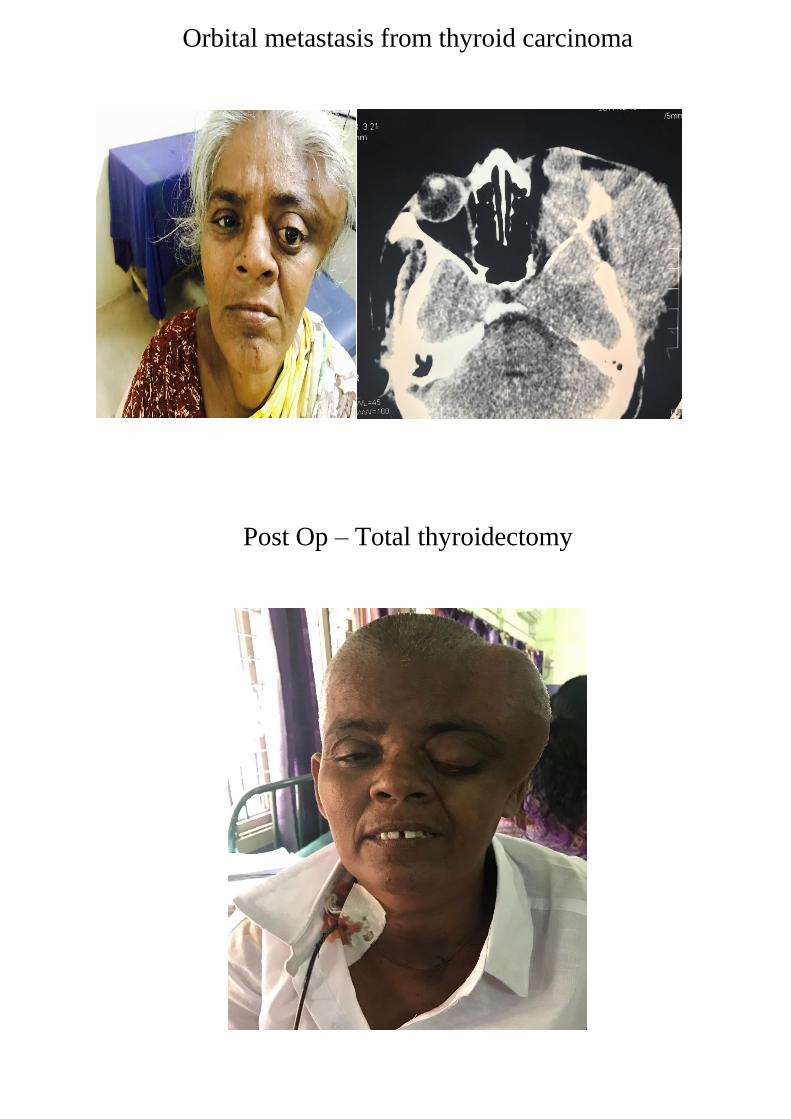
Orbital metastasis from thyroid carcinoma
Post Op – Total thyroidectomy
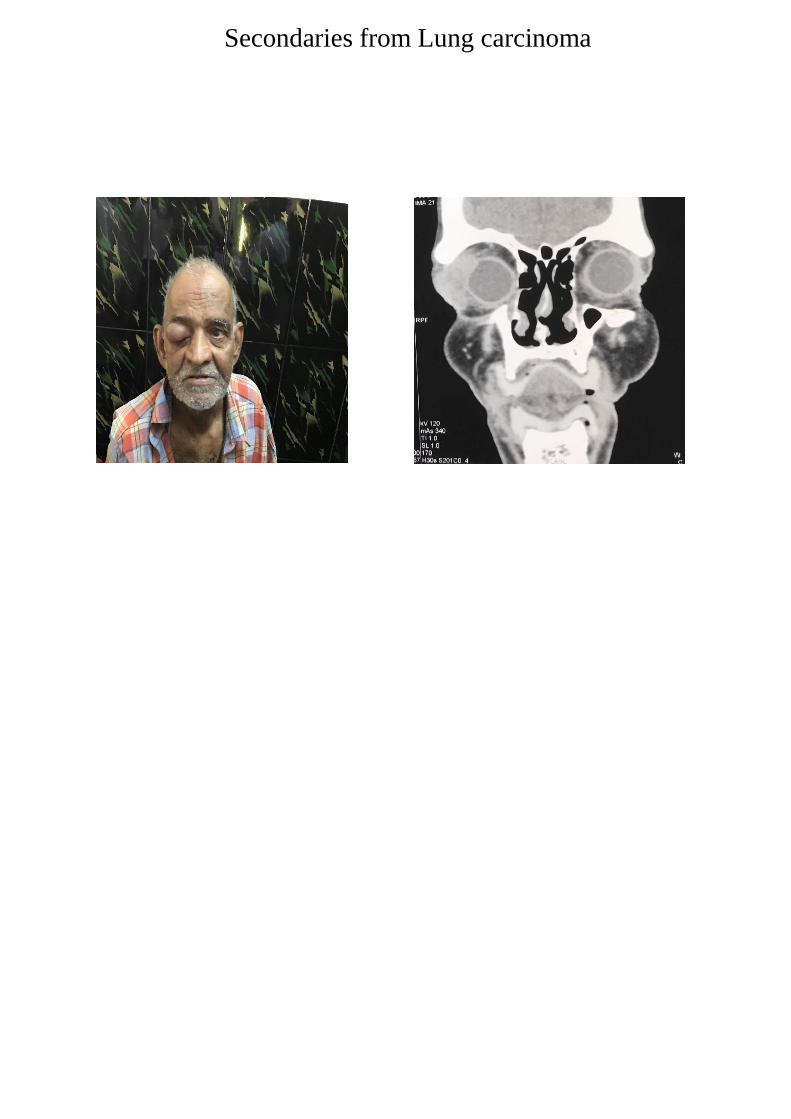
Secondaries from Lung carcinoma
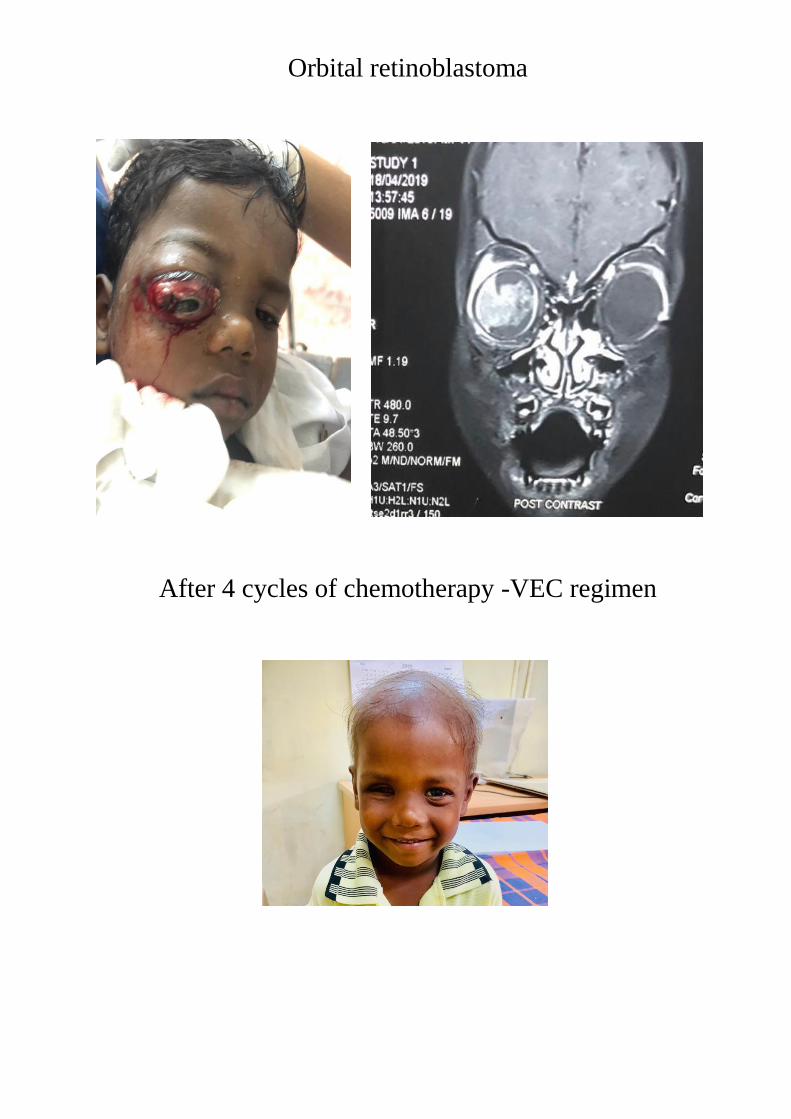
Orbital retinoblastoma
After 4 cycles of chemotherapy -VEC regimen
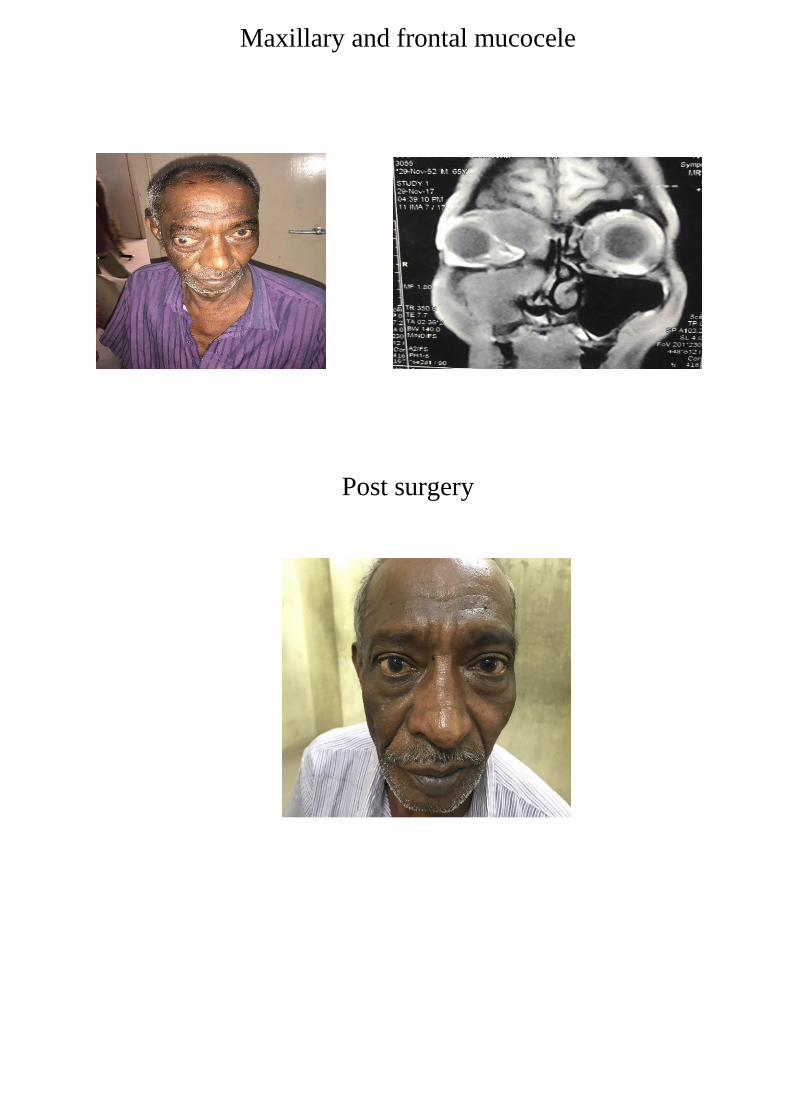
Maxillary and frontal mucocele
Post surgery
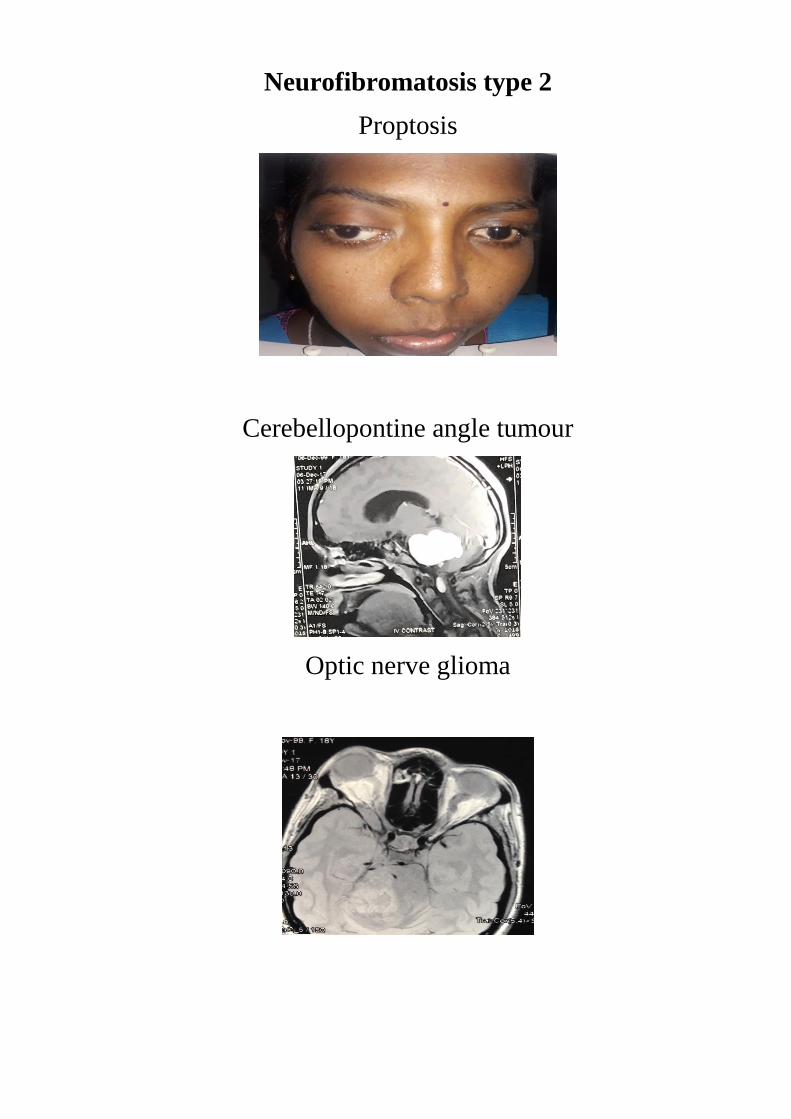
Neurofibromatosis type 2
Proptosis
Cerebellopontine angle tumour
Optic nerve glioma

Complications of Radiotherapy
Keratitis
Skin discolouration
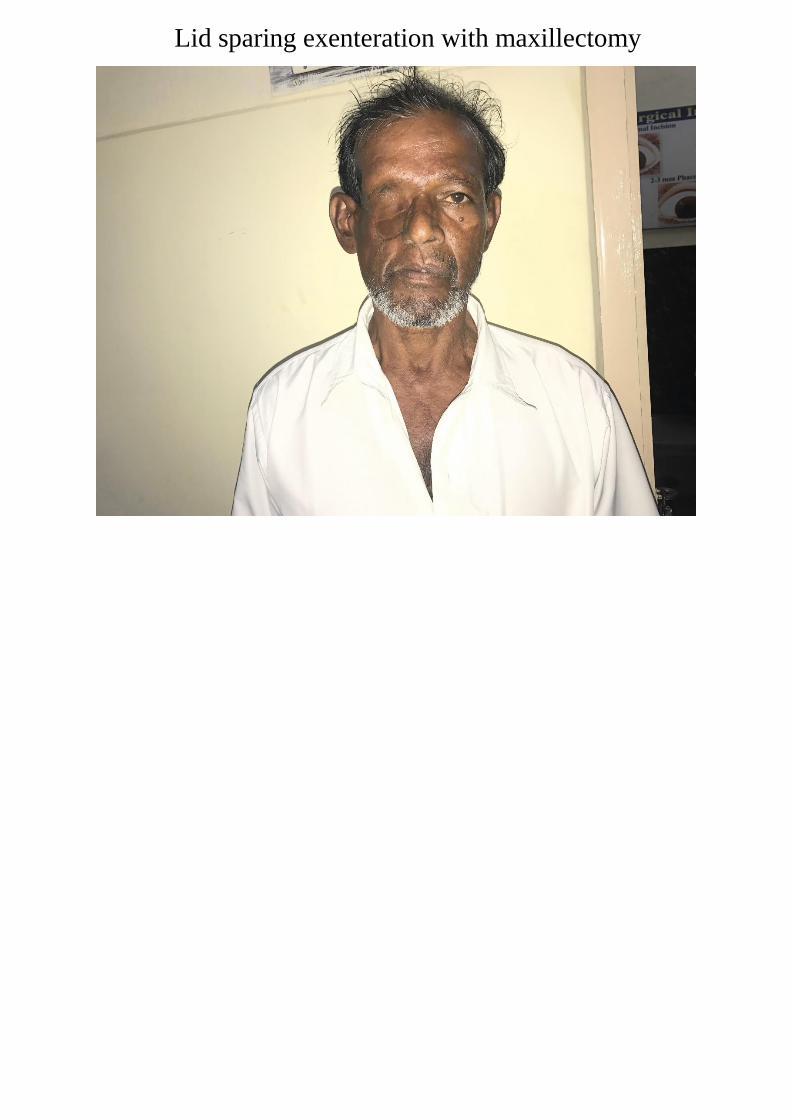
Lid sparing exenteration with maxillectomy
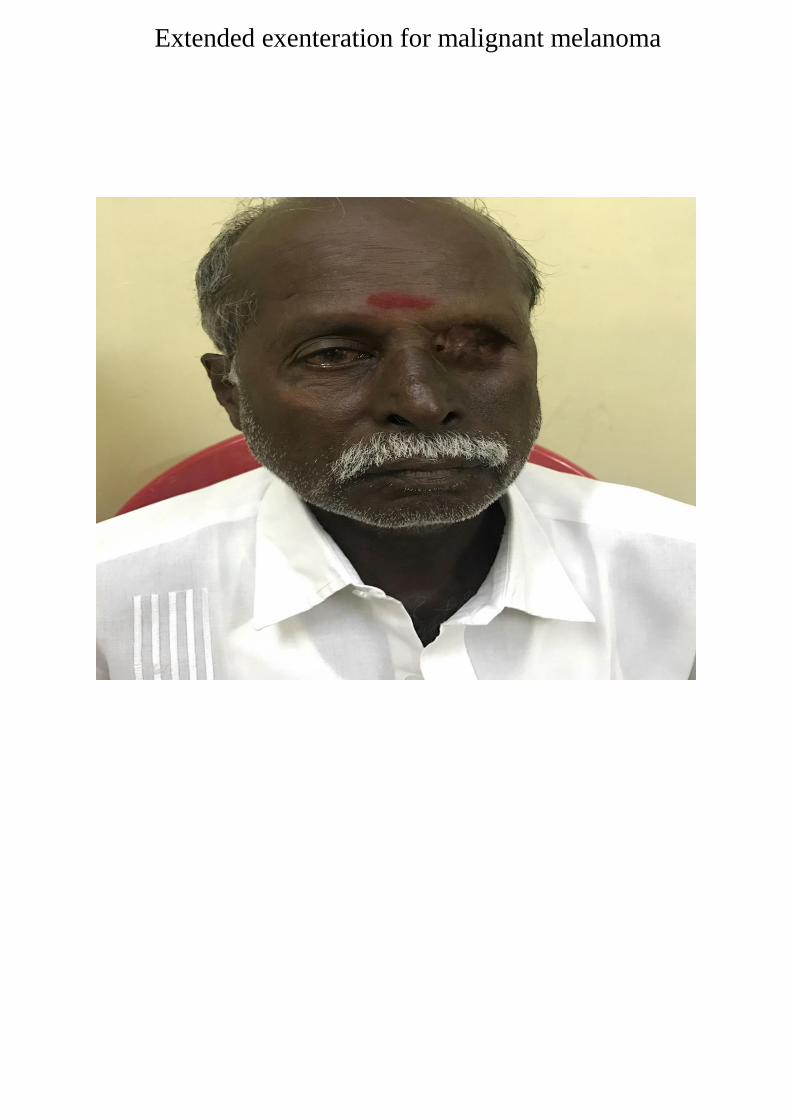
Extended exenteration for malignant melanoma
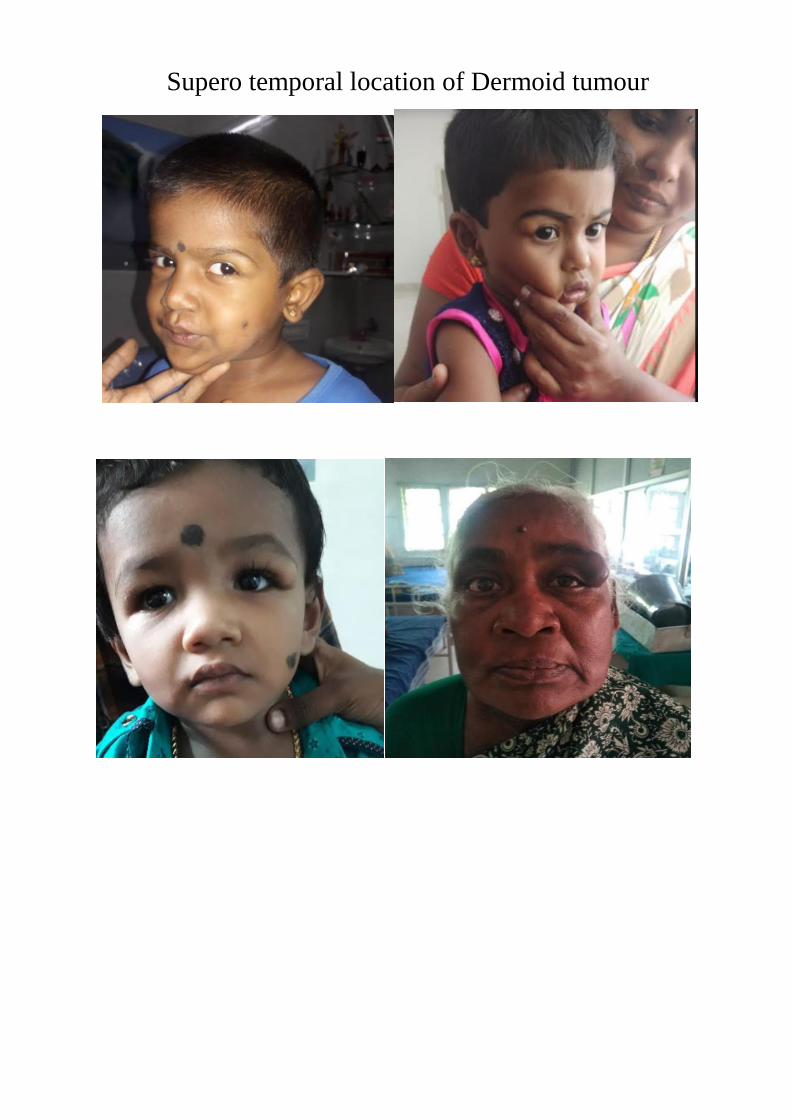
Supero temporal location of Dermoid tumour
BIBLIOGRAPGHY
1. American academy of ophthalmology Adel Alsuhaibani MD, Al Hatoon
Al Najashi Review:by Rona Z. Silkiss, MD, FACS on May 4
2. Henderson’s orbital tumors. Garrity, James A.; Henderson, James A.;
Cameron, J. Douglas
3. 2019Bron, A. J., Tripathi, R. C., Tripathi, B. J., & Wolff, E. (1997). Wolff's
anatomy of the eye and orbit. London: Chapman & Hall Medical.
4. Tandon R , (2014) .Parson's diseases of the eye. India. Elsevier
5. Cavazza S, Laffi GL, Lodi L, Gasparrini, Tassinari G. Orbital Dermoid
Cyst of Childhood: Clinical Pathologic Findings, Classification and
Management. Int Ophthalmol. 2011;31(3):93-97
6. Sherman RP, Rootman J, Lapointe JS. Orbital dermoids: clinical
presentation and management. Br J Ophthalmol. 1984;68: 642-652
7. Singh S, Dass R. The central artery of the retina I. Origin and course. Br J
Ophthalmol. 1960; 44: 193-212.
8. Ryan Machiele; Craig N. Czyz Anatomy, Head and Neck, Eye Lacrimal
Gland
9. Yanoff, M., Duker, J. S., & Augsburger, J. J. (2009). Ophthalmology.
Edinburgh: Mosby Elsevier.
10.Mafee M.F., Putterman A., Valvassori G.E., Campos M., Capek V. Orbital
space-occupying lesions: role of computed tomography and magnetic
resonance imaging. An analysis of 145 cases. Radiol Clin North
America. 1987;25(3):529–559.
11.Bisaria KK, Kumar N, Prakesh M, et al. The lateral rectus spine of the
superior orbital fissure. J Anat 1996;189(Pt 1):243–245
12.Turvey TA, Golden BA. Orbital anatomy for the surgeon. Oral Maxillofac
Surg Clin North Am 2012;24(4):525–536
13.Rhoton AL Jr, Natori Y. The Orbit and Sellar Region: Microsurgical
Anatomy and Operative Approaches. New York, NY: Thieme Medical;
1996
14.Rhoton AL Jr. Rhoton’s Cranial Anatomy and Surgical Approaches.
Baltimore, MD: Lippincott Williams & Wilkins; 2007
15.15.De Battista JC, Zimmer LA, Theodosopoulos PV, Froelich SC, Keller
JT. Anatomy of the inferior orbital fissure: implications for endoscopic
cranial base surgery. J Neurol Surg B Skull Base 2012;73(2): 132–138
16.Markiewicz MR, Dierks EJ, Bell RB. Does intraoperative navigation
restore orbital dimensions in traumatic and post-ablative defects? J
Craniomaxillofac Surg 2012;40(2):142–148
17.Strong EB, Fuller SC, Chahal HS. Computer-aided analysis of orbital
volume: a novel technique. Ophthal Plast Reconstr Surg 2013; 29(1):1–5
18.Schmelzeisen R, Gellrich NC, Schoen R, Gutwald R, Zizelmann C,
Schramm A. Navigation-aided reconstruction of medial orbital wall and
floor contour in cranio-maxillofacial reconstruction. Injury
2004;35(10):955–962
19.Snyderman CH, Harvey RJ. Skull base: meeting place for multidisciplinary
collaboration. Otolaryngol Clin North Am 2011;44(5): xi–xii
20.Snyderman CH, Pant H, Carrau RL, Prevedello D, Gardner P, Kassam AB.
What are the limits of endoscopic sinus surgery?: the expanded endonasal
approach to the skull base. Keio J Med 2009;58(3): 152–160
21.Manson PN, Grivas A, Rosenbaum A, Vannier M, Zinreich J, Iliff N.
Studies on enophthalmos: II. The measurement of orbital injuries and their
treatment by quantitative computed tomography. Plast Reconstr Surg
1986;77(2):203–214
22.Chung EM, Smirniotopoulos JG, Specht CS, Schroeder JW, Cube R. From
the archives of the AFIP: Pediatric orbit tumors and tumorlike lesions:
nonosseous lesions of the extraocular orbit. Radiograph: A Rev Publ
Radiol Soc North America, Inc. 2007;27(6):1777–99.
23.Bisdorff A, Mulliken JB, Carrico J, Robertson RL, Burrows PE.
Intracranial vascular anomalies in patients with periorbital lymphatic and
lymphaticovenous malformations. AJNR Am J Neuroradiol
2007;28(2):335–41.
24.Mafee MF, Goodwin J, Dorodi S. Optic nerve sheath meningiomas. Role
of MR imaging. Radiol Clin North America 1999;37(1):37–58 ix.
25.Westacott S, Garner A, Moseley IF, Wright JE. Orbital lymphoma versus
reactive lymphoid hyperplasia: an analysis of the use of computed
tomography in differential diagnosis. The Brit J
Ophthalmol 1991;75(12):722–5.
26.Hosten N, Schorner W, Zwicker C, et al. Lymphocytic infiltrations of the
orbit in MRT and CT. Lymphoma, pseudolymphoma and inflammatory
pseudotumor. RoFo: Fortschritte auf dem Gebiete der Rontgenstrahlen und
der Nuklearmedizin 1991;155(5):445–51.
27.Issing PR, Ruh S, Kloss A, Kuske M, Lenarz T. Diagnosis and therapy of
lymphoid tumors of the orbits. Hno 1997;45(7):545–50.
28.Sohaib SA, Moseley I, Wright JE. Orbital rhabdomyosarcoma – the
radiological characteristics. Clin Radiol 1998;53(5):357–62.
29.Folpe AL, McKenney JK, Bridge JA, Weiss SW. Am J Surg
Pathol 2002;26(9):1175–83.
30.Mafee MF, Pai E, Philip B. Rhabdomyosarcoma of the orbit. Evaluation
with MR imaging and CT. Radiol Clin North America
1998;36(6):1215–27 xii.
31.Cota N, Chandna A, Abernethy LJ. Orbital abscess masquerading as a
rhabdomyosarcoma. J AAPOS: The Off Publ Am Assoc Pediatr
Ophthalmol Strab/Am Assoc Pediatr Ophthalmol Strab
2000;4(5):318–20.
32.Sepahdari AR, Aakalu VK, Kapur R, et al. MRI of orbital cellulitis and
orbital abscess: the role of diffusion-weighted imaging. AJR Am J
Roentgenol 2009;193(3):W244–50.
33.Holman RE, Grimson BS, Drayer BP, Buckley EG, Brennan MW.
Magnetic resonance imaging of optic gliomas. Am J Ophthalmol
1985;100(4):596–601.
34.Weber AL, Klufas R, Pless M. Imaging evaluation of the optic nerve and
visual pathway including cranial nerves affecting the visual pathway.
Neuroimag Clin North America 1996;6(1):143–77.
35.Tyers AG. Orbital exenteration for invasive skin tumours. Eye
2006;20:1165–70.
35.Fuss M, Hug EB, Schaefer RA, et al. Proton radiation therapy (PRT) for
pediatric optic pathway gliomas: comparison with 3D planned
conventional photons and a standard photon technique. Int J Radiat Oncol
Biol Phys. 1999;45(5):1117—26
36.Combs SE, Behnisch W, Kulozik AE, et al. Intensity Modulated
Radiotherapy (IMRT) and Fractionated Stereotactic Radiotherapy (FSRT)
for children with head- and-neck-rhabdomyosarcoma. BMC Cancer.
2007;7:177
37.Schuller DE, Lawrence TL, Newton WA Jr. Childhood
rhabdomyosarcomas of the head and neck. Arch Otolar- yngol.
1979;105(12):689—94
38.Anteby I, Ramu N, Gradstein L, et al. Ocular and orbital complications
following the treatment of retinoblastoma. Eur J Ophthalmol.
1998;8(2):106—11
39.Finger PT. Anti-VEGF bevacizumab (Avastin) for radia- tion optic
neuropathy. Am J Ophthalmol. 2007;143(2): 335—8
40.Pradhan DG, Sandridge AL, Mullaney P, et al. Radiation therapy for
retinoblastoma: a retrospective review of 120 patients. Int J Radiat Oncol
Biol Phys. 1997;39(1):3—13
41.Schipper J, Tan KE, van Peperzeel HA. Treatment of retinoblastoma by
precision megavoltage radiation therapy. Radiother Oncol.
1985;3(2):117—32
42.Merriam GR Jr. A clinical study of radiation cataracts. Trans rAm
Ophthalmol Soc. 1956;54:611—53
43.Merriam GR Jr, Focht EF. A clinical study of radiation cataracts and the
relationship to dose. Am J Roentgenol Radium Ther Nucl Med.
1957;77(5):759--85l
44.Sagerman R, Alberti WE. Radiosensitivity of ocular and orbital structures.
In Sagerman RH, Alberti WE (eds): Radiotherapy of Intraocular and
Orbital Tumors. Berlin,, Springer, 2003, pp. 269—80
45.Abramson DH, Ellsworth RM, Kitchin FD, Tung G. Second nonocular
tumors in retinoblastoma survivors. Are they radiation-induced?
Ophthalmology. 1984;91(11):1351—5
46.Sagerman RH, Cassady JR, Tretter P, Ellsworth RM. Radiation induced
neoplasia following external beam therapy for children with
retinoblastoma. Am J Roentgenol Radium Ther Nucl Med.
1969;105(3):529—35.
47.Orbital space-occupying lesions: an 11-year study of cases with
histopathologic analysis seen at Hospital das Clínicas of FMUSP.
48.J Pediatr Ophthalmol Strabismus. 2007 Mar-Apr;44(2):106-11.
Orbital space-occupying lesions in Indian children.
49.Bonavolontà G, Strianese D, Grassi P, et al. An analysis of 2,480
spaceoccupying lesions of the orbit from 1976 to 2011. Ophthal Plast
Reconstr Surg. 2013;29:79-86
50.Study sheds light on space-occupying lesions Written By: Matthew W.
Wilson, MD, FACS Ocular Pathology/Oncology
51.Radiographics. 2013 Oct;33(6):1739-58. doi:10.1148/rg.336135502.
Orbital neoplasms in adults: clinical, radiologic, and pathologic review.
Tailor TD1, Gupta D, Dalley RW, Keene CD, Anzai Y.
52.Orbital masses: CT and MRI of common vascular lesions, benign
tumors, and malignancies . Sarah N. Khan and Ali R. Sepahdari .
53.Clinical, radiological and histological correlation in diagnosis of orbital
tumours . Ralene Sim, Stephanie Ming Young , Rupesh Agrawal and
Gangadhara Sundar .
54.Orbital tumors: A prospective study of 95 cases Mohammed Jaber Al-
Mamoori . DOI: 10.4103/MJBL.MJBL_69_18 .
55.McNab AA, Selva D, Hardy TG, et al. The anatomical location and
laterality of orbital cavernous haemangiomas. Orbit. 2014;33:359-362.
56.Gensheimer MF, Rainey D, Douglas JG, et al. Neutron radiotherapy for
adenoid cystic carcinoma of the lacrimal gland. Ophthal Plast Reconstr
Surg. 2013;29:256-260.
57.Isaacson PG, Wright DH. Malignant lymphoma of mucosal associated
lymphoid tissue: a distinctive type of B cell
lymphoma. Cancer. 1983;52:1410–1416. doi: 10.1002/1097-
0142(19831015)52:8<1410::AID-CNCR2820520813>3.0.CO;2-3.
58.Ozgur OK, Yin V, Chou E, et al. Hedgehog pathway inhibition for locally
advanced periocular basal cell carcinoma and basal cell nevus
syndrome. Am J Ophthalmol. 2015;160:220-227.
59.Tuncer S, Tanyıldız B, Basaran M, et al. Systemic rituximab
immunotherapy in the management of primary ocular adnexal lymphoma:
single institution experience. Curr Eye Res. 2015;40:780-785 Orbital
tumors in the older adult population .
60.Recent Developments in Retinoblastoma . Raksha Rao, Santosh G
Honavar . DOI:http://dx.doi.org/10.7869/djo.206 .
61.Hakan Demirci, MD1, Carol L Shields, MD , Jerry A Shields,
MD1, Santosh G Honavar, MD1, Gary J Mercado, MD2, Jose C Tovilla,
MD1
62.Rapid intraoperative diagnosis of tumors of the eye and orbit by squash
and imprint cytology . Geeta Kashyap Vemuganti, MD , Milind N Naik,
MD2, Santosh G Honavar, MD2, G.Chandra Sekhar, MD2
63.Orbital retinoblastoma: An update Santosh G Honavar1, Fairooz P
Manjandavida2, Vijay Anand P Reddy .
64.Orbital metastases: diagnosis and course Devron H Chara, Theodore
Millerb, Stewart Krolla .
PATIENT ID DATE
AGE
1. <1
2. 1-10 years
3. 11-20 years
4. 21-40 years
5. 40-60 years
6. > 60 years
SEX
1. Male
2 . Female
PRESENTING COMPLAINTS
Pain
proptosis
Loss of vision
Dilopia
Proptosis
Duration (DAYS/WEEKS/MONTHS/YEARS)
Unilateral or Bilateral
onset: Insidious or sudden
Progression/stationary/regression
Constant/Intermittent
Variation of proptosis :postural variation or cough or strain
Aggravating or Relieving factors
Assosiated "swishing sound "
Pain
Duration and relation to onset of proptosis(DAYS/WEEKS/MONTHS/YEARS)
site
RAdiation
Character
Aggravating and releiving factors
Relation to eye movement
Vision loss
Duration and relation to proptosis (DAYS/WEEKS/MONTHS/YEARS)
ONset:Insidious or sudden
Progression :Raid or slow
Gaze evoked amarousis
Diplopia
Duration and relation to proptosis (DAYS/WEEKS/MONTHS/YEARS)
Monocular or binocular
Horizontal or vertical
Variablity
Maximum fied of diplopia
Ptosis
lid retraction
Edema
Redness
Watering
Phoophobia
Infraorbital tingling numbness
Swelling elsewhere on body
Trauma
CNS:Headache,nausea,vomiting,convulsion,ataxia
Focal sepsis :
Boil on eyelid
Dacrocystitis :swelling near medial canthus ,discharge,matting of lashes
Sinusitis :Headache,nasal stuffiness or discharge , fever
Tooth pain
EAR: discharge,tinnitus,hearing loss
PAST HISTORY
DIabetes / HT
medical h/o
ocular h/o
previous surgeries
Personal history
Weight loss
Family history
EXAMINATION:
General apperance
vitals:pulse BP Respiratory rate
Pallor,Icterus,Cyanosis,Edema
Lymph nodes
Thyroid
Skin:Naevi,cafe-au-lait,port wine stain
Systemic examination:
ENT
CNS
Breast
Thyroid
CVS
RS
ABDOMEN
MUSCULOSKELETAL
OCULAR EXAMINATION
1.General ocular examination
Head posture
Ocular posture
Fascial assymetry
2.Examination of proptosis
INSPECTION
Unilateral or Bilateral
Axial or Eccentric
Visible pulsatility
change with valsalva ,cough or posture
Lid position: Retraction or Ptosis
Lid fullness
Skin over the Lid :INflammation/Pigmentation/Ecchymosis/venousdilatation
PALPATION
Rise in tmperature
Tenderness
Pulsatility
Thrill
Mass palpated :
size and shape
Discrete/Ill defined
Margins
Consistency
Compressibility
Insunuation
Resistance to retropulsion of globe
Auscultation over orbit
Exophthalmometry
Mild proptosis
Moderate proptosis
Severe proptosis
DETAILED OCULAR EXAINATION
Visual acuity
Colour vision
Field
eyelid : PFH
Lagophthalmos(lid closture /Blink rate )
Eyelid sensation
Bells phenomnon
lid signs of thyroid
Conjunctiva (chemosis ,congestion ,hemorrhage ,conjunctival extension oftumours )
cornea (size ,clarity ,kp ,staining ,sensation)
AC (depth , cells/flare )
Iris (colour,pattern,atrophy,neovascularisation)
Pupil :Rapd ,light near dissosisation
lens
Fundus :
Direct ,IDO
Disc edema , Optic atrophy
Posterior pole indentation
Choroidal folds
Optociliary shunts
Torturous vessels
Refraction
Ocular motility : DUCTIONS AND VERSIONS
IOP :straight ahead gaze
: In upgaze for thyroid ophthamopathy
Diplopia charting
Investigations
1. Complete blood count
2.ESR
3. Random blood sugar
4. Thyroid function test
5. Chest X ray
6. Bscan
7. CT orbit
7. MRI orbit
8.PET scan
9.Histopathology
Treatment
1.Observation
2.Medical
3.Surgery
4.Radiotherapy
5.Chemotherapy
Follow up
1. 1month
Visual acuity
colour vision
Eom Fundus
2. 3 month
3. 6month
4. 1 year

MASTER CHART EXPLANATION
1.SEX
FEMALE 1
MALE 2
AGE
<1 1
1 to 10 2
11 to 20 3
21 to 40 4
40 to 60 5
>60 6
2.COMPLAINTS
Proptosis 1
Loss of vision 2
Diplopia 3
Pain 4
PTOSIS 5
swelling 6
Watering 7
Epistaxis 8
White reflex 9
Growth in eyelid 10
3.DURATION
Days 1
Weeks 2
Months 3
Years 4
4.laterality
Unilateral 1
Bilateral 2
5.ONSET
Insidious 1
Sudden 2
6.COURSE
Progression 1
Stationary 2
Regression 3
7 Types of Tumor
Constant 1
Intermittent 2
PAST HISTORY
Systemic illness no 1
DIABETIC 2
HT 3
CAD 4
TB 5
THYROID 6
CVA 7
BREAST carcinoma 8
Blood malignancy 9
Lung carcinoma 10
Brain tumour 11
PERSONAL HISTORY
Weight loss yes 2
Weight loss no 1
Family history
YES 2
NO 1
GENERAL EXAMINATION
Vitals
Normal 1
Abnormal 2
LYMPHNODES
NO 1
YES 2
Submental and submandibular 3
Upper deep cervical 4
Middle deep cervical 5
Lower deep cervical 6
Posterior triangle lymphnodes 7
Pretracheal prelaryngeal 8
Superior mediastenial nodes 9
Distant lymphnode involvement 10
PALLOR
NO 1
YES 2
CYANOSIS
NO 1
YES 2
CLUBBING ,ICTERUS, EDEMA
NO 1
YES 2
THYROID
NORMAL 1
ABNORMAL 2
BREAST
NORMAL 1
ABNORMAL 2
SKIN
NORMAL 1
ABNORMAL 2
CAFÉ LU SPOTS 1
NEUROFIBROMA 2
Edema 3
OCULAR EXAMINATION
1.GENERAL
Head posture normal 1
Head posture abnormal 2
Ocular posture normal 1
Ocular posture abnormal 2
Facial asymmetry normal 1
Facial asymmetry abnormal 2
INSPECTION
proptosis
Unilateral 1
Bilateral 2
No proptosis 3
Axial 1
Eccentric 2
No proptosis 3
Visible pulsation NO 1
Visible pulsation YES 2
CHANGE WITH VALSALVA NO 1
CHANGE WITH VALSALVA YES 2
SKIN OVER THE LID NORMAL 1
SKIN OVER THE LID ABNORMAL 2
INFLAMMATION 1
PIGMENTATION 2
ECCHYMOSIS 3
VENOUS DILATATION 4
ULCER 5
PALPATION
RISE IN TEMPERATURE 1
TENDERNESS 2
PULSALITITY 3
THRILL 4
Compressibility
yes 1
no 2
Insinuation
yes 1
no 2
Resistance to retropulsion
NO 1
Yes 2
EXOPHTHALMOMETRY
No proptosis 1
Mild proptosis 2
Moderate proptosis 3
Severe proptosis 4
DETAILED OCULAR EXAMINATION
VISUAL ACUITY in log mar
0.00 - 0.50 00.52 – 1 11.02 - 1.30 21.32 - 1.80 31.82 - 3.0 44 5
COLOUR VISION
NORMAL 1
DEFECTIVE 2
COULD NOT BE CHECKED 3
FIELD
NORMAL 1
DEFECTIVE 2
COULD NOT BE CHECKED 3
EYELID
LAGOPHTHALMOS YES 1
LAGOPHTHALMOS NO 2
BELLS INTACT 1
BELLS DEFECTIVE 2
Conjunctiva
Normal 1
chemosis 2
hemorrhage 2
Congestion 3
sch 4
CORNEA NORMAL 1
CORNEA ABNORMAL 2
AC NORMAL 1
AC ABNORMAL 2
PUPIL NORMAL 1
PUPIL ABNORMAL 2
LENS NORMAL 1
LENS ABNORMAL 2
FUNDUS NORMAL 1
FUNDUS ABNORMAL 2
COULD NOT BE CHECKED 3
IOP NORMAL 1
IOP ABNORMAL 2
EOM FULL 1
EOM DEFECT 2
DIAGNOSIS
Normal 0
OPTIC NERVE GLIOMA 1
SECONDARIES 2
LYMPHOMA 3
DERMOID 4
OTHER CA MAXILLA INVOLVING 0RBIT 5
Orbital hemanigioma 6
Lacrimal gland tumour 7
Ca nasopharynx extendinginto orbit 8
Retinoblastoma 9
Optic nerve meningioma 10
Basal cell carcinoma of lid extending into orbit 11
Frontal mucocele 12
Malignant melanoma of eyelid extending into orbit 13
Spenoid wing meningioma 14
Chloroma 15
TREATMENT
CHEMOTHERAPY 1
RADIOTHERAPY 2
CHEMO AND RADIO 3
SURGERY 4
SURGERY WITH CHEMO 5
SURGERY WITH RADIO 6
SURGERY CHEMO AND RADIO 7
Observation 8
FOLLOW UP
1 MONTH
3 MONTHS
6 MONTHS
1 YEAR
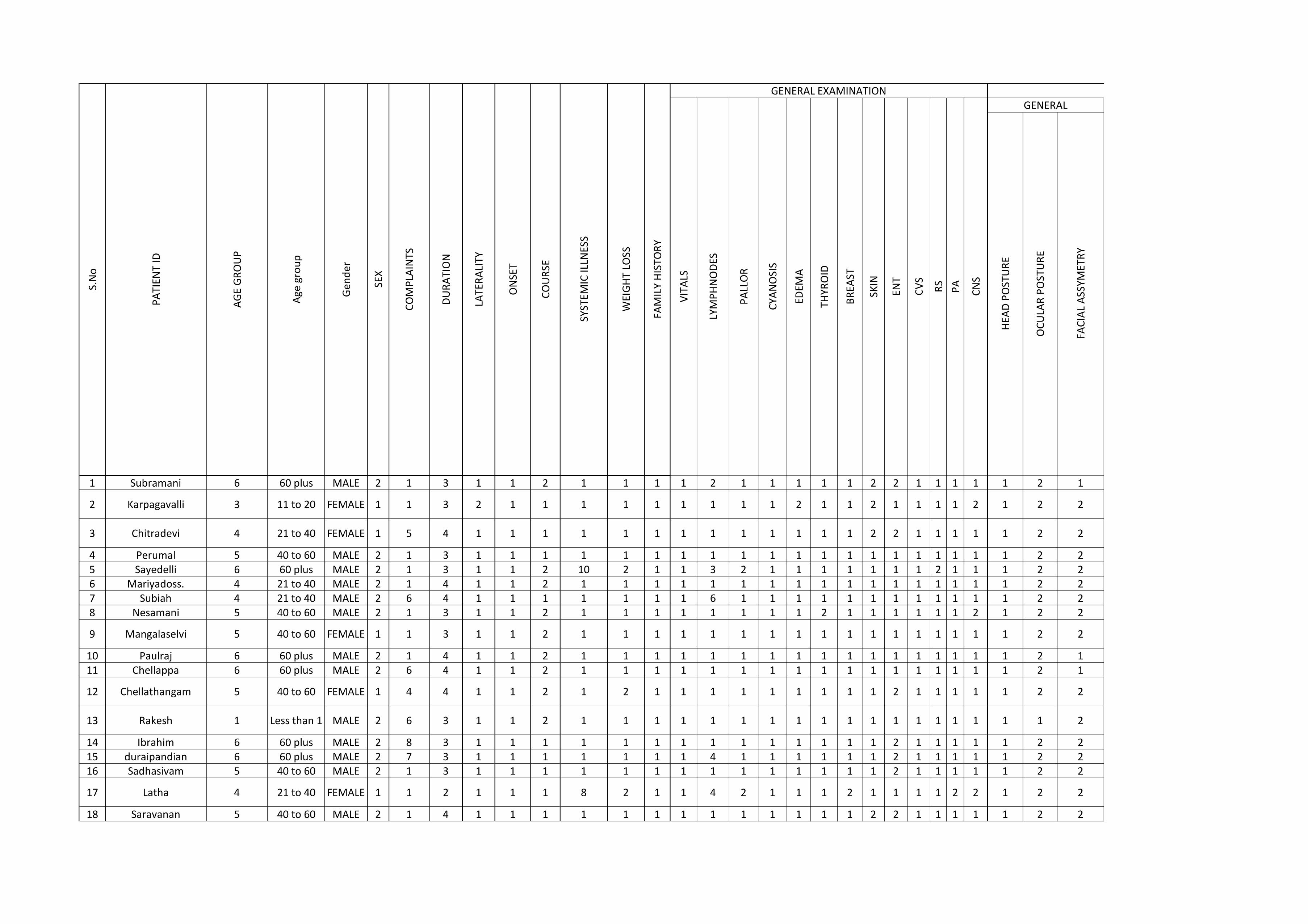
1 Subramani 6 60 plus MALE 2 1 3 1 1 2 1 1 1 1 2 1 1 1 1 1 2 2 1 1 1 1 1 2 1
2 Karpagavalli 3 11 to 20 FEMALE 1 1 3 2 1 1 1 1 1 1 1 1 1 2 1 1 2 1 1 1 1 2 1 2 2
3 Chitradevi 4 21 to 40 FEMALE 1 5 4 1 1 1 1 1 1 1 1 1 1 1 1 1 2 2 1 1 1 1 1 2 2
4 Perumal 5 40 to 60 MALE 2 1 3 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 2 25 Sayedelli 6 60 plus MALE 2 1 3 1 1 2 10 2 1 1 3 2 1 1 1 1 1 1 1 2 1 1 1 2 26 Mariyadoss. 4 21 to 40 MALE 2 1 4 1 1 2 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 2 27 Subiah 4 21 to 40 MALE 2 6 4 1 1 1 1 1 1 1 6 1 1 1 1 1 1 1 1 1 1 1 1 2 28 Nesamani 5 40 to 60 MALE 2 1 3 1 1 2 1 1 1 1 1 1 1 1 2 1 1 1 1 1 1 2 1 2 2
9 Mangalaselvi 5 40 to 60 FEMALE 1 1 3 1 1 2 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 2 2
10 Paulraj 6 60 plus MALE 2 1 4 1 1 2 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 2 111 Chellappa 6 60 plus MALE 2 6 4 1 1 2 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 2 1
12 Chellathangam 5 40 to 60 FEMALE 1 4 4 1 1 2 1 2 1 1 1 1 1 1 1 1 1 2 1 1 1 1 1 2 2
13 Rakesh 1 Less than 1 MALE 2 6 3 1 1 2 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 2
14 Ibrahim 6 60 plus MALE 2 8 3 1 1 1 1 1 1 1 1 1 1 1 1 1 1 2 1 1 1 1 1 2 215 duraipandian 6 60 plus MALE 2 7 3 1 1 1 1 1 1 1 4 1 1 1 1 1 1 2 1 1 1 1 1 2 216 Sadhasivam 5 40 to 60 MALE 2 1 3 1 1 1 1 1 1 1 1 1 1 1 1 1 1 2 1 1 1 1 1 2 2
17 Latha 4 21 to 40 FEMALE 1 1 2 1 1 1 8 2 1 1 4 2 1 1 1 2 1 1 1 1 2 2 1 2 2
18 Saravanan 5 40 to 60 MALE 2 1 4 1 1 1 1 1 1 1 1 1 1 1 1 1 2 2 1 1 1 1 1 2 2
CO
MP
LAIN
TS
DU
RA
TIO
N
LATE
RA
LITY
ON
SET
CO
UR
SE
SYST
EMIC
ILLN
ESS
S.N
o
PA
TIEN
T ID
AG
E G
RO
UP
Age
gro
up
Gen
der
SEX
ENT
CV
S
RS
PA
HEA
D P
OST
UR
E
OC
ULA
R P
OST
UR
E
FAC
IAL
ASS
YMET
RY
WEI
GH
T LO
SS
FAM
ILY
HIS
TOR
Y
GENERAL EXAMINATION OCULAR EXAMINATION
VIT
ALS
LYM
PH
NO
DES
PA
LLO
R
CYA
NO
SIS
EDEM
A
THYR
OID
BR
EAST
SKIN
CN
S
GENERAL
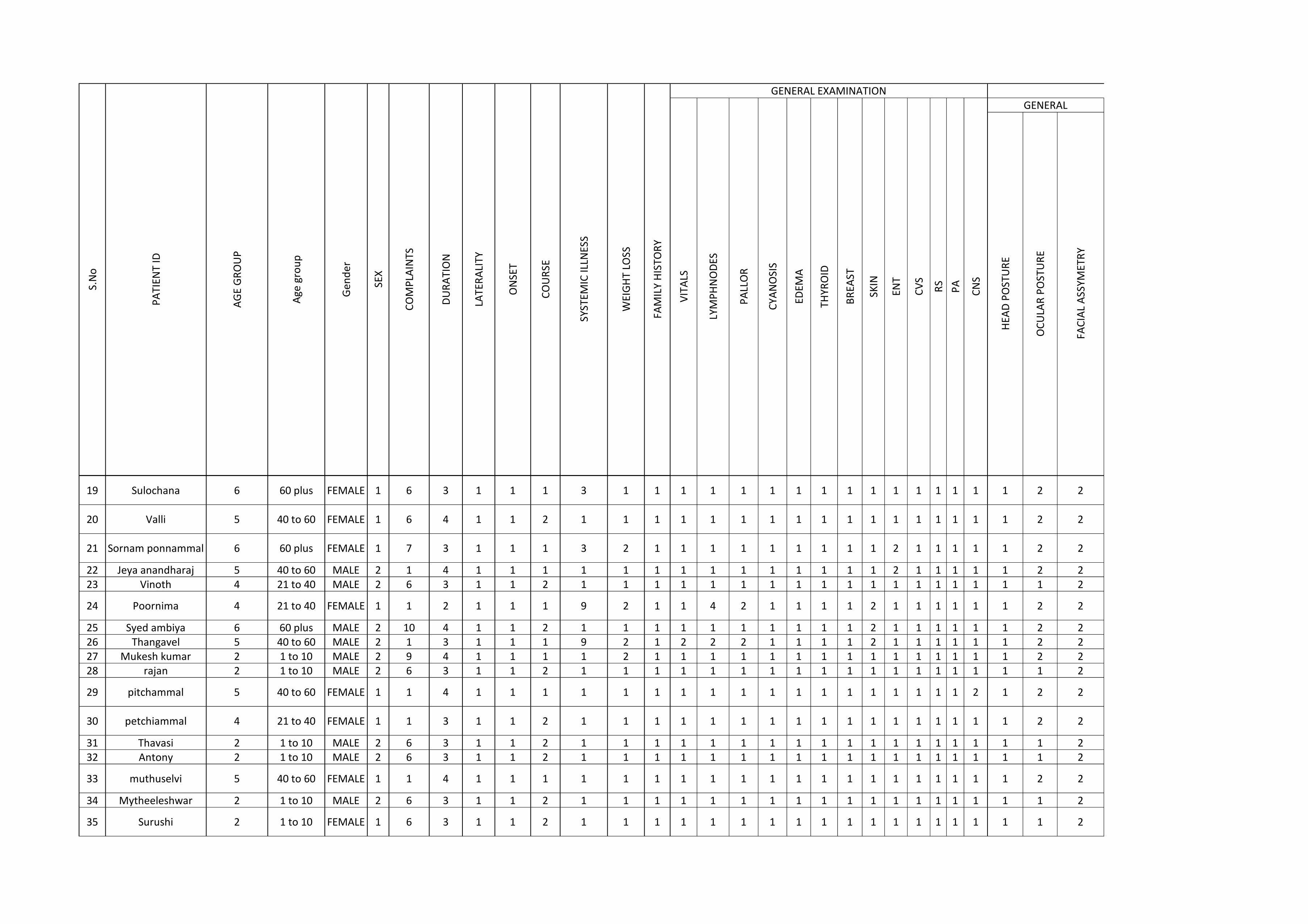
CO
MP
LAIN
TS
DU
RA
TIO
N
LATE
RA
LITY
ON
SET
CO
UR
SE
SYST
EMIC
ILLN
ESS
S.N
o
PA
TIEN
T ID
AG
E G
RO
UP
Age
gro
up
Gen
der
SEX
ENT
CV
S
RS
PA
HEA
D P
OST
UR
E
OC
ULA
R P
OST
UR
E
FAC
IAL
ASS
YMET
RY
WEI
GH
T LO
SS
FAM
ILY
HIS
TOR
Y
GENERAL EXAMINATION OCULAR EXAMINATION
VIT
ALS
LYM
PH
NO
DES
PA
LLO
R
CYA
NO
SIS
EDEM
A
THYR
OID
BR
EAST
SKIN
CN
S
GENERAL
19 Sulochana 6 60 plus FEMALE 1 6 3 1 1 1 3 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 2 2
20 Valli 5 40 to 60 FEMALE 1 6 4 1 1 2 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 2 2
21 Sornam ponnammal 6 60 plus FEMALE 1 7 3 1 1 1 3 2 1 1 1 1 1 1 1 1 1 2 1 1 1 1 1 2 2
22 Jeya anandharaj 5 40 to 60 MALE 2 1 4 1 1 1 1 1 1 1 1 1 1 1 1 1 1 2 1 1 1 1 1 2 223 Vinoth 4 21 to 40 MALE 2 6 3 1 1 2 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 2
24 Poornima 4 21 to 40 FEMALE 1 1 2 1 1 1 9 2 1 1 4 2 1 1 1 1 2 1 1 1 1 1 1 2 2
25 Syed ambiya 6 60 plus MALE 2 10 4 1 1 2 1 1 1 1 1 1 1 1 1 1 2 1 1 1 1 1 1 2 226 Thangavel 5 40 to 60 MALE 2 1 3 1 1 1 9 2 1 2 2 2 1 1 1 1 2 1 1 1 1 1 1 2 227 Mukesh kumar 2 1 to 10 MALE 2 9 4 1 1 1 1 2 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 2 228 rajan 2 1 to 10 MALE 2 6 3 1 1 2 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 2
29 pitchammal 5 40 to 60 FEMALE 1 1 4 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 2 1 2 2
30 petchiammal 4 21 to 40 FEMALE 1 1 3 1 1 2 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 2 2
31 Thavasi 2 1 to 10 MALE 2 6 3 1 1 2 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 232 Antony 2 1 to 10 MALE 2 6 3 1 1 2 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 2
33 muthuselvi 5 40 to 60 FEMALE 1 1 4 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 2 2
34 Mytheeleshwar 2 1 to 10 MALE 2 6 3 1 1 2 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 2
35 Surushi 2 1 to 10 FEMALE 1 6 3 1 1 2 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 2
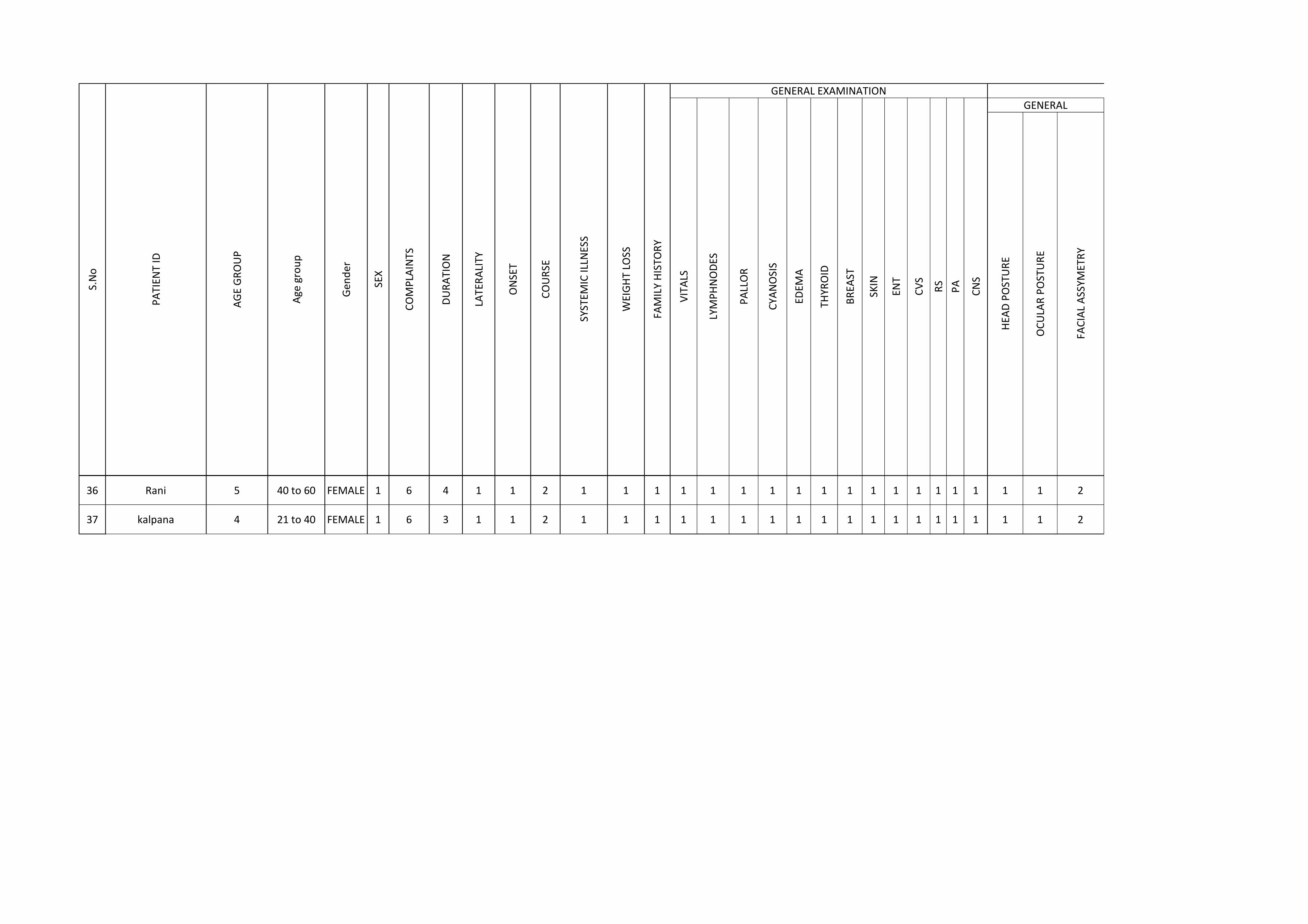
CO
MP
LAIN
TS
DU
RA
TIO
N
LATE
RA
LITY
ON
SET
CO
UR
SE
SYST
EMIC
ILLN
ESS
S.N
o
PA
TIEN
T ID
AG
E G
RO
UP
Age
gro
up
Gen
der
SEX
ENT
CV
S
RS
PA
HEA
D P
OST
UR
E
OC
ULA
R P
OST
UR
E
FAC
IAL
ASS
YMET
RY
WEI
GH
T LO
SS
FAM
ILY
HIS
TOR
Y
GENERAL EXAMINATION OCULAR EXAMINATION
VIT
ALS
LYM
PH
NO
DES
PA
LLO
R
CYA
NO
SIS
EDEM
A
THYR
OID
BR
EAST
SKIN
CN
S
GENERAL
36 Rani 5 40 to 60 FEMALE 1 6 4 1 1 2 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 2
37 kalpana 4 21 to 40 FEMALE 1 6 3 1 1 2 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 2
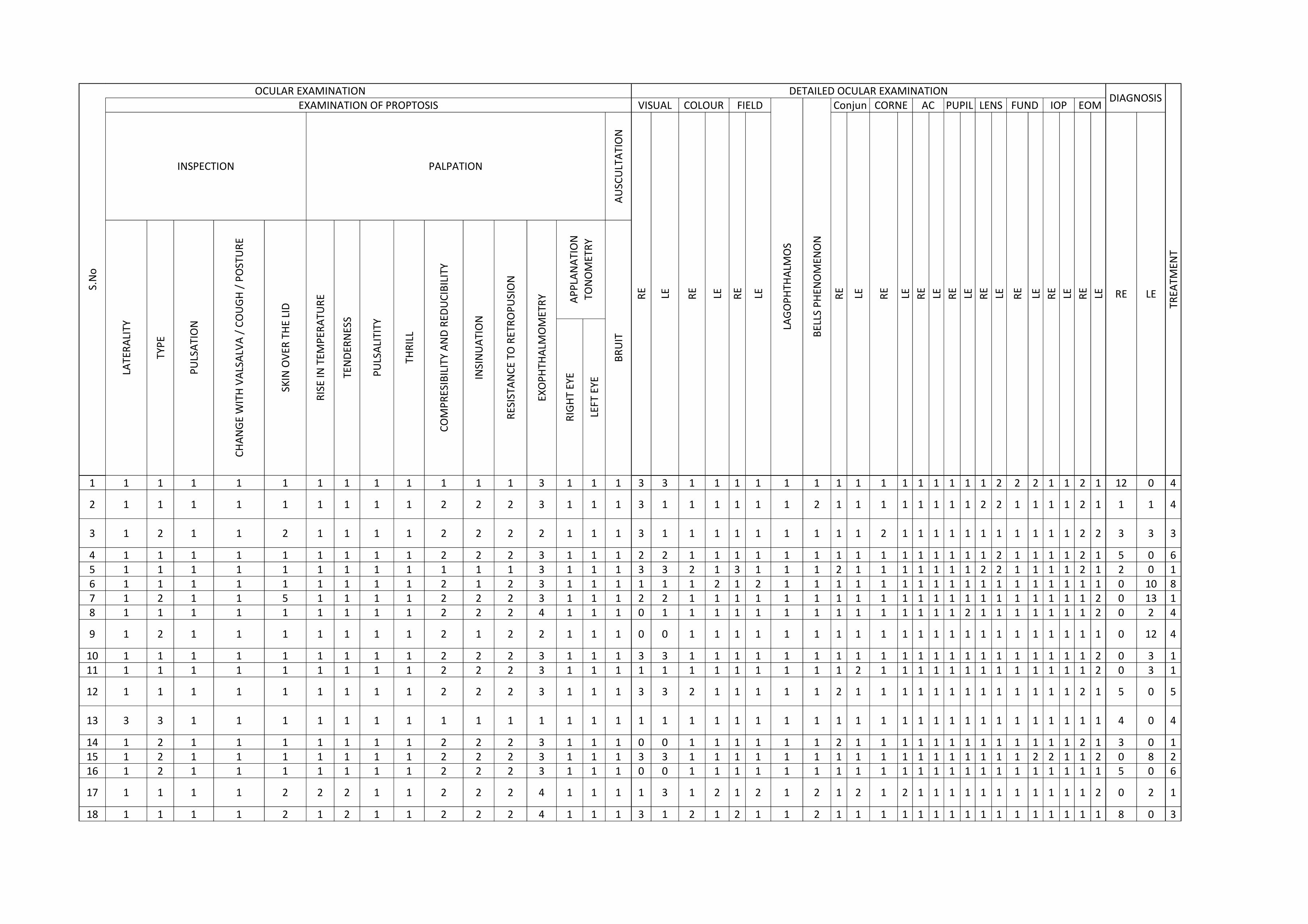
1
2
3
45678
9
1011
12
13
141516
17
18
S.N
o
AU
SCU
LTA
TIO
N
RIG
HT
EYE
LEFT
EYE
1 1 1 1 1 1 1 1 1 1 1 1 3 1 1 1 3 3 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 2 2 2 1 1 2 1 12 0 4
1 1 1 1 1 1 1 1 1 2 2 2 3 1 1 1 3 1 1 1 1 1 1 2 1 1 1 1 1 1 1 1 2 2 1 1 1 1 2 1 1 1 4
1 2 1 1 2 1 1 1 1 2 2 2 2 1 1 1 3 1 1 1 1 1 1 1 1 1 2 1 1 1 1 1 1 1 1 1 1 1 2 2 3 3 3
1 1 1 1 1 1 1 1 1 2 2 2 3 1 1 1 2 2 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 2 1 1 1 1 2 1 5 0 61 1 1 1 1 1 1 1 1 1 1 1 3 1 1 1 3 3 2 1 3 1 1 1 2 1 1 1 1 1 1 1 2 2 1 1 1 1 2 1 2 0 11 1 1 1 1 1 1 1 1 2 1 2 3 1 1 1 1 1 1 2 1 2 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 0 10 81 2 1 1 5 1 1 1 1 2 2 2 3 1 1 1 2 2 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 2 0 13 11 1 1 1 1 1 1 1 1 2 2 2 4 1 1 1 0 1 1 1 1 1 1 1 1 1 1 1 1 1 1 2 1 1 1 1 1 1 1 2 0 2 4
1 2 1 1 1 1 1 1 1 2 1 2 2 1 1 1 0 0 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 0 12 4
1 1 1 1 1 1 1 1 1 2 2 2 3 1 1 1 3 3 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 2 0 3 11 1 1 1 1 1 1 1 1 2 2 2 3 1 1 1 1 1 1 1 1 1 1 1 1 2 1 1 1 1 1 1 1 1 1 1 1 1 1 2 0 3 1
1 1 1 1 1 1 1 1 1 2 2 2 3 1 1 1 3 3 2 1 1 1 1 1 2 1 1 1 1 1 1 1 1 1 1 1 1 1 2 1 5 0 5
3 3 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 4 0 4
1 2 1 1 1 1 1 1 1 2 2 2 3 1 1 1 0 0 1 1 1 1 1 1 2 1 1 1 1 1 1 1 1 1 1 1 1 1 2 1 3 0 11 2 1 1 1 1 1 1 1 2 2 2 3 1 1 1 3 3 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 2 2 1 1 2 0 8 21 2 1 1 1 1 1 1 1 2 2 2 3 1 1 1 0 0 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 5 0 6
1 1 1 1 2 2 2 1 1 2 2 2 4 1 1 1 1 3 1 2 1 2 1 2 1 2 1 2 1 1 1 1 1 1 1 1 1 1 1 2 0 2 1
1 1 1 1 2 1 2 1 1 2 2 2 4 1 1 1 3 1 2 1 2 1 1 2 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 8 0 3
DIAGNOSIS
INSPECTION PALPATION
RE LE RE
LENS FUND IOP EOM
PU
LSA
LITI
TY
THR
ILL
LE
LATE
RA
LITY
CO
MP
RES
IBIL
ITY
AN
D R
EDU
CIB
ILIT
Y
INSI
NU
ATI
ON
RES
ISTA
NC
E TO
RET
RO
PU
SIO
N
EXO
PH
THA
LMO
MET
RY
TYP
E
OCULAR EXAMINATION DETAILED OCULAR EXAMINATION
RE LERE
EXAMINATION OF PROPTOSIS VISUAL COLOUR FIELD
LE RE
PU
LSA
TIO
N
CH
AN
GE
WIT
H V
ALS
ALV
A /
CO
UG
H /
PO
STU
RE
SKIN
OV
ER T
HE
LID
RIS
E IN
TEM
PER
ATU
RE
TEN
DER
NES
S
AP
PLA
NA
TIO
N
TON
OM
ETR
Y
BR
UIT
LAG
OP
HTH
ALM
OS
BEL
LS P
HEN
OM
ENO
N
Conjun CORNE AC PUPIL
RE LE LE RE LERE LE RE LE RE LE
TREA
TMEN
T
LE RE LE RE
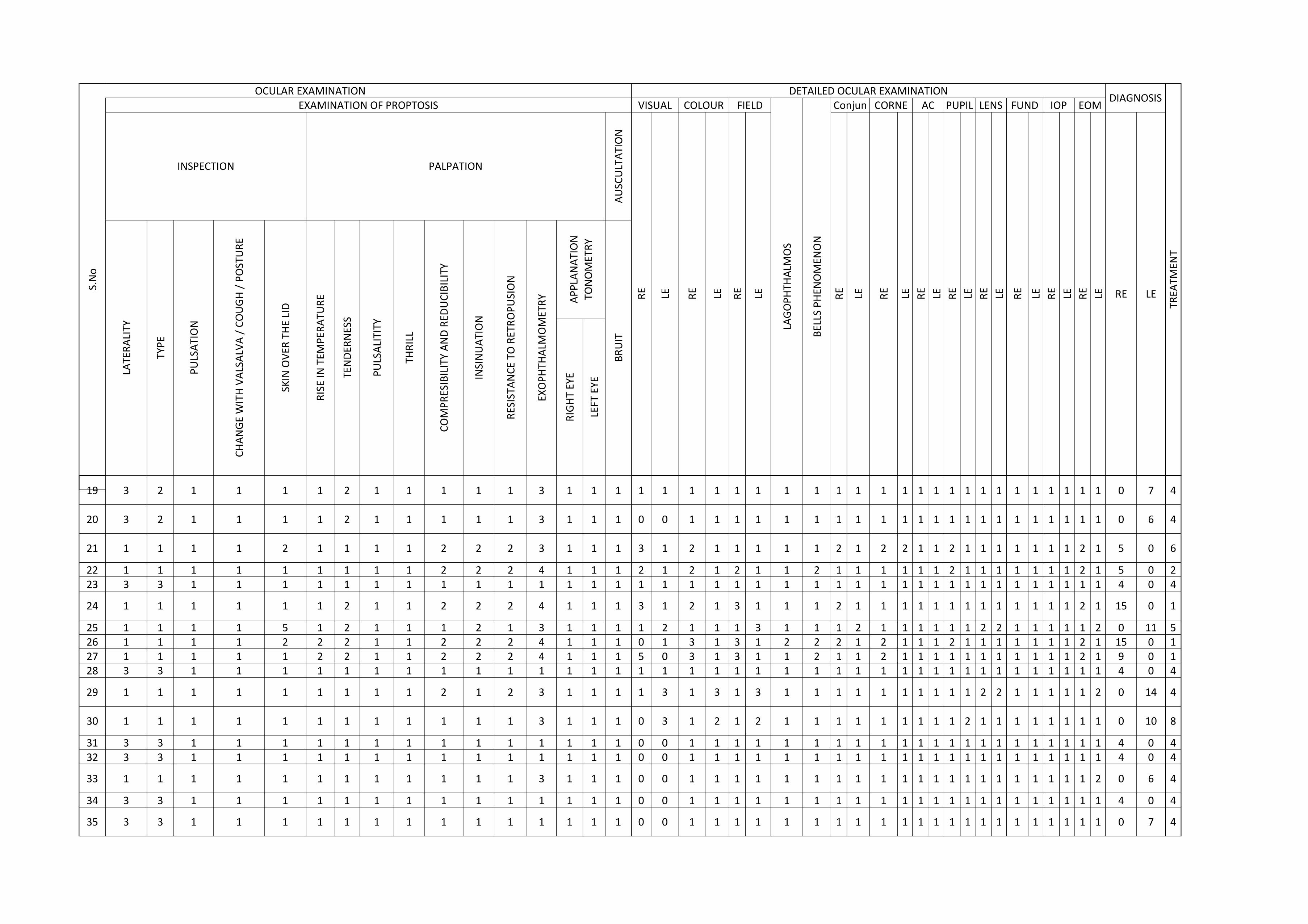
1
S.N
o
19
20
21
2223
24
25262728
29
30
3132
33
34
35
AU
SCU
LTA
TIO
N
RIG
HT
EYE
LEFT
EYE
DIAGNOSIS
INSPECTION PALPATION
RE LE RE
LENS FUND IOP EOM
PU
LSA
LITI
TY
THR
ILL
LE
LATE
RA
LITY
CO
MP
RES
IBIL
ITY
AN
D R
EDU
CIB
ILIT
Y
INSI
NU
ATI
ON
RES
ISTA
NC
E TO
RET
RO
PU
SIO
N
EXO
PH
THA
LMO
MET
RY
TYP
E
OCULAR EXAMINATION DETAILED OCULAR EXAMINATION
RE LERE
EXAMINATION OF PROPTOSIS VISUAL COLOUR FIELD
LE RE
PU
LSA
TIO
N
CH
AN
GE
WIT
H V
ALS
ALV
A /
CO
UG
H /
PO
STU
RE
SKIN
OV
ER T
HE
LID
RIS
E IN
TEM
PER
ATU
RE
TEN
DER
NES
S
AP
PLA
NA
TIO
N
TON
OM
ETR
Y
BR
UIT
LAG
OP
HTH
ALM
OS
BEL
LS P
HEN
OM
ENO
N
Conjun CORNE AC PUPIL
RE LE LE RE LERE LE RE LE RE LE
TREA
TMEN
T
LE RE LE RE
3 2 1 1 1 1 2 1 1 1 1 1 3 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 0 7 4
3 2 1 1 1 1 2 1 1 1 1 1 3 1 1 1 0 0 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 0 6 4
1 1 1 1 2 1 1 1 1 2 2 2 3 1 1 1 3 1 2 1 1 1 1 1 2 1 2 2 1 1 2 1 1 1 1 1 1 1 2 1 5 0 6
1 1 1 1 1 1 1 1 1 2 2 2 4 1 1 1 2 1 2 1 2 1 1 2 1 1 1 1 1 1 2 1 1 1 1 1 1 1 2 1 5 0 23 3 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 4 0 4
1 1 1 1 1 1 2 1 1 2 2 2 4 1 1 1 3 1 2 1 3 1 1 1 2 1 1 1 1 1 1 1 1 1 1 1 1 1 2 1 15 0 1
1 1 1 1 5 1 2 1 1 1 2 1 3 1 1 1 1 2 1 1 1 3 1 1 1 2 1 1 1 1 1 1 2 2 1 1 1 1 1 2 0 11 51 1 1 1 2 2 2 1 1 2 2 2 4 1 1 1 0 1 3 1 3 1 2 2 2 1 2 1 1 1 2 1 1 1 1 1 1 1 2 1 15 0 11 1 1 1 1 2 2 1 1 2 2 2 4 1 1 1 5 0 3 1 3 1 1 2 1 1 2 1 1 1 1 1 1 1 1 1 1 1 2 1 9 0 13 3 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 4 0 4
1 1 1 1 1 1 1 1 1 2 1 2 3 1 1 1 1 3 1 3 1 3 1 1 1 1 1 1 1 1 1 1 2 2 1 1 1 1 1 2 0 14 4
1 1 1 1 1 1 1 1 1 1 1 1 3 1 1 1 0 3 1 2 1 2 1 1 1 1 1 1 1 1 1 2 1 1 1 1 1 1 1 1 0 10 8
3 3 1 1 1 1 1 1 1 1 1 1 1 1 1 1 0 0 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 4 0 43 3 1 1 1 1 1 1 1 1 1 1 1 1 1 1 0 0 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 4 0 4
1 1 1 1 1 1 1 1 1 1 1 1 3 1 1 1 0 0 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 2 0 6 4
3 3 1 1 1 1 1 1 1 1 1 1 1 1 1 1 0 0 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 4 0 4
3 3 1 1 1 1 1 1 1 1 1 1 1 1 1 1 0 0 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 0 7 4
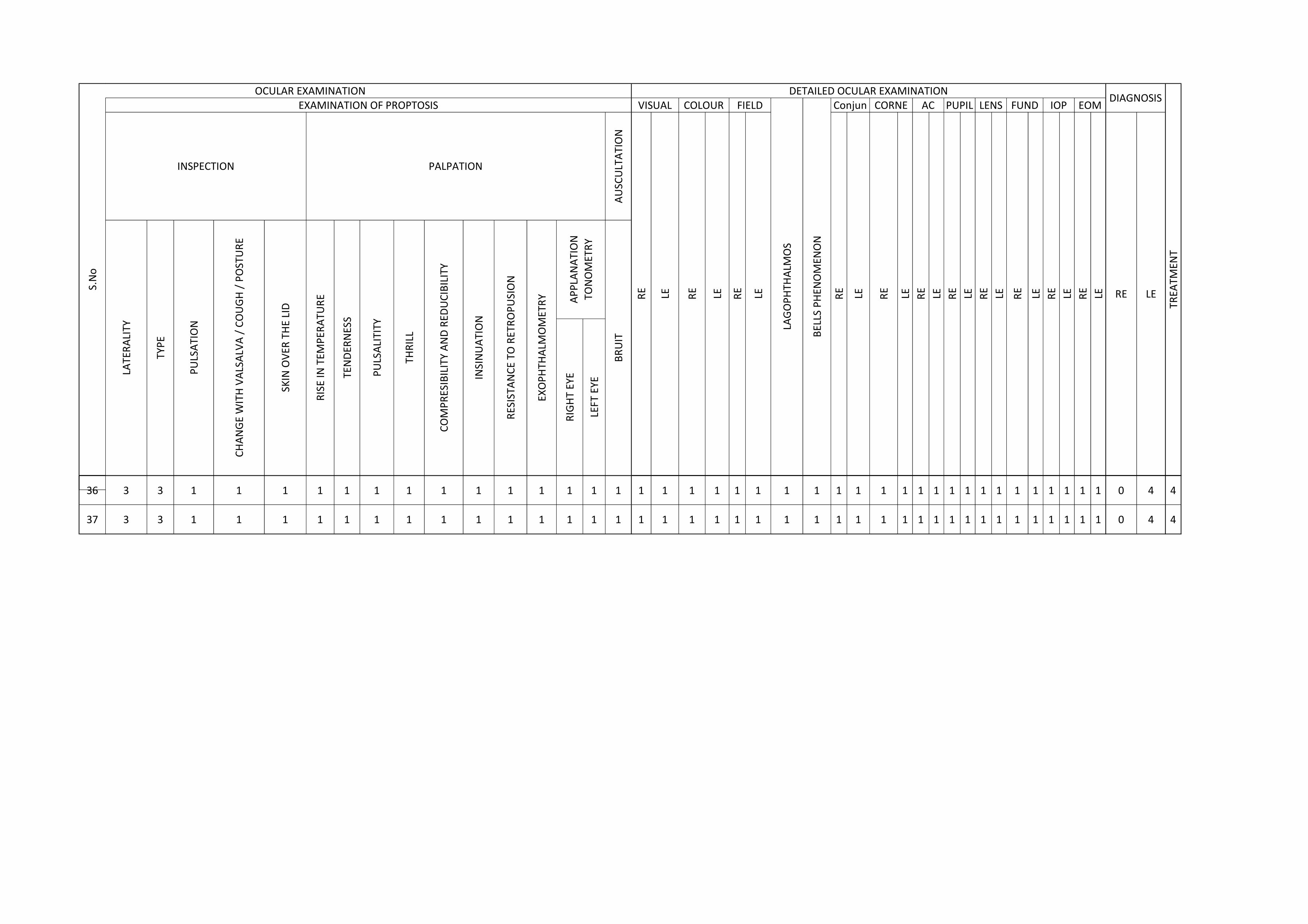
1
S.N
o
36
37
AU
SCU
LTA
TIO
N
RIG
HT
EYE
LEFT
EYE
DIAGNOSIS
INSPECTION PALPATION
RE LE RE
LENS FUND IOP EOM
PU
LSA
LITI
TY
THR
ILL
LE
LATE
RA
LITY
CO
MP
RES
IBIL
ITY
AN
D R
EDU
CIB
ILIT
Y
INSI
NU
ATI
ON
RES
ISTA
NC
E TO
RET
RO
PU
SIO
N
EXO
PH
THA
LMO
MET
RY
TYP
E
OCULAR EXAMINATION DETAILED OCULAR EXAMINATION
RE LERE
EXAMINATION OF PROPTOSIS VISUAL COLOUR FIELD
LE RE
PU
LSA
TIO
N
CH
AN
GE
WIT
H V
ALS
ALV
A /
CO
UG
H /
PO
STU
RE
SKIN
OV
ER T
HE
LID
RIS
E IN
TEM
PER
ATU
RE
TEN
DER
NES
S
AP
PLA
NA
TIO
N
TON
OM
ETR
Y
BR
UIT
LAG
OP
HTH
ALM
OS
BEL
LS P
HEN
OM
ENO
N
Conjun CORNE AC PUPIL
RE LE LE RE LERE LE RE LE RE LE
TREA
TMEN
T
LE RE LE RE
3 3 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 0 4 4
3 3 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 0 4 4
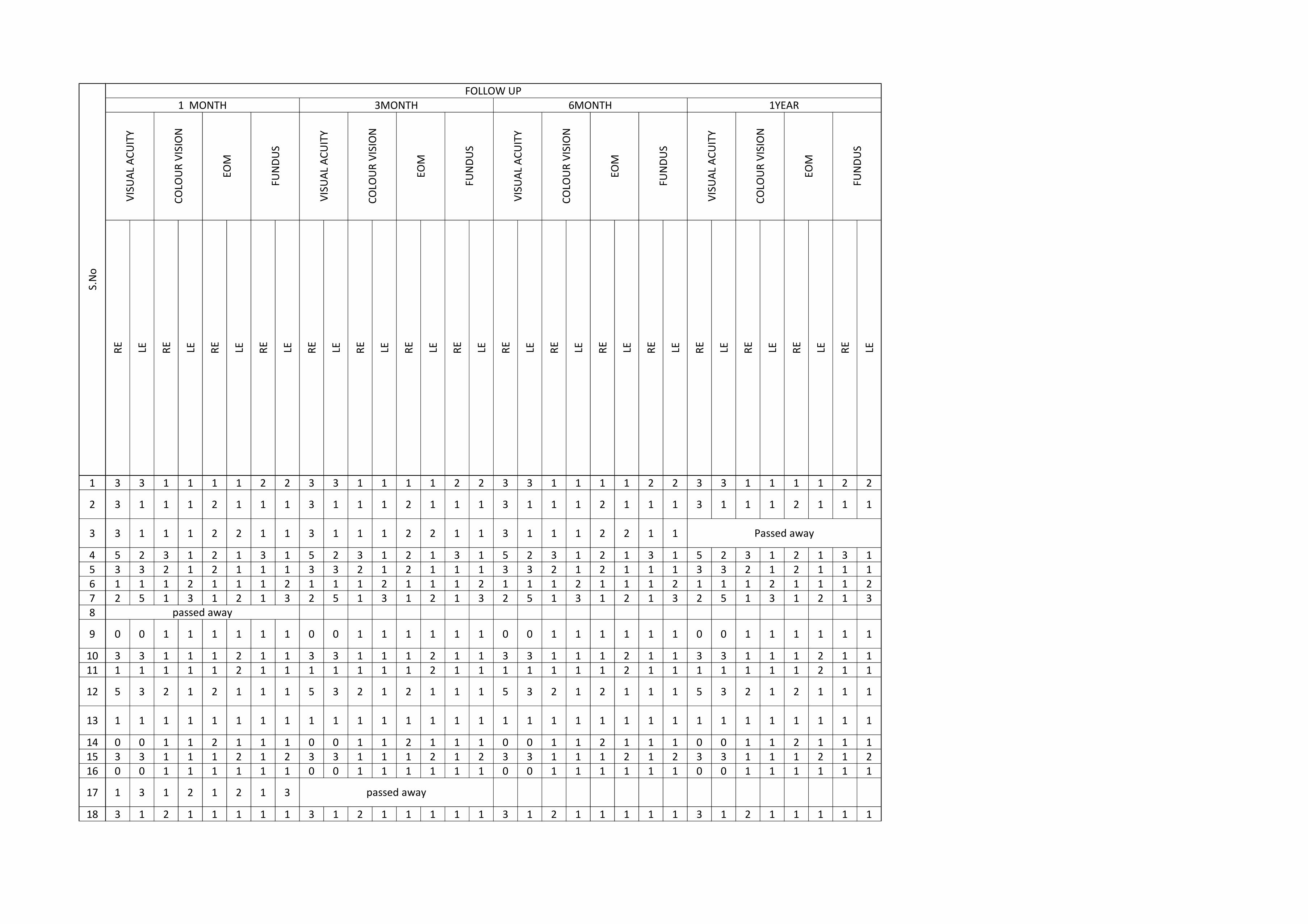
1
2
3
45678
9
1011
12
13
141516
17
18
S.N
o
3 3 1 1 1 1 2 2 3 3 1 1 1 1 2 2 3 3 1 1 1 1 2 2 3 3 1 1 1 1 2 2
3 1 1 1 2 1 1 1 3 1 1 1 2 1 1 1 3 1 1 1 2 1 1 1 3 1 1 1 2 1 1 1
3 1 1 1 2 2 1 1 3 1 1 1 2 2 1 1 3 1 1 1 2 2 1 1
5 2 3 1 2 1 3 1 5 2 3 1 2 1 3 1 5 2 3 1 2 1 3 1 5 2 3 1 2 1 3 13 3 2 1 2 1 1 1 3 3 2 1 2 1 1 1 3 3 2 1 2 1 1 1 3 3 2 1 2 1 1 11 1 1 2 1 1 1 2 1 1 1 2 1 1 1 2 1 1 1 2 1 1 1 2 1 1 1 2 1 1 1 22 5 1 3 1 2 1 3 2 5 1 3 1 2 1 3 2 5 1 3 1 2 1 3 2 5 1 3 1 2 1 3
0 0 1 1 1 1 1 1 0 0 1 1 1 1 1 1 0 0 1 1 1 1 1 1 0 0 1 1 1 1 1 1
3 3 1 1 1 2 1 1 3 3 1 1 1 2 1 1 3 3 1 1 1 2 1 1 3 3 1 1 1 2 1 11 1 1 1 1 2 1 1 1 1 1 1 1 2 1 1 1 1 1 1 1 2 1 1 1 1 1 1 1 2 1 1
5 3 2 1 2 1 1 1 5 3 2 1 2 1 1 1 5 3 2 1 2 1 1 1 5 3 2 1 2 1 1 1
1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1
0 0 1 1 2 1 1 1 0 0 1 1 2 1 1 1 0 0 1 1 2 1 1 1 0 0 1 1 2 1 1 13 3 1 1 1 2 1 2 3 3 1 1 1 2 1 2 3 3 1 1 1 2 1 2 3 3 1 1 1 2 1 20 0 1 1 1 1 1 1 0 0 1 1 1 1 1 1 0 0 1 1 1 1 1 1 0 0 1 1 1 1 1 1
1 3 1 2 1 2 1 3
3 1 2 1 1 1 1 1 3 1 2 1 1 1 1 1 3 1 2 1 1 1 1 1 3 1 2 1 1 1 1 1
LE RE LE RE LE
EOM
FUN
DU
S
VIS
UA
L A
CU
ITY
CO
LOU
R V
ISIO
N
EOM
FUN
DU
S
VIS
UA
L A
CU
ITY
CO
LOU
R V
ISIO
N
1 MONTH 3MONTHR
E LE RE LE
VIS
UA
L A
CU
ITY
CO
LOU
R V
ISIO
N
FOLLOW UP6MONTH 1YEAR
EOM
FUN
DU
S
RE LE RE LE
EOM
FUN
DU
S
VIS
UA
L A
CU
ITY
CO
LOU
R V
ISIO
N
Passed away
passed away
passed away
RE LE RE LE RE LERE LE RE LE RE LERE LE RE LE RE LERE
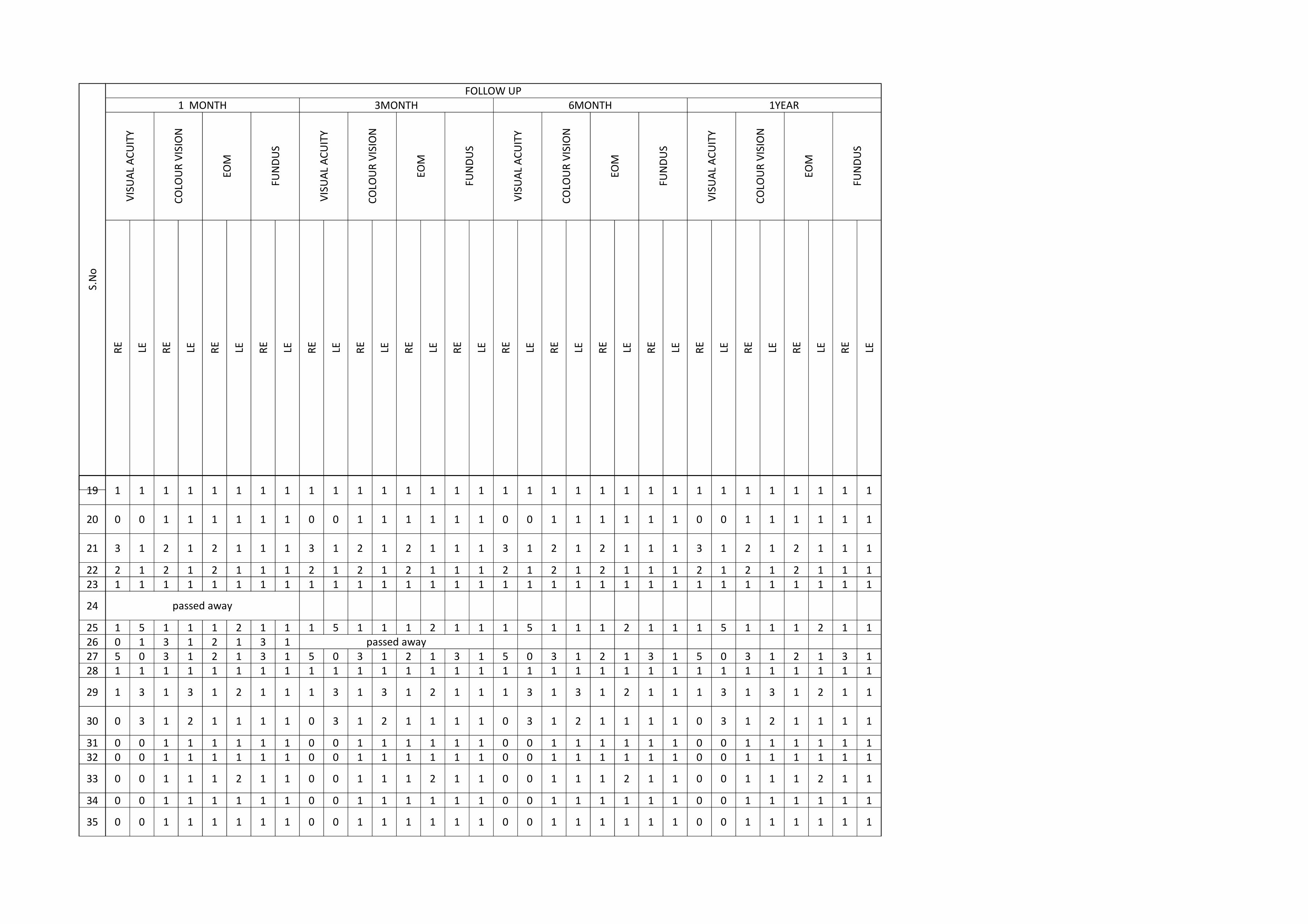
1
S.N
o
19
20
21
2223
24
25262728
29
30
3132
33
34
35
LE RE LE RE LE
EOM
FUN
DU
S
VIS
UA
L A
CU
ITY
CO
LOU
R V
ISIO
N
EOM
FUN
DU
S
VIS
UA
L A
CU
ITY
CO
LOU
R V
ISIO
N
1 MONTH 3MONTHR
E LE RE LE
VIS
UA
L A
CU
ITY
CO
LOU
R V
ISIO
N
FOLLOW UP6MONTH 1YEAR
EOM
FUN
DU
S
RE LE RE LE
EOM
FUN
DU
S
VIS
UA
L A
CU
ITY
CO
LOU
R V
ISIO
N
RE LE RE LE RE LERE LE RE LE RE LERE LE RE LE RE LERE
1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1
0 0 1 1 1 1 1 1 0 0 1 1 1 1 1 1 0 0 1 1 1 1 1 1 0 0 1 1 1 1 1 1
3 1 2 1 2 1 1 1 3 1 2 1 2 1 1 1 3 1 2 1 2 1 1 1 3 1 2 1 2 1 1 1
2 1 2 1 2 1 1 1 2 1 2 1 2 1 1 1 2 1 2 1 2 1 1 1 2 1 2 1 2 1 1 11 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1
1 5 1 1 1 2 1 1 1 5 1 1 1 2 1 1 1 5 1 1 1 2 1 1 1 5 1 1 1 2 1 10 1 3 1 2 1 3 15 0 3 1 2 1 3 1 5 0 3 1 2 1 3 1 5 0 3 1 2 1 3 1 5 0 3 1 2 1 3 11 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1
1 3 1 3 1 2 1 1 1 3 1 3 1 2 1 1 1 3 1 3 1 2 1 1 1 3 1 3 1 2 1 1
0 3 1 2 1 1 1 1 0 3 1 2 1 1 1 1 0 3 1 2 1 1 1 1 0 3 1 2 1 1 1 1
0 0 1 1 1 1 1 1 0 0 1 1 1 1 1 1 0 0 1 1 1 1 1 1 0 0 1 1 1 1 1 10 0 1 1 1 1 1 1 0 0 1 1 1 1 1 1 0 0 1 1 1 1 1 1 0 0 1 1 1 1 1 1
0 0 1 1 1 2 1 1 0 0 1 1 1 2 1 1 0 0 1 1 1 2 1 1 0 0 1 1 1 2 1 1
0 0 1 1 1 1 1 1 0 0 1 1 1 1 1 1 0 0 1 1 1 1 1 1 0 0 1 1 1 1 1 1
0 0 1 1 1 1 1 1 0 0 1 1 1 1 1 1 0 0 1 1 1 1 1 1 0 0 1 1 1 1 1 1
passed away
passed away
1
S.N
o
36
37
LE RE LE RE LE
EOM
FUN
DU
S
VIS
UA
L A
CU
ITY
CO
LOU
R V
ISIO
N
EOM
FUN
DU
S
VIS
UA
L A
CU
ITY
CO
LOU
R V
ISIO
N
1 MONTH 3MONTHR
E LE RE LE
VIS
UA
L A
CU
ITY
CO
LOU
R V
ISIO
N
FOLLOW UP6MONTH 1YEAR
EOM
FUN
DU
S
RE LE RE LE
EOM
FUN
DU
S
VIS
UA
L A
CU
ITY
CO
LOU
R V
ISIO
N
RE LE RE LE RE LERE LE RE LE RE LERE LE RE LE RE LERE
1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1
1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1
Related Documents











