-
7/31/2019 Clinical Review of Larynx Upper Resp Tract
1/36
Clinical Review of Larynx &Upper Respiratory Tract
Manny Trujillo, Jr., MDDepartment of Surgical Education
Spartanburg Regional Healthcare System04.16.12
-
7/31/2019 Clinical Review of Larynx Upper Resp Tract
2/36
"Dispel from your mind the thought thatan understanding of the human body inevery aspect of its structure can be given inwords; the more thoroughly you describe
the more you will confuse... I advise younot to trouble with words unless you arespeaking to blind men."
Leonardo da Vinci
-
7/31/2019 Clinical Review of Larynx Upper Resp Tract
3/36
Objectives
Enumerate the pertinent functions andanatomy of upper respiratory tract and
larynx
Familiarization with consequences of
alterations in normal function of upperrespiratory tract and larynx
-
7/31/2019 Clinical Review of Larynx Upper Resp Tract
4/36
Upper Respiratory Tract
Nasal Cavity Main conducting airway for inhaled air Filtration, conditioning, olfaction, resonating
chamber contributing to sound production
Paranasal Sinuses Frontal, ethmoidal, sphenoidal, maxillary Conditioning, sound resonance, decrease skull weight
Pharynx Nasopharynx, Oropharynx, Laryngopharynx Air passage between nasal cavity and larynx Passageway for swallowed food and drink between
oral cavity and esophagus
-
7/31/2019 Clinical Review of Larynx Upper Resp Tract
5/36
Upper Respiratory Tract
Sagittal depiction Paranasal Sinuses
-
7/31/2019 Clinical Review of Larynx Upper Resp Tract
6/36
Rhinitis
Clinical manifestation of inflammatory response toinfection/allergy
Edema of mucosa (high vascularity) Infections of nasal cavities can spread to:
Anterior cranial fossa through cribiform plate
Nasopharynx and retropharyngeal soft tissues
Middle ear through pharyngotympanic tube Paranasal sinuses
Lacrimal apparatus and conjunctiva
-
7/31/2019 Clinical Review of Larynx Upper Resp Tract
7/36
Nasal Fractures
Fracture of the nasal bones and/or cartilages
Often associated with other maxillofacial fractures
Must rule out concomitant airway, central nervous
system, visceral, and orthopedic injuries
-
7/31/2019 Clinical Review of Larynx Upper Resp Tract
8/36
Nasal Fractures
-
7/31/2019 Clinical Review of Larynx Upper Resp Tract
9/36
Epistaxis
Anterior (90%): Kiesselbachs plexus - anastomosis of the anterior
ethmoidal, greater palatine, sphenopalatine, andsuperior labial arteries
Treatment: Anterior packing
Posterior (10%): Woodruffs plexus anastomosis of pharyngeal,
posterior nasal, sphenopalatine, and posterior septalarteries
Treatment: Posterior packing, reduction of fractures,
embolization
Causes: trauma (#1), hypertension, infections
-
7/31/2019 Clinical Review of Larynx Upper Resp Tract
10/36
Epistaxis
-
7/31/2019 Clinical Review of Larynx Upper Resp Tract
11/36
Deviated Septum
Common occurrence
Variable presentations
Mild subclinical
Severe obstructive
Usually secondary totrauma in adolescence(minor incidencechildbirth)
Surgical correctioncurative
-
7/31/2019 Clinical Review of Larynx Upper Resp Tract
12/36
Sinusitis
Etiologies:
Infection (viral MC!!) Allergy Autoimmune disease
Phases:
Acute New infection lasting up to 4 weeks
RecurrentAcute 4 or more separate episodes in one year
Subacute
Infection lasting between 4 and 12weeks Represents a transition between acute
and chronic infection Chronic
Signs and symptoms lasting more than12 weeks
Acute Exacerbation of Chronic
Exacerbation of chronic symptoms thatreturn to baseline after treatment
Treatment:
Acute Suspected viral
Supportive tx (analgesic, antipyretic,decongestant, intranasal corticosteroid,intranasal saline, mucolytic)
Suspected bacterial Immunocompromised or with severe
illness Antibiotics (10-14 days),Surgery consult
Immunocompetent nonseverewatchful waiting up to 7 days and
supportive tx
Chronic Antibiotics (3-4 weeks) Nasal saline irrigations Intranasal corticosteroids Functional Endoscopic Sinus Surgery
(FESS) reserved for failed medical
management
Inflammation of mucous membrane lining the paranasal sinuses
-
7/31/2019 Clinical Review of Larynx Upper Resp Tract
13/36
Fulminant Fungal Sinusitis
24 hrs after presentation After debridement After partial closure
-
7/31/2019 Clinical Review of Larynx Upper Resp Tract
14/36
Ethmoidal Sinusitis
Obstruction ofethmoidalinfundibulum to middlemeatus
Spread of infectionwith fracture oflamina papyracea
Proximity to optic canal
(optic nerve,ophthalmic artery) Complications include
optic neuritis andblindness
EthmoidalSinus
Pansinusitis with obstruction ofmiddle meatus
-
7/31/2019 Clinical Review of Larynx Upper Resp Tract
15/36
CT scans used to evaluate persistence of chronic sinusitis
Pre-treatment Post-treatment
Sinusitis
-
7/31/2019 Clinical Review of Larynx Upper Resp Tract
16/36
Tonsillitis
Waldeyers Ring
Pharyngeal tonsil(Adenoid)
Tubal tonsils Palatine tonsils
Lingual tonsils
Perfusion/Drainage
Tonsillar artery (viaFacial a.)
External Palatine vein
-
7/31/2019 Clinical Review of Larynx Upper Resp Tract
17/36
Inflammation/infectionof tonsils
Etiologies: Viral (#1) Bacterial (#2)
GABHS
Allergic Neoplastic
Treatment: Non GABHS analgesics GABHS analgesics, ABX
x 10 days, corticosteroids Recalcitrant (>7/yr, >5/yr
x 2 yr, >3/yr x 3 yr) or withexacerbating factorsTonsillectomy
Tonsillitis
Culture-positiveStrep pharyngitis
with tonsillar exudates
-
7/31/2019 Clinical Review of Larynx Upper Resp Tract
18/36
Nasopharyngeal Cancer
Rare in North America,more common in China
40% overall survival at 5years
Complete H&P, carefulotologic, neurologic,cervical and NP exams
Three WHO types - all from
NP epithelium Types II, III - better
prognosis, EBV assoc.
Treatment is primarily XRT
+/- chemo
-
7/31/2019 Clinical Review of Larynx Upper Resp Tract
19/36
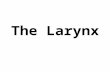
Laryngeal Anatomy
Cartilages(Unpaired, Paired)
Ligaments,Membranes, andSpaces
Musculature
Innervation andVasculature
Anterior View
-
7/31/2019 Clinical Review of Larynx Upper Resp Tract
20/36
Functions of the Larynx
Respiration
Vocalization(Phonation)
Increasing intra-abdominal airpressure
Posterior View
-
7/31/2019 Clinical Review of Larynx Upper Resp Tract
21/36
Vocalization (Phonation)
1. To phonate, the vocal folds must vibrate
2. To vibrate, they must be held close enough together
to impede the airflow through the glottis
3. Muscles bring them together & hold them there
4. The transglottal airflow itself sets them intovibration, and maintains the vibration
Myoelastic Aerodynamic Theory of Phonation(Elastic recoil and Bernoulli forces)
-
7/31/2019 Clinical Review of Larynx Upper Resp Tract
22/36
Vertical views of the vocal folds
during one vibratory cycle
1
2
3
4
5
6
The folds are three-dimensional, and they vibratein three dimensions.
The pattern of vibration is likea wave travelling up them.
The lower sections part first,and come together first.
Cover (outer layer) and body
(inner layers) of folds are oftendistinguished, because theyvibrate fairly independently
After Stevens (1998) Acoustic Phonetics
(Baer, 1975)
-
7/31/2019 Clinical Review of Larynx Upper Resp Tract
23/36
Myoelastic Aerodynamic Theory of
Vocal Fold Vibration
(van den Berg, 1950s)
1. Muscular activity rotates and rocks the arytenoid cartilages so thattheir vocal processes come together in the midline, thus positioningthe vocal folds close together or in actual contact.
2. Air pressure increases below the glottis until folds forced apart.(The subglottal pressure increase leads to a transglottal pressuredrop.)
3. Air travels faster through the glottis when it is narrow. This causesa local drop in air pressure (Bernoulli effect)whichcauses the
folds to be sucked towards each other.
4. The Bernoulli effect, together with the elastic recoil force exerted bythe displaced vocal folds, causes complete glottal closure again.
5. The process begins again at step 2
-
7/31/2019 Clinical Review of Larynx Upper Resp Tract
24/36
Vocal Fold Vibration
-
7/31/2019 Clinical Review of Larynx Upper Resp Tract
25/36
Nerves Supplying Larynx
Superior laryngeal nerve Internal branch sensation
to larynx External branchmotor
innervation to cricothyroidmuscle and anterior portionof cricopharyngeus muscle(posterior portion supplied
by ILN)
Inferior laryngeal nerve Terminal part of recurrent
laryngeal nerve Motor to ALL intrinsic
laryngeal muscles exceptcricothyroid
Nerve supply to larynx entirely from CN X (Vagus n.)
-
7/31/2019 Clinical Review of Larynx Upper Resp Tract
26/36
Nerve of Galli-Curci
1882 - 1963
Italian opera singer
1935 Thyroidectomy forsymptomatic goiter
Continued voice
decline
Nerve of Galli-Curci
-
7/31/2019 Clinical Review of Larynx Upper Resp Tract
27/36
Laryngeal Cancer
Any patient with hoarseness lastinglonger than 2 weeks should undergo
laryngeal examination
Most common cancer of the upperaerodigestive tract
Subtypes Glottic Cancer (59%) Supraglottic Cancer (40%) Subglottic Cancer (1%)
Most subglottic masses areextension from glottic carcinomas
Treatment depends on: Site of lesion Extent of spread Metastasis
Indications for total laryngectomy T3 or T4 unfit for partial Extensive involvement of thyroid
and cricoid cartilages Invasion of neck soft tissues Tongue base involvement beyond
circumvallate papillae
-
7/31/2019 Clinical Review of Larynx Upper Resp Tract
28/36
Foreign Bodies in Laryngopharynx
3000 deaths/yearfrom foreign bodyaspiration (US)
Most in bronchus(80-90%) Larger objects
lodge in larynx
(10%) Emergent
interventionrequired
-
7/31/2019 Clinical Review of Larynx Upper Resp Tract
29/36
Cricothyroidotomy
Needle Cricothyroidotomy
Large bore needle inserted throughcricothyroid ligamentto permit fast entry ofair
Temporizing procedure (CO2
retention)
Surgical Cricothyroidotomy
Incision with dissection to cricothyroidligament and placement of tracheotomy tube
Obstruction at the level of the vestibule of the larynx
-
7/31/2019 Clinical Review of Larynx Upper Resp Tract
30/36
Cricothyroidotomy
Site ofcricothyroidotomy
-
7/31/2019 Clinical Review of Larynx Upper Resp Tract
31/36
Prolonged intubation
Ventilation support
Manage bronchopulmonary secretion Upper airway obstruction
Obstructive sleep apnea
Bilateral vocal cord paralysis Inability to intubate
Major head & neck surgery or trauma
Indications for Tracheostomy
-
7/31/2019 Clinical Review of Larynx Upper Resp Tract
32/36
Advantages Lower risk of
laryngotracheal injury Improved
comfort/mobility Improve airway
stabilization
Allows for oralnutrition Improved secretion
clearance
Tracheostomy
-
7/31/2019 Clinical Review of Larynx Upper Resp Tract
33/36
Tracheostomy
ShoulderRoll
Transverse Incision
Sternal Notch
Incision through skin, fat, andmuscle
-
7/31/2019 Clinical Review of Larynx Upper Resp Tract
34/36
Tracheostomy
Anteriorjugular vein
Sternohyoidmuscle
Isthmusof thyroid
Ligated anteriorjugular vein
Trachea palpatedby index finger
Pretrachealvenous plexus
-
7/31/2019 Clinical Review of Larynx Upper Resp Tract
35/36
Tracheostomy
Index fingeron trachea
Incising thetrachea Knife spreading
the incision
Cruciateincision
Hook elevatingtracheal cartilage
Tape holding tracheotomytube in place
-
7/31/2019 Clinical Review of Larynx Upper Resp Tract
36/36
To know truly is to know by
causes.
- Francis Bacon, De Augmentis Scientiarum
mgtr jillo@srhs com