Clinical Presentation of Congenital Pulmonary Disorders Emily B. Gaerlan – Resurreccion,M.D. Pediatric Pulmonologist

Clinical Presentation of Congenital Pulmonary Disorders Emily B. Gaerlan – Resurreccion,M.D. Pediatric Pulmonologist.
Dec 23, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Clinical Presentation of Congenital Pulmonary Disorders
Emily B. Gaerlan – Resurreccion,M.D.
Pediatric Pulmonologist
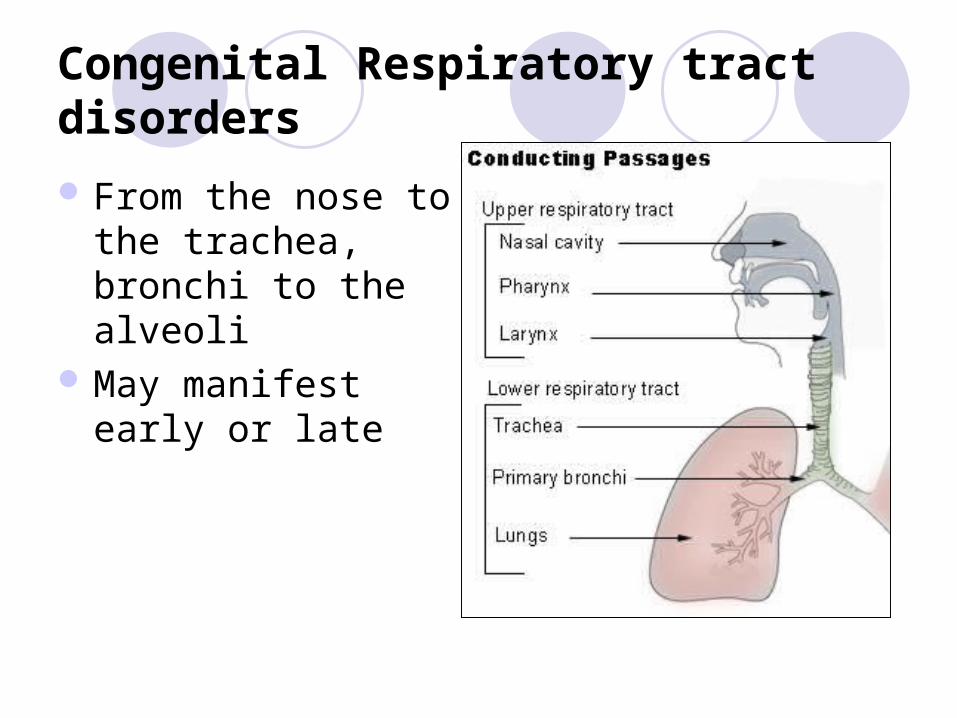
Congenital Respiratory tract disorders
From the nose to the trachea, bronchi to the alveoli
May manifest early or late
Systematic Approach
Six “trees” of the lung: bronchial arterial (systemic and pulmonary) venous (systemic and pulmonary) lymphatic
Systematic Approach
Bronchial venous drainage no known abnormalities
Three other areas with malformations: heart and great vessels chest wall abdomen
Multisystem disease

Presentation of Congenital Lung Disease
I. AntenatalII. NewbornIII. Later childhoodIV. Adulthood

ANTENATAL
Detected during routine fetal anomaly scan
Manifested by abnormalities of amniotic fluid
May also present with short limbs in skeletal dysplasia
Presentation of Congenital Lung Disease
Antenatalintrathoracic mass
pleural effusion
fetal hydrops
oligohydramnios/ polyhydramnios
other associated abnormalities discovered
ANTENATAL
Intrathoracic lesionsA. Solid Lesions
Microcystic adenomatoid malformation Pulmonary sequestration Right-sided diaphragmatic hernia Tracheal/laryngeal atresia Rhabdomyoma Mediastinal teratoma

ANTENATAL
Intrathoracic lesions
B. Cystic LesionsMacrocystic adenomatoid malformationCongenital diaphragmatic herniaBronchogenic cystMediastinal encephalocelePleural and pericardial effusion
NEWBORN PERIOD

Presentation of Congenital Lung Disease
Newborn periodrespiratory distress
stridor
bubbly secretions in mouth
failure to pass nasogastric tube
unable to establish an airway
cardiac failure
Presentation of Congenital Lung Disease
Newborn periodchance finding
cyanosis in a well infant
poor respiratory effort
NEWBORN PERIOD
I. Respiratory distress
II. Stridor
III. Dysphagia/feeding problems
IV. Wheezing
V. Recurrent Respiratory Infections
VI. Asymptomatic
I. Respiratory distress
May be manifested by tachypnea, cyanosis, grunting, presence of retractions
Early onset vs. late onset

I. Respiratory distress
A. Choanal atresia
B. Pyriform Aperture Stenosis
C. Congenital Midline Nasal Masses
D. Tracheal agenesis and atresia
E. Congenital Diaphragmatic Hernia
F. Congenital Large Hyperlucent Lobe
A. Choanal Atresia
most common congenital anomaly of the nose frequency of ≈1/7,000 live birthsCHARGE syndrome (coloboma, heart
disease, atresia choanae, retarded growth and development or CNS anomalies or both, genital anomalies or hypogonadism or both, and ear anomalies or deafness or both)

A. Choanal Atresia
Bilateral:• difficulty with mouth breathing, • make vigorous attempts to inspire, • often suck in their lips, and develop
cyanosis • crying relieves the cyanosis and become
calmer • repeats the cycle after closing their mouths
A. Choanal Atresia
Unilateral:• the infant may be asymptomatic for a prolonged
period, often until the 1st respiratory infection• Present with unilateral nasal discharge or
persistent nasal obstruction

A. Choanal Atresia
Diagnosis:• established by the inability to pass a firm
catheter through each nostril • seen directly with fiberoptic rhinoscopy • high-resolution CT

B. Pyriform Aperture Stenosis
bony abnormality of the anterior nasal aperture
Signs/Symptoms:
severe nasal obstruction at birth or shortly thereafter
Diagnosis: CT scan of the nose

C. Congenital Midline Nasal Masses
Dermoids, gliomas, and encephaloceles Present intranasally or extranasally and
may have intracranial connectionsDiagnosis: CT scan or MRI

D. Tracheal agenesis and atresia
rare anomalies that are incompatible with life
associated with other congenital anomalies, particularly laryngeal conditions and tracheoesophageal fistula
Diagnosis: bronchoscopy in the newborn with severe respiratory distress
E. Congenital Diaphragmatic Hernia
typically refers to the Bochdalek form communication between the abdominal
and thoracic cavities with or without abdominal contents in the thorax
can be associated with other congenital anomalies
E. Congenital Diaphragmatic Hernia
Respiratory distress is a cardinal sign in babies with CDH.
may occur immediately or there may be a “honeymoon” period of up to 48 hr when the baby is relatively stable
E. Congenital Diaphragmatic Hernia
May present beyond the neonatal period may experience vomiting as a result of
intestinal obstruction or mild respiratory symptoms

E. Congenital Diaphragmatic Hernia

F. Congenital Large Hyperlucent Lobe
P.E.• Hyperresonance in
affected hemithorax• diminished breath
sounds,• deviation of mediastinal
structures to the contralateral side
Diagnosis• Chest radiograph
II. Stridor
predominant monophonic noise inspiratory stridor caused by the
extrathoracic lesions of congenital laryngeal anomalies, specifically laryngomalacia and bilateral vocal cord paralysis
intrathoracic lesions typically cause expiratory wheezing or stridor

II. Stridor
A. Laryngomalacia
B. Congenital Subglottic Stenosis
C. Vocal Cord Paralysis
D. Congenital Laryngeal Webs and Atresia
E. Congenital Subglottic Hemangioma
F. Vascular and Cardiac Anomalies
G. Tracheal Stenoses and Webs

A. Laryngomalacia
Comprise 60% of congenital laryngeal anomalies in children
stridor is inspiratory, low pitched, and exacerbated by any exertion (crying, agitation, feeding), supine position, and viral infections of the upper airway
A. Laryngomalacia
Stridor results from the collapse of supraglottic structures inward during inspiration
appear in the first 2 wk of life and increase in severity up to 6 mo, although gradual improvement can begin at any time
Diagnosis: flexible laryngoscopy
B. Congenital Subglottic Stenosis
2nd most common cause of stridor Stridor is biphasic or primarily inspiratoryRecurrent or persistent croup is typical

C. Vocal Cord Paralysis
3rd most common congenital laryngeal anomaly
Congenital central lesions such as myelomeningocele, Arnold-Chiari malformation, and hydrocephalus are often associated

C. Vocal Cord Paralysis
Bilateral vocal cord paralysis:• high-pitched inspiratory • stridor, • a phonatory sound • inspiratory cry
Unilateral paralysis :• aspiration• coughing• choking
D. Congenital Laryngeal Webs and Atresia
Most congenital laryngeal webs are glottic with subglottic extension and associated subglottic stenosis
Diagnosis: direct laryngoscopy
E. Congenital Subglottic Hemangioma
Symptoms of airway obstruction typically occur in the 1st 2 mo of life
Stridor is biphasic but usually more prominent during inspiration

F. Vascular and Cardiac Anomalies
Vascular ring result from abnormal development of the aortic arch complex
symptomatic by 3 mo of age Signs/Symptoms:
• expiratory wheezing • cough • dysphagia
G. Tracheal Stenoses and Webs
typically presents in the 1st year of lifeprecipitated by an acute respiratory illnessDiagnosis: plain radiograph
bronchoscopy

III. Dysphagia/Feeding Problems
A. Vascular Ring
B. Foregut Cysts
C. Tracheoesophageal fistula/Esophageal Atresia

A. Vascular Ring
Respiratory symptoms predominate, but dysphagia may be present
Diagnosis : barium esophagogram

A. Vascular Ring
posterior indentation of the esophagus by the vascular ring.

B. Foregut Cysts
• Include bronchogenic cyst, intramural esophageal cyst (esophageal duplication), and enteric cyst
• Diagnosis: chest radiographs or CT scan

C. Tracheoesophageal fistula/Esophageal Atresia
Associated with maternal polyhydramnios
Signs/Symptoms• frothing • choking • cyanotic episodes
despite oral suction

IV. Wheezing

IV. Wheezing
A. Bronchomalacia
B. Tracheomalacia

A. Bronchomalacia/Tracheomalacia
common cause of persistent wheezing in infancy
either primary or secondary most affected patients are born term
A. Bronchomalacia/Tracheomalacia
Secondary tracheomalacia and bronchomalacia refers to the situation in which the central airway is compressed by adjacent structure (e.g., vascular ring) or deficient in cartilage due to tracheoesophageal fistula
A. Bronchomalacia/Tracheomalacia
dominant finding, low-pitched monophonic wheezing, most prominent over the central airways.
persistent respiratory congestion even in the absence of a viral respiratory infection
Diagnosis: flexible or rigid bronchoscopy

V. Recurrent Respiratory infection
A. Foramen of Morgagni Hernia
B. Congenital Cystic Lung Disease
C. Pulmonary Sequestration
A. Foramen of Morgagni Hernia
anteromedial diaphragmatic defect Signs/Symptoms:
• asymptomatic and are diagnosed beyond the neonatal period
Diagnosis: chest x-ray
B. Congenital Cystic Lung Disease
Congenital pulmonary airway malformationCystic congenital thoracic malformationFive types(0,1,2,3,4)Treatment: surgical excision

B. Congenital Cystic Lung Disease

C. Pulmonary Sequestration
lung tissue that does not connect to a bronchus
receives its arterial supply from the systemic arteries
returns its venous blood to the right side of the heart through the inferior vena cava (extralobar) or pulmonary veins (intralobar).

C. Pulmonary Sequestration
functions as a space-occupying lesion within the chest
it does not function in gas exchangeP.E: dullness to percussion
decreased breath sounds over the lesion
During infection, crackles may also be present
VI. Asymptomatic
Foramen of Morgagni HerniaCongenital Cystic Lung DiseaseEventration of the diaphragm
Eventration of diaphragm
abnormal elevation, consisting of a thinned diaphragmatic muscle producing elevation of the entire hemidiaphragm or, more commonly, the anterior aspect of the hemidiaphragm
produces a paradoxical motion of the affected hemidiaphragm
Most are asymptomatic

Eventration of diaphragm
Presentation of Congenital Lung Disease
Later Childhood/Adulthood
recurrent infection
hemoptysis, hemothorax
bronchiectasis, bronchopleural fistula
steroid-resistant airway obstruction
cardiac failure
malignant transformation
Presentation of Congenital Lung Disease
Later Childhood/Adulthood
cyanosis
coughing on drinking
chance finding of mass or hyperlucent area on chest radiograph

SUMMARY

Congenital Lung Disease
Can present any time from 20 weeks of gestation to old age
May regress to virtually nothingMay require surgery
Congenital Lung Disease
Gaps of knowledge:o long term consequences of the lesions
diagnosed antenatallyo need for registrieso need for refinement of MRI

Thank you
Related Documents











