Clinical Perspective Fracture Dislocations of the Proximal Interphalangeal Ioint Thomas R. Kiefhaber, MD, Peter I. Stern, MD, Cincinnati, OH The unprotected position and long moment arm of the proximal interphalangeal (PIP) joint make it vul- nerable to injury. Some injuries are purely ligamen- tous, while others result in an intra-articular fracture with or without subluxation or dislocation. Unfortu- nately, clinicians and coaches often relegate PIP in- juries to "nuisance status" and treat them with alarming casualness. As a result, patients are fre- quently surprised and frustrated by suboptimal out- comes and persistent impairment. Permanent swell- ing, pain, and variable degrees of stiffness often complicate adequate treatment of PIP joint injuries, and poorly designed or executed treatment frequently leads to marked stiffness, angulation, and degenera- tive changes. A thorough understanding of the forces acting on the injured PIP joint, the desired treatment goals, and available treatment options allows the design of a therapeutic program that maximizes long- term function. Previous reports have addressed treatment of PIP joint fracture dislocation, but several theoretical and practical issues remain unresolved. Is complete cor- rection of joint subluxation necessary? Must the frac- tured joint surface be anatomically restored? What is the role of early motion? How can diverse treatment From Cincinnati Hand Surgery Specialists, Cincinnati, OH; and the Department of Orthopaedic Surgery, University of Cincinnati, College of Medicine, Cincinnati, OH. No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article. Received for publication December 2, 1997; accepted in revised form February 9, 1998. Reprint requests: Thomas R. Kiefhaber, MD, 2800 Winslow Ave, Suite 401, Cincinnati, OH 45206. Copyright 1998 by the American Society for Surgery of the Hand. 0363-5023/98/23A03-000253.00/0 modalities be matched to fracture patterns? We ad- dress each of these issues below. Fracture Patterns Proximal interphalangeal joint fracture disloca- tions occasionally result from a pure extension or flexion force; however, the majority occur when there is some component of longitudinal load. As an example, a bungled ball catch, a frequent cause of PIP joint fracture dislocations, transmits a rapidly applied load containing substantial longitudinal force vectors and strong angulatory moments. The applied load direction and magnitude determine the fracture location and pattern. Middle phalangeal articular fractures at the PIP joint occur in 3 anatomic loca- tions, including dorsal lip fractures, palmar lip frac- tures, and central articular disruptions (Fig. 1). There are 2 fracture mechanisms: avulsion and impaction shear. Middle phalanx palmar lip fractures are the most frequently encountered form of osseous injury asso- ciated with PIP joint fracture dislocations. Pure PIP joint hyperextension nearly always disrupts the pal- mar plate either at its distal insertion or by creating a tension fracture at the palmar lip of the middle pha- lanx. These avulsion fractures range in size from tiny bony flecks to fragments comprising one third of the joint surface. Displacement may be substantial, but avulsion fragments exhibit little comminution. In contrast, a longitudinal load applied to the flexed 1 PIP joint drives the proximal phalanx head into the middle phalangeal base, shearing apart the articular surface and then impacting fragments into the under- lying metaphyseal bone. Comminution of up to 80% of the articular surface is common in these impaction shear injuries (Fig. 1A). Dorsal lip fractures also 368 The Journal of Hand Surgery

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Clinical Perspective Fracture Dislocations of the
Proximal Interphalangeal Ioint
Thomas R. Kiefhaber, MD, Peter I. Stern, MD, Cincinnati, OH
The unprotected position and long moment arm of the proximal interphalangeal (PIP) joint make it vul- nerable to injury. Some injuries are purely ligamen- tous, while others result in an intra-articular fracture with or without subluxation or dislocation. Unfortu- nately, clinicians and coaches often relegate PIP in- juries to "nuisance status" and treat them with alarming casualness. As a result, patients are fre- quently surprised and frustrated by suboptimal out- comes and persistent impairment. Permanent swell- ing, pain, and variable degrees of stiffness often complicate adequate treatment of PIP joint injuries, and poorly designed or executed treatment frequently leads to marked stiffness, angulation, and degenera- tive changes. A thorough understanding of the forces acting on the injured PIP joint, the desired treatment goals, and available treatment options allows the design of a therapeutic program that maximizes long- term function.
Previous reports have addressed treatment of PIP joint fracture dislocation, but several theoretical and practical issues remain unresolved. Is complete cor- rection of joint subluxation necessary? Must the frac- tured joint surface be anatomically restored? What is the role of early motion? How can diverse treatment
From Cincinnati Hand Surgery Specialists, Cincinnati, OH; and the Department of Orthopaedic Surgery, University of Cincinnati, College of Medicine, Cincinnati, OH.
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Received for publication December 2, 1997; accepted in revised form February 9, 1998.
Reprint requests: Thomas R. Kiefhaber, MD, 2800 Winslow Ave, Suite 401, Cincinnati, OH 45206.
Copyright �9 1998 by the American Society for Surgery of the Hand. 0363-5023/98/23A03-000253.00/0
modalities be matched to fracture patterns? We ad- dress each of these issues below.
Fracture Patterns
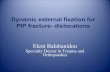
Proximal interphalangeal joint fracture disloca- tions occasionally result from a pure extension or flexion force; however, the majority occur when there is some component of longitudinal load. As an example, a bungled ball catch, a frequent cause of PIP joint fracture dislocations, transmits a rapidly applied load containing substantial longitudinal force vectors and strong angulatory moments. The applied load direction and magnitude determine the fracture location and pattern. Middle phalangeal articular fractures at the PIP joint occur in 3 anatomic loca- tions, including dorsal lip fractures, palmar lip frac- tures, and central articular disruptions (Fig. 1). There are 2 fracture mechanisms: avulsion and impaction shear.
Middle phalanx palmar lip fractures are the most frequently encountered form of osseous injury asso- ciated with PIP joint fracture dislocations. Pure PIP joint hyperextension nearly always disrupts the pal- mar plate either at its distal insertion or by creating a tension fracture at the palmar lip of the middle pha- lanx. These avulsion fractures range in size from tiny bony flecks to fragments comprising one third of the joint surface. Displacement may be substantial, but avulsion fragments exhibit little comminution. In contrast, a longitudinal load applied to the flexed 1 PIP joint drives the proximal phalanx head into the middle phalangeal base, shearing apart the articular surface and then impacting fragments into the under- lying metaphyseal bone. Comminution of up to 80% of the articular surface is common in these impaction shear injuries (Fig. 1A). Dorsal lip fractures also
368 The Journal of Hand Surgery
The Journal of Hand Surgery/Vol. 23A No. 3 May 1998 369
A
Figure 1. Proximal interphalangeal joint fracture dislocation patterns. (A) Palmar lip fracture with dorsal subluxation. Palmar lip fractures can be of the avulsion or impaction shear type. In the impaction shear injury depicted here, the palmar 50% of the articular surface is damaged. The palmar plate remains attached to the anterior lip of the middle phalanx and there is impaction of articular cartilage into the underlying metaphyseal bone. Subtle dorsal subluxation is appreciated by observing a V-shaped gap between the articular surfaces of the head of the proximal phalanx and the undamaged portion of the middle phalanx base. (B) Dorsal lip fracture with palmar subluxation. Dorsal lip fractures can be of the avulsion or impaction shear type. Loss of middle phalangeal articular surface contour, as depicted in this impaction shear injury, accentuates palmar translation of the middle phalanx. (C) Pilon fracture.* By definition, pilon fractures include disruption of both the dorsal and palmar cortical margins. The central articular fragments are often comminuted and impacted into the underlying metaphyseal bone. (*Adapted from Kiefhaber TR. Phalangeal dislocations/periarticular trauma. In: Peimer CA, ed. Surgery of the hand and upper extremity. Vol. 1. New York: McGraw-Hill, 1996:963, with permission of The McGraw-Hill Companies.)

370 Kiefhaber and Stern / PIP Joint Fracture Dislocations
occur by avulsion or impaction shear mechanisms. Forced PIP joint hyperflexion results in central ten- don failure through its substance or at its bony at- tachment. Longitudinal load combined with PIP joint extension I creates a dorsal lip impaction shear frac- ture with characteristics similar to palmar injuries, a rare fracture pattern in our experience (Fig. 1B).
A large, straightforward, longitudinal load crush- ing the middle phalangeal base is a pattern that Stern et al.2 termed a "pilon" fracture. By definition, pilon fractures disrupt both the dorsal and palmar middle phalangeal cortical margins. Articular surface com- minution is extensive, and the central fragments im- pact into the underlying metaphyseal bone (Fig. 1C).
Is Joint Reduction Necessary?
Middle phalangeal translation on the proximal phalangeal head (i.e., PIP joint subluxation or dislo- cation) can be observed with dorsal or palmar lip fractures. Is restoration of PIP joint congruency a prerequisite for an acceptable clinical outcome? De- finitive studies comparing reduced and persistently subluxed PIP joint fracture dislocations are lacking, but several investigators 3-s report poor results with persistent subluxation. Hamer and Quinton 3 reported 27 PIP joint fracture dislocations treated with exten- sion block splinting and noted a "less favorable outcome" in 4 of the 5 joints that healed with slight dorsal subluxation. In a series of 7 PIP joint fracture dislocations treated with a dynamic external fixator, Inanami et al. 4 reported that the only patient experi- encing posttreatment pain had persistent dorsal sub- luxation. Krakauer and Stern s reported 12 PIP frac- ture dislocations treated with a dynamic hinged external fixator. Three developed recurrent subluxa- tion, 1 progressed to bony ankylosis, and 2 exhibited advanced radiographic degenerative changes, lead- ing to the conclusion that satisfactory outcome is predicated on first obtaining, and then maintaining, a congruously reduced joint.
Investigators favoring procedures or devices de- signed to obtain reduction provide indirect evidence supporting congruous PIP joint reduction. Many methods of preventing recurrent subluxation or dis- location by limiting PIP joint extension have been described and include extension limiting splint- ing, 3'6'7 extension block pinning, 8-1~ external fixa- tion devices, 4"5'11-16 and skeletal traction. 16"17 Re- searchers reporting open reduction and internal fixation techniques 18-21 include joint subluxation as their primary surgical indication, and proponents of
palmar plate ar throplas ty 22-27 recommend the proce- dure as an excellent method of restoring joint con- gruency.
Finally, established investigators 28'29 draw conclu- sions regarding correction of subluxation based on their clinical experience. Hastings and C a r r o l l 19 re - viewed 48 palmar lip fractures and summarized, "Results parallel the accuracy of joint reduction- . . . subtle incongruities in the matching articular
surface of the proximal phalanx and the remaining dorsal articular surface of middle phalanx lead to failure." In discussing dorsal subluxation associated with PIP joint fracture dislocations, Bowers 3~ states, "A dorsally subluxed PIP joint cannot be expected to work properly, and it never will." Despite a few anecdotal reports of functional but subluxated PIP joints, 19'31 the preponderance of the literature sup- ports anatomic PIP joint reduction.
In contrast to most other investigators, Schenck's 3a report of the results of PIP joint fracture dislocations treated with traction and early motion does not stress the importance of dorsal subluxation correction. His traction method prevents collateral ligament contrac- tures and allows middle phalanx articular surface re- modeling that leads to "good articular symmetry." We believe that traction keeps the capsular structures dis- tracted, allowing the middle phalanx to glide around the proximal phalangeal head instead of hinging at the fracture margin. A lateral radiograph in extension may reveal slight dorsal subluxation, but a second x-ray obtained with the joint positioned in flexion demon- strates that the middle phalanx reduces and congruently glides around the proximal phalangeal head. Palmar fragment consolidation restores stability and prevents recurrent subluxation.
Based on the literature and our experience, we conclude that successful PIP joint fracture disloca- tion treatment restores the natural middle phalangeal glide around the proximal phalanx head and prevents hinging at the fracture margin. Proximal interphalan- geal joint subluxation precludes a normal gliding flexion arc and must be corrected (Fig. 2).
Is Anatomic Reduction of the Joint Surface Necessary?
In theory, long-term PIP joint function should be enhanced by minimizing articular surface gaps or step off. Clinical experience supports anatomic re- duction of intra-articular fractures in weight-bearing joints such as the hip or knee. Knirk and Jupi ter 33 and Bradway et al . 34 report a substantial reduction in

The Journal of Hand Surgery / Vol. 23A No. 3 May 1998 371
Z < _ _ . _ ~ < ~ �9
3
Figure 2. Proximal interphalangeal flexion/glide versus hinging. (A) Restoration of the normal glide of the middle phalanx around the head of the proximal phalanx requires complete elimination of middle phalangeal dorsal subluxation. (B) Hinging of the middle phalanx (depicted here) portends an unacceptable clinical result.
radiographically apparent posttraumatic degenerative changes when distal radius articular surface step offs or separations are limited to -<2 mm. Should similar guidelines be applied to PIP joint fracture disloca- tions?
Surprisingly, few investigators recommend ana- tomic joint surface reduction. Proponents of open reduction and internal fixation 18a9'21 report good re- suits after anatomic surface reconstruction, but these
studies lack comparison to joints allowed to heal with incompletely reduced articular surfaces. In a review of 16 PIP joint fracture dislocations treated with extension block splinting, Hamer and Quinton 3 blame 5 cases with poor results on the presence of a depressed middle phalanx central fragment; how- ever, they also note that these joints exhibited dorsal subluxation, thus leaving in doubt whether the unac- ceptable outcome resulted from articular irregularity

372 Kiefhaber and Stern / PIP Joint Fracture Dislocations
or persistent PIP joint subluxation. Proponents of the palmar plate arthroplasty note that this procedure allows resurfacing of irregular, fractured articular cartilage with the smooth palmar pla te . 23-25 Malerich and Eaton 22 state, "Incongruities or irregularities of these surfaces inevitably lead to decreasing motion and pain," but their statement is not supported by clinical data.
Most laboratory and clinical reports support the concept that anatomic surface restoration is unnec- essary if subluxation is corrected and motion is in- stituted shortly after injury. Salter's 35 laboratory studies demonstrate that continuous passive motion has a profoundly positive effect on cartilage healing. The practical applicability of Salter's work to PIP joint fracture dislocations is demonstrated by numer- ous clinical reports illustrating good outcomes ob- tained by accepting incomplete articular reduction and instituting early motion. Agee 15 reported that 7 of 16 patients treated with a force couple and imme- diate motion had an excellent outcome in spite of unreduced central fragments. Schenck 32 reported 10 PIP joint fracture dislocations treated with traction and passive motion, and illustrated 2 joints that re- gained a nearly full arc of pain-free motion despite persistent articular surface irregularities. Morgan et al. 16 reported 14 comminuted PIP joint fracture dis- locations treated with traction and immediate mo- tion, and noted that persistent central fragment depression did not adversely affect outcome. Addi- tional evidence is found in several articles that illus- trate cases depicting successful treatment of PIP joint fracture dislocation despite persistently de- pressed middle phalangeal joint surface frag- ments.3,4,7,8,10,11,17,31
Reports of pilon fractures provide the most com- pelling evidence against the necessity of anatomic joint surface reduction. Stem et al. 2 compared the results of pilon fractures treated with splint immobi- lization, open reduction and internal fixation, or trac- tion. Of 4 splinted fractures, all experienced major residual pain, 2 severe enough to warrant arthrodesis. Seven of the 9 fractures treated with open reduction and internal fixation resulted in persistent pain, 1 requiring arthrodesis. Traction provided the best out- come even though anatomic joint surface reduction was not obtained. Four of the 7 pilon fractures treated with traction were pain free, none required additional surgery, and all recovered an acceptable range of motion. Stern et al. also noted that the middle phalanx base remodeled, assuming a widened shape that matched the head of the proximal phalanx,
a phenomenon also observed by others.l~ ,36 Morgan et al. 16 treated 5 pilon fractures with skeletal traction and early range of motion; 4 became pain free and 1 had activity related mild discomfort. Two of Schenck' s 32 10 PIP joint fracture dislocations treated with skeletal traction demonstrated 100% articular surface involvement and fit the definition of a pilon fracture. Both did well even though there was lack of anatomic joint surface reduction. We conclude that anatomic joint surface restoration is unnecessary if subluxation is fully corrected and early motion is instituted.
Treatment Guidelines
We have established the following guidelines in our treatment of PIP fracture dislocations:
1. Restoration of the middle phalangeal glide around the proximal phalangeal head during the flexion arc is paramount. Hinging at the fracture site must be avoided. To accomplish this goal, the surgeon must eliminate joint subluxation and then re-establish joint stability to prevent recurrent subluxation.
2. Early motion should be initiated whenever possible. This enhances cartilage and soft tissue healing and minimizes adhesions or contractures.
3. Anatomic restoration of the fractured joint surface is a desirable but much less important treatment goal.
Classification
A useful classification should help select the sim- plest treatment that restores a concentric stable joint, initiates early motion, and obtains the best, most practical joint surface reconstitution. Understanding the forces acting on the injured joint allows injury classification based on stability and the selection of treatment that neutralizes the deforming forces. We have divided PIP joint fracture dislocations into 3 broad categories based on the location of the middle phalanx articular fracture: dorsal lip, palmar lip, and pilon fractures. Each category is subdivided based on the fracture pattern's postreduction stability (Table 1). Fractures within each subcategory are subjected to identical biomechanical forces and require the application of similar treatment principles to achieve an acceptable outcome.
Joint Stability Biomechanical studies 37 establish the palmar plate
as the primary PIP joint palmar stabilizer; however, recurrent dorsal dislocation after palmar plate arthro- plasty is a recognized complication that occasionally

Table 1. Stability-Based Classification of Proximal Interphalangeal Joint Fracture Dislocations
Palmar lip fracture Stable (<30% articular surface, reduced in extension)
No PIP hyperextension Hyperextensible PIP (swan neck)
Tenuous (30% to 50% articular surface and reduction maintained with <30 ~ flexion)
Unstable (>50% articular surface or 30% to 50% requiring >30 ~ of flexion to maintain reduction)
Dorsal lip fracture Stable (in extension) Unstable (palmar translation of middle phalanx)
Pilon fracture
PIP, proximal interphalangeal.
occurs even when theprocedural details and postop- erative immobilization protocol are accurately exe- cuted. Eaton and Malerich 23 reported redislocation in 1 case despite 3.5 weeks of immobilization. Hastings and C a r r o l l 19 re-explored a re-dislocated palmar plate arthroplasty and found the palmar plate firmly attached to the fracture bed, but the head of the proximal phalanx displaced into the underlying me- taphyseal defect, allowing recurrent dorsal subluxa- tion. At the 1992 American Society for Surgery of the Hand Annual Meeting, we reported 3 palmar plate arthroplasties that re-dislocated after removal of the postoperative transarticular Kirschner wire (K-wire). In each case, the bony defect left by the fracture was wider than the thickness of the palmar plate and settling was observed. We concluded that palmar plate reattachment p e r se does not restore stability to PIP joint fracture dislocations.
In his 1971 classification of PIP joint dislocations, Eaton as postulated stability loss when the "critical corner," the combined lateral collateral ligament and palmar plate insertion, separated from the middle phalanx by avulsion or fracture. In a 1982 reclassi- fication, Eaton and Dray 39 recognized that fractures involving more than 40% of the middle phalanx palmar joint surface are "unstable" and prone to recurrent dorsal subluxation. These investigators postulated that smaller, "stable" fractures are stabi- lized by the few collateral ligament fibers that re- mained attached to the middle phalanx. The dorsal- palmar stability imparted by the collateral ligaments is arguable, but Eaton's classification establishes a direct relationship between the size of the middle phalanx palmar lip fracture and postreduction sta- bility. Several other authors acknowledge this rela-
The Journal of Hand Surgery / Vol. 23A No. 3 May 1998 373
tionship 5'18'2~176 and predict dorsal instability when palmar lip involvement reaches 30% 43 or 40% 5"18"21"23"44"45 of the middle phalanx.
Does the palmar plate and ligamentous insuffi- ciency accompanying large fractures cause PIP joint instability or is the bony architectural alteration to blame? Wilson and Rowland 4~ and Zemel et al.46 advocated the use of osteotomy and bone grafting of malunited palmar lip fractures to reestablish the cup- shaped middle phalanx articular contour to restore joint stability. Wilson and Rowland 4~ stated, "In most fracture dislocations of this joint, however, the buttressing effect of the palmar lip must be restored before joint stability is assured."
In summarizing the biomechanical importance of the middle phalanx palmar lip, Hastings and Car- roll 19 noted several factors that were responsible for dorsal subluxation of the middle phalanx. When the cup-shaped middle phalanx articular surface is al- tered by a palmar lip fracture, the dorsal-proximal to distal-palmar orientation of the remaining articular surface allows the central tendon to lift the middle phalanx up and over the proximal phalanx head. The middle phalangeal flexor digitorum superficialis in- sertion site accentuates the joint's tendency to hinge at the fracture edge and further destabilizes palmar lip fractures (Fig. 3). This biomechanical model combined with the available clinical evidence leads to 2 conclusions: a direct relationship exists between palmar lip fragment size and dorsal instability, and restoration of stability requires reconstruction of an adequate middle phalanx palmar buttress.
Fracture size and pattern are excellent predictors of instability, but actual subluxation proclivity is best confirmed by physical examination. The surgeon can test "unstressed instability ''27 of the PIP joint by asking the patient to actively move the joint, follow- ing digital block anesthesia, through an arc of motion, observing for clinical dislocation or sub- luxation. Stability is confirmed by obtaining a post- reduction lateral radiograph in full PIP joint exten- sion. When subluxation is identified, the surgeon determines the degree of flexion required to maintain reduction, applies the chosen treatment method, and obtains a second radiograph to confirm reduction.
Palmar Lip Fracture Classi f icat ion
Previous classification systems quantify fracture size and subluxation 47 or group PIP joint fracture dislocations into anatomic patterns. 48 Since our goal is to design a classification system that relates post- reduction stability to treatment methods, we must go

374 Kiefhaber and Stern / PIP Joint Fracture Dislocations
Figure 3. Forces acting on palmar lip fractures. The extensor apparatus lifts the middle phalanx over the head of the proximal phalanx, a motion that is accentuated by the slope of the remaining undamaged middle phalangeal articular surface. Dorsal displacement is further accentuated by the distal lever arm of the flexor digitorum superficialis tendon. The only factors resisting dorsal migration of the middle phalanx are the palmar plate and the cup-shaped geometry of the middle phalanx base, stabilizers that are disrupted by palmar lip fractures. (Adapted from Kiefhaber TR. Phalangeal dislocations/periarticular trauma. In: Peimer CA, ed. Surgery of the hand and upper extremity. Vol. 1. New York: McGraw-Hill, 1996:957, with permission of The McGraw-Hill Companies.)
beyond fracture description alone and quantify func- tional stability. McElfresh et al. 6 and Hastings and Carroll 19 provide the foundation for our stability- based classification by stratifying PIP joint fracture dislocations according to the percentage of middle phalanx articular surface disrupted: 30% or less is presumed to be stable; 30% to 50% has tenuous stability; and more than 50% is an unstable joint (Fig. 4). We combine physical examination with fracture site quantification to functionally group PIP joint palmar lip fractures into 3 categories: stable, tenuous, and unstable. Stable. Stable fracture dislocations involve less that 30% of the middle phalanx palmar lip and are stabile in full PIP joint extension. Because the rare, small palmar lip fracture allows dorsal subluxation, ~8'2~ stability should be confirmed by radiographically demonstrating congruent reduction with the PIP joint in full extension. Stable palmar lip fractures are subdivided into 2 groups, those in which the PIP joint actively hyperextends (swan-neck deformity) and those that extend only to neutral.
Figure 4. Palmar lip fracture classification. Stable frac- tures involve less than 30% of the articular surface and demonstrate no tendency to subluxate, even when the proximal interphalangeal (PIP) joint is fully extended. Tenuous fractures involve 30% to 50% of the middle phalangeal articular surface but remain reduced when the joint is flexed to --<30 ~ . All PIP joint fractures involving -->50% of the joint surface are categorized as unstable. Fractures involving 30% to 50% of the middle phalangeal base that require more than 30 ~ of flexion to maintain reduction are also classified as unstable. (Adapted from Kiefhaber TR. Phalangeal dislocations/periarticular trauma. In: Peimer CA, ed. Surgery of the hand and upper extremity. Vol. 1. New York: McGraw-Hill, 1996:958, with permission of The McGraw-Hill Companies.)

The Journal of Hand Surgery / Vol. 23A No. 3 May 1998 375
Tenuous. When 30% to 50% of the middle pha- lanx joint surface is fractured, stability is tenuous and can only be determined by clinical testing. Joints that reduce with --<30 ~ of flexion remain in the tenuous group. Joints requiring more than 30 ~ of flexion are assigned to the unstable category. Unstable. All PIP joint fractures involving ->50% of the joint surface are categorized and treated as unstable, as well as 30% to 50% fractures that re- quire more than 30 ~ of flexion to maintain reduction.
Dorsal Lip Fracture Classification
The stability-based palmar lip classification and treatment principles also apply to dorsal lip fractures. The joint must be reduced and the middle phalanx articular contour restored to attain stability. Addi- tionally, central tendon continuity must be reestab- lished, a task that usually requires immobilization in extension. Because dorsal lip fractures are either stable or unstable in full extension, the tenuous cat- egory is eliminated. Stable. Stable dorsal lip fractures are those in which the PIP joint is positioned in full PIP extension and there is no palmar subluxation. The fracture pattern may be of the avulsion or impaction shear type and involve up to 50% of the joint surface; but a lateral radiograph in full extension demonstrates that the middle phalanx palmar articular surface re- mains in congruous contact with the proximal pha- lanx head. Unstable. All fractures that allow middle phalan- geal palmar translation when the PIP joint is in extension are classified as unstable, regardless of size or comminution.
Treatment Options Proximal interphalangeal joint fracture dislocation
treatment methods are grouped into 5 broad catego- ries: static immobilization, dorsal extension block splinting, longitudinal traction, open reduction and internal fixation, and palmar plate arthroplasty.
Static Immobilization Splint 49 or transarticular K-wire 19'3~ static immo-
bilization is simple but must be used judiciously. Articular reduction must be serially monitored by x-ray, and immobilization for more than 3 weeks may result in permanent stiffness.
Dorsal Extension Block Splints
McElfresh and collegues 6'7 proposed a PIP joint dorsal fracture dislocation treatment program based
on the observation that dorsal subluxation usually corrects with PIP joint flexion. A short arm cast with a dorsal extension block outrigger allows full active PIP joint flexion but blocks extension, thus maintain- ing the joint in a reduced position. Other investiga- tors have modified the splint design, 3'5~ but did not change the principles of maintaining reduction with PIP joint flexion and allowing early motion. Others use the same concept, but provide the extension block with a K-wire protruding from the proximal phalanx head. 3'8"9
Longitudinal Traction Devices
Robertson et al. 17 designed a 3-pin traction device that applies PIP joint distraction through a middle phalanx pin, while 2 additional pins, 1 through the proximal phalanx neck and the other through the middle phalanx base, correct dorsal subluxation. Agee 14'15 proposed a force couple that maintains joint reduction through a palmarly directed force applied to the middle phalanx while simultaneously allowing active motion. Schenck 32 and Morgan et al.16 capitalize on the benefits of early motion by using traction devices that allow both longitudinal distraction and passive PIP joint motion. Other ex- ternal devices provide static immobilization, 3~ apply a longitudinal force alone, 11 or combine traction with a subluxation controlling palmarly directed force. 4 Dynamic external fixators designed by Hastings and Ernst 44 and Kasparyn and Hotchkiss 51 allow imme- diate active motion while maintaining longitudinal traction and subluxation correction.
Open Reduction and Internal Fixation
Open reduction and internal fixation has limited applicability. It can be used to fix a noncomminuted fragment that is sufficiently large to stabilize with small lag screws or K-wires. 2~176 Pull-out su- tures, 18'4~ tension banding, 52 or a combination of techniques secure the more commonly encountered small comminuted fragments. Elevation of impacted fragments often leaves a metaphyseal void that can be filled with cancellous bone graft. 5'18"2~
Palmar Plate Arthroplasty
Malerich and Eaton 22'23 designed and others have used 24'25 an ingenious procedure for the treatment of dorsal fracture dislocations. The palmar plate is ad- vanced into the middle phalanx fracture defect, si- multaneously restoring stability and resurfacing the damaged articular surface. Hastings and col-

376 Kiefhaber and Stern / PIP Joint Fracture Dislocations
leagues, 19"44 Kiefhaber , 53 and Krakauer and Stern 5 advocate replacing the originally proposed postoper- ative K-wire immobilization with a dynamic external fixator to realize the benefits of early motion.
Treatment of Palmar Lip Fractures
If the hypothesis is accepted that restoring the normal gliding motion of the middle phalanx around the proximal phalangeal head is a prerequisite to an acceptable clinical outcome, then obtaining and maintaining a concentric joint reduction becomes the primary treatment goal. The classification system outlined above groups palmar lip fractures based on predicted stability and allows selection of the sim- plest treatment modality that restores stability and allows maximum motion.
Stable Palmar Lip Fractures
Stable palmar lip fractures do not cause PIP joint subluxation and are treated by programs that maxi- mize motion. The minority of stable palmar lip frac- tures permit PIP joint hyperextension, which, if un- corrected, may lead to a swan neck deformity. To promote palmar plate healing, hyperextensible pal- mar lip fractures can be treated with an extension block splint. A figure-of-8 splint 53 can be fabricated to prevent terminal extension but allow full flexion. Alternatively, the double aluminafoam splint method of Strong 5~ can be used to maintain 20 ~ of PIP joint flexion for 3 weeks and then adjusted to 10 ~ of additional extension over the next 2 weeks.
Nonhyperextensible stable palmar lip fractures are best treated with early motion protected by taping the finger to the adjacent digit. Fracture size or displace- ment are unimportant as long as the joint shows no tendency to hyperextend or subluxate. Phair et al., 54 conducting a study of 74 stable palmar lip fractures treated with a variety of techniques, reported frag- ment displacement in 68% and eventual nonunion in 30%, but noted that excessive immobilization was the only factor leading to an unacceptable outcome. Splint immobilization for stable palmar lip fractures is not recommended because it can lead to stiffness and persistent flexion contractures.
Tenuous Palmar Lip Fractures
Tenuous palmar lip fracture dislocations involve 30% to 50% of the palmar articular surface of the proximal phalanx and concentrically reduce with less than 30 ~ of flexion. Treatment must maintain joint reduction until palmar fragment consolidation re-
stores the middle phalanx palmar buttress. This can be accomplished in a number of ways. Static immo- bilization with splint or transarticular wire predict- ably restores stability, but deprives the joint and surrounding soft tissues of the benefits of early mo- tion. Open reduction and internal fixation, external fixation, and traction all require surgical intervention with possible complications. We avoid complex treatments and recommend extension block splint- ing. Regardless of the splint design, congruous joint reduction must be assured by obtaining lateral radio- graphs with the joint extended to the limit allowed by the splint. Any dorsal subluxation of the middle phalanx is unacceptable and must be corrected by increasing the flexion angle.
If 30 ~ of flexion fails to restore reduction, the injury must be reclassified as unstable and an appro- priate treatment method selected. The treatment pro- gram should be monitored carefully with serial lat- eral radiographs and physical examinations to assure patient compliance and reduction maintenance. After 3 weeks, allowed extension is increased weekly in 10 ~ increments and reduction is confirmed radio- graphically. Splinting is discontinued when full ex- tension is achieved, usually 6 to 8 weeks after injury.
Unstable Palmar Lip Fractures
The primary treatment goal for unstable palmar lip fractures is to obtain and maintain reduction so that PIP joint flexion is accomplished by the normal middle phalangeal glide around the proximal phalan- geal head and not by hinging at the fracture edge. Accomplishing this goal requires reconstructing the stability enhancing middle phalanx palmar lip. A large, single fragment may be fixed with Kirschner pins or lag screws, but the more commonly encoun- tered small, comminuted, and impacted fragments require either traction, dynamic external fixation, or palmar plate arthroplasty. Traction or dynamic ex- ternal fixation are appropriate for unstable PIP joint fracture dislocations only when the joint reduces congruently and the fracture fragments align, restor- ing middle phalangeal geometry.
Palmar plate arthroplasty is our preferred form of treatment for unstable PIP fracture dislocations. This procedure reconstructs the middle phalanx palmar buttress and restores palmar plate continuity in a single procedure. Postoperative redislocation is avoided by assuring that the palmar plate is thor- oughly buttressed. The palmar plate, which has been advanced to the articular base of the middle phalanx, may not entirely fill the fracture void. In such cases,

The Journal of Hand Surgery / Vol. 23A No. 3 May 1998 377
any gap between the palmar plate and middle pha- langeal cortex is filled with fragments of excised bone, cancellous bone graft, or a superficialis tendon slip. With increasing frequency, we are abandoning K-wire fixation and using a dynamic external fix- ator 53 to keep the middle phalanx reduced while allowing immediate active and passive motion.
Treatment of Chronic Dorsal Fracture Dislocations
Chronic dorsal dislocation of the PIP joint allows the proximal phalanx head to sink into the middle phalangeal fracture site. Limited flexion occurs by hinging as opposed to gliding, and articular erosion develops at the contact point. When determining whether reduction is practical, the surgeon should assess the condition of the intact articular cartilage by inspecting the lateral radiograph. Irregularities or erosions in the nonarticulated surfaces suggest a poor prognosis and arthrodesis or arthroplasty should be considered. Joint reduction often is possible, even in longstanding, chronic dislocations. Reduction brings the undamaged surfaces into contact and allows a useful flexion arc.
Obtaining and maintaining reduction in longstand- ing subluxations is difficult. Donaldson and Mil- lender 36 stressed the importance of surgically releas- ing all extensor adhesion and clearing scar tissue from the proximal phalangeal retrocondylar recess. Theys investigators restored stability by temporarily pinning the joint in 90 ~ of flexion while the palmar structures consolidate. Patel and Joshi 42 applied an external fixator to gradually stretch contracted tissues followed by joint flexion to obtain reduction and encourage palmar structure contraction.
Several surgeons recommend a soft tissue restraint to PIP joint dorsal translation with 155,56 or both 57 flexor digitorum superficialis tendon slips or a pal- maris longus tendon graft, 58 but predictably, re-es- tablishing stability requires restoration of the cup- shaped geometry of the middle phalanx by corrective osteotomy or palmar plate arthroplasty. 4~ W e pre- fer palmar plate arthroplasty because it resurfaces the palmar surface of the middle phalanx, tightens the palmar plate, and restores the middle phalanx palmar buttress in a single procedure. Since extensor tenol- ysis and dorsal PIP capsulotomy require mobilization in the immediate postoperative period, use of a dy- namic external fixator should be considered to main- tain reduction and allow early postoperative motion.
Treatment of Dorsal Lip Fractures
Successful treatment of PIP joint dorsal lip frac- ture dislocations requires accomplishing all of the goals stated for palmar lip fractures in addition to re-establishing central tendon continuity. At least 1 collateral ligament must rupture for dorsal lip frac- tures to be associated with middle phalangeal palmar subluxation. 59 The continuity of the collateral liga- ments are evaluated by performing a lateral stress test. Lateral instability of greater than 20 ~ indicates complete collateral ligament disruption 6~ and exten- sive soft tissue damage that must be considered when designing treatment strategies. 6~
Stable Fractures
Stable fractures do not palmarly subluxate, and the primary treatment objective is to re-establish central tendon continuity. Most stable fractures are mini- mally comminuted and range in size from a small fleck to a large fragment. Like mallet fractures, mod- erately separated lip fragments proceed to osseous or stable fibrous union. There is debate as to the amount of fragment separation that compromises central ten- don function. Isani 43 suggested that restoration of central slip function required anatomic reduction, but we have achieved acceptable results by accepting up to 2 mm separation.
Stable dorsal lip fractures with -<2 mm of frag- ment displacement should be immobilized in full PIP joint extension for 4 weeks with a splint or transar- ticular K-wire; the distal interphalangeal joint should not be immobilized, and hourly active and passive terminal phalangeal joint motion should be encour- aged. At 4 weeks, the PIP joint should be placed in a dynamic extension splint that allows active flexion, and at 6 weeks, passive flexion and strengthening should be instituted.
Fragments with greater than 2 mm of displacement lead to an excessive extensor deficit and warrant open reduction and internal fixation. Whenever pos- sible, stable fixation that allows immediate postop- erative motion is achieved by using lag screws, 2~ pins coupled with a tension band wire, ~9 a pull-out suture, or 2 K-wires.
Unstable Fractures
The goals of joint reduction, stability restoration, and central tendon repair are accomplished by open reduction and internal fixation of large, noncommi- nuted dorsal fragments, but highly comminuted and

378 Kiefhaber and Stern / PIP Joint Fracture Dislocations
impacted fractures present difficult technical chal- lenges. If the overall cup-shaped geometry of the dorsal lip is restored when the joint is reduced, the PIP joint is pinned in full extension, thus allowing the dorsal fragments and the central tendon insertion to consolidate. Dorsal lip surgical reconstruction be- comes necessary when the middle phalanx cup- shaped geometry is not restored following joint re- duction. Fragment elevation and bone grafting ~9 or central tendon suturing into the fracture bed z8 are options, but significant postoperative stiffness fre- quently complicates both methods. The tendon ad- hesions and joint contractions may be limited by applying a hinged fixator to neutralize palmar trans- location forces and allow early motion, s'44 In a novel departure from the routine treatment protocol, Mor- gan et al. j6 treated 2 palmar fracture dislocations with traction and immediate motion without protect- ing the central tendon. Both patients had excellent results and less than 5 ~ of extensor lag. This method may provide an acceptable treatment alternative when the dorsal lip fragment moves with the middle phalanx and separates less than 2 ram.
Treatment of Pilon Fractures
Good results can be obtained when all 3 PIP joint fracture dislocation treatment principles are applied to pilon fractures. Foremost, the normal middle pha- langeal glide around the proximal phalangeal head must be restored. Accomplishing this requires re- establishment of proximal and middle phalanx colin- earity. Stability of the PIP joint is restored by frag- ment realignment that reapproximates the middle phalanx cup-shaped geometry, including the all-im- portant palmar buttress. Immediate motion compen- sates for less than anatomic joint surface reduction. Stern et al., 2 Morgan et al., 16 and Schenck 32 have clinically demonstrated the efficacy of traction in accomplishing these goals.
The surgeon should place pilon fractures in trac- tion and begin active or passive motion, as soon as possible. The traction method chosen is not as im- portant as the surgeon's experience with the device and adherence to postoperative management details. The biplanar radiographs in traction should be care- fully assessed to determine proximal and middle phalanx colinearity, angulation in the frontal plane, and overall fragment alignment. Occasionally, it may be necessary to perform percutaneous pinning or limited open reduction and internal fixation to ele- vate asymmetric fragment depression, which, if left
untreated, portends unacceptable angulation. A sec- ond indication for limited open reduction and inter- nal fixation is failure of the fracture fragments of the middle phalanx to assume a stable cup-shaped posi- tion. The method of fixation chosen by the surgeon should allow immediate mobilization. Traction is discontinued at 6 weeks and an aggressive range of motion program is maintained. These treatment guidelines usually result in an acceptable motion arc, minimal pain, and long-term remodeling.
Successful treatment of PIP fracture dislocations is dependent on adherence to basic treatment princi- ples. It is of paramount importance that treatment re-establish the normal flexion glide of the middle phalanx around the proximal phalanx head. Accom- plishing this goal requires obtaining joint reduction and re-establishing stability by reconstructing the middle phalanx cup-shaped geometry. Finally, early motion is more important than anatomic joint surface reduction in obtaining acceptable clinical outcome.
References
1. Akagi T, Hashizume H, Inoue H, Ogura T, Nagayarna N. Computer simulation analysis of fracture dislocation of the proximal interphalangeal joint using the finite element method. Acta Med Okayama 1994;48:263-270.
2. Stem P J, Roman R J, Kiefhaber TR, McDonough JJ. Pilon fractures of the proximal interphalangeal joint. J Hand Surg 1991;16A:844-850.
3. Hamer DW, Quinton DN. Dorsal fracture subluxation of the proximal interphalangeal joints treated by extension block splintage. J Hand Surg 1992;17B:586-590.
4. Inanami H, Ninomiya S, Okutsu I, Tarui T. Dynamic external finger fixator for fracture dislocation of the prox- imal interphalangeal joint. J Hand Surg 1993;18A: 160- 164.
5. Krakauer JD, Stern PJ. Hinged device for fractures involv- ing the proximal interphalangeal joint. Clin Orthop 1996; 327:29-37.
6. McElfresh EC, Dobyns JH, O'Brien ET. Management of fracture-dislocation of the proximal interphalangeal joints by extension-block splinting. J Bone Joint Surg 1972;54A: 1705-1711.
7. Dobyns JH, McElfresh EC. Extension block splinting. Hand Clin 1994; 10:229-237.
8. Viegas SF. Extension block pinning for proximal interpha- langeal joint fracture dislocations: preliminary report of a new technique. J Hand Surg 1992;17A:896-901.
9. Inoue G, Tamura Y. Treatment of fracture-dislocation of the proximal interphalangeal joint using extension-block Kirschner wire. Ann Chir Main Memb Super 1991;10: 564 -568.
10. Twyman RS, David HG. The doorstop procedure. A tech- nique for treating unstable fracture dislocations of the proximal interphalangeal joint. J Hand Surg 1993;18B: 714-715.

The Journal of Hand Surgery / Vol. 23A No. 3 May 1998 379
11. Fahmy NRM. The Stockport serpentine spring system for the treatment of displaced comminuted intraarticular pha- langeal fractures. J Hand Surg 1990;15B:303-311.
12. Fahmy NR, Harvey RA. The "S" quattro in the management of fractures in the hand. J Hand Surg 1992;17B:321-331.
13. Bostock SH, Nee PA, Fahmy NR. The S quattro: a new system for the management of difficult intra-articular fractures of the phalanges. Arch Emerg Med 1993;10: 55-59.
14. Agee JM. Unstable fracture dislocations of the proximal interphalangeal joint of the fingers: a preliminary report of a new treatment technique. J Hand Surg 1978;3:386-389.
15. Agee JM. Unstable fracture dislocations of the proximal interphalangeal joint. Treatment with the force couple splint. Clin Orthop 1987;214:101-112.
16. Morgan JP, Gordon DA, Klug MS, Perry PE, Barre PS. Dynamic digital traction for unstable comminuted intra- articular fracture-dislocations of the proximal interphalan- geal joint. J Hand Surg 1995;20A:565-573.
17. Robertson RC, Cawley JJ, Faris AM. Treatment of frac- ture-dislocation of the interphalangeal joints of the hand. J Bone Joint Surg 1946;28:68-70.
18. Weiss A-PC. Cerclage fixation for fracture dislocation of the proximal interphalangeal joint. Clin Orthop 1996;327: 21-28.
19. Hastings H II, Carroll C IV. Treatment of closed articular fractures of the metacarpophalangeal and proximal inter- phalangeal joints. Hand Clin 1988;4:503-527.
20. Freeland AE, Benoist LA. Open reduction and internal fixation method for fractures at the proximal interphalan- geal joint. Hand Clin 1994;10:239-250.
21. Green A, Smith J, Redding M, Akelman E. Acute open reduction and rigid internal fixation of proximal interpha- langeal joint fracture dislocation. J Hand Surg 1992;17A: 512-517.
22. Malerich MM, Eaton RG. The volar plate reconstruction for fracture-dislocation of the proximal interphalangeal joint. Hand Clin 1994;10:251-260.
23. Eaton RG, Malerich MM. Volar plate arthroplasty for the proximal interphalangeal joint: a ten year review. J Hand Surg 1980;5:260-268.
24. Durham-Smith G, McCarten GM. Volar plate arthroplasty for closed proximal interphalangeal joint injuries. J Hand Surg 1992;17B:422-428.
25. Bilos ZJ, Vender MI, Knutson K. Fracture subluxation of proximal interphalangeal joint treated by palmar plate ad- vancement. J Hand Surg 1994;19A:189-195.
26. Eaton RG. The dangerous chip fracture in athletes. Instr Course Lect 1985;34:314-322.
27. Bowers WH. Management of small joint injuries in the hand. Orthop Clin North Am 1983;14:793-810.
28. Steel WM. Articular fractures. In: Barton NJ, ed. Fractures of the hand and wrist. Edinburgh: Churchill Livingstone, 1988:55-73.
29. Stark HH. Troublesome fractures and dislocations of the hand. Instr Course Lect 1970; 19:130-149.
30. Bowers WH. Injuries and complications of injuries to the capsular structure of the interphalangeal joints. In: Bowers WH, ed. The interphalangeal joint. New York: Churchill Livingstone, 1987:56-76.
31. Stark RH. Treatment of difficult PIP joint fractures with a mini-external fixation device. Orthop Rev 1993;22:609-615.
32. Schenck RR. Dynamic traction and early passive move- ment for fractures for the proximal interphalangeal joint. J Hand Surg 1986;11A:850-858.
33. Knirk J, Jupiter J. Intra-articular fractures of the distal end of the radius in young adults. J Bone Joint Surg 1986;68A: 647-659.
34. Bradway J, Amadio PC, Cooney WP. Open reduction internal fixation of displaced, comminuted intra-articular fractures of the distal end of the radius. J Bone Joint Surg 1989;71A:839-847.
35. Salter RB. The physiologic basis of continous passive motion for articular cartilage healing and regeneration. Hand Clin 1994;10:211-220.
36. Donaldson WR, Millender LH. Chronic fracture-subluxa- tion of the proximal interphalangeal joint. J Hand Surg 1978;3:149-153.
37. Bowers WH, Wolf JW Jr, Nehil J, Bittinger S. The prox- imal interphalangeal joint volar plate. I. An anatomical and biomechanical study. J Hand Surg 1980;5:79-88.
38. Eaton RG. Joint injuries of the hand. Springfield, IL: Charles C. Thomas, 1971:9-34.
39. Eaton RG, Dray GJ. Dislocations and ligament injuries in digits. In: Green DP, ed. Operative hand surgery. 3rd ed. New York: Churchill Livingstone, 1982:637-668.
40. Wilson JN, Rowland SA. Fracture-dislocation of the prox- imal interphalangeal joint of the finger. Treatment by open reduction and intemal fixation. J Bone Joint Surg 1966; 48A:493-502.
41. Lubahn JD. Dorsal fracture dislocations of the proximal interphalangeal joint. Hand Clin 1988;4:15-24.
42. Patel MR, Joshi BB. Distraction method for chronic dorsal fracture dislocation of the proximal interphalangeal joint. Hand Clin 1994;10:327-337.
43. Isani A. Small joint injuries requiring surgical treatment. Orthop Clin North Am 1986;17:407-419.
44. Hastings H II, Ernst JM. Dynamic extemal fixation for fractures of the proximal interphalangeal joint. Hand Clin 1993;9:659-674.
45. Kahler DM, McCue FC. Metacarpophalangeal and proxi- mal interphalangeal joint injuries of the hand, including the thumb. Clin Sports Med 1992;11:57-76.
46. Zemel NP, Stark HH, Ashworth CR, Boyes JH. Chronic fracture dislocation of the proximal interphalangeal jo in t - - treatment by osteotomy and bone graft. J Hand Surg 1981; 6:447-455.
47. Schenck RR. Classification of fractures and dislocations of the proximal interphalangeal joint. Hand Clin 1994;10: 179-186.
48. Sent N, Hashizume H, Inque H, Imatani J, Morito Y. Fractures of the base of the middle phalanx of the finger. J Bone Joint Surg 1997;79B:758-763.
49. Spray P. Finger fracture dislocation proximal at the inter- phalangeal joint. J Tenn Med Assoc 1966;59:765-766.
50. Strong ML. A new method of extension block splinting for the proximal interphalangeal joint--preliminary report. J Hand Surg 1980;7A:77-78.
51. Kasparyn NG, Hotchkiss RN. Dynamic skeletal fixation in the upper extremity. Hand Clin 1997;13(4):643-664.

380 Kiefhaber and Stern / PIP Joint Fracture Dislocations
52. Jupiter JB, Sheppard JE. Tension wire fixation of avul- sion fractures in the hand. Clin Orthop 1987;214:113- 120.
53. Kiefhaber TR. Phalangeal dislocations/periarticular trauma. In: Peimer CA, ed. Surgery of the hand and upper extremity. New York: McGraw-Hill, 1996:939-972.
54. Phair IC, Quinton DN, Allen MJ. The conservative man- agement of volar avulsion fractures of the P.I.P. joint. J Hand Surg 1989;14B:168-170.
55. Wiley AM. Chronic dislocation of the proximal interpha- langeal joint: a method of surgical repair. Can J Surg 1965;8:435-439.
56. Wiley AM. Instability of the proximal interphalangealjoint following dislocation and fracture dislocation: surgical re- pair. Hand 1970;2:185-194.
57. Lane CS. Reconstruction of the unstable interphalangeal joint: the double superficialis tenodesis. J Hand Surg 1978; 3:368-369.
58. Adams JP. Correction of chronic dorsal subluxation of the proximal interphalangeal joint by means of a criss-cross volar graft. J Bone Joint Surg 1959;41A: 111-115.
59. Spinner M, Choi BY. Anterior dislocation of the proximal interphalangeal joint. J Bone Joint Surg 1970;52A: 1329- 1336.
60. Kiefhaber TR, Stem PJ, Grood ES. Lateral stability of the proximal interphalangeal joint. J Hand Surg 1986;11A: 661-669.
61. Peimer CA, Sullivan DJ, Wild DR. Palmar dislocation of the proximal interphalangeal joint. J Hand Surg 1984;9A: 39-48.
Related Documents