CLINICAL LECTURE (MBBS 2017 BATCH) Dr. Lubna Zafar Assistant Professor Department of Medicine, JNMCH 24/6/2020 9 (Wednesday)

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

CLINICAL LECTURE
(MBBS 2017 BATCH)
Dr. Lubna Zafar
Assistant Professor
Department of Medicine, JNMCH
24/6/2020 9 (Wednesday)

CASE SCENARIO
A 52-years-old male with 8-years history of recurrent arthritis was admitted for generalized articular pain. He had only taken traditional medicines for joint pains .
He complained of multiple hard swelling over his joints which had developed over 4 years, progressively increasing in size.
Ten hours before seeking medical assistance, a nodule located on the first metatarsophalangeal joint of his left foot had bursted releasing a viscous, chalk-like material.

Past History : Hypertensive for 4 years. On
Amlodipine 10 mg.
Personal History : Non-vegetarian
Alcohol Intake
o Family History : Nothing significant

Examination:
Pallor present (mild)
Icterus absent
Clubbing absent
No LAP
PR : 98/min, regular, no special character
BP: 158/94 mmHg Supine
RR: 18 /min
Temp: 100.2 F
BMI 30.4 kg/m2
Physical examination revealed that there were
multiple large firm tophi over bilateral hands,
feet, elbows, and knees .
A large tophus over MCP right second finger.
Some of them are ulcerated and discharged
white chalky material.


INVESTIGATIONS :
Hb 10 gm%
TLC 13600 cells/mm3
DLC P70L27M3
B.S. 142
Serum creatinine 2.8 mg/dl
Serum electrolytes normal
Serum uric acid 9.8 mg/dl
Thyroid profile normal
RA negative

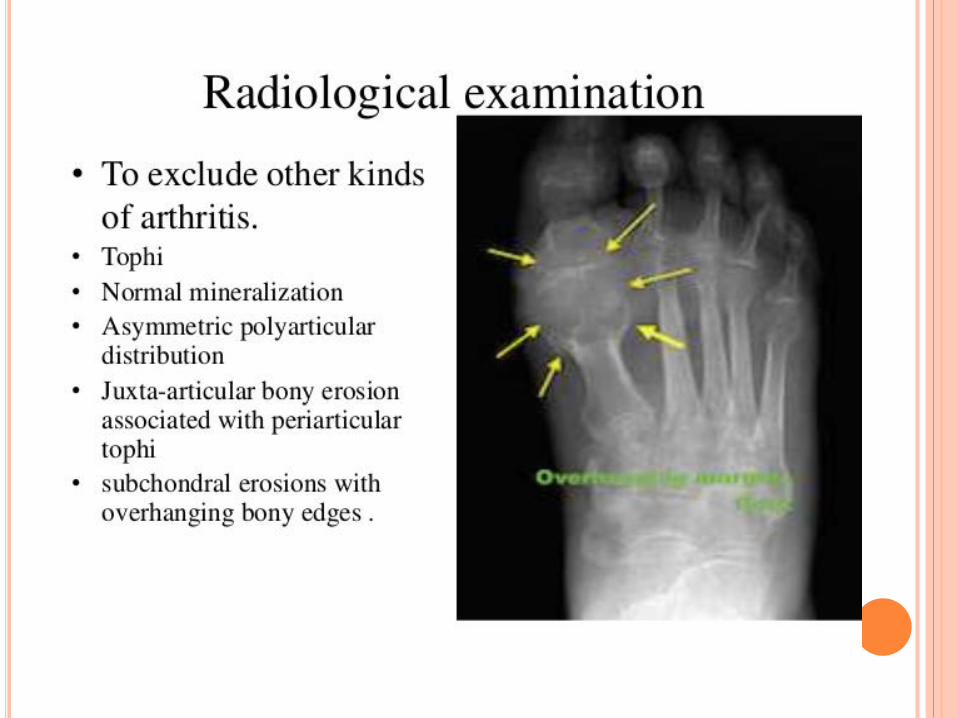
Radiological examination of the feet showed
soft tissue swelling and total destruction of the
first left metatarsophalangeal joint
Abdominal ultrasonography revealed
bilateral caliceal calculi.


DIAGNOSIS
Systemic Hypertension. Chronic tophaceous gout.
Nephrolitiasis. Sepsis. Renal Insufficiency

GOUT
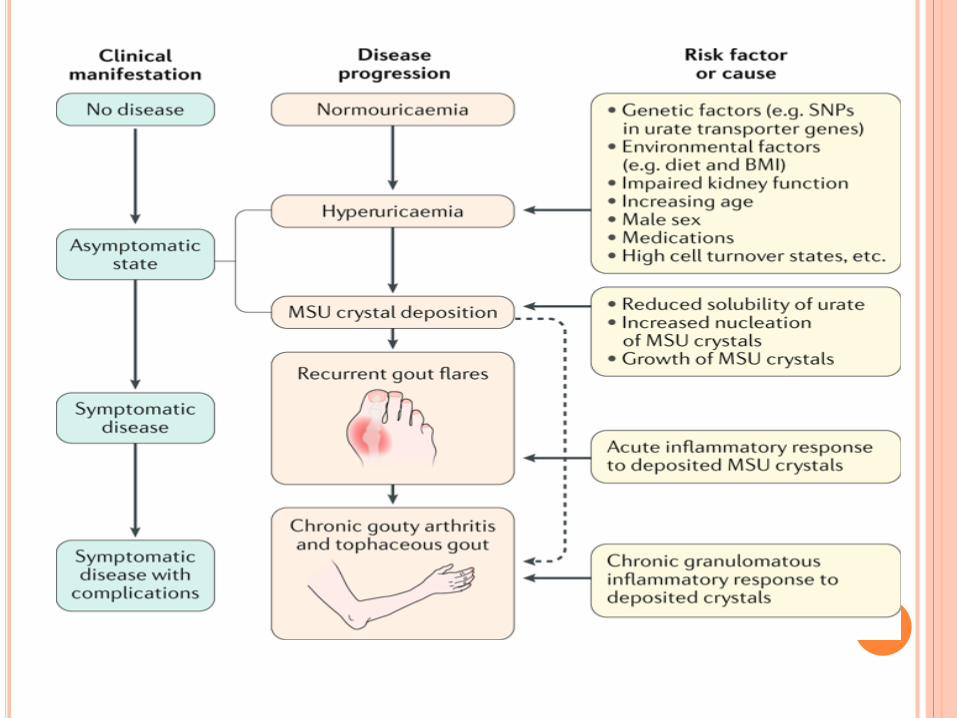
GOUT
Inflammatory response to MSU crystals formed
secondary to hyperuricaemia
Hyperuricaemia defined as plasma urate
concentration greater than 7 mg/dl in males and
6mg/dl in females.
In females, uric acid rises after menopause.
HISTORY
Was known as Disease of the ‘KINGS’ (Rich
foods have a higher concentration of protein. This
was believed to be causative of gout)
Famous personalities affected with the disease:
Benjamin Franklin
Thomas Jefferson
Sir Isaac Newton
Charles Darwin
King Henry VIII

PREDISPOSING FACTORS
Purine rich foods – meat, kidney, liver, seafood,
oatmeal, peas, beans,lentils, mushrooms
Drugs – Loop diuretics, NSAIDs, corticosteroids,
Niacin, Cyclosporine, Salicylates, Pyrazinamide
Trauma
Infection
Other disease – DM, HTN, vascular dx, renal dx,
thyroid dx, sarcoidosis, etc.



HYPERURICEMIA LEADS TO DEPOSIT OF
URATES IN THE JOINT FLUID, TRIGGERING AN
INFLAMMATORY CASCADE

STAGES OF GOUT
Asymptomatic hyperuricemia
Acute gout
Intercritical gout
Chronic tophaceous gout
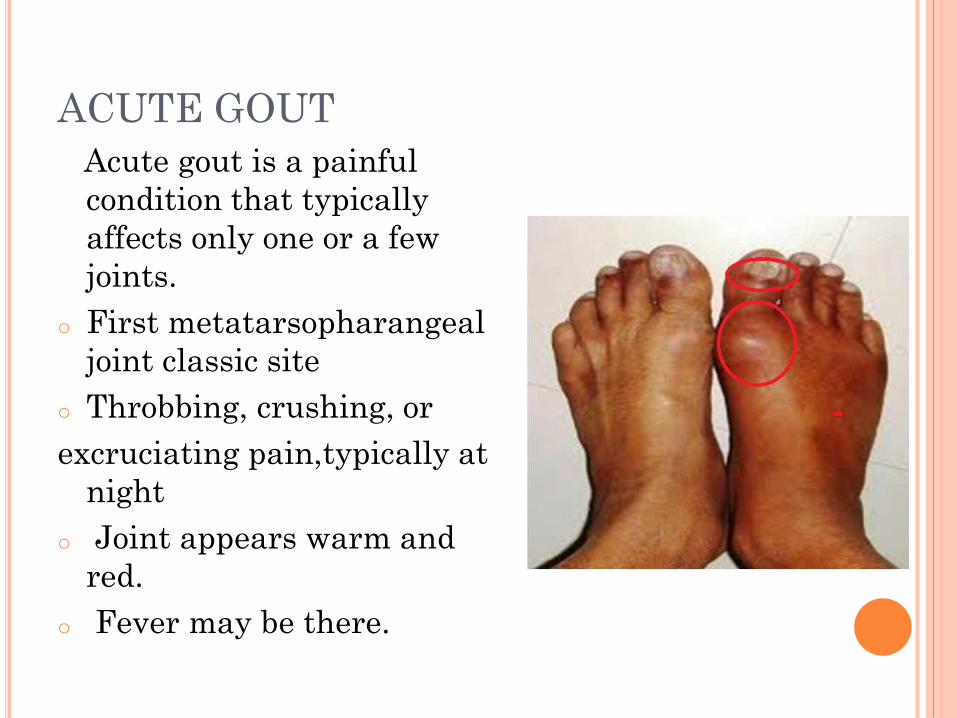
ACUTE GOUT
Acute gout is a painful
condition that typically
affects only one or a few
joints.
o First metatarsopharangeal
joint classic site
o Throbbing, crushing, or
excruciating pain,typically at
night
o Joint appears warm and
red.
o Fever may be there.


The attack may resolve in a few days, but
relapses
Additional attacks often last longer.
CHRONIC GOUT
Joint damage
Loss of motion in the joints
Joint pain and other symptoms most of the time,
throughout the day
Is characterised by massive deposits of monosodium
urate crystals in articular cartilage, subchrondral
bone, synovial membrane, capsule, tendon sheaths
and peri articular tissues.
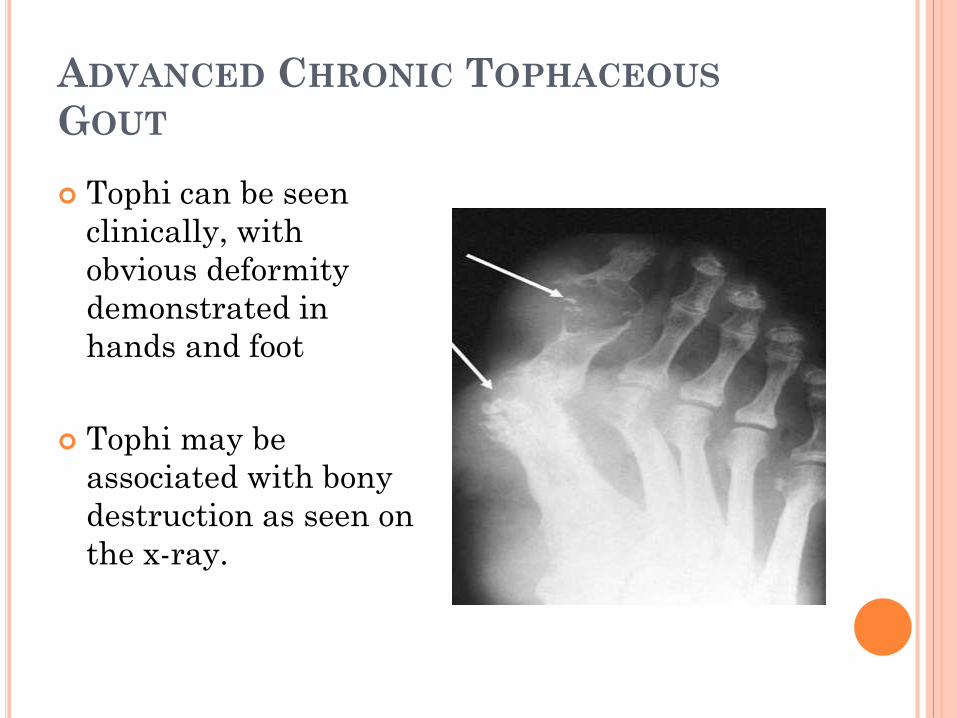
ADVANCED CHRONIC TOPHACEOUS
GOUT
Tophi can be seen
clinically, with
obvious deformity
demonstrated in
hands and foot
Tophi may be
associated with bony
destruction as seen on
the x-ray.
TOPHI
The tophaceous nodules consists of multicentric
deposition of urate crystals and intra cellular
matrix and foreign body granulomatous reaction.
As they enlarge in size, calcify, they can cause
pressure symptoms.
The tophi are firm yellow in colour and
occasionally discharge a chalky material.

RENAL INVOLVEMENT IN GOUT
Most common complication of hyperuricaemia
after gouty arthritis
Urate nephropathy: Deposition of MSU in renal
interstitial tissue
Uric acid calculi
Renal failure accounts for 10-25% deaths in gout
patients

INVESTIGATIONS
Plain radiographs
Serum Uric acid: ≥ 2 raised fasting levels ( may
be normal during acute attack)
Synovial fluid analysis
BUN ,Serum Creatinine
Synovial biopsy
24 hour Urinary urate

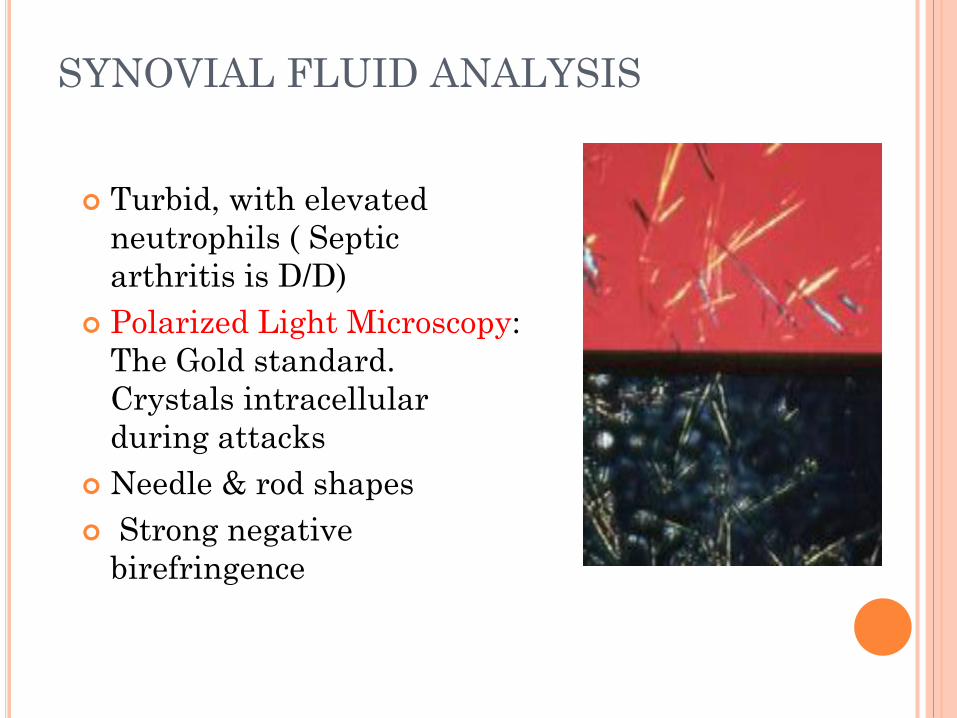
SYNOVIAL FLUID ANALYSIS
Turbid, with elevated
neutrophils ( Septic
arthritis is D/D)
Polarized Light Microscopy:
The Gold standard.
Crystals intracellular
during attacks
Needle & rod shapes
Strong negative
birefringence

DIFFERENTIAL DIAGNOSIS
Pseudogout: Chondrocalcinosis, CPPD
Psoriatic Arthritis
Osteoarthritis
Rheumatoid arthritis
Septic arthritis
Cellulitis


MANAGEMENT
ASYMPTOMATIC HYPERURICAEMIA
No drug therapy
Treatment indicated in tumor lysis syndrome,
uric acid levels more than 10mg/dl, presence of
risk factors or comorbidities

ACUTE GOUT
Treatment as soon as possible
NSAID , Colchicine, Steroids
Xanthine oxidase inhibitor 10-15 days after
resolution of inflammation


NSAID:
Inhibits pain & inflammation.
Inhibits urate crystal phagocytosis by decreasing
the migration of granulocytes into the inflammatory
area.
Indomethacin, Naproxen, Ketorolac.

COLCHICINE:
Produces its anti-inflammatory effects by binding
to the intracellular protein tubulin, preventing
its polymerization leading to the inhibition of
leukocyte migration into affected area.
Inhibits the synthesis & release of leukotrienes.
URICOSURIC AGENTS:
Probenecid & Sulfinpyrazone
They are weak organic acids .
Sulfinpyrazone is a metabolite of phenylbutazone.
Increase the excretion of Uric acid.
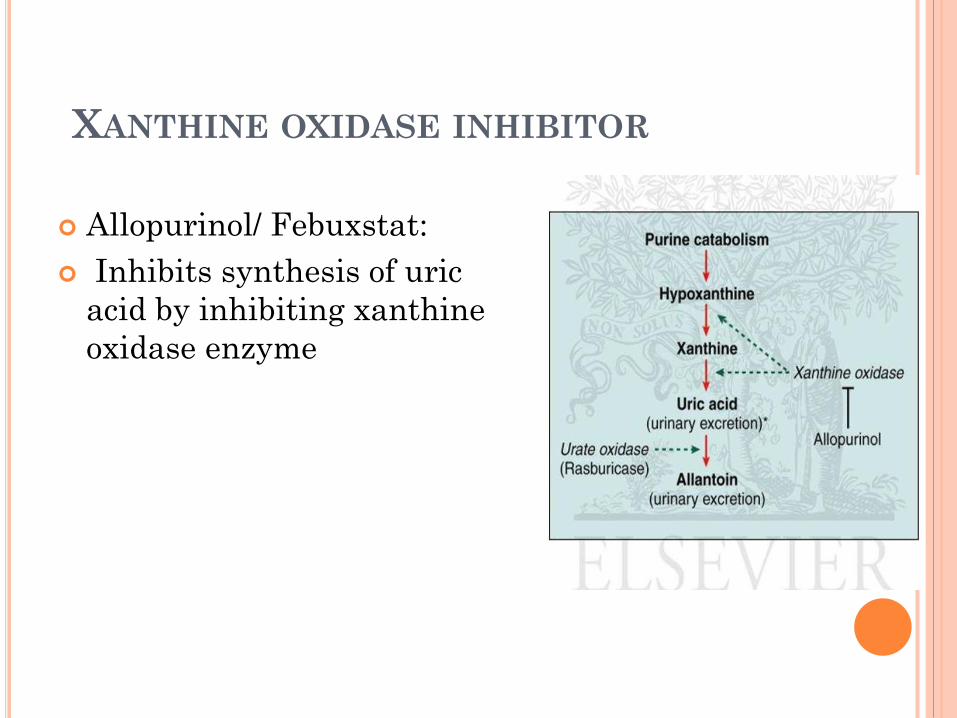
XANTHINE OXIDASE INHIBITOR
Allopurinol/ Febuxstat:
Inhibits synthesis of uric
acid by inhibiting xanthine
oxidase enzyme

URICASE ENZYMES
Catabolize urate to allantoin
More soluble, excretable form
Currently approved for hyperuricemia in tumor
lysis syndrome


Related Documents











