Clinical experience with preimplantation genetic diagnosis and intracytoplasmic sperm injection I.Liebaers 1 ' 3 , K.Sermon 1 , C.Staessen 2 , HJoris 2 , W.Lissens 1 , E.Van Assche 1 , P.Nagy 2 , M.Bonduelle 1 , M.Vandervorst 2 , P.Devroey 2 and A.Van Steirteghem 2 'Centre for Medical Genetics and 2 Centre for Reproductive Medicine, Dutch-speaking Brussels Free University, Laarbeeklaan 101, 1090 Brussels, Belgium 3 To whom correspondence should be addressed Preimplantation genetic diagnosis (PGD) is a novel procedure whose use may be considered to obtain a very early prenatal diagnosis for couples at risk for transmitting genetic diseases. Using the polymerase chain reaction (PCR) or fluorescence in-situ hybridization (FISH) the genotype or the sex of biopsied cleavage-stage embryos obtained after in-vitro fertilization can be determined and selected embryos can then be transferred. In-vitro fertilization with intra- cytoplasmic sperm injection is the method of choice to obtain embryos to be analysed through PCR to reduce contamination by residual sperm DNA. In our series of 61 PGD cycles for 29 couples at risk over a period of 4 years the ongoing pregnancy rate per cycle was 15%, per transfer 19% and per patient 31%. One of the six morphologically normal children born, who is still alive and doing well, weighed 850 g after birth at 25 weeks following a complicated triplet pregnancy. More experience is needed to cor- rectly evaluate the efficiency and safety of this novel technique as well as to determine its place in the prevention of genetic disease. Key words: intracytoplasmic sperm injection/mon- ogenic diseases/preimplantation genetic diagnosis Introduction Preimplantation genetic diagnosis (PGD) is a novel technique which permits determination of the geno- type of an oocyte before fertilization or of an embryo before implantation. On the one hand, this procedure became possible because of the almost simultaneous development of in-vitro fertilization (IVF), micromanipulation, polymerase chain reac- tion (PCR) and fluorescence in-situ hybridization (FISH). On the other hand, patients or couples with a recurrence risk for genetic diseases were requesting such a procedure so as to avoid the need for pregnancy termination after conventional prenatal diagnosis. The first clinical PGD was reported by Handy side et al. (1990). Preclinical studies had convinced them that there was appar- ently no harm in biopsying a cleavage-stage embryo at the 6-8-cell stage (Hardy et al., 1990). Since then several groups have performed PGD successfully using either PCR or FISH to analyse blastomeres from 3 day old embryos (Harper, 1996; Lissens et al., 1996) or to analyse polar bodies from oocytes before fertilization (Verlinsky et al, 1996). Intracytoplasmic sperm injection (ICSI) cer- tainly has its use in PGD. In the first place it has an advantage over conventional in-vitro-fertilization (IVF) in that it avoids contamination by spermato- zoa during PGD of a cleavage-stage embryo, using the PCR. Moreover, for some couples with a concurrent genetic risk such as cystic fibrosis (CF) in cases of congenital bilateral absence of the vas deferens (CBAVD), pregnancy will be obtained more often after ICSI with spermatozoa retrieved from the epididymis than after regular IVF (Silber et al., 1994). Klinefelter patients who on rare occasions may produce a very low number of 186 © European Society for Human Reproduction & Embryology Human Reproduction Volume 13 Supplement 1 1998 Downloaded from https://academic.oup.com/humrep/article/13/suppl_1/186/788956 by guest on 08 July 2022

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Clinical experience with preimplantation geneticdiagnosis and intracytoplasmic sperm injection
I.Liebaers1'3, K.Sermon1, C.Staessen2, HJoris2, W.Lissens1, E.Van Assche1,P.Nagy2, M.Bonduelle1, M.Vandervorst2, P.Devroey2
and A.Van Steirteghem2
'Centre for Medical Genetics and 2Centre for Reproductive Medicine, Dutch-speaking Brussels FreeUniversity, Laarbeeklaan 101, 1090 Brussels, Belgium
3To whom correspondence should be addressed
Preimplantation genetic diagnosis (PGD) is anovel procedure whose use may be consideredto obtain a very early prenatal diagnosis forcouples at risk for transmitting genetic diseases.Using the polymerase chain reaction (PCR) orfluorescence in-situ hybridization (FISH) thegenotype or the sex of biopsied cleavage-stageembryos obtained after in-vitro fertilization canbe determined and selected embryos can thenbe transferred. In-vitro fertilization with intra-cytoplasmic sperm injection is the method ofchoice to obtain embryos to be analysed throughPCR to reduce contamination by residual spermDNA. In our series of 61 PGD cycles for 29couples at risk over a period of 4 years theongoing pregnancy rate per cycle was 15%, pertransfer 19% and per patient 31%. One of thesix morphologically normal children born, whois still alive and doing well, weighed 850 g afterbirth at 25 weeks following a complicated tripletpregnancy. More experience is needed to cor-rectly evaluate the efficiency and safety of thisnovel technique as well as to determine its placein the prevention of genetic disease.Key words: intracytoplasmic sperm injection/mon-ogenic diseases/preimplantation genetic diagnosis
Introduction
Preimplantation genetic diagnosis (PGD) is a noveltechnique which permits determination of the geno-type of an oocyte before fertilization or of an
embryo before implantation. On the one hand, thisprocedure became possible because of the almostsimultaneous development of in-vitro fertilization(IVF), micromanipulation, polymerase chain reac-tion (PCR) and fluorescence in-situ hybridization(FISH). On the other hand, patients or coupleswith a recurrence risk for genetic diseases wererequesting such a procedure so as to avoid theneed for pregnancy termination after conventionalprenatal diagnosis. The first clinical PGD wasreported by Handy side et al. (1990). Preclinicalstudies had convinced them that there was appar-ently no harm in biopsying a cleavage-stageembryo at the 6-8-cell stage (Hardy et al., 1990).Since then several groups have performed PGDsuccessfully using either PCR or FISH to analyseblastomeres from 3 day old embryos (Harper, 1996;Lissens et al., 1996) or to analyse polar bodiesfrom oocytes before fertilization (Verlinsky etal, 1996).
Intracytoplasmic sperm injection (ICSI) cer-tainly has its use in PGD. In the first place it has anadvantage over conventional in-vitro-fertilization(IVF) in that it avoids contamination by spermato-zoa during PGD of a cleavage-stage embryo, usingthe PCR. Moreover, for some couples with aconcurrent genetic risk such as cystic fibrosis (CF)in cases of congenital bilateral absence of the vasdeferens (CBAVD), pregnancy will be obtainedmore often after ICSI with spermatozoa retrievedfrom the epididymis than after regular IVF (Silberet al., 1994). Klinefelter patients who on rareoccasions may produce a very low number of
186 © European Society for Human Reproduction & Embryology Human Reproduction Volume 13 Supplement 1 1998
Dow
nloaded from https://academ
ic.oup.com/hum
rep/article/13/suppl_1/186/788956 by guest on 08 July 2022
Clinical experience with PGD and ICSI
spermatozoa may try to father a child through IVFand ICSI with spermatozoa extracted from anejaculate or more often from a testicular biopsyand in this experimental setting the number of sexchromosomes in the embryos must be evaluatedbefore transfer. The outcome of these treatmentcycles in Klinefelter patients has partially beenpublished and will be updated separately (Staessenet al, 1996; Tournaye et al, 1996). In this articleour clinical PGD experience in cases with a recur-rence risk for monogenic diseases will be reportedand the place of ICSI will briefly be discussed.
Materials and methods
Twenty-nine couples were counselled at the Centrefor Medical Genetics between February 1993 andFebruary 1997 prior to PGD. Except for threecouples who had a reduced risk (see Appendix)they had a 25 or 50% chance of having childrenwith a monogenic disease. The genetic diseases atrisk of transmission were: CF (with or withoutCBAVD in the male) (n = 8), non-fragile X mentalretardation (n — 3), haemophilia A (n = 2),Duchenne's muscular dystrophy (DMD) (n = 4),retinitis pigmentosa (n = 1) and myotonic dys-trophy (n = 11). The reason why these coupleschose PGD rather than regular prenatal diagnosiswere in general: (i) infertility or subfertility neces-sitating IVF in addition to the genetic risk {n =15), (ii) one or several pregnancy terminations afterchorionic villus sampling (CVS) or amniocentesis(AC) (n = 8), (iii) moral, emotional or religiousobjections against abortion in itself (n = 6) or incombination with another indication (n = 4).Table I summarizes the indications and the outcomeof PGD in Brussels over a period of 4 years.Couples were prepared for IVF (four cycles) orfor IVF with ICSI (57 cycles) according to standardprotocols (Staessen et al, 1993; Van Steirteghemet al, 1993, 1995). A brief history of each coupleis given in the Appendix.
Blastomere biopsy
Embryos were biopsied in the morning of day 3after insemination or microinjection. From the 7-cell stage on, two blastomeres per embryo were
removed, while only one blastomere was takenfrom 4-6-cell embryos. A micropipette was usedwith an inner diameter of 40^15 Jim and theembryos were immobilized by means of a holdingpipette. These biopsies were performed in HEPES-buffered Earle's medium. First, a hole was madein the zona pellucida. This was done by blowinga stream of acidic Tyrode's solution until the zonapellucida ruptured. Two different procedures toobtain blastomeres have been used. In the earliercycles, the hole in the zona was rotated to the 12o'clock position. One or two blastomeres werepushed through the hole using a bevelled pipettewith an inner diameter of 40 |J,m. In later cycles,a blunt pipette with an inner diameter of 40-45|im and a smoothened opening was passed throughthe hole, which was positioned at the equatorialplane of a blastomere containing a nucleus beforeaspiration (Ao et al, 1996).
Diagnosis by the PCR method
Under continuous microscopical observation,blastomeres were washed three times in Ca2+- andMg2+-free M2 medium and placed in a 0.5 or0.2 ml PCR tube. Lysis conditions and reactionconditions were established to detect the concernedmutations or DNA sequences in the most efficientand accurate way at the single-cell level. Theresulting DNA fragments were further analysed ona polyacrylamide or Metaphor® agarose gel (Liuet al, 1994a,b, 1995; Sermon et al, 1997).
Diagnosis by the FISH method
The individual blastomeres were first rinsed inmedium, then transferred to a 1-2 ]Lil droplet of0.01 N HCl/0.1% Tween-20 solution on a slideand the FISH procedure as described by Coonenet al (1994) was performed. Double target FISHwas carried out using directly labelled DNA probesspecific for chromosomes X (Vysis, a-satelliteDNA probe, Spectrum Green) and Y (Vysis, satel-lite III DNA probe, Spectrum Orange). The nucleiwere counterstained with DAPI. The nuclei werethen examined using a Zeiss Axioskop fluorescencemicroscope with the appropriate filter set (filter 10for fluorescein isothiocyanate (FITC), filter 02(DAPI) and Omega filter (FITC/Texas Red) (Westet al, 1989; Griffin et al, 1991; Harper et al,
187
Dow
nloaded from https://academ
ic.oup.com/hum
rep/article/13/suppl_1/186/788956 by guest on 08 July 2022
I.Liebaers et al.
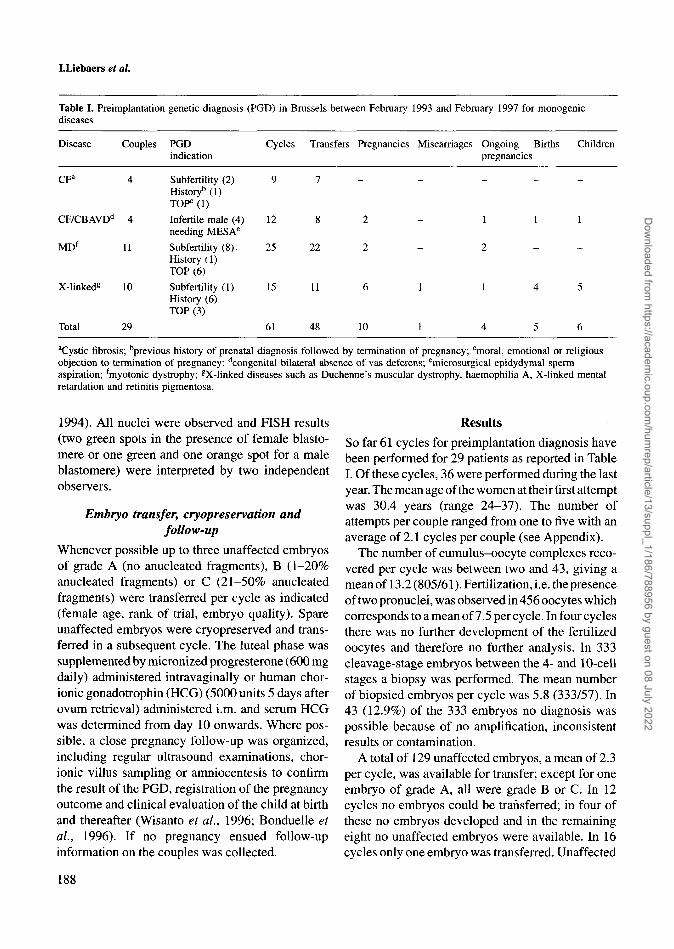
Table I. Preimplantation genetic diagnosis (PGD) in Brussels between February 1993 and February 1997 for monogenicdiseases
Disease Couples PGDindication
Cycles Transfers Pregnancies Miscarriages Ongoing Birthspregnancies
Children
CFa 4
CF/CBAVDd 4
MDf 11
X-linked« 10
Subfertility (2)History5 (1)TOP0 (1)
Infertile male (4)needing MESAe
Subfertility (8).History (1)TOP (6)
Subfertility (1)History (6)TOP (3)
Total 29
12
25
15
61
22
11
48 10
aCystic fibrosis; bprevious history of prenatal diagnosis followed by termination of pregnancy; cmoral, emotional or religiousobjection to termination of pregnancy; dcongenital bilateral absence of vas deferens; emicrosurgical epidydymal spermaspiration; fmyotonic dystrophy; gX-linked diseases such as Duchenne's muscular dystrophy, haemophilia A, X-linked mentalretardation and retinitis pigmentosa.
1994). All nuclei were observed and FISH results(two green spots in the presence of female blasto-mere or one green and one orange spot for a maleblastomere) were interpreted by two independentobservers.
Embryo transfer, cryopreservation andfollow-up
Whenever possible up to three unaffected embryosof grade A (no anucleated fragments), B (1-20%anucleated fragments) or C (21-50% anucleatedfragments) were transferred per cycle as indicated(female age, rank of trial, embryo quality). Spareunaffected embryos were cryopreserved and trans-ferred in a subsequent cycle. The luteal phase wassupplemented by micronized progresterone (600 mgdaily) administered intravaginally or human chor-ionic gonadotrophin (HCG) (5000 units 5 days afterovum retrieval) administered i.m. and serum HCGwas determined from day 10 onwards. Where pos-sible, a close pregnancy follow-up was organized,including regular ultrasound examinations, chor-ionic villus sampling or amniocentesis to confirmthe result of the PGD, registration of the pregnancyoutcome and clinical evaluation of the child at birthand thereafter (Wisanto et al., 1996; Bonduelle etal., 1996). If no pregnancy ensued follow-upinformation on the couples was collected.
Results
So far 61 cycles for preimplantation diagnosis havebeen performed for 29 patients as reported in TableI. Of these cycles, 36 were performed during the lastyear. The mean age of the women at their first attemptwas 30.4 years (range 24-37). The number ofattempts per couple ranged from one to five with anaverage of 2.1 cycles per couple (see Appendix).
The number of cumulus-oocyte complexes reco-vered per cycle was between two and 43, giving amean of 13.2 (805/61). Fertilization, i.e. the presenceof two pronuclei, was observed in 456 oocytes whichcorresponds to a mean of 7.5 per cycle. In four cyclesthere was no further development of the fertilizedoocytes and therefore no further analysis. In 333cleavage-stage embryos between the 4- and 10-cellstages a biopsy was performed. The mean numberof biopsied embryos per cycle was 5.8 (333/57). In43 (12.9%) of the 333 embryos no diagnosis waspossible because of no amplification, inconsistentresults or contamination.
A total of 129 unaffected embryos, a mean of 2.3per cycle, was available for transfer; except for oneembryo of grade A, all were grade B or C. In 12cycles no embryos could be transferred; in four ofthese no embryos developed and in the remainingeight no unaffected embryos were available. In 16cycles only one embryo was transferred. Unaffected
188
Dow
nloaded from https://academ
ic.oup.com/hum
rep/article/13/suppl_1/186/788956 by guest on 08 July 2022

Clinical experience with PGD and ICSI
embryos were cryopreserved in five cycles and mostof these were transferred in three additional cyclesbut without success.
So far 10 pregnancies have ensued from freshtransfers. One miscarriage has occurred, four single-ton pregnancies are ongoing and six children havebeen born from the remaining five pregnancies. Thechildren are aged between 3 months and >2 yearsof age. One of them is a boy, the others are girls.
Discussion
The success rate in terms of pregnancies is 10 outof 61 cycles or 16%. Per transfer the pregnancy rateis 10/48 (21%) and per couple it is 10/29 (34%).Numbers are too small to calculate the take-homebaby rate but if we subtract the one miscarriage andconsider the ongoing pregnancies (n = 4) plus thedeliveries (n = 5), the take-home baby rates are 15%per cycle, 19% per transfer and 31% per couple. Inour regular IVF or IVF/ICSI cycles the pregnancyrate per cycle is currently ~30% and the take-homebaby rate per cycle well over 20%. In the worldfigures for PGD the pregnancy rate was reported as25% per cycle and 29% per transfer (Harper, 1996).The lower success rate in this small series cannot beexplained by the age of our patients which is quitesimilar. One of the reasons for a lower pregnancyrate is most probably the higher number of cycles inwhich none or only one unaffected embryo of gradeB or C was available for transfer. From our availabledata we therefore decided that cycles for PGD withfewer than nine cumulus-oocyte complexes shouldbe cancelled. Another reason for a lower success ratemay be a 'subfertility' of the myotonic dystrophypatients due to their disease, since 25 out of the 61cycles were performed in 11 couples at risk for thisdisease (Sermon et al., 1997).
None of the four couples at risk of CF has becomepregnant so far. Two of these had a subfertility prob-lem as well as the genetic risk; nevertheless one ofthem has since had two spontaneous pregnanciesfollowed by the birth of non-affected children afterchorionic villus sampling. Prior to the pregnanciesthe couple was intending to have another PGD cycle.One couple has had four cycles so far without suc-cess. After CF had been diagnosed in one of theirtwo children 8 years ago, this couple waited for thedevelopment of PGD so as to be able to have at least
one other healthy child, especially since the wifecould not cope with the idea of prenatal diagnosisfollowed by a possible pregnancy termination.Although this couple was proven to be fertile, theoocytes and embryos produced during the four treat-ment cycles were always low in number and ofextremely poor quality.
Pregnancies have ensued in two of the fourcouples who were at risk for CF because the wivesof CB AVD men were carriers. In one case the preg-nancy occurred during the first treatment cycle afterreplacement of three embryos and a healthy boy nowover 2 years of age was born (Liu et al., 1994a).Subsequent cycles were unsuccessful. For thesecond couple, five cycles were needed to obtain asingleton pregnancy after transfer of three embryos.
In six out of 10 patients at risk for an X-linkeddisease, pregnancies have ensued. The mean age ofthese patients was 28 years. Four of the 10 patientswere at risk of DMD. Two of them now have girls.In the first case the pregnancy occurred during thesecond cycle and the diagnosis was based on a PCRassay detecting the presence or absence of a dystro-phin gene deletion. Two embryos were transferred(Liu et al., 1995). The girl is now over 2 years of ageand healthy. In the second case a triplet pregnancyoccurred during the second cycle after transfer ofthree embryos. The triplet was one singleton andone twin (monochorionic, biamniotic) one of whichwas shown to be an acardiacus between 13 and14 weeks of pregnancy. Five weeks later selectivereduction of the malformed twin was performedextramuros, and 4 weeks later the children wereprematurely born at almost 25 weeks of pregnancy.The morphologically normal twin weighed 450 gand subsequently died. The singleton baby girlweighed 850 g and is doing well according to theinformation we obtained so far. In two patients atrisk for haemophilia A, one healthy girl was bornafter transfer of two embryos and two healthy twingirls have recently been born after the replacementof three embryos in the second patient. Of the threepatients at risk of non-fragile-X-linked mentalretardation, one patient became pregnant afterreplacement of three embryos in the first cycle buta miscarriage occurred. Finally, one patient at riskof retinitis pigmentosa is currently pregnant afterone treatment cycle with transfer of two embryos.
189
Dow
nloaded from https://academ
ic.oup.com/hum
rep/article/13/suppl_1/186/788956 by guest on 08 July 2022
I.Liebaers et al.
Two out of 11 couples at risk for myotonic dys-trophy are currently pregnant with singletons, bothafter a third cycle in which respectively two and fourembryos were transferred (Sermon etai, 1997).
The mean age of all the preceding pregnantwomen was 29.8 years (range 24-37); the meannumber of embryos transferred per cycle was 2.5(range 2-3 except in one case where four were trans-ferred).
In our population of 29 couples who had requestedPGD, the indications, apart from the genetic risk,were infertility in the four cases with CBAVD,subfertility in 11 cases (most of which belong to themyotonic dystrophy group), a previous history ofaffected pregnancies which had to be terminated ineight cases and moral problems with termination ofpregnancy in six cases. The high pregnancy rate of60% in the group of patients at risk of sex-linkeddiseases might be explained by the lack of subfertil-ity problems (only one out of 10) and the youngermean age (28 years) of these patients. The one mis-carriage occurred in the subfertile couple with aprevious history of G4P1 A3.
Only the first four cycles in couples withoutCBAVD involved classical IVF. Since then, IVFwith ICSI has been used for insemination. The aimwas to reduce the risk for contamination in PCRreactions from residual sperm DNA. We still con-sider this to be the insemination method of choicein PCR-based PGD. In FISH-based PGD forcouples with no known subfertility or infertility,conventional IVF is probably equally valid asan option.
Before starting the treatment, PGD patients wereasked to agree to a prenatal diagnosis through CVSor amniocentesis to confirm the result of the PGDshould they become pregnant, since at least in PCR-based assays misdiagnoses have been reported(Harper, 1996) and since diagnostic errors mayoccur as a result of contamination or allele-specificdrop-out during the PCR reaction. Of the 10pregnancies, one miscarried before prenatal dia-gnosis. Two patients pregnant after a FISH-basedsex determination and one patient pregnant afterCF diagnosis declined to have prenatal diagnosis.In six cases (one CVS and five amniocenteses) thePGD was confirmed or refined (CF carrier boy,non-carrier DMD girl).
The age of the six children born so far rangesfrom 3 months to over 2 years of age. Four of theseare girls because female embryos were selected fortransfer as a result of a risk of a sex-linked disease.The fifth girl was born to a carrier of DMDbut the PCR-based PGD indicated affected male(absence of fragment) versus unaffected maleembryos and non-carrier as well as carrier femaleembryos (presence of fragment). This girl and theboy born at term in 1994 were morphologicallynormal (Liu et al., 1994a, 1995). At birth and at2 years of age their growth and developmentalmilestones were within the normal range. One ofthe four girls born in 1996 issued from the tripletpregnancy mentioned earlier; she was born at 25weeks of pregnancy and weighed 850 g. At 4months of age the girl weighed 3.2 kg and measured49 cm. According to the parents, who plan to visitus, she was progressing well. The premature birthwas probably the result of the selective reductionperformed on one of the malformed twins at 18-19 weeks of pregnancy. The other twin weighedonly 450 g at birth and did not survive. The causeof the acardiacus malformation is most probablylinked to the twinning process and not to thebiopsy procedure. The other three girls born in1996 are doing well according to informationobtained from the parents and their physicians.One girl was born at 36 weeks of pregnancy andhad a birthweight of 2.4 kg, a length of 47 cm anda head circumference of 32 cm. She is now about1 year old. The other twin girls were born at 35weeks of gestation and weighed 2.6 and 2.1 kgrespectively; they are now 3 months old. So far,the number of children born is too small to drawany firm conclusions concerning possible problemswith morphology, growth or development. As inregular IVF and ICSI, multiple pregnancies shouldbe avoided where possible so as to reduce the riskof complications (Bonduelle et al., 1996; Wisantoet al., 1996; Simpson and Liebaers, 1996).
Our PGD programme is now well structuredand based on a close collaboration between theCentre for Medical Genetics and the Centre forReproductive Medicine. Before starting, patientsare counselled extensively by specialized physi-cians in both Centres. A nurse-coordinator sched-ules the cycles and informs the team members who
190
Dow
nloaded from https://academ
ic.oup.com/hum
rep/article/13/suppl_1/186/788956 by guest on 08 July 2022
Clinical experience with PGD and ICSI
will be involved and especially the laboratoriesdealing with cycle monitoring, IVF and ICSI,embryo biopsy and FISH or PCR analysis. Patientsare asked to come to the clinic for pick-up and onday 3 post-insemination for a possible transfer.The outcome of the embryo diagnosis is discussedwith the couple at the clinic. In any case a follow-up visit is scheduled with the geneticist as well aswith the fertility specialist so as either to organizea pregnancy follow-up with prenatal diagnosis,ultrasound and finally a baby follow-up or to plana subsequent cycle. Organizing the follow-up ofpatients from abroad is more complex and the dataobtained are less complete.
Possible reasons for the slow development ofPGD in our centres and elsewhere are probablylinked to its experimental character and to thecomplexity of the procedure at the clinical as wellas at the laboratory level. Moreover the take-homebaby rate is low as a result of this complexity andthe cost is rather high. Finally, the availability ofthe procedure in general and of specific proceduresfor specific diseases is still limited. Nevertheless,the procedure does not appear to be too stressfulfor many of the patients, since several of themhave had repeated PGD (see Appendix). Furtherdevelopment in diagnostic procedures as well asthe evaluation of patients' experiences are thereforeto be expected. Moreover, continuous data collec-tion at the national and international levels will beof great value to correctly appreciate the valueof this new procedure (ESHRE Special InterestGroup on Reproduction and Genetics/InternationalWorking Group on PGD, 1997).
Acknowledgements
Research funds of the university and the F.W.O.-Vlaand-eren have made the development of these new procedurespossible. Besides the authors, all the other members ofthe Centres for Medical Genetics and ReproductiveMedicine were helpful in taking care of the patients andtheir embryos. Special acknowledgments go to F.Winterfor correcting the grammar and style and J.Heulaerts fortyping the manuscript.
ReferencesAo, A., Ray, P., Harper, J. et al. (1996) Clinical
experience with preimplantation genetic diagnosis ofcystic fibrosis (AF508). Prenat. Didgn., 16, 137-142.
Bonduelle, M., Wilikens, A., Buysse, A. et al. (1996)Prospective follow-up study of 877 children bornafter intracytoplasmic sperm injection (ICSI) withejaculated, epididymal and testicular spermatozoa andafter replacement of cryopreserved embryos afterICSI. Hum. Reprod., 11, 131-159.
Coonen, E., Dumoulin, J.M.C., Ramaekers, F.C.S. et al.(1994) Optimal preparation of preimplantation embryointerphase nuclei for analysis by fluorescence in-situhybridization. Hum. Reprod., 9, 533-537.
ESHRE Special Interest Group on Reproduction andGenetics/International Working Group on PGD (1997)Current status of preimplantation diagnosis. J. Assist.Reprod. Genet., 14, 72-75.
Griffin, D.K., Handyside, A.H., Penketh, R.J.A. et al.(1991) Fluorescent in-situ hybridization to interphasenuclei of human preimplantation embryos with X andY chromosome specific probes. Hum. Reprod., 6,101-105.
Handyside, A.H., Kontiogianni, E.H., Hardy, K. et al.(1990) Pregnancies from biopsied humanpreimplantation embryos sexed by Y specific DNAamplification. Nature, 344, 768-770.
Hardy, K., Martin, K.L., Leese, H. et al. (1990) Humanpreimplantation development in vitro is not adverselyaffected by biopsy at the 8-cell stage. Hum. Reprod.,5, 708-714.
Harper, J.C. (1996) Preimplantation diagnosis ofinherited disease by embryo biopsy: an update of theworld figures. J. Assist. Reprod. Genet., 13, 90-95.
Harper, J.C, Coonen, E., Ramaekers, F.C.S. et al. (1994)Identification of the sex of human preimplantationembryos in two hours using an improved spreadingmethod and fluorescence in-situ hybridization (FISH)using directly labelled probes. Hum. Reprod., 4,721-724.
Lissens, W., Sermon, K., Staessen, C. et al. (1996)Review: Preimplantation diagnosis of inheriteddisease. J. Inker. Metab. Dis., 19, 709-723.
Liu, J., Lissens, W., Devroey, P. et al. (1994a)Amplification of X- and Y-chromosome specificregions from single human blastomeres by polymerasechain reaction for sexing of preimplantation embryos.Hum. Reprod., 9, 716-720.
Liu, J., Lissens, W, Silber, S.J. et al. (1994b) Birth afterpreimplantation diagnosis of the cystic fibrosis AF508mutation by polymerase chain reaction in humanembryos resulting from intracytoplasmic sperminjection with epididymal sperm. J. Am. Med. Assoc,272, 1858-1860.
Liu, J., Lissens, W., Van Broeckhoven, C. et al. (1995)Normal pregnancy after preimplantation DNAdiagnosis of a dystrophin gene deletion. Prenat.Diagn., 15, 351-358.
Sermon, K., Lissens, W, Joris, H. et al. (1997) Clinicalapplication of preimplantation diagnosis for MyotonicDystrophy. Prenat. Diagn., in press.
191
Dow
nloaded from https://academ
ic.oup.com/hum
rep/article/13/suppl_1/186/788956 by guest on 08 July 2022
I.Liebaers et al.
Silber, S.J., Nagy, Z.P., Liu, J. et al. (1994) Conventionalin-vitro fertilization versus intracytoplasmic sperminjection for patients requiring microsurgical spermaspiration. Hum. Reprod., 9, 1705-1709.
Simpson, J.L. and Liebaers, I. (1996) Assessingcongenital anomalies after preimplantation geneticdiagnosis. J. Assist. Reprod. Genet., 13, 170-176.
Staessen, C , Janssenswillen, C , Van den Abbeel, E. etal. (1993) Evidence of triplet pregnancies by selectivetransfer of two quality embryos. Hum. Reprod., 8,1650-1653.
Staessen, C , Coonen, E., Van Assche, E. et al. (1996)Preimplantation diagnosis for X and Y normality inembryos from three Klinefelter patients. Hum.Reprod., 11, 1650-1653.
Tournaye H., Staessen, C , Liebaers, I. et al. (1996)Testicular sperm recovery in nine 47,XXY Klinefelterpatients. Hum. Reprod., 11, 1644-1649.
Van Steirteghem, A.C., Nagy, Z., Joris, H. et al. (1993)
High fertilization and implantation rates afterintracytoplasmic sperm injection. Hum. Reprod., 8,1061-1066.
Van Steirteghem, A.C., Joris, H., Liu, J. et al. (1995)Protocol for intracytoplasmic sperm injection. Hum.Reprod. Update, 1, No. 3, CD-ROM.
Verlinsky, Y, Cieslack, J., Ivakhnenko, V. et al. (1996)Birth of healthy children after preimplantationdiagnosis of common aneuploidies by polar bodyfluorescent in situ hybridization. Fertil. Steril., 66,126-129.
West, J.D., Gosden, CM., Gosden, J.R. et al. (1989)Sexing the human fetus and identification of polyploidnuclei by DNA-DNA in situ hybridisation ininterphase nuclei. Mol. Reprod. Dev., 1, 129-137.
Wisanto, A., Bonduelle, M., Camus, M. et al. (1996)Obstetric outcome of 904 pregnancies afterintracytoplasmic sperm injection. Hum. Reprod., 11,121-131.
192
Dow
nloaded from https://academ
ic.oup.com/hum
rep/article/13/suppl_1/186/788956 by guest on 08 July 2022
Clinical experience with PGD and ICSI
Appendix
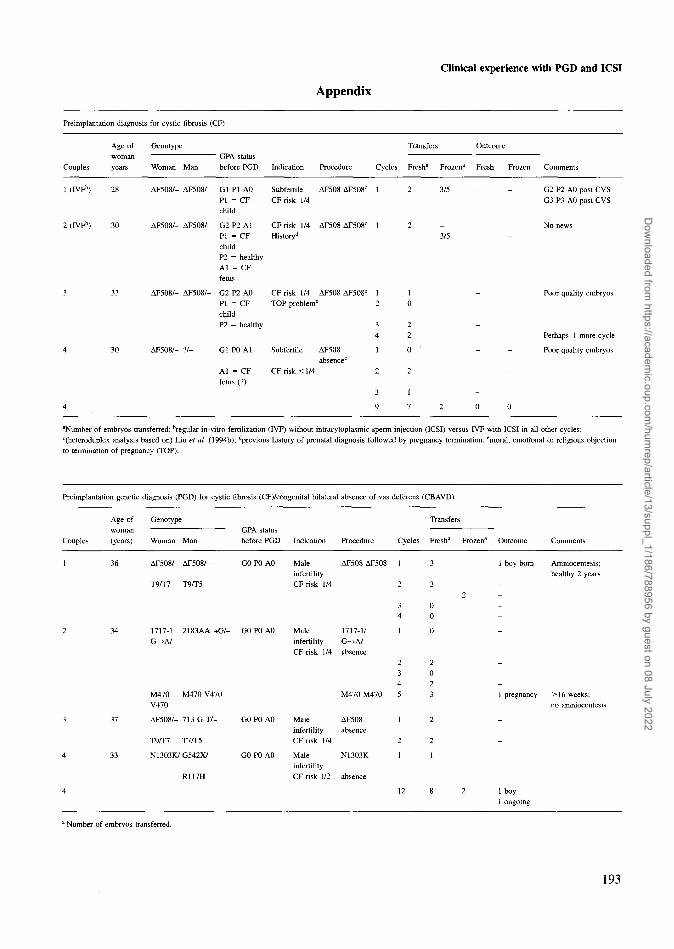
Preimplantation diagnosis for cystic fibrosis (CF)
Age of Genotypewoman GPA status
Couples years Woman Man before PGD Indication Procedure Cycles Fresha Frozena Fresh Frozen Comments
1 (IVFb) 28
2 (IVFb) 30
3 33
4 30
AF5O8/- AF508/- Gl PI A0 Subfertile AF508 AF508c 1PI = CF CF risk 1/4child
AF508/- AF508/- G2 P2 AlPI = CFchildP2 = healthyAl = CFfetus
AF508/- AF508/- G2 P2 A0PI = CFchildP2 = healthy
AF508/- ?/- Gl P0 Al
Al = CFfetus (?)
CF risk 1/4Historyd
CFrisk 1/4TOP problem'
Subfertile
CF risk <l /4
AF5O8 AF508c
AF508 AF5O8C
AF508absence0
1
12
34
1
2
3
9
2
10
22
0
2
1
7
3/5 G2 P2 A0 post CVSG3 P3 A0 post CVS
No news
Poor quality embryos
Perhaps 1 more cycle
Poor quality embryos
2 0 0
aNumber of embryos transferred; bregular in-vitro fertilization (IVF) without intracytoplasmic sperm injection (ICSI) versus IVF with ICSI in all other cycles;c(heteroduplex analysis based on) Liu et al. (1994b); ''previous history of prenatal diagnosis followed by pregnancy termination; emoral, emotional or religious objectionto termination of pregnancy (TOP).
Preimplantation genetic diagnosis (PGD) for cystic fibrosis (CF)/congenital bilateral absence of vas deferens (CBAVD)
Age of Genotypewoman
Couples (years) Woman ManGPA statusbefore PGD Indication Procedure Cycles Fresha Frozena Outcome Comments
AF508/- AF508/-
1717-1 2183AA-GH>A/-
MaleinfertilityCFrisk 1/4
!/- GO PO AO Male 1717-1/infertility G—>A/CF risk 1/4 absence
1
2
34
3
3
00
M470 M470 V470V470
AF5O8/- 713 G-T/-
T9/T7 T7/T5
N1303K/-G542X/
R117H
G0P0 A0
G0P0 A0
MaleinfertilityCF risk 1/4
MaleinfertilityCF risk 1/2
M470 M470
AF508absence
N13O3K
absence
5
1
2
1
3
2
2
1
1 boy born Amniocentesis;healthy 2 years
1 pregnancy >16 weeks;no amniocentesis
1 boy1 ongoing
1 Number of embryos transferred.
193
Dow
nloaded from https://academ
ic.oup.com/hum
rep/article/13/suppl_1/186/788956 by guest on 08 July 2022
I.Liebaers et al.
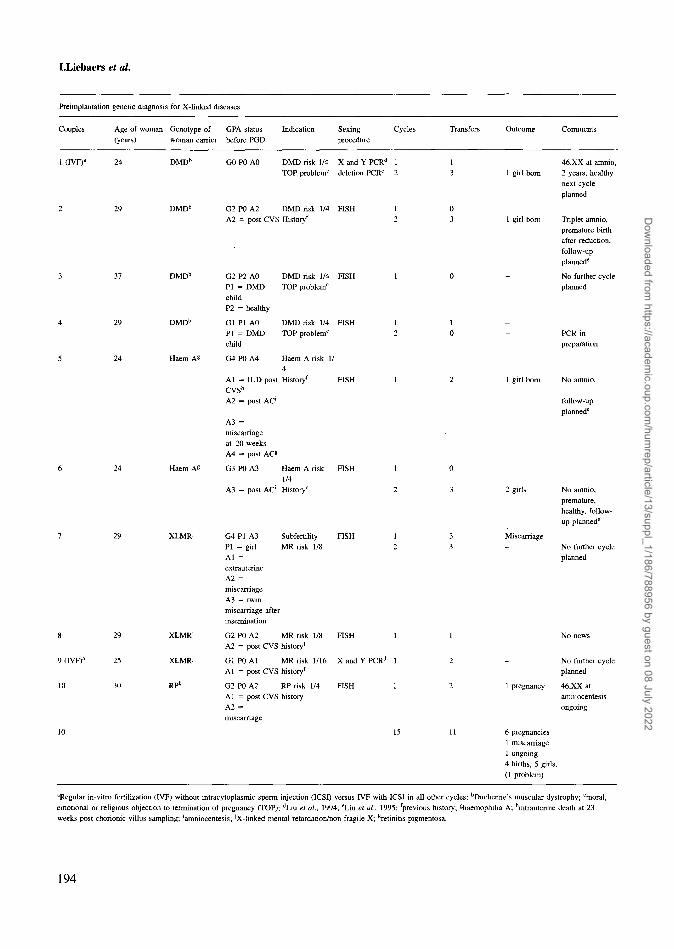
Preimplantation genetic diagnosis for X-linked diseases
Couples Age of woman Genotype of GPA status Indication Sexing Cycles(years) woman carrier before PGD procedure
Transfers Outcome Comments
29
29
DMDb
DMDb
DMDb
DMD"
Haem A*
Haem
9 (IVF)a
10
XLMRJ
XLMRJ
RPk
G0P0 A0 DMD risk 1/4 X and Y PCRd 1TOP problemc deletion PCRe 2
G2 P0 A2 DMD risk 1/4 FISHA2 = post CVS Historyf
G2 P2 A0PI = DMDchildP2 = healthy
Gl PI A0PI = DMDchild
G4P0 A4
DMD risk 1/4TOP problem0
DMD risk 1/4TOP problem0
Haem A risk 1/4
Al = IUD post Historyf FISHCVSh
A2 = post AC'
A3 =miscarriageat 20 weeksA4 = post AC«
G3 P0 A3 Haem A risk FISH1/4
A3 = post AC' History0
G4 PI A3PI = girlAl =extrauterineA2 =miscarriageA3 = twinmiscarriage afterinsemination
SubfertilityMR risk 1/8
FISH
G2 P0 A2 MR risk 1/8 FISH 1A2 = post CVS historyf
Gl P0 Al MR risk 1/16 X and Y PCRd 1Al = post CVS historyf
G2 P0 A2 RP risk 1/4Al = post CVS historyA2 =miscarriage
FISH
15
46,XX at amnio,1 girl born 2 years, healthy
next cycleplanned
1 girl born Triplet amnio,premature birthafter reduction,follow-upplannede
- No further cycleplanned
PCRinpreparation
1 girl born No amnio,
follow-upplannedc
2 girls
Miscarriage
1 pregnancy
No amnio,premature,healthy, follow-up plannede
No further cycleplanned
No further cycleplanned
46.XX atamniocentesisongoing
6 pregnancies1 miscarriage1 ongoing4 births, 5 girls,(1 problem)
aRegular in-vitro fertilization (IVF) without intracytoplasmic sperm injection (ICSI) versus IVF with ICSI in all other cycles; bDuchenne's muscular dystrophy; °moral,emotional or religious objection to termination of pregnancy (TOP); dLiu et al., 1994; eLiu et al, 1995; previous history; ghaemophilia A; hintrauterine death at 23weeks post chorionic villus sampling; 'amniocentesis; JX-linked mental retardation/non-fragile X; ''retinitis pigmentosa.
194
Dow
nloaded from https://academ
ic.oup.com/hum
rep/article/13/suppl_1/186/788956 by guest on 08 July 2022
Clinical experience with PGD and ICSI
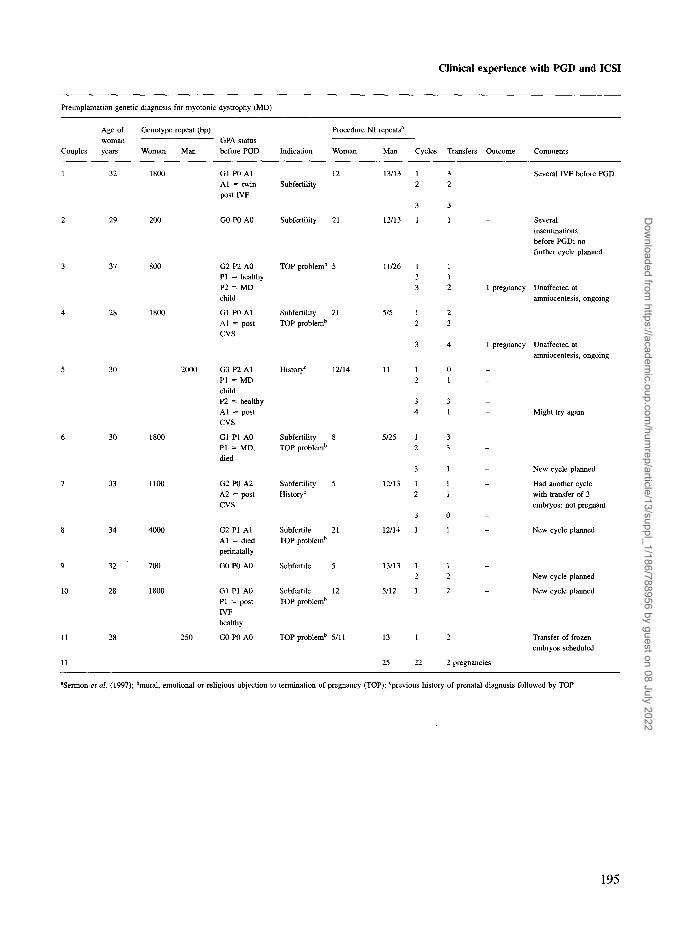
Preimplantation genetic diagnosis for myotonic dystrophy (MD)
Age of Genotype repeat (bp) Procedure NI repeatsa
woman GPA statusCouples years Woman Man before PGD Indication Woman Man Cycles Transfers Outcome Comments
32 1800 G1P0A1 12Al = twin Subfertilitypost IVF
Several IVF before PGD
29 200
800
GO P0 A0 Subfertility 21
28 1800
G2 P2 A0PI = healthyP2 = MDchild
Gl P0 AlAl = postCVS
TOP problem"
SubfertilityTOP problemb
5
21
12/13
11/26
5/5
1
123
12
1
112
23
Severalinseminationsbefore PGD; nofurther cycle planned
1 pregnancy Unaffected atamniocentesis, ongoin
1 pregnancy Unaffected atamniocentesis, ongoing
5
6
7
8
9
10
11
11
30
30
33
34
32
28
28
1800
1100
4000
700
1800
2000
250
G3 P2 AlPI = MDchildP2 = healthyAl = postCVS
Gl PI A0PI = MD,died
G2P0 A2A2 = postCVS
G2 PI AlAl = diedperinatally
G0P0 A0
Gl PI A0PI = postIVFhealthy
G0P0 A0
History1-
SubfertilityTOP problemb
SubfertilityHistory0
SubfertileTOP problemb
Subfertile
SubfertileTOP problem1"
TOP problem13
12/14
8
5
21
5
12
5/11
11
5/25
12/13
12/14
13/13
5/12
13
25
12
34
12
3
12
3
1
12
1
1
22
II
II
33 _
1
11
0
1
j _
2
2
2
2 pregnancies
Might try again
New cycle planned
Had another cyclewith transfer of 3embryos; not pregnant
New cycle planned
New cycle planned
New cycle planned
Transfer of frozenembryos scheduled
aSermon et al. (1997); bmoral, emotional or religious objection to termination of pregnancy (TOP); cprevious history of prenatal diagnosis followed by TOP.
195
Dow
nloaded from https://academ
ic.oup.com/hum
rep/article/13/suppl_1/186/788956 by guest on 08 July 2022
Related Documents











