Clinical Evaluation A/0 Clinical Evaluation Of Continuous Glucose Monitoring Systems

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Clinical Evaluation A/0
Clinical Evaluation
Of
Continuous Glucose Monitoring Systems

Clinical Evaluation A/0
Table of Content
Table of Content 2
1 Summary 3
2 Scope of the clinical evaluation 3
2.1 Product description 3
2.2 Intended use 3
2.3 Contraindication and Caution 5
2.3 Type/models 5
2.4 Product specification 5
2.5 Labelling 12
3 Clinical background, current knowledge, state of the art 12
4 Device under evaluation 14
4.1 Type of evaluation 14
4.2 Demonstration of equivalence 14
4.3 Clinical data held and generated by the manufacturer 19
4.4 Clinical data from literature 25
4.5. Summary and appraisal of clinical data 29
4.6. Analysis of the clinical data 37
5. Conclusions 41
6. Date of the next clinical evaluation 42
7. Dates and signatures 42
8. Qualification of the responsible evaluators 43
References 44
Appendix 1: Main Study Findings and Authors’ Conclusions 46

Clinical Evaluation A/0
1 Summary
This clinical discussion is developed to provide a comprehensive analysis of available
pre and post market clinical data relevant to the intended use of Continuous Glucose
Monitoring Systems, to ensure that there is sufficient evidence to confirm compliance
with relevant essential requirements for safety and performance when using the device
according to the manufacturer’s instructions for use.
2 Scope of the clinical evaluation
2.1 Product description
The Continuous Glucose Monitoring Systems is consist of a disposable sensor,
transmitter, App,and analysis software, in which the core device is the sensor electrode.
It is recommended to wear the sensor to the abdomen and minimize activities extent.
The sensor electrode chemically reacts with glucose in the hypodermic tissue fluid to
generate an electrical signal. Transmitter analysis and calculates the electrical signal,
and generates the blood glucose values, which is transmitted to the mobile App. The
user analysis software downloads and collects data from the mobile App for processing
and analysis, then gives reports.
During the monitoring period, at least two finger blood glucose values need to be
inputted into the Continuous Glucose Monitoring Systems every day for calibration. The
Continuous Glucose Monitoring Systems calculates an average of every three minutes.
The Continuous Glucose Monitoring Systems can record 480 glucose readings every 24
hours, continuously monitor the blood glucose data for 14 days and form a continuous
blood glucose curve. In addition, dining, sports, medication and other activities can be
recorded.
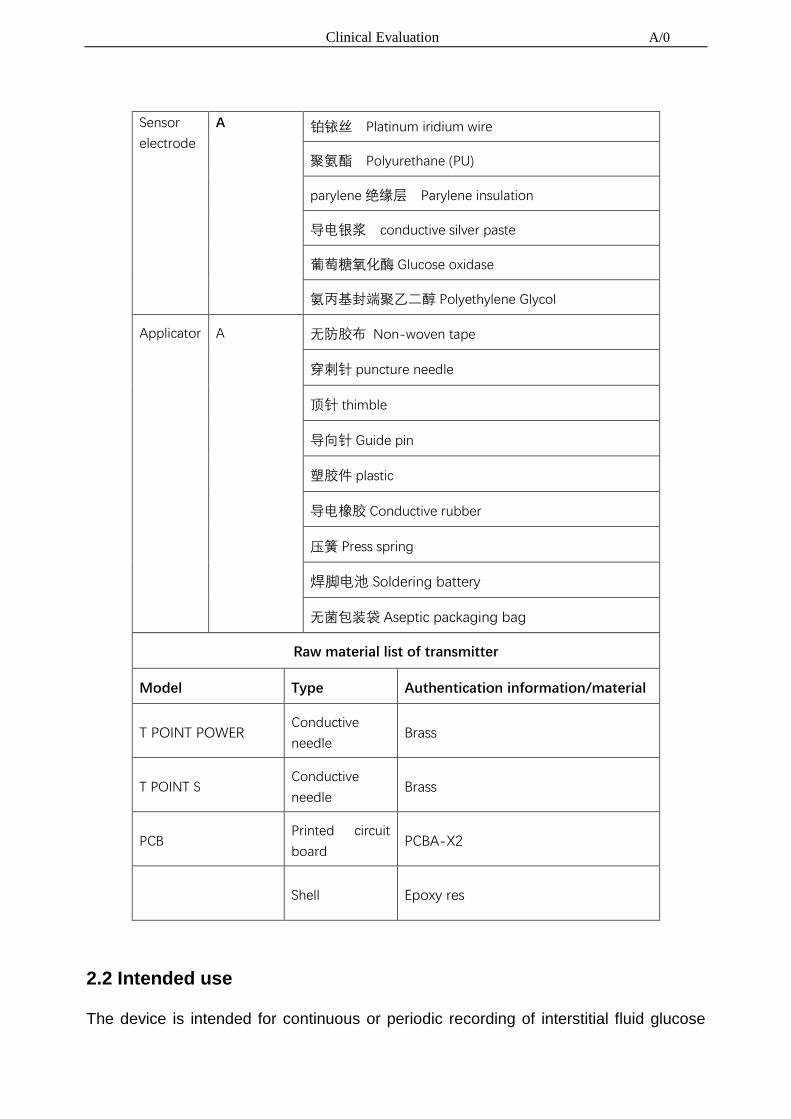
Critical components and materials of the product are listed as follows.
Raw material list of Sensor
Type Level Material
Clinical Evaluation A/0
Sensor
electrode
A 铂铱丝 Platinum iridium wire
聚氨酯 Polyurethane (PU)
parylene 绝缘层 Parylene insulation
导电银浆 conductive silver paste
葡萄糖氧化酶 Glucose oxidase
氨丙基封端聚乙二醇 Polyethylene Glycol
Applicator A 无防胶布 Non-woven tape
穿刺针 puncture needle
顶针 thimble
导向针 Guide pin
塑胶件 plastic
导电橡胶 Conductive rubber
压簧 Press spring
焊脚电池 Soldering battery
无菌包装袋 Aseptic packaging bag
Raw material list of transmitter
Model Type Authentication information/material
T POINT POWER Conductive
needle Brass
T POINT S Conductive
needle Brass
PCB Printed circuit
board PCBA-X2
Shell Epoxy res
2.2 Intended use
The device is intended for continuous or periodic recording of interstitial fluid glucose

Clinical Evaluation A/0
levels in adult patients with diabetes aged 18 or older. The system is designed for
patients to use at home and in medical institutions. The information is intended to supple,
rather than replace, the information obtained from standard glucose monitor like
traditional glucose meter and is intended to detect trends and track patterns and to
provide reference information for patients to manage diabetes. The system provides
real-time blood glucose value, which is received and read by the App. The blood glucose
value data can be further imported into the software for analysis of historical blood
glucose values.
2.3 Contraindication and Caution
Part of sensor electrode need to pierce the skin, so it is recommended that allergy and
skin ulcers people use the device cautiously. The product must be removed before
magnetic resonance imaging (MRI).
Taking acetaminophen while wearing the sensor may falsely raise your sensor glucose
readings.
2.4 Type/models
i3
2.5 Product specification
The Continuous Glucose Monitoring Systems is consist of a disposable sensor,
transmitter, App,and analysis software, in which the core device is the sensor electrode.

Clinical Evaluation A/0
Sensor
Transmitter
APP
Analysis software
Figure 1 Continuous Glucose Monitoring Systems
2.5.1 Sensor overview
Safety lock
Button
Sensor base and Adhesive patch
Figure 2 Sensor
The continuous glucose monitoring sensor is a product with a sterile sealed pouch. The
sensor is mainly composed of an applicator, a base and a sensor electrode. The base
consists of a PC base and an adhesive patch. The sensor electrode is divided into three

Clinical Evaluation A/0
layers: semi-permeable membrane, glucose oxidase layer and microelectrode. Insert
the sensor electrode into the subcutaneous tissue of the abdomen and remove the
applicator. The base is attached to the abdomen for up to 14 days of monitoring. Please
discard disposable sensor after wearing.5.6.1.1 The performance parameters of sensor
Table 1 The performance parameters of sensor
Model No. SI3-WL-03
Measurement range 2.2-22.2 mmol/L
Effective working
time 14 days
Calibration method Glucose meter
Calibration range 2.2-22.2 mmol/L
Storage conditions Temperature:2oC-25 oC;
Relative humidity:15%-85%
Transport conditions Normal temperature transportation
Rated voltage d.c. 3V
Battery lifetime No less than 14 days
Sterilization method Irradiation sterilization
Validity period 8 months
2.5.2 Transmitter overview
The continuous glucose monitoring transmitter is a component fixed on the sensor base
with chips. Once the transmitter is fixed in the sensor base and the sensor probe is
activated through the App, the transmitter sends the blood glucose message to the App.
When properly worn, the transmitter and App have a transmission range of 2 m without
obstruction. Wireless connection in the water is not very good, so the range of
connections in places like swimming pools, bathtubs and waterbeds will be even
smaller.
2.5.2.1 The performance parameters of transmitter
Table 2 The performance parameters of transmitter

Clinical Evaluation A/0
Model No. TI3-WL -03
Size length33 mm *width19 mm *height 4 mm
Weight of transmitter 3.7 g
Display interval 3 min
Calibration method Glucose meter
Calibration frequency 2 times / day(24h)
Data receiving range 2 m(Obstruction free)
Historical data storage
capacity No less than 14 days
Operation mode Continuous working
Power support Internal power supply
Classification Type BF
Protection grade IP27
Working conditions
(After the transmitter placed
in the sensor base)
Temperature:10 oC-40 oC;
Relative humidity:10%-95%
Atmospheric pressure 70kPa-106 kPa
Storage conditions Temperature:0 oC-45 oC;
Relative humidity:10%-95%
Validity period 36 months
Transport protocol Bluetooth 4.0
Operating Frequency Range 2400~2483.5MHz
Maximum Output Power 6dBm
25.5.2.2 EMC Statement
Guidance and manufacture's declaration – electromagnetic emissions
The Continuous Glucose Monitoring Systems is suitable for use in the specified
electromagnetic environment (s) and it has met the following standard’s emission
requirements.
Phenomenon Home healthcare environment
Conducted and radiated RF emissions CISPR 11, Group 1, Class B
Harmonic distortion N/A

Clinical Evaluation A/0
Voltage fluctuations and flicker N/A
Guidance and manufacture's declaration – electromagnetic immunity
The Continuous Glucose Monitoring Systems is suitable for use in the specified
electromagnetic environment (s) and it has met the following immunity test levels.
Higher immunity levels may cause the Continuous Glucose Monitoring Systems’s
essential performance lost or degraded.
Phenomenon Basic EMC standard or
test method
Home healthcare facility environment
Electrostatic
discharge IEC 61000-4-2
+/- 8 kV contact
+/- 2 kV, +/- 4 kV, +/- 8 kV, +/- 15 kV air
Radiated RF EM
fields IEC 61000-4-3
10V/m
80MHz-2.7GHz
80%AM at 1kHz
Proximity fields from
RF
wireless
communications
equipment
IEC 61000-4-3
See the RF wireless communication
equipment table in "Recommended
minimum separation distances".
Rated power
frequency magnetic
fields
IEC 61000-4-8 30A/m; 50 Hz or 60Hz
Electric fast
transients bursts IEC 61000-4-4 N/A

Clinical Evaluation A/0
Surges IEC 61000-4-5 N/A
Conducted
disturbances
induced by RF fields
IEC 61000-4-6 N/A
Voltage dips IEC 61000-4-11
N/A
N/A
Voltage
interruptions IEC 61000-4-11 N/A
Recommended minimum separation distances
Nowadays, many RF wireless equipment have being used in various healthcare
locations where medical equipment and/or systems are used. When they are used in
close proximity to medical equipment and/or systems, the medical equipment and/or
systems’ basic safety and essential performance may be affected. Continuous
Glucose Monitoring Systems has been tested with the immunity test level in the below
table and meet the related requirements of IEC 60601-1-2:2014. The customer and/or
user should help keep a minimum distance between RF wireless communications
equipment and Continuous Glucose Monitoring Systems as recommended below.
Test
frequency
(MHz)
Band
(MHz) Service Modulation
Maximum
power
(W)
Distance
(m)
Immunity
test level
(V/m)
385 380-390 TETRA 400
Pulse
modulation
18Hz
1.8 0.3 27
450 430-470 GMRS 460
FRS 460
FM
± 5 kHz
deviation
1 kHz sine
2 0.3 28
710 704-787
LTE Band
13, 17
Pulse
modulation 0.2 0.3 9
745

Clinical Evaluation A/0
780 217Hz
810
800-960
GSM
800/900,
TETRA 800,
iDEN 820,
CDMA 850,
LTE Band 5
Pulse
modulation
18Hz
2 0.3 28
870
930
1720
1700-1990
GSM 1800;
CDMA
1900;
GSM 1900;
DECT;
LTE Band 1,
3,
4, 25; UMTS
Pulse
modulation
217Hz
2 0.3 28
1845
1970
2450 2400-2570
Bluetooth,
WLAN,
802.11
b/g/n,
RFID 2450,
LTE Band 7
Pulse
modulation
217Hz
2 0.3 28
5240
5100-5800
WLAN
802.11
a/n
Pulse
modulation
217Hz
0.2 0.3 9 5500
5785
Table 3 EMC Statement
2.5.3 APP overview
Continuous glucose monitoring App is a mobile medical application for Continuous
Glucose Monitoring Systems to receive and process glucose readings. The software
displays blood glucose readings, trend curves, trend arrows, and transmitter status. It
has functions of adding events, event records, wearing records, alarm notifications,
reading lists, statistical analysis, data export, account management and so on.

Clinical Evaluation A/0
Figure 3 Main interface of App
The main interface of App mainly displays blood glucose readings, trend curves and
trend arrows. App and transmitter can be connected through bluetooth, pairing for data
communication. A blood glucose meter is also needed to be used with the Continuous
Glucose Monitoring Systems.
2.5.4 Analysis software overview
Continuous glucose monitoring analysis software is the auxiliary software of Continuous
Glucose Monitoring Systems. It can process the data collected in the App and generate
analysis reports.
2.6 Labelling
Label and IFU have been established, e.g. label sample is given in file no.
I3/WJ-XT-BQ-01, and IFU is given in file no. I3/WJ-XT-SMS-01.
3 Clinical background, current knowledge, state of the art
The blood sugar of a person with diabetes is continuously changing every minute of the
day throughout the person’s life. Patients may use glucometers to check blood sugar,
but this gives the value of blood sugar only at the particular time when the test is done.

Clinical Evaluation A/0
However, since blood sugar levels of a patient are changing from minute to minute,
checking simply with blood glucose meters may not be sufficient. Additionally, 60% of
glucose lows may not be revealed with self-monitoring of blood glucose (SMBG) alone.
Another standard way to monitor blood glucose is through the measurement of
glycosylated hemoglobin, more commonly known as hemoglobin A1c (HbA1c). But
again, HbA1c does not tell the whole story as while it provides information about glucose
exposure it is not able to track glycemic variability. HbA1c is a very useful test to detect
how well blood sugar is controlled over the previous 3 months. However, since HbA1c
indicates the average blood sugar, it does not give a correct picture of how much
fluctuations occur. In fact, if a patient has frequent low blood sugar, it could result in low
HbA1c (because HbA1c denotes an average value) and a false sense of security to the
patient and doctor, even when the blood sugar is often high and is actually poorly
controlled.
Thus, while SMBG and HbA1c are important—they do not tell us the complete
picture—especially information on glycemic variability of the patient.
Continuous glucose monitoring (CGM) can help complete the picture for a patient’s
glucose control. An effective way to monitor sugar levels to understand how the blood
sugar is changing throughout the day and to understand the state of glycemic
excursions in a patient is with the help of a technology called Continuous Glucose
Monitoring Systems (CGMS). It keeps a record every 3 minutes so that we can get 480
readings per day during the CGMS study period. A tiny, sterile, flexible electrode is
inserted just under the skin that measures glucose in the interstitial fluid (ISF). This data
is then uploaded onto a computer and clearly visible in the form of a graph which any
one can understand.
There are plenty of patients who have high blood sugar at odd times of the day which is
not detected by the routine tests like fasting blood sugar (FBS) and postprandial blood
sugar (PPBS) (blood sugar after food) or who are unaware that they may be
experiencing low blood sugars at night. The use of a CGMS can provide essential
information to the doctor to allow him/her to appropriately modify the treatment of their
patients to get better control of blood sugar throughout the day.
Clinical Evaluation A/0
Continuous glucose monitoring shows the complete picture of glucose activity, not just
snapshots of glucose levels. It allows users and clinicians to gain more insight by
providing real-time information about glucose levels and showing glucose trends
between finger sticks, leading to improved glucose control. CGM also provides
additional information beyond the “average” of overall glucose levels that is represented
by HbA1c. A recent study has shown that patients who use CGM at least 6 days a week
substantially lower their A1c levels without an increase in hypoglycemia, compared with
patients who use it less frequently. Continuous glucose readings allow patients to better
manage their diabetes by intervening on a real-time basis to reduce the frequency and
severity of hypoglycemic or hyperglycemic episodes. Patients can learn how diet,
exercise, medication, lifestyle and episodes of illness affect their glucose levels.
Furthermore, historical analysis provides insights for both patients and health care
professionals (HCPs) that can be translated into treatment adjustments and optimization.
Several studies have demonstrated a significant difference in A1c outcomes on the
basis of adjustments in insulin regimens in response to CGM.3-5 Hirsch (2002) has also
demonstrated that use of CGM in clinical practice would provide the required monitoring
tool to minimize glycemic variability and superoxide overproduction and may potentially
reduce diabetic complications.
4 Device under evaluation
4.1 Type of evaluation
Assessment of safety and performance of the devices in scope is based on several data
sources, including compliance with recognized standards, biocompatibility assessment
of the devices, and verification activities as well as clinical from relevant published
clinical literatures. The following is a presentation of these various data sources and the
evaluation thereof.
4.2 Demonstration of equivalence
The Continuous Glucose Monitoring Systems is as safe and effective as the predicate

Clinical Evaluation A/0
device as presented in Table 1.
Continuous Glucose Monitoring Systems is equivalent to the devices based on the
comparison given in Table 1.
Table 1 Equivalence demonstration
Characteristics
Continuous Glucose Monitoring
Systems
(Model: i3)
Continuous Glucose Monitoring
Systems
(Model: Dexcom G6)
Comparison
Product
Appearance
Sensor
Transmitter
APP
Analysis software
Substantially
equivalent.
Intended Use
The device is intended for
continuous or periodic recording
of interstitial fluid glucose levels
in adult patients with diabetes
aged 18 or older. The system is
designed for patients to use at
home and in medical institutions.
The device is intended to detect
trends and track patterns and to
provide reference information for
patients to manage diabetes.
The Dexcom G6 Continuous
Glucose Monitoring Systems
(Dexcom G6 System) is a real
time, continuous glucose
monitoring device indicated for the
management of diabetes in
persons age 2 years and older.
The Dexcom G6 System is
intended to replace fingerstick
blood glucose testing for diabetes
treatment decisions. Interpretation
of the Dexcom G6 System results
should be based on the glucose
Substantially
equivalent.
Intended use
and applicable
population of
Dexcom G6 is
wider than i3.

Clinical Evaluation A/0
trends and several sequential
readings over time. The Dexcom
G6 System also aids in the
detection of episodes of
hyperglycemia and hypoglycemia,
facilitating both acute and
long-term therapy adjustments.
The Dexcom G6 System is also
intended to autonomously
communicate with digitally
connected devices, including
automated insulin dosing (AID)
systems. The Dexcom G6 System
can be used alone or in
conjunction with these digitally
connected medical devices for the
purpose of managing diabetes.
Sensor specification
Sensor
Appearance
Safety lock
Button
Sensor base and Adhesive patch
Substantially
equivalent.
Glucose Range 2.2-22.2 mmol/L 40-400 mg/dL (2.2-22.2 mmol/L) Same
Sensor Life 14 days Up to 7 days Substantially
equivalent.
Calibration Glucose meter Commercially available blood Same

Clinical Evaluation A/0
glucose meter
Calibration
Range 2.2-22.2 mmol/L 40-400 mg/dL Same
Storage
Condition
Temperature:2oC-25 oC;
Relative humidity:15%-85%
Temperature: 36° F-77° F
Humidity: 15%-85% RH
Same
Sterilization Sterile by irradiation Sterile by radiation Same
Transmitter Specification
Dimensions
(Including Sensor
Pod)
length32 mm
width15.5 mm
height7.8 mm
Length: 1.5 inches
Width: 0.9 inches
Thickness: 0.5 inches
Minor
difference
does not
change
indication for
use.
Weight (Including
Sensor Pod) 6.2 g 0.4 ounces
Minor
difference
does not
change
indication for
use.
Power Supply
Internal power supply(battery in
base of sensor)
Silver oxide batteries (not
replaceable)
Minor
difference
does not
change
indication for
use.
Operational Temperature:10°C-40°C; Ambient temperature is 10° C-42° Substantially

Clinical Evaluation A/0
Conditions Relative humidity:10%-95% C (50° F-107.6° F)
Equilibrium temperature of less
than 0.5° C (0.9° F) above
ambient
Humidity: 10%-95% RH
equivalent.
Storage
Conditions
Temperature:0°C-45°C;
Relative humidity:10%-95%
Temperature: 32° F-113° F
Humidity: 10%-95% RH
Substantially
equivalent.
Atmospheric
pressure 70kPa-106 kPa
-1300 feet to 13800 feet
(Operating Altitude)
Substantially
equivalent.
Limited Warranty 112 days 3 months
Does not
change
indication for
use
Moisture
Protection IP27
IP28: Protection against insertion
of large objects and immersion in
water
for up to 8 feet for 24 hours
Minor
difference
does not
change
indication for
use.
Protection
Against Type BF
Electrical Shock Type BF applied
part Same
Data
Communication
Range
2m 20 feet
Minor
difference
does not
change
indication for
use.

Clinical Evaluation A/0
Data of the Predicate device (Dexcom G6) was extracted from Dexcom G6 IFU.
These two Continuous Glucose Monitoring Systems are both composed of a disposable
sensor, transmitter,analysis software and are designed for patients to use at home and
in medical institutions. The Dexcom G6 Continuous Glucose Monitoring Systems can
replace finger blood glucose monitoring and used in children more than 2 years old.
Dexcom G6 has wider intended use and applicable population, it contains the
functionality of i3. Thus, the safety and effectiveness of i3 can be proved.
CE certificate Number for the compared device: CE 591560
4.3 Clinical data held and generated by the manufacturer
4.3.1 Applicable standards
Assessment of safety and performance of the Continuous Glucose Monitoring Systems
is in part based on conformance with recognized standards which have established that
the device has been designed and manufactured with appropriate controls, the materials
of the subject device are appropriate for the intended use and the product is
appropriately packaged. The devices are in substantial conformance with the
recognized standards outlined in Table 2 below. Compliance with these standards
provides evidence for the safety and performance.
Table 2 Compliance Standards for Continuous Glucose Monitoring Systems
No. Standards Reference Content
1 EN ISO 15223-1 2016
Medical devices. Symbols to be used with medical
device labels, labelling and information to be
supplied. Part 1: General requirements
2 EN1041 2008/A1:20
13
Information supplied by the manufacturer with
medical devices
3 EN ISO 13485 2016/AC:20
16
Medical devices-quality management
systems-requirements for regulatory purposes
4 EN ISO 14971 2012 Medical devices-application of risk management to
medical devices

Clinical Evaluation A/0
5 EN 60601-1 2012+A1+A
2
Medical electrical equipment-part1: general
requirements for basic safety and essential
performance
6 EN60601-1-2 2015
Medical electrical equipment-part1-2: general
requirements for basic safety and essential
performance-collateral standard:
electromagnetic compatibility-requirements and
tests
7 EN60601-1-6 2010
Medical electrical equipment-part1-6: general
requirements for basic safety and essential
performance-collateral standard: usability
8 EN 60601-1-11 2010
Medical electrical equipment — Part 1-11: General
requirements for basic safety and essential
performance — Collateral standard: Requirements
for medical electrical equipment and medical
electrical systems used in the home healthcare
environment
IEC 60601-1-11:2010
9 EN ISO 10993-1 2009/AC:20
10
Biological evaluation of medical devices - Part 1:
Evaluation and testing within a risk management
process
10 EN ISO 10993-3 2014
Biological evaluation of medical devices — Part 3:
Tests for genotoxicity, carcinogenicity and repro-
ductive toxicity (ISO 10993-3:2014)
11 EN ISO 10993-5 2009 Biological evaluation of medical devices — Part 5:
Tests for in vitro cytotoxicity (ISO 10993- 5:2009)
12 EN ISO 10993-6 2009
Biological evaluation of medical devices — Part 6:
Tests for local effects after implantation (ISO
10993-6:2007)
13 EN ISO
10993-10 2013
Biological evaluation of medical devices – Part 10:
Tests for irritation and skin sensitization (ISO
10993-10:2010)
14 EN ISO
10993-11 2009
Biological evaluation of medical devices — Part 11:
Tests for systemic toxicity (ISO 10993- 11:2006)
15 EN ISO
10993-12 2012
Biological evaluation of medical devices — Part 12:
Sample preparation and reference materials (ISO
10993-12:2012)
16 EN ISO 14644-1 2015
Cleanrooms and associated controlled
environments - Part 1: Classification of air
cleanliness
17 EN ISO 14644-2 2015
Cleanrooms and associated controlled
environments - Part 2: Specifications for testing and
monitoring to prove continued compliance with ISO

Clinical Evaluation A/0
14644-1
18 ISO 14698-1 2003
Cleanrooms and associated controlled
environments - Biocontamination control - Part 1:
General principles and methods
19 ISO 14698-2 2003
Cleanrooms and associated controlled
environments - Biocontamination control - Part 2:
Evaluation and interpretation of biocontamination
data
20 EN 556-1 2001+AC:2
006
Sterilization of medical devices - Requirements for
medical devices to be designated "STERILE" - Part
1: Requirements for terminally sterilized medical
devices
21 EN ISO 11137-1 2015
Sterilization of health care products - Radiation -
Part 1: Requirements for development, validation
and routine control of a sterilization process for
medical devices
22 EN ISO 11137-2 2015 Sterilization of health care products - Radiation -
Part 2: Establishing the sterilization dose
23 EN ISO 11607-1 2009
Packaging for terminally sterilized medical devices -
Part 1: Requirements for materials, sterile barrier
systems and packaging
24 EN ISO 11607-2 2006
Packaging for terminally sterilized medical devices -
Part 2: Validation requirements for forming, sealing
and assembly processes
25 EN ISO 11737-1 2006+AC:2
009
Sterilization of medical devices - Microbiological
methods - Part 1: Determination of a population of
microorganisms on products
26 EN ISO 11737-2 2009
Sterilization of medical devices - Microbiological
methods - Part 2: Tests of sterility performed in the
definition, validation and maintenance of a
sterilization process
27 IEC 60529 2013 Degrees of protection provided by enclosures
28 ISTA 2A 2011 Packaged-Products 150lb (68kg) or less
29 WEEE (2002/96/E
C)
Waste Electrical and Electronic Equipment (WEEE)
Directive
30 RoHS (2011/65/E
U) Restriction of Hazardous Substances
31 EN62304 2006+
A1:2015
Medical device software. Software life-cycle
processes
32 EN62366-1 2015 Medical devices-application of usability engineering
to medical devices

Clinical Evaluation A/0
33 93/42/EEC 2007 Council directive 93/42/EEC of 14 June 1993
concerning medical devices
34 MEDDEV 2.7.1
Rev 4 2016
Clinical evaluation: a guide for manufacturers and
notified bodies.
Directives 93/42/EEC and 90/385/EEC.
35 IEC 62133 2012
Secondary cells and batteries containing alkaline or
other non-acid electrolytes – Safety requirements
for portable sealed secondary cells, and for
batteries made from them, for use in portable
applications
36 RED 2014/53/EU Radio Equipment Directive
4.3.2 Test report
See attached
4.3.2.1 Safety of Medical electrical Equipment 产品安全报告
Safety of medical electrical equipment testing of the device was performed in
accordance with technical standards applied. Refer to the following protocols
and reports.
Document Title 标准号 Document Number 测试报告号
EN 60601-1 Report no. 50276561 001
EN 60601-11
4.3.2.2 Electromagnetic Compatibility 电磁兼容
Electrical compatibility testing of the device was performed in accordance with
the technical standards applied. Refer to the following protocols and reports.
Document Title 标准号 Document Number 测试报告号
EN 60601-1-2 Report no. 50273828 001
4.3.2.3 Biological Safety 生物相容性评估报告
Biological Safety testing of the device was performed in accordance with the
technical standards applied. Refer to the following protocols and reports.
Document Title 标准号 Document Number 测试报告号
EN ISO 10993-1 Report no. I3/BG-XT-002
4.3.2.4 Usability 可用性报告
The device was evaluated against the standards applied. Refer to the
following reports for the scenarios tested.
Document Title 标准号 Document Number 测试报告号
EN62366
EN 60601-1-6
Report no. I3/BG-XT-001

Clinical Evaluation A/0
4.3.2.5 Sterilization Validation 灭菌验证报告
The Sensor is supplied steriled, and sterilized by Radiation sterilization to
ensure SAL≥10 -6. The Radiation sterilization is not conducted in-house but
outsourced to the subcontractor: Suzhou CNNC Huadong Radiation Co., Lt 苏
州中核华东辐照有限公司
The subcontractor has established a QM system according to EN ISO 13485
for provision of Radiation sterilization service of medical device according to
EN ISO 11137. The subcontractor has got EN ISO 13485 certificate and under
annual surveillance audit by the Certification Body. The QMS certificate and
subcontract agreement are enclosed as attachment to this file:
<灭菌协议文件编号>: Radiation Sterilization Subcontract Agreement
<灭菌公司的体系证书编号>: EN ISO 13485 certificate of the subcontractor
The sterilization process has been validated according to EN ISO 11137,
which has thereby determined the routine control and monitoring parameters.
Please refer to attachment:
Radiation sterilization validation report: CHF-TC/ML-19-07-WJ12
Sterilization Dose Setting report: CHF-TC/ML-19-06-SD06
For routine release of sterilization, the sterilization certificate will be provided
for each sterilization batch, reviewed and approved by Quality Department.
4.3.2.6 Sterile packaging system 无菌包装确认
The Sensors in the product are packaged in sterile barrier packaging system
which aims to ensure the sterile condition of the products inside the packaging
within specified shelf life. The primary package material is Tyvek1037b sealed
by heat-sealing machine.
The primary packaging process is evaluated and validated according to EN
ISO 11607-1/2. Please refer to attachment:
Packaging Validation Report 包装确认报告: CHF/TC-PH-19-07-25
Shelf-life validation 货架寿命验证报告: I3/BG-CG-005,I3/BG-FS-004
4.3.2.7 Transportation evaluation 包装运输试验
Document Title 标准号 Document Number 测试报告号
(ISTA)2A Report no. FTS1907074-2E-1/A,
FTS1907074-1E-1/A
4.3.2.8 Software evaluation report 软件评估报告
Document Title 标准号 Document Number 测试报告号
EN62304 Report no. I3/BG-RJ-001
Report no. I2/BG-RJ-W002
4.3.2.9 RED test report
Document Title 标准号 Document Number 测试报告号

Clinical Evaluation A/0
2014/53/EU Report no. 50177806
4.3.2.10 ROHS test report Document Number 测试报告号
Document Title 标准号 Report no. 0154350467a001
2011/65/EU
Due to these test reports, the product has met the requirements of international
standards, and was proved to be safe and effective.
4.3.3 Marketing authorization
The manufacturer has established and applies a quality management system for
manufacturing and distribution of Continuous Glucose Monitoring Systems, and has
been certified according to Directive 93/42/EEC Annex V and EN ISO 13485 by the
following Notified Body:
Name: TÜV Rheinland LGA Products GmbH
Address: Tillystraße 2, 90431, Nürnberg, Germany
CE identifier: 0197
The conformity assessment by the Notified Body follows the procedure relating to the
EC declaration of conformity set out in Annex VII of MDD, coupled with the procedure
set out in Annex V of MDD.
The copy of the certificates is given in the following attachments:
• MDD Annex V Certificate #DD 60135736 0001, issued on 2019-06-05, valid until
2024-02-29;
• EN ISO 13485 certificate #SX 60135737 0001, issued on 2019-06-05, valid
until.2022-02-28.
4.3.4 PMS
The manufacturer instituted and kept up to date a systematic procedure to review
experience gained from devices in the postproduction phase and to implement
appropriate means to apply any necessary corrective action.
The requirements of the PMS should be in direct proportion to the risk associated with

Clinical Evaluation A/0
the device.
In addition, the available scientific knowledge (e.g. long-term effects), market experience
with similar products, and manufacturer experience with the product or technology
should be considered.
No adverse incident or vigilance incident reported up to now.
4.4 Clinical data from literature
4.4.1 The object of literature review
A recent comprehensive literature search was performed to provide evidence of safety
and performance of the devices in question and to identify potential risks and hazards
pertinent to these devices in order to identify critical performance characteristics that
should be considered in the design and conditions for safe use relevant to the devices.
The specific objective and questions addressed by this current report include:
1. Does the literature present performance data pertinent to the equivalent
marketed device when used for the currently approved indications?
2. Does the literature present adverse/side-effect information pertinent to the
equivalent marketed device when used for the currently approved indications?
3. Are there previously unidentified reports/information relative to complications and
concerns associated with the application of subject devices?
4. Does the medical literature support a favorable risk/benefit analysis with respect
to the use of the subject devices for the stated indications?
4.4.2 Literature search and data source used
Information, addressing the performance and potential risk, associated with the use of
the device is retrieved from PUBMED, Cochrane Library, Clinical Trials and Science
Direct which operate independently from the manufacturer of the device(s).
This report is based mainly on original papers. Among the review articles, the data
sources used to obtain the references are listed as follows:

Clinical Evaluation A/0
Elsevier Science Direct: http://www.sciencedirect.com/
Wiley Online Library: http://onlinelibrary.wiley.com/
Springer-Link: http://link.springer.com/
EBSCO: http://search.ebscohost.com/
Nature: http://www.nature.com/
Science: http://www.sciencemag.org/
Lancet: http://www.sciencedirect.com/science/journal/01406736
NEJM: http://www.nejm.org/
JAMA: http://jamanetwork.com/
BMJ: http://journals.bmj.com/
OVID: http://ovidsp.ovid.com/
Cochrane library: http://www.thecochranelibrary.com/view/0/index.html
A broad search of the literature was performed incorporating by both electronic and
manually search components and included publications from 2000 till 2018.
The electronic search was performed using PubMed and a focused Internet search (e.g.
Wanfang Med Online, Google Scholar) to retrieve any articles that may be relevant to
this Clinical Evaluation Report. The clinical literature search focused primarily on
English-language literature with search limits to restrict retrieved articles to human
clinical trials.
Within the database, “Related articles” were selected and reviewed to assure that all
articles of interest had been identified. Additionally, the citations of retrieved literature
were manually reviewed to determine if there were additional data/publications pertinent
to this CER.
The primary aim of this search was to identify literature describing clinical data and
experience with equivalent devices in either randomized or non-randomized clinical
evaluations.

Clinical Evaluation A/0
The following search terms applied in various combinations or alone were used during
the search:
⚫ Continuous Glucose Monitoring Systems
⚫ Dexcom G4/G5/G6
References were included if they provided data pertinent to the assessment of safety
and performance of the devices subject of this CER, or the subject matter was relevant
to the safety and complications relative to the use of the devices.
Studies were excluded if they did not satisfy the selection criteria mentioned above, if
they were published prior to 2008, duplicate publications of the same study.
One reviewer screened the titles and abstracts of the retrieved publications and
evaluated the full-text publications for the final article selection, according to selection
criteria mentioned above.
4.4.3 Literature review protocol
4.4.3.1 Literature review inclusion and exclusion criteria
Table 3: Literature review inclusion and exclusion criteria
Higher priority and included Lower priority or excluded
Studies which target the Continuous
Glucose Monitoring Systems in adult
of either gender.
Multicenter, prospective, randomized
controlled clinical trial.
Studies which use appropriate
qualitative and quantitative research
methods, including meta-analysis and
high-quality literature reviews.
Multiple-centered retrospective
Cadaveric studies
Animal studies
Case report
Biomechanical studies
Studies which focus on devices other than
the proposed or the equivalent device
Interventions that are not indicated for the
use of the proposed device
Expert views

Clinical Evaluation A/0
studies
The data is generated from the
equivalent device.
Studies which contain insufficient
information to be able to undertake a
rational and objective assessment
Studies which has no appropriate statistical
analysis or limited power
4.4.3.2 Searching strategies and results
The following combination of search terms were used through the publications and the
subsequent searching result is shown in the table 4. Additional filters were selected as
Publishing Year to 2019/07/31.
Table 4: Search term and results
Search term Retrieved results Reference screened for
review
Continuous Glucose Monitoring
Systems Sort
by: Relevance Filters: Publication
date from 2000/01/01 to
2019/07/31
459 18
Dexcom G4/G5/G6 Sort
by: Relevance Filters: Publication
date from 2000/01/01 to
2019/07/31
85 8
By applying the up-mentioned inclusion and exclusion criteria, we synthesized the
articles retrieved from databases, a total of 17 articles were then selected for clinical
evaluation after eliminating duplication.

Clinical Evaluation A/0
4.5. Summary and appraisal of clinical data
Qualifying clinical reports were rated in accordance with an evidence rating scale for
therapeutic studies as indicated in Table 5 and all were graded for suitability as
indicated in Table 6.
Table 5 Evidence Rating Scale for Therapeutic Studies
Level of
Evidence Qualifying Literature
I High-quality, multi-centered or single-centered, randomized controlled trial
with adequate power; or systematic review of these studies
II Less-quality, randomized controlled trial; prospective cohort study; or
systematic review of these studies
III Retrospective comparative study; case-control study; or systematic review of
these studies
IV Case series (no, or historical, control group)
V Expert opinion; case report or clinical example; or evidence based on
physiology, bench research or "first principles"
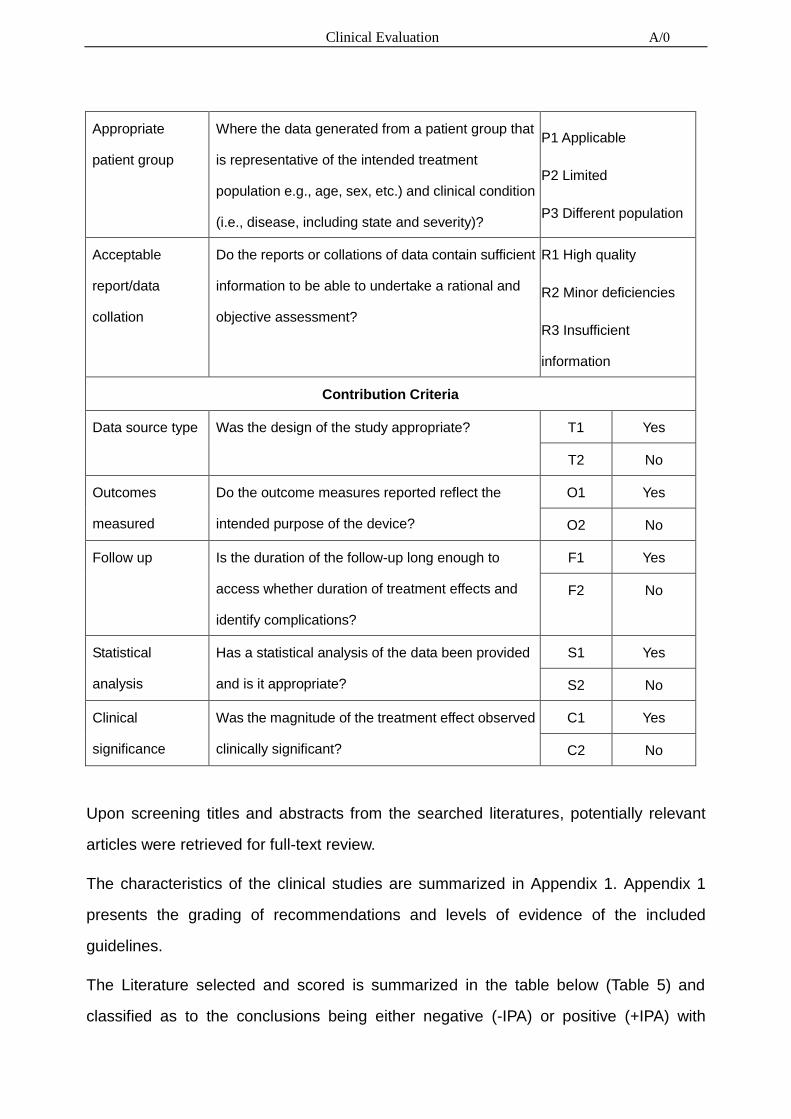
Table 6 Rating Scale for Suitability and Contribution
Suitability Criteria
Appropriate
device
Were the data generated from the device in
question?
D1 Actual device
D2 Equivalent device
D3 Other device
Appropriate
device application
Was the device used for the same intended use
(e.g., methods of deployment application, etc.)?
A1 Same use
A2 Minor deviation
A3 Major deviation
Clinical Evaluation A/0
Appropriate
patient group
Where the data generated from a patient group that
is representative of the intended treatment
population e.g., age, sex, etc.) and clinical condition
(i.e., disease, including state and severity)?
P1 Applicable
P2 Limited
P3 Different population
Acceptable
report/data
collation
Do the reports or collations of data contain sufficient
information to be able to undertake a rational and
objective assessment?
R1 High quality
R2 Minor deficiencies
R3 Insufficient
information
Contribution Criteria
Data source type Was the design of the study appropriate? T1 Yes
T2 No
Outcomes
measured
Do the outcome measures reported reflect the
intended purpose of the device?
O1 Yes
O2 No
Follow up Is the duration of the follow-up long enough to
access whether duration of treatment effects and
identify complications?
F1 Yes
F2 No
Statistical
analysis
Has a statistical analysis of the data been provided
and is it appropriate?
S1 Yes
S2 No
Clinical
significance
Was the magnitude of the treatment effect observed
clinically significant?
C1 Yes
C2 No
Upon screening titles and abstracts from the searched literatures, potentially relevant
articles were retrieved for full-text review.
The characteristics of the clinical studies are summarized in Appendix 1. Appendix 1
presents the grading of recommendations and levels of evidence of the included
guidelines.
The Literature selected and scored is summarized in the table below (Table 5) and
classified as to the conclusions being either negative (-IPA) or positive (+IPA) with

Clinical Evaluation A/0
respect to the use of the equivalent device. For some of the literature reports identified,
the outcomes were neither negative nor positive (denoted as “Balanced”).
Note that the average of the suitability and contribution scores awarded using the criteria
in Table 7 are shown independently but were also multiplied together to produce a
multiplier value for each dataset. The lower the multiplier value the greater the suitability
and contribution of the dataset to this clinical evaluation. For purposes of assigning a
suitability score, the studies performed in a human model is scored as P1 with respect to
appropriate patient group, and P2 if the study was performed in a non-human model,
parameters that were deemed not applicable (NA) or unable to determine (UTD) were
provided the highest score for the assessment. A limitation of this review is that there
were few randomized controlled trials available, with the majority of the publications
identified being prospective or case series (Level IV evidence).
Table 7 Outcome assessment for publications related to clinical data evaluation
Article Suitability
Score
Contribution
Score
Total
Score
Outcome/
Comment
Relevance to our
product
Efficacy and safety
comparison of
continuous glucose
monitoring and
selfmonitoring of blood
glucose in type 1
diabetes
5 5 25 +IPA
It is proved that CGM,
particularly its
real‑time system, has
a favorable effect on
glycemic control and
decreases the
incidence of
hypoglycemic
episodes in both adult
and pediatric patients
with type 1diabetes.
Beneficial effect of
real-time continuous
glucose monitoring
5 5 25 +IPA
It is proved that
RT-CGM is more
beneficial than SBGM

Clinical Evaluation A/0
system on glycemic
control in type 1
diabetic patients:
systematic review and
meta-analysis of
randomized trials
in reducing HbA1c in
patients with type 1
diabetes. Further
studies are needed to
evaluate the efficacy
of this system in the
pediatric population,
especially in very
young children.
Glycemic control in
diabetic CAPD patients
assessed by
continuous glucose
monitoring system
(CGMS) 5 6 30 +IPA
It is proved that
CGMS appears to be
a valid and clinically
useful technology to
gain additional
insights into the
glycemic control of
diabetic CAPD
patients, when
compared to
available methods.
Nocturnal
hypoglycemia detected
with the Continuous
Glucose Monitoring
System in pediatric
patients with type 1
diabetes
5 5 25 +IPA
CGMS is a useful tool
to diagnose
asymptomatic
nocturnal
hypoglycemia.
Performance
Evaluation of the 5 5 25 +IPA
Under household
conditions, CGMS

Clinical Evaluation A/0
MiniMed® Continuous
Glucose Monitoring
System During Patient
Home Use
and blood glucose
meter values have
good consistency.
Detailed blood sugar
information provided
by CGMS should
make the successful
management of
diabetes easier to
achieve.
A Comparative
Effectiveness Analysis
of Three Continuous
Glucose Monitors: The
Navigator, G4
Platinum, and Enlite
5 5 25 +IPA
A comprehensive
head-to-head-to-head
comparison of 3
CGMs revealed
marked differences in
both accuracy and
precision. All 3
devices had similar
reliability.
The Continuous
Glucose Monitoring
System Is Useful for
Detecting
Unrecognized
Hypoglycemias in
Patients with Type 1
and Type 2 Diabetes
but Is Not Better Than
Frequent Capillary
5 5 25 Balanced
The CGMS is useful
for detecting
unrecognized
hypoglycemias in
type 1 and type 2
diabetic subjects;
however, it is not
better than standard
capillary glucose
measurements for

Clinical Evaluation A/0
Glucose Measurements
for Improving Metabolic
Control
improving metabolic
control of type 1
diabetic subjects,
regardless of the
therapeutic regimen.
A randomized
controlled pilot study of
continuous glucose
monitoring and flash
glucose monitoring in
people with Type 1
diabetes and impaired
awareness of
hypoglycaemia
5 5 25 +IPA
CGM more effectively
reduces time spent in
hypoglycaemia in
people with Type 1
diabetes and
impaired awareness
of hypoglycaemia
compared with flash
glucose monitoring.
Head-to-head
comparison of the
accuracy of Abbott
FreeStyle Libre and
Dexcom G5 mobile 6 6 36 +IPA
The data indicate that
both systems perform
safely and efficiently
but the G5 sensor
has greater accuracy
across all glucose
values except in
hypoglycaemia.
Hypoglycemic
Accuracy and Improved
Low Glucose Alerts of
the Latest Dexcom G4
Platinum Continuous
Glucose Monitoring
System
5 5 25 +IPA
RT-CGMS may
provide patients with
timely warning of
hypoglycemia before
the onset of cognitive
impairment, enabling
them to treat

Clinical Evaluation A/0
themselves for
hypoglycemia with
fast-acting
carbohydrates and
prevent
neuroglycopenia
associated with very
low glucose levels.
Impact of Frequent and
Persistent Use of
Continuous Glucose
Monitoring (CGM) on
Hypoglycemia Fear,
Frequency of
Emergency Medical
Treatment, and SMBG
Frequency After One
Year
5 5 25 +IPA
“Almost daily” use of
CGM with the
Dexcom G4 system
reduced incidence of
emergency treatment
events and daily
SMBG utilization
among survey
respondents and a
trend toward reduced
hypoglycemia fear.
Nonadjunctive Use of
Continuous Glucose
Monitors for Insulin
Dosing: Is It Safe?
5 5 25 Balanced
Until the causes of
these sporadic, large
errors have been
identified, it would be
inappropriate to urge
users to regard the
device as safe for
insulin dosing without
confirmation.
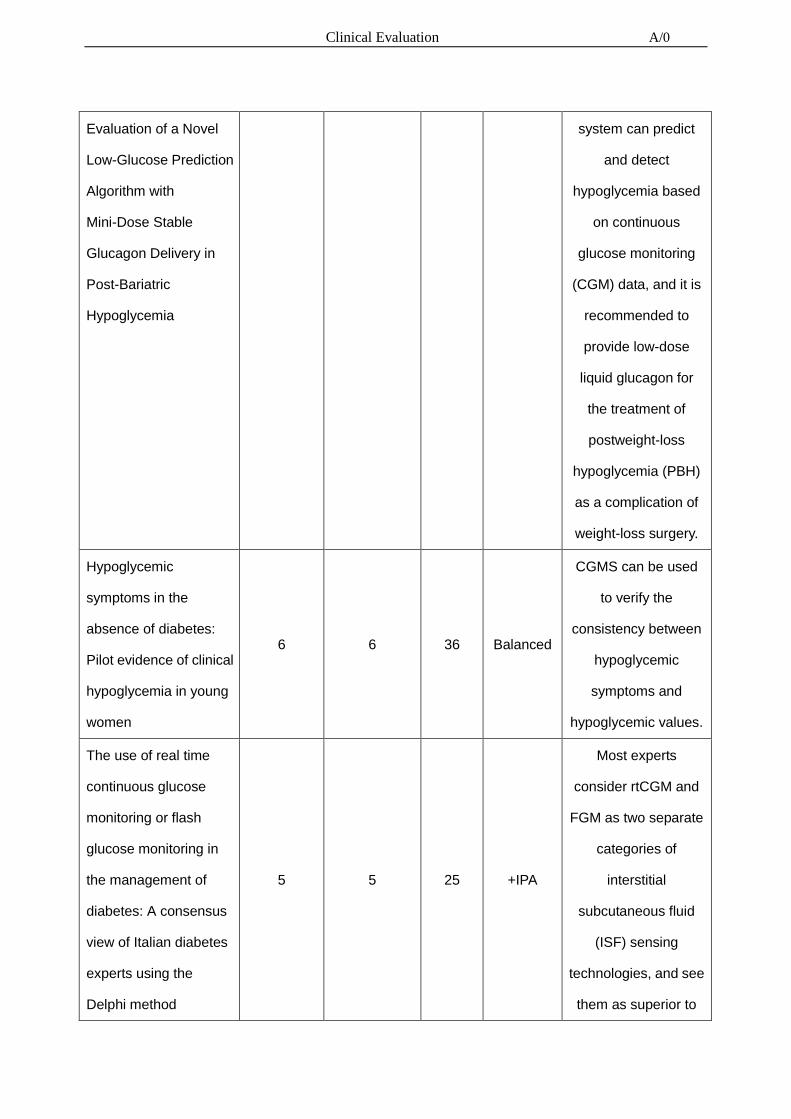
Design and Clinical 6 6 36 +IPA An event-based
Clinical Evaluation A/0
Evaluation of a Novel
Low-Glucose Prediction
Algorithm with
Mini-Dose Stable
Glucagon Delivery in
Post-Bariatric
Hypoglycemia
system can predict
and detect
hypoglycemia based
on continuous
glucose monitoring
(CGM) data, and it is
recommended to
provide low-dose
liquid glucagon for
the treatment of
postweight-loss
hypoglycemia (PBH)
as a complication of
weight-loss surgery.
Hypoglycemic
symptoms in the
absence of diabetes:
Pilot evidence of clinical
hypoglycemia in young
women
6 6 36 Balanced
CGMS can be used
to verify the
consistency between
hypoglycemic
symptoms and
hypoglycemic values.
The use of real time
continuous glucose
monitoring or flash
glucose monitoring in
the management of
diabetes: A consensus
view of Italian diabetes
experts using the
Delphi method
5 5 25 +IPA
Most experts
consider rtCGM and
FGM as two separate
categories of
interstitial
subcutaneous fluid
(ISF) sensing
technologies, and see
them as superior to

Clinical Evaluation A/0
SMBG. Furthermore,
there is strong
consensus that
rtCGM and FGM
reduce hypoglycemia
risk, increase the
amount of time in the
target glucose range
and augment
treatment
satisfaction.
Retrofitting Real-Life
Dexcom G5 Data 5 5 25 +IPA
Improved algorithm
can improve the
accuracy of CGMS
4.6. Analysis of the clinical data
4.6.1. Requirement on safety (MDD ER1)
A series of verification evaluations were conducted to assess the safety and
performance of the devices. Studies performed were identified on the basis of risk
analysis activities and testing of the product’s performance. Specific the following
variable and attribute characteristics were evaluated and the residual risks were
reduced to acceptable level:
• Biocompatibility: biocompatibility evaluation was conducted according to EN ISO
10993 series standards and passed all relevant tests.
• Operational/Information: Indication/contraindication, warning and direction for
use were presented in user manual.
• Electro/magnetic hazards: electronic performance/safety and EMC were

Clinical Evaluation A/0
evaluated based on applicable EN 60601-1 series standards.
• Radiation hazards: Risk of retinal injury was reduced by adequate warning given
in user manual.
4.6.2. Requirement on acceptable benefit/risk profile (MDD ER1)
Risk management process was implemented as addressed in Risk Management Report
#. I3/WJ-XT-FXFX-01.The risks associated with the intended purpose are minimized
and acceptable when weighed against the benefits to the patient and are compatible
with a high level of protection of health and safety.
IFU has been established based on the MDD ER1 Sec. 13 and clinical data from
literature searching, related information about contraindication, warnings, precautions
and instructions were adequately given, e.g. indication, contraindication, application
method and relevant warnings, and so on.
4.6.3. Requirement on performance (MDD ER3)
The Continuous Glucose Monitoring Systems is intended for continuous or periodic
recording of interstitial fluid glucose levels in adult patients with diabetes aged 18 or
older. The system is designed for patients to use at home and in medical institutions,
and the main findings of the clinical studies are presented in Appendix 1.
4.6.4. Requirement on acceptability of side-effects (MDD ER6)
Articles Pertaining to Potential Complications/Side-effect were reviewed and analyzed
as presented in Appendix 1.
Side-effects and complications identified from literature search were reviewed and
summarized.
Adequate information was given in IFU to minimize the risks.
According to risk management output, the overall residual risks were within acceptable
level.

Clinical Evaluation A/0
4.6.5 Postmarket surveillance Data
To supplement the literature review, an assessment of postmarket surveillance data via
review of the U.S. Food and Drug Administration’s Manufacturer and User Facility
Device Experience (MAUDE) database for similar products with same product code
was conducted.
The database was searched for a ten-years’ period starting in Jan 01 2008 through Dec
31, 2017 to identify reportable events associated with competitor products that are
similar in intended use and function to the CONTINUOUS GLUCOSE MONITORING
SYSTEMS identified within this CER.

Clinical Evaluation A/0
These reportable events are mainly due to: Wireless Communication Problem,
Imprecision, Retraction Problem and Use of Device Problem, which are all indicated in
the adverse events in the user manual, as well as evaluated and controlled in the risk
management process.
We considered these events and their reasons during the design and manufacturing

Clinical Evaluation A/0
process of the devices to avoid or decrease the probability of these events occurred.
We implemented the corresponding measures to control these potential hazards, and it
has been proved that the control measures are effective.
Problem 1: Wireless Communication Problem
Control measures: WJ-XT-FXFX-01 Risk management file, H15: Failure of connection
between sensor and transmitter. H16: The transmitter and App cannot be connected
normally. H22: Device may interfere with other equipment when it is working.
Problem 2: Imprecision
Control measures: WJ-XT-FXFX-01 Risk management file, H9: The blood sugar level
tested is not accurate. H10: The software is abnormal, the blood glucose level is not
accurate. H11: Forgetting calibration or incorrect calibration data results in inaccurate
blood glucose values. H12: Life expectancy, sensor coating enzyme inactivation or
transmitter battery loss lead to inaccurate blood glucose values. H14: Equipment was
used by untrained personnel
Problem 3: Retraction Problem
Control measures: WJ-XT-FXFX-01 Risk management file, H8: When the sensor is
implanted, the operation method is wrong. H27: Incomplete IFU, cause the operator
cannot use the product correctly
Problem 4: Use of Device Problem
Control measures: WJ-XT-FXFX-01 Risk management file, H32: Menu prompt is not
clear, ambiguous, or the user fails to understand the content of the menu correctly. H33:
The prompt tone is not clear. H34: The menu is not clearly displayed. H35: Unclear
Prompt or path
5. Conclusions
The limitations of the study are that only published literature is collected and
unpublished documents about negative result cannot be examined. The collected

Clinical Evaluation A/0
literature mainly concerns the assessment of the treatment efficacy and safety.
Base on evaluation on identification of data, pre-clinical evaluation, literature,
post-market surveillance and risk analysis, the evaluation conclusion is:
The safety and performance of the device from the evaluation with respect to the
intended use of the device as claimed have been established, and the risks associated
with the use of the device are acceptable when weighed against the Benefits to the
patient.
The risk/ benefit analysis shows that the benefits when using the device outweigh the
risks. Product is safety and effective in clinical use as system for human being.
The plan for Post-Market Clinical Follow-Up (PMCF) for device will include monitoring of
information such as complaints, adverse events, investigation reports, and possible
off-label use and user trends on an on-going basis in accordance with company
procedures. Further clinical evaluation will be documented periodically based on
observed trends or new emerging risks.
6. Date of the next clinical evaluation
The clinical evaluation is actively updated:
• when the manufacturer receives new information from PMS that has the potential to
change the current evaluation;
• if no such information is received, then
- At least annually if the device carries significant risks or is not yet well established;
or
- Every 2 years if the device is not expected to carry significant risks and is well
established, a justification should be provided.
7. Dates and signatures
Date of Signature:

Clinical Evaluation A/0
Name of Author: Signature
Name of Author: Signature
8. Qualification of the responsible evaluators
MISS.WANG Xiaoyu, Graduated from China Pharmaceutical University, now working in
Infinovo Medical CO., LTD.,5 years’ medical experience.
MR XIAO linchun, now working in Infinovo Medical CO., LTD., over 10 years’ medical
experience.

Clinical Evaluation A/0
References
1. Efficacy and safety comparison of continuous glucose monitoring and
self‑monitoring of blood glucose in type 1 diabetes, Piotr Wojciechowski1,
Przemysław Ryś1, Anna Lipowska2,3, Magdalena Gawęska1, Maciej T. Małecki3,4
2. Beneficial effect of real-time Continuous Glucose Monitoring Systems on glycemic
control in type 1 diabetic patients systematic review and meta-analysis of
randomized trials, A Szypowska, A Ramotowska, K Dz˙ygało and D Golicki1
3. Glycemic control in diabetic CAPD patients assessed by Continuous Glucose
Monitoring Systems (CGMS), JENNIFER MARSHALL, PETER JENNINGS,
ADRIAN SCOTT, RICHARD J. FLUCK, and CHRISTOPHER W. MCINTYRE
4. Nocturnal hypoglycemia detected with the Continuous Glucose Monitoring Systems
in pediatric patients with type 1 diabetes, Francine Ratner Kaufman, MD, Juliana
Austin, MD, Aaron Neinstein, BA, Lily Jeng, BA, Mary Halvorson, RN, MSN, CDE,
Debra J. Devoe, MD, and Pisit Pitukcheewanont, MD
5. Performance Evaluation of the MiniMed® Continuous Glucose Monitoring Systems
During Patient Home Use, TODD M. GROSS, Ph.D.,1 BRUCE W. BODE, M.D.,2
DANIEL EINHORN, M.D.,3 DAVID M. KAYNE, M.D.,4 JOHN H. REED, M.D.,5 NEIL
H. WHITE, M.D.,and JOHN J. MASTROTOTARO, Ph.D.1
6. A Comparative Effectiveness Analysis of Three Continuous Glucose Monitors: The
Navigator, G4 Platinum, and Enlite. Edward R. Damiano, PhD1, Katherine McKeon,
MEng1, Firas H. El-Khatib, PhD1, Hui Zheng, PhD2, David M. Nathan, MD3, and
Steven J. Russell, MD, PhD
7. The Continuous Glucose Monitoring Is Useful for Detecting Unrecognized
Hypoglycemias in Patients With Type 1 and Type 2 Diabetes but Is Not Better Than
Frequent Capillary Glucose Measurements for Improving Metabolic, ANA CHICO,
MD, PHD,PABLO VIDAL-R IOS, MD, PHD,MONTSERRAT SUBIR`A, NPANNA
NOVIALS, MD, PHD
8. A Practical Approach to Using Trend Arrows on the Dexcom G5 CGM System to
Manage Children and Adolescents With Diabetes. Laffel LM, Aleppo G, Buckingham

Clinical Evaluation A/0
BA, Forlenza GP, Rasbach LE, Tsalikian E, Weinzimer SA, Harris DR
9. A randomized controlled pilot study of continuous glucose monitoring and flash
glucose monitoring in people with Type 1 diabetes and impaired awareness of
hypoglycaemia. Reddy M, Jugnee N, El Laboudi A, Spanudakis E, Anantharaja S,
Oliver N
10. Head-to-head comparison of the accuracy of Abbott FreeStyle Libre and Dexcom
G5 mobile. Boscari F, Galasso S, Acciaroli G, Facchinetti A, Marescotti MC, Avogaro
A, Bruttomesso
11. Hypoglycemic Accuracy and Improved Low Glucose Alerts of the Latest Dexcom G4
Platinum Continuous Glucose Monitoring Systems. Peyser TA, Nakamura K, Price D,
Bohnett LC, Hirsch IB, Balo A
12. Impact of Frequent and Persistent Use of Continuous Glucose Monitoring (CGM) on
Hypoglycemia Fear, Frequency of Emergency Medical Treatment, and SMBG
Frequency After One Year. Chamberlain JJ, Dopita D, Gilgen E, Neuman A.
13. Nonadjunctive Use of Continuous Glucose Monitors for Insulin Dosing: Is It Safe?
Shapiro AR
14. Design and Clinical Evaluation of a Novel Low-Glucose Prediction Algorithm with
Mini-Dose Stable Glucagon Delivery in Post-Bariatric Hypoglycemia
15. Hypoglycemic symptoms in the absence of diabetes: Pilot evidence of clinical
hypoglycemia in young women
16. The use of real time continuous glucose monitoring or flash glucose monitoring in
the management of diabetes: A consensus view of Italian diabetes experts using the
Delphi method
17. Retrofitting Real-Life Dexcom G5 Data. Favero SD, Facchinetti A, Sparacino G,
Cobelli C

Clinical Evaluation A/0
Appendix 1: Main Study Findings and Authors’ Conclusions
Article Experimental Design (or
Article Description)
Subjects Evaluated Outcomes/Relevant Findings Level of
Evidence
Suitability and
Contribution
Efficacy and safety
comparison of continuous
glucose monitoring and
selfmonitoring of blood
glucose in type 1 diabetes
Based on a systematic review
and meta‑analysis, we aimed
to assess the efficacy and
safety of various CGM
systems compared with
SMBG
We searched major medical
databases up to June 2011
for randomized controlled
trials comparing CGM and
SMBG in type 1 diabetes.
Studies of at least 12‑week
duration were included.
CGM, partcicularly its real‑time
system, has a favorable effect on
glycemic control and decreases
the incidence of hypoglycemic
episodes in both adult and
pediatric patients with type 1
diabetes.
Level I evidence
D2, A1, P1, R1
T1, O1, F1, S1,
C1
Beneficial effect of
real-time continuous
glucose monitoring
system on glycemic
control in type 1 diabetic
patients: systematic
review and meta-analysis
The aimof this studywas to
explore the potential
beneficial effects of the use of
RT-CGMon diabetes
management compared with
self blood glucose
measurement (SBGM) in
patients with type 1 diabetes
mellitus (T1DM), bymeans of
a systematic review
MEDLINE, EMBASE, and
the Cochrane Library were
searched through by two
independent investigators
for RCTs concerning the
use of RT-CGM in patients
with T1DM.
RT-CGM is more beneficial than
SBGM in reducing HbA1c in
patients with type 1 diabetes.
Further studies are needed to
evaluate the efficacy of this
system in the pediatric
population, especially in very
young children.
Level I evidence
D2, A1, P1, R1
T1, O1, F1, S1,
C1

Clinical Evaluation A/0
Article Experimental Design (or
Article Description)
Subjects Evaluated Outcomes/Relevant Findings Level of
Evidence
Suitability and
Contribution
of randomized trials andmeta-analysis of
randomized controlled trials
(RCTs).
Glycemic control in
diabetic CAPD patients
assessed by continuous
glucose monitoring
system (CGMS)
The aims of this study were
to investigate the use of the
continuous glucose
monitoring system (CGMS) to
assess overall 24-hour
glycemic control and the
effects of both nonglucose
containing and more
biocompatible alternative
peritoneal dialysis solutions in
insulin-treated continuous
ambulatory peritoneal dialysis
(CAPD) patients.
We studied eight patients
with ESRF. All patients had
been treated with CAPD as
their only dialysis modality.
CGMS appears to be a clinically
useful tool to gain additional
insights into the glycemic control
of diabetic CAPD patients.
Level ǁ evidence
D2, A1, P2, R1
T1, O1, F1, S1,
C1
Nocturnal hypoglycemia
detected with the
Continuous Glucose
To use the Continuous
Glucose Monitoring Systems
(CGMS, MiniMed, Sylmar,
Calif) to determine if bedtime
blood glucose levels were
Patients (n = 47, 18 boys,
mean age 11.8 ± 4.6 years)
with type 1 diabetes used
CGMS for 167 nights. Data
were analyzed for glucose
Nocturnal hypoglycemia is
frequent, of long duration,
associated with bedtime glucose
values ≤100 to 150 mg/dL, and
predominately in the early part of
Level ǁ evidence
D2, A1, P2, R2
T1, O1, F1, S2,

Clinical Evaluation A/0
Article Experimental Design (or
Article Description)
Subjects Evaluated Outcomes/Relevant Findings Level of
Evidence
Suitability and
Contribution
Monitoring System in
pediatric patients with
type 1 diabetes
associated with the
occurrence of nocturnal
hypoglycemia
≤40 or ≤50 mg/dL,
comparing bedtime blood
glucose levels of ≤100
or >100 mg/dL and ≤150
or >150 mg/dL.
the night. CGMS is a useful tool
to diagnose asymptomatic
nocturnal hypoglycemia.
C1
Performance Evaluation
of the MiniMed®
Continuous Glucose
Monitoring System During
Patient Home Use
The present study evaluates
the performance of the
MiniMed® Continuous
Glucose Monitoring Systems
(CGMS) in patients with
diabetes during home use.
Performance data from the
first 135 uses of the CGMS
reported to the device
manufacturer have been
summarized.
These results demonstrate the
reliable and accurate
performance of the CGMS under
conditions of outpatient use.
Level ǁ evidence
D2, A1, P1, R1
T1, O1, F1, S1,
C1
A Comparative
Effectiveness Analysis of
Three Continuous
Glucose Monitors: The
Navigator, G4 Platinum,
and Enlite
The effectiveness and safety
of continuous glucose
monitors (CGMs) is
dependent on their accuracy
and reliability. The objective
of this study was to compare
Twenty-four subjects (12
adults) with type 1 diabetes
each participated in one
48-hour closed-loop BG
control experiment. Venous
plasma glucose (PG)
measurements obtained
every 15 minutes (4657
values) were paired in time
with corresponding CGM
Results: The Navigator and G4
Platinum (G4) had the best
overall accuracy, with an
aggregate mean absolute relative
difference (MARD) of all paired
points of 12.3 ± 12.1% and 10.8 ±
9.9%, respectively. Both had
lower MARDs of all paired points
than Enlite (17.9 ± 15.8%, P
< .005). Very large errors
Level ǁ evidence
D2, A1, P1, R1
T1, O1, F1, S1,
C1

Clinical Evaluation A/0
Article Experimental Design (or
Article Description)
Subjects Evaluated Outcomes/Relevant Findings Level of
Evidence
Suitability and
Contribution
3 CGMs in adult and pediatric
subjects with type 1 diabetes
under closed-loop
blood-glucose (BG) control.
glucose (CGMG)
measurements obtained
from 3 CGMs (FreeStyle
Navigator, Abbott Diabetes
Care; G4 Platinum,
Dexcom; Enlite, Medtronic)
worn simultaneously by
each subject.
(MARD > 50%) were less
common with the G4 (0.5%) than
with the Enlite (4.3%, P = .0001)
while the number of very large
errors with the Navigator (1.4%)
was intermediate between the G4
and Enlite (P = .1 and P = .06,
respectively). The average MARD
for experiments in adolescent
subjects were lower than in adult
subjects for the Navigator and
G4, while there was no difference
for Enlite. All 3 devices had
similar reliability. Conclusions:
A comprehensive
head-to-head-to-head
comparison of 3 CGMs revealed
marked differences in both
accuracy and precision. The
Navigator and G4 were found to
outperform the Enlite in these
areas

Clinical Evaluation A/0
Article Experimental Design (or
Article Description)
Subjects Evaluated Outcomes/Relevant Findings Level of
Evidence
Suitability and
Contribution
The Continuous Glucose
Monitoring System Is
Useful for Detecting
Unrecognized
Hypoglycemias in
Patients with Type 1 and
Type 2 Diabetes but Is
Not Better Than Frequent
Capillary Glucose
Measurements for
Improving Metabolic
Control
To evaluate whether the
Continuous Glucose
Monitoring Systems (CGMS;
MiniMed, Sylmar, CA) is
useful for investigating the
incidence of unrecognized
hypoglycemias in type 1 and
type 2 diabetic patients and
for improving metabolic
control in type 1 diabetic
patients.
A total of 70 diabetic
subjects (40 type 1 and
30 type 2 subjects) were
monitored using the CGMS.
The CGMS is useful for detecting
unrecognized hypoglycemias in
type 1 and type 2 diabetic
subjects; however, it is not better
than standard capillary glucose
measurements for improving
metabolic control of type 1
diabetic subjects, regardless of
the therapeutic regimen.
Level ǁ evidence
D2, A1, P1, R1
T1, O1, F1, S1,
C1
A randomized controlled
pilot study of continuous
glucose monitoring and
flash glucose monitoring
in people with Type 1
diabetes and impaired
awareness of
hypoglycaemia
Hypoglycaemia in Type 1
diabetes is associated with
mortality and morbidity,
especially where awareness
of hypoglycaemia is impaired.
Clinical pathways for access
to continuous glucose
monitoring (CGM) and flash
glucose monitoring
technologies are unclear. We
A randomized, non-masked
parallel group study was
undertaken. Adults with
Type 1 diabetes using a
multiple-dose
insulin-injection regimen
with a Gold score of ≥ 4 or
recent severe
hypoglycaemia were
recruited. Following 2 weeks
RESULTS:
CONCLUSION:
CGM more effectively reduces
time spent in hypoglycaemia in
people with Type 1 diabetes and
impaired awareness of
hypoglycaemia compared with
flash glucose monitoring
Level ǁ evidence
D2, A1, P2, R1
T1, O1, F1, S1,
C1

Clinical Evaluation A/0
Article Experimental Design (or
Article Description)
Subjects Evaluated Outcomes/Relevant Findings Level of
Evidence
Suitability and
Contribution
assessed the impact of CGM
and flash glucose monitoring
in a high-risk group of people
with Type 1 diabetes.
of blinded CGM, they were
randomly assigned to CGM
(Dexcom G5) or flash
glucose monitoring (Abbott
Freestyle Libre) for 8 weeks.
The primary outcome was
the difference in time spent
in hypoglycaemia (below 3.3
mmol/l) from baseline to
endpoint with CGM versus
flash glucose monitoring.
Head-to-head
comparison of the
accuracy of Abbott
FreeStyle Libre and
Dexcom G5 mobile
The aim of this study was to
compare the performance of
FSL and DG5M. Differently
from the previous study, here
both sensors were used
according to their
manufacturer specified
Recently, we published in
Nutrition Metabolism
Cardiovascular Disease an
article comparing the
accuracy of flash glucose
monitoring Freestyle Libre
(FSL, Abbott Diabetes Care,
Our data indicate that both
systems perform safely and
efficiently but the DG5M sensor
has greater accuracy across all
glucose values except in
hypoglycaemia. Furthermore, as
shown before , Libre’s accuracy
Level ǁ evidence
D2, A1, P1, R2
T1, O1, F1, S1,
C2

Clinical Evaluation A/0
Article Experimental Design (or
Article Description)
Subjects Evaluated Outcomes/Relevant Findings Level of
Evidence
Suitability and
Contribution
life times, patients received
only one breakfast test and
used a glucometer
independently of the devices
to avoid bias in assessing the
accuracy at home.
Alameda, CA; wear lifetime
14 days) with that of the
continuous glucose
monitoring device Dexcom
G4 Platinum (DG4P,
Dexcom, San Diego, CA)
[3]. After the completion of
that study, using the same
methodology, we compared
the accuracy of FSL with
that of Dexcom G5 Mobile
(DG5M; wear lifetime 7
days), the most recent
sensor produced by
Dexcom Inc.
decreases between days 11 and
14, an important finding for
patients, especially when using
the sensor as non-adjunctive
device continuously for 14 days

Clinical Evaluation A/0
Article Experimental Design (or
Article Description)
Subjects Evaluated Outcomes/Relevant Findings Level of
Evidence
Suitability and
Contribution
Hypoglycemic Accuracy
and Improved Low
Glucose Alerts of the
Latest Dexcom G4
Platinum Continuous
Glucose Monitoring
System
Accuracy of continuous
glucose monitoring (CGM)
devices in hypoglycemia has
been a widely reported
shortcoming of this
technology. We report the
accuracy in hypoglycemia of
a new version of the Dexcom
(San Diego, CA) G4 Platinum
CGM system (software 505)
and present results regarding
the optimum setting of CGM
hypoglycemic alerts.
CGM values were
compared with YSI analyzer
(YSI Life Sciences, Yellow
Springs, OH)
measurements every
15 min. We reviewed the
accuracy of the CGM
system in the hypoglycemic
range using standard
metrics. We analyzed the
time required for the CGM
system to detect
biochemical hypoglycemia
(70 mg/dL) compared with
the YSI with alert settings at
70 mg/dL and 80 mg/dL. We
also analyzed the time
between the YSI value
crossing 55 mg/dL, defined
as the threshold for
cognitive impairment due to
hypoglycemia, and when
CONCLUSIONS:
Use of an 80 mg/dL threshold
setting for hypoglycemic alerts on
the G4 Platinum (software 505)
may provide patients with timely
warning of hypoglycemia before
the onset of cognitive impairment,
enabling them to treat themselves
for hypoglycemia with fast-acting
carbohydrates and prevent
neuroglycopenia associated with
very low glucose levels.
Level ǁ evidence
D2, A1, P2, R1
T1, O1, F1, S1,
C2

Clinical Evaluation A/0
Article Experimental Design (or
Article Description)
Subjects Evaluated Outcomes/Relevant Findings Level of
Evidence
Suitability and
Contribution
the CGM system alerted for
hypoglycemia.
Impact of Frequent and
Persistent Use of
Continuous Glucose
Monitoring (CGM) on
Hypoglycemia Fear,
Frequency of Emergency
Medical Treatment, and
SMBG Frequency After
One Year
We assessed the impact of
"almost daily" use of
continuous glucose
monitoring (CGM) in adults
with type 1 diabetes who had
at least 1 year of CGM
experience
In this single-center survey,
we utilized a 16-item
questionnaire to assess
changes hypoglycemia fear,
incidence of emergency
medical treatment and
utilization of self-monitoring
of blood glucose (SMBG)
before and after 1 year of
CGM use. Participation was
restricted to individuals who
used the same brand of
CGM system to avoid
confounding responses due
to differences between
commercial devices.
Participants were recruited
on an "as-seen" basis from
a major, urban internal
medicine clinic and
"Almost daily" use of CGM with
the Dexcom G4 system reduced
incidence of emergency
treatment events and daily SMBG
utilization among survey
respondents and a trend toward
reduced hypoglycemia fear. This
may indicate cost savings in
reduction of emergency medical
intervention and likely improved
quality of life without increasing
safety concerns related to
hypoglycemia.
Level ǁ evidence
D2, A1, P1, R1
T1, O1, F1, S1,
C1

Clinical Evaluation A/0
Article Experimental Design (or
Article Description)
Subjects Evaluated Outcomes/Relevant Findings Level of
Evidence
Suitability and
Contribution
associated diabetes
education center. The
questionnaire was
completed during the clinic
visit. Responses to the
survey were analyzed by
standard descriptive
statistics.
Nonadjunctive Use of
Continuous Glucose
Monitors for Insulin
Dosing: Is It Safe?
With the increasing accuracy
of continuous glucose
monitors (CGM) have come
calls for the Food and Drug
Administration (FDA) to label
these devices as safe for
nonadjunctive dosing of
insulin. However, there is
evidence that these devices
are subject to sporadic,
unpredictable, large errors.
A text analysis of reports to
the FDA MAUDE database
since 2015 reveals over 25
000 complaints of CGM
sensor inaccuracy, with
instances directly leading to
serious outcomes. These
new data were not
considered at a recent FDA
Advisory Panel meeting that
voted to approve Dexcom
G5 relabeling for
nonadjunctive use.
Social media is another source of
surveillance data providing
evidence of large CGM
inaccuracies in real-world use.
We need to improve safety
procedures, not remove them.
CGMs offer unique information
and alerts for managing diabetes,
but the issue is not whether they
are better than other approaches
to monitoring glucose, but how
they can be best used in
conjunction with devices that offer
the confirmatory readings needed
Level III
evidence
D2, A1, P1, R1
T1, O1, F2, S1,
C1

Clinical Evaluation A/0
Article Experimental Design (or
Article Description)
Subjects Evaluated Outcomes/Relevant Findings Level of
Evidence
Suitability and
Contribution
for patient safety
Design and Clinical
Evaluation of a Novel
Low-Glucose Prediction
Algorithm with Mini-Dose
Stable Glucagon Delivery
in Post-Bariatric
Hypoglycemia
Postbariatric hypoglycemia
(PBH) is a complication of
bariatric surgery with limited
therapeutic options. We
developed an event-based
system to predict and detect
hypoglycemia based on
continuous glucose monitor
(CGM) data and recommend
delivery of minidose liquid
glucagon.
We performed an iterative
development clinical study
employing a novel glucagon
delivery system: a Dexcom
CGM connected to a
Windows tablet running a
hypoglycemia prediction
algorithm and an Omnipod
pump filled with an
investigational stable liquid
glucagon formulation. Meal
tolerance testing was
performed in seven
participants with PBH and
history of neuroglycopenia.
Glucagon was administered
when hypoglycemia was
predicted. Primary outcome
measures included the
safety and feasibility of this
system to predict and
Preliminary results indicate that
our event-based automatic
monitoring algorithm successfully
predicted likely hypoglycemia.
Minidose glucagon therapy was
well tolerated, without prolonged
or severe hypoglycemia, and
without rebound hyperglycemia.
Level III
evidence
D2, A1, P1, R1
T1, O1, F1, S2,
C1

Clinical Evaluation A/0
Article Experimental Design (or
Article Description)
Subjects Evaluated Outcomes/Relevant Findings Level of
Evidence
Suitability and
Contribution
prevent severe
hypoglycemia. Secondary
outcomes included
hypoglycemia prediction by
the prediction algorithm,
minimization of time below
hypoglycemia threshold
using glucagon, and
prevention of rebound
hyperglycemia.
Hypoglycemic symptoms
in the absence of
diabetes: Pilot evidence
of clinical hypoglycemia
in young women
Clinical visits of non-diabetic
patients reporting
hypoglycemic symptoms are
common in endocrinology
practices, but remain
understudied and lack clinical
definition and evidence-based
recommendations for
diagnosis or treatment. Our
goal was to pilot test the
concordance of hypoglycemic
symptoms with low glucose
We recruited eight
individuals who reported
regularly experiencing
symptoms consistent with
hypoglycemia to wear a
blinded Dexcom continuous
glucose monitor and report
symptoms for seven days.
We excluded individuals with
diabetes or other known
causes of hypoglycemia or
similar symptoms.
Individuals with hypoglycemic
symptoms in the absence of
diabetes experience clinical
hypoglycemia, indicating the need
to understand the etiology,
behavioral responses, and other
health risks that might be
associated with this understudied
condition.
Level IV
evidence
D2, A1, P2, R1
T1, O1, F2, S2,
C1

Clinical Evaluation A/0
Article Experimental Design (or
Article Description)
Subjects Evaluated Outcomes/Relevant Findings Level of
Evidence
Suitability and
Contribution
values in young non-diabetic
individuals.
The use of real time
continuous glucose
monitoring or flash
glucose monitoring in the
management of diabetes:
A consensus view of
Italian diabetes experts
using the Delphi method
the use of continuous glucose
monitoring (CGM) systems has
been limited, but is now
rapidly increasing, including
the so-called real-time CGM
(rtCGM) and the intermittently
viewed CGM (iCGM), also
called Flash Glucose
Monitoring (FGM). These
technologies overcome many
of the limitations of
self-monitoring of blood
glucose (SMBG) by fingerprick
and allow to go beyond
HbA1c to check glucose
control in diabetes. However,
standardized protocols for
applying and interpreting
rtCGM and FGM data are
lacking
In this paper, we delineate a
consensus amongst Italian
diabetes physicians on the
attributes of rtCGM and FGM
technologies, and introduce
a consistent approach for
their use by Italian healthcare
professionals.
Most experts consider rtCGM and
FGM as two separate categories of
interstitial subcutaneous fluid (ISF)
sensing technologies, and see
them as superior to SMBG.
Furthermore, there is strong
consensus that rtCGM and FGM
reduce hypoglycemia risk, increase
the amount of time in the target
glucose range and augment
treatment satisfaction. However,
there is still no agreement on the
indication of the FGM for subjects
who suffer asymptomatic
hypoglycemia. Consensus on the
role of education in initiating and
optimizing use of rtCGM/FGM and
about the interpretation of glucose
trends was near unanimous,
whereas no consensus was
Level IV
evidence
D2, A1, P2, R1
T1, O1, F2, S2,
C2

Clinical Evaluation A/0
Article Experimental Design (or
Article Description)
Subjects Evaluated Outcomes/Relevant Findings Level of
Evidence
Suitability and
Contribution
reached on the statement that
there are no disadvantages/risks of
rtCGM/FGM.
Retrofitting Real-Life
Dexcom G5 Data
We proposed in 2014 a
retrofitting algorithm to
retrospectively increase the
accuracy of continuous
glucose monitoring (CGM)
data by using some blood
glucose (BG) measurements.
The method proved effective
on Dexcom SEVEN Plus
when about 10 highly
accurate YSI
measurements/session were
available. In this study, we
test the method on Dexcom
G5 sensor in a more realistic
setup, where only five
capillary BG measurements
(self-monitoring blood
glucose [SMBG]) per
The algorithm was tested in
51 adults and 46
adolescents studied for 7
days with Dexcom G5. Each
patient also underwent an
∼12-h hospital admission
where frequent SMBG and
YSI measurements were
collected. First, five SMBGs
per 12-h session were used
to retrofit the CGM. Then,
we varied the number of
SMBGs provided to the
method from 2 to 10 per
12-h session.
RESULT:
Retrofitted CGM traces with five
SMBGs per 12-h session have
lower mean absolute difference
than original CGM, reduced from
16.2 to 10.7 mg/dL (P < 0.001) in
adults and from 17.6 to
11.5 mg/dL (P < 0.001) in
adolescents, and mean absolute
relative difference is reduced
from 9.0% to 6.4% (P < 0.001) in
adults and from 10.3% to 6.8%
(P < 0.001) in adolescents.
Reducing the number of BG
measurements reduces
improvement in the accuracy
from >30% with 10 SMBGs per
12-h session to <16% with 2
SMBGs/day.
Level II evidence
D2, A1, P1, R1
T1, O1, F1, S1,
C1

Clinical Evaluation A/0
Article Experimental Design (or
Article Description)
Subjects Evaluated Outcomes/Relevant Findings Level of
Evidence
Suitability and
Contribution
12 h-session are available.
Furthermore, we investigate
how accuracy is affected by
the number of BG
measurements
CONCLUSION:
The retrofitting method
retrospectively improves the
accuracy of CGM data, even if
applied to one of the most
accurate CGM sensors currently
available on the market.
Related Documents











