Health Studies 315 Health Studies 315 1 Clinical Epidemiology: Evidence of Risk and Harm Clinical Epidemiology: Evidence of Risk and Harm

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Health Studies 315Health Studies 315
1
Clinical Epidemiology:
Evidence of Risk and Harm
Clinical Epidemiology:
Evidence of Risk and Harm

2
Patients encounter (possibly) risky exposuresPatients encounter (possibly) risky exposures
• Alcohol during pregnancy (fetal risk)
• Electromagnetic fields (cancer risk)
• Vasectomy (prostate cancer risk)
• Oral contraceptives (thromboembolism risk)
• Alcohol during pregnancy (fetal risk)
• Electromagnetic fields (cancer risk)
• Vasectomy (prostate cancer risk)
• Oral contraceptives (thromboembolism risk)

To examine such risksTo examine such risks
• Evaluate validity of data
• Evaluate strength of association between risk and outcome
• Evaluate relevance to particular individuals
• Evaluate validity of data
• Evaluate strength of association between risk and outcome
• Evaluate relevance to particular individuals
3

Most studies of risk are observational studiesMost studies of risk are observational studies
• These studies are nonrandomized
• Need:
• Basic rules of evidence for nonrandomized studies
• Pitfalls to which observational studies are prone
• These studies are nonrandomized
• Need:
• Basic rules of evidence for nonrandomized studies
• Pitfalls to which observational studies are prone
4

Types of observational studiesTypes of observational studies
• Cohort studies
• Case-control studies
• In each case, we need
• Well-defined outcome
• Well-defined exposure
• Clearly identified comparison groups
• Similarity between groups wrt all other factors that might affect the outcome
• Cohort studies
• Case-control studies
• In each case, we need
• Well-defined outcome
• Well-defined exposure
• Clearly identified comparison groups
• Similarity between groups wrt all other factors that might affect the outcome
5

Compare to randomized trialCompare to randomized trial
• Well-defined outcome: Primary endpoint
• Well-defined exposure: Active treatment
• Clearly identified comparison groups: Control group for comparison
• Similarity between groups wrt all other factors that might affect the outcome: Randomization
• Well-defined outcome: Primary endpoint
• Well-defined exposure: Active treatment
• Clearly identified comparison groups: Control group for comparison
• Similarity between groups wrt all other factors that might affect the outcome: Randomization
6

Cohort studiesCohort studies
• Prospective
• Useful when pts cannot be randomized to exposure
• Identify groups of exposed and non-exposed
• Follow forward to determine rate of outcome in each group
• Prospective
• Useful when pts cannot be randomized to exposure
• Identify groups of exposed and non-exposed
• Follow forward to determine rate of outcome in each group
7

Example of question for cohort studyExample of question for cohort study
• Do operating room personnel suffer higher rates of miscarriage than do others?
• Outcome
• Exposure
• Clearly identified comparison groups
• Similarity between groups re outcome
• Do operating room personnel suffer higher rates of miscarriage than do others?
• Outcome
• Exposure
• Clearly identified comparison groups
• Similarity between groups re outcome
8

Problems with cohort studiesProblems with cohort studies
• Primary issue: self-selection to group• Same factors that affect selection might also
affect outcome• Example: relationship of NSAIDs to GI bleeding
• Increased age associated with increased use of NSAIDs
• Increased age associated with increased GI bleeding
• Age here is a “confounding variable”• Document differences
• Adjust for statistically (regression)
• Primary issue: self-selection to group• Same factors that affect selection might also
affect outcome• Example: relationship of NSAIDs to GI bleeding
• Increased age associated with increased use of NSAIDs
• Increased age associated with increased GI bleeding
• Age here is a “confounding variable”• Document differences
• Adjust for statistically (regression)
9
Relative strength of evidence: RCT & CohortRelative strength of evidence: RCT & Cohort
• Can never rule out the presence of unidentified confounders
• A good cohort study requires a great deal of investigator ingenuity
• Identify possible biases
• Document and/or adjust for potential biasing factors
• Thus, cohort studies are inherently less convincing than well-conducted clinical trials
• Can never rule out the presence of unidentified confounders
• A good cohort study requires a great deal of investigator ingenuity
• Identify possible biases
• Document and/or adjust for potential biasing factors
• Thus, cohort studies are inherently less convincing than well-conducted clinical trials
10
Case-control studiesCase-control studies• Retrospective• Useful in assessing risks for very rare outcomes• Useful when time between exposure and risk is
long• in utero exposure to DES, clear-cell adenocarcinoma of the
vagina
• asbestos, mesothelioma
• Identify persons with the outcome of interest (“cases”)
• Identify similar individuals (“controls”) who• do not have outcome
• are similar wrt all other factors associated with outcome
• Compare frequency of exposure between groups
• Retrospective• Useful in assessing risks for very rare outcomes• Useful when time between exposure and risk is
long• in utero exposure to DES, clear-cell adenocarcinoma of the
vagina
• asbestos, mesothelioma
• Identify persons with the outcome of interest (“cases”)
• Identify similar individuals (“controls”) who• do not have outcome
• are similar wrt all other factors associated with outcome
• Compare frequency of exposure between groups11

Example of question for case-control studyExample of question for case-control study
• What exposures predispose to lung cancer?
• Outcome
• Exposure
• Clearly identified comparison groups
• Similarity between groups re outcome
• What exposures predispose to lung cancer?
• Outcome
• Exposure
• Clearly identified comparison groups
• Similarity between groups re outcome
12

Problems with case-control studiesProblems with case-control studies
• Susceptiblity to unmeasured confounders
• Outcome = identified with outcome of interest
• Ascertainment bias
• Exposure = retrospective documentation of exposure
• Recall bias
• Interviewer bias
• Strength of C-C evidence is inherently more limited than cohort study
• Susceptiblity to unmeasured confounders
• Outcome = identified with outcome of interest
• Ascertainment bias
• Exposure = retrospective documentation of exposure
• Recall bias
• Interviewer bias
• Strength of C-C evidence is inherently more limited than cohort study 13

Second primary guide:Second primary guide:
• Were the exposures and outcomes measured in the same way in the groups being compared?
• RCT, cohort: ascertainment of outcome
• Case-control: ascertainment of exposure
• Were the exposures and outcomes measured in the same way in the groups being compared?
• RCT, cohort: ascertainment of outcome
• Case-control: ascertainment of exposure
14

Secondary guidesSecondary guides
• Is the temporal relationship correct?
• Is there a dose-response gradient?
• Is the temporal relationship correct?
• Is there a dose-response gradient?
15

Measuring the association between exposure and outcomeMeasuring the association between exposure and outcome
• Most common and useful: relative risk = p1/p2
• Exposure to encainide was associated with a 2.6-fold elevation in risk of death
• Can obtain relative risk from cohort studies or RCT (prospective)
• Most common and useful: relative risk = p1/p2
• Exposure to encainide was associated with a 2.6-fold elevation in risk of death
• Can obtain relative risk from cohort studies or RCT (prospective)
16

Case-control studies: No RR estimateCase-control studies: No RR estimate
17
• CC studies cannot produce an estimate of the relative risk
• RR = a/(a+b) / c/(c+d)
• OR = a/b / c/d = ad / bc
• When outcome is rare, OR RR
• CC studies cannot produce an estimate of the relative risk
• RR = a/(a+b) / c/(c+d)
• OR = a/b / c/d = ad / bc
• When outcome is rare, OR RR
aa bb
cc dd

18
Assessing applicabilityAssessing applicability
• Recall that the number needed to treat (NNT) depends on the absolute risk difference, not the relative risk
• Need to know something about the prevalence of the bad outcome
• Recall that the number needed to treat (NNT) depends on the absolute risk difference, not the relative risk
• Need to know something about the prevalence of the bad outcome

19
Case ControlCase Control
OR= 3.7p = 0.50OR= 3.7p = 0.50
Exposed
Unexposed
Exposed
Unexposed
Outcome: CC Adeno CAExposure: Maternal SmokingOutcome: CC Adeno CAExposure: Maternal Smoking
77 2121
11 1111
20
Case ControlCase Control
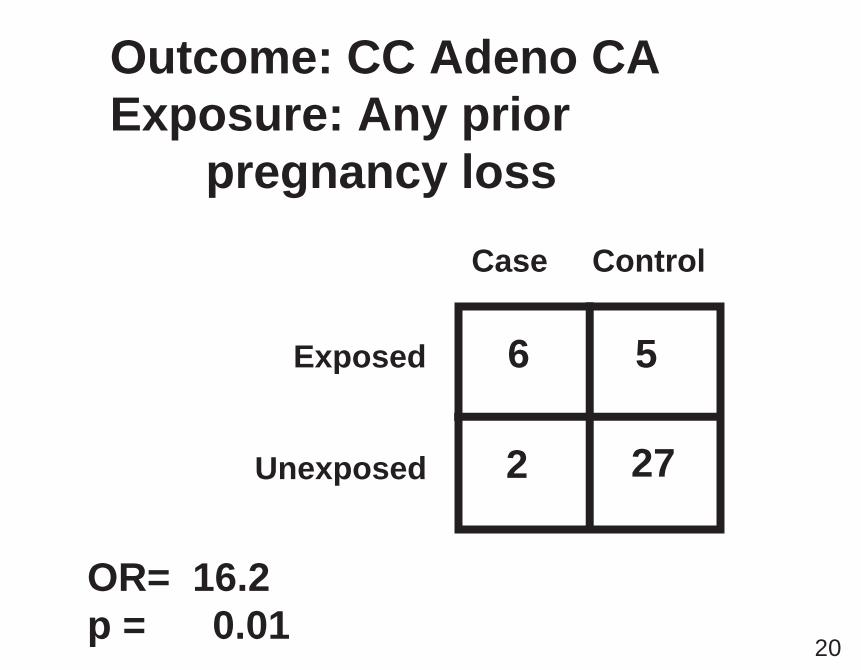
OR= 16.2p = 0.01OR= 16.2p = 0.01
Exposed
Unexposed
Exposed
Unexposed
Outcome: CC Adeno CAExposure: Any prior
pregnancy loss
Outcome: CC Adeno CAExposure: Any prior
pregnancy loss
66 55
22 2727

21
Case ControlCase Control
OR 300-400 p < 0.0001OR 300-400 p < 0.0001
Exposed
Unexposed
Exposed
Unexposed
Outcome: CC Adeno CAExposure: In utero estrogenOutcome: CC Adeno CAExposure: In utero estrogen
77 00
11 3232
Related Documents











