Ghada M.H. Abdel-Salam et al. 391 Clinical, Electroencephalographic (EEG), Neuroradiological and Molecular Correlations in Late-Detected Phenylketonuria (PKU) Patients Ghada M.H. Abdel-Salam 1 , Ann A. Abdel-Kader 4 , Laila Effat 2 , Amr Gouda 3 , Amina Hindawy 5 , Mona A. El-Gammal 1 Departments of Clinical Genetics 1 , Human Molecular Genetics 2 , Biochemical Genetics 3 , Human Genetics and Genome Research Division, National Research Centre, Clinical Neurophysiology 4 , Pediatric 5 , Cairo University ABSTRACT The potential benefits of treating late diagnosed 60 patients with phenylketonuria (PKU) were investigated. Patients subjected to clinical, biochemical, IQ and electroencephalography (EEG) assessment and followed up in correlation with nutritional status. Further, a subset received magnetic resonance imaging (MRI). Screening for six common mutations (IVS10-11>A, R261Q, R252W, Y277D, E221D, V245V) was also performed. Patients were divided into different groups according to the onset of intervening year; imaging and molecular findings and the profiles of these groups were compared. Results showed that higher susceptibility to various patterns of seizures in 21 cases (35%) in the first two years of life however, this incidence decreased with age in spite of the elevated phenylalanine (Phe) level in blood. Alternately, EEG abnormalities increased with advancing age. Those exhibiting white matter abnormalities (WMAs) extending into subcortical/frontal regions (No=5) or WMAs with hypogenesis of corpus callosum (No=5) and or atrophy (No=11), displayed significant impairments in a number of domains. On the other hand patients showed no WMAs (No =10), or pathology restricted to the posterior periventricular region (No=15), displayed mild deficits. The most prevalent mutations were IVS-10-11 G>A (64.3%), and R261Q (35.7 %). The 14 patients characterised (23.3%) were homozygous for the mutations that they carry. This is consistent with the high rate of consanguinity (71.1%) among families with PKU. Unexpectedly, hyperphenylalanemia and mild PKU have been detected in 4 of the patients` mothers. The data of the present study show that dietary restriction could substantially improve the most serious consequences of PKU even for late-diagnosed mentally retarded persons with PKU. (Egypt J. Neurol. Psychiat. Neurosurg., 2005, 42(2): 391-406). INTRODUCTION Phenylketonuria (PKU) is one of the first amino acid metabolic diseases to be characterized and the most common inborn error of amino acid metabolism in Caucasians, with an average incidence of 1/10,000 1 . This autosomal recessive genetic disorder is caused by a deficiency of phenylalanine hydroxylase (PAH) enzyme. PAH is the rate-controlling enzyme of phenylalanine (Phe) homeostasis. In the liver, PAH, which requires tetrahydrobiopterin (BH4) as a cofactor, converts Phe, an essential amino acid, to tyrosine. Thus, Phe accumulates to plasma levels exceeding 1200 μmol/L and low plasma levels of tyrosine. The deficiency of PAH enzyme is caused by mutations in the PAH gene resulting in, intolerance to the dietary intake of Phe and production of the phenylketonuria (PKU) disease 2 . The PAH gene, located at 12q22-q24.1, includes about 90kb and contains 13 exons. The degree of PAH enzyme impairment depends on the nature and position of mutations. To date,

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Ghada M.H. Abdel-Salam et al.
391
Clinical, Electroencephalographic (EEG),
Neuroradiological and Molecular Correlations in
Late-Detected Phenylketonuria (PKU) Patients
Ghada M.H. Abdel-Salam1, Ann A. Abdel-Kader
4, Laila Effat
2,
Amr Gouda3, Amina Hindawy
5, Mona A. El-Gammal
1
Departments of Clinical Genetics1, Human Molecular Genetics
2, Biochemical Genetics
3,
Human Genetics and Genome Research Division, National Research Centre,
Clinical Neurophysiology4, Pediatric
5, Cairo University
ABSTRACT
The potential benefits of treating late diagnosed 60 patients with phenylketonuria (PKU) were investigated.
Patients subjected to clinical, biochemical, IQ and electroencephalography (EEG) assessment and followed up in
correlation with nutritional status. Further, a subset received magnetic resonance imaging (MRI). Screening for
six common mutations (IVS10-11>A, R261Q, R252W, Y277D, E221D, V245V) was also performed. Patients were
divided into different groups according to the onset of intervening year; imaging and molecular findings and the
profiles of these groups were compared. Results showed that higher susceptibility to various patterns of seizures
in 21 cases (35%) in the first two years of life however, this incidence decreased with age in spite of the elevated
phenylalanine (Phe) level in blood. Alternately, EEG abnormalities increased with advancing age. Those
exhibiting white matter abnormalities (WMAs) extending into subcortical/frontal regions (No=5) or WMAs with
hypogenesis of corpus callosum (No=5) and or atrophy (No=11), displayed significant impairments in a number
of domains. On the other hand patients showed no WMAs (No =10), or pathology restricted to the posterior
periventricular region (No=15), displayed mild deficits. The most prevalent mutations were IVS-10-11 G>A
(64.3%), and R261Q (35.7 %). The 14 patients characterised (23.3%) were homozygous for the mutations that
they carry. This is consistent with the high rate of consanguinity (71.1%) among families with PKU. Unexpectedly,
hyperphenylalanemia and mild PKU have been detected in 4 of the patients` mothers. The data of the present
study show that dietary restriction could substantially improve the most serious consequences of PKU even for
late-diagnosed mentally retarded persons with PKU. (Egypt J. Neurol. Psychiat. Neurosurg., 2005, 42(2):
391-406).
INTRODUCTION
Phenylketonuria (PKU) is one of the first
amino acid metabolic diseases to be characterized
and the most common inborn error of amino acid
metabolism in Caucasians, with an average
incidence of 1/10,0001. This autosomal recessive
genetic disorder is caused by a deficiency of
phenylalanine hydroxylase (PAH) enzyme. PAH
is the rate-controlling enzyme of phenylalanine
(Phe) homeostasis. In the liver, PAH, which
requires tetrahydrobiopterin (BH4) as a cofactor,
converts Phe, an essential amino acid, to tyrosine.
Thus, Phe accumulates to plasma levels exceeding
1200 µmol/L and low plasma levels of tyrosine.
The deficiency of PAH enzyme is caused by
mutations in the PAH gene resulting in,
intolerance to the dietary intake of Phe and
production of the phenylketonuria (PKU)
disease2. The PAH gene, located at 12q22-q24.1,
includes about 90kb and contains 13 exons. The
degree of PAH enzyme impairment depends on
the nature and position of mutations. To date,

Egypt J. Neurol. Psychiat. Neurosurg. Vol. 42 (2) – July 2005
392
more than 440 different alterations have been
identified in the PAH gene3. Deletions, insertions,
point mutations, and splicing mutations have been
described. In the Mediterranean region the most
common mutation is IVS10-11G > A4,5
that is
associated with severe phenotype. The number of
possible mutations and the fact that most
individuals are compound heterozygotes account
only in part for the large biochemical and clinical
phenotypic variability seen in PKU patients
ranging from classical PKU to moderate
hyperphenylalaninemia6. It is noteworthy to
mention that, impaired metabolism BH4 leads to
malignant hyperphenylalanemia, which is more
difficult to treat than PKU.
PAH deficiency is a highly heterogeneous
trait that shows a broad spectrum of phenotypes.
Plasma Phe levels of patients who are off-
treatment may be above 1200 mol/L or 20 mg/dl
(‘classical PKU’), between 600 and 1200 mol/L
or 10-20 mg/dl (‘mild PKU’), or below 600
mol/L or 2-10 mg/dl (‘non-PKU
hyperphenylalaninemia’), as compared to levels of
40–120 mol/L or < 2mg/dl in normal persons7,8
.
Timing is everything for children exposed to
elevated levels of phenylalanine. The earliest
possible recognition of disorders so that the early
start of a phenylalanine-restricted diet can prevent
the most serious consequences and the child’s
development will be normal if the diet is adhered
to9. When dietary control is poor or late, PKU
causes severe mental retardation, microcephaly,
epilepsy, spasticity, tremor, clumsiness, and in
some cases occasionally extrapyramidal features,
owing to the damaging effects of
hyperphenylalaninemia on the developing nervous
system10
and effects related to insufficient tyrosine
(fair colour of skin and hair and
neuropsychological deficits). Seizures and
imaging abnormalities in patients with PKU are
consequences of hyperphenylalanemia. However,
It is a curious fact, that this association of PKU
and seizures had scarcely been studied in the
literature, although there have been numerous
short notes or case reports in literatures11,12,13
.
Interestingly, white matter abnormalities (WMAs)
found in PKU patients either early treated or late
treated. The WMAs are thought to represent
elevated water content in the myelin and, possibly,
disturbed myelin synthesis14,15
. They are found
predominantly in the posterior periventricular
cerebral white matter, but in more severe cases
they also extend into anterior and subcortical
regions14,16
. Hypoplasia of the corpus callosum is
a feature of maternal PKU and is probably a result
of inhibition of corpus callosum development at 8
to 20 weeks of gestation17
. Moreover, cerebral
atrophy could be the late result of chronic
exposure to high phenylalanine concentrations18
.
The incidence and severity of WMAs increase
with age, but it seems to be individual variation in
the vulnerability of the brain to blood
phenylalanine levels19
. The clinical significance of
PKU-related WMAs is not known, although there
is some evidence to suggest a possible link
between PKU-related WMAs and cognitive
impairment20
especially WMAs pathology
extending into subcortical and/or frontal regions
are at increased risk for significant
neuropsychological deficits. A raised Phe level
may impair transport into the brain of other large
neutral amino acids that share the same
transporter, including tyrosine and tryptophan,
with resultant alteration in neurotransmitter levels.
Consequently, the neurons of the dopamine-
dependent prefrontal cortex have specific
characteristics, causing this area of the brain to be
particularly sensitive to fluctuations in dopamine
precursor tyrosine and this could be the cause of
neuropsychological deficits found mainly in speed
of information processing and higher integrative
functioning and attention deficit hyperactivity
disorder (ADHD)-inattentive type21
.
The present study thought to determine
seizure, imaging abnormalities and EEG
abnormalities frequency and type in a cohort of
males and females with late treated PKU
according to the intervening year, to examine
further the relationship between WMAs and its
impact on the IQ, and seizure frequency (children
were differentiated according to the severity of
their pathology). More interestingly to present the

Ghada M.H. Abdel-Salam et al.
393
pregnancies outcomes of untreated females with
maternal hyperphenylalanemia and mild PKU and
to present simple correlation between the
genotype of two mutations and the clinical
phenotype
PATIENTS AND METHODS
Sixty cases with typical PKU (serum Phe
level more than 20 mg/dl.) were evaluated. These
patients were diagnosed in our Clinical Genetics
Department from July 1997 through January
2005. Severe learning disability, poor behavior
control, hyperactivity, seizures and delayed
speech development were common presenting
complaints. Moreover, neurological deterioration
and seizures was the complaint of two cases. A
detailed medical history including family history
consanguinity, similarly affected family members
(pedigree), case history of mothers and fathers,
history of the present condition (date of diagnosis,
onset of initiation of low Phe diet) and seizure
type and frequency were obtained for each patient.
Patients were divided into four groups
according to the onset of intervening year: group 1
(started after the age of 6 month but at 1st year of
life; n = 9), group 2 (started at 2nd
year of life; n =
17), group 3 (started from 3 to 6-year-old; n = 27)
and group 4 (started after the age of 6; n=7). All
the 60 cases were subjected to anthropometric
examination (weight, height and head
circumference) and full clinical evaluation with
special emphasis on the neurological assessment
regarding tone, reflexes, Babinski sign, gross
motor function, function of the lower extremities
and fine motor functions.
Biochemical: Blood Phe concentrations for
all the patients were determined by the enzymatic
colourimetric method in dried blood spot
(Quantase). Typical PKU was diagnosed
according to serum phenylalanine (Phe) level
more than 20 mgl/dl. In addition, Phe
concentration were evaluated for 20 mothers who
had more than affected child with PKU,
congenital microcephaly and or congenital heart
disease with PKU.
Diet: Current treatment of PKU consists of a
Phe-restricted diet (well-adjusted to the tolerance)
supplemented with a tyrosine-, vitamin-, and
oligoelement-enriched amino acid mixture or with
a specific formulation high in all the other amino
acids necessary for protein synthesis
EEG was performed for all patients using the
international 10-20 system of electrode placement
with sedation (by chloral hydrate). The length of
the EEG recording was 20 minutes with
hyperventilation in co-operative cases but without
photic stimulation. Further, the previous EEGs
were also reviewed. For each case with epilepsy,
extensive data collection through personal
interview was done by two of the authors
concerning the onset, type, frequency, and
response to treatment. We reviewed 137 EEGs
from 60 patients with PKU. Moreover, EEG was
performed to the 4 mothers who showed elevated
Phe level.
Intelligence quotient and /or
Developmental Quotients (IQ/ DQ): All the
patients were tested using Wechseler test and / or
portage scale for evaluating the developmental
quotient in young patients (up to 5 –year-old). The
degree of mental retardation (MR) was evaluated
according to WHO classification: normal 80,
borderline =70-79, mild = 51-69, moderate = 36-
50, severe = 21-35, profound = 0-20.
CT and /or MRI: These examinations were
performed for 46 patients (76.7%). Mild white
matter abnormalities (WMAs) if confined to the
posterior periventricular region, moderate if
extending into subcortical and/or frontal regions
and sever if associated with hypogenesis of corpus
callosum17,21
. Rating scales were used to grade the
severity of imaging abnormalities. 0 = normal 1 =
mild WMAs, 2 = moderate WMAs, 3 = severe
WMAs, 4 = if WMAs associated with brain
atrophy.
Molecular Study of the PAH Gene
Genomic DNA was isolated from peripheral
blood samples using the salting out procedures as
described by Miller et al22
. Cases were screened
for six mutations (IVS-10-11 G>A, R261Q,

Egypt J. Neurol. Psychiat. Neurosurg. Vol. 42 (2) – July 2005
394
R252W Y277D, E221D and V245V) by
polymerase chain reaction (PCR) of the PAH gene
followed by restriction analysis. This entailed
amplification of the mutation site and its flanking
sequences using specific primers followed by
restriction enzyme cutting within the mutation
sites following the procedure of Eiken et al23
.
Statistical analysis of data, Package for
Social Science (SPSS for Windows Release 6;
SPSS Inc., Chicago, IL, USA) was used. Simple
linear regression (rs) was used to evaluate the
relationship between epilepsy and the degree of
MR, head circumference, height, body weight of
patients at time of assessment. In addition, to
evaluate the relationship between the grades of
MRI abnormalities and the degree of MR, head
circumference, height, and body weight of patients
at time of assessment. Student t-test was used to
compare the means of continuous variables
between different groups. For the evaluation of
categorical variables, Chi square test was used.
All tests were two sided and P values < 0.05 were
considered significant.
RESULTS
General features
This study included sixty cases from 45
families with classic PKU. Age range of the
children was from 6 months to 22 years with the
mean of 5.65±0.67 year. Sex ratio was 0.51 in the
total group. Mean maternal age at the birth of
affected child was 27 ±0.92 years and the mean
paternal age was 32±0.91 years. Parents having 1
child with PKU or 2 and 3 children with PKU
represented 60.8% 28.3% and 10.9%,
respectively, of families surveyed. Four of these
mothers proved to have high Phe level (3 with
hyperphenylalanemia and one with classic PKU).
Mean Z-scores for weight, height and head
circumference of the PKU children were -0.53
SD, -0.92 SD and -1.67 SD, respectively.
Moreover, 20 cases (33.3%) had microcephaly
(head circumference -2 SD). All mothers who
showed high Phe level had microcephalic PKU
patients but none of them had congenital heart
disease. Three cases (5%) with PKU had
associated congenital anomalies in the form of
spina bifida occulta, mitral prolapse and albinoid
fundus. In addition to a unique occurrence of PKU
in a patient with Down syndrome (Fig. 1). An
important finding, consanguinity was documented
in 32 families (71.1%) and our sample included
12 sibships 9 of them from consanguineous
marriage. Calculated sibling recurrence risk for all
the cases was 32.8 % with mean inbreeding
coefficient 0.0630.
Seizures and intelligence
Of the 60 cases with classic PKU, (Table 1)
21 cases (35%) had epilepsy. In this study, there
was higher prevalence of epilepsy in males 66.7%
versus 33.3% in females. Twenty cases had the
age of onset of epilepsy at the first year of life
(95.2%). The main seizure type was generalized
tonic-clonic seizures which was evident in 11
cases (52.4%), however, 3 patients (14.3%) had
west syndrome and 7 (33.3%) cases with focal or
partial seizures. Sixteen cases (76.2%) were well
controlled 2 of them were well controlled only on
diet while the rest (14 cases) on diet and
antiepileptic drugs. On the other hand 5 (23.8%)
had partially controlled seizures.
The IQ of the PKU patients ranged from mild
to profound mental retardation. The mean IQ for
our 60 patients in the study was 47.72.62.
An important finding was the inverse
correlation between the occurrence of epilepsy
and the IQ (rs = -2.5, p=0.01). Meanwhile, no
correlation was observed between the occurrence
of epilepsy and head circumference at time of
assessment of all patients in the study (rs = -0.16,
p=0.3). The body weight, height and biochemical
phenotype of all patients at time of assessment
also inversely correlated with epilepsy (rs = –
0.08, -0.12, – 0.2 and - 0.961, respectively)
however, they did not reach the level of statistical
significance.
As shown in table (1), the number of cases is
limited in different subgroups for a precision
statistical analysis. Group 1 and 2 had higher

Ghada M.H. Abdel-Salam et al.
395
incidence of epilepsy when compared with group
3 and 4, however, the incidence of brain imaging
abnormalities did not show marked difference
between groups (Table 1). In our group of patients
there was minimal effect on the IQ of the timing
of diet onset.
EEG changes
PKU patients who had no history of epilepsy
at any stage of their life showed normal EEGs in
69.2% (27/39) of the cases. Meanwhile, focal
paroxysmal discharge (Fig. 2) and subcortical
epileptogenic dysfunction (fig.3) were seen in 7
(58.3%) and 5 (41.7%) cases respectively. Three
of these cases (3/12; 25%) had normal EEGs in
infancy but abnormal EEGs when retested later
even 2 of them though remain on a relaxed diet.
On the other hand, severe alterations were seen in
epileptic patients. The EEG of patients with
epilepsy (n=21), showed focal spikes, generalized
spikes/waves or mixed. In addition,
hypsarrhythmia (fig. 4) was recognised in 3
patients (14.3%). Group classification showed
higher incidence of EEG abnormalities among
cases in group 3 and 4 compared with group 1 and
2. EEG done for the four mothers who showed
high level of Phe revealed normal pattern. In
epileptic patients with infantile spasm, there was
significant association between the initial EEG
pattern and response to diet and antiepileptic
treatment and between clinical remission and EEG
normalization and long-term seizure control.
MRI findings
The overall incidence of imaging
abnormalities was 78.3% (36/46 cases). Fifteen
patients had pathology restricted to the posterior
periventricular region (mild WMAs) and 5
patients (Fig. 5) had pathology extending into
subcortical and/or frontal regions (moderate
WMAs). White matter abnormalities and thining
of corpus callosum (Fig. 6) were evident in five
cases (severe WMAs). Moreover, one of them had
cerebellar atrophy (Fig. 7). Further 11 cases
showed WMAs and brain atrophy (Fig. 8) and the
remaining 10 patients had no detectable
abnormalities (Table 1).
An important finding was the significant
inverse correlation between the severity of MRI
findings and the IQ ( rs=-2.962 P< 0.005). In the
meantime, there was significant correlation
between the severity of abnormal MRI findings
and occurrence of seizures (rs=3.25; P< 0.002). In
addition, no correlation was observed between the
severity of abnormal MRI findings and age or
biochemical level (p=0.06 and p=0.48,
repectively). These data indicate an association
between severity of MRI findings and occurrence
of seizures and the low IQ values among cases
with PKU.
Next step in our data analyses involved
grouping of the cases according to the type of
brain abnormalities and comparing them with
cases with no detectable brain abnormalities
(Table 2). Cases with mild, moderate and severe
brain abnormalities showed decrease in the IQ
values when compared with cases with no
detectable brain abnormalities, although it was
significant in the groups that showed severe white
matter abnormalities and group with brain
atrophy. Further, group with moderate and severe
white matter abnormalities showed significant
decrease in the head circumference but increase in
the incidence of seizures.
Therapy and prognosis
All PKU patients were treated with low phe
diet immediately after the diagnosis of PKU was
established. It was a major challenge because
most of these cases who never have been exposed
to the relatively unpalatable Phe-free medical
product essential for metabolic control. With the
start of diet two patients (9.5%) who received
only diet therapy were seizures free without any
antiepileptic drugs (AEDs). On the other hand, 14
(66.7%) patients who received a combination of
low phe diet therapy and AEDs (valproate and/or
nitrazepam) ceased to show seizures within 9
months after initiating the therapy and only two
patients relapsed. While, 5 patients (23.8%)
showed partial control.
In group 1, 2 and 3, the hyperactivity and
autistic behavior was gradually decreased when

Egypt J. Neurol. Psychiat. Neurosurg. Vol. 42 (2) – July 2005
396
serum phe concentrations dropped to 6 mg/dl or
below even 11 patients (20.7%) showed
intellectual improvement after diet therapy. In
group 4, patients failed to adhere to diet.
Hyperactivity, aggression and autistic behavior
were marked but showed some improvement on
valporates and risperidone.
Biochemical phenotype:
The mean Phe level of the patients ranged
from 20 to 36 mg/dl with the mean of 24.81.3
mg/dl. The mean of Phe level among groups is
presented in table1. An important finding was
high Phe level found in 4 of the PKU mothers
(4/20; 20%). One of them had mild PKU (15
mg/dl) while the others had hyperphenylalanemia
(6 mg/dl). This could partially explain the high
sibling recurrence risk.
Mutation screening in correlation to clinical
and biochemical phenotype.
Screening for six mutations (IVS10-11>A,
R261Q, R252W, Y277D, E221D, V245V) that
are relatively common in this geographical area
allowed the characterization of 23.3% (14 cases)
of cases. 64.3% of the mutant alleles are IVS10-
11>A (9 cases). Only 35.7% alleles were R261Q
(5 cases). However, other mutations were
(R252W, Y277D, E221D, V245V) not detected.
The biochemical phenotype of the 14 patients
with the two mutations did not differ significantly
(Table 2). It was noted that 19.04% of epileptic
patients (4 cases) were harboring IVS10-11>A
mutation in contrast to 4.8% (one case) that
showed R261Q. None of these cases had west
syndrome. Of 14 patients with homozygous
IVS10-11>A alleles and R261Q mutations, 19.4%
(7/36) versus 5.5%(2/36) exhibited brain imaging
abnormalities, respectively. In the former group,
one patient showed partially controlled seizures
(33.3%). The mean IQ of IVS10-11>A patients
was significantly lower than those who had
R261Q (41.9 5.5 vs 61 5.8) p =0.02.
However, one patient with IVS10-11>A (1/11;
9.1%) showed intellectual improvement after diet
therapy. Alternately, one of the patients with
R261Q did not show any intellectual improvement
although diet intervening was earlier than the
IVS10-11>A patient.
Table 1. Characteristics of patients with PKU according to the subgroup classification.
Group 1
(n=9)
1year
Group 2
(n=17)
2-3 year
Group 3
(n=27)
3-6 year
Group 4
(n=7)
>6 year
Total
Age (years) 3.5 1.3 3.91.1 5.80.9 11.72 5.60.7
Sex ratio (M/M+F) 0.55 0.5 0.5 0.7 0.51
Phenylalanine level (mg/dl) 25.62.3 20.61.4 25.81.9 27.96.5 24.31.1
IQ 50.78 53.65.6 46.53.4 37.35.9 47.72.6
Weight (SD) -0.80.3 -0.010.5 -0.80.2 -0.50.4 -0.50.2
Height (SD) -1.20.6 -0.70.3 -0.90.2 -1.10.4 -0.90.2
Head circumference (SD) -1.40.4 -1.50.3 -1.90.2 -1.40.6 -1.70.2
Epilepsy (%) 4 (44.4%) 9 (52.9%) 7 (25.9%) 1 (14.3%) 21 (35%)
Abnormal EEG (%) - - 8/20 (40%) 4/6 (66.7%) 12/39 (30.8%)
MRI abnormalities (%)**** 6/7 (85.7%) 8/12 (66.7%) 16/21(76.2%) 6/6 (100%) 36/46 (78.3%)
White matter abnormalities (No) 5 6 14 - 25/36 (69.4%)
Atrophic changes (No) 1 2 2 6 11/36 (30.6%)
No. of cases with IVS10-A G - 1 6 2 9
No. of cases with R261Q - 3 1 1 5
* Incidence of epilepsy was significant statistically when compared with group 1 and 2 (P= 0.048 and 0.029, respectively)

Ghada M.H. Abdel-Salam et al.
397
Table 2. Characteristics of PKU patients with brain imaging abnormalities compared with those having no
brain imaging abnormalities.
Patients with
no brain
abnormalities
(No= 10)
Patients with
mild
WMAs
(No= 15)
Patients with
moderate
WMAs
(No= 5)
Patients with
severe
WMAs
(No= 5)
Patients with
brain
atrophy
(No= 11)
Age (years) 5.7 5.2 2.2 4.04 7
Weight (SD) 0.4 -0.6 -0.8 -0.2 -0.5
Height (SD) 0.1 -1.1* -1.4* -1.4* -0.9*
Head circumference (SD) -1.1 -1.6 -2.4* -2.2* -1.01
Phe level (mg/dl) 23.8 24.3 26.7 25.7 26
IQ 60 48.9 46.6 34* 33.6*
Seizures (no; %) - 6 (40%) 4 (80%)** 4 (80%)** 5 (45%)
Patients with no brain abnormalities were taken as referent in the statistical analysis.
* P< 0.05 ** P< 0.005
Table 3. Characteristics of patients with PKU according to the mutation type.
IVS10-11>A
(No= 9)
R261Q
(No= 5)
P value
Age (years) 5.3 12 0.12
Sex ratio (M/M+F) 0.55 0.4 1
Epilepsy (%) 4 (19.04%) 1 (4.8%) 0.6
Abnormal EEG (%) 2 (16.7%) - -
MRI abnormalities (%) 8 (22.2%) 2(5.6%) 1
Phenylalanine level (mg/dl) 25.61.7 230.6 0.2
IQ 41.95.5 615.8 0.02*
Weight (SD) -0.531.4 -0.20.2 0.4
Height (SD) -0.980.3 -0.10.4 0.09
Head circumference (SD) -1.90.43 -0.40.5 0.04*
Mild WMAs (No. of cases) 6 1 -
Moderate WMAs (No. of cases) 1 1 -
Severe WMAs (No. of cases) 1 - -
Atrophic changes (No. of cases) - -
Fig. (1): Facial picture of Egyptian
patient with classic PKU and the
unique association with Down
syndrome.

Egypt J. Neurol. Psychiat. Neurosurg. Vol. 42 (2) – July 2005
398
Fig. (2): EEG in classic PKU girl aged 3-year old showing frequent focal sharp waves over either fronto-
temporal regions. Background activity of 3-6C/s delta waves and sleep spindles.
Fig. (3): EEG in classic 1.5-year old boy with PKU showing 3-6 C/sec delta and theta waves mixed with
sleep spindles. There were recurrent periodic paroxysms of sharp and notched slow waves suggesting
subcortical epileptogenic dysfunction

Ghada M.H. Abdel-Salam et al.
399
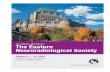
Fig. (4): EEG in classic 6-month- old girl with hypsarrhythmia.
Fig. (5): Flair axial T2 MRI showing abnormal high signal intensity in the deep white matter region
around anterior and posterior horns and the body of both lateral ventricles (grade 2).

Egypt J. Neurol. Psychiat. Neurosurg. Vol. 42 (2) – July 2005
400
Fig. (6): (A) axial T2 weighted MRI showing abnormal high signal intensity in the deep white matter region around
anterior and posterior horns and the body of both lateral ventricles (B) Mid sagittal MRI view of brain; note thining of
corpus callosum (grade 3).
Fig. (7): A) axial T2 weighted MRI showing abnormal high signal intensity in the deep white matter region around the
body and posterior horns of lateral ventricles (B) Coronal MRI showing high signal intensity in the deep white matter
region around anterior horns of both lateral ventricles (c) Mid sagittal MRI view of brain; note agenesis of corpus
callosum and vermal atrophy (grade 3).
Fig. (8): A) axial T1 weighted MRI showing abnormal high signal intensity in the deep white matter region
around anterior and posterior horns and the body of both lateral ventricles and brain atrophy (B) Mid sagittal
MRI view of brain; note agenesis of corpus callosum (grade 4).

Ghada M.H. Abdel-Salam et al.
401
DISCUSSION
In this study we investigated the impact of
late diagnosed PKU-patients on the occurrence of
epilepsy, EEG changes and brain imaging
abnormalities that might be sensitive to long-term
elevation of phenylalanine levels and correlating
these findings to the mutations screened.
The incidence of epilepsy observed in this
study was 35% on 60 Egyptian patients with PKU
compared to 25.5% recorded in 603 Chinese
patients with PKU24
. This apparent slightly higher
incidence may be attributed to the number of the
tested samples. It is rather difficult to classify
epilepsy (secondary to metabolic disorders) into
precise epileptic syndromes. However, the
association of west syndrome with PKU has long
been recognised in literatures since Low et al.’s
first report in 195713,25
. Similar frequency of west
syndrome was 14.3% among our cases in contrast
to 12.3% reported by Zhongshu et al.13
.
By differentiating our 60 cases into four
groups according to the intervening year, (despite
the variation among individuals within these
groups) certain conclusions are apparent. PKU
patients showed higher incidence of epilepsy in
the first year of life and this finding is consistent
with the literature26
. In addition, this incidence
decreases with age in spite of the elevated Phe
level in blood. On the other hand, older non-
epileptic patients (in group 3 and 4) were more
likely to have abnormal EEGs. In another word no
one of the non epileptic patients in group 1 and 2
had abnormal EEGs before the age of 3 had
abnormal records. This observation had also been
reported in prospective studies of PKU 24,27,28,29
.
So it is most likely that EEG abnormalities
increased with advancing age independently of
MRI abnormalities and showed no relation to IQ
development28
.
Given the ongoing debate about the clinical
importance of WMAs and whether it affects the
cognitive function, we were particularly surprised
that our sample of late-detected PKU patients
showed lower incidence (78.3%) of white matter
abnormalities (WMAs) than that reported in early
treated PKU samples20,30,31
. However, the age
distribution of our sample was significantly
younger. It is noteworthy to mention that
Anderson et al.21
reported on similar incidence of
WMAs (81.3%) in his sample and regarded that to
the same reason. So, it seems likely that the
incidence of WMAs increase with advancing
age19
. Taking into consideration that the regional
distribution of the WMAs does not seem to be age
dependent as infants and adults show the same
regional distribution pattern or related to the
intervening time as it is found in early, late, and
untreated patients17
. Children without detectable
WMAs also displayed deficits but better in the
mean of IQ, head circumference values and
incidence of seizures when compared with cases
with brain abnormalities. Further, our results
showed that the severity of brain abnormality (the
extent of MRI abnormalities) was most strongly
associated with low IQ values but not to the blood
Phe concentration at the time of imaging. This
finding strongly supports hypothesis of Anderson
et al21
. In addition, not only WMAs, that extend
beyond the posterior periventricular region but
also hypoplasia of corpus callosum may adversely
affect IQ.
In view of the results that no relationship had
been found between occurrence of epilepsy and
severity of brain lesion and level of serum Phe, it
is interesting to confirm the same results obtained
from recent study by Brumm et al.32
.
Nevertheless, this is not a universal finding as
many previous studies showed significant
relationship to serum Phe level7,13,33,34
.
Confirming results from previous study35
that
the most common mutations in Egypt are the
IVS10-11G>A and R261Q and comparing our
results with reported mutations. These mutations
include R408W in China, Eastern Europe, East
Russia, Germany and Brazil, R413P in Japan,
IVS10-11G>A in the Mediterranean and Iran,
IVS12→1G>A in Denmark and England, Y414C
in Scandinavia, I65T in Western Europe3,4,36-40
. In
addition, R261Q is common mutation in Brazil,
Iran, Sicily, France, Netherlands, Cuba and South

Egypt J. Neurol. Psychiat. Neurosurg. Vol. 42 (2) – July 2005
402
Italy. Moreover, R252 was reported as a common
mutation in Italy, Iran, Chile, Brazil, Portugal3,4,36-40
.
After the identification of mutations in 23.3%
of our patients the interest lies in the elucidation
of the clinical phenotype underlying these
mutations. IVS10-11G>A mutation correspond to
the category of second most frequently reported in
all populations especially Mediterranean
populations5. Nine cases (15%) were homozygous
for this mutation. Further, 5 cases (8.3%) were
homozygous for R261Q mutation. Generally,
PKU has been cited as an example of
conformational disease in which the increase in
degradation of folding intermediates and
improperly folded proteins is the main molecular
mechanism. IVS10-11G>A mutation had a
putative folding defect that showed no residual
effect of the PHE and that explains that it is
considered as severe mutation. On the other hand
R261Q are folding defects as well but it is
associated with low-intermediate levels of activity
(10–70%)5. R261Q causes reduced stability and
accelerated degradation.
Based on the results obtained in this work,
patients with IVS10-11G>A showed significant
lower IQ values, smaller head circumference
higher incidence of imaging abnormalities and
epilepsy with bad response to AEDs and diet
control when compared with cases with R261Q.
In view of these results obtained, it is interesting
to confirm that the clinical impact of the mutations
corresponds to the severity estimated by Pey et
al5. Although this observation is interesting, but it
shouldn’t be taken as a hard evidence because the
number of children in this sample was small. In
addition, late treated PKU patients do not have IQ
scores fully concordant with the predicted severity
of the PAH genotype41
and close correlation
between its metrical value in PKU subjects and
the PAH genotype requires cautious interpretation
and needs further research. It is noteworthy to
mention, it was suggested that R408W mutation
that cause no residual effect of the PHE (similar to
IVS10-11G>A) predispose to mental illness42,43
.
One of the major questions remaining in PKU
research is why cases who share the same
mutations IVS10-11>A in the phenylalanine
hydroxylase (PAH) gene had different disease
courses as regard to occurrence of seizures or not,
type of seizures and response to dietary treatment
and outcome. We suppose that in IVS10-11>A
mutation, the differences in the courses of the
disease between cases appear to be related to
variations in their blood-brain barriers and
suggesting that there is not a simple correlation
between genotype and intellectual phenotype44
.
Alternately, variation in cases with R261Q
mutation could be regarded to individual variation
in the quality control system5.
Hoping for complete characterization of
PKU mutations in Egypt so, reasonable
predictions of the phenotype of a large number of
patients may be deduced. The homozygosity for
the mutation is due to the high rate of
consanguineous marriages in the family (71.1%)
of the patients. Although this was a preliminary
study on the analysis of PKU in Egypt, but the
data obtained could be used as a base for further
investigation of the disease in this population.
Another interesting observation was that
39.2% of the mothers have more than one affected
child with PKU which attracted our attention to
determine the blood Phe level for these mothers
and to our surprise that 3 of them had non-PKU
mild hyperphenylalaninemia and another one had
mild PKU. A particular question is whether
maternal non-PKU mild hyperphenylalaninemia
(MHP) presented a threat to the fetus.
Retrospective international survey of untreated
maternal MHP concluded that this entity did not
have serious consequences for the fetus, although
the birth measurements and IQ scores were
slightly lower in offspring when maternal blood
Phe was > 400 µmol/l and these authors found at
least 30% of those infants were identified to have
hyperphenylalanemia45
. Unexpectedly, our series
comprised six children with classic PKU (rather
than hyperphenylalaninemia) born to 4 mothers 3
of them with HPA and the other with classic PKU.
This could be regarded to the additive deleterious
effect of consanguinity. This finding shows that
although the inheritance of the mutant genotype is
recessive, PKU is a complex trait.

Ghada M.H. Abdel-Salam et al.
403
Confirming the impact of high blood Phe on
brain growth, all these sibs had congenital
microcephaly, white matter abnormalities and
hypogenesis of corpus callosum and low IQ
values but none of them had congenital heart
disease. Nevertheless, hypoplastic corpus
callosum could be a marker for brain effect in
maternal hyperphenylalaninemia. Although there
is not an established precise relationship between
maternal phe levels and outcome46
. Women with
HPA need early identification, education
regarding the importance of dietary compliance,
careful monitoring, and emotional support to
increase the chance for a better outcome.
Given heterozygote frequency of 1:50 to 1:70 47
, several mechanisms have been proposed to
explain the relatively high PKU frequency in
humans including founder effect/genetic drift,
selective advantage of heterozygotes, reproductive
compensation, high mutational rate, and
involvement of multiple loci that give rise to
similar disease phenotypes48
. Down syndrome
(Trisomy 21) is the most prevalent unbalanced
chromosomal aberration with an incidence of
1:600 live birth or 1: 150 conception49
. Our series
comprised another unique association of PKU and
Down syndrome. The association of these two
rare conditions could be due to random
association of the two syndromes. It is noteworthy
to mention that PKU has been reported in
association with Goldenhar's syndrome50
.
In conclusion, the high incidence of seizure
in first two years of life is due to high Phe level
whereas it is well controlled on diet and AEDs.
While the abnormal EEG and MRI changes are
secondary to the chronic exposure to high Phe.
Although, Phe levels were not correlated with
severity of the MRI abnormalities, incidence of
seizures or IQ values but indeed lifetime Phe were
associated with deficits in several aspects.
Accordingly, seizures, EEG and /or MRI and
neurological manifestation are at least partially
reversible by lowering the blood Phe
concentration at any age especially before the age
of 6 year old. Based on this results patients with
IVS10-11G>A showed significant lower IQ
values, smaller head circumference higher
incidence of imaging abnormalities and seizure
with bad response to AEDs and diet control when
compared with cases with R261Q.
It is very important to carry out neonatal
screening program in Egypt for prevention of
PKU and reducing the burden of disease.
Laboratory testing is only availability of testing to
all individuals. Education regarding the program,
effectiveness of low Phe diet, long-term benefits
both for individuals and society, ethical issues,
and cost benefits has to be cleared.
REFERENCES 1. Cederbaum S, 2002: Phenylketonuria: an update.
Curr. Opin. Pediatr.; 14:702–6.
2. Vallian S, Barahimi E, Moeini H, 2003:
Phenylketonuria in Iranian population: A study in
institutions for mentally retarded in Isfahan.
Mutat. Res.;15:45-52.
3. Santana da Silva LC, Carvalho TS, da Silva FB,
Morari L, Fachel AA, Pires R, et al, 2003:
Molecular characterization of phenylketonuria in
South Brazil. Mol Genet. Metab. ;79:17-24.
4. Zschocke J, 2003: Phenylketonuria mutations in
Europe. Hum. Mutat.;21:345-56.
5. Pey AL, Desviat LR, Gámez A, Ugarte M, Pérez
B, 2003: Phenylketonuria: genotype-phenotype
correlations based on expression analysis of
structural and functional mutations in PAH. Hum.
Mutat.; 21:370-8.
6. Burgard P, Bremer HJ, Buhrdel P, Clemens PC,
Monch E, Przyrembel H, et al, 1999: Rationale
for the German recommendations for
phenylalanine level control in phenylketonuria
1997. Eur.J.Pediatr.;158: 46–54.
7. Weglage J, Pietsch M, Fünders B, Koch H,
Ullrich K, 1996: Deficits in selective and
sustained attention processes in early treated
children with phenylketonuria result of impaired
frontal lobe function. Eur.J.Pediatr; 155: 200–
204.
8. Koch R, Levy HL, Matalon R, Rouse B, Hanley
WB, et al, 1994: The international collaborative
study of maternal phenylketonuria: Status report
1994. Acta Paediatr.;407 (Suppl): 111–119.
9. Antshel KM, Waisbren SE, 2003: Timing is
everything: executive functions in children
exposed to elevated levels of phenylalanine.
Neuropsychology.;17:458-68.

Egypt J. Neurol. Psychiat. Neurosurg. Vol. 42 (2) – July 2005
404
10. Huttenlocher PR, 2000: The neuropathology of
phenylketonuria: human and animal studies.
Eur.J.Pediatr;159 (Suppl 2):S102–S106.
11. Watanabe K, 1998: West syndrome: etiological
and prognostic aspects. Brain Dev.; 20:1-8.
12. Mikaeloff Y, Plouin P, Dhondt J-L, Ponsot G,
Dulac O, 2000:Clinical and EEG video-
polygraphic features of epileptic spasms in a child
with dihydropteridine reductase deficiency.
Efficiency of hydrocortisone. Epileptic
Disord.;2:213-217.
13. Zhongshu Z, Weiming Y, Yukio F, Cheng-
(L)Ning Z, Zhixinga W, 2001: Clinical analysis of
West syndrome associated with phenylketonuria.
Brain Dev.;23: 552-557.
14. Pietz J, 1998: Neurological aspects of adult
phenylketonuria. Curr. Opin Neurol.; 11:679-88.
15. Cleary MA, Walter JH, Wraith JE, Jenkins JP,
Alani SM, Tyler K, et al, 1994: Magnetic
resonance imaging of the brain in
phenylketonuria. Lancet; 344: 87-90.
16. Kahler SG, Fahey MC, 2003: Metabolic
Disorders and Mental Retardation. Am. J. Med.
Genet.; 117C: 31-41.
17. Levy HL, Waisbren SE, Lobbregt D, Allred E,
Leviton A, Koch R, et al, 1996: Maternal non-
phenylketonuric mild hyperphenylalaninemia.
Eur.J.Pediatr.; 155(Suppl.1): S20-5.
18. Leuzzi V, Trasimeni G, Gualdi GF, Antonozzi I,
1995: Biochemical, clinical and neuroradiological
(MRI) correlations in late-detected PKU patients.
J. Inherit. Metab. Dis.; 18: 624-34.
19. Weglage J, Bick U, Schuierer G, Pietsch M,
Sprinz A, Zab R, et al, 1997: Progression of
cerebral white matter abnormalities in early-
treated patients with phenylketonuria during
adolescence. Neuropediatrics; 28: 239-240.
20. Pietz J, Meyding-Lamade U, Schmidt H, 1996:
Magnetic resonance imaging of the brain in
adolescents with phenylketonuria and in one case
of 6-pyruvoyl tetrahydropteridine synthase
deficiency. Eur. J. Pediatr.; 155 (Suppl. 1): 69–
73.
21. Anderson PJ, Wood SJ, Coleman L, Warwick L,
Casanelia S, Anderson VA et al, 2004:
Neuropsychological functioning in children with
early-treated phenylketonuria: impact of white
matter abnormalities. Dev. Med. Child Neurol.,
46: 230–238
22. Miller SA, Dykes DD, Polesky HF, 1988: A
simple salting out procedure for extracting DNA
from human nucleated cells. Nucleic Acids Res.;
16: 1215-1219.
23. Eiken HG, Knappskog PM, Apold J, 1993:
Restriction enzyme-based assays for complete
genotyping of phenylketonuria patients. Dev.
Brain Dysfunction; 6: 53-59.
24. Yu WM, Xu L, Li XW, He C, Shen M, Zhang
ZX, et al, 2003: An eighteen-year study on
phenylketonuria. Zhongguo Yi Xue Ke Xue Yuan
Xue Bao.; 25: 218-22 (Article in Chinese).
25. Low NL, Bosma JF, Armstrong MD, 1957:
Studies on phenylketonuria. Arch Neurol.
Psychiatry; 77: 359.
26. Vigevano F and Bartuli A, 2002: Infantile
epileptic syndromes and metabolic etiologies. J.
Child. Neurol.; 17: 3S9-3S14.
27. Gross PT, Berlow S, Schuett VE, Fariello RG,
1981: EEG in phenylketonuria. Attempt to
establish clinical importance of EEG changes.
Arch. Neurol.; 38: 122-6.
28. Pietz J, Benninger C, Schmidt H, Scheffner D,
Bickel H, 1988: Long-term development of
intelligence (IQ) and EEG in 34 children with
phenylketonuria treated early. Eur. J. Pediatr.;
147: 361-7.
29. Zhang SX, Yu WM, Wang GZ, et al, 1995: An
electroencephalogram analysis of 94 PKU
patients. J. Clin. Electroencephalogr; 4: 139–141
(in Chinese).
30. Bick U, Fahrendorf G, Ludolph A, Vassallo P,
Weglage J, Ullrich K, 1991: Disturbed
myelination in patients with
hyperphenylalaninaemia: evaluation with
magnetic resonance imaging. Eur.J. Pediatr.; 150:
185-189.
31. Thompson A, Tillotson S, Smith I, Kendall B,
Moore S, Brenton D, 1993: Brain MRI changes in
phenylketonuria: associations with dietary status.
Brain; 116: 811-821.
32. Brumm VL, Azen C, Moats RA, Stern AM,
Broomand C, Nelson MD, et al, 2004:
Neurophysiological outcome of subjects
participating in the PKU adult collaborative
study: A preliminary review. J. Inherit. Metab.
Dis.; 27: 549-566.
33. Diamond A, Prevor MB, Callender G, Druin
DP,1997: Prefrontal cortex cognitive deficits in
children treated early and continuously for PKU.
Monogr. Soc. Res. Child. Dev.; 62: 1-208.
34. Griffiths P, Campbell R, Robinson R, 1998:
Executive function in treated phenylketonuria as
measured by the one-back and twoback versions
of the continuous performance test. J. Inherit.
Metab. Dis.; 21: 125-135.

Ghada M.H. Abdel-Salam et al.
405
35. Effat L, Kuzmin A, Kasem N, Meguid NA, Kotb
S, Eisensmith RC, et al, 1999: Haplotypes and
mutations of PAH locus in Egyptian families with
PKU. Eur J. Hum. Genet.; 7: 259-262.
36. Sueoka H, Nagao M, Chiba S, 2000: Rapid
mutation screening of phenylketonuria by
polymerase chain reaction-linked restriction
enzyme assay and direct sequence of the
phenylalanine hydroxylase gene: clinical
application in northern Japan and northern China.
Gene. Test; 4: 249-56.
37. Sueoka H, Moshinetsky A, Nagao M, Chiba S,
1999: Mutation screening of phenylketonuria in
the Far East of Russia. J. Hum. Genet.; 44: 368-
71.
38. Dianzani I, S. Giannattasio, L. de Sanctis, C.
Alliaudi, P. Lattanzio, C.D. Vici, A. et al, 1995:
Characterization of phenylketonuria alleles in the
Italian population, Eur. J. Hum. Genet.; 3: 294-
302.
39. Desviat LR, Perez B, Gutierrez E, Sanchez A,
Barrios B, Ugarte M, 2001: Molecular basis of
phenylketonuria in Cuba. Hum. Mutat.; 18: 252.
40. Vallian S, Barahimi E, Moeini H, 2003:
Phenylketonuria in Iranian population: A study in
institutions for mentally retarded in Isfahan.
Mutat. Res.; 15: 45-52.
41. Ramus SJ, Forrest SM, Pitt DB, Saleeba JA,
Cotton RGH, 1993: Comparison of genotype and
intellectual phenotype in untreated PKU patients.
J. Med. Genet.; 30: 401-405
42. Aulehla-Scholz C, Heilbronner H, 2003:
Mutational spectrum in German patients with
phenylalanine hydroxylase deficiency. Hum.
Mutat.; 21: 399-400.
43. Schuler A, Sowogyi C, Toros I, et al, 1996: 20
years of experience with phenylketonuria in
Hungary. Int. Pediatr.; 114–117.
44. Gizewska M, Cabalska B, Cyrytowski L, Nowacki
P, Zekanowski C, Walczak M, et al, 2003:
Different presentations of late-detected
phenylketonuria in two brothers with the same
R408W/R111X genotype in the PAH gene. J.
Intellect. Disabil. Res.; 47: 146-52.
45. Levy HL, Waisbren SE, Güttler F, Hanley WB,
Matalon R, Rouse B, et al, 2003: Pregnancy
Experiences in the Woman With Mild
Hyperphenylalaninemia. Pediatrics; 112: 1548-
1552.
46. Allen RJ, Brunberg J, Schwartz E, Schaefer AM,
Jackson G, 1994: MRI characterization of
cerebral dysgenesis in maternal PKU. Acta
Paediatr.; 407: 83-5.
47. Scriver CR, Kaufman S, 2001:
Hyperphenylalaninaemia: Phenylalanine
hydroxylase deficiency, In The Metabolic and
Molecular Bases of Inherited Disease. Scriver CR,
Beaudet AL, Sly WS, Valle D, Kinzler K.E.,
Vogelstem B. (eds.), eighth ed. New York:
McGraw-Hill, pp. 1667-1724.
48. Eisensmith RC, Woo SL, 1995: Molecular
genetics of phenylketonuria: from molecular
anthropology to gene therapy. Adv. Genet.; 32:
199-271.
49. James S, Pogribna M, Pogribny I, Melnyke S,
Hine RJ, Gibson JB, et al, 1999: Abnormal folate
metabolism and mutation in the
methyltetrahydrofolate reductase gene may be
maternal risk factor for Down syndrome. Am. J.
Clin. Nutr.; 70: 495-501.
50. Tokatli A, Coskun T, Kocabas CN, Ozalp I, Balci
S, 1994: Classical phenylketonuria associated
with Goldenhar's syndrome. A case report. Turk.
J. Pediatr.; 36: 153-6.

Egypt J. Neurol. Psychiat. Neurosurg. Vol. 42 (2) – July 2005
406
الملخص العزبى
االشعة التشخيصية والبيىلىجيب الىراثية الجزيئية, رسم المخ الكهزببئى ,اإلكلينيكيةالظىاهز
متأخزاوعالقتهب بمزضى الفينيل كيتىنىريب الذين بدؤا العالج
1
3521
23.3IVS-10-11 G>A 64.3R261Q35.771.1
Related Documents