Clinical Controversies in Endometriosis American Society of Reproductive Medicine Baltimore, Maryland October 21, 2015 D an C. Martin, M.D. Interim Director Gynecology Director Minimally Invasive Surgery Director Reproductive Endocrinology and Infertility Department of Obstetrics and Gynecology University of Tennessee Health Science Center Memphis, Tennessee 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Clinical Controversies in
EndometriosisAmerican Society of Reproductive Medicine
Baltimore, Maryland
October 21, 2015
Dan C. Martin, M.D.Interim Director Gynecology
Director Minimally Invasive Surgery
Director Reproductive Endocrinology and Infertility
Department of Obstetrics and Gynecology
University of Tennessee Health Science Center
Memphis, Tennessee
1
Disclaimer
Abbvie – Consultant on a new product not to be
discussed today.
Subject matter expert for Epic EHR for Baptist Memorial
Health Care Corporation
------------------------------------------------
Please confirm that you have the right to use copy
righted material.
Permission to use slides from
The Laparoscopic Appearance of Endometriosis
http://www.danmartinmd.com/files/coloratlas1990.pdf
is on page iii of the PDF
2
Subjects
Classical Appearance
Laparoscopic Appearances
Histology
Why biopsy?
Empirical therapy
Intentional delayed diagnosis
Is mild endometriosis a disease?
3
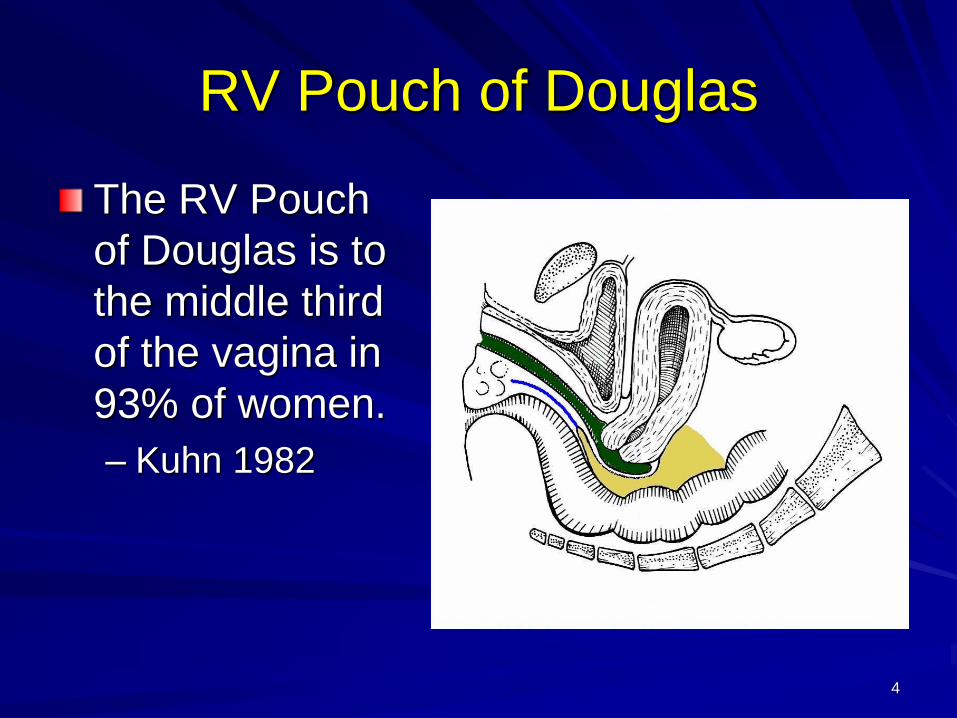
RV Pouch of Douglas
The RV Pouch
of Douglas is to
the middle third
of the vagina in
93% of women.
– Kuhn 1982
4
5
Greek Architecture Slide
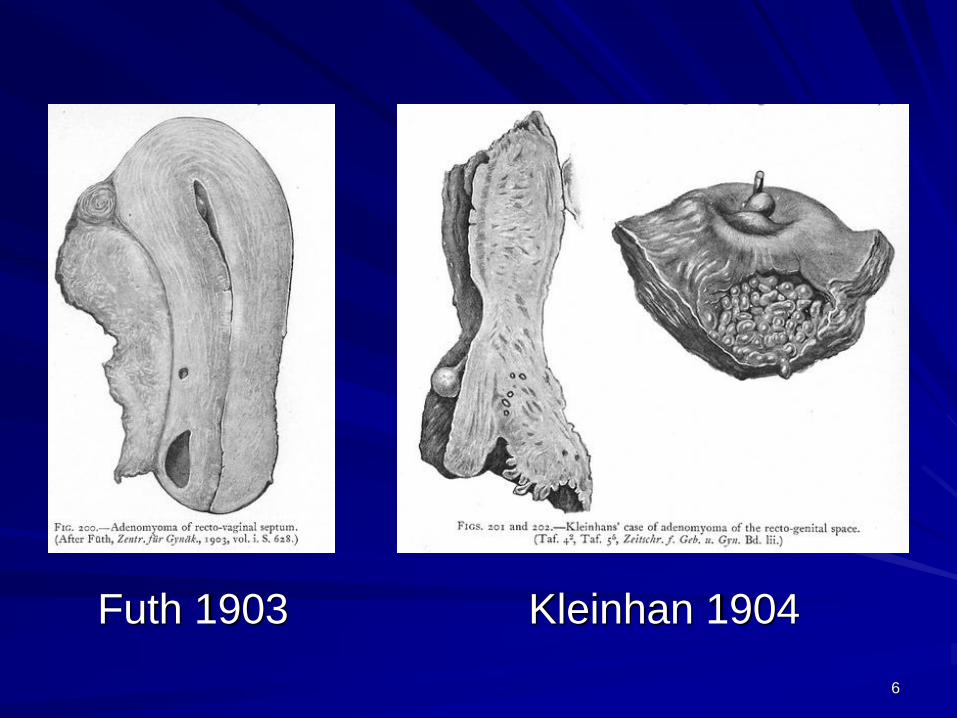
Kleinhan 1904Futh 1903
6
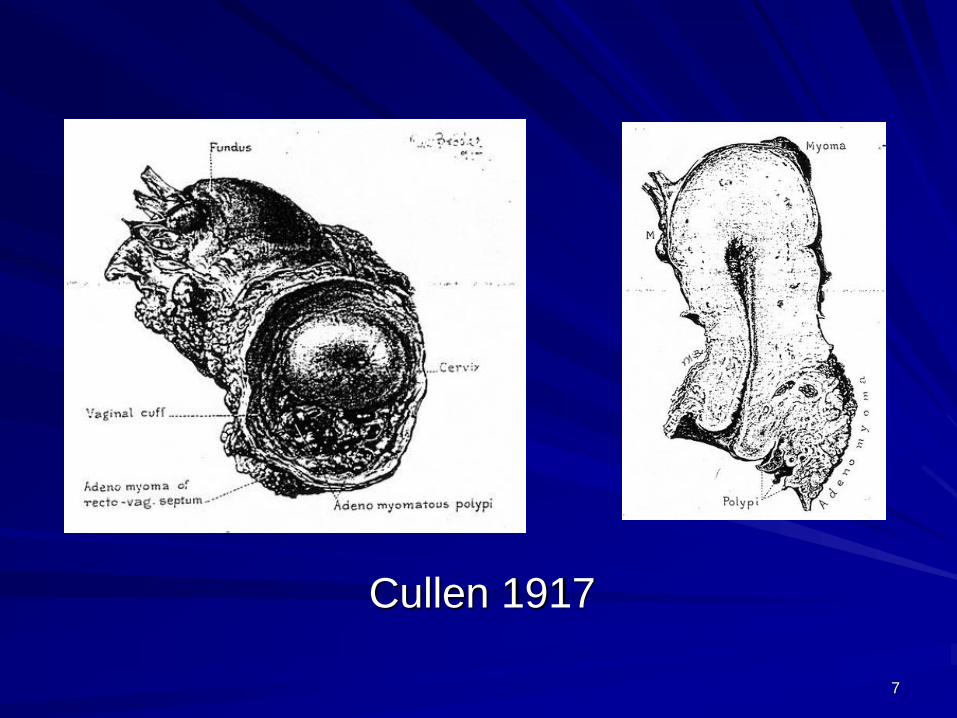
Cullen 1917
7
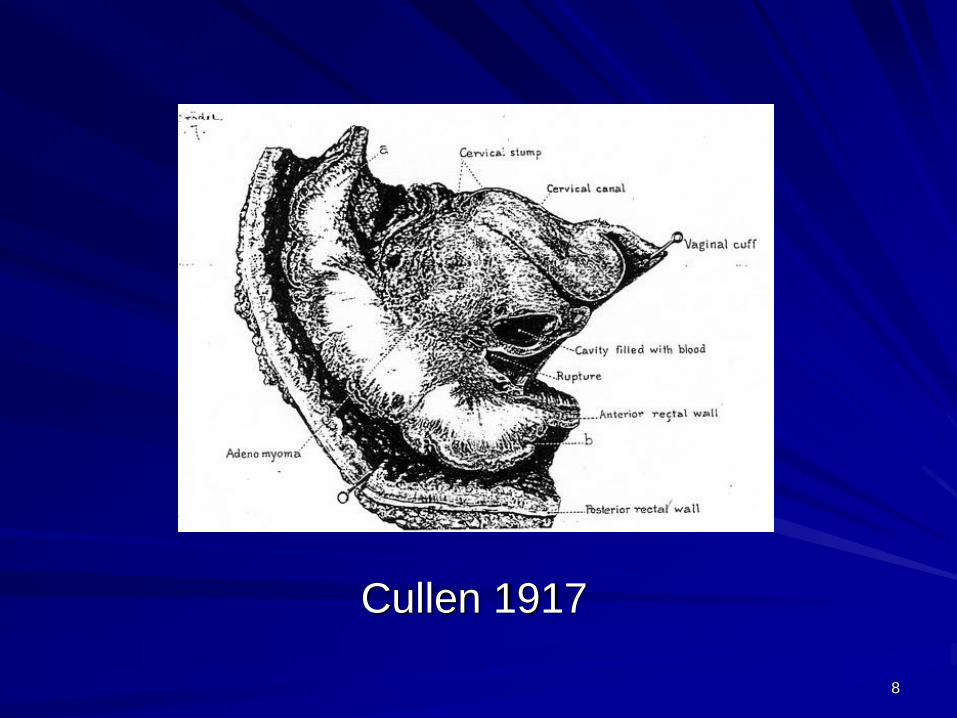
Cullen 1917
8
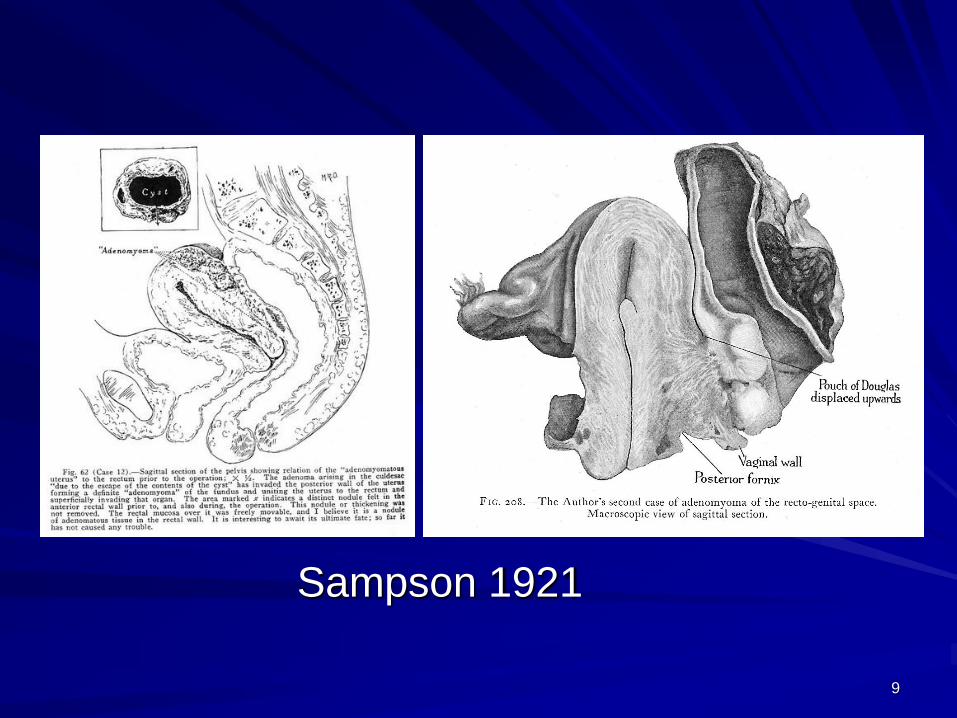
Sampson 1921
9
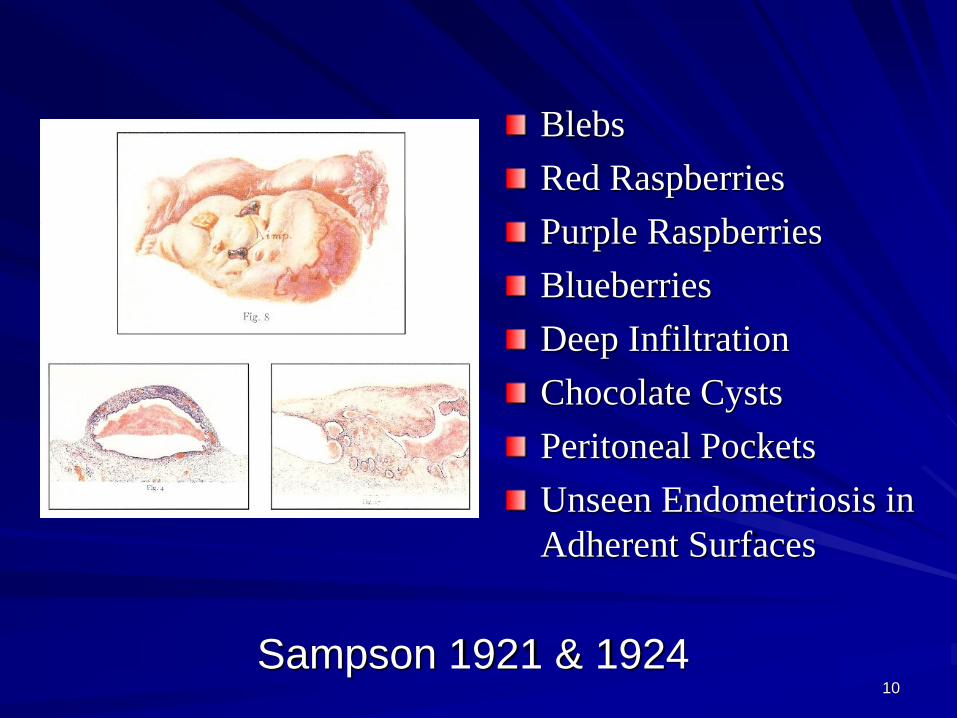
Sampson 1921 & 1924
Blebs
Red Raspberries
Purple Raspberries
Blueberries
Deep Infiltration
Chocolate Cysts
Peritoneal Pockets
Unseen Endometriosis in
Adherent Surfaces
10
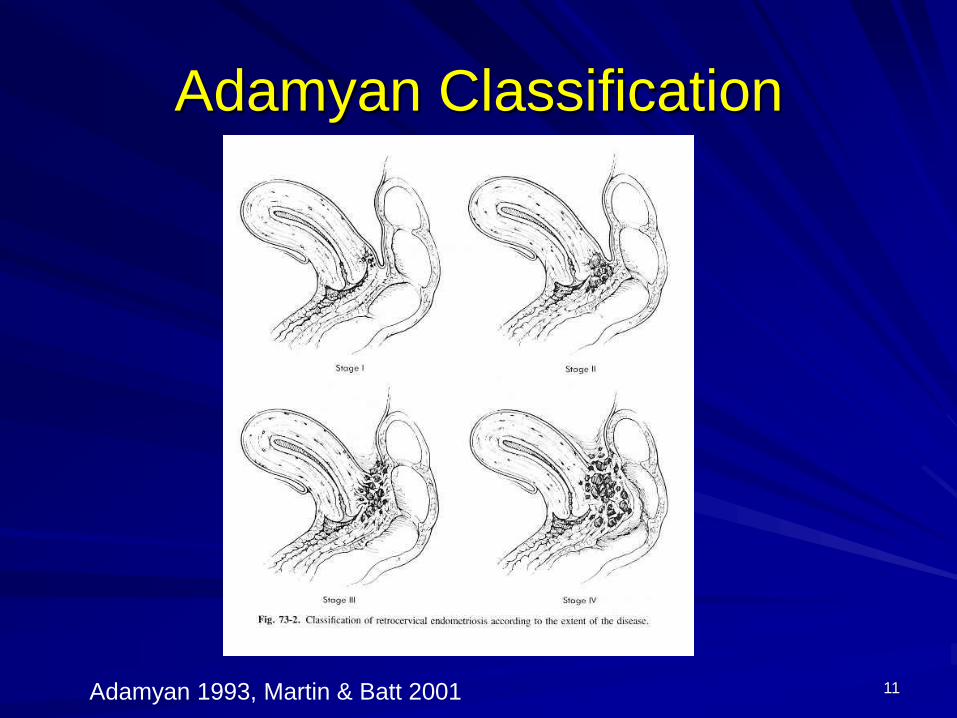
Adamyan Classification
Adamyan 1993, Martin & Batt 2001 11

12
Rectovaginal Septum
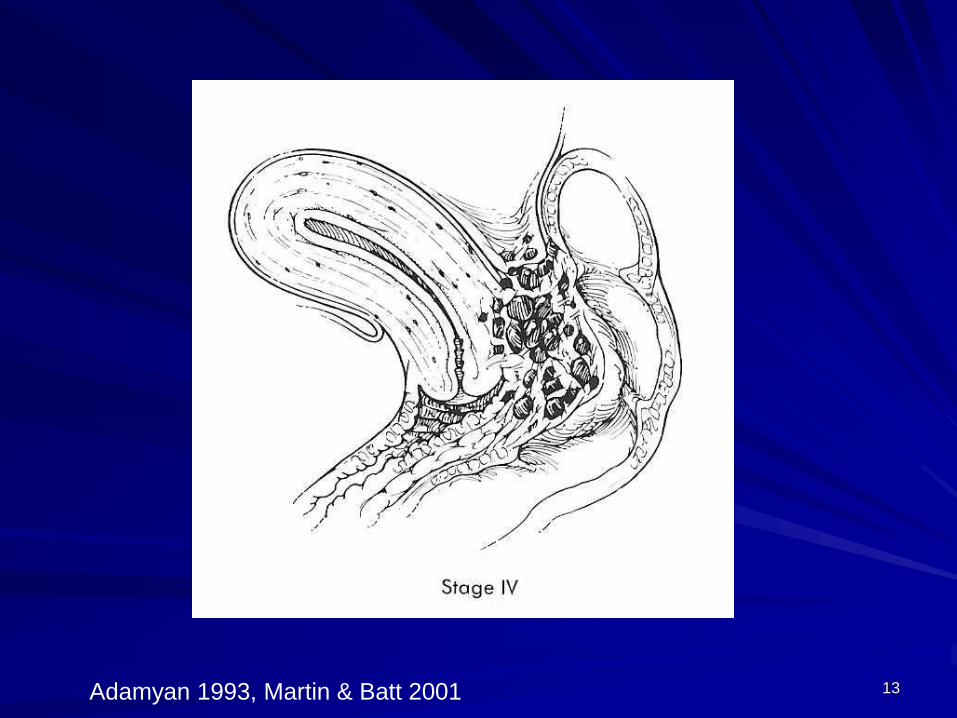
Adamyan 1993, Martin & Batt 2001 13

Dark Scarred 1990
14

15
Dark Scarred 1990
Carbon
Endometriosis deep
in fibromuscular scar →
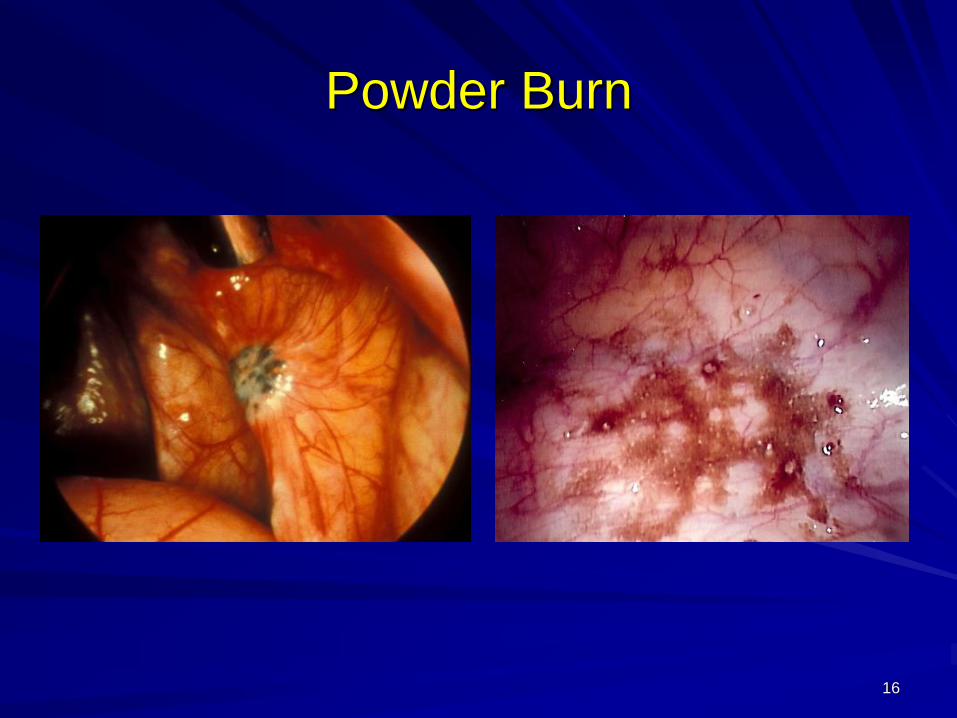
Powder Burn
16
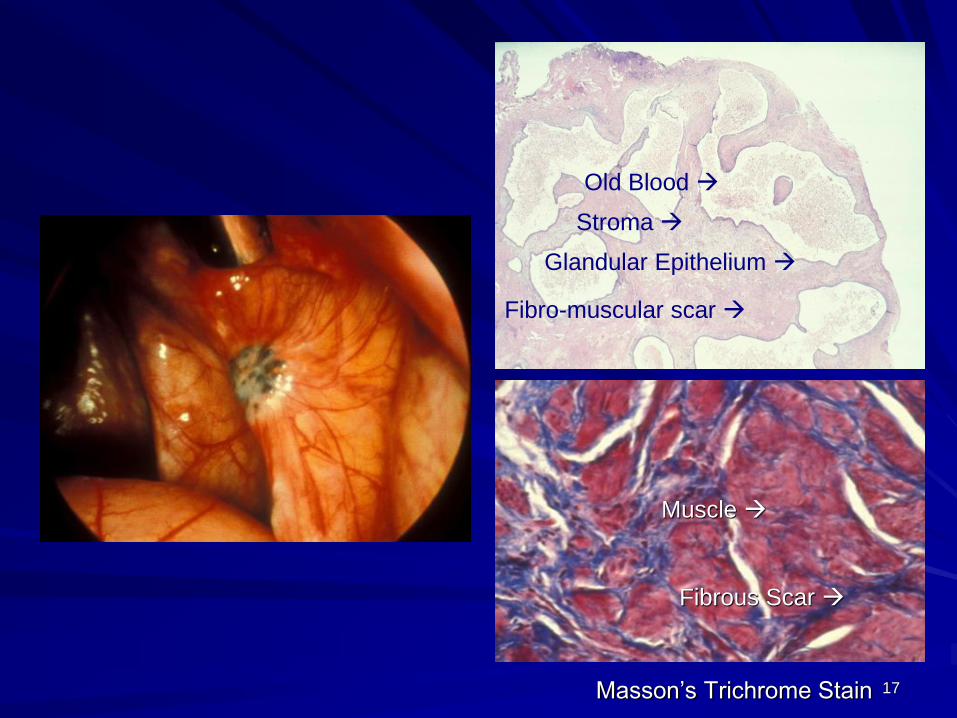
Old Blood →
Fibro-muscular scar →
Stroma →
Glandular Epithelium →
Muscle →
Masson’s Trichrome Stain
Muscle →
Fibrous Scar →
17
18
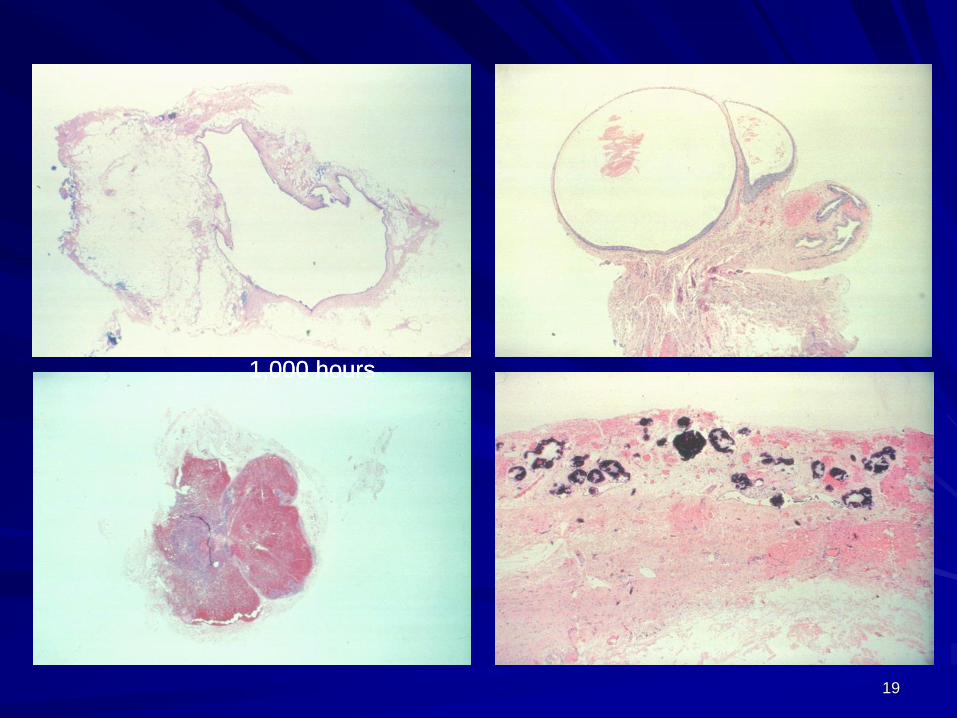
1,000 hours1,000 hours
19
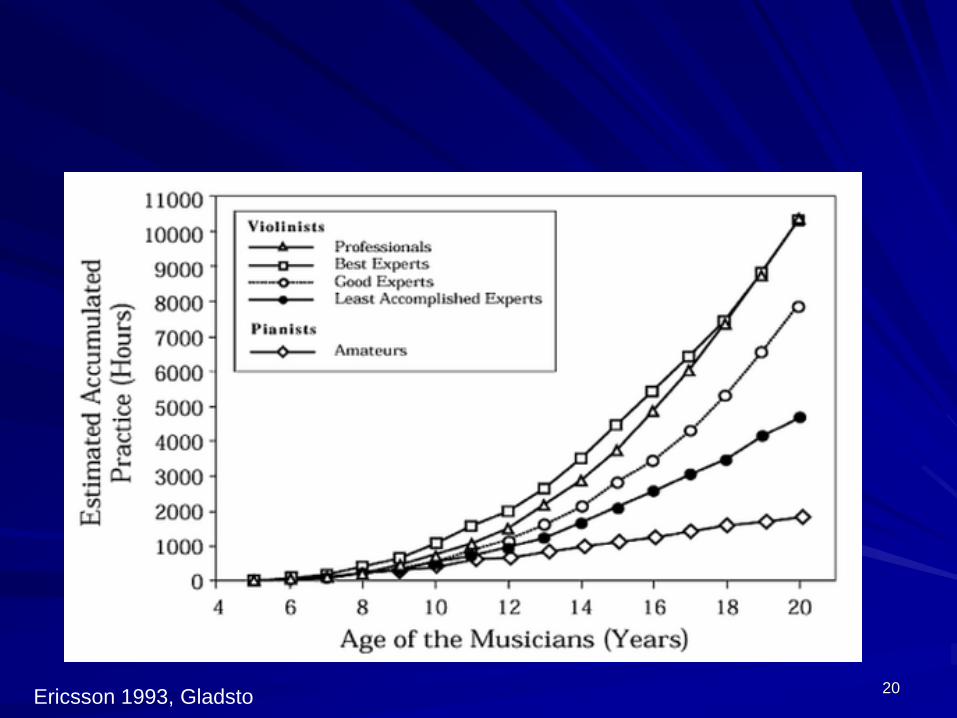
Ericsson 1993, Gladsto20
21
Statistics
There are three kinds of lies: lies, damned
lies, and statistics– Benjamin Disraeli (1804–1881)
– Mark Twain (1835-1910)
Statistics don’t lie just statisticians.
Politicians use statistics in the same way
that a drunk uses lamp-posts —
for support rather than illumination – Andrew Lang (1844-1912)
22
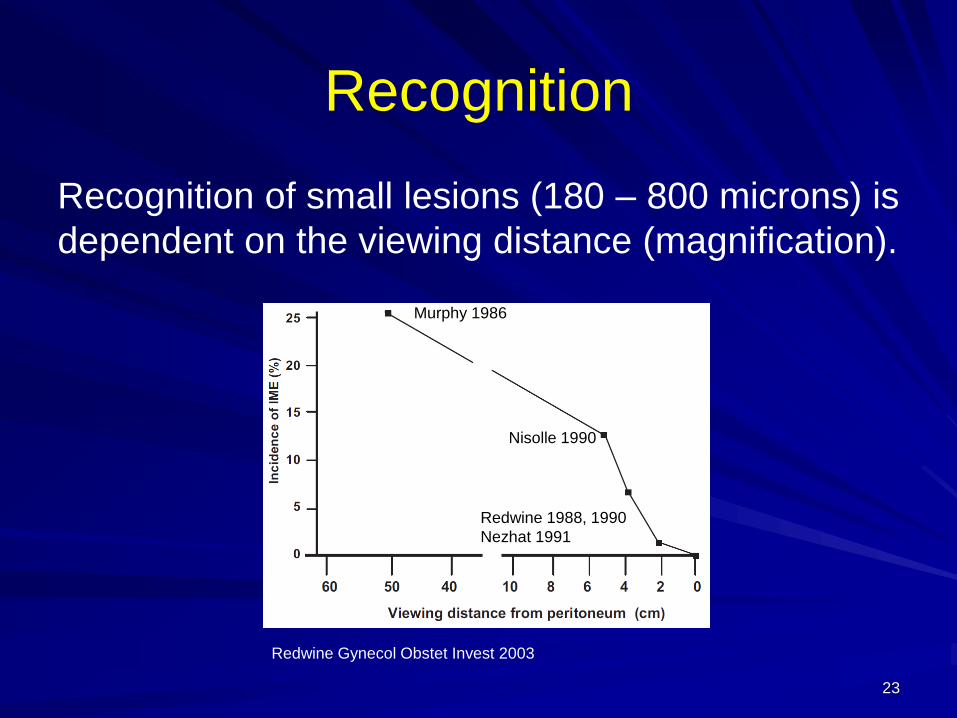
Recognition
Recognition of small lesions (180 – 800 microns) is
dependent on the viewing distance (magnification).
Redwine Gynecol Obstet Invest 2003
Murphy 1986
Nisolle 1990
Redwine 1988, 1990
Nezhat 1991
23
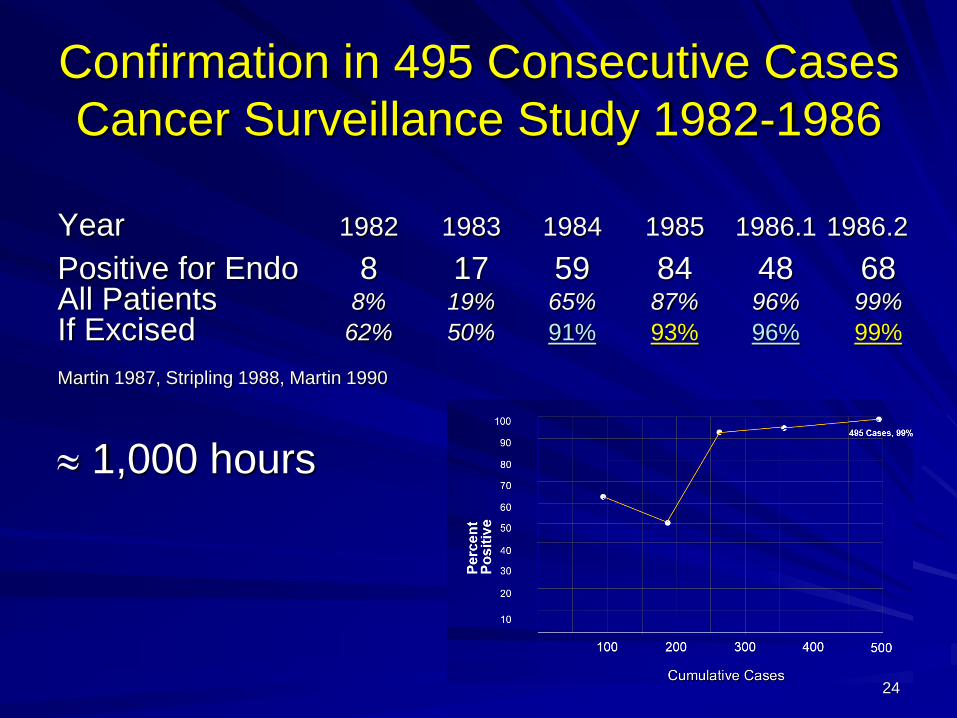
Confirmation in 495 Consecutive Cases
Cancer Surveillance Study 1982-1986
Year 1982 1983 1984 1985 1986.1 1986.2
Positive for Endo 8 17 59 84 48 68All Patients 8% 19% 65% 87% 96% 99%
If Excised 62% 50% 91% 93% 96% 99%
Martin 1987, Stripling 1988, Martin 1990
1,000 hours
24
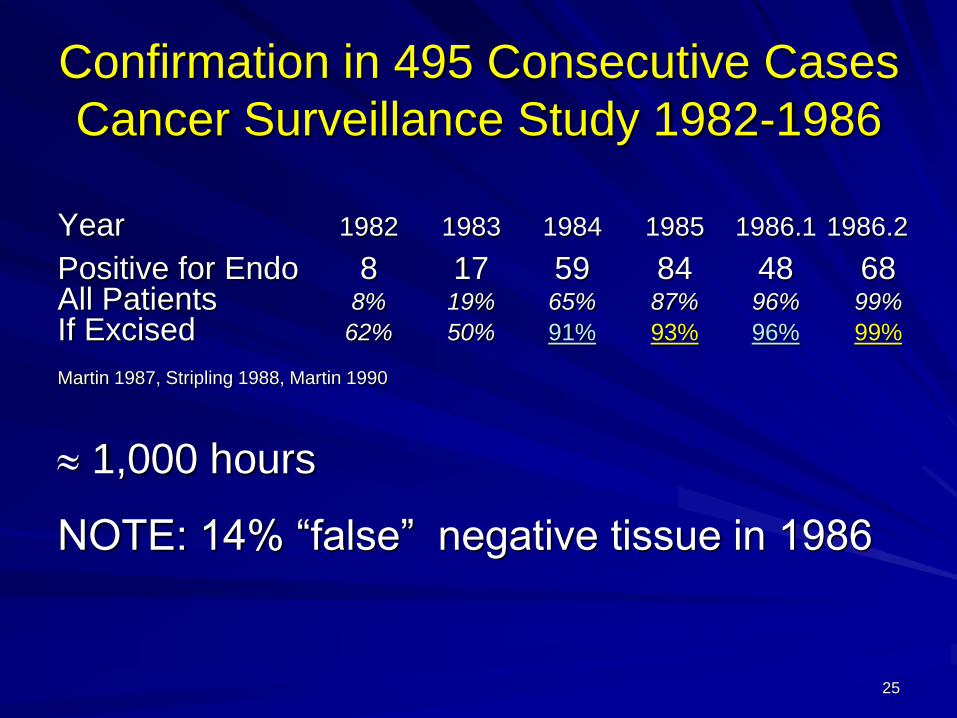
Confirmation in 495 Consecutive Cases
Cancer Surveillance Study 1982-1986
Year 1982 1983 1984 1985 1986.1 1986.2
Positive for Endo 8 17 59 84 48 68All Patients 8% 19% 65% 87% 96% 99%
If Excised 62% 50% 91% 93% 96% 99%
Martin 1987, Stripling 1988, Martin 1990
1,000 hours
NOTE: 14% “false” negative tissue in 1986
25
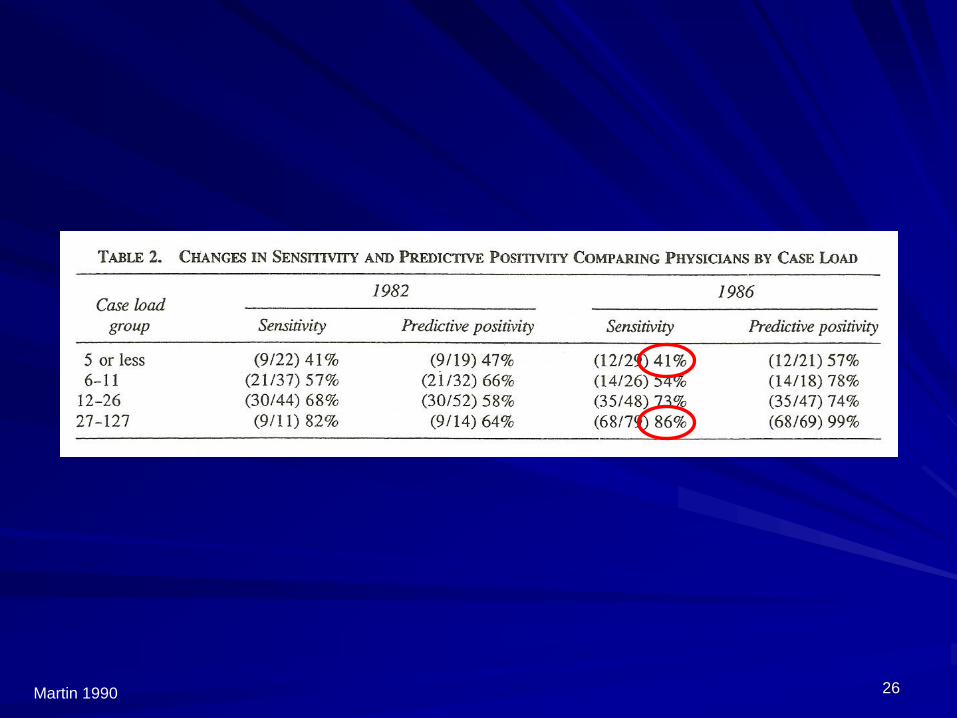
Martin 1990 26
Confirmation at a Research Level
Requirements
• Pathologist must be requested to perform several sections.
• A large number of tissue samples must be taken for histologic confirmation of the diagnosis, and each one should be submitted in a separate container.
• An average of 1.2 samples/patient is not sufficient.
Buchweitz 2003 27
Confirmation at a Research LevelNo Expectation of Appearance
Biopsy Techniques–Power density of 4,000 to 26,000 watt/cm2 (0.2 to 0.5 cm spot, 110 watt laser)
–Alignment for TEM00 mode
Adequate Number of Biopsies
Signal to Noise Ratio
Tagging the Specimen Location
Marking the Specimen Side
Notations on Pathology Request
Uniform Specimen Size in Container
Cell Block
Transferring the Specimen to Container
Processing by the Surgeon
Communications with the Cutters
Communications with the Pathologist
Re-cutting Specimens
Require a Histologic DescriptionA 1 mm lesion requires histology compatible with a 1 mm lesion.
Histologic Criteria (Batt 1989)
Reviewing Slides
Surgeon Experience
Fixed Protocol* Protocol in yellow may not be compatible with STARD.
This level of concern for accuracy
can be attained in research.
There is no documentation that
this is useful outside of a research
setting.
A STARD level research protocol
would not allow communications
or review. The protocol would
need to clarify the procedures.
28
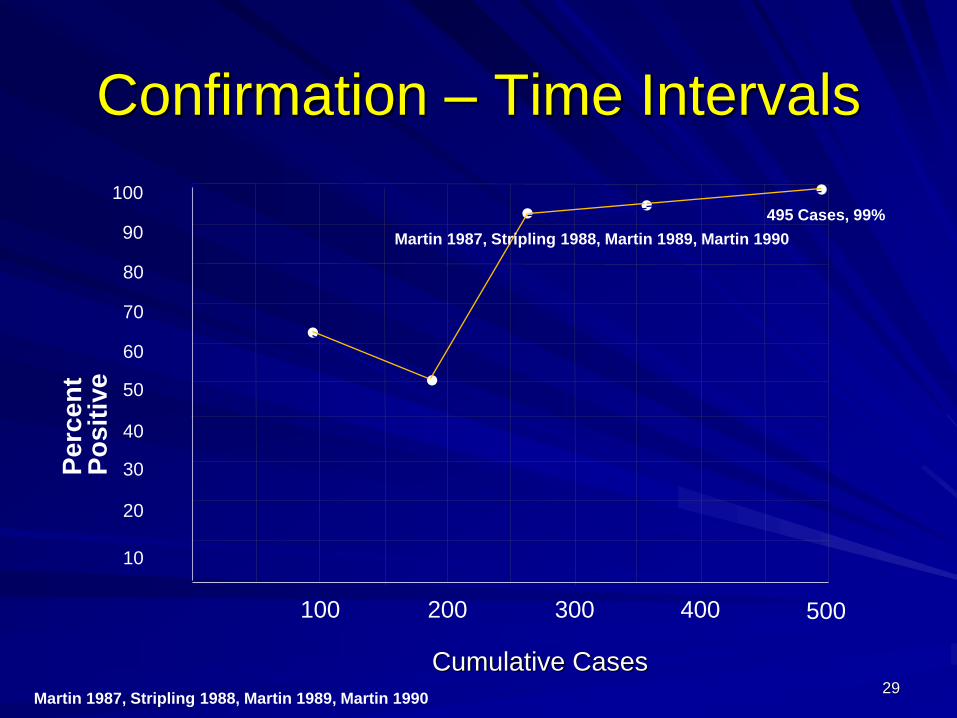
Confirmation – Time Intervals
Cumulative Cases
100 500
100
90
80
70
60
50
40
30
20
10
200 300 400
Pe
rce
nt
Po
sit
ive ●
●●
●
●
Martin 1987, Stripling 1988, Martin 1989, Martin 1990
495 Cases, 99%
Martin 1987, Stripling 1988, Martin 1989, Martin 1990
29

Confirmation – Time Intervals
Cumulative Cases
100 500
100
90
80
70
60
50
40
30
20
10
200 300 400
Pe
rce
nt
Po
sit
ive ●
●●
●
●
Martin 1987, Stripling 1988, Martin 1989, Martin 1990
Stratton 2002, Stegmann 2008, 179 Cases
●●●
Dulumba 2012
● 280 Cases, 80%
495 Cases, 99%
30
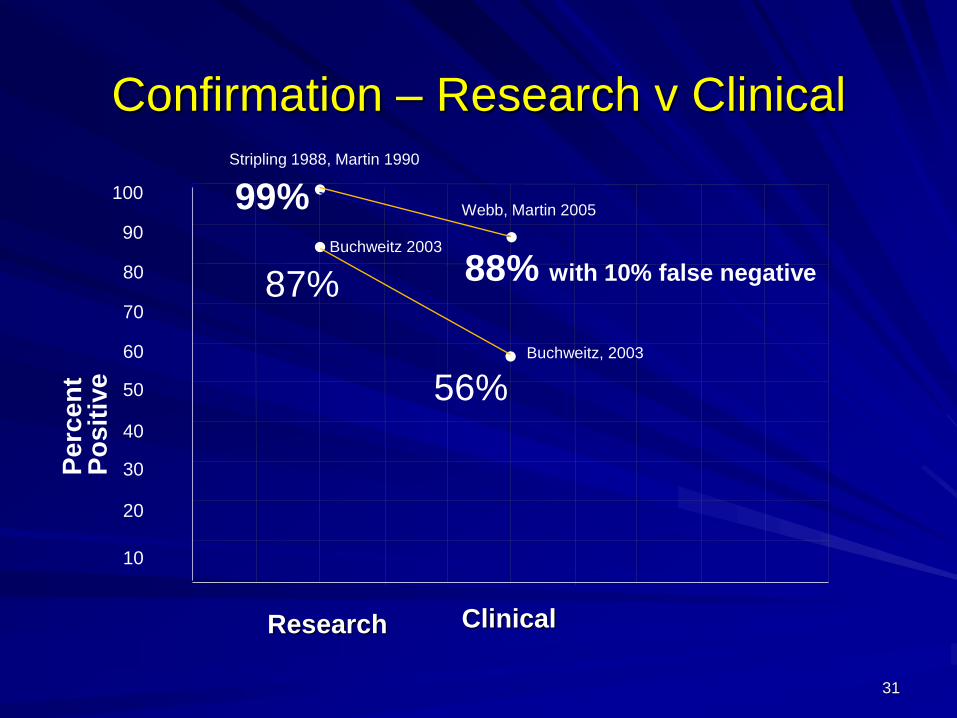
Confirmation – Research v Clinical
100
90
80
70
60
50
40
30
20
10
Pe
rce
nt
Po
sit
ive
●
●
●
●
ClinicalResearch
Stripling 1988, Martin 1990
Webb, Martin 2005
Buchweitz 2003
Buchweitz, 2003
99%
88% with 10% false negative87%
56%
31
What Can We Do with a Biopsy?
Rule out cancer
Determine a histological diagnosis
Guide therapy in some casesThis does not include deciding on therapy of endometriosis with non-specific histology.
– Therapeutic conclusions in the literature are based on appearance, “appearance or histology” or history but not on histology only.
– The literature says to treat it like endometriosis if it looks like endometriosis.
– Histology is used to clarify other concerns.
Research32
Histologic Grading System
Grade 1: possible residua of resorbed endometriosis, i.e., hemosiderin, calcium, nerve, blood vessels, and smooth muscle.
Grade 2: consistent with endometriosis, i.e., hemosiderin, characteristic glands, or stroma.
Grade 3: definite endometriosis, i.e., characteristic glands and stroma with hemosiderin.
Grade 4: grade 3 with structures conveying an organoid pattern, i.e., glandular-stromal layer with overlying well-developed smooth muscle layer.
Batt RE, et al. 1989
33
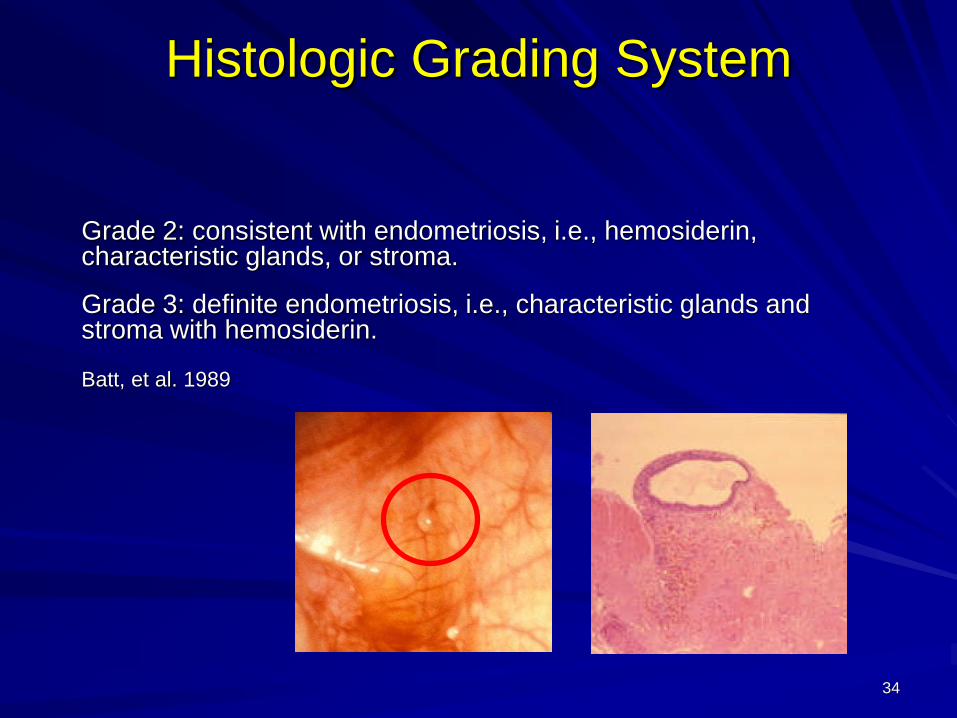
Histologic Grading System
Grade 2: consistent with endometriosis, i.e., hemosiderin, characteristic glands, or stroma.
Grade 3: definite endometriosis, i.e., characteristic glands and stroma with hemosiderin.
Batt, et al. 1989
34
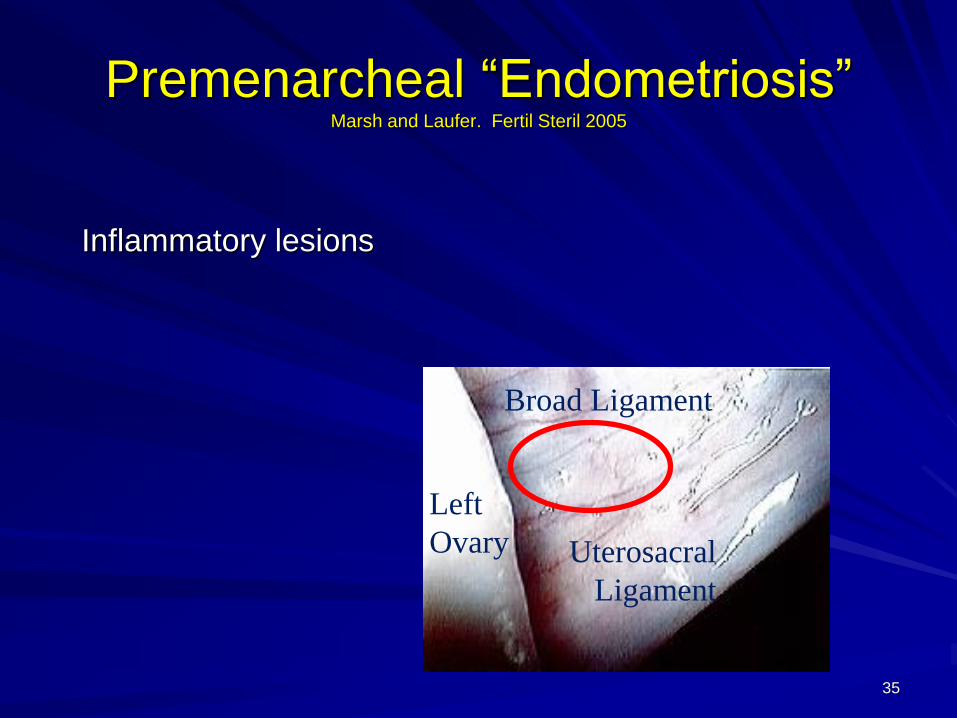
Premenarcheal “Endometriosis”Marsh and Laufer. Fertil Steril 2005
Inflammatory lesions
Left
Ovary Uterosacral
Ligament
Broad Ligament
35
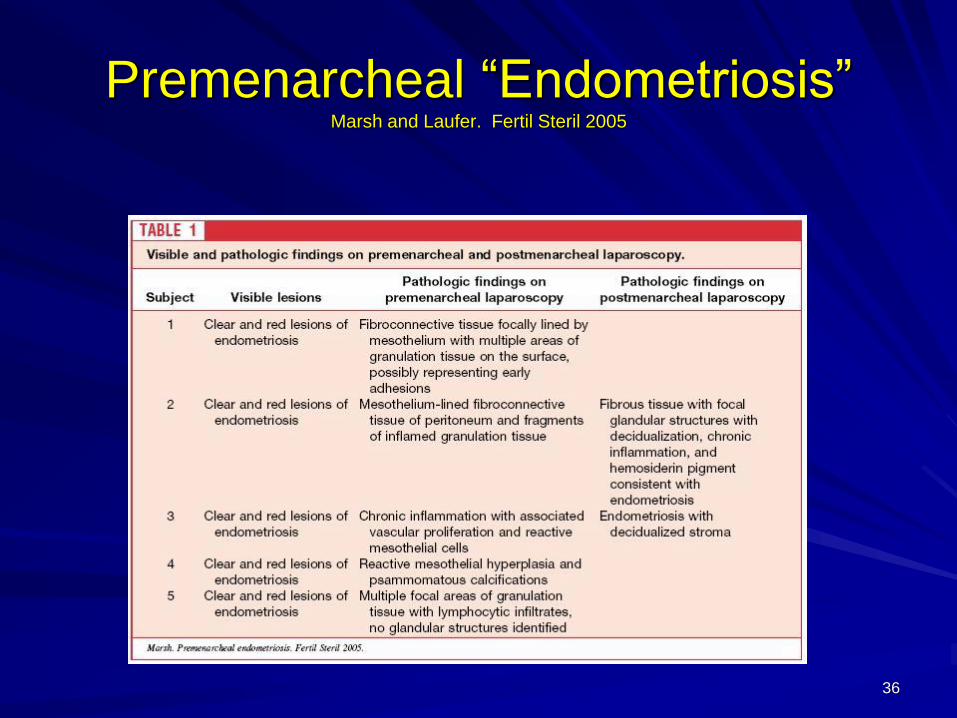
Premenarcheal “Endometriosis”Marsh and Laufer. Fertil Steril 2005
36
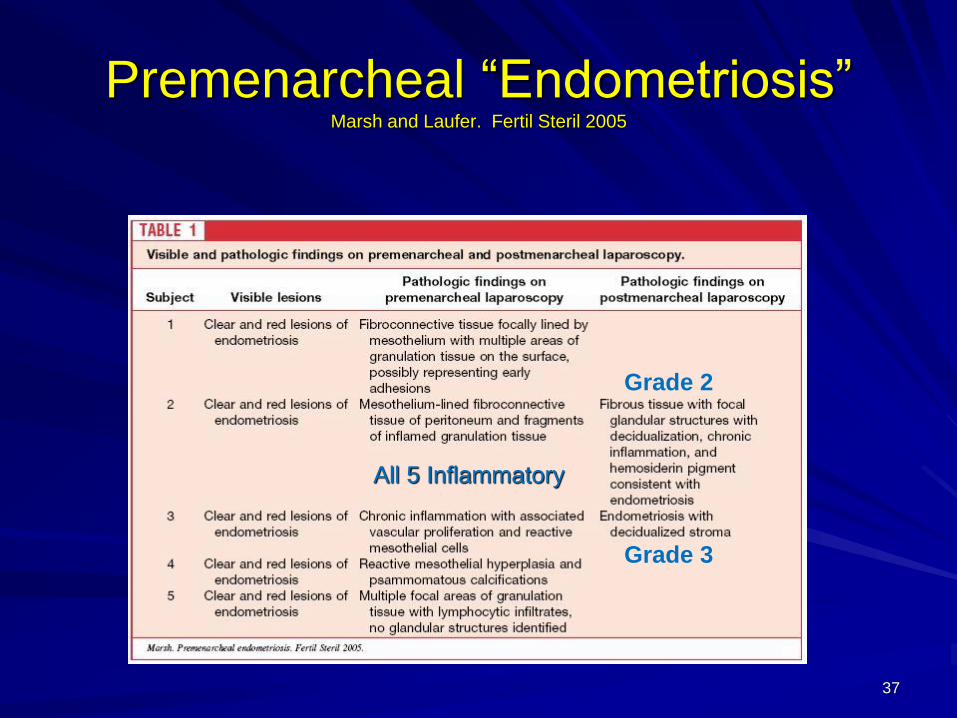
Premenarcheal “Endometriosis”Marsh and Laufer. Fertil Steril 2005
All 5 Inflammatory
Grade 2
Grade 3
37
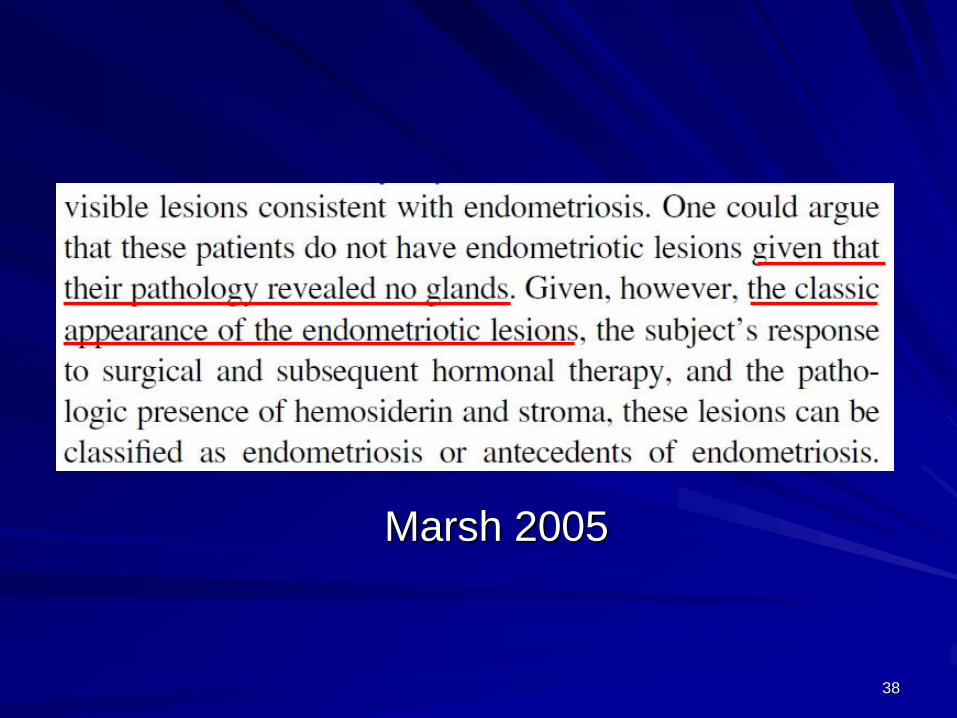
Marsh 2005
38
Drs. Tasuku Harada , Fuminori Taniguchi and Yukihiro Azuma
Tottori University School of Medicine, Yonago, Japan 39
40
Tadpole who thinks they
are a sperm slide
Delayed Diagnosis
Majority of adults with endometriosis had
severe dysmenorrhea as teeagers.
Data on what percent of adults with no
diagnosis of endometriosis had severe
dysmenorrhea as a teen?
Data on what percent of women with mild
endometriosis as a teen have severe
endometriosis 20 years later.
41
Empirical Therapy
Dysmenorrhea – Oral Contraceptives
Pelvic Pain – NSAIDs
Combined OC & NSAID therapy
Persistent Pain
– Depo-MPA
– Depo-GnRH agonist
– Narcotics
– Laparoscopy
42
Delayed Diagnosis
Natural Course?
Suppressive Therapy?
Surgical Therapy?
Physical Therapy?
Acupuncture?
Meditation?
…
43
Is Superficial Implantation a Disease?
Is Transient Occurrence a Disease?
“Disease exists with aggressive infiltration or cystic ovarian endometriosis.”
Koninckx PR. Is mild endometriosis a condition occurring intermittently in all
women? Human Reproduction. 1994;9:2202-5.
“Endometriotic disease is not simply the finding of glands and stroma
(endometriosis) as these findings can be the result of retrograde
menstruation with early peritoneal implantation. Early implantation may be
recognized and eradicated by the immune system.”
Evers JLH. Endometriosis does not exist; all women have endometriosis.
Human Reproduction. 1994;9(12):2206-9.
Compare with the Pimple Model
44
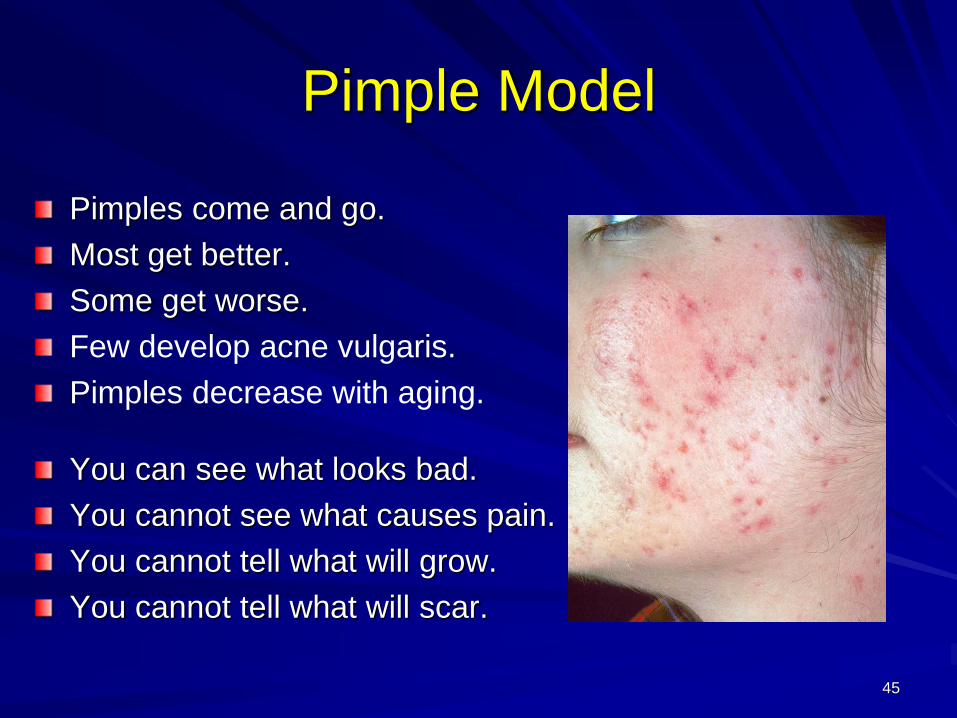
Pimple Model
Pimples come and go.
Most get better.
Some get worse.
Few develop acne vulgaris.
Pimples decrease with aging.
You can see what looks bad.
You cannot see what causes pain.
You cannot tell what will grow.
You cannot tell what will scar.
45
All M.C. Escher works (c) 2013 The M.C. Escher Company - the Netherlands.
All rights reserved. Used by permission. www.mcescher.com
46
Escher Relativity Slide
http://www.mcescher.com/gallery/back-in-holland/relativity/
http://www.mcescher.com/gallery/back-in-holland/relativity/
47

48
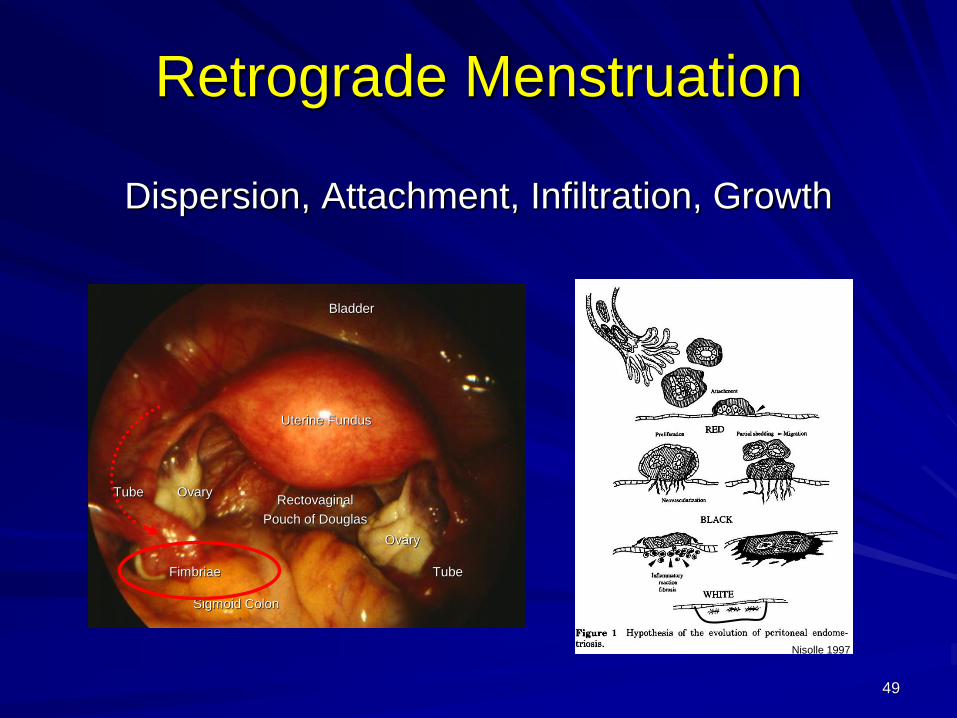
Retrograde Menstruation
Dispersion, Attachment, Infiltration, Growth
Sigmoid Colon
Uterine Fundus
Ovary
Ovary
Tube
Rectovaginal
Pouch of Douglas
Bladder
Fimbriae
Tube
Nisolle 1997
49
Retrograde Menstruation
What % of women have retrograde menstruation?
37%
51%
76%
87%
97%
100%
50
Retrograde Menstruation
What % of women have retrograde menstruation?
37% - D’Hooghe, et al. 1996* – Recurrent
51% - D’Hooghe, et al. 1996 – Single
76% - Liu and Hitchcock 1986 – All Women
87% - D’Hooghe, et al. 1996 – Stage I
97% - Liu and Hitchcock 1986 – Endometriosis
100% - D’Hooghe, et al. 1996 – Stage II to IV
* * Higher prevalence and recurrence with spontaneous endometriosis.
** Less than 100% Mayer-Rokitansky-Küster-Hauser.
51
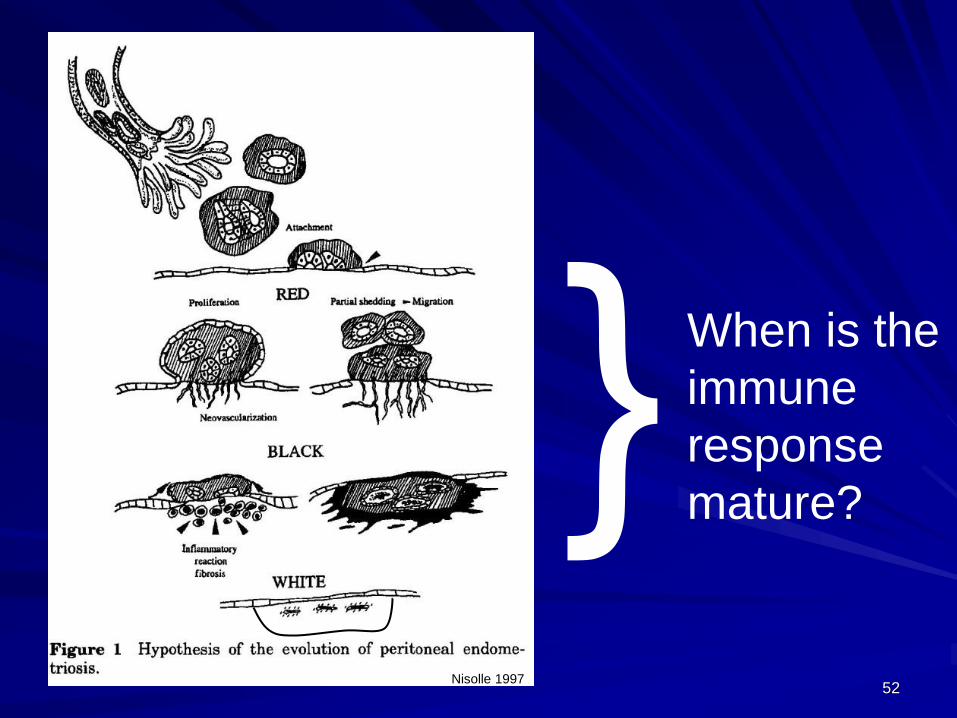
When is the
immune
response
mature?
Nisolle 199752
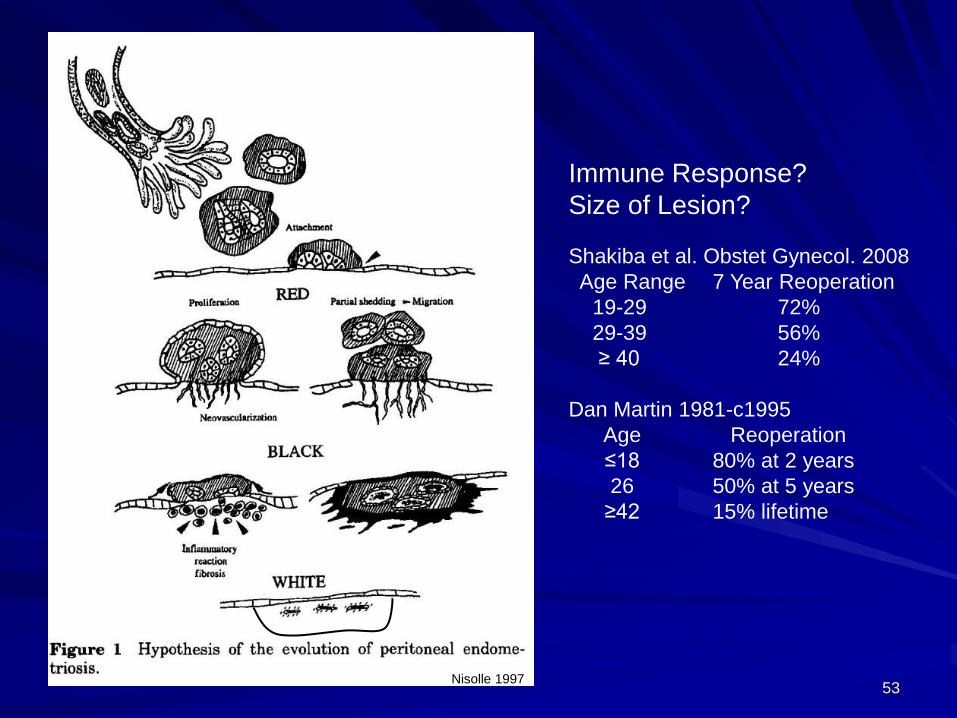
Immune Response?
Size of Lesion?
Shakiba et al. Obstet Gynecol. 2008
Age Range 7 Year Reoperation
19-29 72%
29-39 56%
≥ 40 24%
Dan Martin 1981-c1995
Age Reoperation
≤18 80% at 2 years
26 50% at 5 years
≥42 15% lifetime
Nisolle 199753

54
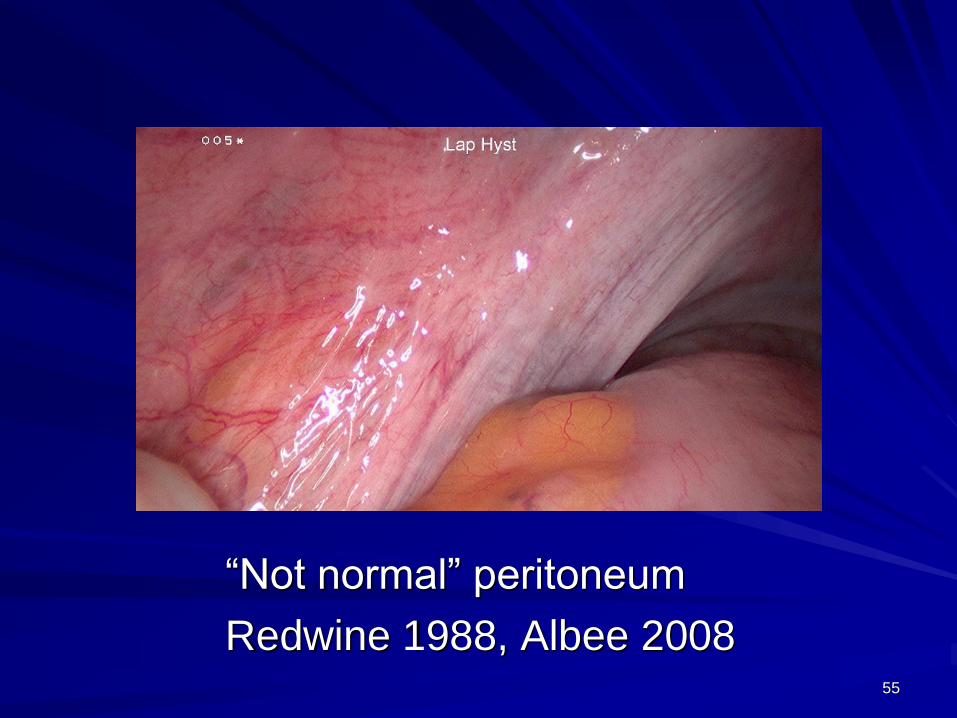
“Not normal” peritoneum
Redwine 1988, Albee 200855
Visually Normal Peritoneum
Criteria for selection of visually normal peritoneum by near-contact
laparoscopy.
Peritoneal surface perfectly smooth with no texture irregularity or
specular light reflections
No abnormal vascular patterns
Transparent peritoneum without associated color
No suggestion of subperitoneal cystic structures
No superficial fibrosis
Redwine 1988, Albee 2008
56
Related Documents











