Clinical Cases

Clinical Cases. For each case, there is first a slide with some history –Think about a likely differential diagnosis, based on the clinical information.
Dec 19, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Clinical Cases

Clinical Cases
• For each case, there is first a slide with some history– Think about a likely differential diagnosis, based on the
clinical information
• The next slide features the CXR– Look at it carefully, and think how you would describe it
– either over the telephone to your Registrar, or a written report in the medical notes
• The next slide has an annotated explanation of the CXR findings with the diagnosis– Think what the physical examination findings would be– Think what additional investigations might be useful– Try to decide what treatment would be appropriate

CASE 1
Elderly male, 2 previous myocardial infarctions, presents with crushing
central chest pain radiating to jaw and left
arm, and extreme breathlessness
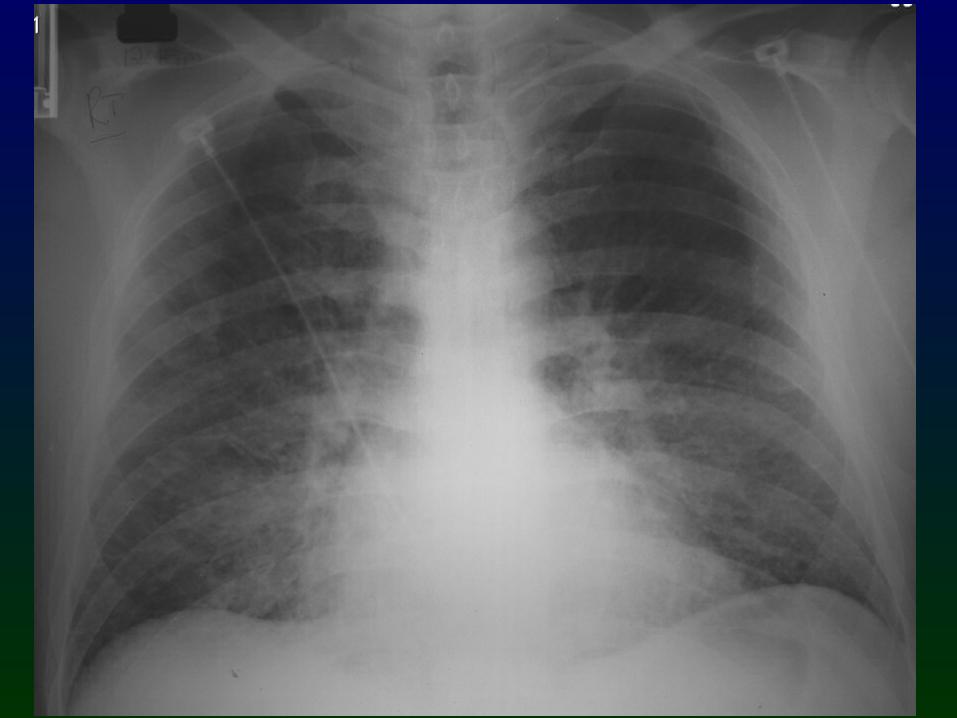

Pulmonary Oedema
Kerley B Lines
Enlarged Heart
Alveolar Oedema
Perihilar haze
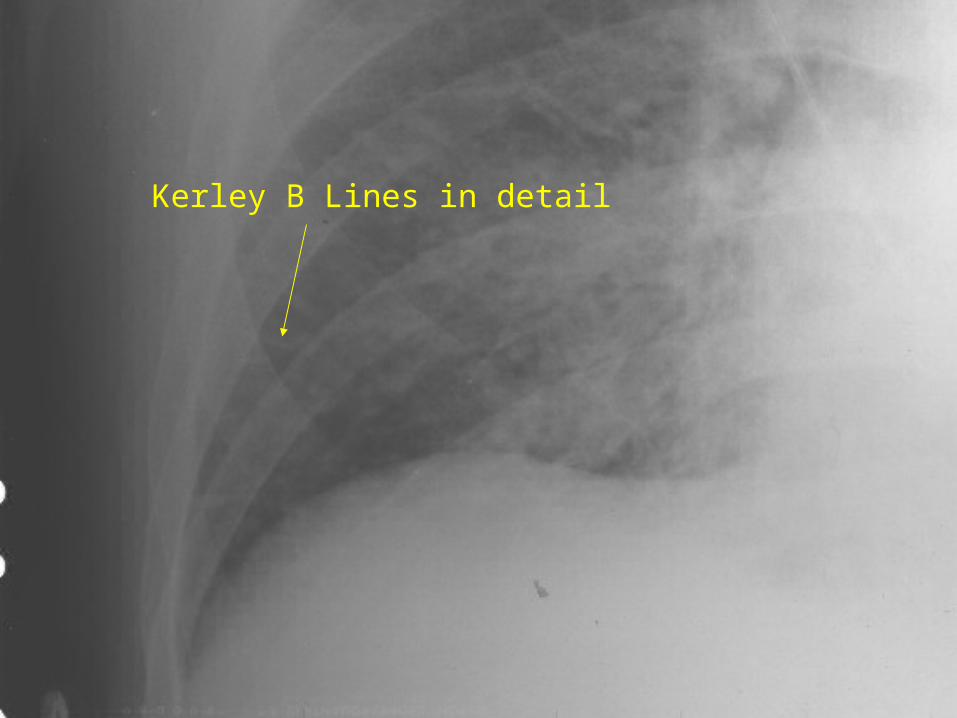
Kerley B Lines in detail
CASE 2
70 year old man. Left pneumonectomy three
years ago for lung cancer.
Admitted with haemoptysis, weight loss


Tracheal deviation
White out
Heart moved over here(mediastinal shift)
…these are all features of the previous left pneumonectomy (which are
identical to total left lung collapse). What however is the other
abnormality?
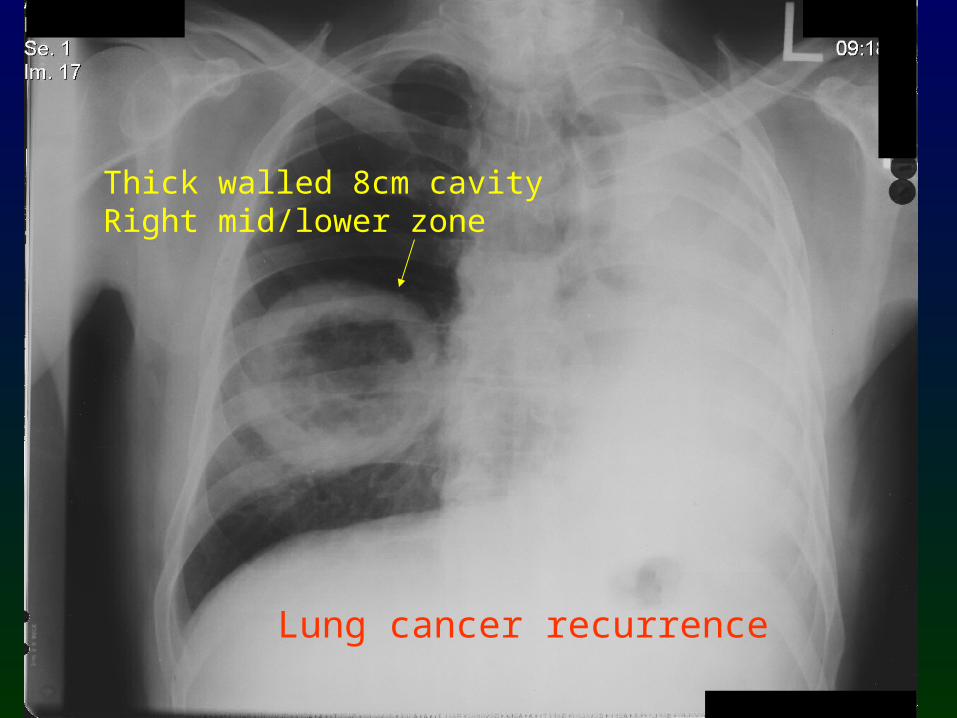
Lung cancer recurrence
Thick walled 8cm cavityRight mid/lower zone
CASE 3
40 year old man. 3 month history of increasing
breathlessness. Reduced left chest expansion and
stony dull percussion note.

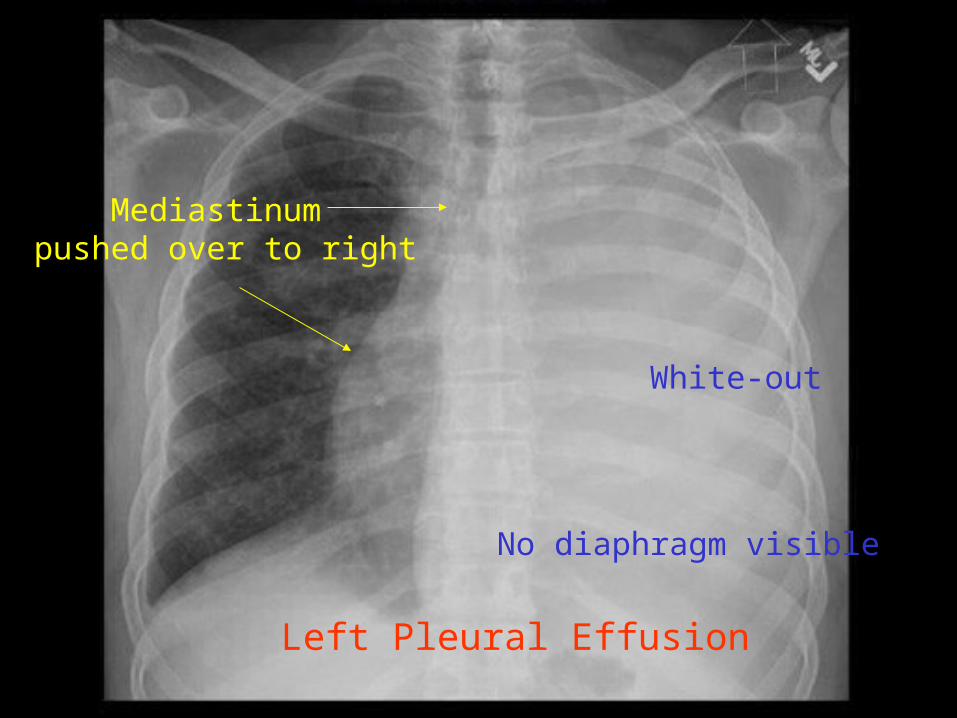
Left Pleural Effusion
Mediastinum pushed over to right
White-out
No diaphragm visible
CASE 4
30 year old, acute onset of breathlessness and pleuritic chest pain.
Afebrile.

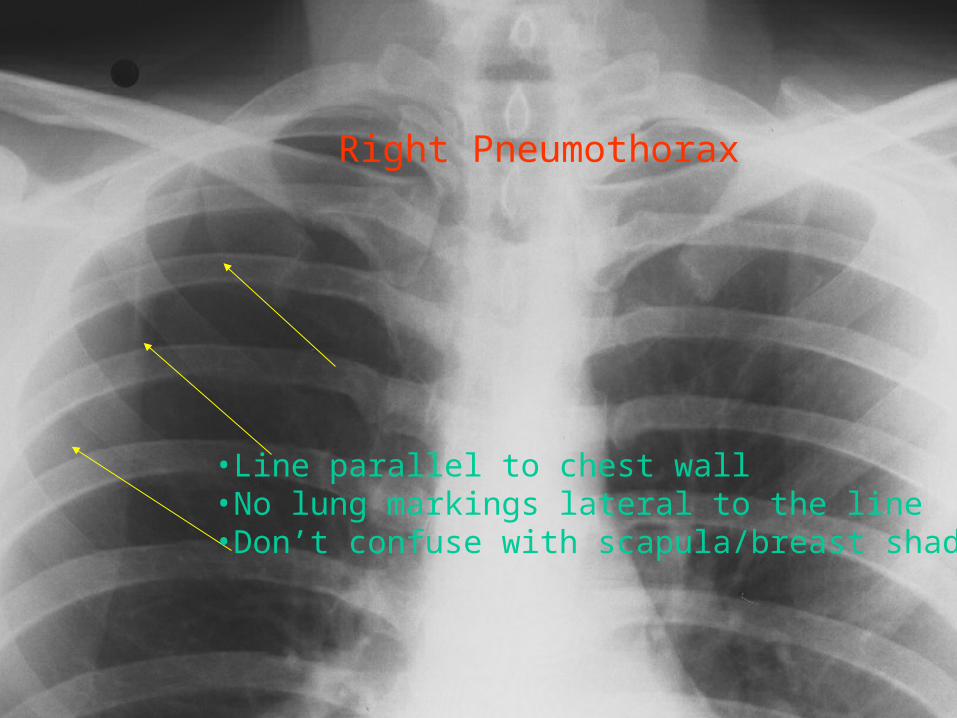
Right Pneumothorax
•Line parallel to chest wall•No lung markings lateral to the line•Don’t confuse with scapula/breast shadow

CASE 5
55 year old alcoholic with severe abdominal pain.
Tender +++ epigastrium with guarding and
rebound
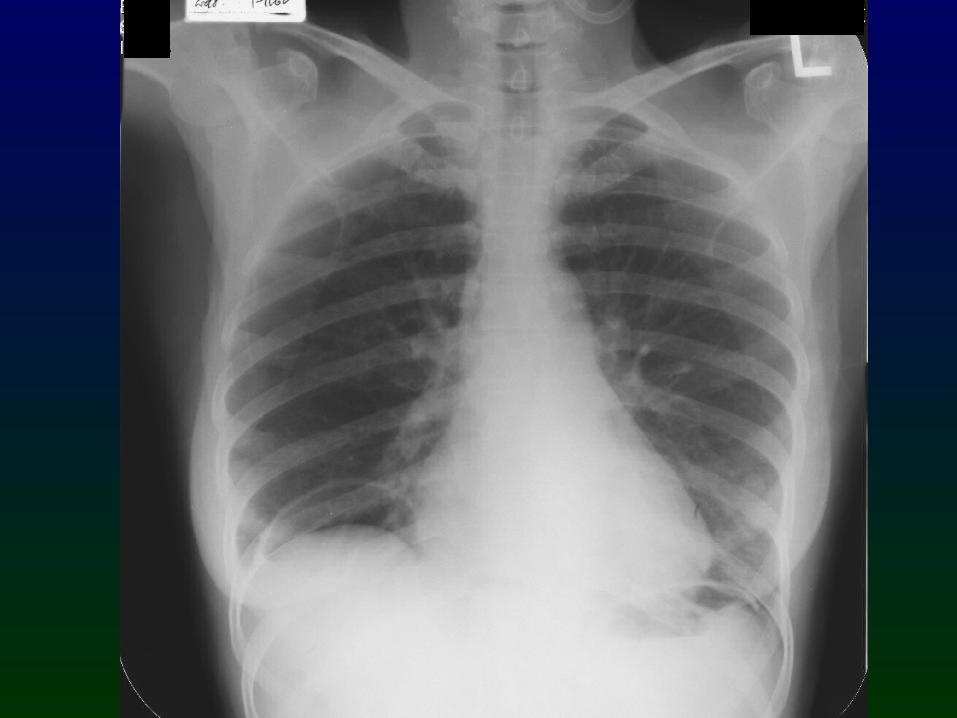
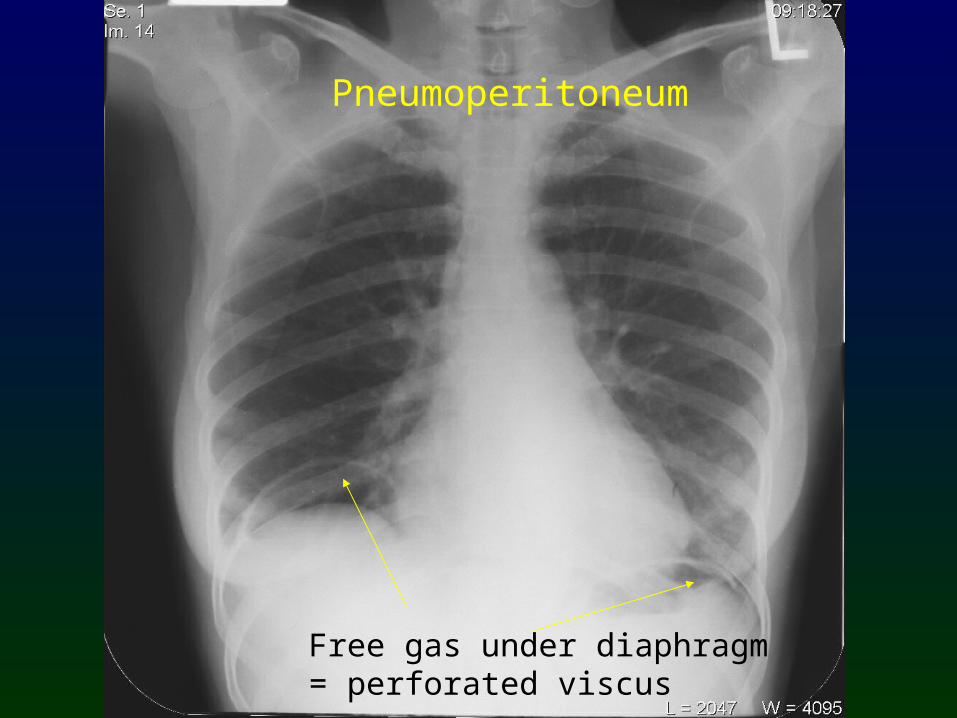
Free gas under diaphragm= perforated viscus
Pneumoperitoneum

Other examples of Pneumoperitoneum

CASE 6
74 year old female. 2 month history of
progressive weight loss, malaise, drenching night sweats and itch. She has
found a lump in her neck.


Mediastinal Lymph node enlargement
Probable Lymphoma

CASE 7
26 year old female. 3 month history of malaise.
Shiny, painful rash on shins and red, dry eyes.


Bilateral Hilar Lymph node enlargement
Sarcoidosis

CASE 8
65 year old. Admitted for elective surgery (inguinal
hernia repair). No past history. Smoker. Recent weight loss and cough.


Multiple bilateral pulmonary masses
…multiple metastases until proven otherwise

CASE 9
19 year old motorcyclist.Involved in high speed
road traffic incident.

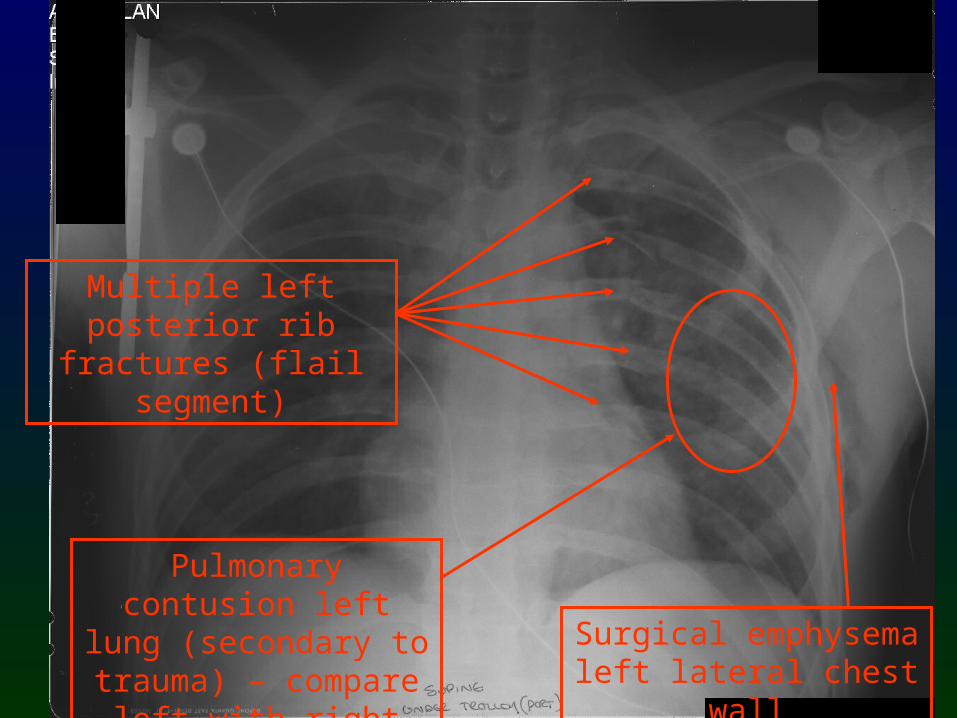
Multiple left posterior rib
fractures (flail segment)
Surgical emphysema left lateral chest wall
Pulmonary contusion left lung (secondary
to trauma) – compare left with right side
CASE 10
55 year old man. 6 month history of progressive
breathlessness and a dry cough. No haemoptysis.


Fibrosing Alveolitis
Generalised increased interstitial shadowing, particularly in mid/lower
zones
Loss of clear cardiac and mediastinal
contours
CASE 11
20 year old, sudden onset of extreme breathlessness
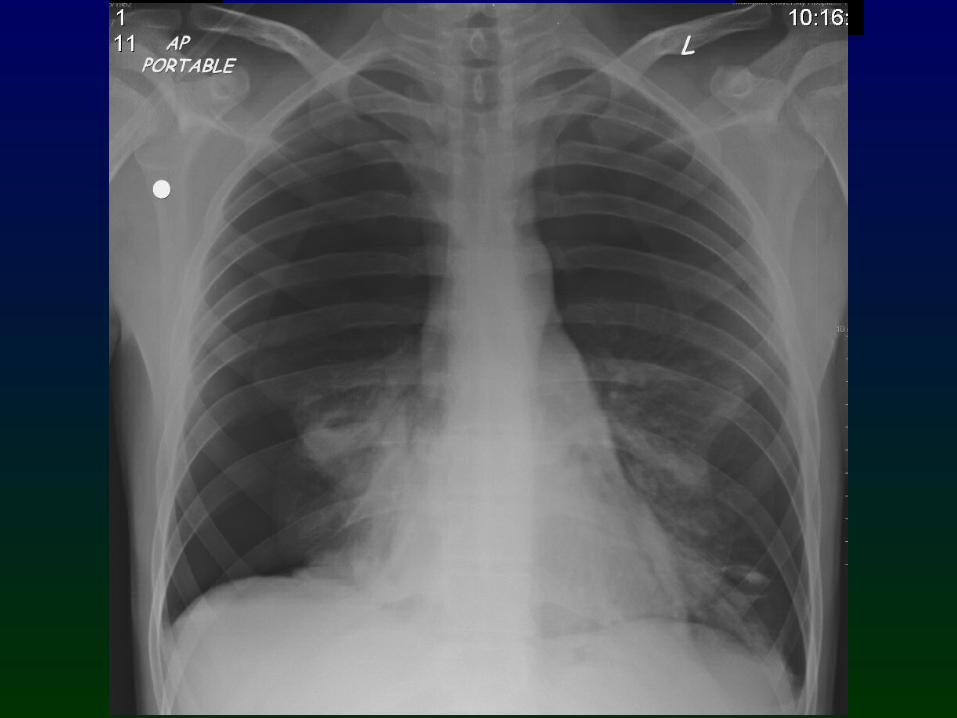
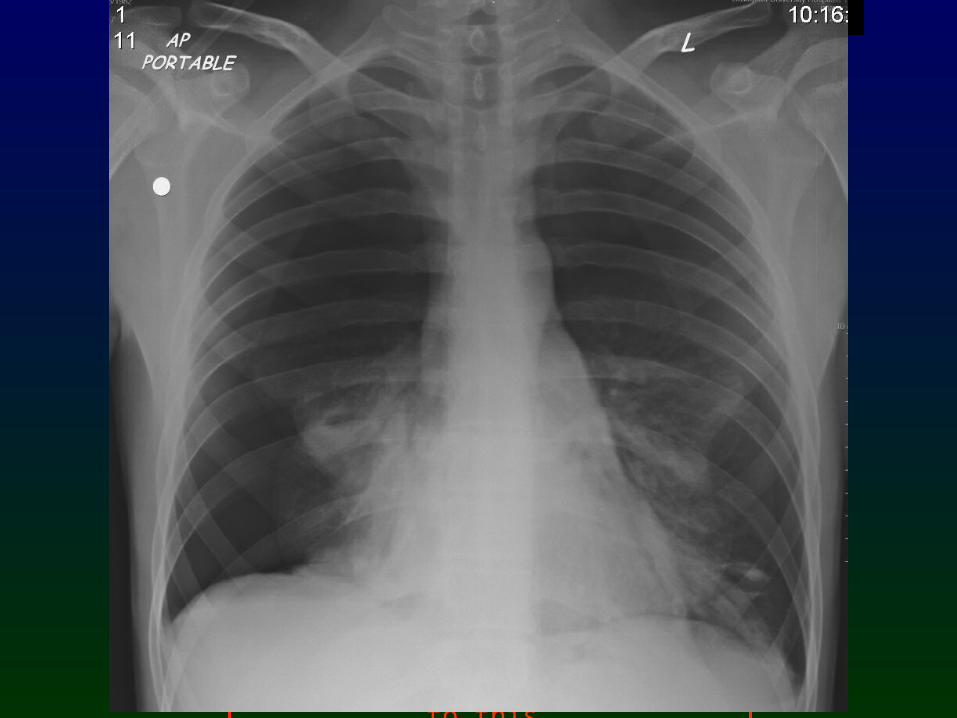
Bilateral Pneumothoraces
Red arrows denote lung edge. Note no lung markings lateral to
this.

CASE 12
20 year old, sudden onset of extreme breathlessness

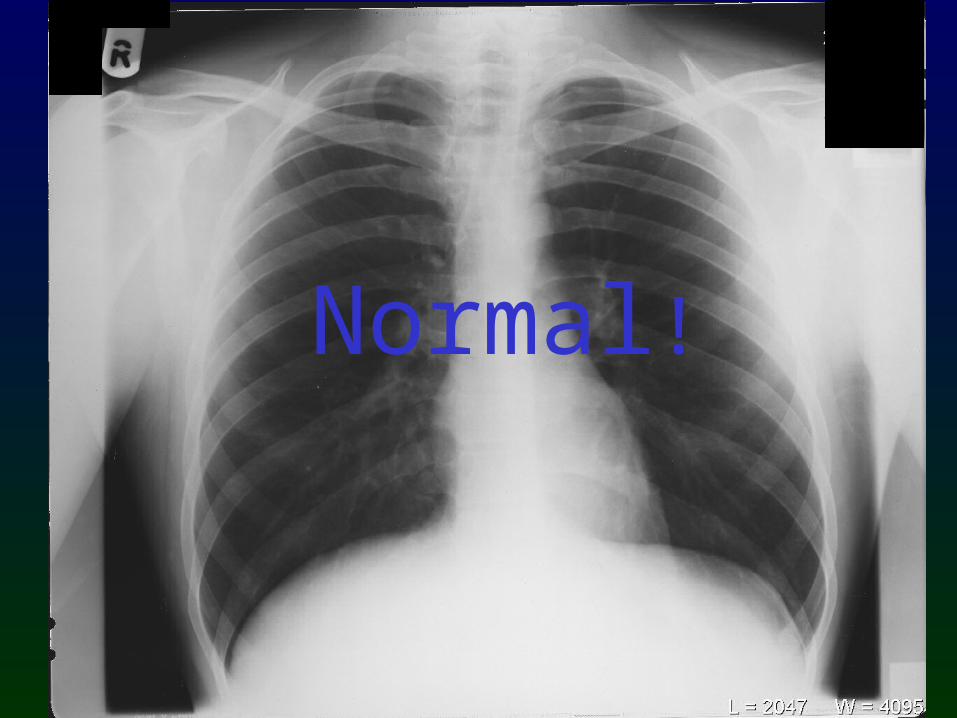
Normal!

Take Home Points
• Have a systematic approach to looking at a CXR
• Always interpret the CXR in conjunction with other clinical and investigative findings
• Always ask yourself “does my interpretation make sense?”
Related Documents











