Clinical and lab Clinical and lab aspect of anaerobic aspect of anaerobic infection infection ALI SOMILY MD ALI SOMILY MD

Clinical and lab aspect of anaerobic infection ALI SOMILY MD.
Jan 02, 2016
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Clinical and lab aspect of Clinical and lab aspect of anaerobic infectionanaerobic infection
ALI SOMILY MDALI SOMILY MD

ClassificationClassification1.1. Anaerobic spore forming bacilli Anaerobic spore forming bacilli
(Clostridia)(Clostridia)2.2. Gram negative bacilli non-sporing Gram negative bacilli non-sporing
(Bacteroides)(Bacteroides)3.3. Anaerobic streptococci Anaerobic streptococci
((PeptostreptococcusPeptostreptococcus))4.4. Anaerobic staphylococcus (Peptococcus)Anaerobic staphylococcus (Peptococcus)5.5. Gram negative diplococci (Veillonella)Gram negative diplococci (Veillonella)6.6. Gram positive bacilli (Actinomyces)Gram positive bacilli (Actinomyces)

PropionibacteriumPropionibacterium

BacteroidesBacteroides fragilisfragilis

FusobacteriumFusobacterium nucleatumnucleatum

AntimicrobiolialAntimicrobiolial SensitivitySensitivity
• All of them resistant to aminoglycosidesAll of them resistant to aminoglycosides– GentamicineGentamicine
– TobramycinTobramycin
– AmikacinAmikacin
• Almost all are sensitive to metranidazole Almost all are sensitive to metranidazole (flagyl)(flagyl)

AnaerobiosisAnaerobiosis
• Lack Lack cytochromecytochrome-cannot use oxygen as hydrogen -cannot use oxygen as hydrogen acceptoracceptor
• Most LackMost Lack– CatalaseCatalase– PeroxidasePeroxidase
• Contain Contain flavoproteinflavoprotein so in the presence of oxygen so in the presence of oxygen produce H2O2 which is toxicproduce H2O2 which is toxic
• Some lack enzyme superoxide dismutase so many Some lack enzyme superoxide dismutase so many killed , peroxide and toxic radicales enzyme like killed , peroxide and toxic radicales enzyme like fumarate reductase must be reduced form to workfumarate reductase must be reduced form to work

Anaerobic chamberAnaerobic chamber

NONSPORINGNONSPORING ANAEROBESANAEROBES

HABITATHABITAT I :I :
• These organism are normal flora in:These organism are normal flora in:
• A.A. OropharynxOropharynx• eg. 1. Bacteroides melaninogenicuseg. 1. Bacteroides melaninogenicus
Now called provetella melaninogenicus Now called provetella melaninogenicus
– 2. 2. FusobacteriaFusobacteria
– 3. 3. VeillonellaVeillonella

HABITAT IIHABITAT II::
• B.B. Gastrointestinal tractGastrointestinal tract
– Found mainly in the large colon in large numbersFound mainly in the large colon in large numbers– Total number of anaerobes = 10 Total number of anaerobes = 10 1111
– While all aerobes (including E. While all aerobes (including E. coli) = coli) = 10 10 44
– examples areexamples are (1) B acteroides fragilis(1) B acteroides fragilis (2) Bifidobacterium species(2) Bifidobacterium species
• C.C. Female genital tract (mainly in the vagina)Female genital tract (mainly in the vagina)

CLINICAL ASPECTS
• ANAEROBES ARE INDIGENOUS FLORA OF SKIN & MUCOUS MEMBRANES
• NORMALLY CONTAINED AWAY FROM INTERNAL STERILE BODY SITES
• HIGH MORBIDITY & MORTALITY

FEATURES OF ANAEROBIC FEATURES OF ANAEROBIC INFECTIONSINFECTIONS• Characterized by foul smellCharacterized by foul smell• Gas formationGas formation• Infections are always near to the site of the body which are Infections are always near to the site of the body which are
habitat.habitat.• Deep abscessesDeep abscesses• The infections are also polymicrobialThe infections are also polymicrobial• Failure to grow organism from pus if not culture Failure to grow organism from pus if not culture
anaerobically.anaerobically.• Failure to respond to usual antibiotics.Failure to respond to usual antibiotics.• Infection from animal bites.Infection from animal bites.• Detection of "Sulphur granules"' due to actinomycosisDetection of "Sulphur granules"' due to actinomycosis

INFECTIONS CAUSED INFECTIONS CAUSED BY ,NONSPORING ANAEROBESBY ,NONSPORING ANAEROBES
• A.A. The head, neck and respiratory tractThe head, neck and respiratory tract
• B. The lower abdomen and the pelvisB. The lower abdomen and the pelvis


INFECTIONS BEGIN
• DISRUPTION OF BARRIERS – TRAUMA
– OPERATIONS
– CANCEROUS INVASION OF TISSUES
• DISRUPTION OF BLOOD SUPPLY– DROPS OXYGEN CONTENT OF TISSUE
– DECREASE IN Eh POTENTIAL
– TISSUE NECROSIS

WHAT ARE THE INFECTION WHAT ARE THE INFECTION CAUSED BY THESE ANAEROBIC CAUSED BY THESE ANAEROBIC ORGANISMS IORGANISMS I
1.1. Post operative wound infectionPost operative wound infection
2.2. Brain abscessBrain abscess
3.3. Dental abscesses Dental abscesses
4.4. Lung abscessLung abscess
5.5. Intra abdominal abscess, appendicitis, Intra abdominal abscess, appendicitis, diverculitis diverculitis
6.6. All these infection can cause bacteriaemiaAll these infection can cause bacteriaemia

WHAT ARE THE INFECTION WHAT ARE THE INFECTION CAUSED BY THESE ANAEROBIC CAUSED BY THESE ANAEROBIC ORGANISMS IIORGANISMS II
1.1. Infection of the female genital tractInfection of the female genital tract
2.2. Septic abortionSeptic abortion
3.3. PuerperalPuerperal infection or sepsisinfection or sepsis4.4. EndometritisEndometritis5.5. Pelvic abscessPelvic abscess
6.6. 12. Other infections12. Other infections– a)a) Breast abscess in puerperal sepsisBreast abscess in puerperal sepsis– b) Infection of diabetic patients (diabetic foot infections).b) Infection of diabetic patients (diabetic foot infections).– c) Infection of pilonidal sinusc) Infection of pilonidal sinus

LABORATORY DIAGNOSIS:LABORATORY DIAGNOSIS:
• When anaerobic infection is suspected;When anaerobic infection is suspected;– a) Specimens have to be collected from the site a) Specimens have to be collected from the site
containing necrotic tissue.containing necrotic tissue.– b) Pus is better than swabs.b) Pus is better than swabs.– c) Specimens has to be send to the laboratory within c) Specimens has to be send to the laboratory within
1/2 hour why?1/2 hour why?– d) Fluid media like cooked meat broth are the best d) Fluid media like cooked meat broth are the best
culture media.culture media.– e) Specimens have to incubated anaerobically for 48 e) Specimens have to incubated anaerobically for 48
hours.hours.

TREATMENT:TREATMENT:
• Bacteroides fragilisBacteroides fragilis is always resistant to is always resistant to penicillin. penicillin.
• But penicillin can he used for other But penicillin can he used for other anaerobesanaerobes
• Flagyl (metronidazole) is the drug of choice. Flagyl (metronidazole) is the drug of choice.
• Clindamycin can also be used.Clindamycin can also be used.

ORAL & DENTAL
• > 400 SPECIES OF ANO2 IN MOUTH
• MOST INFECTIONS = POLYMICROBIC– MIXED ORGANISMS
– ENTER AS A GROUP
• ANO2 NOT INITIAL INVADER– USUALLY SECONDARY
– 1ST ORGANISM DECREASES [O2] & Eh

ORAL & DENTAL
• COMMONLY ASSOCIATED WITH1. DENTAL ABSCESSES
2. ROOT CANALS
3. JUVENILE PERIODONTITIS
4. ADULT PERIODONTITIS
5. CLENCHED FIST INJURIES

ENT – HEAD & NECK
1. CHRONIC OTITIS MEDIA
2. CO-PATHOGENS WITH CHRONIC STREP TONSILLITIS
3. ACUTE SINUSITIS– POST-DENTAL EXTRACTIONS OR
TRAUMA
– 2o INVADER

ENT – HEAD & NECK
• VINCENT’S ANGINA– COMBINATION OF FUSOBACTERIUM &
SPIROCHETE SPECIES OVERGROWTH
– ANAEROBIC PHARYNGITIS
– GRAY MEMBRANE
– FOUL ODOR

Vincent’s diseaseVincent’s disease
• Trench mouthTrench mouth
• Sudden onset of pain in the gingiva (mastication)Sudden onset of pain in the gingiva (mastication)
• Necrosis of the gingivaNecrosis of the gingiva– interdental papillainterdental papilla
– a marginated, punched-out, and eroded appearancea marginated, punched-out, and eroded appearance
• A superficial grayish pseudomembraneA superficial grayish pseudomembrane
• altered taste sensation is presentaltered taste sensation is present
• Fever, malaise, and regional lymphadenopathyFever, malaise, and regional lymphadenopathy

Ludwig’s AnginaLudwig’s Angina

Lemierre SyndromeLemierre Syndrome

Expansion of the retropharyngeal soft Expansion of the retropharyngeal soft tissuestissues

PLELRO PULMONARY I FECTIONPLELRO PULMONARY I FECTION
• ASPIRATION PNEUMONIAASPIRATION PNEUMONIA
• ASPIRATION LUNG ABSCESSASPIRATION LUNG ABSCESS
• M ETASTATIC LUNG ABSCESS M ETASTATIC LUNG ABSCESS
• BRONCHIACTSISBRONCHIACTSIS
• ALL OF ABOVE CAN CAUSE ALL OF ABOVE CAN CAUSE EMPYEMAEMPYEMA
• MALIGNANCIES LEUKOPENIA

THORACIC ACTINOMYCOSISTHORACIC ACTINOMYCOSIS

THORACIC ACTINOMYCOSISTHORACIC ACTINOMYCOSIS

ACTINOMYCOSISACTINOMYCOSIS

Molar tooth appearance of Molar tooth appearance of Actinomyces israeIiiActinomyces israeIii

Macroscopic colony (left) Macroscopic colony (left) Gram stain (right) of ActinomycesGram stain (right) of Actinomyces

SKIN & SOFT TISSUE
• TRAUMATIZED & DEVITALIZED TISSUE
1. TRAUMATIC WOUNDS
2. HUMAN/ANIMAL BITES
3. ISCHEMIA OF EXTREMITIES• DIABETES
• ATHEROSCLEROSIS

CLENCHED FIST INJURIES

DIABETIC FOOTDIABETIC FOOT

HUMAN BITEHUMAN BITE

NECROTIZING CELLULITISNECROTIZING CELLULITIS

FEMALE UROGENITAL
• CHORIOAMNIOTIC INFECTIONS
• ENDOMETRITIS
• PID – ABDOMINAL INFECTIONS
• BACTERIAL VAGINOSIS WITH GARDNERELLA & BACTEROIDES SP.

PUERPERAL INFECTION SEPTIC PUERPERAL INFECTION SEPTIC ABORTIONABORTION
• PUERPERAL ABSCESS PUERPERAL ABSCESS • SEPTIC ABORTIONSEPTIC ABORTION• BACTERAEMIABACTERAEMIA
• PELVIC ABSCESS PELVIC ABSCESS • ADENXAL ABSCESS ADENXAL ABSCESS • PERITONITISPERITONITIS• ENDOMETRITIS ENDOMETRITIS

ABDOMINAL INFECTIONS
• MANIPULATION, INVASION OR TRAUMA TO GI TRACT
1. TRAUMA
2. SURGERY
3. APPENDICITIS
4. MALIGNANCIES• COLON CANCER

CNS
1. HEAD TRAUMA
2. HEMATOGENOUS SPREAD– FROM ANY INFECTED BODY SITE
3. GEOGRAPHIC SPREAD– SINUS INFECTIONS
– DENTAL ABSCESSES

BONE & JOINT
• HEMATOGENOUS SPREAD
• TRAUMA
• PERIVASCULAR DISEASE
• JUVENILE PERIODONTITIS

OTHEROTHER INFECTIONSINFECTIONS
• GRAM NEGATIVE BACTREMIAGRAM NEGATIVE BACTREMIA
• BREAST ABSCESSBREAST ABSCESS
• AXILLARY ABSCESSAXILLARY ABSCESS
• INFECTION OF DIABETIS EG.DIABETIC INFECTION OF DIABETIS EG.DIABETIC ULCERSULCERS
• INFECTION OF PILONIDAL SINUS INFECTION OF PILONIDAL SINUS
• PARONYCHIAPARONYCHIA

CLASSIFICATIONCLASSIFICATION1.1. Anaerobic spore forming bacilli Anaerobic spore forming bacilli
(Clostridia)(Clostridia)2.2. Gram negative bacilli nonsporing Gram negative bacilli nonsporing
(Bacteroides)(Bacteroides)3.3. Anaerobic streptococci Anaerobic streptococci
(Peptostreptococcus)(Peptostreptococcus)4.4. Anaerobic staphylococcus (Peptococcus)Anaerobic staphylococcus (Peptococcus)5.5. Gram negative diplococci (Veillonella)Gram negative diplococci (Veillonella)6.6. Gram positive bacilli (Actinomyces)Gram positive bacilli (Actinomyces)

ORGANISM GROUPS
• GRAM NEGATIVE RODS– BACTEROIDES
– PREVOTELLA
– PORPHYROMONAS
– FUSOBACTERIUM
– BUTYRIVIBRIO
– SUCCINOMONAS

Bacteroides fragilisBacteroides fragilis

BACTEROIDESBACTEROIDES
• STRICT ANAEROBESTRICT ANAEROBE• PLEOMORPHICPLEOMORPHIC• GRAM NEGATIVE BACILLI (COCCO GRAM NEGATIVE BACILLI (COCCO
BACILLI)BACILLI)• NORMAL FLORA INNORMAL FLORA IN
– OROPHARYNXOROPHARYNX– GASTROINTESTINAL TRACTGASTROINTESTINAL TRACT– VAGINAVAGINA

BACTEROIDES FRAGILIS GP
• GROUP = B. FRAGILIS, B. VULGARIS, B.THETAIOTAMICRON, B. UNIFORMIS– ACCOUNT FOR 1/3 OF ALL ISOLATES
– RESISTANT TO 20% BILE
– RESISTANT TO MANY ANTIBIOTICS• PENICILLIN, KANAMYCIN, VANCOMYCIN,
COLISTIN – AND MANY MORE

BACTEROIDES FRAGILIS GP
• GLC = MAJOR ACETIC & SUCCINIC, LACTIC & PROPIONIC ACIDS
• NO PIGMENTATION OF COLONIES OR FLUORESCENCE

BACTEROIDES OTHER SP
• BACTEROIDES SPECIES OTHER, NOT B. FRAGILIS GROUP– GLC = MAJOR ACETIC & SUCCINIC ONLY
– BILE SENSITIVE
– RESISTANT TO KANAMYCIN ONLY
– SOME PIGMENTED

BACTEROIDESBACTEROIDES
• B. FRAGILIS B. FRAGILIS IN THE GUT AND VAGINAIN THE GUT AND VAGINA• B.MELANINOGESUS AND B.ORALIS B.MELANINOGESUS AND B.ORALIS IN IN
THE MOUTH AND OROPHARYNXTHE MOUTH AND OROPHARYNX• B. FRAGILIS PENICILLIN B. FRAGILIS PENICILLIN RESISTANTRESISTANT, , • OTHER ARE OTHER ARE SENSITIVE,SENSITIVE, • IT IS THE IT IS THE COMMONESTCOMMONEST ORGANISM IN ORGANISM IN
THE GUT 10 THE GUT 10 1212 ORGANISM /GRAM OF ORGANISM /GRAM OF FAECESFAECES

Bacteroides and other anaerobic bacilliBacteroides and other anaerobic bacilli

BACTEROIDES AND BACTEROIDES AND FUSOBCTERIUMFUSOBCTERIUM
B.FRAGB.FRAG B.NECROPB.NECROPHORUSHORUS
B.MELANINB.MELANINOGENICUSOGENICUS
B.CORRODB.CORRODENSENS
FUSOBACTFUSOBACTERIUMERIUM
BLACKBLACK
PIG.PIG.-- -- ++ -- --
PITTINGPITTING -- -- -- ++ --INDOLE+INDOLE+ -- -- ++ -- --LYSINE+LYSINE+ ++BILE GROWTHBILE GROWTH ++

Growth of Growth of Bacteroides fragilisBacteroides fragilis on on Bacteroides bile-esculin agarBacteroides bile-esculin agar

Bacteroides fragilisBacteroides fragilis
• Special-potency kanamycin, Special-potency kanamycin, vancomycin, and colistin vancomycin, and colistin antimicrobial agent disks to antimicrobial agent disks to first quadrant of this plate. first quadrant of this plate.

PORPHYROMONAS
• GLC = ACETIC, SUCCINIC PLUS PROPIONIC, BUTYRIC, ISOBUTYRIC,& ISOVALERIC
• BILE SENSITIVE
• USUALLY BLACK PIGMENTED COLONIES– P. GINGIVALIS, P. ENDODONTITIS &
P.ASACCHAROLYTICA

PREVOTELLA
• GLC = ACETIC, SUCCINIC, ISOVALERIC, NO BUTYRIC
• BILE SENSITIVE
• BLACK PIGMENT & FLUORESCENCE– Pr. INTERMEDIA – LIPASE +
– Pr. MELANINOGENICA – BRICK RED FLUORESCENCE

FUSOBACTERIUM
• GLC = ACETIC, PROPIONIC, &BUTYRIC, NO SUCCINIC
• ANTIBIOTICS– SENSITIVE TO KANAMYCIN
– RESISTANT TO VANCOMYCIN
– COLISTIN VARIABLE

Fusobacterium nucleatumFusobacterium nucleatum

FUSOBACTERIUM
• F. NUCLEATUM = LIPASE Ø
• F. NECROPHORUM = LIPASE +
• F. NUCLEATUM >> F. NECROPHORUM ISOLATES
• COMMON IN ASPIRATION PNEUMONIAS

MISCELLANEOUS GNB
• BUTYRIVIBRIO– CURVED GNB
– GLC = MAJOR BUTYRIC
• SUCCINOMONAS– CURVED GNB
– GLC = ACETIC & SUCCINIC

PEPTOCOCCUS NIGER
• GRAM POSITIVE COCCI
• GLC = ACETIC, BUTYRIC, ISOBUTYRIC, ISOVALERIC, CAPROIC
• BLACK PIGMENT

PEPTOSTREPTOCOCCUS
• GRAM POSITIVE COCCI
• GLC = ACETIC, SOME BUTYRIC
• Ps. ASACCHAROLYTICUS INDOLE +
• Ps. ANAEROBIUS, Ps. MAGNUS, Ps.PREVOTI, Ps. INDOLECUS

STREP & STAPH
• ANAEROBIC SPECIES OF STAPH AND STREP
• STREPTOCOCCUS INTERMEDIUS
• STAPHYLOCOCCUS SACCHAROLYTICUS
VEILLONELLA PARVULA
• GRAM NEGATIVE COCCI
• GLC = ACETIC & PROPIONIC
• NITRATE +
• HEAD AND NECK INFECTIONS
• DENTAL ABSCESSES

CLOSTRIDIACLOSTRIDIA

CLOSTRIDIUM SPECIES
• LARGE GRAM POSITIVE RODS
• SPORE FORMATION
• SPECIFIC DISEASES– PSEUDOMEMBRANOUS COLITIS
– TETANUS
– BOTULISM
– GANGRENE - MYONECROSIS

C. difficileC. difficile

CLOSTRIDIACLOSTRIDIA
• Causative Agents ForCausative Agents For– 1.G1.Gas gangreneas gangrene :: Cl. Cl. perfringensperfringens and other and other
e.g e.g C.septicum C.septicum
– 2.2.TetanusTetanus : : Cl. Cl. tetanitetani
– 3.3.BotulismBotulism : : Cl. Cl. botulinumbotulinum
– 4.4.Toxic enterocolitisToxic enterocolitis : : Cl. Cl. difficiledifficile (Pseudomembernous colitis)(Pseudomembernous colitis)

Clostridium perfringensClostridium perfringens (CI . welchii) (CI . welchii)
• Morphology large rods gram +ve Morphology large rods gram +ve
• With bulging endosporesWith bulging endospores
• Not motileNot motile
• CapsulatedCapsulated

Clostridium perfringensClostridium perfringens

C. perfringensC. perfringens

C. perfringensC. perfringens

Culture:Culture:
• A)A) Blood agar with haemolytic colonies Blood agar with haemolytic colonies (double zone of (double zone of haemolysishaemolysis
• B)B) Cooked meat mediumCooked meat medium
• Gives the NAGLAR'S Reaction & toxin Gives the NAGLAR'S Reaction & toxin neutralization on Egg yolk medium & toxin is neutralization on Egg yolk medium & toxin is a phospholipase a phospholipase

C. C. perfringensperfringens

NAGLAR'S ReactionNAGLAR'S Reaction

Lipase and/or lecithinase (EYA),Lipase and/or lecithinase (EYA),

Diseases Caused by C.Diseases Caused by C. perfringensperfringens
• 1) Wound Contamination1) Wound Contamination• 2) Wound infection2) Wound infection• 3) 3) Gas GangreneGas Gangrene - most important disease - most important disease• 4) Gas Gangrene of the uterus in criminal abortion4) Gas Gangrene of the uterus in criminal abortion• 5) Food Poisoning5) Food Poisoning
• Spores are swallowed Germinate in gut after 18 hoursSpores are swallowed Germinate in gut after 18 hours• ToxinToxin• abdominal pain and diarrhoeaabdominal pain and diarrhoea

GAS GANGRENEGAS GANGRENE
• CausesCauses mainly mainly – (Cl perfringens) (Cl. welchil)(Cl perfringens) (Cl. welchil)– CI. novyl, CI. novyl, – CI. SepticumCI. Septicum– CI oedemaritiansCI oedemaritians
• Pathogenesis:Pathogenesis:– Traumatic open wounds Traumatic open wounds – Compound fractures Compound fractures – Muscle damagesMuscle damages– Contamination with dirt etc, Contamination with dirt etc,
• Mainly in war wounds,Mainly in war wounds,
• Old age, Old age, – Low blood supplyLow blood supply
• Amputation of thighAmputation of thigh– Prophylaxis with Prophylaxis with
penicillinpenicillin

NECROTIZING FASCIATITISNECROTIZING FASCIATITIS

NECROTIZING FASCIATITISNECROTIZING FASCIATITIS

MYOSITISMYOSITIS

Gram Stain of vaginal aspirateGram Stain of vaginal aspirate
1. Clostridiae necrotizing (myonecrosis)

Prevention and TreatmentPrevention and Treatment
• Remove dead tissue Remove dead tissue
• Remove debrisRemove debris
• Foreign bodiesForeign bodies
• PenicillinPenicillin
• Hyperbaric oxygenHyperbaric oxygen

TETANUSTETANUS

Cl.tetaniCl.tetani
• Causative organism Causative organism Cl.tetaniCl.tetani• Morphology gram +ve anaerobic with terminal spore Morphology gram +ve anaerobic with terminal spore
Drum Stick appearanceDrum Stick appearance• Lives in soil and animal feaces. e,g horse Lives in soil and animal feaces. e,g horse • ProduceProducess a powerful exotoxin tetanospasmin a powerful exotoxin tetanospasmin • Toxin is a protein,Toxin is a protein,• It inhibits transmission of normal inhibitory messages It inhibits transmission of normal inhibitory messages
from central nervous system at anterior horn cells of from central nervous system at anterior horn cells of cordcord

C. tetaniC. tetani

Clinical patterns:Clinical patterns:
• Generalized Generalized
• Local Local
• Cephalic Cephalic
• Neonatal Neonatal
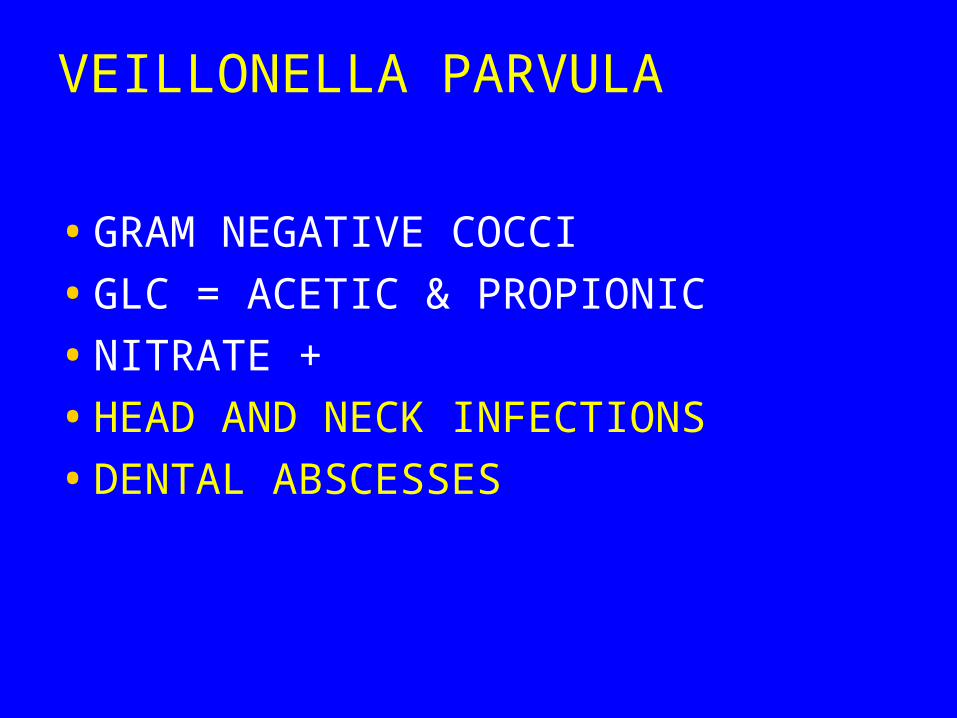
Clinical FeaturesClinical Features
• Incubation period 1-2 weeksIncubation period 1-2 weeks• Symptoms: Painful muscle spasm around infected Symptoms: Painful muscle spasm around infected
wound wound • Contraction of muscles Contraction of muscles of face=of face=
– TrismusTrismus ( (Lockjaw)Lockjaw)– Risus SardonicusRisus Sardonicus
• BackBack– Araching of Back Araching of Back

OpisthotonusOpisthotonus

PathogenesisPathogenesis
• 1 )1 ) Tetanospasmin and TotanolysinTetanospasmin and Totanolysin• 1)1) Tetanospasmin most important Tetanospasmin most important • No invasion or BacteraerniaNo invasion or Bacteraernia• ToxinToxinAnterior horn cell of Spinal CordAnterior horn cell of Spinal Cord• Any wound can infected if contaminated by Any wound can infected if contaminated by
sporesspores• Face & neck wounds are more dangerous Face & neck wounds are more dangerous
why ?why ?

PathogenesisPathogenesis

DiagnosisDiagnosis
• Mainly by clinical Mainly by clinical
• Laboratory not importantLaboratory not important
• LabLab– Organism strict anaerobeOrganism strict anaerobe
– Very motile , spread on agar.Very motile , spread on agar.

C. C. tetanitetani

PreventionPrevention
• Toxoid vaccine:Toxoid vaccine:
• Vaccination D P TVaccination D P T
• 2 , 4 , 6 , 18 months &2 , 4 , 6 , 18 months & 5 Year5 Year
• Booster every 10 yearsBooster every 10 years

TreatmentTreatment . .
• Cleaning of wound Cleaning of wound • Removal of Foreign body Removal of Foreign body • Specific by antitoxinSpecific by antitoxin
– Horse serum can caused anaphylaxis & shock Horse serum can caused anaphylaxis & shock must be tested firstmust be tested first
– Human immunoglobulinHuman immunoglobulin– Antibiotics . PenicillinAntibiotics . Penicillin
• Supportive treatmentSupportive treatment– 2. 2. Dark pace, fluidsDark pace, fluids– 3. Sedative valium3. Sedative valium

CLOSTRIDIUM BOTULINUIMCLOSTRIDIUM BOTULINUIM

HabitatHabitat
• Soil,Ponds AND LakesSoil,Ponds AND Lakes

BotulismBotulism
• FromFrom vegetables, fruits, seafood, and in soil vegetables, fruits, seafood, and in soil and marine sediment worldwide canned food., and marine sediment worldwide canned food.,
• Not well cooked Not well cooked
• Spores resist heat at 100 Spores resist heat at 100 ooCCthen multiply and produce toxinthen multiply and produce toxin

Botulism PatogenesisBotulism Patogenesis
• Ingested - incubation period 12-36 hourIngested - incubation period 12-36 hour
• 8 Types8 Types
• Mainly types Mainly types A, B, E, F and GA, B, E, F and G
• Attacks neuromuscular junctionsAttacks neuromuscular junctions
• Prevents release of acetylcholinePrevents release of acetylcholine

ToxinToxin
• ExotoxinExotoxin• ProteinProtein• Heat labile at 100 Heat labile at 100 OOCC
– The most powerful toxin known Lethal dose 1 µg The most powerful toxin known Lethal dose 1 µg humanhuman
• 3 kg kill all population of the world 3 kg kill all population of the world • Dictated for by lysogenic phage Dictated for by lysogenic phage • Resist gastrointestinal enzymesResist gastrointestinal enzymes

FormsForms
• Food-borne botulism Food-borne botulism
• Infant botulism Infant botulism
• Wound botulism Wound botulism
• Adult enteric infectious botulism Adult enteric infectious botulism
• Inhalational botulism Inhalational botulism

ENFANTILE BOTULISMENFANTILE BOTULISM
• Ingestion of Ingestion of Spores Spores germination in the germination in the gutgutBotulismBotulism
• Week childWeek child
• Cranial nerveCranial nerve
• ConstipationConstipation
• OtherOther

SymptomsSymptoms
• Abnormal eye movement as if cranial nerve Abnormal eye movement as if cranial nerve affected when bulbar area of the brain affectedaffected when bulbar area of the brain affected
• Respiratory and circulatory collapseRespiratory and circulatory collapse

SPECIMENSSPECIMENS
• Suspected food Suspected food
• From the patientFrom the patient– Faeces growthFaeces growth
– SerumSerum
• Toxin detection by mouseToxin detection by mouse– incubation paralysis and deathincubation paralysis and death

INFANTILE BOTULISMINFANTILE BOTULISM
• Week lethargic child Week lethargic child
• ConstipationConstipation
• Respiratory and cardiac arrestRespiratory and cardiac arrest
• Due to colonization of intestine by Due to colonization of intestine by CI. CI. botulinumbotulinum
• Diagnosis by -Diagnosis by - Culture of stoolsCulture of stools
• Detection of toxin in feacesDetection of toxin in feaces

• TreatmentTreatment
• 1) Supportive1) Supportive
• 2) Horse antitoxin2) Horse antitoxin
• PreventionPrevention
• 1)1) Adequate Adequate pressure cooking pressure cooking autoclavingautoclaving
• 2)2) Heating of food Heating of food for 10 minutes at 100 for 10 minutes at 100 OOCC

BotoxBotox
C. DIFFICILE
• PSEUDOMEMBRANOUS COLITIS– 90% OF CASES CAUSED BY C. DIFF
– LONG TERM TREATMENT WITH BROAD SPECTRUM ANTIBIOTICS OR CHEMO• NOSOCOMIAL DISEASE
• KNOCK DOWN NORMAL FLORA
• CLINDAMYCIN, AMPICILLIN, CEPHALOSPORINS
• CHEMOTHERAPEUTIC AGENTS

C. DIFFICILE
• OVERGROWTH OF C. DIFFICILE– TOXIN THEN PRODUCED
• A FRAGMENT = ENTEROTOXIN
• B FRAGMENT = CYTOLYTIC TOXIN
• PSEUDOMEMBRANE SIMILAR TO THAT OF C. DIPHTHERIAE– BACTERIA, FIBRIN, WBC, DEAD
– TISSUE CELLS - TOUGH

C. DIFFICILE
• DIARRHEA FIRST– ELECTROLYTE & FLUID LOSS
– LEADS TO DEHYDRATION
• INTESTINAL BLOCKAGE– CONTENTS BLOCKED
– COLON BULGES
• PERFORATION, RUPTURE SEPSIS

Clinical picturesClinical pictures

C. DIFFICILE
• RAPID AGGRESSIVE COURSE IN YOUNG CHILDREN
• DIFFICULT TO SELECTIVELY
• CULTURE– 5-10% CULTURE + EVEN WITH CONFIRMED
DISEASE
– TOO MANY NORMAL ANO2 PRESENT

C. DIFFICILE
• SPECIALIZED ISOLATION MEDIA– CCFA – CYCLOSERINE ,
CEFOXITIN,FRUCTOSE, EGG YOLK AGAR
– CCMA – CCFA BUT MANNITOL FOR FRUCTOSE
– CDMN – CYSTEINE HYDROCHLORIDE, MOXALACTAM, NORFLOXACIN AGAR

C. difficileC. difficile

C. difficileC. difficile

C. DIFFICILE
• C. DIFFICILE IS NORMAL FLORA– ISOLATION NOT ENOUGH
• NEED TOXIN ASSAY TO CONFIRM
• CELL-FREE STOOL EXTRACT– LATEX AGGLUTINATION SCREEN
• SOME CROSS-REACTIVITY
– EIA TO CONFIRM

Major Clostridial DiseasesMajor Clostridial Diseases
Related Documents