I can’t swallow! A tutorial covering the history taking and examination process, for patients presenting with dysphagia. INTRODUCTION When presented with a patient who appears to have difficulty or pain when swallowing (dysphagia) the underlying pathology will only be revealed by a careful and detailed history. Examination of the patient often demonstrates signs, but these are generally less helpful than the details of the history. This tutorial helps you to learn how to go about this process and gives you opportunity to revise relevant anatomy, physiology and pathology if you wish to. Management of these patients is also briefly summarised. You should complete the tutorial during your attachment to med/surg B and then assess your knowledge by

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

I can’t swallow!
A tutorial covering the history taking and examination process, for patients presenting with dysphagia.
INTRODUCTION
When presented with a patient who appears to have difficulty or pain when swallowing (dysphagia) the underlying pathology will only be revealed by a careful and detailed history. Examination of the patient often demonstrates signs, but these are generally less helpful than the details of the history.
This tutorial helps you to learn how to go about this process and gives you opportunity to revise relevant anatomy, physiology and pathology if you wish to. Management of these patients is also briefly summarised.
You should complete the tutorial during your attachment to med/surg B and then assess your knowledge by completing the dysphagia quiz (link). This is a formative assessment designed to help you to learn more and your score isn’t counted towards a final mark. However you MUST complete the task before the end of the unit. When you’ve finished it, our central records will confirm completion. You will be told your mark immediately, which will give you some feed back on your performance.

AIMS AND OBJECTIVES:
Aims:
1) To understand the reasoning behind taking a history and examining a patient presenting with dysphagia.
2) To begin to consideration of patient management issues.
Objectives:
This describes what you should be able to do by the end of the tutorial:
1) Formulate a list of potential differential diagnoses causing dysphagia
2) Formulate a list of questions you would ask a patient to establish the presence of dysphagia and the pathology behind it.
3) To examine a patient in a logical sequence, being able to focus on systems relevant to dysphagia
4) To consider salient management issues for a patient with dysphagia. This area is not essential at your stage of training, but will be in the near future!
HISTORY TAKING:
In establishing that a patient actually has dysphagia, you may need to use a variety of questions, as patients interpret their symptoms in many different ways. In essence you’re just finding out from the patient whether there is a problem with food getting from the mouth to the stomach.

Mr Adam Pain has arrived at your GP practice. You are the GP trainee seeing him.
What questions could you ask Mr Pain to establish whether he has ‘dysphagia’? You should think of at least 3 different ways of asking this.
<question textentry2><title>Establishing dysphagia</title><text> What could you ask Mr Pain to establish whether he has ‘dysphagia’?</text>
<feedback>
These are a few suggestions:1) Do you have any difficulty swallowing food or liquid?2) What happens when you swallow solid food?3) Do you find that food ‘sticks’ on the way down?4) Is this any pain or discomfort when you swallow?
</feedback></question>

Now you’ve established the presence of ‘dysphagia’ you need to work out where the pathology lies.
Anatomy-Oropharynx
Label the structures on the diagrams below, which demonstrate
structures that may be involved in oropharyngeal causes of dysphagia:

Diagram 2
Diagram 1
1) Tongue [link to innervation question]2) Soft palate3) Hard palate4) Palatine tonsil 5) Epiglottis6) Pharynx [link to anatomy]
Diagram 2
7) Uvula8) Palatine tonsil9) Pharyngopalatine Arch10)Glossopalatine Arch
Complete the empty boxes in the diagram to show relevant tongue innervation:

Sensation: Taste: Motor:
TONGUE -
Posterior 1/3 A: (IX)(IX) (V)Glosso Glosso
Lingual
Anterior 2/3
A: (V) (VII) (V)Lingual Chorda tympani
Lingual
Anatomy-Pharynx
For each gap in the text below, select the most appropriate word(s).:
The pharynx extends from the base of the skull to the inferior border of the [5th ,6th, 7th] cervical vertebra, level with the [thyroid cartilage, cricoid cartilage, first tracheal ring ].
Its narrowest part is [opposite the hyoid bone, at its inferior end, at the thryroid cartilage].
The pharynx is composed of [2, 3, 4] layers of muscle, the most external of which is made up by the [constrictor, vertebral, paravertebral] muscles, which have a major role in the swallowing process.
Contraction of these muscles is [voluntary, involuntary] and occurs [sequentially, randomly], stimulated by a bolus of food entering the oropharynx.
Innervation of the pharynx is by the [pharyngeal plexus, facial nerve, hypoglossal nerve]

Anatomy-Oesophagus
Why don’t you check how well you remember your anatomy?
<question truefalse1><text true> It starts at the lower end of the pharynx:</text>
<feedback correct> Well done</feedback><feedback incorrect>As you know, the pharynx and the oesophagus are in continuity</feedback>
</question>
<question truefalse1><text false> It is a muscular tube with voluntary innervation </text>
<feedback correct> Well done</feedback><feedback incorrect>It is made up of involuntary smooth muscle</feedback>
</question>
<question truefalse1><text false> It lays anterior to the trachea in the mediastinum </text>
<feedback correct> Well done</feedback><feedback incorrect> Posterior. Remember the organisation of the larynx and pharynx. They maintain their position in the mediastinum </feedback>
</question>
<question truefalse1><text true> It pierces the diaphragm just to the left of the median plane
</text>
<feedback correct> Well done</feedback>

<feedback incorrect>Sorry, have a look at this diagram of structures that pass through the diaphram and think again </feedback>
</question>
<question truefalse1><text false> It enters the cardia of the stomach at T12 </text>
<feedback correct> Well done</feedback><feedback incorrect>Are you sure, remember that it enters at the level of the 7th costal cartilage and T10 </feedback>
</question>
<question truefalse1><text true> It is innervated by the oesophageal plexus
</text>
<feedback correct> Well done</feedback><feedback incorrect>This is a combination of </feedback>
</question>
<question truefalse1><text false> Blood supply originates from the superior mesenteric artery
</text>
<feedback correct> Well done</feedback><feedback incorrect>Are you sure, remember that it is supplied by branches from the aorta, left gastric artery and left inferior phrenic artery </feedback>
</question>

If its all greek to you, you need to revise your anatomy in more detail. The links below are far too detailed, but provide useful diagrams.
In the window below showing the bartleby.com website, scroll down to find chapter XI and the links to mouth tonsils . pharynx and oesophagus
<include><size>big</size>
http://www.bartleby.com/107/
</include>

Swallowing (Deglutition)
Do you need a reminder about the physiology of swallowing?
Click here to review the voluntary oral stage
Click here to view the Pharyngeal stage
Click here to view the Oesophageal stage
Please complete the following phrases, by selecting the correct word:
<popup>
<size>scrolling</size>
After mastication, food bolus is rolled posteriorly into pharynx by pressure of tongue upward and backward against palate.scrolling

</popup>
<popup>
<size>scrolling</size>
Pharyngeal Stage
The bolus of food enters pharynx, stimulating swallow receptor areas all around the opening of the pharynx. Impulses pass to the brainstem and a series of automatic pharyngeal muscle contractions are triggered:
1. Soft palate pulled upwards and closes the posterior nares2. Palatopharyngeal folds either side of the pharynx pulled medially to only allow masticated food to pass through3. Vocal folds strongly approximated, larynx pulled up and anterior. Epiglottis swings posteriorly to cover the entrance to the larynx.4. Relaxation of the Upper Oesophageal Sphincter.5. Contraction of the muscular pharyngeal wall, causing a rapid peristaltic wave propelling food bolus into oesophagus.
</popup>
<popup>
<size>scrolling</size>
Oesophageal Stage
The oesophagus exhibits two types of peristaltic movements.

Primary peristalsis is a continuation of the wave formed in the
pharynx (see above). Passes from pharynx to stomach in 8-10
seconds. Secondary peristaltic wave occurs when primary wave
fails to propel bolus into stomach. It is initiated by distension of
the oesophagus by the remaining food bolus, and continues until
the bolus has been propelled into the stomach.
</popup>
IMPAIRMENT AT ANY OF THESE STAGES OF DEGLUTITION CAN RESULT IN SWALLOWING DIFFICULTIES. (I.e.: Problems affecting the tongue, mouth, tonsils, palate, pharynx, larynx, vocal cords, oesophagus and gastro-oesophageal junction.
This is where your history taking will provide you with the answers.
History –establishing course of symptoms:
Now that you have established that the patient does in fact have dysphagia, you need to lead your history taking in a way that will localise the pathology causing the symptoms:
In other words which questions will you ask?<question textentry2>
<title>Course of symptoms</title>
<text> How will you establish the onset, duration and subsequent course of
Mr Pain’s symptoms? </text><feedback>
These are suggested answers Is the problem staying about the same, progressively worsening, or intermittent? (I.e. COURSE of the condition)

Do you have difficulty swallowing food or liquids or both? Can you manage to swallow your own saliva? What CAN you swallow? (SEVERITY of symptoms)How quickly did these symptoms develop? Over hours, days, weeks, or months? (Onset of symptoms)</feedback>
</question>
The suggestions in the feedback to the above question are basic, essential questions, which start to shape the picture of your patient’s compliant. For example, acute inflammatory conditions present with acute onset symptoms over hours to days, of varying severity and are not usually progressive, whereas many neurological causes have a slowly progressive course.
Regarding the progression of symptoms, malignant diseases tend to follow a relentlessly progressive course, the patient initially finding it difficult to swallow solids, then liquids and finally their own saliva. Foreign body (e.g. meat bolus) occlusion is associated with a sudden complete inability to swallow and therefore has an immediate onset of symptoms.
When the patient describes pain or the sensation of a lump in the throat that prevents swallowing but is also present when NOT swallowing, the cause could be a sore throat associated with tonsillitis or Globus Hystericus.
SITES: Mapping the problem
Pathology of dysphagia relating to the different sites of the upper GI tract:
The patient often knows exactly where the problem is located if you ask them. That won’t help you if you don’t have a list of potential causes in your head relating to different sites of potential pathology from mouth to stomach.

1)
<question textentry1><text> Write a comprehensive list of causes of dysphagia relating to the following areas, not including neurological causes (we will deal with those later):
2) Mouth:3) PharynxOesohagus </text>
<feedback>To check your answers, move the mouse over the relevant areas of the diagram below. </feedback>
</question>
To check your answers, move the mouse over the relevant areas on the diagrams below.
(Scanned graphic of a cross section with a ‘roll over’)

Mouth: Aphthous ulcers
Candida
Tonsilitis
Macroglossia (pathologically large tongue e.g. Downs syndrome)
Tonsillar hypertrophy
Tumours of the mouth, tonsils and tongue
Pharynx: Pharyngeal pouch
Tumour of the pharynx
Pharyngitis
Oesophagus: Diffuse oesophageal spasm
Achalasia
Scleroderma
dermatomyositis
Extrinsic compression -Tumours of the head and neck,
-Enlarged mediastinal lymph nodes
-Thyroid enlargement
- Enlarged right atrium
Intrinsic tumours (Squamous cell or adeno- carcinoma)
Benign oesophageal stricture

Oesophageal web (a mucosal abnormality)
Foreign body
Candida
Herpes
Oesophagitis relating to acid reflux
Post radiation oesophagitis
<question textentry1>
<text> How will you work out from your patient whether the cause of the problem is localised or part of a generalised disease process?
Think of a question to identify the level of the obstruction/pathology
</text>
<feedback>.(These are suggested questions)
Can you point to the level where you feel the food sticking?
Does the food get as far as the stomach?
</feedback></question>
<question textentry1>
<text> Think of questions that may establish a neurological cause:
</text>
<feedback>.

(These are suggested questions)5) Has your voiced changed recently
6) Do you find it hard to chew and swallow due to weakness?
</feedback></question>
Medical Causes
There are an enormous list of medical causes, which can affect the mouth, oropharynx and oesophagus to varying degrees as part of a generalised medical condition. You will hopefully establish these conditions by asking for a detailed past medical history and drug history.
<question textentry1>
<text> Can you list any of these? </text>
<feedback>. Recent stroke, Neuromuscular disease Parkinsons disease Alzheimers Multiple sclerosis Brain tumours Huntingtons disease Polio Myasthenia gravis Diabetes Thyroid disease Dementia Traumatic brain injury Drugs
</feedback></question>
Find yourself a BNF (British National Formulary), which are found on every ward, and complete the T/F below:

These drugs can cause dysphagia:
<question truefalse1><text true>Nitrates</text>
<feedback correct></feedback><feedback incorrect></feedback>
</question>
<question truefalse1><text true> Anticholinergic agents </text>
<feedback correct></feedback><feedback incorrect></feedback>
</question>
<question truefalse1><text false>Thryozine</text>
<feedback correct></feedback><feedback incorrect></feedback>
</question>
<question truefalse1><text false>Codiene</text>
<feedback correct></feedback><feedback incorrect></feedback>
</question>
<question truefalse1><text true> Calcium tablets </text>
<feedback correct></feedback><feedback incorrect></feedback>
</question>
<question truefalse1><text false> Paracetamol </text>
<feedback correct></feedback><feedback incorrect></feedback>
</question>
<question truefalse1><text true>Asperine</text>
<feedback correct></feedback>

<feedback incorrect></feedback></question>
<question truefalse1><text false>OCP</text>
<feedback correct></feedback><feedback incorrect></feedback>
</question>
<question truefalse1><text true>Iron tablets</text>
<feedback correct></feedback><feedback incorrect></feedback>
</question>
<question truefalse1><text true> Vitamin C(enteric coated)</text>
<feedback correct></feedback><feedback incorrect></feedback>
</question>
<question truefalse1><text true> Tetracycline </text>
<feedback correct></feedback><feedback incorrect></feedback>
</question>
REGURGITATION:
Pharyngeal pouches are rare causes of dysphagia, but tend to be a popular medical because they’re quite interesting. Regurgitation of food is a presenting symptom of patients with a pharyngeal pouch or achalasia and so you should ask about this symptom:
7) Do you tend to regurgitate undigested food?
Other symptoms include foul smelling breath, as the food in the pouch collects there and stagnates. Dysphagia is a late symptom, developing when the pouch

has reached such a large size that it impinges on the oesophagus lower down. The barium swallow illustrates the extent of a pouch.
Barium collecting in pouch.
Remember, this condition really is quite rare and the patients may be describing a symptom of achalasia to you, or misinterpreting the gastric content reflux associated with GORD (gastro-oesophageal reflux disease)
Further info about this condition can be found here:
http://www.edu.rcsed.ac.uk/photoalbum/ph50.htm
http://www.surgical-tutor.org.uk/default-home.htm?system/hnep/pharyngeal_pouch.htm~right

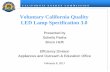
This diagram shows you a barium swallow in a patient with achalasia, showing the classical tapering into a ‘birds beak’ or ‘rats tail’ and the pre-stenotic dilatation.
Use this link to find out more about achalasia: http://www.medicinenet.com/Achalasia/article.htm
ASSOCIATED PAIN:
8) Do you have any pain associated with the problem? (?severity, location, onset, radiation, character etc)
Benign strictures resulting from gastro-oesophageal reflux disease will usually be preceded by dyspeptic symptoms of heartburn or epigastric discomfort (as well as acid reflux). If this is the case you will need to find out more about the severity of their reflux symptoms, including waterbrash. A proportion of malignant strictures present with constant aching pain that radiates to the back. Inflammatory conditions, for example tonsillitis or candidiasis of the mouth, pharynx or oesophagus, are also associated with pain or discomfort, usually closely corrulating with the swallowing process. Motility disorders of the oesophagus can produce oesophageal spasm, which presents with severe chest pain.

ASPIRATION:
<question textentry2>
<text> Define the term ‘aspiration’ set in this context: </text>
<feedback>.
Aspiration can be defined as entry of material into the airway below the true vocal cords.
</feedback></question>
One way of finding out whether your patient is aspirating may be by asking:
Do you find that food or liquids go ‘down the wrong way’? Do you cough or splutter when you take a drink?
If the pharyngeal stage of deglutition is disrupted, then a disorganised swallow reflex may result in the bolus of solid or liquid entering the larynx and subsequently the trachea (aspiration). This can lead to pneumonia, which in a potentially malnourished patient with reduced immunity can have catastrophic septic consequences.
<question multiresponse3>
<text> Which particular pathological causes of dysphagia does this occur with? Pick the most likely causes below:
</text>
<answer true>Neurological Diseases</answer>

<answer true>GORD</answer>
<answer false>Inflammatory conditions</answer>
<answer false>Malignancy</answer>
<feedback correct> Yes, this tends to be a problem associated with neurological pathologies [link]. It can also be secondary to refluxing large volumes of stomach contents in GORD. This is most noticeable at night, when the patient is unconscious and not guarding their airways well.
</feedback>
<feedback incorrect> No, this tends to be a problem associated with neurological pathologies [link]. It can also be secondary to refluxing large volumes of stomach contents in GORD. This is most noticeable at night, when the patient is unconscious and not guarding their airways well.</feedback>
</question>
Look at the video fluoroscopy image below, which shows the fluid entering the trachea, after an attempted swallow.

WEIGHT LOSS AND NUTRITION:
Any prolonged difficulty with swallowing is inevitably going to lead to a degree of malnutrition.
<question multichoice1>
<text> What is ‘malnutrition’</text>
<answer>1</answer>
<answer correct>An alteration in body composition, caused by an acute or chronic deprivation of caloric intake, which leads on to reduced functional

capacity of several organs or systems, which INCREASES THE PATIENTS MORBIDITY AND MORTALITY</answer>
<answer>3</answer>
<answer>4</answer>
<feedback correct> </feedback>
<feedback incorrect></feedback>
</question>
Asking a simple question about weight may give a rough indication to the presence of malnutrition. If a patient is uncertain, asking whether their normal clothes are looser fitting than before can yield the information you want. When inability to take full nutrition due to dyphagia is coupled with a malignant process (where weight loss is already common) the resultant weight loss can be dramatic.
Have you lost any weight? How much? Over what sort of time frame?
THE OTHER BITS AND PIECES:
As explained before, you need to establish their background state of health, family history, drug history and whether they are smokers.
9) Do you have any significant past medical history?
You’re looking for things like connective tissue disorders (eg scleroderma, dermatomyosities), neurological disorders (CVA, MS, Parkinson’s, Alzheimers) and ENT pathologies. A significant family history may be present, especially in association with connective tissue disorders and is worth persuing.
10) Which medications do you take? [link to drugs that cause dysphagia]

11) Do you smoke? (Quantify pack years) Do you drink alcohol? (Quantify)
Smokers have a higher incidence of oropharyngeal and oesophageal cancer. Alcoholics may have gastro oesophageal reflux disease or cirrhosis associated with varicies.
12) Systems review.
Questioning here may reveal or confirm, symptoms relating to connective tissue or neurological diseases.
EXAMINATION
GENERAL:
Look at the patient’s general state.
What signs relating to causes of dysphagia could you find? List at least 4:
-------------------------------------------
-------------------------------------------
------------------------------------------
---------------------------------------

---------------------------------------
These are all fairly straight forward:
i) Are there any signs of malnutrition (wasting/cachexia)
ii) Dehydration (Mucosal membranes look dry? Decreased skin turgor?)
iii) Is the patient anaemic or jaundiced?
iv) Are there any neck abnormalities? (cervical lymphadenopathy, thyroid enlargement, or a pharyngeal pouch?)
v) Overt neurological abnormalities (eg hemiplegia following a CVA)
CVS AND RS EXAMINATION:
Other than establishing that your patient is alive, why are these important systems to review?
You are looking for evidence of: -
i) Pneumonia secondary to aspiration.
ii) Lung metastases or malignant pleural fluid.
iii) Co morbidity unrelated to the presenting complaint, which will be important when considering the patients management, for

example whether, if surgery is an option, the patient is fit enough to perform it.
ABDOMINAL EXAMINATION:
What may you find here which would be relevant to dysphagia?
i) Masses in the epigastrium relating to lymphadenopathy or tumour of the cardia of the stomach
ii) Hepatosplenomegaly
iii) Ascites
CNS and PNS:
PNS: During this examination, you need to look for any of the physical findings consistent with neurological causes of dysphagia[link].

CNS: Regarding cranial nerves, dyphagia can be caused by any interference with the normal function of several of the nerves.
Click on the nerves, which when interrupted, may cause difficulties with swallowing
CN I No – Swallowing is OK but they can’t smell their food very well!
CN II No – Swallowing is OK but they can’t see their food very well!
CN III No - Swallowing is OK but they may see double the quantity of food (diplopia)
CN IV No - Swallowing is OK but they may see double the quantity of food (diplopia)
CN V Yes - Innervation to muscles of mastication affected.
CN VI No - Swallowing is OK but they may see double the quantity of food (diplopia)
CN VI I Yes. Sensation of the oropharynx would be abnormal
Taste to the anterior 2/3 of the tongue would be affected
CN VIII No Swallowing will be fine, although they may not hear the call to the dinner table and may fall over due to poor balance, whilst eating it!
CN IX Yes Motor and sensory innervation of the pharynx is affected. Aspiration could be a problem
Taste will be poor over the posterior 1/3 of the
CN X Yes Motor and sensation innervation of the larynx and the laryngo- pharynx will be affected
Taste to the oropharynx will be reduced
Protection of the airway will be absent – more potential for aspiration
CN XI No
CN XIIYes Motor innervation of the tongue

To revise examination of the cranial nerves and PNS, refer to the black board tutorial in the neurology teaching documents. [link]
SPECIAL INVESTIGATIONS:
This is included for your interest and is less important than the preceding history and examination sections.
1) If the problem appears to be related to the pharynx or larynx NASENDOSCOPY may be appropriate. This is usually organised by the ENT surgeons and looks at the pharynx, larynx and vocal folds in detail.
2) ENDOSCOPY of the oesophagus and stomach will detect any abnormalities, such as a tumour, inflammation, stricture or foreign body bolus. The procedure is usually carried out as a day case intervention and is done by a gastroenterologist or surgeon. If a lesion is encountered, a biopsy can be taken to confirm diagnosis. Dilatation or stenting of a narrowed lumen can also be performed, so endoscopy can also be ‘therapeutic’.
Just to give you an idea of what they may see, have a go at this quiz. Any idea what these endoscopic views show you? Click on the image to find the answer.
: Candidiasis of the oesophagus

A:benign stricture
Linear ulcers fairly classical for GORD
oesophageal carcinoma

3) A BARIUM SWALLOW gives further information about strictures and motility disorders (including achalasia) and may demonstrate a pharyngeal pouch [link].
4) OESOPHAGEAL MANOMETRY gives more information about motility disorders (e.g. Achalasia, diffuse oesophageal spasm, GORD)
5) CT scans give good structural information about the oesophagus and surrounding structures. Where a malignancy has been detected, this is an important investigation to stage the disease and direct appropriate treatment.
6) Oesophageal ultrasound (EUS)also yields important information regarding the stage of oesophageal cancers.
This diagram shows you how the EUS demonstrates the different anatomical layers of the oesophagus and how it clearly shows the depth of tumour invasion.
MANAGEMENT OF DYSPHAGIA:
Obviously this needs to be tailored to the different pathology encountered. In all cases, nutrition and hydration need urgent attention and this may be best tackled with a multidisciplinary team, which includes:

Speech and language therapists (S.A.L.T) – these specialists assess the patients with deficiencies seen in functional dysphagia and advise about which exercises may improve symptoms or whether the consistencies of food require modification (e.g. fluid thickeners).
Nursing specialists
Dieticians
Gastroenterologists
Neurologists
Surgeons (ENT, Endocrine, GI)
SPECIFIC MANAGEMENT:
This is a brief overview only.
INFLAMMATORY CAUSES [link] STRUCTURAL CAUSES[link]
NEUROLOGICAL CAUSES[link]
MOTILITY DISORDERS[link]
INFLAMMATORY CAUSES:
1)Infection is treated with antifungal, antiviral or antibiotic agents if appropriate.
Perhaps one of the commonest causes

– What is it and which agents if any would you use?
- Tonsilitis. Penicillin V – an oral preparation.
2) Inflammation relating to reflux disease is treated with drugs that reduce the acid production of the stomach (Proton pump inhibitors e.g. Omeprazole). Where patients are unable to tolerate these medications, perhaps because of an allergy or side effects, OR if the patient does not wish to take a lifetimes worth of medication, there is the option of laparoscopic fundoplication. The effectiveness of this is being established by a large national trial at the moment, but most evidence to date suggests that it is an effective treatment modality. [this link tells you much more about it: http://www.limit.ac.uk/nissen1.htm]
STRUCTURAL:
Mostly these causes require a surgical assessment and treatment where appropriate. Malignant oesophageal causes will need a full staging assessment and if deemed potentially curable after this, chemotherapy and resection.
A foreign body is retrieved via endoscopy
A squamous cell carcinoma of the oesophagus or oropharynx, may respond to radio-chemotherapy but is often treated surgically where possible.
A benign stricture is assessed with endoscopy and dilated with a bougie or a balloon device, having passed a guidewire initially.
NEUROLOGICAL:
S.A.L.T specialists are the best specialists to treat these conditions, as there is usually no ‘quick fix’ solution, dysphagia simply being a function of the disease process. In advanced

stages of neurological disease, dysphagia is so marked that a supplementary form of nutrition if necessary, for example an NG tube or a percutaneous feeding gastrostomy.
Achalasia can be treated by an endoscopic ballon dilatation, localised botulinum toxin injection and if all else fails, a Hellers Myotomy. This divides the hypertrophied muscle which obstructs the lower end of the oesophagus, leaving the mucosal layer maintaining the luminal integrity. [Use this link to see diagrams of this http://www.hopkins-gi.org/pages/latin/templates/index.cfm?pg=disease3&organ=1&disease=37&lang_id=1&pagetype=12&pagenum=625]
The other causes are mostly connective tissue disorders and stricturs may respond to endoscopic dilatation.
SUMMARY:
Hurreh – you’ve got to the end
This tutorial has covered the basics in history taking and examination of a patient presenting with dysphagia. It is not meant to cover all the core knowledge required concerning the background conditions, because that is all in your books.
Now you should be able to know exactly what you want to ask your patient about which you will do in a systematic way and which signs to look out for during the examination and finally, come up with a reasonable differential diagnosis.
I hope it’s been a useful exercise!
Related Documents