collum fractures. Even today, a classification according to anatomical criteria is still commonly used (Fig. 1). Fracture of the condylar base Fracture of the condylar collum Diacapitular fracture through the condylar head This classification describes the location of the fracture, however the equally important and treatment relevant degree of displacement and dislocation is not represented. According to Müller 13) , Dingmann and Natvig 2) the insertion line of the lateral pterygoid muscle is an essential criteria for the classification of condylar process fractures. This anatomical classification is rarely used in clinical practice due to the fact that this insertion line is difficult to find clini- cally 19) . Nevertheless, Müller 13) classified the degree of dis- placement and dislocation respectively into three classes of axial deviation from 10 to 90 degrees. In clinical practice, the classification according to Spiessl and Schroll 19) proved most useful, however it is instead of this difficult to differen- tiate displacement and dislocation 4) . The relation of the fossa to the condylar position can only be precisely evaluat- ed in cases where the fracture fragment of the condylar head is located in the projection level of the x-ray image. Dislocated fractures cause a disarticulation of the condylar head and a rupture of the joint capsule. According to Wassmund 22) and Gilhuus Moe 5) , a degree of fragment mal- position of more than 60 degrees can be presumed to be a dislocation. An important prerequisite for the appropriate treatment of fractures of the mandibular condyle is an unambiguous and therapy-relevant classification. In the clinical situation, any fracture that is located above the mandibular foramen and that runs from the posterior edge of the ramus into the sigmoid notch or the condylar head, is classified as a fracture of the condylar process. There is a subclassification into deep, medium and high condylar process fractures. Fractures of the condylar head are referred to as intraarticular or diacapitular fractures. However, different systems of classification of these frac- tures make any comparison of treatment results difficult 12) . Regarding malposition of the fracture, the German classifi- cation differentiates between displacement (Dislokation) and dislocation (Luxation). Displacement describes the shift of the fracture fragments. According to Wassmund 21) , dis- placement occurs ad axim, ad latus, ad longitudinum cum contractionem and, in rare cases, due to muscle traction cum distractionem. The term dislocated fracture is applied in cases where the cranial fracture fragment exarticulates. In such cases, the distal fracture fragment is often dis- placed or dislocated medially or anteromedially. Sometimes anterior or posterior, rarely lateral displacement or disloca- tion is encountered. In the English classification however, the terms “deviation”, “displacement” and “dislocation” differentiate the fractures. “Deviation” describes a simple deviation of the proximal fragment, while the shifted frac- ture fragments are still in primary contact. “Displacement” is applied in cases, where there is no contact of the fracture fragments. A “Dislocation” describes the entire exarticula- tion of the joint. In the past, there have been various attempts to classify condylar process fractures 11) 13) 16) 17) 18) 21) . In 1927, Wassmund 21) classified mandibular condylar fractures, by subdividing the fractures according to their anatomical position and to the cause of trauma: Vertical collum fracture, including rupture of the condylar head Transverse collum fracture Diagonal collum fracture Köhler 8) developed a classification based purely on the anatomical position. He differentiated between high diaca- pitular and subcondylar fractures, medium collum fractures and basal or deep collum fractures at the level of the sig- moid notch. Reichenbach 16) differentiated high and deep Classification of condylar process fractures M. Schneider, U. Eckelt 10 Classification of condylar process fractures Chapter 3 Fig. 1: Elementary classification of condylar process fractures – without information about displacement or degree of dislocation.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

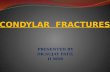
collum fractures. Even today, a classification according toanatomical criteria is still commonly used (Fig. 1).
Fracture of the condylar baseFracture of the condylar collumDiacapitular fracture through the condylar head
This classification describes the location of the fracture,however the equally important and treatment relevantdegree of displacement and dislocation is not represented.
According to Müller 13), Dingmann and Natvig 2) the insertionline of the lateral pterygoid muscle is an essential criteria forthe classification of condylar process fractures. Thisanatomical classification is rarely used in clinical practicedue to the fact that this insertion line is difficult to find clini-cally 19). Nevertheless, Müller 13) classified the degree of dis-placement and dislocation respectively into three classes ofaxial deviation from 10 to 90 degrees. In clinical practice,the classification according to Spiessl and Schroll 19) provedmost useful, however it is instead of this difficult to differen-tiate displacement and dislocation 4). The relation of thefossa to the condylar position can only be precisely evaluat-ed in cases where the fracture fragment of the condylarhead is located in the projection level of the x-ray image.Dislocated fractures cause a disarticulation of the condylarhead and a rupture of the joint capsule. According toWassmund 22) and Gilhuus Moe 5), a degree of fragment mal-position of more than 60 degrees can be presumed to be a dislocation.
An important prerequisite for the appropriate treatment of fractures of the mandibular condyle is an unambiguousand therapy-relevant classification.
In the clinical situation, any fracture that is located abovethe mandibular foramen and that runs from the posterioredge of the ramus into the sigmoid notch or the condylarhead, is classified as a fracture of the condylar process.There is a subclassification into deep, medium and highcondylar process fractures. Fractures of the condylar headare referred to as intraarticular or diacapitular fractures.However, different systems of classification of these frac-tures make any comparison of treatment results difficult 12).
Regarding malposition of the fracture, the German classifi-cation differentiates between displacement (Dislokation)and dislocation (Luxation). Displacement describes the shiftof the fracture fragments. According to Wassmund 21), dis-placement occurs ad axim, ad latus, ad longitudinum cumcontractionem and, in rare cases, due to muscle tractioncum distractionem. The term dislocated fracture is appliedin cases where the cranial fracture fragment exarticulates.In such cases, the distal fracture fragment is often dis-placed or dislocated medially or anteromedially. Sometimesanterior or posterior, rarely lateral displacement or disloca-tion is encountered. In the English classification however,the terms “deviation”, “displacement” and “dislocation”differentiate the fractures. “Deviation” describes a simpledeviation of the proximal fragment, while the shifted frac-ture fragments are still in primary contact. “Displacement”is applied in cases, where there is no contact of the fracturefragments. A “Dislocation” describes the entire exarticula-tion of the joint.
In the past, there have been various attempts to classifycondylar process fractures 11) 13) 16) 17) 18) 21). In 1927,Wassmund 21) classified mandibular condylar fractures, bysubdividing the fractures according to their anatomicalposition and to the cause of trauma:
Vertical collum fracture, including rupture of the condylar headTransverse collum fractureDiagonal collum fracture
Köhler 8) developed a classification based purely on theanatomical position. He differentiated between high diaca-pitular and subcondylar fractures, medium collum fracturesand basal or deep collum fractures at the level of the sig-moid notch. Reichenbach 16) differentiated high and deep
Classification of condylar process fracturesM. Schneider, U. Eckelt
10 Classification of condylar process fracturesChapter 3
Fig. 1: Elementary classification of condylar process fractures – without information about displacement ordegree of dislocation.

Fig. 3: Fractures type III and IV according to Spiessl and Scholl.
Classification of collum fractures according to Spiessl and Schroll 20)
Type I: Collum fractures without considerable displace-ment (Fig. 2)
Type II: Deep collum fractures with displacement (Fig. 2)
Type III: High collum fractures with displacement (Fig. 3)
Type IV: Deep collum fractures with dislocation (Fig. 3)
Type V: High collum fractures with dislocation (Fig. 4)
Type VI: Intracapsular/diacapitular fractures (Fig. 4)
Classification of condylar process fractures 11
The fragment can be dislocated medially, laterally, ventrallyand dorsally. Although this classification does not explicitlydemarcate the degree of displacement or dislocation, whichis relevant to the prognosis, it is currently considered the
Chapter 3 11
basis of many comparative studies and multiple publica-tions.
Fig. 2: Fractures type I and II according to Spiessl and Scholl.
Type I
Type III
Type II
Type IV

An explicit definition of high and deep fracture displace-ment is still not available. According to Lund 11), Loukota etal. 10) proposed the sigmoid notch to be the border betweenhigh and deep condylar process fractures (Fig. 5).
Following the classification of Spiessl and Schroll 19), Rasse15), Neff 14), Hlawitschka 6) and Loukota 9) additionally classi-fied the intraarticular or diacapitular condylar fracturesaccording to the fracture line. A diacapitular fracture isdefined by a fracture line starting within the articulation sur-face (Fig. 6).
12 Classification of condylar process fracturesChapter 3
Type A (VI A): Displacement of medial condylar pole withpreservation of the vertical dimension. The fracture is sup-ported, stable and not shortened. The joint supporting artic-ulation surface is partially affected at the medial condylarhead fragments.
Type B (VI B): The lateral condylar pole is involved with lossof the vertical dimension. The fracture is not supported,unstable and shortened. The joint supporting articulationsurface is subtotally affected, together with the lateral gaugeand the lateral ligament.
Fig. 5: Classification of fractures of the condylar process in accordance with the height of fracture. First, a tangent line is placedbetween the dorsal gauge of the condylar process and the mandibular angle. Line A is perpendicular to the tangent line andcrosses the deepest point of the semilunar notch. High condylar fracture: The fracture line starts below line A and runs toover 50% of its length above line A. Deep condylar fracture: The fracture line runs above the mandibular foramen and iswith over 50% of its length below line A.
Fig. 4: Fractures type V and VI according to Spiessl and Scholl.
Type V Type VI

Classification of condylar process fractures Chapter 3 13
This classification is clinically relevant as diacapitular fracturesof type VI A and do not lose support within the articular fossa.There is no shortening, functional impairment is minimal andan open reduction is not indicated (Fig. 7).
Fig. 6: A diacapitular fracture exists if the fracture line runs within the area of the articular capsule. Left picture: Fracture type Awith continuous bony contact within the articular fossa (no loss of ramus height). Middle picture: Fracture type B with lossof the support within the articular fossa and loss of height of the mandibular ramus. Right picture: Fracture type C with theuppermost part of the fracture below the base of the lateral ligament – also with loss of ramus height.
Type C (V): The joint supporting articulation surface isentirely affected with a dislocation of the entire condylarhead. This corresponds to class V according to Spiessl andSchroll 19).
Fig. 7: Computertomographic demonstration of diacapitular fractures in a coronal section. Left: Diacapitular fracture Type VI Awithout loss of the support in the articular fossa. Right: Diacapitular fracture Type VI B with considerable loss of the support and indication for open treatment by osteosynthesis.
Type A Type B Type C

Hlawitschka and Eckelt 7) added an additional type of frac-ture to fractures of type VI A and VI B 14):
Type M, comminuted fracture with loss of vertical dimen-sion. The fracture is shortened and not supported.
Conventional radiography is important in routine diagnosis ofmandibular fractures. As a basic principle in fracture diag-nosis, visualisation in two radiographic planes is necessary.According to Clementschitsch, panoramic tomography andposterior-anterior radiography are the established basicviews.
In order to select a surgical approach and to choose theappropriate osteosynthesis, computer tomography (CT) ordigital volume tomography (DVT) are necessary, offeringmore differentiated sectional images. This is especially thecase for the preoperative diagnosis of diacapitular condylarfractures 3) 18). Fracture height and the degree of displace-ment can be properly visualised in coronal tomographic
sections (Fig. 7). Three-dimensional reconstructionimproves the accuracy of classification, especially for highfractures. In relation to the significance of computer tomog-raphy, exposure to radiation is relatively low and will be fur-ther decreased by modern techniques and the applicationof digital volume tomography (DVT).
The Spiessl and Schroll 19) classification of fracture types Ito VI and together with the explicit differentiation betweencondylar base and condylar collum fractures Loukota 10)
allows a clear and therapy-relevant classification. The addi-tional identification of the degree of displacement and dis-location in millimeters and the determination of the degreeof angulation enable an even more precise evaluation of theseverity of the fracture. The classification according toRasse 15) and Neff 14) together with Hlawitschka 6) andLoukota 9) prove useful for the classification of diacapitularfractures. In summary, Fig. 8 illustrates the relation bet-ween commonly applied classifications and the surgicalapproaches.
14 Classification of condylar process fracturesChapter 3
Fig. 8: Classification of condylar fractures and surgical approach
Martin Bildat
Notiz
Stimmt diese Referenzierung?

12) Mokros, S. Die operative Behandlung von Gelenkfortsatzfrakturendes Unterkiefers über den intraoralen Zugang -Optimierung der Methodik, Ergebnisse. Magdeburg, 1997.
13) Müller, W. Neuere Erkenntnisse in der Diagnostik und Therapieder Gelenkfortsatzfrakturen des Unterkiefers. Dtsch Stomatol 1971;21:685-90.
14) Neff, A., Kolk A.,Deppe H., Horch H.-H. Neue Aspekte zur Indikation der operativen Versorgungintraartikulärer und hoher Kiefergelenkluxationsfrakturen.[New aspects for indications of surgical management ofintra-articular and high temporomandibular dislocationfractures]. Mund Kiefer Gesichtschir 1999;3(1): 24-9.
15) Rasse, M. Diakapituläre Frakturen der Mandibula. Eine neueOperationsmethode und erste Ergebnisse. Stomatolgie 1993(90): 413-28.
16) Reichenbach, E. Zur Frage der operativen Knochenbruchbehandlungim Bereich des Gesichtsschädels. Dtsch Zahn Mund Kieferheilkd Zentralbl 1953;17: 220-43.
17) Rowe, N., Killey H.C. Fractures of the Facial Skeleton. Edinburgh and London, E.&S. Livingstone Ltd., 1968.
18) Schimming, R., Eckelt U., Kittner T. The value of coronal computer tomograms in fracturesof the mandibular condylar process. Oral Surg Oral Med Oral Pathol Oral Radiol Endod1999;87(5): 632-9.
19) Spiessl, B., Schroll K. Spezielle Frakturen- und Luxationslehre. Ein kurzesHandbuch in fünf Bänden. Band I/1 Gesichtsschädel.H. Ningst. Stuttgart, New York, Georg Thieme Verlag 1972.
20) Spiessl, B., Schroll K. Spezielle Frakturen- und Luxationslehre. Ein kurzesHandbuch in fünf Bänden. Band I/1 Gesichtsschädel.Stuttgart, New York: Georg Thieme Verlag, 1972:317.
21) Wassmund, M. Frakturen und Luxationen des Gesichtsschädels unterBerücksichtigung der Komplikationen des Hirnschädels. Ihre Klinik und Therapie. Berlin: Meusser 1927.
22. Wassmund, M. Über Luxationsfrakturen des Kiefergelenks. Dtsch Kieferch 1934;1:27-54.
Classification of condylar process fractures Chapter 3 15
References
1) Cattaneo, G. Nachuntersuchung von Kiefergelenkfrakturen von 1972bis 1982 der Zahn-, Mund- und Kieferklinik Erlangen. Erlangen, 1984
2) Dingman R. O., P. Natvig Surgery of Facial Fractures. Philadelphia London, W.B. Saunders 1964.
3) Eckelt, U. Gelenkfortsatzfrakturen. [Fractures of the mandibularcondyle].Mund Kiefer Gesichtschir 2000;4 Suppl 1: S110-7.
4) Eulert, S. Die Behandlung von Gelenkfortsatzfrakturen desUnterkiefers unter besonderer Berücksichtigung derWürzburger Zugschrauben-Platte. Würzburg, Julius-Maximilians-Universität, 2002.
5) Gilhuus-Moe, O. Fractures of Mandibular Condyle in the Growth Period. Oslo Norway, Universitetförlaget, 1969.
6) Hlawitschka, M. Klinische, radiologische und funktionsdiagnostischeErgebnisse konservativ funktionell und operativbehandelter Frakturen des Caput mandibulae. Dresden, Technische Universität Dresden, 2002.
7) Hlawitschka, M., Eckelt U. Assessment of patients treated for intracapsular fractures of the mandibular condyle by closed techniques. J Oral Maxillofac Surg 2002,60(7): 784-91; discussion 92.
8) Köhler, J. Diagnostik und Therapie der Kieferfrakturen.Heidelberg, Hüthig 1951.
9) Loukota, R., Neff A., Rasse M. Nomenclature/classification of fractures of themandibular condylar head. Br J Oral Maxillofac Surg 2009, doi:10.1016/j.bjoms.2009.08.036 (online first).
10) Loukota, R. A., Eckelt U., DeBont L., Rasse M. Subclassification of fractures of the condylar processof the mandible. Br J Oral Maxillofac Surg 2005;43(1): 72-73.
11) Lund, K. Mandibular growth and remodelling processes aftercondylar fracture. A longitudinal roentgencephalo-metric study.Acta Odontol Scand Suppl 1974;32(64): 3-117
Related Documents




![Oral & Maxillofacial Surgeryopenaccessebooks.com/oral-maxillofacial-surgery/condylar-fractures.pdftreatment of mandibular condylar process fractures [10]. It was found that treatment](https://static.cupdf.com/doc/110x72/5e27326a457720282958fba6/oral-maxillofacial-sur-treatment-of-mandibular-condylar-process-fractures.jpg)





