THE HISTORY OF THE PAP TEST SAMPLING AND PREPARATION METHODS Conventional Smears Liquid-based Preparations ThinPrep™ SurePath™ AUTOMATED SCREENING Historical Overview Focal Point™ ACCURACY AND REPRODUCIBILITY DIAGNOSTIC TERMINOLOGY AND REPORTING SYSTEMS THE BETHESDA SYSTEM Specimen Adequacy General Categorization Interpretation and Results THE NORMAL PAP Squamous Cells Endocervical Cells Exfoliated Endometrial Cells Abraded Endometrial Cells/Lower Uterine Segment Trophoblastic Cells and Decidual Cells Inflammatory Cells Lactobacilli Artifacts and Contaminants ORGANISMS AND INFECTIONS Shift in Flora Suggestive of Bacterial Vaginosis Trichomonas vaginalis Candida Actinomyces Herpes Simplex Cytomegalovirus Chlamydia Trachomatis Rare Infections REACTIVE CHANGES Reactive Changes Due To Inflammation, Including ‘Repair’ Radiation Cellular Changes Associated With Intrauterine Devices Glandular Cells Status Posthysterectomy Other Benign Changes VAGINAL SPECIMENS IN ‘DES DAUGHTERS’ SQUAMOUS ABNORMALITIES Squamous Intraepithelial Lesions Grading Squamous Intraepithelial Lesions Low-grade Squamous Intraepithelial Lesions High-grade Squamous Intraepithelial Lesions Problems in The Diagnosis of Squamous Intraepithelial Lesions Overdiagnosing LSIL Distinguishing LSIL From HSIL Distinguishing HSIL From Invasive Carcinoma Squamous Cell Carcinoma Atypical Squamous Cells Atypical Squamous Cells of Undetermined Significance Atypical Squamous Cells, Cannot Exclude High-grade Squamous Intraepithelial Lesion GLANDULAR ABNORMALITIES Endocervical Adenocarcinoma In Situ Adenocarcinoma Endocervical Adenocarcinoma Endometrial Adenocarcinoma Differential Diagnosis of Adenocarcinoma Atypical Glandular Cells OTHER MALIGNANT NEOPLASMS Small Cell Carcinoma Malignant Melanoma Malignant Lymphoma Malignant Mixed Mesodermal Tumors Metastatic Tumors ENDOMETRIAL CELLS IN WOMEN ≥ 40 YEARS OF AGE HORMONAL EVALUATION 1 CERVICAL AND VAGINAL CYTOLOGY Edmund S. Cibas 1 In the United States both the incidence and mortality rates for cervical cancer declined significantly in the 20th century, a decline attributed to the Papanicolaou (Pap) test. In the 1930s, before screening was intro- duced, cervical cancer was the most common cause of cancer deaths in women in the United States. 65 Today it is not even one of the top five. 66 In 2002, the incidence of cervical cancer in the United States was 13 000 cases, with 4100 deaths. 66 Worldwide, however, the incidence and mortality rates S2638-01.qxd 12/11/02 11:42 Page 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

THE HISTORY OF THE PAP TEST
SAMPLING AND PREPARATION METHODSConventional SmearsLiquid-based PreparationsThinPrep™SurePath™
AUTOMATED SCREENINGHistorical OverviewFocal Point™
ACCURACY AND REPRODUCIBILITY
DIAGNOSTIC TERMINOLOGY AND REPORTING SYSTEMS
THE BETHESDA SYSTEMSpecimen AdequacyGeneral CategorizationInterpretation and Results
THE NORMAL PAPSquamous CellsEndocervical CellsExfoliated Endometrial CellsAbraded Endometrial Cells/Lower Uterine SegmentTrophoblastic Cells and Decidual CellsInflammatory CellsLactobacilliArtifacts and Contaminants
ORGANISMS AND INFECTIONSShift in Flora Suggestive of Bacterial VaginosisTrichomonas vaginalisCandidaActinomycesHerpes SimplexCytomegalovirusChlamydia TrachomatisRare Infections
REACTIVE CHANGES
Reactive Changes Due To Inflammation, Including ‘Repair’RadiationCellular Changes Associated With Intrauterine DevicesGlandular Cells Status PosthysterectomyOther Benign Changes
VAGINAL SPECIMENS IN ‘DES DAUGHTERS’
SQUAMOUS ABNORMALITIESSquamous Intraepithelial Lesions
Grading Squamous Intraepithelial LesionsLow-grade Squamous Intraepithelial LesionsHigh-grade Squamous Intraepithelial Lesions Problems in The Diagnosis of Squamous Intraepithelial Lesions
Overdiagnosing LSILDistinguishing LSIL From HSILDistinguishing HSIL From Invasive Carcinoma
Squamous Cell CarcinomaAtypical Squamous CellsAtypical Squamous Cells of Undetermined Significance Atypical Squamous Cells, Cannot Exclude High-gradeSquamous Intraepithelial Lesion
GLANDULAR ABNORMALITIESEndocervical Adenocarcinoma In SituAdenocarcinoma
Endocervical Adenocarcinoma Endometrial AdenocarcinomaDifferential Diagnosis of Adenocarcinoma
Atypical Glandular Cells
OTHER MALIGNANT NEOPLASMSSmall Cell CarcinomaMalignant MelanomaMalignant LymphomaMalignant Mixed Mesodermal TumorsMetastatic Tumors
ENDOMETRIAL CELLS IN WOMEN ≥ 40 YEARS OF AGE
HORMONAL EVALUATION
1CERVICAL AND VAGINAL CYTOLOGY
Edmund S. Cibas
1
In the United States both the incidence and mortalityrates for cervical cancer declined significantly in the20th century, a decline attributed to the Papanicolaou(Pap) test. In the 1930s, before screening was intro-duced, cervical cancer was the most common cause of
cancer deaths in women in the United States.65 Today itis not even one of the top five.66
In 2002, the incidence of cervical cancer in theUnited States was 13 000 cases, with 4100 deaths.66
Worldwide, however, the incidence and mortality rates
S2638-01.qxd 12/11/02 11:42 Page 1

for cervical cancer are second only to breast cancer, andin many places cervical cancer is the most commoncause of death in women of reproductive age, a disparityattributed to the absence of screening programs. Fewerthan 5% of women in developing countries have everhad a Pap test.158 In contrast, 89% of women in theUnited States report having had a Pap test in thepreceding 3 years.139
THE HISTORY OF THE PAP TEST
The Pap test is the most cost-effective cancer reductionprogram ever devised.65 Credit for its conception anddevelopment goes to Dr George N. Papanicolaou. In1928 he reported that malignant cells from the cervixcould be identified in vaginal smears.123 Later, hiscollaboration with a gynecologist, Dr Herbert Traut,provided him with a large number of clinical samplesand resulted in detailed descriptions of preinvasivelesions.120,121 Initially, pathologists and clinicians greetedthis technique with skepticism. By the late 1940s, how-ever, Papanicolaou’s observations had been confirmedby others. A Canadian gynecologist, Dr J. Ernest Ayre,suggested taking samples directly from the cervix with awooden spatula rather than from the vagina with apipette as originally described by Papanicolaou.11
Eventually, cytologic smears were embraced as an idealscreening test for preinvasive lesions, which, if treated,would be prevented from developing into invasive cancer.
The first screening clinics were established in the1940s.101 The Pap test was never evaluated in a con-trolled, prospective study, but several pieces of evidencelink it to the prevention of cervical cancer. First, themortality rate from cervical cancer fell dramaticallyafter screening was introduced: by 72% in BritishColumbia4 and 70% in Kentucky.32 Second, there was adirect correlation between the intensity of screeningand the decrease in mortality from cervical cancer.Among Scandinavian countries, the death rate fell by80% in Iceland, where screening was greatest; inNorway, where screening was lowest, the death rate fellby only 10%.84 A similar correlation was observed inhigh and low screening regions of Scotland94 andCanada.104 In the United States, the decrease in deathsfrom cervical cancer was proportional to the screeningrates in various states.35 Finally, women who do notdevelop invasive cancer are more likely to have had aPap test than women with cancer. In a Canadian study,the relative risk for women who had not had a Pap testfor 5 years was 2.7,33 and screening history was a
CERVICAL AND VAGINAL CYTOLOGY2
highly significant risk factor independent of otherfactors such as age, income, education, sexual history,and smoking. In Denmark, a woman’s risk of developingcervical cancer decreased in proportion to the numberof negative smears she had had: by 48% with just onenegative smear, 69% with two to four negative smears,and 100% with five or more smears.93 At present, fewdoubt the role the Pap test has played in reducing theincidence of cervical cancer.
Recommended screening intervals vary amongdifferent countries. The American Cancer Societyrecommends that all women who are or have beensexually active or are 18 years of age or older have anannual Pap test and pelvic examination. After three ormore consecutive normal annual results, the Pap testmay be performed less frequently at the discretion of thewoman’s physician.139
SAMPLING AND PREPARATIONMETHODS
To obtain an ideal specimen, the following guidelineshave been established by the National Committee forClinical Laboratory Standards.112
Patient instructions:
• schedule the examination 2 weeks after the firstday of the last menstrual period (LMP) – morespecifically, it is preferable to avoid examinationduring menses because blood may obscuresignificant findings
• do not use vaginal medication, vaginalcontraceptives, or douches for 48 hours before theappointment
• Intercourse is not recommended the night beforethe appointment
Specimen collection:
• specimens should be obtained after a non-lubricated speculum (moistened only with warmwater if needed) is inserted
• excess mucus or other discharge should be removedgently with ring forceps holding a folded gauze pad
• the sample should be obtained before theapplication of acetic acid or Lugol’s iodine
• an optimal sample includes cells from theectocervix and endocervix
S2638-01.qxd 12/11/02 11:42 Page 2

Conventional smears
Conventional smears are often obtained using acombination of a spatula and brush. The spatula is usedfirst. Although a wooden or plastic spatula is acceptable,the plastic spatula is recommended because woodenfibers may trap diagnostic material. The spatula isrotated at least 360°. The sample may be smeared onone half of a slide and spray fixed (the other half shouldbe covered to avoid coating it with fixative before theendocervical sample is applied). Alternatively, one mayset aside the spatula sample momentarily while theendocervical brush sample is obtained.
After the brush is inserted in the endocervical canal,some bristles should still be visible. If inserted too far,there may be inadvertent sampling of the lower uterinesegment (LUS), which causes diagnostic difficultiesbecause its epithelium resembles HSIL and adeno-carcinoma in situ (AIS). The brush should be rotatedgently only one quarter turn. A larger rotation is un-necessary because the circumferential bristles are incontact with the entire surface the moment the brush isinserted.
The spatula sample, if not already applied and fixed,should be applied, then the brush sample rolled over theslide, followed by immediate fixation. The two samplescan be placed in quick succession on two separate halvesof the slide, or the endocervical sample can be rolleddirectly over the spatula sample, both covering theentire slide. Immediate fixation (within seconds) is criticalin order to prevent air-drying artifact, which distorts thecells and hinders interpretation.
The broom-like brush (‘broom’) has a flat array ofplastic strips contoured to conform to the cervix, withlonger strips in the middle. This design allows simul-taneous sampling of the endocervix and ectocervix. Thelong middle strips are inserted into the os until theshorter outer strips bend against the ectocervix. Thebroom is rotated three to five times. To transfer thematerial, each side of the broom is stroked once acrossthe slide in a painting motion.
The cotton swab moistened with saline was muchused in the past, but is no longer recommended becauseits fibers trap cells, reducing the efficiency of celltransfer onto slides.
SAMPLING AND PREPARATION METHODS 3
Coating fixatives contain alcohol and polyethyleneglycol and are applied by pump sprays, by droppers fromdropper bottles, or by pouring from an individualenvelope included as part of a slide-preparation kit.Alternatively, the smear can be immersed directly into acontainer filled with 95% ethanol.
Samples for liquid-based preparations (see ‘Liquid-based preparations’ below) are obtained as describedabove except instead of smearing the cells on a slide, thecollection device is rinsed in a vial containing a liquidfixative.
Liquid-based preparations
An important landmark in the history of the Pap test occurred in 1996 when the Food and DrugAdministration (FDA) approved the ThinPrep™ (CytycCorporation, Boxborough, MA) as an alternative to theconventional cervicovaginal smear, followed, in 1999,by approval of the AutoCyte Prep™ (now known asSurePrep™) (TriPath Imaging, Burlington, NC). Theseso-called ‘liquid-based preparations’ were a byproduct of the development of automated screening devices.They were developed to minimize cell overlap so that automated screeners would perform better inidentifying abnormal cells. These preparations per-formed so well in clinical trials against conventionalsmears that they found a market even withoutautomated screening.22,88
The two preparation methods, although different intheir mechanics, produce preparations that are remark-ably similar in appearance. They are both approved foruse with non-gynecologic specimens.
ThinPrep™
The practitioner obtains the ThinPrep sample witheither a ‘broom’-type device or a plastic spatula/endocervical brush combination. (The FDA did notapprove it for use with wooden spatulas.) The samplingdevice(s) is (are) rinsed in a methanol-based pre-servative solution (PreservCyt) for transport to thecytology laboratory and the sampling device isdiscarded. The vials are placed one at a time on the
Choices of sampling devices:
• spatula plus brush
• ‘broom’
Fixatives for conventional smears:
• coating fixatives
• 95% ethanol (‘wet fixation’)
S2638-01.qxd 12/11/02 11:42 Page 3
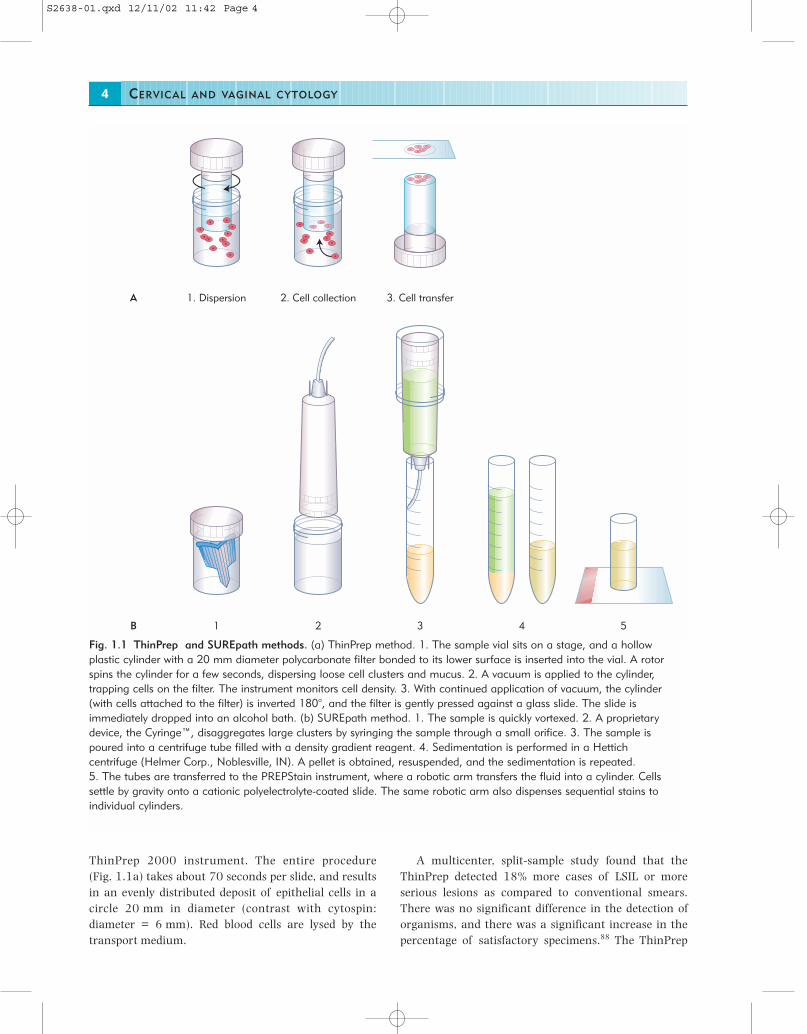
ThinPrep 2000 instrument. The entire procedure (Fig. 1.1a) takes about 70 seconds per slide, and resultsin an evenly distributed deposit of epithelial cells in acircle 20 mm in diameter (contrast with cytospin:diameter = 6 mm). Red blood cells are lysed by thetransport medium.
CERVICAL AND VAGINAL CYTOLOGY4
A multicenter, split-sample study found that theThinPrep detected 18% more cases of LSIL or moreserious lesions as compared to conventional smears.There was no significant difference in the detection oforganisms, and there was a significant increase in thepercentage of satisfactory specimens.88 The ThinPrep
1. Dispersion 2. Cell collection 3. Cell transferA
1 2 3 4 5B
Fig. 1.1 ThinPrep and SUREpath methods. (a) ThinPrep method. 1. The sample vial sits on a stage, and a hollowplastic cylinder with a 20 mm diameter polycarbonate filter bonded to its lower surface is inserted into the vial. A rotorspins the cylinder for a few seconds, dispersing loose cell clusters and mucus. 2. A vacuum is applied to the cylinder,trapping cells on the filter. The instrument monitors cell density. 3. With continued application of vacuum, the cylinder(with cells attached to the filter) is inverted 180°, and the filter is gently pressed against a glass slide. The slide isimmediately dropped into an alcohol bath. (b) SUREpath method. 1. The sample is quickly vortexed. 2. A proprietarydevice, the Cyringe™, disaggregates large clusters by syringing the sample through a small orifice. 3. The sample ispoured into a centrifuge tube filled with a density gradient reagent. 4. Sedimentation is performed in a Hettichcentrifuge (Helmer Corp., Noblesville, IN). A pellet is obtained, resuspended, and the sedimentation is repeated. 5. The tubes are transferred to the PREPStain instrument, where a robotic arm transfers the fluid into a cylinder. Cellssettle by gravity onto a cationic polyelectrolyte-coated slide. The same robotic arm also dispenses sequential stains toindividual cylinders.
S2638-01.qxd 12/11/02 11:42 Page 4

appears to be at least as good as the conventional smearin the detection of significant endocervical lesions.132 Ina case–control study, the prevalence of significantglandular abnormalities diagnosed by the ThinPrep(0.14%) was similar to that for conventional smears(0.11%), and there was no apparent decrease inspecificity.6 Classical features of glandular lesions arepreserved in ThinPreps.43,67
Data also show comparable results between ThinPrepslides and conventional smears for the detection ofendometrial pathology.57,128
In 1996, the FDA cleared the ThinPrep 2000 systemfor cervical cancer screening. Subsequently, the FDAapproved the claim that the ThinPrep test is ‘signifi-cantly more effective’ than the conventional smear forthe detection of LSIL and more severe lesions, and thatthe specimen quality was ‘significantly improved’ overthat of the conventional smear.
A batch-processing version, the ThinPrep 3000,received FDA approval in the year 2000. It uses thesame consumables (filters and solutions), but allowsautomated processing of 80 samples at one time.
The ThinPrep collection vial has been approved bythe FDA for direct testing for human papillomavirus(HPV). The results of HPV testing are useful for man-aging women whose smears show atypical squamouscells (ASC).141
SUREPath™
TriPath Imaging has developed the SUREPath Pap test(formerly AutoCyte Prep, formerly CytoRich) for sam-ples collected in an ethanol-based transport medium. Incontrast to the ThinPrep method, the clinician snips offthe tip of the collection device and submits it to thelaboratory in the sample vial. The process is shown inFig. 1.1b. The equipment to prepare slides includes aHettich centrifuge (Helmer Corp., Noblesville, IN) and aPREPStain robotic sample processer with computer andmonitor. The PrepMate‘ is an optional accessory thatautomates mixing the sample and dispensing it onto thedensity reagent; it can batch up to 12 specimens. Inaddition to preparing an evenly distributed deposit ofcells in a circle 13 mm in diameter, the method incor-porates a final staining step that discretely stains eachindividual slide.
A multicenter, split-sample clinical trial showed a7.2% increase in LSIL or more serious lesions with theAutoCyte Prep and than with the ThinPrep, a signi-ficant increase in the percentage of satisfactoryspecimens.22
AUTOMATED SCREENING 5
AUTOMATED SCREENING
Historical overview
Automated cytology screening devices have been underdevelopment since the 1950s. The first computerizedscreening system was developed in the United States by Airborne Instruments Inc. and was called theCytoanalyzer.150 In preclinical trials it did not performas well as expected, and the project was discontinued.The difficulty of the task was soon appreciated, espe-cially the inherent problems with analyzing smearsprepared in the conventional manner. Despite setbacks,research into cervical cytology screening continued,especially in Europe and Japan, throughout the 1970sand 1980s, with the development of systems such asthe Quantimet,63 BIOPEPR,168 CERVIFIP,151 CYBEST,149
DIASCANNER,115,143 FAZYTAN,129 and LEYTAS.126
Some of these instruments are now in museums; othershave served as prototypes for systems that arecommercially available or are still under development.
Although European investigators largely lost interestin cytology automation in the 1990s,152 researchers inthe United States and Canada, supported primarilythrough venture capital, retained their enthusiasm,resulting in advances in research and development.Foremost in the field in recent years have been AutoCyteInc. (formerly Roche Image Analysis Systems), CytycCorp., Neopath Inc., and Neuromedical Systems, Inc. Animportant three-way merger took place in 1999, whenAutoCyte, after purchasing the intellectual property ofNeuromedical Systems, merged with Neopath to form anew company called TriPath Imaging. In 1998, the FDAapproved the AutoPap System (now called FocalPoint™)(TriPath Imaging, Burlington, NC) as a primaryscreener for cervicovaginal smears.
FocalPoint™
The FocalPoint is a self-contained instrument thatclassifies conventionally prepared smears withouthuman intervention. The device uses algorithms tomeasure cellular features such as nuclear size, inte-grated optical density, nuclear to cytoplasmic ratio, andnuclear contour. The development team worked closelywith its Medical Director, Dr Stanley Patten, to incor-porate the morphologic criteria he had establishedthrough planimetry and ocular micrometry for thediagnosis of squamous and glandular lesions.86
The FocalPoint (formerly AutoPap) was originallydesigned as a primary screening device that would
S2638-01.qxd 12/11/02 11:42 Page 5

eliminate the need to screen as many as one-half of allsmears. The instrument was temporarily redesigned as arescreening device called the AutoPap 300 QC System,for which it obtained FDA approval in 1995. This systembecame obsolete in the year 2000. Subsequently, a newalgorithm was incorporated, which obtained FDAapproval as a primary screening device in 1998(AutoPap System-Primary Screener). In this mode, thedevice is used in the initial screening of smears. Itidentifies up to 25% of slides as requiring no furtherreview. Of the remaining 75% of slides that requirereview, it identifies at least 15% for a second manualreview. This population may be used as a substitute forthe 10% random review mandated by federalregulations (see Chapter 17).
A barcode is applied to each slide, and slides areloaded into slide trays. Up to 288 slides can be loaded at a time (eight slides per tray). Each slide is analyzedand assigned a score, which the device uses to rankslides according to the likelihood of an abnormality. Anyslide deemed unsuitable for analysis because ofpreparation or coverslipping problems requires manualreview.
The accuracy of the instrument was evaluated in amulticenter, two-arm, prospective clinical trial at fivecommercial laboratories.160 Each slide was first eva-luated in the conventional manner, and 10% of thecases judged ‘within normal limits’ were rescreened.The same slides were then processed by the AutoPapSystem. The AutoPap System detected significantlymore abnormal slides – atypical squamous cells ofundetermined significance (ASCUS) or greater – thanconventional practice (86 vs 79%).
CERVICAL AND VAGINAL CYTOLOGY6
reviewer to specific locations, mapped by the FocalPoint,which contain the most abnormal cells.86
ACCURACY AND REPRODUCIBILITY
Like most tests, the Pap test suffers from both falsenegatives and false positives. In fact, many women withcervical cancer have a history of one or more negativesmears.7,14,17,40,45,49,80,81,109,124,134,153 The false-negativerate for invasive cancer ranges from 16 to 82%. Therelative contributions of sampling and laboratory erroralso vary from study to study, and may depend on howcarefully retrospective rescreening is performed.
The false-negative rate for preinvasive lesions isdifficult to establish. With invasive cancer, cases can beobtained from tumor registries, whereas most studies of preinvasive lesions suffer from ‘verification bias’ (i.e.cases are referred for biopsy on the basis of an abnormalsmear, and women with negative Paps are not biopsied).The few relatively unbiased studies show that the meansensitivity of the Pap test is 47% (range 30–80%), andthe mean specificity is 95% (range 86–100%).110
The interobserver reproducibility of cytologic inter-pretations is also not perfect. In a large study of women,most of whom had mild cytologic abnormalities, theunweighted kappa statistic for four categories of diag-nosis – negative, atypical, low-grade squamous intra-epithelial lesion (LSIL), and high-grade intraepitheliallesion (HSIL) was 0.46, indicating moderate repro-ducibility.145 (Roughly, a kappa of 0 or less representspoor agreement, 0–0.2 slight agreement, 0.2–0.4 fairagreement, 0.4–0.6 moderate agreement, 0.6–0.8 verygood agreement, and 0.8–1.0 almost perfect agree-ment.) Cytopathologists can take heart from the factthat, in the same study, the reproducibility of histologicinterpretations of cervical biopsies, also for four cate-gories of diagnosis, was identical (0.46). The greatestdisagreement with Paps involved those originallyinterpreted as showing ASC-US; the second revieweragreed with only 43% of cases. The greatest dis-agreement with biopsies involved those originallyinterpreted as LSIL; the second reviewer concurred inonly 43% of cases.145
DIAGNOSTIC TERMINOLOGY ANDREPORTING SYSTEMS
Papanicolaou devised a class system for reportingcervical smears, which was originally intended to
Limitations of FocalPoint include:
• it is not approved for Pap slides from ‘high-risk’women, however that is defined by the laboratory
• performance characteristics have not beenestablished for:– endometrial cells in women ≥ 40 years of age – reactive changes of radiation and atrophy– rare malignant tumors
• it is not compatible with all staining methods
Although originally approved for use with conventionalsmears only, FocalPoint subsequently obtained FDAapproval for use with SurePath/PrepStain slides (but notThinPrep slides). TriPath is developing location-guidedscreening, which incorporates electronic slide dottingand an automated stage. The goal is to guide the human
S2638-01.qxd 12/11/02 11:42 Page 6

convey his degree of suspicion that the patient hadcancer: class I, absence of atypical or abnormal cells;class II, atypical cytology but no evidence of malig-nancy; class III, cytology suggestive of but not con-clusive for malignancy; class IV, cytology stronglysuggestive of malignancy; and class V, cytology con-clusive for malignancy. Over time, however, thePapanicolaou class system underwent many modifica-tions by different laboratories and was not used in auniform fashion.95 Over the years, it was replaced insome laboratories by descriptive terms borrowed fromhistologic classifications of preinvasive squamouslesions. These were originally divided into carcinoma insitu, which was a high-risk lesion of immature, un-differentiated atypical cells, and dysplasia (subdividedinto mild, moderate, and severe), considered to be a low-risk lesion comprised of more mature squamous cells. Inthe 1960s, Dr Ralph Richart challenged the duality ofdysplasia/carcinoma in situ and proposed a new term,cervical intraepithelial neoplasia (CIN). CIN was gradedfrom 1 to 3, but Dr Richart believed that CIN 1 (milddysplasia) had a strong propensity to progress to CIN 3and, by implication, to cancer. He based his belief inlarge part on his studies of the natural history of CIN 1.The high rate of progression found in his study131 mostlikely related to the very stringent entry criteria: he onlyfollowed women who had three consecutive Paps withCIN 1. His data showed a higher progression rate formild dysplasia than most other natural historystudies.76 The CIN concept was highly influential. It ledto the belief that the behavior of any given CIN wasunpredictable, and that they are all better treated on thebasis of size and location rather than grade. So thingsremained for two decades.
In 1989, the Bethesda System was introduced tostandardize the reporting of cervical cytology results111
and to incorporate new insights gained from thediscovery of HPV. The name for preinvasive squamouslesions was changed to squamous intraepithelial lesion,subdivided into only two grades, low and high, based onthe evolving understanding of the biology of HPV (see‘Squamous intraepithelial lesions’ below). The firstBethesda System workshop, in 1988, was followed bytwo others, in 1991 and 2001, which made modifica-tions to the original framework and terminology. The2001 workshop broadened participation by using adedicated website on the Internet, and an electronicbulletin board received more than 1000 commentsregarding draft recommendations. The 2001 BethesdaSystem, like its predecessors, recommends a specificformat for the cytology report, starting with an explicit
THE BETHESDA SYSTEM 7
statement on the adequacy of the specimen, followed bya general categorization and an interpretation/result.140
THE BETHESDA SYSTEM
Specimen adequacy
One of the most important advances of the BethesdaSystem is its recommendation that each Pap reportshould begin with a statement of adequacy. In 1988,the Bethesda System proposed three categories forspecimen adequacy: ‘satisfactory’, ‘less than optimal’(renamed ‘satisfactory but limited by ….’ in 1991), and‘unsatisfactory’. The 2001 Bethesda System eliminatedthe middle category because it was confusing toclinicians and prompted unnecessary repeat Pap tests.Nevertheless, the 2001 Bethesda System advocatesmentioning the presence or absence of a transformationzone component, and permits comments on obscuringelements. The 2001 Bethesda System criteria foradequacy are listed in Table 1.1. They are somewhatarbitrary, because scientific data on adequacy arelimited at present, particularly regarding the minimumnumber of cells needed for an adequate sample.
Table 1.1 The 2001 Bethesda System CategoriesFor Specimen Adequacy
Satisfactory for evaluationA satisfactory squamous component must bepresent (see text)Note the presence/absence of endocervical/transformation zone componentObscuring elements (inflammation, blood, dryingartifact, other) may be mentioned if 50–75% ofepithelial cells are obscured
Unsatisfactory for evaluationSpecimen rejected/not processed because (specifyreason). Reasons may include:
• lack of patient identification
• unacceptable specimen (e.g. slide broken beyondrepair)
Specimen processed and examined, butunsatisfactory for evaluation of an epithelialabnormality because (specify reason). Reasons mayinclude:
• insufficient squamous component (see text)
• obscuring elements cover more than 75% ofepithelial cells.
S2638-01.qxd 12/11/02 11:42 Page 7

It is easy to determine whether a specimen is adequateor unsatisfactory in most cases. Slides received withoutpatient identification or broken beyond repair should berejected as unsatisfactory. An appropriately labeledsmear with an adequate complement of well-preservedsquamous and endocervical cells is clearly satisfactory.
One of the components of an adequate smear is anadequate squamous component. In the 1988 and 1991Bethesda Systems, the requirement for an adequatesquamous component was defined as ‘well-preserved andwell-visualized squamous epithelial cells should cover morethan 10% of the slide surface’.83 This guideline, however,was interpreted differently by different cytologists. Evenin laboratories that interpreted it literally, observersconsistently overestimated the percentage of slidecoverage by squamous cells.130
During the 2001 Bethesda System conference, therequirement was redefined as an ‘estimated number ofsquamous cells’, the minimum being different forconventional versus liquid-based preparations:
CERVICAL AND VAGINAL CYTOLOGY8
The minimum number of 5000 squamous cells for anadequate liquid-based preparation was based on dataobtained during the development of the AutoCyte Prep(now SurePath/PrepStain), during which correlationswere made between the false-negative rate and squam-ous cell cellularity.51 Because liquid-based preparationslikely represent a more homogeneous representation ofthe material obtained by the collection device,64 a morestringent requirement was imposed on conventionalsmears.
Whether or not a slide contains an adequate squam-ous cell component is immediately apparent in mostcases. In borderline cases, techniques are available forestimating adequacy: reference images for conventionalsmears and a spot-counting procedure for liquid-basedpreparations.
With conventional smears, reference images of knowncell counts are useful for estimating cellularity.130
Because of this, the Bethesda 2001 System developedtemplates to standardize the estimation of squamouscell cellularity on conventional smears (Fig. 1.2).
For liquid-based preparations, a minimum of ten fieldsshould be counted along a diameter that includes thecenter of the slide (Fig. 1.3a). If the preparation has‘holes’, these should be represented in the fields counted(Fig. 1.3b). The average number of squamous cells is
Type of preparation and minimumnumber of cells:
• liquid-based – 5000
• conventional – 8000–12 000
Illustration continued on following page(a)
Figure 1.2 Templates forestimating squamous cellcellularity of conventionalsmears. These images can beused for estimating theadequacy of the squamouscell component ofconventional smears. Theydemonstrate a fixed numberof cells observed using low-magnification (4× objective,10× ocular, and field number20). A. Approximately 150squamous cells. The entireslide would need to becovered at this level ofcellularity to have 10,000cells.
S2638-01.qxd 12/11/02 11:42 Page 8

THE BETHESDA SYSTEM 9
Figure 1.2 ContinuedTemplates for estimatingsquamous cell cellularity ofconventional smears. Theseimages can be used forestimating the adequacy ofthe squamous cellcomponent of conventionalsmears. They demonstrate afixed number of cellsobserved using low-magnification (4× objective,10× ocular, and field number20). B. Approximately 500squamous cells. 20 fieldswould need to be covered at this cellularity for a total of 10,000 cells. C. Approximately 1000squamous cells. 10 fieldswould need to be covered atthis cellularity for a total of10,000 cells. (Courtesy of Dr.George G. Birdsong, GradyHealth System, Atlanta, GA.)
(b)
(c)
S2638-01.qxd 12/11/02 11:43 Page 9
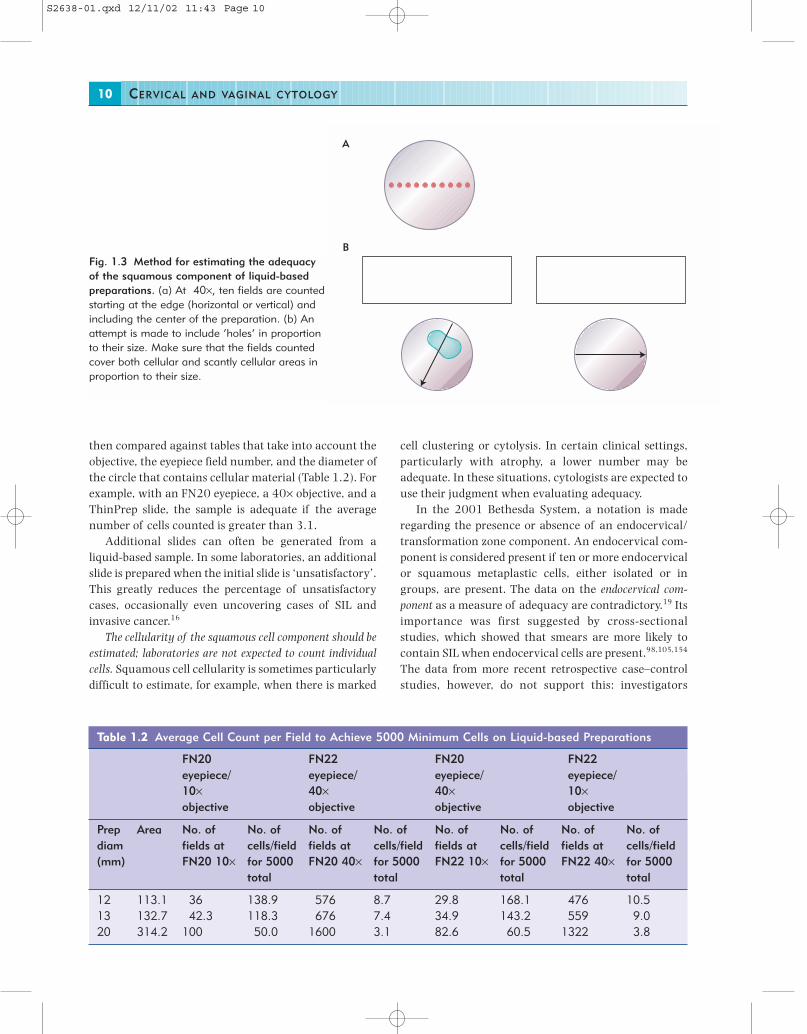
then compared against tables that take into account theobjective, the eyepiece field number, and the diameter ofthe circle that contains cellular material (Table 1.2). Forexample, with an FN20 eyepiece, a 40× objective, and aThinPrep slide, the sample is adequate if the averagenumber of cells counted is greater than 3.1.
Additional slides can often be generated from aliquid-based sample. In some laboratories, an additionalslide is prepared when the initial slide is ‘unsatisfactory’.This greatly reduces the percentage of unsatisfactorycases, occasionally even uncovering cases of SIL andinvasive cancer.16
The cellularity of the squamous cell component should beestimated; laboratories are not expected to count individualcells. Squamous cell cellularity is sometimes particularlydifficult to estimate, for example, when there is marked
CERVICAL AND VAGINAL CYTOLOGY10
cell clustering or cytolysis. In certain clinical settings,particularly with atrophy, a lower number may beadequate. In these situations, cytologists are expected touse their judgment when evaluating adequacy.
In the 2001 Bethesda System, a notation is maderegarding the presence or absence of an endocervical/transformation zone component. An endocervical com-ponent is considered present if ten or more endocervicalor squamous metaplastic cells, either isolated or ingroups, are present. The data on the endocervical com-ponent as a measure of adequacy are contradictory.19 Itsimportance was first suggested by cross-sectionalstudies, which showed that smears are more likely tocontain SIL when endocervical cells are present.98,105,154
The data from more recent retrospective case–controlstudies, however, do not support this: investigators
A
BFig. 1.3 Method for estimating the adequacyof the squamous component of liquid-basedpreparations. (a) At 40×, ten fields are countedstarting at the edge (horizontal or vertical) andincluding the center of the preparation. (b) Anattempt is made to include ‘holes’ in proportionto their size. Make sure that the fields countedcover both cellular and scantly cellular areas inproportion to their size.
Table 1.2 Average Cell Count per Field to Achieve 5000 Minimum Cells on Liquid-based Preparations
FN20 FN22 FN20 FN22eyepiece/ eyepiece/ eyepiece/ eyepiece/10× 40× 40× 10×objective objective objective objective
Prep Area No. of No. of No. of No. of No. of No. of No. of No. ofdiam fields at cells/field fields at cells/field fields at cells/field fields at cells/field(mm) FN20 10× for 5000 FN20 40× for 5000 FN22 10× for 5000 FN22 40× for 5000
total total total total
12 113.1 36 138.9 576 8.7 29.8 168.1 476 10.513 132.7 42.3 118.3 676 7.4 34.9 143.2 559 9.020 314.2 100 50.0 1600 3.1 82.6 60.5 1322 3.8
S2638-01.qxd 12/11/02 11:43 Page 10

have found no association between false-negative Papsand the absence of endocervical cells.107,118 Finally,retrospective cohort studies have shown that womenwhose initial smears lack endocervical cells do notdevelop more lesions on follow-up than women whosesmears do have an endocervical component,26,75,106
implying that an endocervical component is notessential. Currently, therefore, a smear without endo-cervical cells is not considered unsatisfactory, althoughthe absence of an endocervical/transformation zonecomponent is mentioned as a ‘quality indicator’. This isnot to imply that a repeat Pap is necessary. Clinicians areexpected to use their judgment, and to considerrepeating the Pap if the patient is at high risk forcervical cancer.
General categorization
The ‘general categorization’ is an optional component ofthe 2001 Bethesda System.
THE NORMAL PAP 11
THE NORMAL PAP
Squamous cells
The ectocervix is lined by a stratified squamous epithe-lium that matures under the influence of estrogen. Themost mature squamous cells are called superficial cells.They have a small, pyknotic nucleus that is 5–6 µm indiameter. Intermediate cells have a larger nucleusmeasuring 8 µm in diameter, which is not pyknotic butinstead has a finely granular texture. Both superficialand intermediate cells are large polygonal cells withtransparent pink or green cytoplasm (Fig. 1.4).
Immature squamous cells are called parabasal cellsand basal cells. Because a Pap test does not usuallyscrape off the entire thickness of the epithelium, onlythe upper few layers, immature cells near the base of amature epithelium are not sampled. An immatureepithelium, such as that seen in low-estrogen states, iscomposed throughout its thickness by parabasal-typeand/or basal-type cells, which can be and are obtainedby Pap sampling devices.
Three categories:
• negative for intraepithelial lesion or malignancy
• epithelial cell abnormality
• other
The 1991 Bethesda categories ‘within normal limits’and ‘benign cellular changes’ were combined into asingle ‘negative’ category in 2001. ‘Other’ includes casesthat do not fit neatly into one of the other two cate-gories: non-epithelial malignancies such as melanomaand lymphoma, and benign-appearing endometrial cellsin women over 40 years of age.
Specimens are categorized according to the mostsignificant abnormality identified.
Interpretation and results
Recommended terminology for reporting findings islisted in Table 1.3.
Non-neoplastic findings, other than organisms, areoptional, given that many clinicians desire the Pap test report to be as concise as possible. Findings of noclinical consequence, if mentioned, may result inconfusion and even unnecessary repeat testing.Nevertheless, many cytologists believe it is important todocument that certain findings were interpreted asbenign, particularly those that can mimic a neoplasm.
Low estrogen states include:
• menarche
• postpartum period (Fig. 1.5)
• postmenopause (Fig. 1.6)
• Turner’s syndrome
• status post bilateral oophorectomy
So-called parabasal cells are round or oval rather than polygonal and have a variably sized nucleus that is usually larger than that of an intermediate cell. ‘Basal cells’ are even smaller and have very scantcytoplasm.
Basal and parabasal cells are the hallmark of atrophyin postmenopausal women. In deeply atrophic smearsno superficial or intermediate cells are seen, only para-basal and basal cells. In addition, atrophic epithelium inpostmenopausal women is prone to injury and inflam-mation and often shows a spectrum of changes thatmust be recognized as normal and not confused with asignificant lesion. The sheets of immature cells arecrowded and syncytial, mimicking the architecturalfeatures of an HSIL (see Fig. 1.6). Nevertheless, thechromatin texture in atrophy is finely granular andevenly distributed, and nuclear contours remain mostlysmooth and thin. A curious variant, termed transitionalcell metaplasia, is notable for prominent longitudinal
S2638-01.qxd 12/11/02 11:43 Page 11

nuclear grooves, wrinkled nuclei, and small perinuclearhalos157 (see Fig. 1.6b). Cellular degeneration is seen insome cases of atrophy (Fig. 1.7a). Air-drying, a com-mon artifact in atrophic specimens, causes artificialnuclear enlargement. Dark blue, rounded, amorphous
CERVICAL AND VAGINAL CYTOLOGY12
masses known as ‘blue blobs’, thought to representeither condensed mucus or degenerated bare nuclei, aresometimes seen (Fig. 1.7b), as is a granular background(see Fig. 1.7) that resembles the tumor diathesisassociated with invasive cancers.
Table 1.3 The 2001 Bethesda System (Abridged)
SPECIMEN ADEQUACY (see Table 1.2)
GENERAL CATEGORIZATION (Optional)Negative for intraepithelial lesion or malignancyEpithelial cell abnormalityOther
INTERPRETATION/RESULTSNegative for Intraepithelial Lesion or Malignancy
OrganismsTrichomonas vaginalisFungal organisms morphologically consistent with Candida speciesShift in flora suggestive of bacterial vaginosisBacteria morphologically consistent with Actinomyces speciesCellular changes consistent with herpes simplex virus
Other non-neoplastic findings (Optional to report; list not comprehensive)Reactive cellular changes associated with: inflammation (includes typical repair); radiation; intrauterine
contraceptive device (IUD)Glandular cells status post-hysterectomyAtrophy
Epithelial cell abnormalitiesSquamous cell
Atypical squamous cells (ASC)of undetermined significance (ASC-US)cannot exclude HSIL (ASC-H)
Low-grade squamous intraepithelial lesion (LSIL)encompassing: human papillomavirus (HPV)/mild dysplasia/cervicalintraepithelial neoplasia (CIN) 1
High-grade squamous intraepithelial lesion (HSIL)encompassing: moderate and severe dysplasia, carcinoma in situ; CIN 2 and CIN 3
Squamous cell carcinomaGlandular cell
Atypical glandular cells (AGC) (specify endocervical, endometrial, or not otherwise specified)Atypical glandular cells, favor neoplastic (specify endocervical or not otherwise specified)
Endocervical adenocarcinoma in situ (AIS)Adenocarcinoma
Other (List not comprehensive)Endometrial cells in a woman ≥ 40 years of age
AUTOMATED REVIEW AND ANCILLARY TESTING (INCLUDE AS APPROPRIATE)
EDUCATIONAL NOTES AND SUGGESTIONS (OPTIONAL)
S2638-01.qxd 12/11/02 11:43 Page 12

Parabasal cells are also the constituents of squamousmetaplasia of the endocervix. Squamous metaplasia is acommon morphologic alteration of the endocervicalepithelium usually limited to the transformation zone inwomen who otherwise have good squamous matura-tion. It is identified on smears as flat sheets of immaturesquamous cells (parabasal cells) arranged in aninterlocking fashion like paving stones (Fig. 1.8). Theparabasal cells may show mild variation in nuclear size, with slightly irregular contours and slighthyperchromasia.
THE NORMAL PAP 13
Squamous metaplasia, as defined cytologically, isalways composed of parabasal cells (immature squam-ous cells). So-called mature squamous metaplasia, ahistologic term describing mature squamous epitheliumoverlying endocervical glands, is not recognized as suchon cytologic preparations.
Other normal changes of squamous cells arehyperkeratosis and parakeratosis. Hyperkeratosis is abenign response of stratified squamous epithelium dueto chronic mucosal irritation, as in uterine prolapse.Anucleate, mature, polygonal squamous cells may benumerous and appear as single cells or plaques oftightly adherent cells (Fig. 1.9a). Such cells are benign
Fig. 1.4 Superficial and intermediate squamous cells.The mature squamous epithelium of the ectocervix inwomen of reproductive age is composed throughout mostof its thickness by superficial (small arrow) andintermediate (large arrow) cells. Rare lactobacilli arepresent.
Fig. 1.5 Parabasal and basal cells (postpartum smear).Parabasal cells (large arrow) are oval and typically havedense cytoplasm. Basal cells (small arrow) are similar, buthave less cytoplasm. Many cells have abundant pale-yellow staining glycogen, a characteristic but non-specificfeature of squamous cells of pregnancy and thepostpartum period.
(a)
(b)Fig. 1.6 Parabasal cells (postmenopausal smear).(a) Atrophic epithelium is composed almost exclusively ofparabasal cells, often arranged in broad, flowing sheets(b) Transitional cell metaplasia. In this uncommoncondition, the atrophic epithelium in postmenopausalwomen resembles transitional cell epithelium by virtue ofits longitudinal nuclear grooves. Nuclear membraneirregularities raise the possibility of an HSIL, but thechromatin is pale and finely textured.
S2638-01.qxd 12/11/02 11:43 Page 13

and should not be considered to be an epithelial cellabnormality. This cytologic picture is mimicked bycontamination of the slide by squamous cells of thevulva or skin from the fingers of the persons handlingthe slide.
Parakeratosis, a benign reactive change also causedby chronic irritation, is characterized by small, heavilykeratinized squamous cells with dense orangeophiliccytoplasm and small, pyknotic nuclei (Fig. 1.9b). Whensuch densely keratinized cells show nuclear atypia inthe form of enlargement and membrane irregularitywith hyperchromasia, they are called ‘dyskeratocytes’or ‘atypical parakeratosis’ and should be categorized asan epithelial cell abnormality (see below).
CERVICAL AND VAGINAL CYTOLOGY14
(a)
(b)Fig. 1.7 Parabasal cells (postmenopausal smear). (a)Sometimes degenerated parabasal cells in atrophic smearshave hypereosinophilic cytoplasm and pyknotic nuclei(pseudoparakeratosis). Note the granular debris in thebackground, which is commonly seen in normal atrophicsmears. (b) Dark blue blobs are seen in some atrophicsmears. These featureless structures should not beinterpreted as a significant abnormality.
Fig. 1.8 Squamous metaplasia. Interlocking parabasalcells, as seen here, represent squamous metaplasia of theendocervix.
(a)
(b)
Fig. 1.9 Keratosis. (a) Hyperkeratosis. Anucleate squamesare a protective response of the squamous epithelium. (b)Parakeratosis. Parakeratosis appears as plaques, as seenhere, or as isolated cells.
S2638-01.qxd 12/11/02 11:43 Page 14

appearance of a picket fence; when in sheets theyresemble a honeycomb because of the well-defined cellborders and uniform cell arrangement (Fig. 1.10).Rarely, mitoses are identified. They should not raisesuspicion of a neoplasm if the cells are otherwisenormal in appearance. Tubal metaplasia is a benignalteration of the endocervical epithelium found in about30% of cone biopsy and hysterectomy specimens68
(Fig. 1.11).
THE NORMAL PAP 15
Endocervical cells
The endocervix is lined by a mucin-producing columnarcell that has an eccentrically placed nucleus with afinely granular chromatin texture and abundant vacuo-lated cytoplasm. Nucleoli are inconspicuous but becomevery prominent in reactive conditions such as cervicitis(see ‘Reactive changes’ below). Endocervical cells areoften identified in strips or sheets rather than as isolatedcells. When arranged as strips, the cells have the
(a) (b)
Fig. 1.10 Endocervical cells. (a) Normal endocervical cells are often arranged in cohesive sheets. Note the even spacingof the nuclei, their pale, finely granular chromatin, and honeycomb appearcnce. (b) Sometimes they appear as strips orisolated cells. Abundant mucin results in cup-shaped nuclei.
Fig. 1.11 Tubal metaplasia.Ciliated endocervical cellsare common.
S2638-01.qxd 12/11/02 11:43 Page 15

It is not possible to tell whether these degenerated endo-metrial cells are of epithelial or stromal origin. Sheddingof endometrial cells after day 12 (‘out of phase’) hasbeen associated with endometritis, endometrial polyps,and intrauterine devices (IUDs). In the premenopausalwoman, abnormal shedding is almost never due toendometrial adenocarcinoma.55,166 For this reason,endometrial cells do not need to be mentioned in thereport for women under 40 years of age. Some labora-tories do so anyway, to document that the cells wereidentified and interpreted as benign endometrial cells.In fact, endometrial cells can cause diagnostic diffi-culty because they are mimicked by a variety ofneoplastic cells.
CERVICAL AND VAGINAL CYTOLOGY16
Some lesions like HSIL, invasive squamous carcinoma,AIS, and small cell carcinoma, can mimic endometrialcells and are mistakenly dismissed as normal endo-metrial cells, particularly if the woman is in the first 12days of her menstrual cycle (Fig. 1.13).
Abraded endometrial cells and loweruterine segment
Occasionally, the endocervical sampling device in-advertently samples the LUS or endometrium.38 This isespecially likely when the endocervical canal isabnormally shortened, as it is after a cone biopsy.87
Cytomorphology:
• large and small tissue fragments
• glands and stroma
• stromal cells:– uniform– oval or spindle-shaped– finely granular chromatin– occasional mitoses– capillaries traverse larger fragments
• glands– tubular– straight or branching– mitoses (some cases)– extreme nuclear crowding– scant cytoplasm
Fig. 1.12 Endometrial cells. Spontaneously desquamatedendometrial cells, as in menses, are small cells arrangedin balls. Cytoplasm is scant. Nuclei around the perimeterappear to be wrapping around adjacent cells (arrows), acharacteristic but non-specific feature.
Exfoliated endometrial cells
Spontaneously exfoliated endometrial cells are oftenseen during the first 12 days of the menstrual cycle155
(Fig. 1.12).
Cytomorphology:
• balls of small cells
• scant cytoplasm
• dark nuclei
• nuclear molding
• nuclear fragmentation
Differential diagnosis:
• HSIL• invasive squamous cell carcinoma (SQC)• AIS• small cell carcinoma
The characteristic feature is the combination of glandsand stroma, often in large fragments (Fig. 1.14), eithertogether or separated. Glandular cells of the LUS re-semble endocervical cells, but have a higher nuclear tocytoplasmic ratio, are more hyperchromatic, and can bemitotically active. Because of their very high nuclear tocytoplasmic ratio, they can be confused with a signi-ficant squamous or glandular lesion38 (Fig. 1.14b,c).
Trophoblastic cells and decidual cells
Syncytiotrophoblastic cells from placental tissue areseen very rarely, perhaps in about 0.1% of smears from
S2638-01.qxd 12/11/02 11:43 Page 16

pregnant women.46 The cells are large, with abundantblue or pink cytoplasm. They have multiple nuclei thathave a granular chromatin texture and slightly irre-gular contours. Trophoblastic cells can be distinguishedfrom multinucleated histiocytes because their nuclei aredarker and more irregular in contour (Fig. 1.15). Theydo not show the prominent molding and ground-glassappearance of nuclei of Herpes simplex infection.Immunostains for human chorionic gonadotropin andhuman placental lactogen can be used to confirm theiridentity as trophoblastic cells. The presence of syncytio-trophoblastic cells is not a reliable predictor of animpending abortion.46
Decidual cells are isolated cells with abundantgranular cytoplasm, a large vesicular nucleus, and a
THE NORMAL PAP 17
prominent nucleolus. They often show degenerativechanges.
Inflammatory cells
Neutrophils are seen in all cervical specimens and donot necessarily indicate infection, but they are presentin increased numbers after injury or infection. Lympho-cytes and plasma cells are rare, but occasionally – mostoften in older women – they are numerous (Fig. 1.16).This pattern is called follicular cervicitis because biopsiesshow lymphoid follicle formation. The lymphocytes offollicular cervicitis can be confused with cells of anHSIL, endometrial cells, or lymphoma. Histiocytes areassociated with a myriad of conditions, such as menses,
(a) (b)
(c) (d)Fig. 1.13 Mimics of exfoliated endometrial cells. (a) HSIL. The cells of some HSILs are small, but are usually a littlelarger than endometrial cells, and usually arranged in flatter aggregates, not spheres. (b) SQC. Some poorly differentiatedSQCs are indistinguishable from endometrial cells. The granular debris (‘tumor diathesis’) seen here can also be seen innormal menstrual Paps. (c) AIS. Some cases of AIS have an ‘endometrioid’ appearance, but mitoses (arrows) are distinctlyuncommon in exfoliated endometrial cells. (d) Small cell carcinoma. The cells strongly resemble endometrial cells, but areeven darker, and show nuclear smearing, which is rarely seen with benign endometrial cells.
S2638-01.qxd 12/11/02 11:43 Page 17

CERVICAL AND VAGINAL CYTOLOGY18
(a) (b)
(c)
Fig. 1.14 Endometrial cells, directly sampled. (a) Anintact endometrial tubule is surrounded by well-preservedendometrial stromal cells. (b) Benign stromal cells areelongated and mitotically active (arrow), and may suggestan HSIL or a malignancy. The pale, finely granularchromatin and the association with intact endometrialglands are clues to a benign diagnosis. (c) The glandularcells are crowded and mitotically active (arrow), but evenlyspaced.
Fig. 1.15Syncytiotrophoblast. Thenuclei of thesemultinucleated cells are darkand coarsely granular, unlikethose of histiocytes.
S2638-01.qxd 12/11/02 11:43 Page 18

pregnancy, foreign bodies, radiotherapy, and endometrialhyperplasia and carcinoma (Fig. 1.17), but by them-selves are a non-specific finding of no clinicalsignificance.
Lactobacilli
The vagina of most women is colonized by a Gram-positive rod-shaped bacterium called Lactobacillus,which stains blue with the Papanicolaou stain (see Fig. 1.4). It is not pathogenic. It metabolizes the glyco-
THE NORMAL PAP 19
Fig. 1.16 Follicularcervicitis. This smear from a61-year-old woman containsnumerous lymphocytes invarious stages ofmaturation, including anoccasional plasma cell(arrow). Mitoses are present.Most normal lymphocyteshave round nuclearcontours, unlike the cells ofa high-grade SIL, to whichthey bear a superficialresemblance.
Fig. 1.17 Histiocytes. Histiocytes have abundanttransparent cytoplasm and oval, occasionally folded,nuclei.
gen contained within squamous cells, and in theresulting cellular pattern known as cytolysis, the cyto-plasm of cells has disappeared, leaving behind only bareintermediate cell nuclei (Fig. 1.18). Cytolysis can inter-fere with one’s ability to evaluate nuclear to cytoplasmicratio, an important criterion in grading SILs.
Artifacts and contaminants
The more commonly encountered artifacts and speci-men contaminants are illustrated in Fig. 1.19.
Fig. 1.18 Lactobacilli. These bacteria are part of thenormal flora of the vagina. Note the bare nuclei ofintermediate cells, which are subject to cytolysis by theseorganisms.
S2638-01.qxd 12/11/02 11:43 Page 19

ORGANISMS AND INFECTIONS
Shift in flora suggestive of bacterialvaginosis
A predominance of coccobacilli on cervical/vaginalsmears is associated with bacterial vaginosis, a disordercharacterized by a thin, milky vaginal discharge. At onetime attributed solely to Gardnerella vaginalis, it is nowclear that bacterial vaginosis can be caused by otherbacteria as well.136
CERVICAL AND VAGINAL CYTOLOGY20
The cytologic hallmark is the replacement of the normallactobacilli by shorter bacilli (coccobacilli), curvedbacilli, and mixed bacteria (Fig. 1.20). These small
Cytomorphology:
• short bacilli (coccabacilli), curved bacilli, or mixedbacteria
• no lactobacilli
• ‘filmy’ appearance of the slide
• ‘clue cells’
(a) (b)
(c) (d)
Fig. 1.19 Artifacts and contaminants. (a) ‘Cornflaking’. This refractile brown artifact results from bubbles of air trappedon superficial squamous cells, resulting in obscuring of nuclei. It can be reversed by returning the slide through xylene andalcohol to water, then restaining and recoverslipping. (b) Cockleburrs. This is the name given to radiate arrays of club-shaped orange bodies composed of lipid, glycoprotein and calcium, surrounded by histiocytes. They are most commonlyassociated with, but not limited to, pregnant patients. They have no clinical significance. (c) Trichome. These large star-shaped structures are derived from the arrow-wood plant. They stain a pale yellow and have from three to eight legs.Trichomes are produced by many different plants and vary in color, size, and shape. (d) Carpet beetle parts. These arrow-shaped structures are contaminants from sources such as gauze pads and tampons.
S2638-01.qxd 12/11/02 11:43 Page 20

organisms are numerous, give a filmy appearance to thepreparation, and frequently adhere to squamous cells,completely covering them (‘clue cells’). The charac-teristic ‘clue’ cells are not necessary for the diagnosis,however. Neutrophils are often scarce.
This pattern is common and seen in about 50% ofpatients referred to a dysplasia clinic.136 Clinical corre-lation is required for a definite diagnosis of bacterialvaginosis because the cytologic pattern is neithersufficient nor necessary for the diagnosis. Women whoare symptomatic are treated with metronidazole.
Trichomonas vaginalis
Trichomonas vaginalis is usually sexually transmitted;patients may be asymptomatic or may experienceburning, itching, and vaginal discharge.
ORGANISMS AND INFECTIONS 21
pathogenic, long, filamentous bacterium. Some squam-ous cells have a small, narrow, indistinct perinuclearhalo that is distinct from the cytopathic changes of HPV.
Patients and their sexual partners are treated withmetronidazole.
Candida
Candida albicans and Candida glabrata are fungal speciesthat can infect the vulva, vagina, and cervix. Patientsmay be asymptomatic, or they may complain ofburning, itching, and a thick, cheesy discharge.
Cytomorphology:
• 15–30 µm long
• pear shaped
• pale, eccentrically-placed nucleus
• red cytoplasmic granules
Fig. 1.20 Shift in florasuggestive of bacterialvaginosis. Numerous smallbacteria cover the slide. In some but not all cases,these bacteria adhere tosquamous cells (‘clue cells’),giving them the appearanceof a shag rug, as seen here.The Lactobacillus is absent.
The organism is a 15–30 µm pear-shaped protozoanthat has a small, very pale, eccentrically placed nucleus(Fig. 1.21). The cytoplasm often contains red granules.It is commonly accompanied by Leptothrix, a non-
Fig. 1.21 Trichomonas vaginalis. This organism has anindistinct, ghostly appearance, with a pale oval nucleusand faint red granules.
S2638-01.qxd 12/11/02 11:43 Page 21

These fungi are eosinophilic and often identified amongtangles of squamous cells (Fig. 1.22). In many cases, thesquamous cells appear skewered by the pseudohyphae.
Not all women with this finding are symptomatic,and usually only symptomatic women are treated.
Actinomyces spp.
Actinomyces species are Gram-positive anaerobic bacte-ria that are normal inhabitants of the mouth and bowel.They cause disease when mucosal barriers are breachedby mechanical trauma. The organisms spread acrossanatomic barriers and form sinus tracts. Female genitalactinomycosis is associated with the IUD and vaginalpessary. It is estimated that 7% of women with an IUDhave Actinomyces spp. on their Pap.47
CERVICAL AND VAGINAL CYTOLOGY22
Larger masses, called granules, are less common andconsist of numerous neutrophils that adhere to smallcolonies of bacteria. These organisms are usuallyharmless, but in about 15% of cases they cause pelvicinflammatory disease.142 For asymptomatic patients inwhom Actinomyces spp. are identified on smears, it isrecommended that the IUD be removed and that arepeat smear be free of the organism before the IUD isreinserted.142 Some authors have suggested thatasymptomatic patients are treated with antibioticsfollowing removal of the IUD,59 but there is no evidencethat these patients develop pelvic inflammatory diseasewithout antibiotics. Therefore, treatment of asympto-matic women is not recommended.47
Herpes simplex
Infection by the herpes simplex virus is identified by the characteristic nuclear changes of infected epithelialcells.
Cytomorphology:
• pink
• yeast forms (3–7 µm diameter)
• long pseudohyphae and true hyphae
• tangles and skewers of squamous cells(‘shishkebabs’)
Cytomorphology (Fig. 1.23):
• tangled clumps of bacteria (‘cotton balls’, ‘dustbunnies’)
• long, filamentous organisms
Fig. 1.22 Candida. Pseudohyphae and yeast forms, someof them budding from pseudohyphae, are seen. Note theskewered squamous cells.
Fig. 1.23 Actinomyces spp. These bacterial coloniesresemble dark cotton balls. The organisms arefilamentous, shown here protruding from the mass ofbacteria.
Cytomorphology:
• multinucleation
• molding of nuclei
• margination of chromatin
• ground-glass nuclei
• eosinophilic intranuclear inclusions
The nucleus has a homogeneous, glassy appearance(‘ground-glass’), and nuclear membranes are thick dueto peripheral margination of chromatin (Fig. 1.24a).
S2638-01.qxd 12/11/02 11:43 Page 22

ORGANISMS AND INFECTIONS 23
(a)
(b)
Fig. 1.24 Viral infection. (a) Herpes simplex. The nuclei of infected cells are filled withviral particles, which impart a pale, homogeneous appearance. Nuclear chromatin isvisible only at the periphery of some nuclei. Some have well-defined eosinophilicintranuclear inclusions. (b) Cytomegalovirus. Each cell has a large basophilic intranuclearinclusion that is surrounded by a halo; the cytoplasm contains small basophilic inclusionsas well. This patient was immunocompetent and asymptomatic, and the inclusions wereidentified in only a few cells.
S2638-01.qxd 12/11/02 11:43 Page 23

Multinucleation is common, with molding of nuclei.Eosinophilic intranuclear inclusions may be present.
Cytomegalovirus
Exposure to and infection by cytomegalovirus (CMV) iscommon in the general population, but clinical mani-festations, such as mononucleosis, are relatively un-common. The cytologic changes of CMV infection canbe seen on cervical–vaginal preparations from immuno-competent as well as immunocompromised patients.52
In immunocompetent patients, the infection is transientand usually asymptomatic.
CERVICAL AND VAGINAL CYTOLOGY24
Granuloma venereum (granuloma inguinale) is asexually transmitted, ulcerative condition that usuallyinvolves the labia, but can cause cervical lesions. Thecausative organism (Calymmatobacterium granulomatis,also known as the Donovan body) is an encapsulatedGram-negative bacterium that is concentrated inmacrophages and difficult to see with the Papanicolaoustain. A Giemsa stain demonstrates the intracellularorganisms.27 Another condition in which intracellularbacteria are seen is malacoplakia, which rarely involvesthe cervix.72
REACTIVE CHANGES
Whether a response to trauma, infection, hormonalstimulation, or radiation, benign reactive alterations ofsquamous and endocervical cells can be so exuberantthat they mimic a significant squamous or glandularlesion. For this reason, federal regulations require that acytotechnologist refers all cases with ‘reactive orreparative’ changes to a pathologist for review (seeChapter 17). Familiarity with their characteristicmorphologic attributes is important to preventmisdiagnoses.
Reactive changes due to inflammation,including ‘repair’
Inflammatory changes affect both squamous andendocervical cells, but the changes are often moredramatic in endocervical cells.
Reactive squamous cells show nuclear enlargementwithout significant hyperchromasia or nuclear mem-brane irregularity. The chromatin is finely anduniformly granular (Fig. 1.25). Binucleated and multi-nucleated cells are occasionally seen. Non-specificperinuclear cytoplasmic clearing is seen in benigninflammatory conditions and is distinguished from HPVeffect by its small size and the absence of increasedcytoplasmic density outlining the cavity (Fig. 1.26).
Reactive endocervical cells show much more variationin nuclear size than squamous cells, and some reactiveendocervical cell nuclei are four or five times larger than normal. They also frequently have large nucleoli(Fig. 1.27). Such changes are not uncommon in preg-nancy, where in their extreme form, they represent theArias–Stella reaction;15 in patients with endocervicalpolyps; and in inflammation of any cause. Thesechanges are also seen in microglandular hyperplasia, arelatively common benign alteration of endocervical
Cytomorphology:
• mononuclear cells
• markedly enlarged
• basophilic intranuclear inclusions
• small granular cytoplasmic inclusions
Infected cells are markedly enlarged, and the nucleihave large basophilic inclusions that are surrounded bya halo. Multiple small, granular cytoplasmic inclusionsare also present (Fig. 1.24b). The infected cells are endo-cervical and/or ectocervical in origin.62
Chlamydia trachomatis
Chlamydia trachomatis is one of the most commonsexually transmitted pathogens and a leading cause ofcervicitis, endometritis, and pelvic inflammatory dis-ease. Cytologic criteria for diagnosis, such as cyto-plasmic vacuolization or an inflammatory infiltratecomposed of transformed lymphocytes, have beenshown to have low diagnostic accuracy.18 Laboratorieshave therefore abandoned cytologic diagnosis in favor ofother methods such as culture.
Rare infections
Amebiasis of the female genital tract caused by Enta-moeba histolytica is uncommon; 10–20% of cases havebeen associated with neoplasms.5 The organisms, whichrange in size from 12 to 40 µm and have small, eccentricnuclei and abundant vacuolated cytoplasm, may bemisinterpreted as large histiocytes. Erythrophagocytosisis common. Unlike E. histolytica, Entamoeba gingivalis isnot associated with a pathogenic role in genitalinfections, although it has been described as accom-panying Actinomyces spp. in patients using IUDs.37
S2638-01.qxd 12/11/02 11:43 Page 24

epithelium associated with oral contraceptive use.Microglandular hyperplasia was originally described inhistologic material, where it was sometimes confusedwith adenocarcinoma. Cytologic changes range fromentirely normal endocervical cells to marked endo-cervical atypia, often with prominent cytoplasmicvacuolization165 (Fig. 1.28). In all cases of reactiveendocervical atypia the benign nature of the cells isbetrayed by the fine, uniform granularity of theirchromatin and by a spectrum of changes that includesbenign endocervical cells.
Reparative changes result from injury to the cervicalepithelium and the proliferation of reserve cells, whichgrow to re-epithelialize a focus of ulceration. Typicalrepair is composed of flat sheets of cells with enlarged
REACTIVE CHANGES 25
(a)
(b)
Fig. 1.25 Reactive squamous cells. Benign squamouscells show only nuclear enlargement; there is very littlenuclear irregularity or hyperchromasia. Such changes,whether in mature (a) or metaplastic (b) squamous cellsare common, particularly in perimenopausal women, andshould not be mistaken for atypical cells.
Fig. 1.26 Non-specific haloes. Small haloes around thenuclei of squamous cells are non-specific and do notrepresent HPV-related changes.
(a)
(b)
Fig. 1.27 Reactive endocervical cells. (a) A commonfinding, reactive endocervical cells are enlarged and haveprominent nucleoli. (b) Isolated cells can be as big asmature squamous cells and mimic an LSIL, but nucleoliare uncharacteristic of an LSIL.
S2638-01.qxd 12/11/02 11:44 Page 25

nuclei, prominent nucleoli, and occasional mitoses.Repair cells often maintain a uniform polarity that givesthe sheets the appearance of streaming (like a school offish) or being pulled out (like taffy) (Fig. 1.29). Becausethe sheets are very cohesive, individual abnormal cells –so characteristic of carcinomas – are generally absent inrepair reactions. Nevertheless, some repair reactions areso extensive, with unusual features such as crowdednuclei and a coarsely granular chromatin texture, thatdoubt about their benign nature is raised. Such a case isbest interpreted as ‘atypical squamous (or endocervical)cells, with features of atypical repair.’
CERVICAL AND VAGINAL CYTOLOGY26
Radiation
Radiation induces changes in cells that either disappearwith time or persist for many years.
Fig. 1.28 Reactiveendocervical cells(microglandularhyperplasia). These cells are enlarged and haveprominent cytoplasmicvacuoles.
Differential diagnosis of repair:
• SQC (see Fig. 1.48)
• endocervical adenocarcinoma (see Fig. 1.62)
Fig. 1.29 Typical repair. Typical reparative epithelium iscohesive and arranged in a monolayered, streaming sheet.
Cytomorphology:
• large, bizarre cells
• normal nuclear to cytoplasmic ratio
• cytoplasmic vacuolization
• features of repair
• multinucleation
The characteristic changes are marked cellular andnuclear enlargement with preservation of the nuclearto cytoplasmic ratio, cytoplasmic vacuolization, andpolychromasia (‘two-tone’ cytoplasm) (Fig. 1.30). Cellsare isolated or arranged in groups, and multinucleationis common. Some chemotherapeutic drugs inducesimilar changes.
S2638-01.qxd 12/11/02 11:44 Page 26

Cellular changes associated withintrauterine devices
IUD use can result in two patterns of benign endo-cervical and endometrial cell atypia.48
REACTIVE CHANGES 27
hyperchromatic, and coarsely granular, and nucleoliare usually visible. The second pattern consists ofisolated cells with enlarged hyperchromatic nuclei and avery high nuclear to cytoplasmic ratio; they resemblecells from an HSIL except that they have nucleoli.58
Sometimes reparative changes are also present and thebackground is inflamed. If the patient has an IUD, thesechanges should be regarded as benign.
Glandular cells status post-hysterectomy
Glandular cells resembling normal endocervical cellsare seen in approximately 2% of vaginal Paps fromwomen who have had a total hysterectomy.148 Thisfinding is more common in women who have hadpostoperative radiotherapy and may therefore representa therapy-induced metaplasia of squamous epithelium.The cells look entirely benign (Fig. 1.32), but they arepuzzling to the uninitiated, who may worry about thepossibility of an adenocarcinoma, particularly if thehysterectomy was carried out for an adenocarcinoma of the cervix or endometrium. A line in the reportnoting ‘glandular cells status post-hysterectomy’ isappropriate.
Given that many hysterectomies are supracervical,sometimes endocervical cells on a ‘vaginal’ Pap from awoman who has had a ‘hysterectomy’ are merely fromthe cervical stump.
Other benign changes
Often, cells of tubal metaplasia of the endocervix looklike normal endocervical cells, only with cilia, butsometimes they have a higher nuclear to cytoplasmic
Fig. 1.30 Radiation effect. Radiation looks like a wildreparative reaction, with very large cells, multinucleation,cytoplasmic vacuolization, and a curious ‘two-tone’cytoplasmic staining pattern.
Cytomorphology (Fig. 1.31):
• vacuolated cells
• small cells resembling HSIL
Fig. 1.31 IUD effect. The two types of cells are seenhere: a vacuolated cell and a small dark cell with scantcytoplasm. This combination is characteristic of IUD effect.
In the first pattern, which mimics adenocarcinoma,atypical glandular cells are arranged in small groups oras isolated cells with abundant vacuolated cytoplasm,including some signet ring cells. Nuclei are enlarged,
Fig. 1.32 Glandular cells status posthysterectomy. Thesquamous mucosa of the vagina has undergone mucinousmetaplasia.
S2638-01.qxd 12/11/02 11:44 Page 27

ratio and slight hyperchromasia, and may be mistakenfor a significant squamous or glandular lesion if a care-ful search is not made for cilia.116 In the great majorityof cases, cilia are reliable evidence that cells are benign,but rare ciliated adenocarcinomas of the endocervix doexist.167 Endometriosis of the cervix is a similar pitfall; itresembles abraded endometrium (see above).
VAGINAL SPECIMENS IN ‘DESDAUGHTERS’
The daughters of women who were given diethylstil-bestrol (DES) during pregnancy to prevent a threatenedabortion are at risk for a variety of abnormalities, mostof them benign, of the vagina, cervix, and uterus.About one-third of these ‘DES daughters’ developvaginal adenosis, the presence of glands in the vagina.Mucinous epithelium is the most frequently encoun-tered type of glandular epithelium, but tubal andendometrial-type epithelium is sometimes seen. Adiagnosis of vaginal adenosis is supported by thepresence of glandular or squamous metaplastic cells ona direct sample from the wall of the vagina.
Clear cell carcinoma of the vagina is the least com-mon, but most dreaded, complication of in-utero DESexposure (see ‘Endocervical adenocarcinoma’, below).
SQUAMOUS ABNORMALITIES
Squamous intraepithelial lesions
The term ‘squamous intraepithelial lesion’ (SIL) en-compasses the spectrum of precursors to invasive SQC,previously called ‘dysplasia,’ ‘carcinoma in situ,’‘borderline lesion,’ and ‘CIN’. Strong evidence links SILwith invasive squamous cancer. Epidemiologic riskfactors, such as sexual history, are similar for patientswith SIL and those with invasive cancer and both are
CERVICAL AND VAGINAL CYTOLOGY28
associated with HPV. Both SIL and cancer have similarchromosomal abnormalities as measured by cytogeneticor image-analysis methods. Women with SIL are at least10 years younger on average than those with invasivecancer; this chronology suggests progression of SIL toinvasion. Finally, SIL resembles cancer morphologicallyand is often present in histologic sections directlyadjacent to invasive cancer.
The natural history of SIL is not easy to study. Ethicalconsiderations prohibit using a control group, especiallywomen with high-grade lesions.28 Many studies havechosen a high-grade lesion as their endpoint forinvestigating the behavior of low-grade lesions, becauseallowing a lesion to progress to invasive cancer is out ofthe question. Yet, it is precisely the risk of progression toinvasion that is of paramount interest. A biopsy itselfinterferes with the natural history of a lesion byremoving it entirely or by causing a surroundinginflammatory reaction that can destroy it.79 Follow-upbiopsies or smears may not be representative of theunderlying lesion, and follow-up time may be inade-quate. Finally, the criteria for diagnosing and gradingSIL and entering patients into a study differ amongobservers.76 A meta-analysis of this large and incon-sistent body of data suggests that over 50% of cases ofLSIL regress and only about 1% progress to invasivecancer.117 Fewer high-grade lesions regress, and manymore progress to invasive cancer (Table 1.4).
The sexually transmitted HPV explains the well-known epidemiologic association between sexual his-tory and increased risk of cervical cancer.76 Althoughdetected in virtually all cervical cancers by currentmolecular techniques,156 HPV was originally identifiedin association with a distinctive altered squamous cellknown as a koilocyte. This unusual cell was firstdescribed in 1949 by Ayre, who called it ‘precancer cellcomplex,’ speculating that it was a precursor tocancer.12 In 1960 he correctly suggested a viral etiology.They were recognized by Papanicolaou, who illustratedthem with ‘dyskaryotic’ cells in his Atlas of Exfoliative
Table 1.4 The Natural History of Squamous Intraepithelial Lesions
Regress (%) Persist (%) Progress to CIN 3 (%) Progress to invasive cancer (%)
LSIL (CIN 1) 57 32 11 1HSIL (CIN 2) 43 35 22 5HSIL (CIN 3) 32 <56 — >12
From Östör, 1993117
CIN, cervical intraepithelial neoplasia; SIL, squamous intraepithelial lesion; LSIL, low-grade SIL; HSIL, high-grade SILWith permission from Lippincott Williams & Wilkins.
S2638-01.qxd 12/11/02 11:44 Page 28

Cytology.122 The term ‘koilocytosis’ was coined by Kossand Durfee in 1956 after the Greek koilos (‘hollow’),because of the prominent, sharply defined cytoplasmiccavities of the cells.78 Two decades later, two groups ofinvestigators working independently made the con-nection between koilocytes and HPV.102,127 Subsequentultrastructural,61 immunocytochemical, and in-situhybridization103 studies confirmed the presence of viruswithin koilocytes (Fig. 1.33). When it was first realizedthat these changes were due to a virus, an attempt wasmade to separate them from dysplasia and CIN.102
Ultimately, it became apparent that a morphologic dis-tinction was not possible,23 and evidence began to accu-mulate linking HPV to the pathogenesis of squamouscancer.42,97,99 Currently there is little doubt that HPVplays a central role in causing cervical cancer, makingHPV a ‘sexually transmitted disease with potentially life-threatening consequences’.76 HPV has a number ofeffects on cells that lead to malignant transformation.1
SQUAMOUS ABNORMALITIES 29
stimulating cell division. The viral oncoproteins alsomediate disruption of centrosome duplication, leadingto genomic instability. Finally, E6 mediates theupregulation of telomerase.
More than 80 types of HPV have been isolated, ofwhich more than 40 are known to infect the femalegenital tract. These are divided into low- and high-risktypes based on the frequency of their association withinvasive cancer. By definition, an HPV is low risk if it hasnever been isolated from a carcinoma, and high risk if itever has been.
Fig. 1.33 Detection of human papillomavirus by in-situhybridization. The dark brown signal is centered aroundthe nucleus of infected cells. (Courtesy of Miu-Fun Chau,DakoCytomation, Carpinteria, CA, USA.)
HPV effects on cells leading tomalignant transformation:
• direct effects on the cell cycle
• effects on centrosome duplication
• upregulation of telomerase
The genes of HPV are classified as ‘early’ (E) or ‘late’ (L)depending on the timing of expression, and it is the E6and E7 gene products that play the most significant partin oncogenesis. The binding of E6 to p53 and E7 to theretinoblastoma gene product has a direct effect on
Some examples of low- and high-riskHPVs:
• low-risk HPVs: 6, 11, 42, 43, 44, 53, 54, 57, 66
• high-risk: 16, 18, 31, 33, 35, 39, 45, 51, 52, 56,58, 59, 68.
HPV 16 is the prototype of the high-risk viruses and theone most commonly detected in cervical cancers.
A variety of molecular techniques – the Southernblot, the polymerase chain reaction, in-situ hybridiza-tion (see Fig. 1.33), and hybrid capture – can be used todetect specific HPV types within cervical lesions. TheHybrid Capture 2™ test, which was evaluated in themulticenter ASCUS/LSIL Triage Study (ALTS) trialsponsored by the National Cancer Institute, uses probesfor the 13 high-risk HPV types listed above, whichaccount for nearly 90% of HPVs detected in HSIL andinvasive cancers.141
Grading squamous intraepithelial lesionsThe Bethesda System recommends a low-grade/high-grade approach to grading SIL. This reflects a paradigmshift away from the CIN concept, based on the sub-stantial evidence that most LSILs are transient infec-tions that carry little risk for oncogenesis, whereas mostHSILs are associated with viral persistence, with asignificant potential for progression to invasive cancer.LSIL encompasses lesions previously described separ-ately as koilocytosis (flat condyloma) and mild dysplasia(CIN 1). This distinction is not reproducible91,138 andboth lesions contain a heterogeneous distribution oflow-risk and high-risk HPV types. HSIL encompasseslesions previously described as moderate dysplasia (CIN2) and as severe dysplasia/carcinoma in situ (CIN 3). Inthe United States, management of these lesions is basedprincipally on their size and location rather than on thedistinction between CIN 2 and 3.
S2638-01.qxd 12/11/02 11:44 Page 29

HPV typing plays no role in the grading of SIL.Although low-risk viruses are more common in LSILthan HSIL, high-risk viruses predominate in both.8,141
Morphologic assessment by conventional light micro-scopy is still the gold standard for grading SILs.
Low-grade squamous intraepithelial lesionsLSIL is a low-risk intraepithelial lesion caused by a largenumber of different HPVs, including low-risk and high-risk types. The majority of LSILs regress spontane-ously76,117 (see Table 1.4), but some persist for longperiods of time. Approximately 11% progress to HSIL; itis possible that at least some of these may have beenHSILs throughout, but were misclassified as LSILs. Infact, 18% of women with an LSIL Pap result prove tohave HSIL on biopsy.69 Only very few, perhaps 1% ofuntreated LSILs, progress to invasive cancer.117
CERVICAL AND VAGINAL CYTOLOGY30
Colposcopy with directed biopsies of all suspiciouslesions is recommended for women with an LSIL Papresult164 (Fig. 1.36a). HPV testing to triage women withLSIL Paps is not recommended because the high rate ofpositivity (83%) limits its usefulness.8 The routine use ofdiagnostic excisional procedures such as loop electro-surgical excision procedure or ablative procedures isunacceptable in the absence of a biopsy-proven SIL. Ifcolposcopy is satisfactory and no lesion is seen, or ifcolposcopy is unsatisfactory, endocervical sampling isrecommended if the patient is not pregnant. The recom-mended management of women with LSIL in specialcircumstances is illustrated in Fig. 1.36b,c.
Cytomorphology:
• intermediate-sized cells
• nuclear atypia:– enlargement– irregular contour– hyperchromasia– slight chromatin coarseness
• cytoplasmic cavities (‘koilocytes’)
• keratinizing variant
LSIL is a lesion of intermediate or superficial cells,which show nuclear enlargement accompanied bymoderate variation in nuclear size and slight irregu-larities in nuclear shape and contour. Hyperchromasiais present and can take the form of either a uniformlygranular increase in chromatin or the smudgyhyperchromasia seen in some koilocytes. Nucleoli areinconspicuous. Classic koilocytes have large, sharplydefined perinuclear cytoplasmic cavities surrounded bydense rims of cytoplasm. Their nuclei are usuallyenlarged and atypical, but not always, and they arediagnostic of LSIL even in the absence of nuclearenlargement (Fig. 1.34). Some LSILs show prominentkeratinization manifested by deeply orangeophiliccytoplasm and squamous pearls (Fig. 1.35).
Differential diagnosis:
• reactive squamous cells (see Fig. 1.25a)
• cells with non-specific haloes (see Fig. 1.26)
• reactive endocervical cells (see Fig. 1.27b)
• ASC-US (Figs 1.49, 1.51)
(a)
(b)
Fig. 1.34 Low-grade squamous intraepithelial lesions.(a) LSIL. Classic koilocytes, as seen here, have a largecytoplasmic cavity with a sharply defined inner edge andare frequently binucleated. Nuclear enlargement may notbe as marked as in the nonkoilocytic LSILs. (b) ‘Non-koilocytic’ LSIL. Nuclei are significantly enlarged and showmild hyperchromasia and nuclear contour irregularity. Nodefinite koilocytes are seen. This pattern was once calledmild dysplasia or CIN 1.
S2638-01.qxd 12/11/02 11:44 Page 30

High-grade squamous intraepithelial lesionsHSIL is an intraepithelial lesion that carries a significantrisk for progression to cervical cancer117 (see Table 1.4);97% of women with an HSIL Pap result test positive forhigh-risk HPV.141
SQUAMOUS ABNORMALITIES 31
HSIL is usually a lesion of smaller, less mature squam-ous cells. Nuclear enlargement is generally in the samerange as in LSILs, but the nuclear to cytoplasmic ratio ishigher because the cells are smaller (Fig. 1.37). In gene-ral, hyperchromasia, irregular chromatin distribution,and membrane contour irregularity are all more severethan in LSIL. Architecturally, the cells of HSILs arearranged in two main patterns: as distinct individual cells(Fig. 1.37), or as cohesive groups of cells with indistinctcell borders (syncytial-like groupings) (Fig. 1.38). Theyare often completely undifferentiated in appearance andlack all defining squamous features. In fact, cytoplasmic
Cytomorphology:
• usually parabasal-sized cells
• discrete cells or syncytial groups (‘hyperchromaticcrowded groups’)
• nuclear atypia– enlargement– marked irregularity in contour– usually marked hyperchromasia– marked chromatin coarseness
• keratinizing variant
Fig. 1.35 Low-grade squamous intraepithelial lesion,keratinizing type. A squamous pearl is being formed.
≥ ASC or HPV (+)
Repeat colposcopy
Negative
Routine screening
Satisfactory colposcopy and lesion identified – endocervical sampling acceptableSatisfactory colposcopy and NO lesion identified – endocervical sampling preferred
Unatisfactory colposcopy examination – endocervical sampling preferred
Cytology at 6 & 12 months ORHPV DNA testing at 12 months
No CIN/Cancer
Manage per ASCCP Guideline
Colposcopic examination
LSIL
CIN/Cancer
(a)
Fig. 1.36 Management guidelines for women with a low-grade squamous intraepitheliallesion Pap. (a) The options outlined here may be varied if the woman is postmenopausal,pregnant, or an adolescent.
Illustration continued on following page
S2638-01.qxd 12/11/02 11:44 Page 31

pallor and vacuoles (Fig. 1.39) and an elongated confi-guration (Fig. 1.40) can cause them to be mistaken forcells of glandular origin. Although usually a lesion ofsmall, immature squamous cells, mature keratinizingcells with marked nuclear atypia are classified as HSIL(Fig. 1.41).
CERVICAL AND VAGINAL CYTOLOGY32
Negative
Routine screening
Repeat cytology at 4–6 months
4–6 months afterindex Pap
(acceptableoption)
HPV DNA testing12 months after index Pap
Intravaginalestrogen therapy
If clinical or cytologic evidence ofatrophy and no contraindications
to estrogen therapy
Repeat cytologyat 12 months
Negative
1 week aftercompletionof therapy
≥ ASC
≥ ASC HPV positive(for high-risk types)
HPV negative(for high-risk types)
Repeat cytology
Colposcopy
LSIL - post menopausal women
Repeat cytology6 months after index Pap
Negative
Routine screening
Repeat cytology 6 months later
HPV DNA testing12 months after index Pap
Repeat cytologyat 12 months
Negative
≥ ASC
≥ ASC HPV positive(for high-risk types)
HPV negative(for high-risk types)
Colposcopic triage
LSIL – adolescents
Colposcopy
Per algorithm for LSIL
(b)
(c)
Fig. 1.36 Continued Management guidelines for women with a low-grade squamous intraepithelial lesion Pap.(b) Guidelines for low-risk postmenopausal women with an LSIL Pap and a history of negative screening. (c) Guidelinesfor adolescents with an LSIL Pap. (Reprinted with the permission of ASCCP © American Society for Colposcopy andCervical Pathology 2002.)
Differential diagnosis:
• atrophy (see Fig. 1.6a) and transitionalmetaplasia (see Fig. 1.6b)
• exfoliated endometrial cells (see Fig. 1.12)
• abraded LUS/endometrial stroma (see Fig. 1.14b)and glands (see Fig 1.14c, Fig. 1.42)
• follicular cervicitis (see Fig. 1.16)
• IUD effect (see Fig. 1.31)
• ASC-H (see Fig. 1.55)
• ASC-US associated with atrophy (see Fig.1.50b–d)
• AIS (see Fig. 1.57)
S2638-01.qxd 12/11/02 11:44 Page 32

The management of women with an HSIL Pap is illus-trated in Fig. 1.43. Colposcopy with directed biopsies ofall suspicious lesions and ‘endocervical assessment’(evaluating the canal using the colposcope or tissuesampling) are recommended. If no lesion or only LSIL(CIN I) is confirmed by biopsy, a review of the cytologic,histologic, and colposcopic findings is recommended. If the original interpretations are upheld, then adiagnostic excisional procedure is recommended in non-pregnant patients. A repeat colposcopy with endo-cervical assessment is acceptable in young women ofreproductive age.
In pregnant women with an HSIL Pap, it is recom-mended that colposcopy with directed biopsies is
SQUAMOUS ABNORMALITIES 33
performed by a clinician experienced with this tech-nique in pregnant patients. Endocervical curettage isunacceptable. If there is no colposcopic or histologicevidence of invasive cancer, women should undergo arepeat colposcopy and cytologic examination, but nomore biopsies unless the lesion worsens or the cytologysuggests invasive cancer. Treatment of HSIL in pregnantwomen is unacceptable unless invasive cancer isidentified. If invasive cancer is identified, a diagnosticexcisional procedure is recommended.164
(a)
(b)
Fig. 1.37 High-grade squamous intraepithelial lesion.(a) These squamous cells have scant cytoplasm andmarkedly hyperchromatic nuclei with highly irregularnuclear contours. (b) Cells with a moderate amount ofcytoplasm, formerly called ‘moderate dysplasia’ or ‘CIN 2’,are incorporated in the HSIL category.
Fig. 1.38 High-grade squamous intraepithelial lesion.The cells of an HSIL are often arranged in three-dimensional groups in which individual cell borders areindistinct (syncytial-like).
Fig. 1.39 High-grade squamous intraepithelial lesion.Some HSILs are comprised of very small, dispersed, highlyatypical cells. The nuclei of these small cells are not muchlarger than those of normal intermediate cells, but arenevertheless identified as abnormal because ofhyperchromasia or markedly irregular nuclear outlines, orboth. Sometimes they have cytoplasmic vacuoles. Thesedo not indicate a glandular lesion.
S2638-01.qxd 12/11/02 11:44 Page 33

Problems in the diagnosis of squamousintraepithelial lesionsOverdiagnosing LSIL Care must be taken not tooverinterpret non-specific changes such as indistinct orsmall halos or binucleation seen in reactive conditions(see Fig. 1.26). In particular, Paps from perimenopausalwomen (aged 40–55 years) often contain cells withenlarged but otherwise bland nuclei that are entirelybenign.96 Without hyperchromasia or nuclear mem-brane irregularity, such cells are best called negative
CERVICAL AND VAGINAL CYTOLOGY34
(see Fig. 1.25). Cellular changes that include somehyperchromasia and/or nuclear membrane irregularityare suggestive of LSIL and should be categorized as ASC-US.
Distinguishing LSIL from HSIL If a specimen iscomposed of both LSIL and HSIL, it should be reportedas an HSIL even if the HSIL cells are less numerous thanthe LSIL cells. In a small percentage of cases, morpho-logic features intermediate between typical LSIL and
Fig. 1.40 High-grade squamous intraepithelial lesion.The cells of some HSILs have an elongated configurationthat makes them look columnar. In the absence of strips,rosettes, or feathering, this should not be taken forevidence of glandular differentiation (i.e. an AIS).
Fig. 1.41 High-grade squamous intraepithelial lesion,keratinizing type. Although the cells show differentiationby keratinizing, they are classified as HSIL if the nuclei aresufficiently abnormal.
Fig. 1.42 Lower uterinesegment. The crowded cellsof LUS are good mimics of HSIL (compare with Fig. 1.40). The nuclei areless hyperchromatic, and astromal component (notshown) was presentelsewhere on the slide; these point to the correctdiagnosis.
S2638-01.qxd 12/11/02 11:44 Page 34

HSIL make grading difficult.100 Although there aregenerally fewer abnormal cells in an an LSIL than in an HSIL, the quantity of cells is an unreliablediscriminator.
SQUAMOUS ABNORMALITIES 35
carcinoma are by no means perfect. Not infrequently, aclassic case of HSIL on cytology will turn out to beinvasive squamous cancer on biopsy. Conversely, thepossibility of invasive cancer is often raised in cases ofHSIL in which the cells have marked nuclear abnor-malities associated with abundant, heavily keratinizedcytoplasm and unusual cell shapes, but the lesion turnsout to be only a keratinizing HSIL on biopsy. A clinicianmust understand that no diagnosis of HSIL on cytologicmaterial excludes the possibility of invasive cancer, andthat colposcopy and biopsy are necessary for confirma-tion. Some HSILs with features worrisome for invasivecancer can be reported as ‘HSIL, with featuressuggestive of invasive cancer’.
Squamous cell carcinoma
SQC is the most common malignant tumor of the cervix.Although most patients are between the ages of 45 and55 years, invasive tumors occur in younger patients,including those under 30 years of age.17 Histologicallyand cytologically, SQCs range from well-differentiated,keratinizing tumors to poorly differentiated, non-keratinizing tumors. Some cannot be distinguished fromHSIL cytologically, particularly the smaller, less deeply
No CIN or onlyCIN 1 on biopsy
Biopsy-confirmedCIN 2,3
Review of material*
No change
Diagnosticexcisionalprocedure
Change indiagnosis
Manage perASCCP Guideline
for changed diagnosis
Satisfactory colposcopy
Colposcopic examination (with endocervical assessment)
Manage perASCCP Guideline
No lesionidentified
Biopsy-confirmedCIN (of any grade)
Review of material*
No change(or review not possible, or
only biopsy-confirmed CIN 1)
Diagnosticexcisionalprocedure
Change indiagnosis
Manage perASCCP Guideline
for changed diagnosis
Unsatisfactory colposcopy
Manage perASCCP Guideline
'See and treat'acceptable if
lesion identified
HSIL
Fig. 1.43 Management guidelines for women with a high-grade squamous intraepithelial lesion Pap. Colposcopy, withbiopsies and endocervical assessment, is recommended for all women with an HSIL Pap. The management options mayvary if the woman is pregnant, postmenopausal, or adolescent. *Includes referral cytology, colposcopic findings, and allbiopsies. (Reprinted with the permission of ASCCP © American Society for Colposcopy and Cervical Pathology 2002.)
Cytomorphologic patterns of ‘SIL, cannotdetermine grade’:
• very few dysplastic cells
• LSIL, with a small number of equivocal HSIL cells
• extensively keratinized SILs, without definite HSIL
Grading is difficult in some cases where the dysplasticcells are few in number, or when an LSIL is accompaniedby a small number of cells suggestive of but not con-clusive for HSIL. Extensively keratinized SILs without de-finite HSIL are especially difficult to grade44 (Fig. 1.44).In all such cases a diagnosis of ‘SIL; cannot determinegrade’ is appropriate. In a College of AmericanPathologists survey, this diagnosis accounted for 3.4%of all cytologic diagnoses of SIL.69
Distinguishing HSIL from invasive carcinomaThe criteria used to distinguish HSIL from invasive
S2638-01.qxd 12/11/02 11:44 Page 35

invasive tumors.133 Others can be confidently diagnosedas invasive cancers, however.
CERVICAL AND VAGINAL CYTOLOGY36
The classic pattern of SQC shows abundant necroticdebris: a granular, amorphous precipitate with nucleardebris and red blood cells called ‘tumor diathesis’ (Fig. 1.45). It is not specific for invasive cancers; a simi-lar pattern is seen in some atrophic smears and evenduring heavy menstrual bleeding. When associatedwith hyperchromatic crowded groups of atypical cells orabundant atypical keratinized cells with unusual shapes(‘tadpoles’, ‘fiber cells’), the pattern is diagnostic.
The cells of non-keratinizing SQC look like trans-formed HSIL cells (Fig. 1.46). They are hyperchromatic
(a) (b)Fig. 1.44 Squamous intraepithelial lesion, cannot determine grade. When a lesion is extensively keratinized and there isno definite HSIL, it is difficult to grade. Colposcopically directed biopsies showed subsequently that the case illustrated in(a) was low grade and that in (b) was high grade.
Cytomorphology:
• HSIL features, plus– macronucleoli– irregular chromatin distribution– tumor diathesis
• ‘tadpoles’ and ‘fiber cells’ (keratinizing type)
Fig. 1.45 Squamous cellcarcinoma. Slides fromdeeply invasive tumors showabundant tumor diathesis,which is a granularprecipitate of lysed bloodand cell fragments. In suchcases, the malignant cellscan be hard to identify. Inother cases, the tumordiathesis is focal, and, ifmissed, the case ismisclassified as HSIL.
S2638-01.qxd 12/11/02 11:44 Page 36
Related Documents








