LIVER FAILURE/CIRRHOSIS/PORTAL HYPERTENSION Circulating Neutrophil Dysfunction in Acute Liver Failure Nicholas J. Taylor, 1,2 Anirudh Nishtala, 2 Godhev K. Manakkat Vijay, 2 R. Daniel Abeles, 1,2 Georg Auzinger, 1 William Bernal, 1,2 Yun Ma, 2 Julia A. Wendon, 1,2 * and Debbie L. Shawcross 1,2 * Systemic inflammation and susceptibility to developing sepsis is common in acute liver failure (ALF) resulting in tissue damage and organ failure. This study characterized the function of circulating neutrophils in 25 patients with ALF and subacute liver failure (SALF). ALF (n 5 15) / SALF (n 5 10) patients were prospectively studied and compared with 11 healthy (HC) and 6 septic controls (SC). Neutrophils were isolated on admission to intensive care and every 3-4 days until death / liver transplantation / recovery. Neutro- phil phenotype was determined using fluorochrome-labeled antibodies to CD16 and CD11b and assessed by flow cytometry. Neutrophil phagocytic activity (NPA) was deter- mined using fluorescein isothiocyanate-labeled opsonized Escherichia coli and oxidative burst (OB) was determined by the percentage of neutrophils producing reactive oxygen species (ROS) at rest and after stimulation with opsonized E. coli. Physiological variables, biochemistry, arterial ammonia, microbiology, and outcomes were collected. Plasma pro- and antiinflammatory cytokine profiles were performed by enzyme-linked immunosorbent assay. Neutrophil expression of CD16 which recognizes the FccRIII region of immuno- globulin G was significantly reduced in the ALF cohort (P < 0.001) on day 1 compared to HC. NPA was significantly impaired in the SALF cohort compared to HC (P < 0.01). Impaired NPA in the ALF and SALF cohorts on admission predicted nonsurvival without liver transplantation (P 5 0.01). Spontaneous neutrophil production of ROS was not sig- nificantly increased in any of the cohorts. E. coli-stimulated OB was preserved in ALF/ SALF cohorts but was significantly impaired in the SC group (P < 0.05). Conclusion: Cir- culating neutrophils in ALF/SALF have impaired bacteriocidal function similar to that seen in severe sepsis. Neutrophil function indices are important biomarkers in ALF and may be implicated in the development of organ dysfunction and the increased susceptibil- ity to developing sepsis. (HEPATOLOGY 2013;57:1142-1152) A cute liver failure (ALF) is a rare but frequently catastrophic consequence of an acute primary hepatic injury arising from a wide variety of insults. It is characterized by coagulopathy and encephalopathy, with a variable dynamic of progres- sion to multiple organ dysfunction syndrome (MODS) and death. 1 Liver transplantation (LT) remains the only curative option for advanced ALF with poor prognostic criteria and contributes to 10% of LT in the Western world. 2 Neutrophils are a major innate immune cell subset involved in the first line of defense against infection. Neutrophils are produced in vast numbers in the bone marrow (1-2 10 11 per day) and have a short half- life of 12-18 hours. They are rapidly recruited to sites of infection and inflammation. Neutrophils Abbreviations: AALF, acetaminophen-induced liver failure; ALF, acute liver failure; APACHE, acute physiology and chronic health evaluation; CARS, compensatory antiinflammatory response syndrome; fMLP, formyl-Met-Leu-Phe; ICU, intensive care unit; IQR, interquartile range; LT, liver transplantation; MAP, mean arterial blood pressure; MELD, model for endstage liver disease; MFI, mean fluorescence intensity; NPA, neutrophil phagocytic activity; OB, oxidative burst; PMA, phorbol 12-myristate 13-acetate; ROS, reactive oxygen species; SALF, subacute liver failure; SIRS, systemic inflammatory response syndrome; SOFA, sequential organ failure assessment. From the 1 Liver Intensive Care Unit and 2 Institute of Liver Studies and Transplantation, King’s College London School of Medicine at King’s College Hospital, London, UK. Received May 22, 2012; accepted October 3, 2012. Supported by a Young Investigator Grant awarded to Dr. D.L Shawcross and Professor J.A Wendon from the Intensive Care Society in 2008. Additional laboratory consumables were also funded from the Institute of Liver Studies Liver Intensive Care Charitable Fund. Dr. D.L. Shawcross is funded by a 5-year Department of Health HEFCE Clinical Senior Lectureship and Dr. R.D. Abeles holds a Department of Health NIHR Clinical Research PhD Fellowship. *Joint senior authors 1142

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

LIVER FAILURE/CIRRHOSIS/PORTAL HYPERTENSION
Circulating Neutrophil Dysfunction in Acute Liver FailureNicholas J. Taylor,1,2 Anirudh Nishtala,2 Godhev K. Manakkat Vijay,2 R. Daniel Abeles,1,2 Georg Auzinger,1
William Bernal,1,2 Yun Ma,2 Julia A. Wendon,1,2* and Debbie L. Shawcross1,2*
Systemic inflammation and susceptibility to developing sepsis is common in acute liverfailure (ALF) resulting in tissue damage and organ failure. This study characterized thefunction of circulating neutrophils in 25 patients with ALF and subacute liver failure(SALF). ALF (n 5 15) / SALF (n 5 10) patients were prospectively studied and comparedwith 11 healthy (HC) and 6 septic controls (SC). Neutrophils were isolated on admissionto intensive care and every 3-4 days until death / liver transplantation / recovery. Neutro-phil phenotype was determined using fluorochrome-labeled antibodies to CD16 andCD11b and assessed by flow cytometry. Neutrophil phagocytic activity (NPA) was deter-mined using fluorescein isothiocyanate-labeled opsonized Escherichia coli and oxidativeburst (OB) was determined by the percentage of neutrophils producing reactive oxygenspecies (ROS) at rest and after stimulation with opsonized E. coli. Physiological variables,biochemistry, arterial ammonia, microbiology, and outcomes were collected. Plasma pro-and antiinflammatory cytokine profiles were performed by enzyme-linked immunosorbentassay. Neutrophil expression of CD16 which recognizes the FccRIII region of immuno-globulin G was significantly reduced in the ALF cohort (P < 0.001) on day 1 compared toHC. NPA was significantly impaired in the SALF cohort compared to HC (P < 0.01).Impaired NPA in the ALF and SALF cohorts on admission predicted nonsurvival withoutliver transplantation (P 5 0.01). Spontaneous neutrophil production of ROS was not sig-nificantly increased in any of the cohorts. E. coli-stimulated OB was preserved in ALF/SALF cohorts but was significantly impaired in the SC group (P < 0.05). Conclusion: Cir-culating neutrophils in ALF/SALF have impaired bacteriocidal function similar to thatseen in severe sepsis. Neutrophil function indices are important biomarkers in ALF andmay be implicated in the development of organ dysfunction and the increased susceptibil-ity to developing sepsis. (HEPATOLOGY 2013;57:1142-1152)
Acute liver failure (ALF) is a rare but frequentlycatastrophic consequence of an acute primaryhepatic injury arising from a wide variety of
insults. It is characterized by coagulopathy andencephalopathy, with a variable dynamic of progres-sion to multiple organ dysfunction syndrome(MODS) and death.1 Liver transplantation (LT)remains the only curative option for advanced ALF
with poor prognostic criteria and contributes to�10% of LT in the Western world.2
Neutrophils are a major innate immune cell subsetinvolved in the first line of defense against infection.Neutrophils are produced in vast numbers in the bonemarrow (1-2 � 1011 per day) and have a short half-life of 12-18 hours. They are rapidly recruited to sitesof infection and inflammation. Neutrophils
Abbreviations: AALF, acetaminophen-induced liver failure; ALF, acute liver failure; APACHE, acute physiology and chronic health evaluation; CARS,compensatory antiinflammatory response syndrome; fMLP, formyl-Met-Leu-Phe; ICU, intensive care unit; IQR, interquartile range; LT, liver transplantation; MAP,mean arterial blood pressure; MELD, model for endstage liver disease; MFI, mean fluorescence intensity; NPA, neutrophil phagocytic activity; OB, oxidative burst;PMA, phorbol 12-myristate 13-acetate; ROS, reactive oxygen species; SALF, subacute liver failure; SIRS, systemic inflammatory response syndrome; SOFA,sequential organ failure assessment.From the 1Liver Intensive Care Unit and 2Institute of Liver Studies and Transplantation, King’s College London School of Medicine at King’s College Hospital,
London, UK.Received May 22, 2012; accepted October 3, 2012.Supported by a Young Investigator Grant awarded to Dr. D.L Shawcross and Professor J.A Wendon from the Intensive Care Society in 2008. Additional
laboratory consumables were also funded from the Institute of Liver Studies Liver Intensive Care Charitable Fund. Dr. D.L. Shawcross is funded by a 5-yearDepartment of Health HEFCE Clinical Senior Lectureship and Dr. R.D. Abeles holds a Department of Health NIHR Clinical Research PhD Fellowship.*Joint senior authors
1142

phagocytose invading microbes3 and proceed to killthem by generating superoxide anions and hydrogenperoxide along with other reactive oxygen species(ROS) through activation of nicotinamide adenine di-nucleotide phosphate (NADPH)-oxidase, a processtermed respiratory or oxidative burst (OB).4 The OBproducts are effective in eradicating invading microor-ganisms, but unfortunately may damage ‘‘innocentbystanders,’’ leading to tissue destruction, inflamma-tion, and organ failure. Neutrophils possess receptorsfor the Fc region of immunoglobulin G (FccRIII/CD16 and FccRII/CD32) and for complement mole-cules such as iC3b (MAC-1/CD11b-CD18), whichbind to the surface of the microbe (opsonization).Complement-opsonized particles are gently internal-ized within the neutrophil with Fcc receptor ligationaugmenting the process through the extension of pseu-dopods which surround and engulf the microbe.3
Neutrophils are rapidly recruited to the liver inresponse to hepatic injury in ALF,5 and once therethey become activated by cytokines (e.g., interleukin[IL]-8 and tumor necrosis factor alpha [TNF-a]), andmay contribute to further tissue damage by release ofproteolytic enzymes and ROS.6 An exaggerated sys-temic inflammatory response (SIRS) is frequently pres-ent in ALF and increasingly it is being recognized toplay a key role in the pathogenesis and outcome.7 Sys-temic neutrophil activation with associated immuneparesis is well recognized in severe sepsis, a conditionthat shares many phenotypic features with ALF includ-ing microvascular dysfunction, hemodynamic instabil-ity, coagulopathy, encephalopathy, and high levels ofboth proinflammatory and antiinflammatory cyto-kines.8 In severe sepsis excessive activation of neutro-phils has been implicated in the pathogenesis of acutelung and kidney injury.9 Neutrophils might thereforeserve as critical effector cells of the progressive paren-chymal liver damage and MODS in ALF.There is a high incidence of bacterial and fungal
infection early in the course of ALF (10) which maypreclude listing for LT. ALF is also associated with anacute and often precipitous increase in plasma ammo-nia levels.2 A recent study has shown that neutrophilsexposed to ammonia have reduced phagocytic activityof opsonized E. coli and high spontaneous productionof ROS, suggesting a direct toxic effect of ammonia
on neutrophils.11 Neutrophil dysfunction has also beenpreviously reported in ALF with reduced complementexpression,12 impaired neutrophil adhesion,13
decreased production of ROS,14 and decreased neutro-phil phagocytosis and intracellular killing.We postulate that circulating neutrophil dysfunction
is present in ALF and may add value as a prognosticmarker of severity and outcome. The aim of this pro-spective case-control longitudinal study was thereforeto characterize circulating neutrophil phenotype, phag-ocytic activity (NPA) and production of ROS in neu-trophils isolated from the peripheral blood of patientswith ALF and comparing it to healthy (HC) and septiccontrols (SC). Indices of neutrophil phenotype andfunction were examined with respect to severity andnature of liver injury, severity of organ failure, liverprognostic criteria of survival, and eventual outcome.The relationship between plasma-derived factors andneutrophil function was also examined in order to aididentification of other associated biomarkers in ALF.
Patients and Methods
Study Design. A cross-sectional case-control cohortstudy was performed. Patients with ALF (n ¼ 15) andsubacute liver failure (SALF) (n ¼ 10) were prospec-tively studied. Neutrophil phenotype, NPA, and OB(spontaneous and stimulated with opsonized E. coli)were determined and compared to n ¼ 11 HC and n ¼6 SC. The dynamics of neutrophil function during thecourse of the illness were compared between patientgroups and in relation to those who survived comparedto those who did not survive. Patients who were trans-planted were considered nonsurvivors. Baseline sam-pling was performed within 24 hours of admission to anintensive care (ICU) and every 3-4 days until spontane-ous recovery, death, or LT. In those who underwent LTfurther sampling was performed 72 hours post-LT. Sub-jects were followed up for 90 days.Patients. Twenty-five patients with ALF or SALF
were recruited nonconsecutively on admission to theliver ICU at King’s College Hospital between October2008 and August 2010. ALF was defined by the onsetof hepatocellular dysfunction in the absence of preex-isting liver disease characterized by coagulopathy and
Address reprint requests to: Dr. Debbie L. Shawcross, Institute of Liver Studies and Transplantation, King’s College London School of Medicine at King’s CollegeHospital, Denmark Hill, London, SE5 9RS, UK. E-mail: [email protected]; fax: þ44 020 3299 3167.CopyrightVC 2012 by the American Association for the Study of Liver Diseases.View this article online at wileyonlinelibrary.com.DOI 10.1002/hep.26102Potential conflict of interest: Nothing to report.Additional Supporting Information may be found in the online version of this article.
HEPATOLOGY, Vol. 57, No. 3, 2013 TAYLOR ET AL. 1143
encephalopathy and an illness of less than 26 weeksduration. ALF was further subclassified according tothe criteria defined by O’Grady et al.15 depending onthe time between the onset of jaundice and encephal-opathy. (1) Hyperacute (jaundice to encephalopathytime <7 days) consisting predominantly of patientswith acetaminophen-induced liver failure (AALF). (2)Acute liver failure (jaundice to encephalopathy time8-28 days) typified by patients presenting with fulmi-nant viral hepatitis. (3) SALF (jaundice to encephalop-athy time 5-12 weeks) typified by those presentingwith nonacetaminophen drug-induced liver injury andseronegative/acute autoimmune hepatitis.Inclusion Criteria. Patients with ALF/SALF were
included if they were age >18 years and <80 years.Healthy age- and sex-matched nonsmoking volunteerswith no history of liver disease were used as HC. TheHC alcohol intake was <20 g/day and volunteers hadnot drunk alcohol or exercised excessively in the 24hours prior to blood being drawn. SC patients wererecruited from the general ICU and had severe sepsiswith MODS. Severe sepsis was defined by the presenceof an SIRS score �2,16 with radiological and/or labo-ratory evidence of infection and one or more extrahe-patic organ failure(s). Patients presenting with ALF/SALF were given empirical intravenous antibiotic andantifungal cover as standard of care. This consisted oftazocin 4.5 g every 8 hours (substituted for merope-nem 1 g every 8 hours if penicillin allergic) and fluco-nazole 400 mg once daily.Exclusion Criteria. Patients were excluded from the
ALF/SALF cohorts if on presentation they had evi-dence of bacterial, fungal, or viral infection on clinicalexamination, radiological or laboratory investigation,malignancy, and any coexisting history of immunodefi-ciency including human immunodeficiency virus(HIV) and glycogen storage disease. Patients with pre-existing liver disease, a history of alcohol intake >20g/day, or who were on immunosuppressive therapiessuch as steroids or azathioprine were also excluded.Consent and Data Collection. The study was per-
formed in accordance with the Declaration of Helsinkiand ethical permission was granted from the NorthEast London Research Ethics Committee (Ref. No.08/H0702/52). Following obtaining fully informedconsent/assent, clinical, biochemical, and physiologicaldata were collected. Data included tobacco and alcoholuse, arterial ammonia (lmol/L), serum sodium levels(mmol/L), arterial blood gas analysis including lactate(mmol/L), differential leukocyte count (�109), com-plement, and immunoglobulin and lipoprotein levels.SIRS score16 was also calculated on admission and on
subsequent neutrophil sampling days. A number oforgan failure scores were also quantified including themodel of endstage liver disease score (MELD), sequen-tial organ failure assessment score (SOFA),17 and theacute physiology and chronic health evaluation(APACHE) II score.18 Length of ICU stay, survival,and number of days requiring vasopressors, ventilation,or hemofiltration were also recorded.Antibiotic use and details of potentially immuno-
modulatory therapies such as corticosteroids, hypother-mia, hemofiltration, and plasmapheresis were recorded.The occurrence of bacterial and fungal infection wasrecorded along with other relevant patient outcomesincluding the development of organ failure and 90-daysurvival.Blood Sampling. Venous blood was collected asep-
tically from patients/volunteers into heparinized pyro-gen-free tubes and was immediately precooled to 0-4�C for 10 minutes. Neutrophil phenotype and func-tion test analyses were performed within 1 hour ofblood being drawn. Plasma was obtained by centrifu-gation at 4,500 rpm for 10 minutes at 4�C and storedat �80�C for subsequent cytokine determination byenzyme-linked immunosorbent assay (ELISA).Characterization of Neutrophil Phenotype. Poly-
morphonuclear granulocytes (PMN) were isolatedusing a blood lysis method. One hundred microliteraliquots of whole blood were placed in flow cytometrytubes and 1 mL of lysis solution (containing <15 mLformaldehyde and <50 mL diethylene glycol; BectonDickinson, UK) was added to each tube at room tem-perature for 15 minutes. The solution was centrifugedat 1,600 rpm for 5 minutes at 18�C and the supernatantdiscarded leaving the PMN pellet at the bottom of thetube. Twenty microliters of each of two antibody stains(antihuman CD16-phycoerythrin(PE)IgG1j and anti-human CD11b-APCCy7IgG1j; Becton Dickinson,UK) was then added and incubated at room tempera-ture in darkness for 25 minutes. The cells were thenwashed twice with sterile phosphate-buffered saline(PBS) prior to analysis by fluorescence activated cellsorting (FACS) using a FACS Canto II analyzer andFACS Diva 6.0 software (Becton Dickinson, San Jose,CA). Neutrophils were gated from the PMNs on for-ward and side-scatter characteristics and the percentageof CD16/CD11b-positive cells were calculated alongwith the mean fluorescence intensity (MFI).Ex Vivo Neutrophil Function Studies. The neutro-
phil function studies were performed as described.11
All ex vivo studies were performed in pyrogen-freeconditions. Neutrophil function was examined in freshneutrophils isolated from whole blood to more closely
1144 TAYLOR ET AL. HEPATOLOGY, March 2013
resemble physiological conditions and to prevent neu-trophil activation during separation, with all samplesbeing performed in triplicate.(1) Phagocytic Activity. Phagocytosis was quanti-
fied using the Phagotest (Orpegen Pharma), whichuses fluorescein isothiocyanate (FITC)-labeled opson-ized E. coli bacteria and analyzed using flow cytome-tery. In brief, 100 lL of heparinized whole blood wasmixed with 20 lL of FITC-labeled opsonized E. coli(2 � 107) (opsonized with immunoglobulin and com-plement of pooled sera) and incubated in a water bathat 37�C for 20 minutes. Fluorescence of bacteria atthe cell surface was quenched using ice-cold Trypanblue solution. Red blood cells were lysed and PMNswere washed twice with sterile PBS prior to analysis.Neutrophils were gated on forward and side-scattercharacteristics and stained with anti-CD16-Phycoery-thrin(PE)IgG1 j and analyzed by FACS. NPA wasexpressed as the percentage of neutrophils undergoingphagocytosis along with the MFI. The interassay andintraassay coefficient of variance for triplicate sampleswere 1.6% and 10.1%, respectively.(2) Oxidative Burst. Neutrophil OB was quantified
using the Burstest (Orpegen Pharma) which measuresthe percentage of phagocytic cells that produce ROS.In brief, 100 lL of heparinized whole blood was incu-bated for 20 minutes with 20 lL of opsonized E. coli
(2 � 107), or without stimulus at 37�C. Neutrophilhigh burst capacity was assessed by adding 5 lL ofphorbol 12-myristate 13-acetate (PMA), a protein ki-nase C activator, to 100 lL of heparinized wholeblood. Neutrophil low burst was assessed by adding 5lL of the chemotactic synthetic peptide formyl-Met-Leu-Phe (fMLP) for 20 minutes at 37�C. fMLP is asynthetic peptide that mimics the activity of bacteriallyderived peptides with formylated N-terminal methioninegroups. The formation of ROS was detected using the ox-idation of dihydrorhodamine-123 to rhodamine-123which emits green fluorescence. Red blood cells werelysed and PMNs were washed with sterile PBS prior toanalysis. Neutrophils were gated on forward and side-scatter characteristics and stained with anti-CD16-Phy-coerythrin(PE)IgG1 j and analyzed by FACS. OB wasdetermined by the percentage of CD16-positive cells pro-ducing ROS, which was calculated along with the MFI.The interassay coefficient of variance was 4.7% and 2.4%for spontaneous and stimulated OB, respectively. Theintraassay coefficient of variance was 5.4% and 4.2% forspontaneous and stimulated OB, respectively.Cytokine Measurement. Plasma levels of the pro-
and antiinflammatory cytokines (TNF-a, IL-1b, IL-6,CXC8/IL-8, IL-10, and IL-17) were determined fromsamples previously stored at �80�C using sandwichELISA (R&D Systems DuoSets, UK).
Table 1. Baseline Demographic Data for Patients With ALF/SALF
Severe
Sepsis
Acute Liver
Failure
Subacute Liver
Failure
Liver Failure Spontaneous
Survivors
Liver Failure Death /
Liver Transplantation
Number 6 15 10 10 15
Median age (range) 40.5 (24-70) 33 (26-48) 52.5 (44-60) 34 (28-44) 51 (32-59)
Female (%) 2 (33) 10 (67) 6 (60) 7 (70) 9 (60)
Etiology (%)
Acetaminophen 6 (40) — 3 (30) 3 (20)
Viral hepatitis (HAV, HBV, HEV). 3 (20) 1 (10) 2 (20) 2 (13)
Seronegative hepatitis 1 (7) 7 (70) 3 (30) 5 (33)
Drug-induced (nonacetaminophen) 2 (13) 2 (20) — 4 (27)
Ischemia/Budd-Chiari/eosinophilic. 3 (20) — 2 (20) 1 (7)
Etiology of sepsis (%)
Infected pancreatic pseudocyst 3 (50)
Aspiration pneumonia† 1 (17)
Infective endocarditis 1 (17)
Fecal peritonitis‡ 1 (17)
Transplant-free 90 day survival (%) 7/15 (40) 3/10 (30) 10/10 (100) 0 (0)
Met King’s criteria for LT (%)* 9/15 (60) 8/10 (80) 2/10 (20) 15 (100)
Declined LT due to comorbidity (%) 4/9 (44) 1/10 (10) 2/2 (100) 3/15 (20)
Underwent LT (%) 4/9 (44) 6/10 (60) 10/15 (67)
Listed for LT but died before graft
became available (%)
1/9 (12) — 1/15 (7)
Listed but survived without LT — 1/10 (10) 1/10 (10)
Died (%) 4 (67) 4/15 (27) 2/10 (20) 6/15 (40)
*Fulfilled King’s College Hospital poor prognostic criteria (19).
†This patient had comorbidities that included hypertension, diabetes mellitus, hypercholesterolemia, and a previous cerebral vascular accident.
‡This patient had preexisting chronic obstructive pulmonary disease.
ALF, acute liver failure; SALF, subacute liver failure; HAV, hepatitis A virus; HBV, hepatitis B virus; HEV, hepatitis E virus; LT, liver transplantation.
HEPATOLOGY, Vol. 57, No. 3, 2013 TAYLOR ET AL. 1145
Statistics. Where appropriate, values are expressedas median and interquartile range (IQR). Group com-parisons were performed using the chi-squared test forcategorical and Mann-Whitney U test for continuousvariables. When comparing three or more groupssimultaneously, the Kruskal-Wallis test was utilizedwith Dunn’s multiple comparison test. Comparisons ofpaired observations were performed using Wilcoxonmatched pairs test. P < 0.05 was considered statisti-cally significant. All statistical analyses were performedusing GraphPad Prism 4.0 (GraphPad Software, SanDiego, CA).
Results
Patient Baseline Demographics and ClinicalParameters. Fifteen nonconsecutive patients with ALFand 10 patients with SALF were recruited. Baseline(on admission to ICU) patient demographics, bio-chemical, and physiological parameters are detailed inTables 1 and 2, respectively. The ALF group was heter-ogeneous in terms of etiology and severity of liver
injury (acetaminophen n ¼ 6; acute viral hepatitis n ¼3; other n ¼ 6). The predominant etiology in SALF
was seronegative/acute autoimmune hepatitis n ¼ 7.
Table 2. Clinical, Biochemical, Neutrophil, and Organ Failure Parameters of Patients With ALF/SALF
Clinical/Biochemical/Organ Failure Variables
Severe Sepsis
n¼6
Acute Liver Failure
n¼15
Subacute Liver
Failure n¼10 P value
Body mass index 24.5 (20.8-29.7) 21.8 (21.4-24.7) 25.3 (23.2-27.4) 0.74
Empirical antibiotics and antifungals* 6 (100%) 13 (87%) 9 (90%) 0.65
Grade of encephalopathy
Grade 0-2 4 (27%) 5 (50%)
Grade 3-4 11 (73%) 5 (50%) 0.62
Mean arterial pressure (mmHg) 83 (74-88) 71.5 (67-81.5) 80 (73-94) 0.05
SIRS score 3 (2-3) 2 (1-2.5) 1 (1-2) 0.22
MELD score 13 (9-14) 34.2 (31.7-41.4) 42.4 (28.1-48.8) 0.001†
SOFA score 6 (4.5-6.5) 16 (14.5-17.0) 16 (15.5-17.5) 0.04†
APACHE II score 14 (11-17) 21 (17.5-24.5) 22 (18.5-23.5) 0.17
Number requiring invasive ventilation 3 (50%) 9 (60%) 6 (60%) 0.91
Number requiring vasopressors 4 (66%) 6 (40%) 3 (30%) 0.36
Number requiring hemofiltration 2 (33%) 10 (66%) 6 (60%) 0.37
Days on hemofiltration 3 (3-5) 4.0 (3.25-7.25) 4.0 (1.5-5.0) 0.63
Hemoglobin (g/dL) 9.0 (8.2-9.7) 9.5 (8.2-11) 9.3 (8.7-12.8) 0.44
White cell count (x 109/L) 13.6 (9.7-18.7) 12.7 (5.3-13.7) 9.6 (6.4-12.9) 0.38
Neutrophil count (x 109‡L) 11.7 (8.2-15.5) 7.5 (5.5-11.0) 7.9 (5.1-10.1) 0.31
Lymphocyte count (x 109/L) 1.1 (0.8-1.2) 1.0 (0.5-2.0) 0.7 (0.5-1.7) 0.77
Platelets (x 109/L) 319 (161-508) 92 (60-197) 89.5 (75.5-180.5) 0.06
INR 1.32 (1.19-1.38) 3.21 (2.25.4.70) 3.18 (2.27-7.15) 0.002†
Aspartate aminotransferase (IU/L) 35 (32-42) 386 (237-2577) 203 (131-1062) 0.001†
Bilirubin (lmol/L) 9 (7-10) 106 (80.0-210.5) 189 (136.8-266.0) 0.001†
Albumin (g/L) 27 (20-29) 21 (19.5-25.0) 17 (13.8-27.0) 0.39
Sodium (mmol/L) 142 (137-146) 142 (140.5-145.5) 143 (136.5-144.8) 0.90
Creatinine (lmol/L) 105 (69-138) 161 (89.5-214.0) 132 (89.3-120.5) 0.51
Glucose (mmol/L) 7.8 (6.8-8.6) 7 (6.1-9.1) 5.7 (4.7-10.1) 0.65
Ferritin (lg/L) 198 (198-198) 1665 (170-20,853) 2177 (1453-10,401) 0.30
Lactate (mmol/L) 0.9 (0.7-1.2) 2 (1.4-3.0) 2 (1.65-2.5) 0.025†
C-reactive protein (mg/L) 226 (116-349) 17.3 (5.3-31.8) 23 (8.1-29.5) 0.001‡
Arterial ammonia (lmol/L) 22 (19-25) 75 (62-107) 61.5 (44-84) 0.001†
High density lipoprotein (mmol/L) 0.5 (0.35-0.65) 0.35 (0.18-0.50) 0.1 (0.10-1.13) 0.02§
Arterial pH 7.4 (7.38-7.43) 7.4 (7.37-7.46) 7.49 (4.43-7.52) 0.15
% Neutrophil phagocytic activity 70.2 (55.6-78.3) 66.0 (48.8-81.5) 39.6 (32.5-63.9) 0.16
% Neutrophil resting burst 6.8 (6.3-8.1) 13.8 (6.4-22.8) 6.3 (2.7-10.0) 0.35
% Neutrophil stimulated burst 52.2 (39.3-75.3) 85.4 (76.3-92.0) 85.8 (71.8-90.5) 0.11
Data presented as number of cases (percentage) or median (IQR) for the variables as appropriate.
ALF, acute liver failure; SALF, subacute liver failure; MELD, model of endstage liver disease; SOFA, sequential organ failure score; APACHE II, acute physiology and
chronic health evaluation II; SIRS, systemic inflammatory response syndrome score
*Patients presenting with ALF/SALF were given empirical intravenous antibiotic and antifungal cover as standard of care. This was tazocin 4.5 g every 8 hours
(substituted for meropenem 1 g every 8 hours in those who were penicillin allergic) and fluconazole 400 mg once daily.
†Values in both ALF and SALF cohorts were significantly increased compared with septic controls.
‡C-reactive protein was significantly greater in septic controls compared with both ALF and SALF cohorts.
§HDL values were significantly lower in SALF cohort compared to the ALF cohort. The Kruskal-Wallis test was utilized with Dunn’s multiple comparison test and P< 0.05 was considered statistically significant.
1146 TAYLOR ET AL. HEPATOLOGY, March 2013
Within the ALF cohort 9/15 (60%) fulfilled King’sCollege Hospital criteria for poor prognosis,19 ofwhom 4/9 (44%) underwent successful LT, 4/9 (44%)were declined LT due to comorbidity, and 1/9 (12%)was listed but died of cerebral edema before a graftbecame available. One patient met poor prognostic cri-
teria but was declined due to psychiatric comorbidityand survived following plasmapheresis. In the SALFcohort 8/10 (80%) fulfilled poor prognostic criteria, ofwhom 6/10 (60%) underwent LT, 1/10 (10%) wasdeclined due to comorbidity, and 1/10 (10%) recov-ered and was delisted. Two SALF patients died (onepost-LT from MODS).All patients with ALF/SALF were significantly unwell
with MODS and, indeed, MELD and SOFA scoreswere significantly higher in the ALF and SALF cohortscompared to the SC (P ¼ 0.001 and P ¼ 0.0035,respectively) (Table 2). Patients with SALF had a tend-ency to be older, with higher bilirubin and lower arterialammonia, but due to the small numbers in the groupsthese comparisons did not reach significance.Neutrophil Phenotype. Neutrophil surface receptor
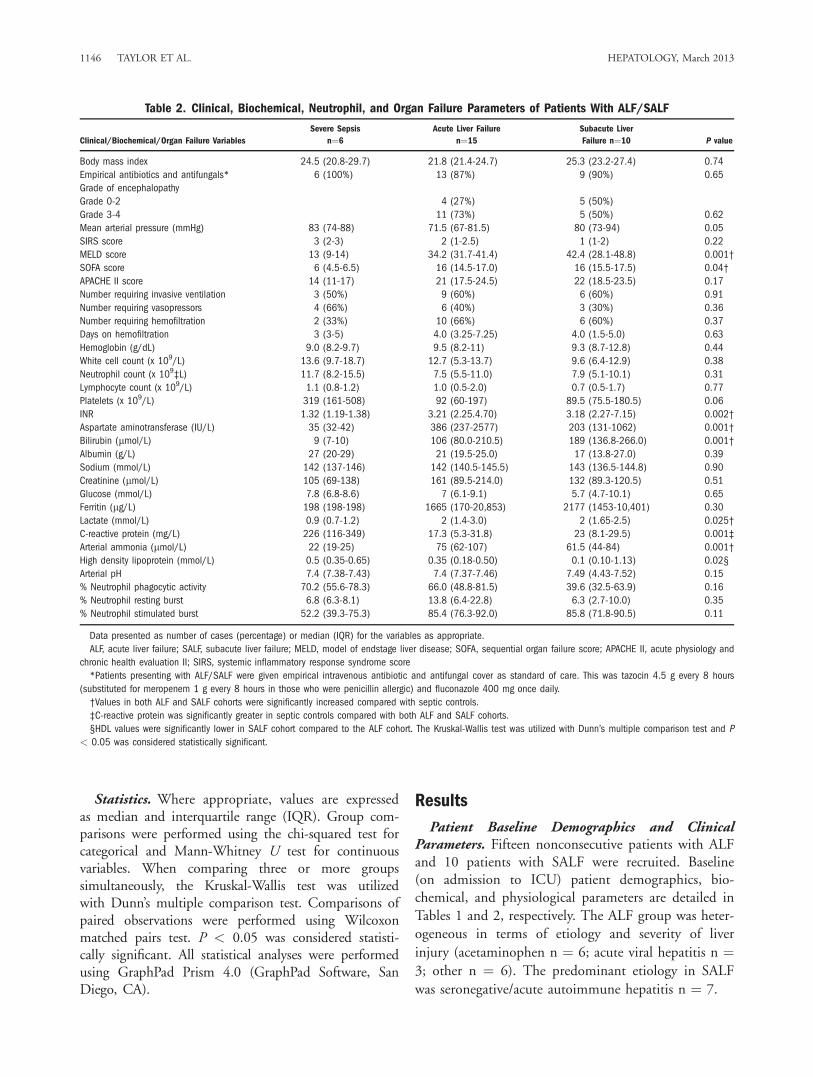
expression of CD16 (FccRIII) and CD11b (Mac-1)was performed on days 1, 4, and 7 in 8/15 of theALF cohort and compared to HC (n ¼ 8) and SC (n¼ 5). Neutrophil expression of CD16 was significantlyreduced in the ALF cohort compared to HC (P <0.001) on day 1 (Fig. 1). CD16 expression was alsoreduced in the SC group compared to HC but this
Fig. 1. Neutrophil CD16 expression (Immunoglobulin G: FccRIII) inhealthy controls (n ¼ 8) compared to septic controls (n ¼ 5) andpatients with ALF (n ¼ 8) on day 1 of ICU admission. Differencesbetween healthy controls and patients were calculated using the Krus-kal-Wallis test (P ¼ 0.0006) with Dunn’s multiple comparison test.ALF patients had significantly reduced neutrophil CD16 expressioncompared to controls (***P < 0.001).
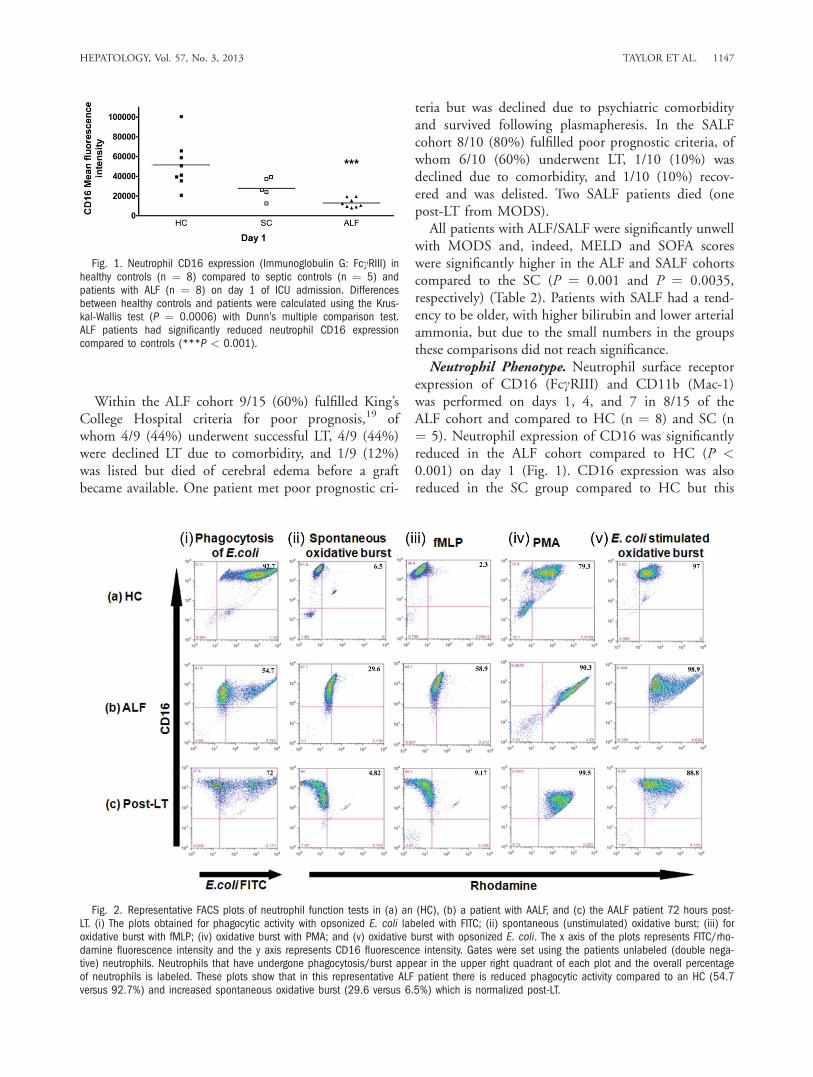
Fig. 2. Representative FACS plots of neutrophil function tests in (a) an (HC), (b) a patient with AALF, and (c) the AALF patient 72 hours post-LT. (i) The plots obtained for phagocytic activity with opsonized E. coli labeled with FITC; (ii) spontaneous (unstimulated) oxidative burst; (iii) foroxidative burst with fMLP; (iv) oxidative burst with PMA; and (v) oxidative burst with opsonized E. coli. The x axis of the plots represents FITC/rho-damine fluorescence intensity and the y axis represents CD16 fluorescence intensity. Gates were set using the patients unlabeled (double nega-tive) neutrophils. Neutrophils that have undergone phagocytosis/burst appear in the upper right quadrant of each plot and the overall percentageof neutrophils is labeled. These plots show that in this representative ALF patient there is reduced phagocytic activity compared to an HC (54.7versus 92.7%) and increased spontaneous oxidative burst (29.6 versus 6.5%) which is normalized post-LT.
HEPATOLOGY, Vol. 57, No. 3, 2013 TAYLOR ET AL. 1147
did not reach statistical significance. The CD16 down-regulation persisted in the ALF group on days 4 and 7regardless of outcome but normalized within 72 hourspost-LT. No differences were observed in neutrophil
surface receptor expression of CD11b in patients withALF/SALF or in SC (data not shown).Neutrophil Phagocytic Activity (NPA). Neutrophils
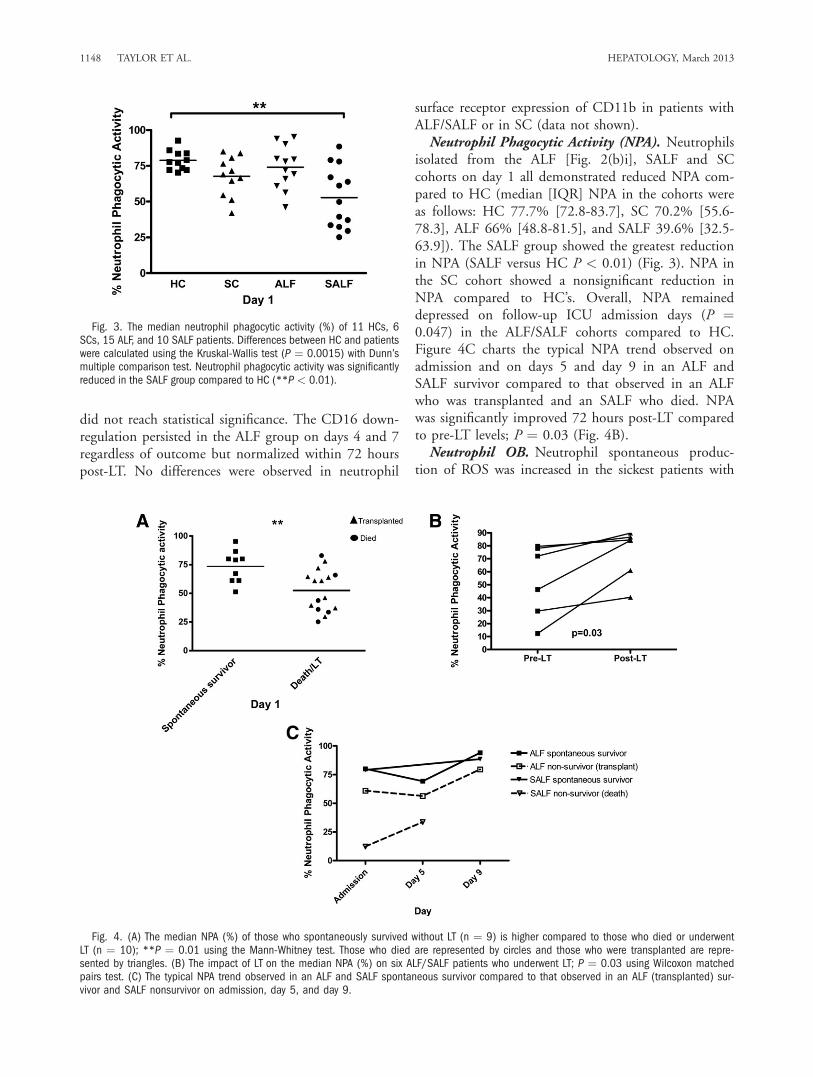
isolated from the ALF [Fig. 2(b)i], SALF and SCcohorts on day 1 all demonstrated reduced NPA com-pared to HC (median [IQR] NPA in the cohorts wereas follows: HC 77.7% [72.8-83.7], SC 70.2% [55.6-78.3], ALF 66% [48.8-81.5], and SALF 39.6% [32.5-63.9]). The SALF group showed the greatest reductionin NPA (SALF versus HC P < 0.01) (Fig. 3). NPA inthe SC cohort showed a nonsignificant reduction inNPA compared to HC’s. Overall, NPA remaineddepressed on follow-up ICU admission days (P ¼0.047) in the ALF/SALF cohorts compared to HC.Figure 4C charts the typical NPA trend observed onadmission and on days 5 and day 9 in an ALF andSALF survivor compared to that observed in an ALFwho was transplanted and an SALF who died. NPAwas significantly improved 72 hours post-LT comparedto pre-LT levels; P ¼ 0.03 (Fig. 4B).Neutrophil OB. Neutrophil spontaneous produc-
tion of ROS was increased in the sickest patients with
Fig. 3. The median neutrophil phagocytic activity (%) of 11 HCs, 6SCs, 15 ALF, and 10 SALF patients. Differences between HC and patientswere calculated using the Kruskal-Wallis test (P ¼ 0.0015) with Dunn’smultiple comparison test. Neutrophil phagocytic activity was significantlyreduced in the SALF group compared to HC (**P < 0.01).
Fig. 4. (A) The median NPA (%) of those who spontaneously survived without LT (n ¼ 9) is higher compared to those who died or underwentLT (n ¼ 10); **P ¼ 0.01 using the Mann-Whitney test. Those who died are represented by circles and those who were transplanted are repre-sented by triangles. (B) The impact of LT on the median NPA (%) on six ALF/SALF patients who underwent LT; P ¼ 0.03 using Wilcoxon matchedpairs test. (C) The typical NPA trend observed in an ALF and SALF spontaneous survivor compared to that observed in an ALF (transplanted) sur-vivor and SALF nonsurvivor on admission, day 5, and day 9.
1148 TAYLOR ET AL. HEPATOLOGY, March 2013
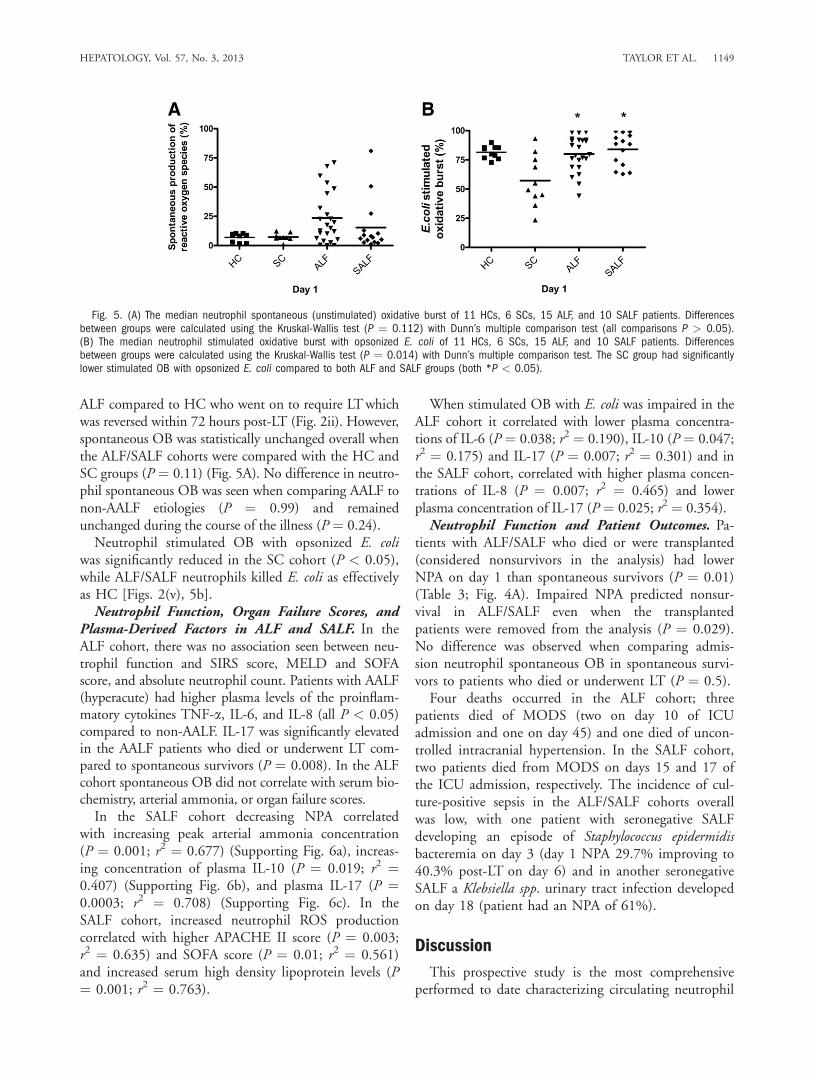
ALF compared to HC who went on to require LTwhichwas reversed within 72 hours post-LT (Fig. 2ii). However,spontaneous OB was statistically unchanged overall whenthe ALF/SALF cohorts were compared with the HC andSC groups (P ¼ 0.11) (Fig. 5A). No difference in neutro-phil spontaneous OB was seen when comparing AALF tonon-AALF etiologies (P ¼ 0.99) and remainedunchanged during the course of the illness (P ¼ 0.24).Neutrophil stimulated OB with opsonized E. coli
was significantly reduced in the SC cohort (P < 0.05),while ALF/SALF neutrophils killed E. coli as effectivelyas HC [Figs. 2(v), 5b].Neutrophil Function, Organ Failure Scores, and
Plasma-Derived Factors in ALF and SALF. In theALF cohort, there was no association seen between neu-trophil function and SIRS score, MELD and SOFAscore, and absolute neutrophil count. Patients with AALF(hyperacute) had higher plasma levels of the proinflam-matory cytokines TNF-a, IL-6, and IL-8 (all P < 0.05)compared to non-AALF. IL-17 was significantly elevatedin the AALF patients who died or underwent LT com-pared to spontaneous survivors (P ¼ 0.008). In the ALFcohort spontaneous OB did not correlate with serum bio-chemistry, arterial ammonia, or organ failure scores.In the SALF cohort decreasing NPA correlated
with increasing peak arterial ammonia concentration(P ¼ 0.001; r2 ¼ 0.677) (Supporting Fig. 6a), increas-ing concentration of plasma IL-10 (P ¼ 0.019; r2 ¼0.407) (Supporting Fig. 6b), and plasma IL-17 (P ¼0.0003; r2 ¼ 0.708) (Supporting Fig. 6c). In theSALF cohort, increased neutrophil ROS productioncorrelated with higher APACHE II score (P ¼ 0.003;r2 ¼ 0.635) and SOFA score (P ¼ 0.01; r2 ¼ 0.561)and increased serum high density lipoprotein levels (P¼ 0.001; r2 ¼ 0.763).
When stimulated OB with E. coli was impaired in theALF cohort it correlated with lower plasma concentra-tions of IL-6 (P ¼ 0.038; r2 ¼ 0.190), IL-10 (P ¼ 0.047;r2 ¼ 0.175) and IL-17 (P ¼ 0.007; r2 ¼ 0.301) and inthe SALF cohort, correlated with higher plasma concen-trations of IL-8 (P ¼ 0.007; r2 ¼ 0.465) and lowerplasma concentration of IL-17 (P ¼ 0.025; r2 ¼ 0.354).
Neutrophil Function and Patient Outcomes. Pa-tients with ALF/SALF who died or were transplanted(considered nonsurvivors in the analysis) had lowerNPA on day 1 than spontaneous survivors (P ¼ 0.01)(Table 3; Fig. 4A). Impaired NPA predicted nonsur-vival in ALF/SALF even when the transplantedpatients were removed from the analysis (P ¼ 0.029).No difference was observed when comparing admis-sion neutrophil spontaneous OB in spontaneous survi-vors to patients who died or underwent LT (P ¼ 0.5).Four deaths occurred in the ALF cohort; three
patients died of MODS (two on day 10 of ICUadmission and one on day 45) and one died of uncon-trolled intracranial hypertension. In the SALF cohort,two patients died from MODS on days 15 and 17 ofthe ICU admission, respectively. The incidence of cul-ture-positive sepsis in the ALF/SALF cohorts overallwas low, with one patient with seronegative SALFdeveloping an episode of Staphylococcus epidermidisbacteremia on day 3 (day 1 NPA 29.7% improving to40.3% post-LT on day 6) and in another seronegativeSALF a Klebsiella spp. urinary tract infection developedon day 18 (patient had an NPA of 61%).
Discussion
This prospective study is the most comprehensiveperformed to date characterizing circulating neutrophil
Fig. 5. (A) The median neutrophil spontaneous (unstimulated) oxidative burst of 11 HCs, 6 SCs, 15 ALF, and 10 SALF patients. Differencesbetween groups were calculated using the Kruskal-Wallis test (P ¼ 0.112) with Dunn’s multiple comparison test (all comparisons P > 0.05).(B) The median neutrophil stimulated oxidative burst with opsonized E. coli of 11 HCs, 6 SCs, 15 ALF, and 10 SALF patients. Differencesbetween groups were calculated using the Kruskal-Wallis test (P ¼ 0.014) with Dunn’s multiple comparison test. The SC group had significantlylower stimulated OB with opsonized E. coli compared to both ALF and SALF groups (both *P < 0.05).
HEPATOLOGY, Vol. 57, No. 3, 2013 TAYLOR ET AL. 1149
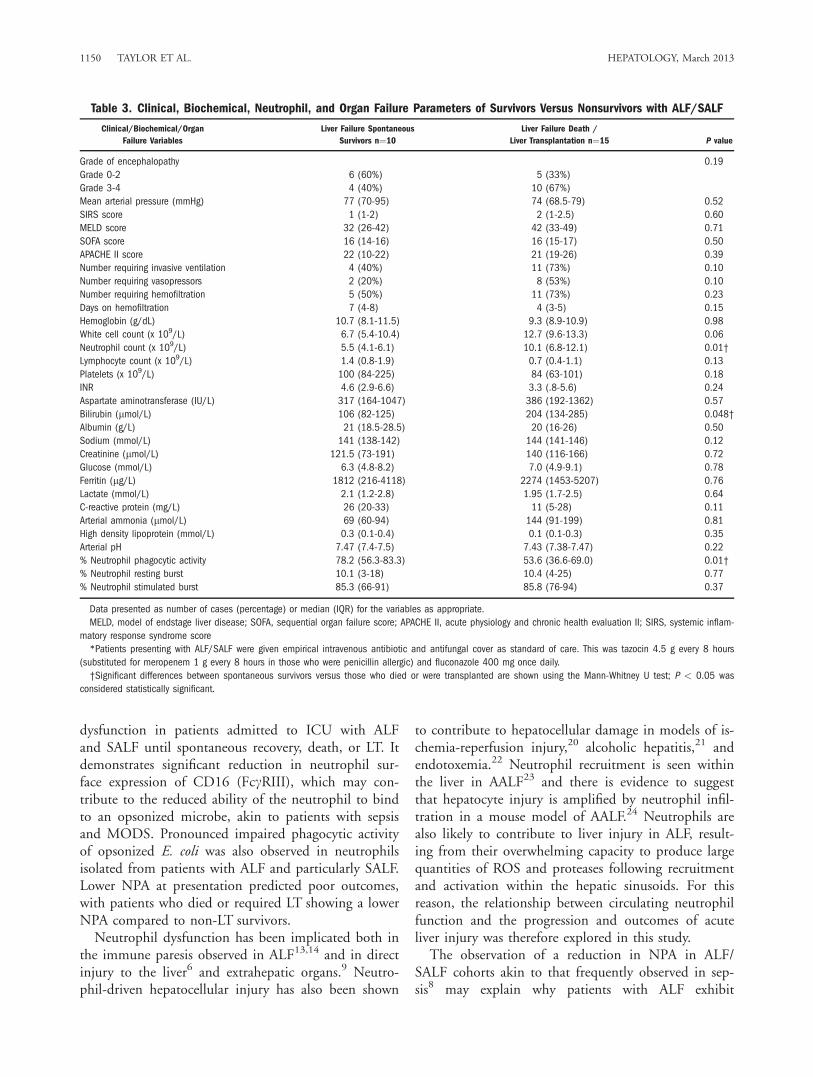
dysfunction in patients admitted to ICU with ALFand SALF until spontaneous recovery, death, or LT. Itdemonstrates significant reduction in neutrophil sur-face expression of CD16 (FccRIII), which may con-tribute to the reduced ability of the neutrophil to bindto an opsonized microbe, akin to patients with sepsisand MODS. Pronounced impaired phagocytic activityof opsonized E. coli was also observed in neutrophilsisolated from patients with ALF and particularly SALF.Lower NPA at presentation predicted poor outcomes,with patients who died or required LT showing a lowerNPA compared to non-LT survivors.Neutrophil dysfunction has been implicated both in
the immune paresis observed in ALF13,14 and in directinjury to the liver6 and extrahepatic organs.9 Neutro-phil-driven hepatocellular injury has also been shown
to contribute to hepatocellular damage in models of is-chemia-reperfusion injury,20 alcoholic hepatitis,21 andendotoxemia.22 Neutrophil recruitment is seen withinthe liver in AALF23 and there is evidence to suggestthat hepatocyte injury is amplified by neutrophil infil-tration in a mouse model of AALF.24 Neutrophils arealso likely to contribute to liver injury in ALF, result-ing from their overwhelming capacity to produce largequantities of ROS and proteases following recruitmentand activation within the hepatic sinusoids. For thisreason, the relationship between circulating neutrophilfunction and the progression and outcomes of acuteliver injury was therefore explored in this study.The observation of a reduction in NPA in ALF/
SALF cohorts akin to that frequently observed in sep-sis8 may explain why patients with ALF exhibit
Table 3. Clinical, Biochemical, Neutrophil, and Organ Failure Parameters of Survivors Versus Nonsurvivors with ALF/SALF
Clinical/Biochemical/Organ
Failure Variables
Liver Failure Spontaneous
Survivors n¼10
Liver Failure Death /
Liver Transplantation n¼15 P value
Grade of encephalopathy 0.19
Grade 0-2 6 (60%) 5 (33%)
Grade 3-4 4 (40%) 10 (67%)
Mean arterial pressure (mmHg) 77 (70-95) 74 (68.5-79) 0.52
SIRS score 1 (1-2) 2 (1-2.5) 0.60
MELD score 32 (26-42) 42 (33-49) 0.71
SOFA score 16 (14-16) 16 (15-17) 0.50
APACHE II score 22 (10-22) 21 (19-26) 0.39
Number requiring invasive ventilation 4 (40%) 11 (73%) 0.10
Number requiring vasopressors 2 (20%) 8 (53%) 0.10
Number requiring hemofiltration 5 (50%) 11 (73%) 0.23
Days on hemofiltration 7 (4-8) 4 (3-5) 0.15
Hemoglobin (g/dL) 10.7 (8.1-11.5) 9.3 (8.9-10.9) 0.98
White cell count (x 109/L) 6.7 (5.4-10.4) 12.7 (9.6-13.3) 0.06
Neutrophil count (x 109/L) 5.5 (4.1-6.1) 10.1 (6.8-12.1) 0.01†
Lymphocyte count (x 109/L) 1.4 (0.8-1.9) 0.7 (0.4-1.1) 0.13
Platelets (x 109/L) 100 (84-225) 84 (63-101) 0.18
INR 4.6 (2.9-6.6) 3.3 (.8-5.6) 0.24
Aspartate aminotransferase (IU/L) 317 (164-1047) 386 (192-1362) 0.57
Bilirubin (lmol/L) 106 (82-125) 204 (134-285) 0.048†
Albumin (g/L) 21 (18.5-28.5) 20 (16-26) 0.50
Sodium (mmol/L) 141 (138-142) 144 (141-146) 0.12
Creatinine (lmol/L) 121.5 (73-191) 140 (116-166) 0.72
Glucose (mmol/L) 6.3 (4.8-8.2) 7.0 (4.9-9.1) 0.78
Ferritin (lg/L) 1812 (216-4118) 2274 (1453-5207) 0.76
Lactate (mmol/L) 2.1 (1.2-2.8) 1.95 (1.7-2.5) 0.64
C-reactive protein (mg/L) 26 (20-33) 11 (5-28) 0.11
Arterial ammonia (lmol/L) 69 (60-94) 144 (91-199) 0.81
High density lipoprotein (mmol/L) 0.3 (0.1-0.4) 0.1 (0.1-0.3) 0.35
Arterial pH 7.47 (7.4-7.5) 7.43 (7.38-7.47) 0.22
% Neutrophil phagocytic activity 78.2 (56.3-83.3) 53.6 (36.6-69.0) 0.01†
% Neutrophil resting burst 10.1 (3-18) 10.4 (4-25) 0.77
% Neutrophil stimulated burst 85.3 (66-91) 85.8 (76-94) 0.37
Data presented as number of cases (percentage) or median (IQR) for the variables as appropriate.
MELD, model of endstage liver disease; SOFA, sequential organ failure score; APACHE II, acute physiology and chronic health evaluation II; SIRS, systemic inflam-
matory response syndrome score
*Patients presenting with ALF/SALF were given empirical intravenous antibiotic and antifungal cover as standard of care. This was tazocin 4.5 g every 8 hours
(substituted for meropenem 1 g every 8 hours in those who were penicillin allergic) and fluconazole 400 mg once daily.
†Significant differences between spontaneous survivors versus those who died or were transplanted are shown using the Mann-Whitney U test; P < 0.05 was
considered statistically significant.
1150 TAYLOR ET AL. HEPATOLOGY, March 2013

phenotypic features of septic shock with microvasculardysfunction, hemodynamic instability, coagulopathy,encephalopathy, MODS, and high levels of circulatingproinflammatory cytokines. Why the severity of NPAis less so in those presenting with ALF compared toSALF is less clear but the development of impairedNPA may occur in a time-dependent manner, as evi-denced by the most severe reduction in phagocyticability seen in cases of SALF, where the liver injurytakes on a more insidious course over several weeks.Indeed, many patients with established SALF maypresent with moderate portal hypertension with fea-tures of splenomegaly and ascites. Nevertheless, NPAon admission appears to be a predictor of spontaneoussurvival compared to conventional organ failure scoressuch as SOFA and MELD, which did not predictpoor outcome in this study. Trying to understand therelationship between neutrophil phagocytic dysfunctionand poor prognosis therefore seems critical. LT resultedin rapid improvement of neutrophil phagocytic func-tion within 72 hours but not complete reversal, whichcould be the result of ischemia-reperfusion phenom-ena, ongoing production of proinflammatory cyto-kines/SIRS, or sepsis.The incidence of ‘‘culture-positive’’ sepsis was low in
this ALF/SALF cohort overall, and indeed the deathscould not be directly attributed to infection, suggestingphagocytic dysfunction is either a reflection of generalimmune activation or a specific factor related to liverfailure. Peak plasma ammonia levels demonstrated arobust correlation with poor phagocytic function inSALF and high circulating levels of IL-10 and IL-17.Ammonia was previously shown to impair NPA andinduce spontaneous OB in healthy neutrophils exposedto supraphysiological concentrations of ammonia exvivo and in rats fed an ammonia-rich diet.11 The peakarterial ammonia concentration did not, however, cor-relate with impaired NPA in the ALF cohort butmight be attributed to the impact of rapid ammoniareduction by continuous veno-venous hemofiltrationprior to neutrophil sampling.Pro- and antiinflammatory cytokine profiles might
be expected to show a closer association with neutro-phil OB than phagocytic activity, although this wasnot generally the case. Higher plasma IL-10 and IL-17concentrations correlated with impaired NPA and maysuggest the development of a compensatory antiinflam-matory response syndrome (CARS) in this condition25
with involvement of T-regulatory cells.26 However, thecondition with the highest levels of proinflammatorycytokines, AALF demonstrated only modest neutrophildysfunction. CD4þCD25þCD127-FOXP3þ T-regu-
latory cells directly inhibit neutrophil function, pro-moting apoptosis and death when exposed to lipopoly-saccharide through TLR4 expressed on their surfacewhich inhibits proinflammatory activities.27 This is animportant role in the direct control of innate immuneresponses. Upon activation, these T-regulatory cells caneither induce themselves or CD4þCD25-FOXP3-Teffector cells to differentiate into IL-17A-producingcells, Th17, in the presence of TGF-beta, and/or IL-6.28 In contrast to the role of T-regs on neutrophils,one of the functions of Th17 is to recruit neutrophilsinto inflamed tissue, further increasing the antimicro-bial response in vitro and in vivo.29,30
The evidence for a role of increased circulating neu-trophil production of ROS as a contributor to the de-velopment of MODS and poor outcomes in ALF inthis study is less clear than that of NPA. Interestingly,in the SALF cohort increased spontaneous OB corre-lated with increased serum high density lipoproteinlevels and higher SOFA and APACHE II scores. High-density lipoprotein plays an important role in thetransport of cholesterol to the adrenal gland for steroi-dogenesis, which may modulate the response to sepsisand critical illness. Low concentrations of high-densitylipoprotein have recently been shown to be a predictorof poor outcome in ALF but were not associated withan increased risk of sepsis.31 The problem with meas-uring spontaneous neutrophil ROS production in iso-lated circulating cells is that this may not reflect theproduction within the hepatic parenchyma or otherorgans, so it is difficult to draw firm conclusions. Inaddition, ALF and SALF patients are a heterogeneouspatient group who are prone to deteriorating rapidly,necessitating a number of invasive interventions suchas high flow hemofiltration and mild hypothermiapotentially influencing neutrophil function and whichare difficult to control for, constituting the main weak-ness of this study. Furthermore, the empirical use ofpotent broad-spectrum antibiotics and antifungals asstandard of care in this study is also likely to haveabrogated any increased susceptibility to developingsepsis in this cohort.Neutrophil stimulated OB with E. coli was signifi-
cantly reduced in the SC group, while ALF/SALF neutro-phils killed E. coli as effectively as HC. This may repre-sent the fact that neutrophils in patients with sepsis havebeen exhausted fighting the infection and have very littlecapacity left for responding to the E. coli. Alternatively, itcould result from the development of CARS.In summary, circulating neutrophils in patients with
ALF/SALF have impaired bacteriocidal function simi-lar to that seen in patients with severe sepsis and
HEPATOLOGY, Vol. 57, No. 3, 2013 TAYLOR ET AL. 1151

MODS. Neutrophil function indices are importantbiomarkers of poor prognosis in ALF/SALF and can beimplicated as important mediators in the developmentof cellular and organ dysfunction and the increased sus-ceptibility to developing sepsis. Clearly these neutrophilfunction tests in their present format are cumbersome toperform and cannot be performed at the bedside, butdevelopment of a rapid test of neutrophil dysfunctionmay offer the possibility for refinement of current prog-nostic criteria and might tailor therapy to those at high-est risk. These data also support the circulating neutro-phil as a novel therapeutic target in ALF.
Acknowledgment: We are indebted to Dr. LeeMarkwick for invaluable input into article preparation.
References1. Trey C, Davidson CS. The management of fulminant hepatic failure.
Prog Liver Dis 1970;3:282-298.2. Bernal W, Auzinger G, Dhawan A, Wendon J. Acute liver failure. Lan-
cet 2010;376:190-201.3. Lee W, Harrison R, Grinstein S. Phagocytosis by neutrophils. Microbes
Infect 2003;5:1299-1306.4. Dahlgren C, Karlsson A. Respiratory burst in human neutrophils. J
Immunol Methods 1999;232:3-14.5. Schlayer HJ, Laaff H, Peters T, Woort-Menker M, Estler HC, Karck
U, et al. Involvement of tumor necrosis factor in endotoxin-triggeredneutrophil adherence to sinusoidal endothelial cells of mouse liver andits modulation in acute phase. J Hepatol 1988;7:239-249.
6. Ramaiah SK, Jaeschke H. Role of neutrophils in the pathogenesis ofacute inflammatory liver injury. Toxicol Pathol 2007;35:757-766.
7. Rolando N, Wade J, Davalos M, Wendon J, Philpott-Howard J, Wil-liams R. The systemic inflammatory response syndrome in acute liverfailure. HEPATOLOGY 2000;32:734-739.
8. Brown KA, Brain SD, Pearson JD, Edgeworth JD, Lewis SM, TreacherDF. Neutrophils in development of multiple organ failure in sepsis.Lancet 2006;368:157-169.
9. Awad AS, Rouse M, Huang L, Vergis AL, Reutershan J, Cathro HP,et al. Compartmentalization of neutrophils in the kidney and lung fol-lowing acute ischemic kidney injury. Kidney Int 2009;75:689-698.
10. Karvellas CJ, Pink F, McPhail M, Cross T, Auzinger G, Bernal W,et al. Predictors of bacteraemia and mortality in patients with acuteliver failure. Intensive Care Med 2009;35:1390-1396.
11. Shawcross D, Wright G, Stadlbauer V, Hodges S, Wheeler-Jones C,Pitsillides A, et al. Ammonia impairs neutrophil phagocytic function inliver disease. HEPATOLOGY 2008;48:1202-1212.
12. Wyke RJ, Yousif-Kadaru AG, Rajkovic IA, Eddleston AL, Williams R.Serum stimulatory activity and polymorphonuclear leucocyte movementin patients with fulminant hepatic failure. Clin Exp Immunol 1982;50:442-449.
13. Altin M, Rajkovic IA, Hughes RD, Williams R. Neutrophil adherencein chronic liver disease and fulminant hepatic failure. Gut 1983;24:746-750.
14. Clapperton M, Rolando N, Sandoval L, Davies E, Williams R. Neutro-
phil superoxide and hydrogen peroxide production in patients with
acute liver failure. Eur J Clin Invest 1997;27:164-168.15. O’Grady JG, Schalm SW, Williams R. Acute liver failure: redefining
the syndromes. Lancet 1993;342:273-275.16. Levy M, Fink M, Marshall J, Abraham E, Angus D, Cook D, et al.
2001 SCCM?ESICM/ACCP/ATS/SIS International Sepsis DefinitionsConference. Intensive Care Med 2003;29:530-538.
17. Vincent JL, Moreno R, Takala J, Willatts S, De Mendonca A, Bruining
H, et al. The SOFA (sepsis-related organ failure assessment) score to
describe organ dysfunction/failure. On behalf of the Working Group
on Sepsis-Related Problems of the European Society of Intensive Care
Medicine. Intensive Care Med 1996;22:707-710.18. Knaus W, Draper E, Wagner D, Zimmerman J. Prognosis in acute
organ-system failure. Ann Surg 1985;202:685-693.19. O’Grady J, Alexander G, Hayllar K, Williams R. Early indicators of
prognosis in fulminant hepatic failure. Gastroenterology 1989;97:439-445.
20. Jaeschke H. Mechanisms of neutrophil-mediated liver cell injury duringischaemia-reperfusion and other acute inflammatory conditions. Am JPhysiol Gastrointest Liver Physiol 2006;290:G1083-G1088.
21. Bautista A. Neutrophilic infiltration in alcoholic hepatitis. Alcohol2002;27:17-21.
22. Dorman RB, Gujral JS, Bajt ML, Farhood A, Jaeschke H. Generation
and functional significance of CXC chemokines for neutrophil-induced
liver injury during endotoxemia. Am J Physiol Gastrointest Liver Phys-
iol 2005;288:G880-G886.23. Lawson JA, Farhood A, Hopper RD, Bajt ML, Jaeschke H. The he-
patic inflammatory response after acetaminophen overdose: role of neu-trophils. Toxicol Sci 2000;54:509-516.
24. Marques PE, Amaral SS, Pires DA, Nogueira LL, Soriani FM, Freire
Lima BH, et al. Chemokines and mitochondrial products activate neu-
trophils to amplify organ injury during mouse acute liver failure. HEPA-
TOLOGY 2012 [Epub ahead of print].25. Antoniades CG, Berry PA, Wendon JA, Vergani D. The importance of
immune dysfunction in determining outcome in acute liver failure. J
Hepatol 2008;49:845-861.26. Lewis DH, Chan DL, Pinheiro D, Armitage-Chan E, Garden OA. The
immunopathology of sepsis: pathogen recognition, systemic inflamma-tion, the compensatory anti-inflammatory response, and regulatory Tcells. J Vet Intern Med 2012;26:457-482.
27. Lewkowicz P, Lewkowicz N, Sasiak A, Tchorzewski H. LPS-activatedCD4þCD25þ T regulatory cells inhibit neutrophil function andpromote their apoptosis and death. J Immunol 2006;177:7155-7163.
28. Xu L, Kitani A, Fuss I, Strober W. Cutting edge: regulatory T cellsinduce CD4þCD25-Foxp3- T cells or are self-induced to becomeTh17 cells in the absence of exogenous TGF-beta. J Immunol 2007;178:6725-6729.
29. Annunziato F, Cosmi L, Liotta F, Maggi E, Romagnani S. The pheno-type of human Th17 cells and their precursors, the cytokines thatmediate their differentiation and the role of Th17 cells in inflamma-tion. Int Immunol 2008;20:1361-1368.
30. Kolls JK, McCray PB Jr, Chan YR. Cytokine-mediated regulation of
antimicrobial proteins. Nat Rev Immunol 2008;8:829-835.31. Atogo-Asse FE, Vincent RP, Hughes SA, Auzinger G, Le Roux CW,
Wendon J, et al. High density lipoprotein in patients with liver failure;relation to sepsis, adrenal function and outcome of illness. Liver Int2012;32:128-136.
1152 TAYLOR ET AL. HEPATOLOGY, March 2013
Related Documents











