Circles of Care III Bidders Meeting Systems of Care for Native American Youth Day 1 January 2005

Circles of Care III Bidders Meeting Systems of Care for Native American Youth Day 1 January 2005.
Dec 27, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Circles of Care III Bidders Meeting
Systems of Care for Native American Youth
Day 1
January 2005
Welcome and Introductions
• National Indian Child Welfare Association– Staff members and consultants
• Circles of Care Evaluation and Technical Assistance Center– Staff members and consultants
• Center for Mental Health Services– Project Officer
• Participants/Prospective Bidders

Overview of Agenda
• Understanding Circles of Care
• Basics of the Funding Opportunity
• Working Sessions– Nuts and Bolts of the application– Logic Models and strategic planning– Developing your Project Narrative
• Optional consultation sessions
Meeting Goals and Process
• Primary Goal: assist participants in developing a strong proposal and application for the Circles of Care grant program
• Secondary Goal: increase participants awareness of the systems of care approach to community development and evaluation that can be used in a variety of future local initiatives
• Process:– Facilitated working group sessions– Individual consultation– Electronic resource material

Background and History of the Circles of Care Initiative
Jill Erickson, MSWCMHS Project Officer
CIRCLES OF CARE IIISM 05-008
• Tribal Infrastructure Grants for Transforming Behavioral Health Systems for American Indian and Alaska Native (AI/AN) Children and their Families
• Standard Grant Announcement, Infrastructure Grants-INF 05 PA
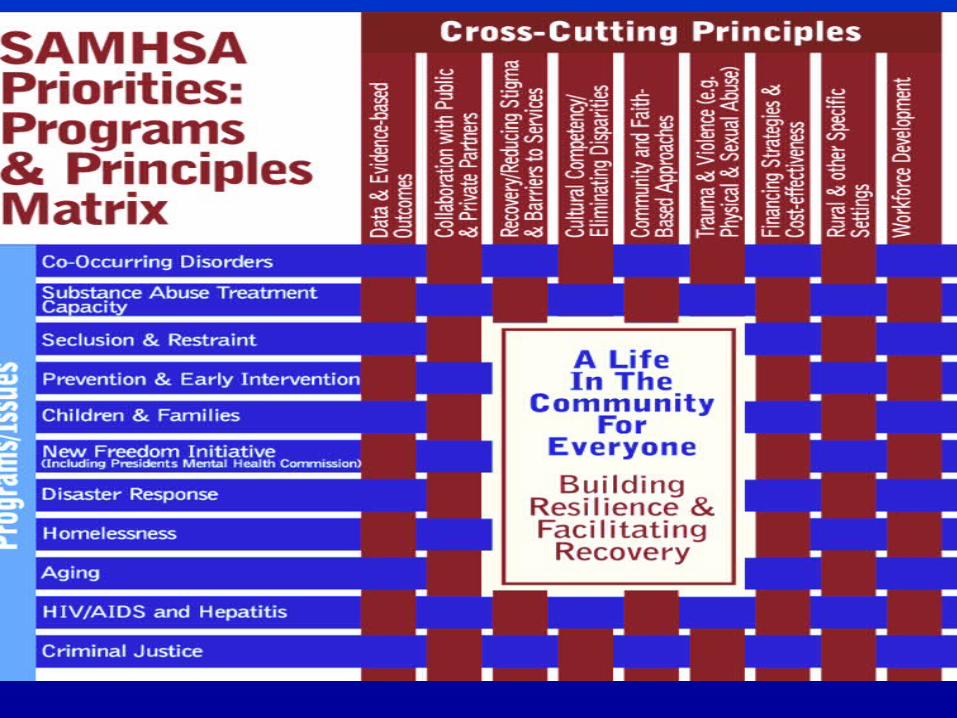

New Freedom Commission: Transforming Mental Health Care in America
• Americans understand that MH care is essential for all overall health
• MH is consumer and family driven
• Disparities in MH care are eliminated, cultural and rural/remote
• Early MH screening, assessment and referral: common practice
• Excellent MH care is delivered and research is accelerated
• Technology is used to access MH care and information.
Goals, Circles of Care
• To develop system of care models designed by AI/AN community members, in partnership with program and evaluation staff.
• To engage community in assessing service system needs, gaps, potential resources, and plans .
• To include special emphasis on mental health/substance abuse.
• To increase system response and options based on values of community served
• To evaluate the feasibility per available resources.
• To support Healthy People 2010 goals: reduce suicides, increase access to treatment
History of the Initiative
• CASSP grants to States 1984, to plan a system of care, excluded Tribes
• OTA Report of 1990, found only 17 child trained MH providers for total Tribal population.
• 1992+ Series of meetings, SAMHSA, Indian Health Service, other federal agencies, providers, and Tribal leaders to address disparities.
• Circles of Care I awarded in 1998, followed by Circles of Care II in 2001.

ELIGIBILITY, Circles of Care
• Tribal Governments, Federally Recognized, as defined by PL 93-638
• Urban Indian Programs, as defined by PL 94-437
• Tribal Colleges and Universities (TCU), added in 2004
• Previous Grantees not Eligible.

Award Information
• $2.4 Million for 7-9 awards.• Average annual award, $250k to $350k• Awards may be requested up to 3 years, depending on
availability of funds• Cost sharing/match is not required.• Technical assistance provided on-site and in grantee
meetings

Circles of Care I Grantees(1998-2001 Projects)
• Cheyenne River Sioux Tribe – SD• Feather River Tribal Health - CA• Shared Vision Project - MT• First Nations Community Healthsource – NM• Oglala Sioux Tribe – SD• Choctaw Nation of Oklahoma• Urban Indian Health Board – Oakland, CA• Fairbanks Native Association- AK• Inter-Tribal Council of Michigan

Circles of Care II Grantees(2001-2004 Projects)
• Tlingit and Haida Tribes - AK• Pascua Yaqui Tribe - AZ• Salt River Pima-Maricopa Indian Community - AZ• United American Indian Involvement - CA• Blackfeet Indian Tribe - MT• Ute Indian Tribe - UT• Puyallup Tribal Health Authority - WA

Technical Assistance
• National Indian Child Welfare Association, Program Technical Assistance, (IAA, IHS)
• National Center for American Indian and Alaska Native Mental Health Research, (IAA, NIMH)

Tribal Consultation
• E.O. 13175, DHHS Policy on Tribal Consultation. SAMHSA participates in regional meetings with other agencies and tribes.
• Circles of Care was developed over 5 year period, beginning with exploratory meeting at the National Indian Health Board.
• An advisory committee of tribal leaders and providers in the field developed the concept for the grants.
Special Journal Edition, U of CO
• American Indian and Alaska Native Mental Health Research, V.11, #2, 2004
• Circles of Care I, outcomes
• http://uchsc.edu/ai/ncaianmhr/journal/11(2).pdf
Circles III, New Announcement
• Announced December 16, 2004
• Due date: February 25, 2005
• Notification planned to all tribal programs, urban Indian programs, TCU’s
• TA for prospective applicants, January 2005
• www.samhsa.gov
SAMHSA - New Address
• 1 Choke Cherry Road, Rockville MD, 20857– Center for Mental Health Services– Center for Substance Abuse Treatment– Center for Substance Abuse Prevention
• (240) 276-1926

Systems of Care Philosophy:A Native Perspective on the National
Initiative
Andy Hunt, MSWNICWA
Director of Community Development for Children’s Mental Health

System of Care Principles
• Family Focused• Culturally Competent• Community Based• Accessible• Individualized• Least Restrictive• Accountable• Interagency• Coordinated & Collaborative
Family Focused
• Not about only children
• Not about only parenting
• “Family” is defined by the community
• Families are involved as key partners at every level of the system, from direct service to policy and evaluation
Cultural Competence
1. Awareness and acceptance of difference
2. Awareness of own cultural values
3. Understanding the “dynamics of difference”
4. Development of cultural knowledge
5. Ability to adapt practice to fit the cultural context of the client/family

Cultural Competence
• At the system level…
“A set of congruent behaviors, attitudes, [practices] and policies that come together in a system, or agency…and enable that system, or agency… to work effectively in cross-cultural situations”.
(Cross, et. al)

Community-Based
• Children should be served in their own community by people from the community
• The community should shape and drive the design of the system
• The system should reflect the values of the local community
• Community members should remain an integral part of the service delivery and planning process

Accessible
• Children and families should be able to get all necessary services with ease
• Elimination of barriers to service:– Physical/Geographic Location– Policy, Procedures and Processes– Language and culture– Stigma and perceptions– Funding restrictions
Individualized Care
• Assessments that are based on discovering the strengths of each child
• A “plan of care” that is truly unique to meet the needs of each individual child
• A wraparound approach that respects individuals
• Services are flexible and adapted to the family

Least Restrictive
• Children should remain in their own homes and communities or in the most home-like setting possible
• Creativity is needed to develop alternatives to more restrictive service models and keep children in their own communities
• Group residential treatment should be avoided unless clinically indicated

Accountable
• Everyone in the system is answerable to each other to meet the needs of the children being served– The system to the community members
– The system to the funding source
– Service providers to the families
– Service providers to their supervisors
– Partners agencies to each other
– Standards of practice and ethics

Interagency
• Systems of care involve multiple agencies to meet the multiple needs of children and families
• Interagency agreements are formalized
• New partnerships are sought out
• Care is taken to build relationships between agencies at service level, and leadership level

Coordinated and Collaborative
• Agencies and other partner organizations work together cooperatively towards the same goals
• Each agency, partner and stakeholder has input and offers resources to meet the community’s goals
• Everyone is on the same page, and everyone knows and understands their role in working together to meet the goals

Partnership in Action:The Indian Children’s Mental Health Initiative
• SAMHSA (CMHS & CSAT)• Indian Health Service (IHS)• Department of Justice (DOJ)• National Indian Child Welfare Association (NICWA)• Circles of Care Evaluation and Technical Assistance
Center (CoCETAC)• American Institutes for Research (AIR)• American Indian/Alaska Native Communities

Systems of CareChildren’s Mental Health Program
• Program funded though CMHS began in early 1990’s for State, Counties, and Cities as 5 year grants
• First Tribe funded in 1994 (Navajo)• Grants extended to 6 years in 2001• US Territories are eligible to apply as of 2003 when
grants became “cooperative agreements”• Plan, design and implement a children’s mental health
system of care• Target population: Children with Severe Emotional
Disturbance and their families
Native CMHS Service Sites(6 Year Implementation Grants)
• Navajo Nation – NM (Graduated 1999)• Passamaquoddy Tribe – ME (Graduated 2003)• Sacred Child Project – ND (Graduated 2003)• Saulte Ste. Marie Chippewa Tribe – MI (Graduated
2004)• Northern Arapaho Tribe – WY (Graduated 2004)• Oglala Sioux Tribe – SD (Year 6)• Yukon Kuskokwim Health Corp. – AK (Year 6)• United Indian Health Services – CA (Year 5.5)

Native CMHS Service Sites(6 Year Cooperative Agreements)
• Fairbanks Native Association – AK (Year 3)
• Choctaw Nation – OK (Year 3)
• Urban Trails Project – CA (Year 2)

Circles of Care Grant Program
• 3 Year grant funded though CMHS • Tribal and Urban Indian programs• Plan, design and assess feasibility of implementing a
culturally appropriate system of care• Target population: American Indian/Alaska Native
children with Severe Emotional Disturbance and their families
• Goal to give grantees opportunity to compete for System of Care implementation grants
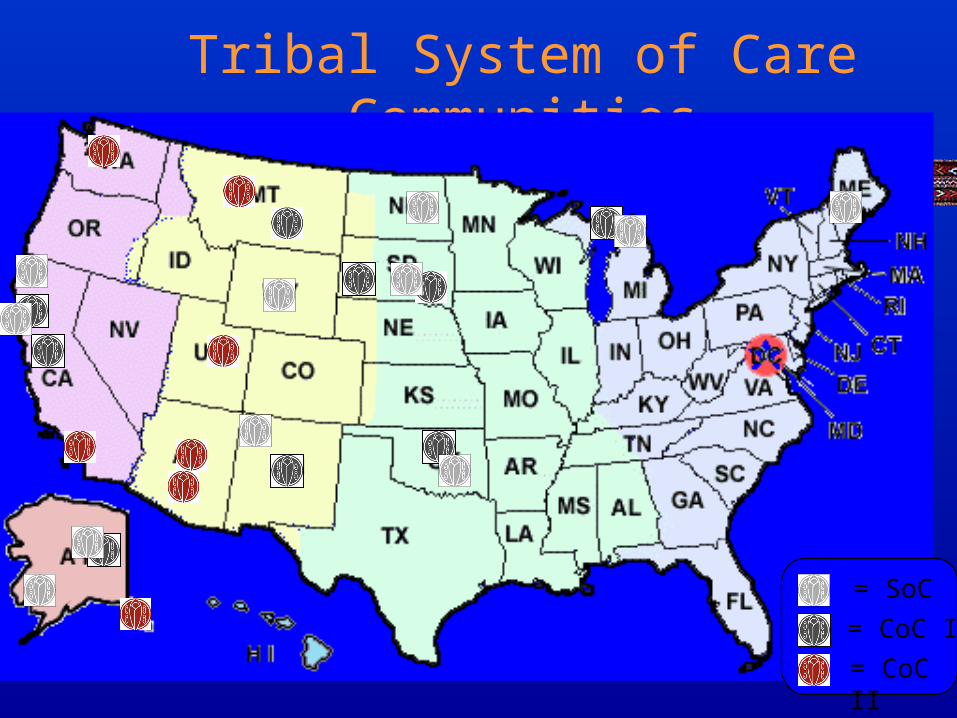
Tribal System of Care Communities
= SoC
= CoC I
= CoC II

For more information visit some of the following websites:
• www.nicwa.org
• www.systemofcare.net
• www.air.org/tapartnership/
• http://mentalhealth.samhsa.gov/cmhs/ChildrensCampaign/default.asp
• http://www.uchsc.edu/ai/coc/


Tribal Perspectives on Wraparound and Community-
Based Strategic Planning
Ethleen Iron Cloud Two Dogs
Oglala Lakota Nation
Annette Squetimkin-Anquoe
Puyallup Tribal Health Authority


Participatory Evaluation
Mary Phillips, BMEFormer Circles of Care Program Coordinator, Oakland and
an Evaluator, Los Angeles, CA

It’s Not Just an Evaluation Methodology
• “We all have a lot in common. We all care very deeply about the communities that we come from and about American Indian and Alaska Native communities across the country. We all share deep concern about the well-being and future of Indian children and families. We are all very self-sacrificing. We are in this business because of our personal beliefs and our desire to make a difference. Our personal backgrounds, our training, our education, and our professional experience all contribute to our desire to make a difference.”
• Holly-Echo Hawk, M.S., Echo Hawk and Associates
It’s Not Just an Evaluation Methodology
• Participation Evaluation is a key component of the systems of care evaluation process that informs the mission, vision and authority of the Tribe/community throughout the Circles of Care program.
• Participation evaluation allows the community to voice its cultural values and promote cultural appropriateness in systems changes development at all levels.
•
It’s Not Just an Evaluation Methodology
• The Circles of Care initiative represented one of the first opportunities for American Indian/Alaska Native AI/AN families and their communities have substantial input into the design of services to address the needs of their children, from their own understanding of these needs.
• The Standard Infrastructure Program Announcement, INF 05 PA and the Circles of Care III NOFA have included community involvement and participation measures that you MUST address throughout the application and are considered in the review process.
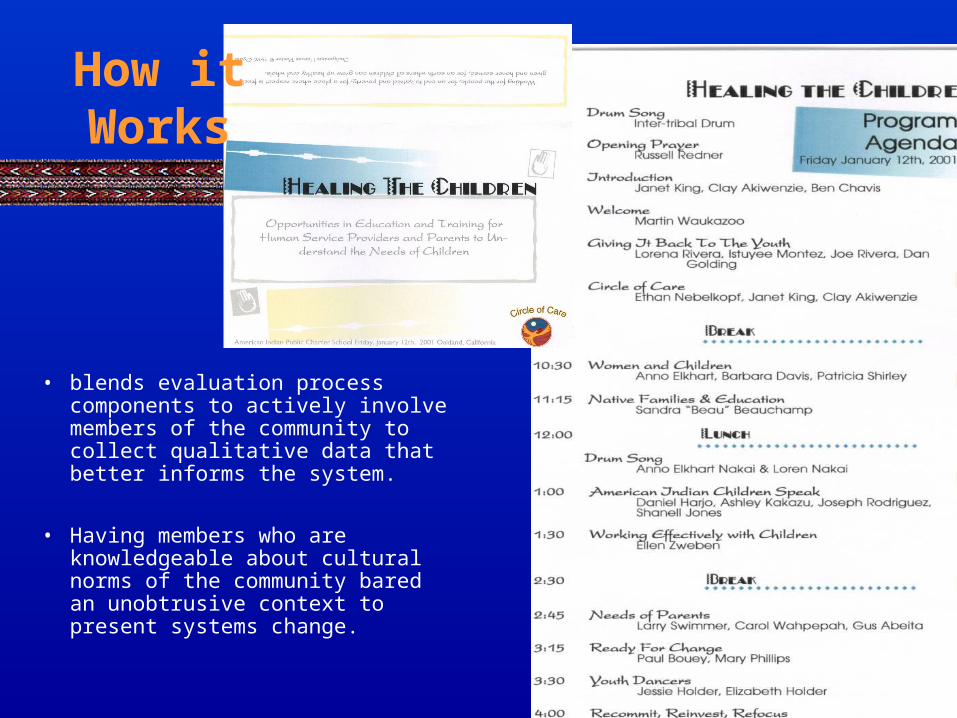
How it Works
• blends evaluation process components to actively involve members of the community to collect qualitative data that better informs the system.
• Having members who are knowledgeable about cultural norms of the community bared an unobtrusive context to present systems change.

The Process of Participatory Evaluation
• Planning the assessment will require a working process between the project staff and evaluation staff and the key informants of each community. Taking into consideration the current status of delivery systems for Native youth and mental health, developing the assessment tool(s) was pivotal in getting necessary information on contextual issues of the system.
• Example: Community Readiness Model was developed at the Tri-Ethnic Center for Prevention Research at Colorado State University to measure systems change in Native American and other communities.

Community Readiness Model
• An innovative methodology to evaluate systems change and focus community efforts toward realizing its objectives. It identifies characteristics related to problem awareness and readiness for change within the community, fostering sound strategic planning, ongoing feedback, and realistic assessments of accomplishments.
Community Readiness Model
• The tool focused on collective information from these Native American resources: 3 community identified leaders, 3 agency directors, 2 cultural advisors, 3 community members and 2 youth group representatives.
• Input from key stakeholders and community members was collected through interview questions related to:– Community Efforts, Knowledge of Efforts, Leadership,
Community Climate, Knowledge About the Issues, Resources for Prevention Efforts.
Community Readiness Model
• The information collected allowed our program to measure where the urban Native American community stands with respect to its knowledge and readiness to implement a specific program (Strategic Plan for Urban Native Americans and their families Oakland, CA

Ongoing Particpation
• The evaluation participation process also incorporated resource development within the community. Linkages were made throughout the project as community coordinators and cultural leaders were provided information on the core elements of the system of care. This process required continuous interaction between agencies and cultural groups that concentrated the efforts to achieve child and adolescent behavior goals among agencies and family empowerment through focus groups.

SYSTEM OF CARE MODEL FOR AMERICAN INDIAN CHILDREN & FAMILIES
ADVISORY BOARD
RECOMMENDATIONS
VISION
COMMUNITY NEEDS ASSECOMMUNITY NEEDS ASSECOMMUNITY NEEDS ASSESSMENT SSMENT SSMENT Circle of Care Evaluation Process Flow
SER
VIC
E
PR
OVID
ER
S
CO
MM
UN
ITY
SURVEY
CIRCLE OF CARE EVALUATION
KEY INFORMANT INTERVIEWS
FOCUS GROUPS
AMERICAN INDIAN COMMUNITY
PRIORITY AREAS
Access
Outreach/Awareness
Family Support Services
Training Cultural Appropriate
Youth Services
Cultural Programs Community
Needs Assessment
Service System
Assessment
YOUTH, PARENTS, SERVICE PROVIDERS
Commitment Ownership Community
Items from Standard Infrastructure Program Announcement and Circles of
Care NOFA
• Respond to each of these required information items with statements to let the reviewer know what work has been done; the work that the program intends to do; and how you will address each issue.
• Though not all requirements listed here are given points, providing this information can help understand the ability of the program to connect and involve the community.
• These should be written in Sections B. Proposed Approach, C. Staff, Management and Relevant Experience, D. Evaluation and Data
Items from Standard Infrastructure Program Announcement and Circles of
Care NOFA
• Program Goals:– Engage their community members in assessing service
system needs, gaps, potential resources, and plan infrastructure development strategies that meet those needs.
– Increase the participation of families, tribal leaders, and spiritual advisors in planning and developing service systems and treatment options based on the values and principles of the AI/AN community served by the project.
– (Circles of Care III NOFA, p.2)

Items from Standard Infrastructure Program Announcement and Circles of
Care NOFA
• Grantees must use funds to carry out the following required activities:– Facilitate culturally respectful strategic planning
activities engaging community members, key stakeholders, youth, elders, spiritual advisors, and tribal leaders to identify outcome expectations and measures; (Circles of Care III NOFA, p.3)

• In “Section D: Evaluation and Data,” add the following bullet:– Describe how project staff will work with evaluation staff to
support the evaluation effort. The program planning activities and the evaluation activities will be expected to inform each other in a constant cycle, locally and collectively. (Circles of Care III NOFA, p.12)
• The Circles of Care process values participatory, community-based outcomes that are reflected heavily in the planning process.
Items from Standard Infrastructure Program Announcement and Circles of Care NOFA
Items from Standard Infrastructure Program Announcement and Circles of
Care NOFA
• Providing a venue for the Tribal/community to receive information and respond to with appropriate audience members can include meetings at all levels within the community.
• Example: Two community-visioning meetings were conducted at 2 separate locations within the community, and were documented based on invited quests, attendance, activities planned to collect feedback, and information passed on to community participants. This type of community visioning planning resulted in setting priority areas to build a Youth Development Facility.
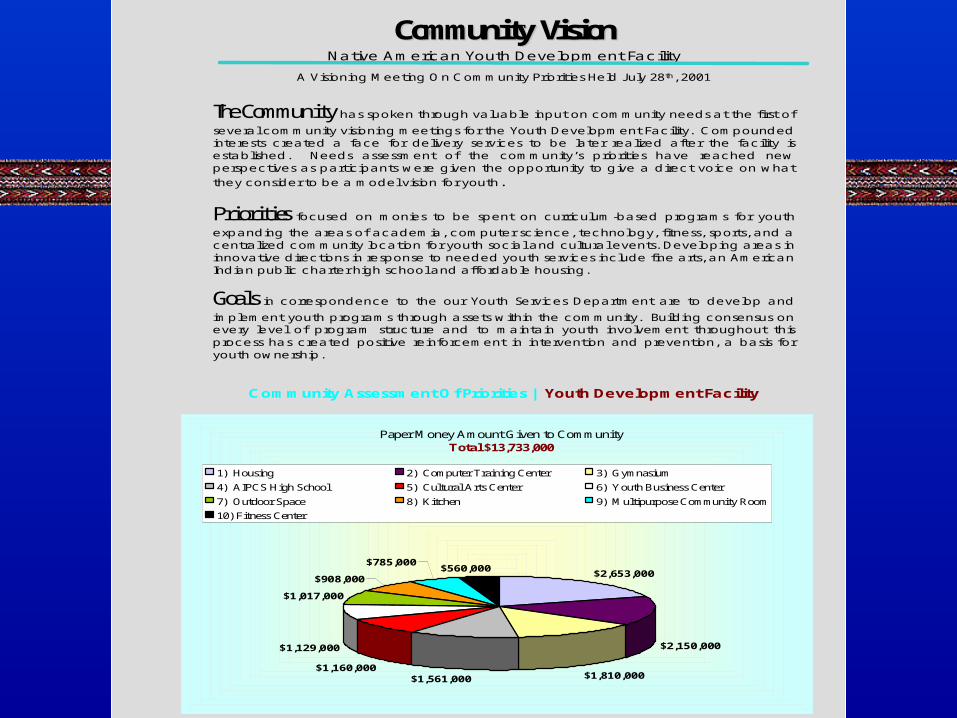
CCoommmmuunniittyy VViissiioonn Native American Youth Development Facility
A Visioning Meeting On Community Priorities Held J uly 28th, 2001
The Community has spoken through valuable input on community needs at the first of
several community visioning meetings for the Youth Development Facility. Compounded interests created a face for delivery services to be later realized after the facility is established. Needs assessment of the community’s priorities have reached new perspectives as participants were given the opportunity to give a direct voice on what they consider to be a model vision for youth.
Priorities focused on monies to be spent on curriculum-based programs for youth
expanding the areas of academia, computer science, technology, fitness, sports, and a centralized community location for youth social and cultural events. Developing areas in innovative directions in response to needed youth services include fine arts, an American Indian public charter high school and affordable housing.
Goals in correspondence to the our Youth Services Department are to develop and
implement youth programs through assets within the community. Building consensus on every level of program structure and to maintain youth involvement throughout this process has created positive reinforcement in intervention and prevention, a basis for youth ownership.
Community Assessment Of Priorities | Youth Development Facility
Paper Money Amount Given to Community Total $13,733,000
$2,653,000
$2,150,000
$1,810,000$1,561,000$1,160,000
$1,129,000
$1,017,000
$908,000
$785,000$560,000
1) Housing 2) Computer Training Center 3) Gymnasium
4) AIPCS High School 5) Cultural Arts Center 6) Youth Business Center
7) Outdoor Space 8) Kitchen 9) Multipurpose Community Room
10) Fitness Center

Participatory Feasibility Assessment
• Complete the feasibility assessment and process evaluation, leading to adoption of the model. (Circles of Care III NOFA, p.4)– Strengthening Tribal capacity for evaluation of service systems
through ongoing involvement with staff and evaluation partners.
– Careful deliberation on setting up effective strategies with an “evaluation team”, to engage all participants that have a stake in the evolution of the infrastructure.
– This integration of tasks contributes to and OPEN style of communication that in turn enhanced the collaboration of evaluation and program staff.
Participatory Evaluation related to President’s New Freedom Commission
Goals
• The agenda of the President’s New Freedom Commission’s Report towards a transformation of mental health systems states:– 2. Mental Health Care is Consumer and Family Driven
• Involve consumers and families fully in orienting the mental health system toward recovery. (Circles of Care III NOFA, p.5)
• The consumer of the community has a voice in the process and is able to tell their story at the point in the process they choose.
• Parents are empowered through ongoing interaction in the process.
Participatory Evaluation related to President’s New Freedom Commission
Goals
• Circles of Care approach emphasizes flexibility as stakeholders shift positions and encourage converge of a the cultural knowledge base within children’s mental health.
• Example: A parent that attends parent focused support groups from the AI/AN clinic and has a child receiving services that is also attending the school in the same community will better inform on how services are impacting the service needs and accessibility.
Participatory Evaluation related to President’s New Freedom Commission
Goals
• The outcome of involving parents can result in a cultural definition of Severely Emotionally Disturbed:
– “Emotional disturbance is a temporary disharmony often involving the family, school, and community, which may affect the mental, physical, spiritual, and/or emotional well being of its members.” Choctaw Nation of Oklahoma, Circles of Care I grantee.

Evaluation to Support Strategic Planning in Indian/Native
Communities
Doug Novins, PhD
Candace Fleming, PhD
The Role of the Evaluation in CoC
• Provide a knowledge base for the planning effort
• Facilitate the process for developing the capacity for ongoing evaluation efforts
• Examine the feasibility of the service system models
• Document and disseminate the results of the initiative

Key Differences:CoC versus Typical Evaluation
• In CoC, evaluation provides important information (“data”) that is used in the planning effort

Refine Service SystemModel
A Typical Evaluation Model for Strategic Planning Efforts
Design Service SystemModel
Assess Service System Model(Feasibility Assessment)
Assess Planning Effort
(Process Evaluation)

Refine Service SystemModel
The Circles of CareEvaluation Model
Design Service SystemModel
Assess Service System Model(Feasibility Assessment)
Assess Planning Effort
(Process Evaluation)
Assess Needs and Existing Services Measure Development
Key Differences:CoC versus Typical Evaluation
• In CoC, evaluation provides important information (“data”) that is used in the planning effort
• In CoC, the evaluator is a full participant in the planning effort, and not an outside “objective” observer

A Typical Evaluation Model for Strategic Planning Efforts
ProgramStaff
Evaluator
The Circles of CareEvaluation Model
ProgramStaff
Evaluator
The Circles of CareEvaluation Model
Program&
EvaluationTeam
Key Differences:CoC versus Typical Evaluation
• In CoC, evaluation provides important information (“data”) that is used in the planning effort
• In CoC, the evaluator is a full participant in the planning effort, and not an outside “objective” observer
• In CoC, the community is an active participant in designing and implementing the evaluation plan, not simply the “target” of evaluation activities
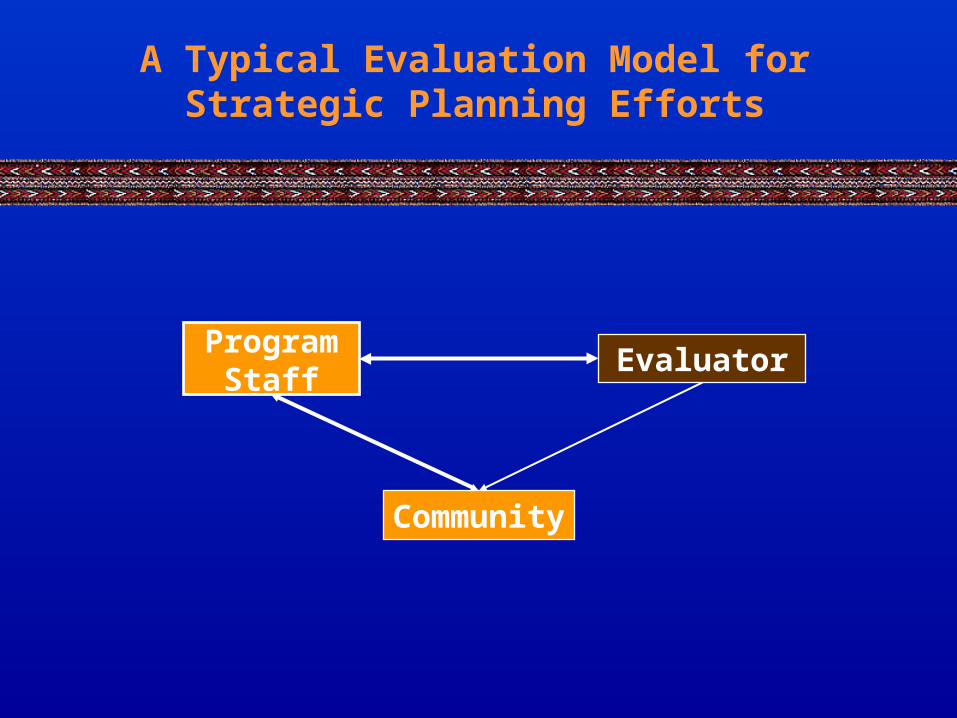
A Typical Evaluation Model for Strategic Planning Efforts
ProgramStaff
Evaluator
Community

The Circles of CareEvaluation Model
Program&
EvaluationTeam
Community

The Circles of CareEvaluation Model
Program&
EvaluationTeam
Community

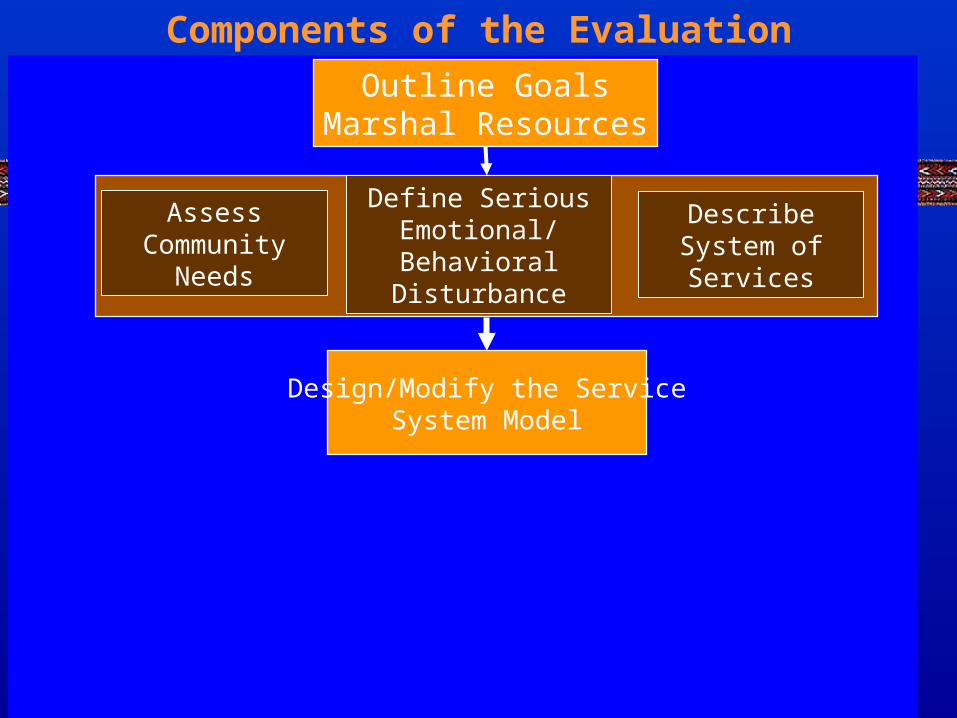
Components of the Evaluation
Outline GoalsMarshal Resources

Components of the Evaluation
Define SeriousEmotional/Behavioral
Disturbance
AssessCommunity
Needs
DescribeSystem ofServices
Outline GoalsMarshal Resources
Components of the Evaluation
Design/Modify the ServiceSystem Model
Define SeriousEmotional/Behavioral
Disturbance
AssessCommunity
Needs
DescribeSystem ofServices
Outline GoalsMarshal Resources

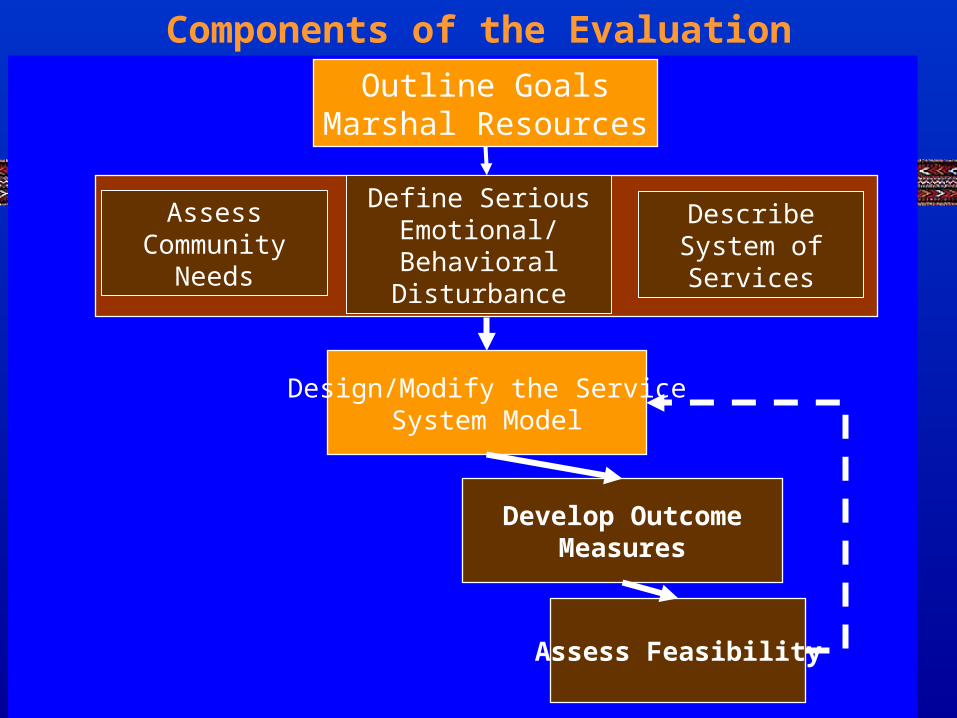
Components of the Evaluation
Design/Modify the ServiceSystem Model
Develop OutcomeMeasures
Define SeriousEmotional/Behavioral
Disturbance
AssessCommunity
Needs
DescribeSystem ofServices
Outline GoalsMarshal Resources
Components of the Evaluation
Design/Modify the ServiceSystem Model
Develop OutcomeMeasures
Assess Feasibility
Define SeriousEmotional/Behavioral
Disturbance
AssessCommunity
Needs
DescribeSystem ofServices
Outline GoalsMarshal Resources

Components of the Evaluation
Design/Modify the ServiceSystem Model
Develop OutcomeMeasures
Assess Feasibility
Assess Planning Effort(Process Evaluation)
Define SeriousEmotional/Behavioral
Disturbance
AssessCommunity
Needs
DescribeSystem ofServices
Outline GoalsMarshal Resources
Our Role and Mandate
• To provide a clear framework for the grantees to use in designing their evaluation efforts
• To allow the grantees to design an evaluation effort that is most consistent with the priorities of their communities.
• To facilitate a process for identifying common domains for each of the evaluation components.
Our Role and Mandate
• To provide a clear delineation of CoCETAC and grantee roles and responsibilities in the evaluation effort.
• To provide consistently high quality technical assistance through a specific set of activities.
CoCETAC Technical Assistance Activities
• Grantee Meetings• Evaluator Meetings• Site Visits• Scheduled Technical Assistance Conference Calls• Ad Hoc Conference Calls and Email Exchanges• Detailed Reviews and Critiques of Evaluation Reports• Maintain World Wide Web Site• CoC Distribution List

Grantees Role and Mandate
• Development of site specific domains, constructs, and measures
• Obtain necessary IRB and other research approvals• Data collection, reduction, and analysis• Provide site-specific content to CoCETAC website• The writing and submission of local interim and final
reports.
AIANP Resourceson the World Wide Web
• AIANP– http://www.uchsc.edu/ai
• CoCETAC:– http://www.uchsc.edu/ai/coc
• NCAIANMHR– http://www.uchsc.edu/ai/ncaianmhr
• The Healthy Nations Initiative– http://www.uchsc.edu/ai/hni
Former Circle of Care Grantee Experiences
Ethleen Iron Cloud Two Dogs
Oglala Lakota Nation
Annette Squetimkin-Anquoe
Puyallup Tribal Health Authority


Cultural Collaboration: The Evaluators’ Role
Brenda Freeman, Ph.D.
Kenneth Coll, Ph.D
Friere on Oppression
• Domination, aggression and violence are an intrinsic part of human and social life. Few human encounters are exempt from oppression of one kind or another because by virtue of race, class, or gender, people tend to be victims and/or perpetrators of oppression.
People’s knowledge/expert knowledge
•O Officially sanctioned knowledge•K Knowledge pipeline – reversing the flow• “We should not be objects of observation for those who do nothing to help us.” (Vine Deloria, Jr.)•G Massacres, history as the tale of the victors
Question 1
In what ways might an evaluator contribute to oppression?

Cultural Challenges to Evaluators
• “Status” • “Expertness” • Privilege• “Proceeding in the right way”• Paternalism (the culture of the project is not
authenticated)• Being seen as an “Indian agent” for the
government (historical mistrust)
Cultural Challenges to the Project
• Dealing with the two-sided issue of “unequal credentials”
• Example: a Ph.D.(“western education”) vs. indigenous/traditional knowledge

Question 2
How does the evaluator interface with project staff?
Participatory Research (PAR) Model
– Community ownership and leadership of the evaluation process (e.g., survey design, methodology, data analysis and results dissemination).
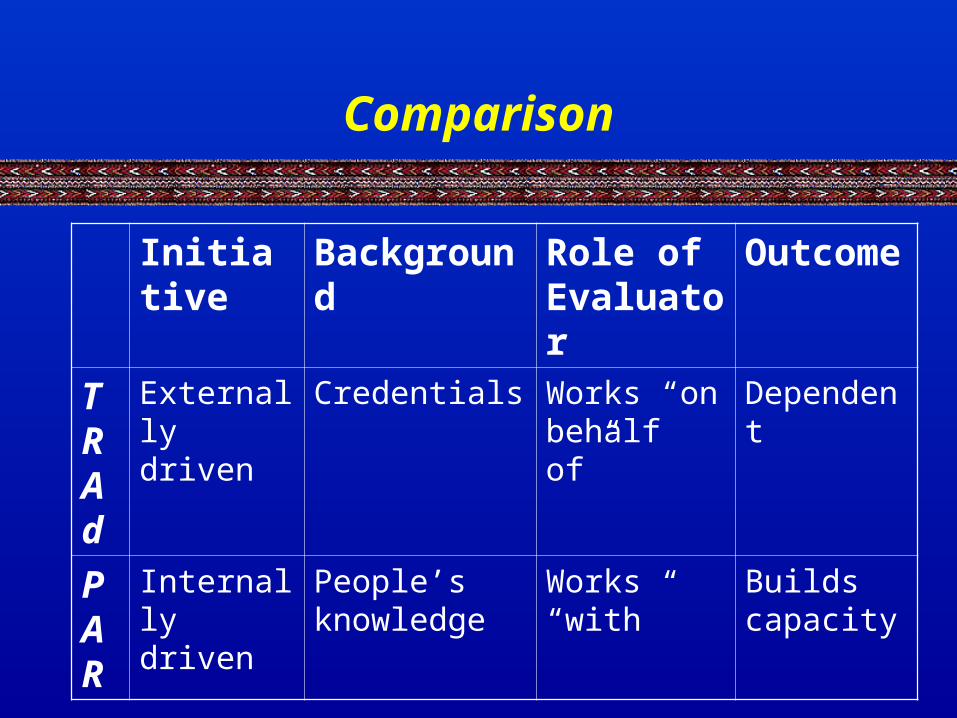
Comparison
Initiative Background Role of Evaluator
Outcome
TRAd
Externally driven
Credentials Works “on behalf of”
Dependent
PAR
Internally driven
People’s knowledge
Works “with” Builds capacity
Question 3
• What evaluator attitudes and behaviors promote project success?
Collaborative Goals
• Evaluator:– A mirror– Part of the circle– As a “passenger, not the driver”– With and for – not on behalf of– A tool, and an equal– Values the culture, not overwhelms it

Question 4
• How does the culture of the staff fit with the characteristics of the evaluator?
Screening suggestions for selecting evaluators
• Develop a culturally appropriate screening method
• Screen for:– Authenticity– Genuineness, respectfulness– Identity Achievement
Process after selection
• Orientation
• Community acceptance through on-going interaction with community members on a “human” level

Nagi Kicopi’s Culturally Collaborative Practice
• Inipi
• Local site sets the agenda
• Cultural Trainings
• Evaluation Trainings
• Community ownership
• Following cultural protocol
Review of NOFA RequirementsCircles of Care and Standard
Infrastructure Grants
Jill Shepard Erickson, MSW
Project Officer
Center for Mental Health Services
Application Review Information
Page 21, Infrastructure Grants
Page11, Circles of Care
Section A: Statement of Need, 10 points
• Describe target population, numbers, language, culture, geography, and socioeconomic factors
• Document the need, tribal, state, SAMHSA data. • Describe service gaps, barriers
– Describe stakeholders and resources– Identify initiatives funded by Indian Health Service,
Department of Justice, other SAMHSA grants, etc.– Describe how initiatives will be coordinated
• Describe needs related to priorities of state, county, or tribe. (Copies of strategic plans in Appendix 5)

Section B: Proposed Approach35 Points
• State purpose with goals, objectives per NOFA and community
• Describe proposed project• Provide logic model• Describe advisory body• Describe partner organizations, (letters of commitment
in Appendix 1)– Describe and include community schools and tribal college if
available
Section B continued
• Describe how age, race/ethnicity, culture, language, sexual orientation, disability, and gender will be addressed
• Describe how members of the target population have been and will be involved in proposal
• Describe potential barriers• Describe how activities will improve substance abuse
prevention and treatment and/or treatment of mental health services
• Provide a plan for sustainability

Section C: Staff, Management, Relevant Experience - 25 points
• Time line on chart or graph, (include within narrative)• Capability and experience with target population• List staff and roles each will play• Describe racial/ethnic and linguistic characteristics of
staff, re target population• Describe resources, facilities
Section D: Evaluation and Data30 points
• Describe the process and outcome evaluation, performance measures and target outcomes re goals and objectives
• Describe ability to collect and report required performance measures per NOFA
• Describe plans for data collection, management, analysis, interpretation and reporting (instruments in Appendix 2)
• Describe reliability and validity of evaluation methods and instruments per gender/age/culture of target population
• Describe how collection, analysis, and reporting of data will be integrated• Describe how project staff will work with evaluation staff to support the
evaluation effort, informing each other in a constant cycle, locally and collectively

Evaluation and Data #2GPRA Measures (Preliminary)
Document plan for collecting and reporting:
1. Involvement of community leaders, consumers and families in planning, policy development and strategy for treatment planning implementation in: – quarterly reports
– Completion of cross-site evaluation tasks
– Minutes from community planning meetings
Evaluation and Data #3GPRA Data
2. Plan for documenting improved access to quality care for AI/AN children, youth and families of community, examples include:– New sources of funding– Increased use of telemedicine, telepsychiatry
Evaluation and Data #4GPRA Measures
3. Adherence to the TA guidance provided
– Products developed– Timely completion of phases of activities– Feedback on satisfaction with TA provided
Individual clinical/patient data will not be collected
SAMHSA Standard Grant Announcements and NOFA’s
Basics of the Funding Opportunity
FY 2005
Jill Erickson, CMHS Project Officer

Four Standard Grant Announcements
1. Infrastructure: Increase capacity of service systems to support effective programs and services
2. Services: Funding to implement services3. Best Practices Planning and Implementation: ID
practices and adapt for pilot-testing4. Service to Science: Document and evaluate
innovative practices to fill gaps, not yet formally evaluated.

Notice of Funding Availability (NOFA/Circles of Care)
• Used in addition to a Standard Grant Announcement• Specifies purpose, target population, issue area, and
other requirements of the program• Identifies funding, expected size and number of awards• Provides deadline• Specifies eligibility, allowable activities,
evaluation/GPRA requirements.

Application and Submission
• Call for kit to be mailed, – Mental Health: 1-800-798-2647 – Substance Abuse: 1-800-729-6686
• Download from www.samhsa.gov, “grant opportunities”
• Download from www.grants.gov.
Infrastructure Grants, Basic Expectations
• Allowable Activities
• Data and Performance Measurement: Government Performance and Results Act of 1993, GPRA
• Grantee Meetings
• Evaluation

Application Requirements
• Application Kits contain the following and must be used:– PHS 5161-1 Application forms: face page, budget
forms, assurances, certification, and checklist– Program Announcement (PA)– Notice of Funding Availability (NOFA), as
published in the Federal Register, www.samhsa.gov, and www.grants.gov .
Required Components
• Face Page: SF 424, part of PHS 5161-1. – Including a Dun and Bradstreet (DUNS) number, obtainable
from www.dunandbradstreet.com, or 1-866-705-5711
• Abstract: 35 lines maximum, used in publications.• Table of Contents• Budget Form: SF 424A• Project Narrative and Supporting Documentation• Appendices• Assurances, Certifications, Disclosure of Lobbying, and
Checklist
Application Formatting Requirements
• Non compliance results in proposal being screened out prior to review:– Type size in narrative cannot exceed an average of
15 characters per inch. (excludes type size within charts, graphs, footnotes)
– Text cannot exceed 6 lines per vertical inch– White paper, 8.5inch by 11.0 inch– Margins at least 1 inch– 25 page limit for narrative.
Formatting Recommendations
• Type single space in black ink, one column per page• Number pages including cover page #1, Abstract #2,
Table of Contents through the Appendices.• 30 page limit for Appendices• Send original and 2 copies to mailing address in
Section IV-6.1. • No staples, paper clips, fasteners, heavy papers,
posters, CD-ROM’s, etc. • Proposal must be easily copied.
Electronic Submission Option
• Use the www.grants.gov apply site• Find application package by CFDA #• Download copy of application package,
complete off line• Submit via www.grants.gov, e-mail submissions
not accepted.• Use Microsoft, font Times New Roman 12, or
PDF files.
Prior Requirements for Electronic Submission (allow 2 wks+)
• Obtain DUNS number• Obtain Central Contractor Registry (CCR)• Obtain Credential Provider registration• Obtain Grants.gov registration• User guide available at www.grants.gov, • Or e-mail: [email protected]• Or call 1-800- 518-4726, 7:00 am-9:00 pm, Eastern,
Monday through Friday.
Back Up Paper Submission
• Label as “Back up for electronic submission”• Paper copy must meet “postmark” requirements• If both received, electronic version will be official• Automatic acknowledgement from Grants.gov with
Grants.gov tracking number• Electronic signatures cannot be accepted now, so
signed paper originals of face page, assurances, and certifications must be mailed, referencing the grants.gov tracking number, within 5 business days of the electronic submission.
Budget Form
• SF 424A, from the 5161-1
• Fill out Sections B, C, E.
• Follow the sample budget and justification from Appendix D of Standard Announcement
• Include figures for each year of the grant
• Total budget will include direct cost and negotiated indirect cost rate.

SAMHSA’s Guidelines for Assessing Cultural Competence
• Experience with the target population
• Training and staffing, gender/age/cultural competence
• Language accommodations
• Materials appropriate for target population
• Evaluation, methods and instruments appropriate for population
• Community representation on boards
• Plan for implementation

Part II
• General Policies and Procedures Applicable to all SAMHSA Applications for Discretionary Grants and Cooperative Agreements.
• Used in addition to the Program Announcement/NOFA and Standard Grant Announcement
• Contains the Cultural Competence

Confidentiality, Participant Protection, Human Subjects
Mary Phillips, M.A.
Kenneth M. Coll, Ph.D.
Brenda Freeman, Ph.D.
Part of Section D of the NOFA: Evaluation and Data
• “Applicants must document their ability to collect and report required data”, including:– Evidence of involving community key informants
(e.g., families, leaders) in the process

Such Involvement will include
• Descriptions of Plans for:– Data Collection – Data Management and Analysis– Data Reporting– Existing Approach to the collection of data
Data Collection
• Confidentiality and Participant Protection (of Human Subjects) through:– Informed consent from the Participant, including:
• Purpose and background• Procedures for collecting the data• Description of risks/discomforts• Benefits• Costs• Payments• Questions • Voluntary consent (signed)• Participant Bill of Rights (Safety Monitoring Plan)

Data Management and Analysis
• Confidentiality and Participant Protection (of Human Subjects) through– Data entry person(s) signs a confidentiality
statement– Works from a secure location and computer– Trains in HIPPA guidelines– Enters data without identifying information (e.g,
names, other identifications)
Continued
• Confidentiality and Participant Protection (of Human Subjects) through– Securely storing raw data in a locked file cabinet for
a specified period of time then shredded
Continued- Inclusion of Children
• Informed consent is needed from both the youth (if at an age of understanding) and the caregiver(s)
• SEE EXAMPLE
Data Reporting
• To Whom?– Key informants (e.g., families, community leaders and
members, service providers)
• How often?– Monthly
– Quarterly
– Semi-annually
• In what formats, venues?– e.g., Radio, newspaper, executive summaries, newsletters

Existing Approach to the Collection of Data
• Description of Current Management Information System
Data Collection Instruments/Interview Protocols?
• See examples
• Reliability and validity of evaluation methods and instruments in terms of gender/age/culture of the target population– Community based-committee in development stage– Focus groups– Piloting

An Introduction to Logic Models
Kenneth Coll, Ph.D. and Brenda Freeman, Ph.D.
A Circles of Care Planning Logic Model
• A road map (or picture) of the planning process for your program, highlighting overall how you plan to go about the planning process, including:– Some of the beliefs (conditions, assumptions, or background
factors) that will drive the planning process in your community– The goals of the planning process (hoped for outcomes)– Examples of the planning activities your community might engage
in to reach the goals – The participants involved in the planning process – Desired overall impact of the planning process itself
(adapted from W.K. Kellogg Foundation)
Definition of a Logic Model
• SAMHSA Infrastructure Grant Glossary:– “A logic model is a diagrammatic representation of a
theoretical framework. A logic model describes the logical linkages among program resources, conditions, strategies, short-term outcomes, and long-term impact.”
– Logic Model Should Include:• Identified need
• Proposed approach
• Outcomes

Logic Model for Circles of Care
• A visual representation of answers to these questions…1. Based upon information gathered from other projects or
what you know from experience, what are some of the needs of your community related to mental health and related services for troubled youth and their families? (Needs)
2. Keeping those needs from #1 in mind, at the end of the three year planning process what is your overall dream related to the planning of services for children and families? (Impact)
Logic Model Planning Questions
3. What concrete changes will need to occur in the community related to the planning of mental health services for children and families in order to reach your dream? (Outcomes)
4. What are you going to do to bring about the changes that are part of, or the result of, the planning process? (Proposed Approach)
Logic Model Planning Questions
5. What groups would be impacted by changes in the delivery system for mental health and related fields? (Participants in the Planning Process)
6. How will others—and you--know if the outcomes in #3 above are being reached? (Measures)
7. Why do you believe the activities (#4 above) will lead toward the outcomes (#3 above) you hope to accomplish? (Change Theory)

Visual of a Logic Model
Goals Activities Outcome
Activities
Activities
Activities
Outcome
Outcome
Outcome
Goal
Impact
Needs MeasuresAssumptions About Change

Planning Form for a Circles of Care Logic Model
Needs of Community Related to
MH & Related
Services for Children &
Families
Impact
What you hope to have accomplished at the end of the project.
Desired Outcomes
(more specific than
impact)
Proposed Approach
(Activities that will lead
to the outcomes)
Strategies If---Then Assumptions &Theory of
Why Change Will Occur

Day 1 Wrap up
• Understanding Circles of Care
• The Basics of the Funding Opportunity
• Working Session on Developing a Logic Model
• Have a nice evening – see you in the morning!
Related Documents











