CINERADIOGRAPHIC ASSESSMENT OF COMBINED ISLAND FLAP PUSHBACK AND PHARYNGEAL FLAP IN THE SURGICAL MANAGEMENT OF SUBMUCOUS CLEFT PALATE 1 By JOHN E. HOOPES,M.D., z A. LEE DELLON, 3 JACOB I. FABRIKANT, M.D., and ANN H. SOLIMAN From the Division of Plastic Surgery, the Department of Radiology, and the Division of Otolaryngology, The Johns Hopkins Hospital and The Johns Hopkins University School of Medicine, Baltimore, Maryland. OBJECTIVE methods of pre- and post-operative evaluation are essential for assessment of the numerous surgical procedures available for correction of velopharyngeal incompetence and cineradiographic investigation of the velopharynx has proved of clinical value for this purpose. It allows : I. Elucidation of the functional anatomy and pathophysiology of the velopharynx. 2. Precise diagnosis of the discrete anatomical factors responsible for velopharyngeal incompetence. 3. Accurate measurement of the anatomical modifications achieved surgically. 4. Estimation of prognosis. ANTERIOR POSTERIOR NASAL SPINE NASAL SPINE "~o ~ ~ POSTERIOR PHARYNGEAL LEVATOR WALL EMINENCE UVULA-...~ FIG. I Tracing obtained on the basis of frame-by-frame analysis demonstrating the anatomical reference points and the arc traversed by the levator eminence. Material and Method.--Four patients with hypernasal speech secondary to submucous cleft palate provided the basis for this investigation. A combined island flap pushback and pharyngeal flap was performed in each patient by the same surgeon using the same technique. Two additional patients were studied cineradiographically and received the operative procedure but subsequently were lost to follow-up evaluation. The technique and instrumentation for cineradiographic evaluation of the vocal tract with synchronous sound recording has been described in detail (Hoopes and Fabrikant, 1968), and a method of frame-by-frame analysis correlating objectively measur- able anatomical parameters with subjective evaluation of speech has been presented i This work is supported in part by the United States Public Health Service Grant No. 5 ToI GM o1328-o4 and by a gift from the Robert Garrett Foundation. Plastic Surgeon-in-Chief, The Barnes and Allied Hospitals and The St Louis Children's Hospital, The Washington University School of Medicine, St Louis, Missouri 631 IO. 3 Henry Strong Denison Scholar for 1968-1969. 39

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
CINERADIOGRAPHIC A S S E S S M E N T OF C O M B I N E D ISLAND FLAP P U S H B A C K A N D P H A R Y N G E A L FLAP IN THE SURGICAL
M A N A G E M E N T OF S U B M U C O U S CLEFT PALATE 1
By JOHN E. HOOPES, M.D., z A. LEE DELLON, 3 JACOB I. FABRIKANT, M.D., and ANN H. SOLIMAN
From the Division of Plastic Surgery, the Department of Radiology, and the Division of Otolaryngology, The Johns Hopkins Hospital and The Johns Hopkins University School of
Medicine, Baltimore, Maryland.
OBJECTIVE methods of pre- and post-operative evaluation are essential for assessment of the numerous surgical procedures available for correction of velopharyngeal incompetence and cineradiographic investigation of the velopharynx has proved of clinical value for this purpose. It allows :
I. Elucidation of the functional anatomy and pathophysiology of the velopharynx. 2. Precise diagnosis of the discrete anatomical factors responsible for velopharyngeal
incompetence. 3. Accurate measurement of the anatomical modifications achieved surgically. 4. Estimation of prognosis.
ANTERIOR POSTERIOR
NASAL SPINE NASAL SPINE
" ~ o ~ ~ POSTERIOR
PHARYNGEAL LEVATOR WALL EMINENCE
UVULA-...~ FIG. I
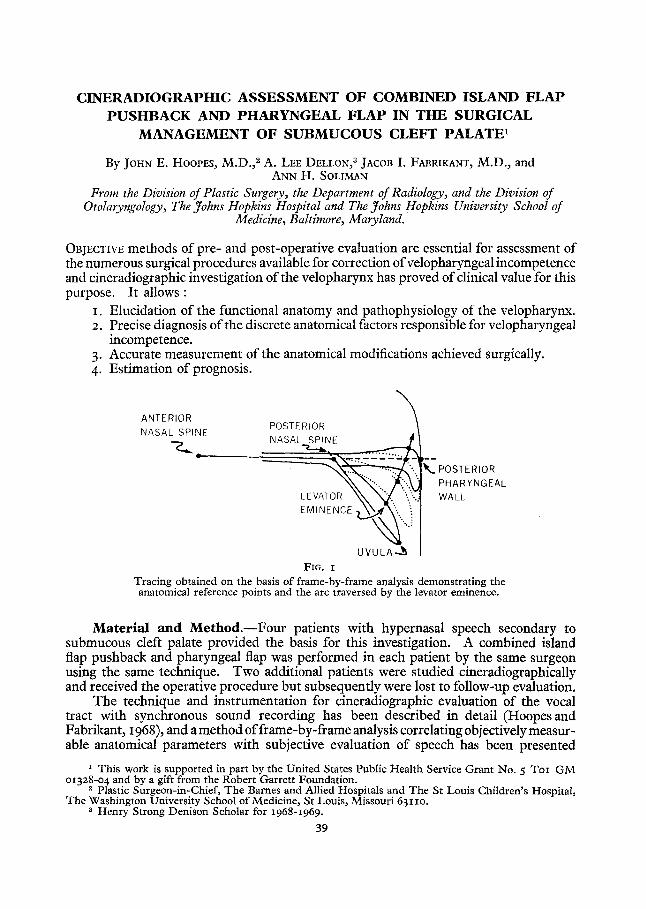
Tracing obtained on the basis of frame-by-frame analysis demonstrating the anatomical reference points and the arc traversed by the levator eminence.
Materia l and Method.- -Four patients with hypernasal speech secondary to submucous cleft palate provided the basis for this investigation. A combined island flap pushback and pharyngeal flap was performed in each patient by the same surgeon using the same technique. Two additional patients were studied cineradiographically and received the operative procedure but subsequently were lost to follow-up evaluation.
The technique and instrumentation for cineradiographic evaluation of the vocal tract with synchronous sound recording has been described in detail (Hoopes and Fabrikant, 1968), and a method of frame-by-frame analysis correlating objectively measur- able anatomical parameters with subjective evaluation of speech has been presented
i This work is supported in part by the United States Public Health Service Grant No. 5 ToI G M o1328-o4 and by a gift from the Robert Garret t Foundation.
Plastic Surgeon-in-Chief, The Barnes and Allied Hospitals and The St Louis Children's Hospital, The Washington University School of Medicine, St Louis, Missouri 631 IO.
3 Henry Strong Denison Scholar for 1968-1969.
39
4o B R I T I S H JOURNAL OF PLASTIC SURGERY
(Hoopes et al., I968a, b). The following reference points serve as the basis for analysis (Fig. I ) :
ANS and PNS : The anterior and posterior nasal spines. The plane of the hard palate is represented by a straight line connecting the points .4NS and PNS.
PPW : The posterior pharyngeal wall at the point intersected by the plane of the hard palate.
U : The position of the uvular tip at rest. Levator Eminence : The midpoint on the convexity (" knee ") of the ~.sal surface
of the soft palate during movement. LE : The point at which the arc traversed by the levator eminence during closure
intersects the plane of the hard palate. Levator Insertion : The distance PNS-LE ; the smaller this measurement, the more
anterior the levator insertion.
The following data are derived from the cineradiographic tracing : Relative Length of Soft Palate : The ratio of the length of the soft palate to the depth
of the nasopharynx, viz., PNS-U/PNS-PBW. A functional measurement of soft palate length such that the value is greater than unity (I-OO) indicates a velum having the capacity to achieve closure.
Relative Depth of Nasopharynx : The ratio of the depth of the nasopharynx to the total distance ANS-PPW, viz., PNS-PPW/ANS-PPW. The depth of the naso- pharynx varies considerably from individual to individual but exhibits a reason- ably constant relationship to the length of the hard palate. An increased ratio indicates a functionally deepened nasopharynx of some significance.
Velopharyngeal Incompetence : The ratio of the distance LE-PPW and PNS-PPW, viz., LE-PPW/PNS-PBW. A measure of the " g a p " or inability to achieve closure.
Listener judgement of tape-recorded speech samples is expressed according to the Speech Rating Scale of Bloomer (1957) :
o---No hypernasality. Normal voice. 1--Very mild hypernasality. May be inconsistently present. Is not more notice-
able than sometimes found in speakers with anatomically normal palates. 2--Mild hypernasality. Can be identified as associated with cleft palate quality
and is acceptable, but not good, quality. 3--Moderately severe hypernasality. Definitely characteristic of " cleft palate
quali ty". 4--Severe hypernasality. Indicative of very poor palatopharyngeal function.
Speech evaluation was performed by one of the authors (A. H. S.) totally independently and without knowledge of the cineradiographic analyses.
D a t a . - - T h e cineradiographic data are presented in Table I. The subjective speech evaluations are presented in Table II.
Resul ts . - -Comparison of the post-operative and the pre-operative radiographs reveals that the surgical procedure resulted in :
I. No change in the relative depth of the nasopharynx. 2. An average increase in the absolute length of the soft palate of IO ram., producing
a 20 to 45 per cent increase in functional length, and a posterior displacement of the levator insertion averaging 6 ram. Both of these factors contributed to the achievement of broad vdopharyngeal closure with a reduction of the pre-operative
CINERADIOGRAPHIC ASSESSMENT OF COMBINED ISLAND FLAP PUSHBACK 41
velopharyngea] incompetence to the normal range in three of the four patients (Fig. 2).
3. A moderate decrease in velar excursion with no change in the rate of velar ascent.
TABLE I
Patient
Relative depth of nasopharynx
Velar excursion (ram.) Rate of velar ascent
(mm./sec.) Length of soft palate
(ram.) Relative length of soft
palate Levator insertion (ram.) Velopharyngeal
incompetence (%) Type of velopharyngeal
closure
R . B.
Pre- i Post-
0"40 12
59
30
1"02 2 0
31
n o n e
[
[0"40 I 2
59
45
I ' 5 0 25
16
D . H .
Pre- Post-
o'41 0"40 14 i i
60 58
26 34
1"o8 1-35 17 24
31 3 J
none broad I
n . P .
broad
TABLE I I
Speech Rating
Pre- Post-
O ' 5 I 0"50 , I I IO
55 51
29 35
0"92 I ' I2 2I 27
33 14
touch broad
J° K .
Pre- Post-
0 5 4
41 ~,
30 43
0-83 1.23 18 24
49 30
none none
Age at Patient Surgery
(Yrs.)
R.B. D . H . 29
B . P . 5
J . K . 7
Pre- Post-
I
4 2
4 4
Post-operative Interval (Mos.)
I 2 I 2
IO
x9
Type of Speech
Therapy
None Public
School Private
Private
Therapist's Prognostic Comment
Still progressing
Rapidly progressing
No progress
Qualitative analysis of the cineradiographs showed : I. Increased elevation of the velum in the rest position. 2. Rigidity and immobility of that portion of the velum immediately posterior to
the hard palate. 3- Migration of the pharyngeal flap from a superior to a horizontal position and
anterior displacement of the posterior pharyngeal wall immediately superior to the pedicle of the pharyngeal flap.
DISCUSSION
Recent investigations (Hoopes et al., I968a, b) have defined the anatomical factors responsible for velopharyngeal incompetence in patients with submucous cleft palate (Table III) ; specifically, a soft palate which is both absolutely and relatively short, and an anteriorly displaced levator insertion. Comparison of the post-operative data in Table I with the normal data in Table III reveals the specific contributions of the surgical procedure to the post-operative speech improvement: length of soft palate, relative length of soft palate and levator insertion are within normal limits post-operatively. Hage (I966) evaluated the island flap pushback procedure radiographically by means of
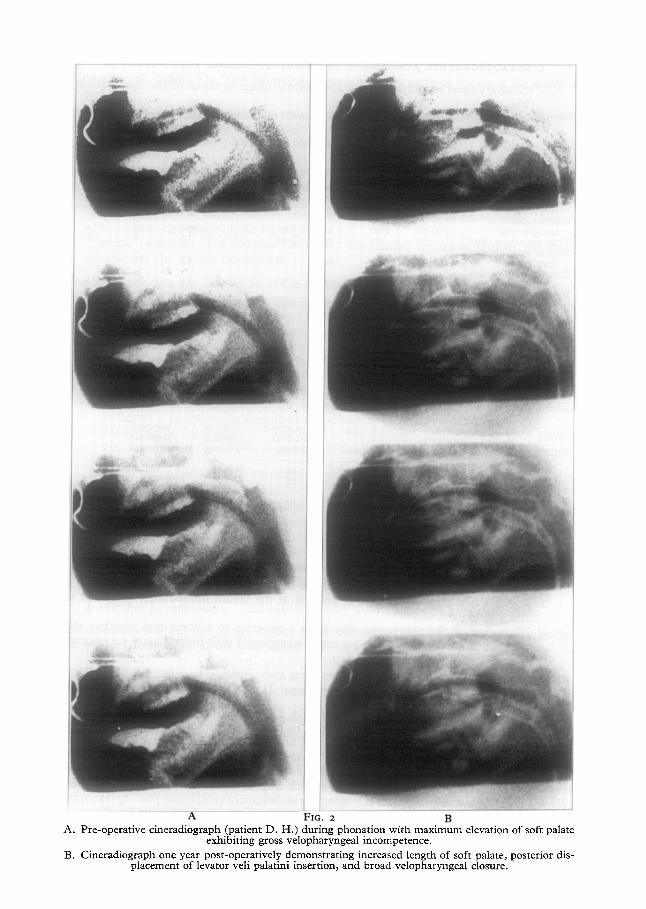
A FIG. 2 B &. Pre-operative cineradiograph (patient D. H.) during phonation with maximum elevation of soft palate
exhibiting gross velopharyngeal incompetence. B. Cineradiograph one year post-operatively demonstrating increased length of soft palate, posterior dis-
placement of levator veil palatini insertion, and broad velopharyngeal closure.
C I N E R A D I O G R A P H I C ASSESSMENT OF C O M B I N E D I S L A N D FLAP P US HBACK 43
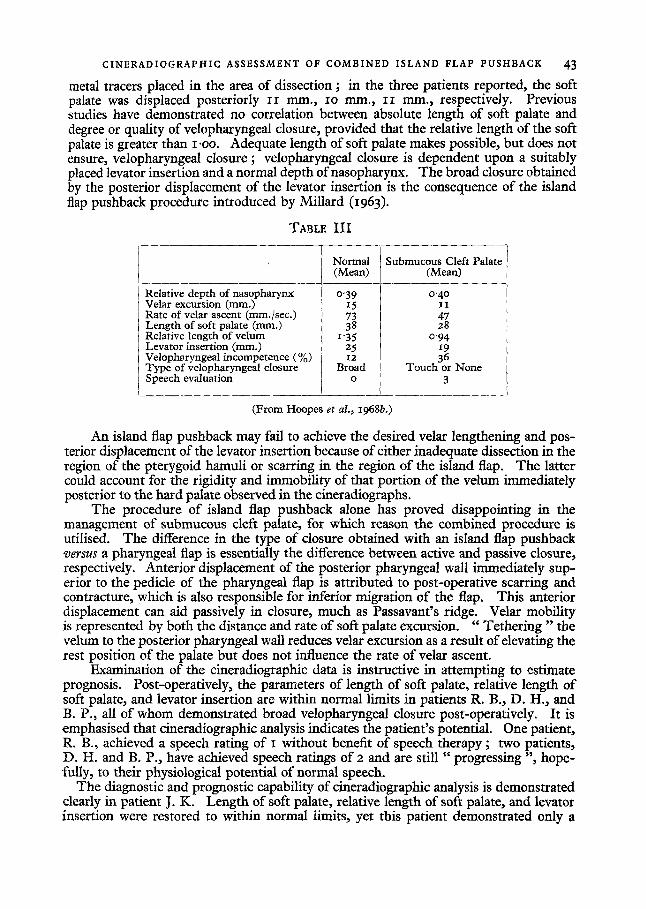
metal tracers placed in the area of dissection ; in the three patients reported, the soft palate was displaced posteriorly II mm., IO mm., II ram., respectively. Previous studies have demonstrated no correlation between absolute length of soft palate and degree or quality of velopharyngeal closure, provided that the relative length of the soft palate is greater than I.OO. Adequate length of soft palate makes possible, but does not ensure, velopharyngeal closure ; velopharyngeal closure is dependent upon a suitably placed levator insertion and a normal depth of nasopharynx. The broad closure obtained by the posterior displacement of the levator insertion is the consequence of the island flap pushback procedure introduced by Millard (1963).
TABLE I I I
Normal (Mean)
Relative depth of nasopharynx 0"39 Velar excursion (ram.) 15 Rate of velar ascent (mm./sec.) 73 Length of soft palate (ram.) 38 Relative length of velum i r.35 Levator insertion (ram.) I 25 Velopharyngeal incompetence (%) 12 Type of velopharyngeal closure Broad Speech evaluation ~ o
Submucous Cleft Palate (Mean)
0-40 I I 47 28
0"94 19 36
Touch or None 3
(From Hoopes et al., x968b.)
An island flap pushback may fail to achieve the desired velar lengthening and pos- terior displacement of the levator insertion because of either inadequate dissection in the region of the pterygoid hamuli or scarring in the region of the island flap. The latter could account for the rigidity and immobility of that portion of the velum immediately posterior to the hard palate observed in the cineradiographs.
The procedure of island flap pushback alone has proved disappointing in the management of submucous cleft palate, for which reason the combined procedure is utilised. The difference in the type of closure obtained with an island flap pushback v e r s u s a pharyngeal flap is essentially the difference between active and passive closure, respectively. Anterior displacement of the posterior pharyngeal wall immediately sup- erior to the pedicle of the pharyngeal flap is attributed to post-operative scarring and contracture, which is also responsible for inferior migration of the flap. This anterior displacement can aid passively in closure, much as Passavant's ridge. Velar mobility is represented by both the distance and rate of soft palate excursion. "Tethering " the velum to the posterior pharyngeal wall reduces velar excursion as a result of elevating the rest position of the palate but does not influence the rate of velar ascent.
Examination of the cineradiographic data is instructive in attempting to estimate prognosis. Post-operatively, the parameters of length of soft palate, relative length of soft palate, and levator insertion are within normal limits in patients R. B., D. H., and B. P., all of whom demonstrated broad velopharyngeal closure post-operatively. It is emphasised that cineradiographic analysis indicates the patient's potential. One patient, R. B., achieved a speech rating of I without benefit of speech therapy ; two patients, D. H. and B. P., have achieved speech ratings of 2 and are still "progressing ", hope- fully, to their physiological potential of normal speech.
The diagnostic and prognostic capability of cineradiographic analysis is demonstrated clearly in patient J .K. Length of soft palate, relative length of soft palate, and levator insertion were restored to within normal limits, yet this patient demonstrated only a
44 BRITISH JOURNAL OF PLASTIC SURGERY
minimal decrease in velopharyngeal incompetence, gross failure to achieve velopharyn- geal closure, and no improvement in speech post-operatively. The depth of naso- pharynx in this patient is approximately 35 per cent. greater than normal. In retrospect, pre-operative cineradiographic analysis revealed that no form of palate lengthening procedure could reduce velopharyngeal incompetence to within normal limits and should have suggested the necessity of posterior pharyngeal wall augmentation. It may be predicted on the basis of this objective data that this patient will achieve little or no improvement, and this seems to be confirmed by the report o f " no progress "
SUMMARY
The application of cineradiographic analysis to the diagnosis, treatment, and prog- nosis of cleft palate speech is presented.
Posterior displacement of the levator veli palatini insertion is essential in the surgical correction of velopharyngeal incompetence.
We wish to thank M r Henri C. Hessels for his expert technical assistance.
REFERENCES
BLOOMER, H. H. (I957). In " Handbook of Speech Pathology ", ed. Travis, L. E., Ch. 21, p. 6o8. New York : Appleton-Century-Crofts.
HAGE, J. (1966). Br. ]. plast. Surg. 19, 317 • HOOPES, J. E. and FABRIKANT~ J. I. (I968). Plastic reconstr. Surg. 42, I. HooPEs, J. E., DELLON, A. L., FABmr, ANT, J. I. and SOLIMAN, A. H. (I968a). Plastic reconstr.
Surg. (In press.) HooPEs, J. E., DELLON, A. L., Fm3RIKANT, J. I. and SOLIMAN, A. H. (I968b). (Submitted for
publication.) MILLARD, D. R. (I963). Surgery Gynec. Obstet. I16, 297.
Related Documents











