Pharmacokinetics/Pharmacodynamics of Antibiotics: Refresher Part 2 CHSPSC, LLC Antimicrobial Stewardship Education Series ProCE, Inc. www.ProCE.com 1 CHSPSC, LLC Antimicrobial Stewardship Education Series June 14, 2017 Pharmacokinetics/Pharmacodynamics of Antibiotics: Refresher Part 2 Featured Speaker: Larry Danziger, Pharm.D. Professor of Pharmacy and Medicine University of Illinois at Chicago 2 Submission of an online post‐test and evaluation is the only way to obtain CE credit for this webinar Go to www.ProCE.com/CHSRx Webinar attendees will also receive an email with a direct link to the web page Print your CE statement of completion online – Credit for live or enduring (not both) Deadline: July 14, 2017 CPE Monitor (applicable to pharmacists) – CE credit automatically uploaded to NABP/CPE Monitor upon completion of post‐test and evaluation (user must complete the “claim credit” step) Online Evaluation, Self-Assessment and CE Credit Attendance Code Code will be provided at the end of today’s activity

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Pharmacokinetics/Pharmacodynamics of Antibiotics: Refresher Part 2CHSPSC, LLC Antimicrobial Stewardship Education Series
ProCE, Inc.www.ProCE.com 1
CHSPSC, LLC Antimicrobial Stewardship Education Series
June 14, 2017Pharmacokinetics/Pharmacodynamics of Antibiotics: Refresher Part 2
Featured Speaker:
Larry Danziger, Pharm.D.Professor of Pharmacy and MedicineUniversity of Illinois at Chicago
2
Submission of an online post‐test and evaluation is the only way to obtain CE credit for this webinar
Go to www.ProCE.com/CHSRx Webinar attendees will also receive an email with a direct link to the
web page Print your CE statement of completion online
– Credit for live or enduring (not both)
Deadline: July 14, 2017 CPE Monitor (applicable to pharmacists)
– CE credit automatically uploaded to NABP/CPE Monitor upon completion of post‐test and evaluation (user must complete the “claim credit” step)
Online Evaluation, Self-Assessmentand CE Credit
Attendance Code
Code will be provided at the end of today’s activity

Pharmacokinetics/Pharmacodynamics of Antibiotics: Refresher Part 2CHSPSC, LLC Antimicrobial Stewardship Education Series
ProCE, Inc.www.ProCE.com 2
How to Ask a Question
Locate menu bar on your computer desktop
Click orange arrow button to open menu box
Type question into question box
Click Send
Do not close menu box
– This will disconnect you
from the Webcast
Please submit questions throughout
presentation
Click No!
Click
Enter question
3
Accessing PDF Handout Click the hyperlink that is
located directly above the question box
Do not close menu box
– This will disconnect you
from the Webcast
No!
Clickhyperlink
4

Pharmacokinetics/Pharmacodynamics of Antibiotics: Refresher Part 2CHSPSC, LLC Antimicrobial Stewardship Education Series
ProCE, Inc.www.ProCE.com 3
2016 Pharmacy Education Series
5
It is the policy of ProCE, Inc. to ensure balance, independence, objectivity and scientific rigor in all of its continuing education activities. Faculty must disclose to participants the existence of any significant financial interest or any other relationship with the manufacturer of any commercial product(s) discussed in an educational presentation. Dr. Danziger has disclosed the following financial/commercial relationships: Speaker for Allergan, MedCo, and Merck.
Please note: The opinions expressed in this activity should not be construed as those of the CME/CE provider. The information and views are those of the faculty through clinical practice and knowledge of the professional literature. Portions of this activity may include unlabeled indications. Use of drugs and devices outside of labeling should be considered experimental and participants are advised to consult prescribing information and professional literature.
June 14, 2017Pharmacokinetics/Pharmacodynamics of Antibiotics: Refresher Part 2
Featured Speaker:
Larry Danziger, Pharm.D.Professor of Pharmacy and MedicineUniversity of Illinois at Chicago
CE Activity Information & Accreditation
ProCE, Inc. (Pharmacist CE)
– 1.0 contact hour
6
Funding:This activity is self‐funded through CHSPSC.

Pharmacokinetics/Pharmacodynamics of Antibiotics: Refresher Part 2CHSPSC, LLC Antimicrobial Stewardship Education Series
ProCE, Inc.www.ProCE.com 4
Antimicrobial Pharmacokinetics / Pharmacodynamics: Optimizing Therapeutic Outcomes
June 14, 2017
Larry H. Danziger, Pharm.DProfessor of Pharmacy and MedicineUniversity of Illinois at Chicago
7
ObjectivesUpon completion of this presentation, the participant
should be able to:
• Describe the pharmacodynamic (PD) properties of antimicrobials
• Identify strategies to maximize the PD properties in selecting and dosing aminoglycosides, beta-lactams and vancomycin
• Also when to monitor serum concentrations logically and how to interpret them
8
Pharmacokinetics/Pharmacodynamics of Antibiotics: Refresher Part 2CHSPSC, LLC Antimicrobial Stewardship Education Series
ProCE, Inc.www.ProCE.com 5
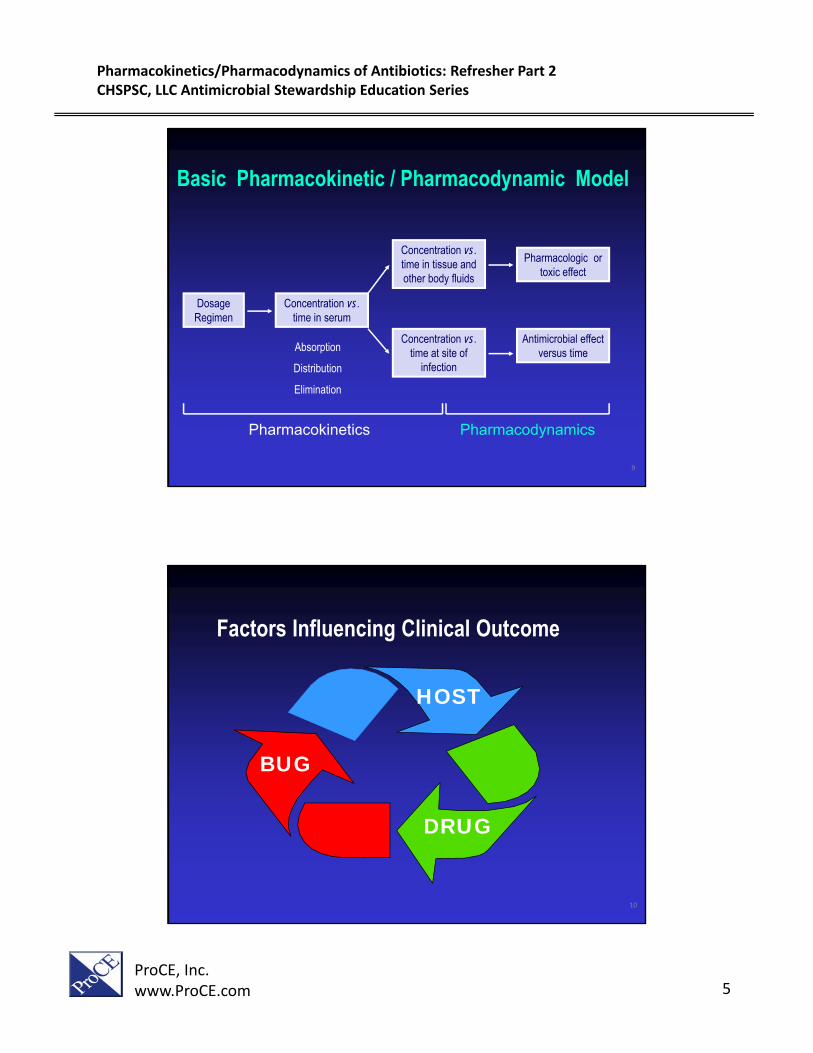
Basic Pharmacokinetic / Pharmacodynamic Model
Dosage Regimen
Concentration vs. time in serum
Concentration vs. time at site of
infection
Concentration vs. time in tissue and other body fluids
Pharmacologic or toxic effect
Antimicrobial effect versus time
Pharmacokinetics Pharmacodynamics
Craig WA. Clin Infect Dis 1998;26:1-12.
Absorption
Distribution
Elimination
9
HOST
BUG
DRUG
Factors Influencing Clinical Outcome
10

Pharmacokinetics/Pharmacodynamics of Antibiotics: Refresher Part 2CHSPSC, LLC Antimicrobial Stewardship Education Series
ProCE, Inc.www.ProCE.com 6
Pharmacodynamic Goals• Concentration dependent
– Cmax/MIC: Optimize dose to produce higher unbound drug concentrations
– AUC/MIC: Optimize the dose and exposure to unbound drug concentrations
• Concentration independent– T > MIC: Optimize duration of unbound drug
concentration at or above the MIC11
Pharmacodynamics of Specific AntimicrobialsPharmacodynamic Parameter
Cmax/MIC AUC/MIC T > MIC
• Aminoglycosides
• Fluoroquinolones• Metronidazole
• Aminoglycosides
• Azithromycin
• Daptomycin
• Glycopeptides
• Ketolides
• Quinupristin/dalfopristin
• Beta-lactams
• Aztreonam
• Erythromycin
• Clarithromycin
• Linezolid
• Clindamycin
•Vancomycin
Rodvold KA. Pharmacotherapy 2001;21:319S-330S.
Nicolau DP. J Infect Chemother 2003;9:292-296.12

Pharmacokinetics/Pharmacodynamics of Antibiotics: Refresher Part 2CHSPSC, LLC Antimicrobial Stewardship Education Series
ProCE, Inc.www.ProCE.com 7
Pharmacodynamics of Specific Antimicrobials
Peak/MIC 10x ( Gm - ) Aminoglycosides / Fluoroquinolones
AUC/MIC >125 ( Gm - ) or >30 ( Gm + ) Fluoroquinolones
Time > MIC >50% Cephalosporins / Macrolides
AUC/MIC >100 Daptomycin or >50 Colistin or > 400 Vancomycin
Time (Hours) 24 Hours 13
Dosing Mystery
How is the proper dose and dosage interval determine?
In some instances, agents whose half-lives in serum differ by as much as 10 to 18-fold have been administered at the same dosage, with the same interval between doses
14
Pharmacokinetics/Pharmacodynamics of Antibiotics: Refresher Part 2CHSPSC, LLC Antimicrobial Stewardship Education Series
ProCE, Inc.www.ProCE.com 8
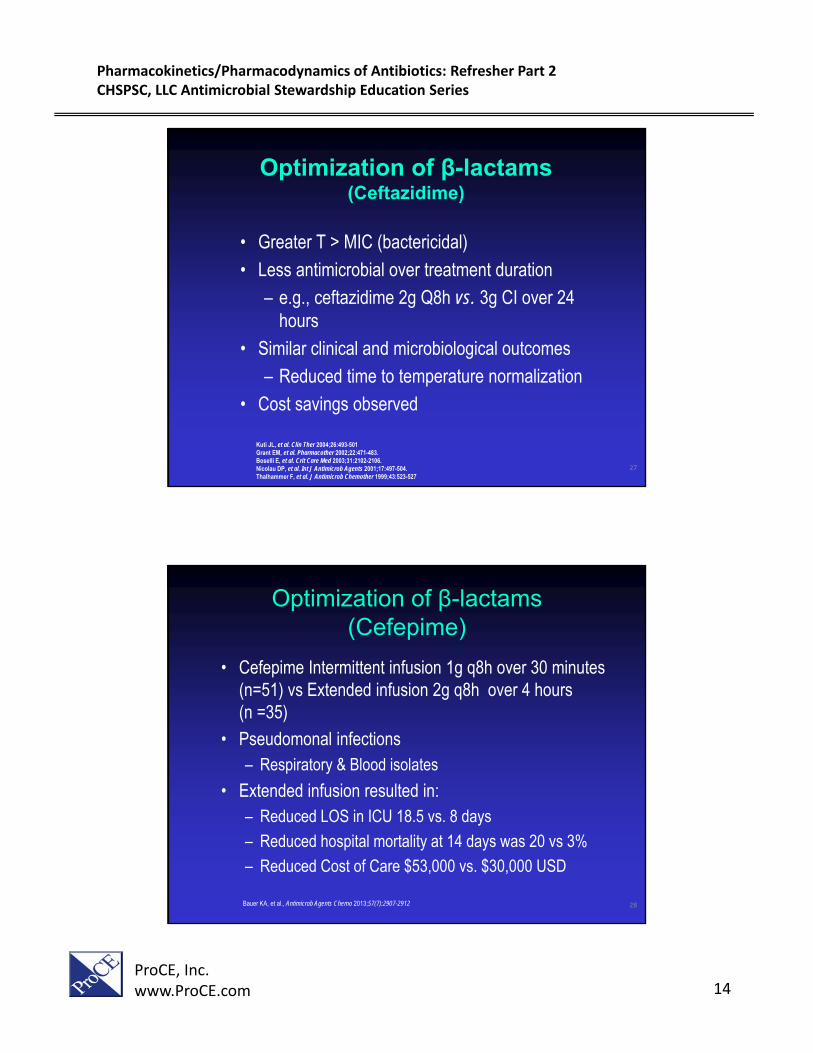
Garnacho-Montero et al
Luna et al
0 20 40 60 80 100
Ibrahim et al
Alvarez-Lerma
Rello et al
Mortality (%)
Vallés et al
Rello et al. Am J Respir Crit Care Med 1997;156:196–200; Alvarez-Lerma. Intensive Care Med 1996;22:387–394Ibrahim et al. Chest 2000;118:146–155; Vallés et al. Chest 2003;123:1615–1624Luna et al. Chest 1997;111:676–685 Garnacho-Montero et al. Crit Care Med 2003;31:2742–2751;
Mortality Associated with Appropriate Therapy (Critically Ill Patients)
Why continued Mortality? Delay of initial therapy
Inadequate drug exposure
Wrong dose
Persistence of disease process
15
Do We Deliver Effective Doses in Critically Ill Patients
Prospective, observational study to assess clinical and microbiologic response rates in 19 critically ill patients with empiric therapy
Only 3/19 patients met appropriate PK/PD target goal with initial empiric antibiotic
After dose changed to appropriate PK/PD target goal
– 17/19 (89%) patients had a clinical cure or improvement
– 16/19 (84%) had either microbiologic eradication or presumed eradication
Mohr JF, et al. Diagn Micro Infect Dis 2004;48:125-30.16

Pharmacokinetics/Pharmacodynamics of Antibiotics: Refresher Part 2CHSPSC, LLC Antimicrobial Stewardship Education Series
ProCE, Inc.www.ProCE.com 9
Pharmacokinetic /Pharmacodynamic Considerations
• Beta-Lactams– PK/PD Effect relationships
– Dosage regimen design
• Gentamicin– PK/PD Effect relationships
– Dosage regimen design
• Vancomycin– PK/PD Effect relationships
– Dosage regimen design
17
Optimization of β-lactams
• β-Lactam antibiotics are the most widely produced and used antibacterial drugs in the world, and have been ever since their initial clinical trials in 1941
• The critical parameter is the time the antibiotic concentration remains above the MIC of the organism expressed as
– T > MIC
18

Pharmacokinetics/Pharmacodynamics of Antibiotics: Refresher Part 2CHSPSC, LLC Antimicrobial Stewardship Education Series
ProCE, Inc.www.ProCE.com 10
Optimization of β-lactams
• Duration of exposure was documented as being important for β-lactam antibiotics more than 70 years ago (Eagle 1940s and Schmidt 1950s)
• Noted most effective way to treat an infection with penicillin (a β-lactam) was to maintain MIC in the plasma throughout the course of treatment
• Repository formulations of penicillin G, were designed to maintain concentrations of the drug above the MIC in plasma and tissues for protracted time periods
Chain E, et al. Lancet 1940, 1: 226-228Schmidt L, Walley A, J Pharmacol Ther 1951, 103: 479-488 19
Serum Concentrations of Penicillin GVarious Routes of Administration
20

Pharmacokinetics/Pharmacodynamics of Antibiotics: Refresher Part 2CHSPSC, LLC Antimicrobial Stewardship Education Series
ProCE, Inc.www.ProCE.com 11
Intravenous Therapy(A History)
• First IV antibiotic penicillin administered at Mass General in 1940s
• Until about the 1930s-1940s, the administration of IV fluids and medications was usually performed by physicians
• In fact, in some locations, IV cannulation and IV medication administration remained exclusively a medical role until about the 1970s
Millam D. J Intraven Nur, 1996;19:5-14 Reusable Syringe Kit (1880s)21
• Continuous intravenous infusions of penicillin fell out of favor as a treatment strategy in the 1960s
• IV medications were often only given during the day
• In the 1950s and 1960s fear of IV administration because
• Bottle might fall on the patient
• Air embolus of solution running out
• Toxicity associated with accidental over administration of fluid and drug
Millam D. J Intraven Nur, 1996;19:5-14
Intravenous Therapy(A History)
22

Pharmacokinetics/Pharmacodynamics of Antibiotics: Refresher Part 2CHSPSC, LLC Antimicrobial Stewardship Education Series
ProCE, Inc.www.ProCE.com 12
• Research of continuous infusion β-lactams in humans again occurs in earnest again in the late 1970s– Febrile neutropenic patients
– Carbenicillin + intermittent or continuous infusion cefamandole
– ↑ cure rates with continuous vs. intermittent infusion
Bodey GP, et al. Am J Med 1979;67:608-616.
Optimization of β-lactams
23
The optimum level of exposure varies for different agents within the beta-lactam class
Required %T>MIC for efficacy:
~ 50%–70% for cephalosporins
~ 50% for penicillins
~ 40% for carbapenems
Drusano GL. Clin Infect Dis. 2003;36(suppl 1):S42-S50.
Optimization of β-lactams
24

Pharmacokinetics/Pharmacodynamics of Antibiotics: Refresher Part 2CHSPSC, LLC Antimicrobial Stewardship Education Series
ProCE, Inc.www.ProCE.com 13
Optimization of β-lactams
25
Concentration
Time
MIC
Intermittent Infusion
Ceftazidime 2g Q8h = TDD 6g
Ceftazidime 3g daily Continuous Infusion
Optimization of β-lactams(Ceftazidime)
26
Pharmacokinetics/Pharmacodynamics of Antibiotics: Refresher Part 2CHSPSC, LLC Antimicrobial Stewardship Education Series
ProCE, Inc.www.ProCE.com 14
• Greater T > MIC (bactericidal)
• Less antimicrobial over treatment duration
– e.g., ceftazidime 2g Q8h vs. 3g CI over 24 hours
• Similar clinical and microbiological outcomes
– Reduced time to temperature normalization
• Cost savings observed
Kuti JL, et al. Clin Ther 2004;26:493-501 Grant EM, et al. Pharmacother 2002;22:471-483. Boselli E, et al. Crit Care Med 2003;31:2102-2106. Nicolau DP, et al. Int J Antimicrob Agents 2001;17:497-504. Thalhammer F, et al. J Antimicrob Chemother 1999;43:523-527;35:391-402.
Optimization of β-lactams(Ceftazidime)
27
• Cefepime Intermittent infusion 1g q8h over 30 minutes (n=51) vs Extended infusion 2g q8h over 4 hours (n =35)
• Pseudomonal infections– Respiratory & Blood isolates
• Extended infusion resulted in:– Reduced LOS in ICU 18.5 vs. 8 days
– Reduced hospital mortality at 14 days was 20 vs 3%
– Reduced Cost of Care $53,000 vs. $30,000 USD
Bauer KA, et al., Antimicrob Agents Chemo 2013;57(7):2907-2912
Optimization of β-lactams(Cefepime)
28

Pharmacokinetics/Pharmacodynamics of Antibiotics: Refresher Part 2CHSPSC, LLC Antimicrobial Stewardship Education Series
ProCE, Inc.www.ProCE.com 15
1.0 mcg/ml
Cirillo I et al. J Clin Pharm. 2009;7:798
Optimization of β-lactams(Doripenem)
29
• A recent randomized trial in VAP patients comparing doripenem 4 hr extended-infusion with imipenem-cilastatin was prematurely terminated because of higher rates of clinical failures and mortality in the doripenem
• In the MITT clinical cures was lower in the doripenem treated patients 45.6% vs 56.8% in imipenem-cilistatin patients
• In the intent-to-treat population, the 28-day all-cause mortality was higher in the doripenem arm (23.0 percent; n=31/135) than in the imipenem-cilastatin arm (16.7 percent; n=22/132)
FDASafety Announcement [03-06-2014] https://www.fda.gov/Drugs/DrugSafety/ucm387971.htm
Optimization of β-lactams(Doripenem)
30

Pharmacokinetics/Pharmacodynamics of Antibiotics: Refresher Part 2CHSPSC, LLC Antimicrobial Stewardship Education Series
ProCE, Inc.www.ProCE.com 16
Meta-analysis to determine whether prolonged β-lactam infusions were associated with a reduction in mortality and improvement in clinical success
A search of PubMed, EMBASE and The Cochrane Library for randomized controlled trials (RCTs) and observational studies comparing prolonged infusion with intermittent bolus administration of the same antibiotic in hospitalized adult patients was conducted
Primary outcomes evaluated were mortality and clinical success
A total of 29 studies with 2206 patients (18 RCTs and 11 observational studies) were included in the meta-analysis
31
Prolonged Infusion vs Intermittent Boluses of β-lactam Antibiotics
(A meta-analysis )
Teo J et al, Inter J of Antimicrob Agents 2014; 43: 403-411
Clinical Success Mortality
Use of prolonged infusion appears to be associated with improvement in clinical success (RR=1.12,95% CI 1.03-1.21)
Use of prolonged infusion appears to be associated with improvement in mortality (RR=1.12,95% CI 1.03-1.21)
32

Pharmacokinetics/Pharmacodynamics of Antibiotics: Refresher Part 2CHSPSC, LLC Antimicrobial Stewardship Education Series
ProCE, Inc.www.ProCE.com 17
Optimization of β-lactams
33
• Although studies to date thus far very small
• Clinical data suggest that prolonged infusions are at least as effective as intermittent infusions for gram-negative infections
• More randomized, well powered studies needed
• May not be necessary for all bacteria ( or infections)
• Questionable role: Critically ill patients with meningitis, VAP, or those with suspected or confirmed MDR pathogen
Gillespie EL, et al. Expert Opin Drug Metab Toxicol 2005;1:351-61 Lodise TP, et al. CID 2007;44:357-63 Teo J et al, Inter J of Antimicrob Agents 2014; 43: 403-411
Optimization of β-lactams(Issues for Extended Infusion)
34

Pharmacokinetics/Pharmacodynamics of Antibiotics: Refresher Part 2CHSPSC, LLC Antimicrobial Stewardship Education Series
ProCE, Inc.www.ProCE.com 18
Once-Daily Aminoglycosides(Extended Interval Dosing)
• This approach exploits the concentration-dependent killing and post-antibiotic effect of aminoglycosides
• Considered as efficacious as traditional dosing with possibly less toxicity
• However, this strategy has not been adequately studied in all populations
35
Meta-Analysis Once Daily Dosing Aminoglycosides
• Randomized, controlled trials that compared intravenous once-daily aminoglycoside regimen with a standard aminoglycoside regimen in infected immunocompetent adults
• Examined efficacy, mortality, or toxicity
• 42 studies were reviewed for possible inclusion
• 13 independent studies met the selection criteria, and their results were pooled
Hatala R et al; Annals of Internal Medicine. 124(8):717‐725, April 15, 1996.36

Pharmacokinetics/Pharmacodynamics of Antibiotics: Refresher Part 2CHSPSC, LLC Antimicrobial Stewardship Education Series
ProCE, Inc.www.ProCE.com 19
Figure 1Once-Daily Aminoglycoside Dosing Meta-Analysis
Hatala, R et al. Annals of Internal Medicine. 124(8):717‐725, April 15, 1996.
Once‐daily compared with standard aminoglycoside dosing. The individual study risk ratios for clinical cure, with 95% CIs. Risk ratios to the left of 1.0 favor standard aminoglycoside dosing; those to the right favor once‐daily aminoglycoside dosing. Test for heterogeneity, P equals 0.07.
Once‐daily compared with standard aminoglycoside dosing. The individual study and pooled risk ratios for nephrotoxicity, with 95% CIs. Risk ratios to the left of 1.0 favor once‐daily aminoglycoside dosing; those to the right favor standard aminoglycoside dosing Test for heterogeneity, P more than 0.2.
Clinical Cure Nephrotoxicity
N equals the total individual study sample for the outcome N equals the total individual study
sample for the outcome
37
Once Daily Aminoglycoside Dosing NomogramsInitial Doses and CrCL Based Dosing
38

Pharmacokinetics/Pharmacodynamics of Antibiotics: Refresher Part 2CHSPSC, LLC Antimicrobial Stewardship Education Series
ProCE, Inc.www.ProCE.com 20
Once-Daily Aminoglycosides
• Most Use Hartford Nomogram
• Recommends a single level be drawn 6 to 14 hours after the dose
• Less intensive monitoring of serum concentrations
• With extended interval dosing there should be no significant accumulation with multiple dosing, therefore, measurements can be obtained after any dose
Freeman C et al. JAC 1997;39:677-686
Nicolau D et al. Antimicrob Agents Chemother 1995; 39:650-65539
Freeman C et al. JAC1997;39:677-686.
Hartford Aminoglycoside Nomogram
Hartford Nomogram 7 mg/Kg OD
If level falls in area designated 24 hours, 36 hours or 48 hours, dosing interval is 24, 36 or 48 hourly respectively.
If level falls on a line between dosing intervals, choose longer interval.
If level is above 48 hour line then STOP the treatment. If gentamicin is to be continued, take daily levels, but do not give any more gentamicin until level falls below 2mg/L 40

Pharmacokinetics/Pharmacodynamics of Antibiotics: Refresher Part 2CHSPSC, LLC Antimicrobial Stewardship Education Series
ProCE, Inc.www.ProCE.com 21
Once-Daily Aminoglycosides• This approach provides high peaks and undetectable
troughs
• Dose: 5-7mg/kg/24hrs (ABW)
• Target peak 14-20 mcg/ml
• Allows low troughs (<1mcg/ml )
• If elevated concentrations noted consider:• Blood collected too early
• Patient not clearing Gentamicin
• Blood collected from lumen used to infuse Gentamicin earlier on
Bertino JS, et al. Clin Infect Dis 1997;24:820-823. Brown GH, et al. Clin Infect Dis 2000;30:440-441. Barclay ML, et al. Clin Pharmacokinet 1999;36:89-98.
41
Once-daily AminoglycosidesProposed Benefits/Cautions
• Equal efficacy
• Maximizes Cmax/MIC ratio
• Reduced toxicity (lower drug accumulation)• Nephrotoxicity and ototoxicity
• Avoid in patients with altered Vd or clearance:• Burns, CF, pregnancy, endocarditis, meningitis,
ascites or CrCl < 20ml/min
Freeman CD, et al. Pharmacother 1996;16:1093-1102. Bailey TC, et al. Clin Infect Dis 1997;24:786-795. Rybak MJ, et al. Antimicrob Agents Chemother 1999;43:1549-1555.
42

Pharmacokinetics/Pharmacodynamics of Antibiotics: Refresher Part 2CHSPSC, LLC Antimicrobial Stewardship Education Series
ProCE, Inc.www.ProCE.com 22
Aminoglycosides Summary
• Dosing methods: traditional dosing or once daily dosing
• Once Daily Dosing is recommended; provides high peaks and undetectable troughs, with equal or better clinical outcomes and less nephrotoxicity
Traditional Dosing Extended Dosing
Tobramycin/Gentamicin 2 mg/kg Q8 hr 5-7 mg/kg daily
Amikacin 5-7.5 mg/kg Q8 hr 15 mg/kg daily
Provides therapeutic troughs and peaksConsidered in pts with severe renal failureCheck peak and trough
Appropriate for most patients or good renal function or moderate renal insufficiency. Check a level 8-12 hours after end of infusion
43
Vancomycin - Background
– A glycopeptide antibiotic
– Inhibition of cell wall synthesis
– Used IV for treatment of patients with suspected or proven invasive gram-positive infections, including methicillin-resistant Staphylococcus aureus (MRSA)
– Emerging Vancomycin resistance: VRE and VRSA
44

Pharmacokinetics/Pharmacodynamics of Antibiotics: Refresher Part 2CHSPSC, LLC Antimicrobial Stewardship Education Series
ProCE, Inc.www.ProCE.com 23
Vancomycin Nephrotoxicity and Ototoxicity
• Early reports: impure product
• Nephrotoxicity– May potentiate aminoglycoside nephrotoxicity
– Trough >15 or >20 mg/L
– Css average >28 mg/L
– AUC >952 mg.h/L
• Ototoxicity– Little evidence if monotherapy
– However reported in some patients with vancomycin concentrations > 80 mg/L
45
Ebert, S. ICAAC #439, 1987
VancomycinConcentration - Effect Relationships
46
Pharmacokinetics/Pharmacodynamics of Antibiotics: Refresher Part 2CHSPSC, LLC Antimicrobial Stewardship Education Series
ProCE, Inc.www.ProCE.com 24
• Moise-Broder et al, Clin Pharmacokinet 43: 925, 2004
– 108 patients, MRSA
– Better outcome if ssAUC24 /MIC > 400 mg.h/L
– No relationship with time >MIC
• Jeffres et al, Chest 130: 947, 2006
– 102 patients, retrospective study
– No difference in trough (14 mg/L) or AUC (350 mg.h/L) between survivors and non-survivors (no MIC data)
VancomycinConcentration - Effect Relationships
47
Vancomycin Background
Incorrect vancomycin dosing and/or increased vancomycin MIC’s compromise possibility of target attainment
The method of determining the MIC also matters in reporting and calculating this ratio
Rybak et al, Am J Health-Syst Pharm 66: 1 Jan 2009Therapeutic monitoring of vancomycin in adult patients: a consensus review
48

Pharmacokinetics/Pharmacodynamics of Antibiotics: Refresher Part 2CHSPSC, LLC Antimicrobial Stewardship Education Series
ProCE, Inc.www.ProCE.com 25
Vancomycin Background
IDSA/ASHP/SIDP guidelines for vancomycin promote an AUC/MIC ratio of > 400 to optimize outcome
We use trough concentrations as surrogates for AUC
Rybak et al, Am J Health-Syst Pharm 66: 1 Jan 2009Chest 2006; 130:947-55
Mean Trough Mean AUC
9.4 µg/mL 318 ± 111 µg/h/mL
20.4 µg/mL 418 ± 152 µg/h/mL
49
Vancomycin and MICs
• Probability of achieving target AUC/ MIC is 0% if vancomycin MIC = 2 µg/mL with low or high-dose vancomycin
• Vancomycin MICs of 2 µg/mL associated with increased treatment failures
• “MIC creep” observed in some centers but not others
Sakoulas JCM 2004;42:2398-402; Hidayat L Arch Intern Med 2006;166:2138-44; Lodise AAC 2008;52:3315-20; Maor JID 2009;199:619-24 2Alos JAC 2008;62:773-5; Holmes AAC 2008;52:757-60; Jones CID 2006;42:S13-24; Sader AAC 2009; 53:4127-32
Mohr CID 2007;44:1536-42
50

Pharmacokinetics/Pharmacodynamics of Antibiotics: Refresher Part 2CHSPSC, LLC Antimicrobial Stewardship Education Series
ProCE, Inc.www.ProCE.com 26
Per
cent
Suc
cess
Adapted from Sakoulas, et. al., 2004 JCM 42:2398; Moise-Broder et al. 2004 CID 38: 1700-5;Hidayat et al. 2006 Arch Intern Med 166:2138-2144; Moise et al. 2007 AAC 51:2582-6
Vancomycin Increased MICs: Poor Response
(MRSA Patients)
51
Vancomycin MICs A Guide to Therapy?
• Isolates with a vancomycin MIC ≤ 2 µg/mL, the patient’s clinical response should determine continued use of vancomycin, independent of the MIC
• If clinical and microbiological response to vancomycin noted, continue with close follow-up
• If no clinical or microbiologic response an alternative to vancomycin should be considered regardless of MIC
• For isolates with a vancomycin MIC 2 µg/mL (VISA or VRSA), an alternative to vancomycin should be used
Infectious Diseases Society of America (IDSA) 201152

Pharmacokinetics/Pharmacodynamics of Antibiotics: Refresher Part 2CHSPSC, LLC Antimicrobial Stewardship Education Series
ProCE, Inc.www.ProCE.com 27
Vancomycin DosingBased on total body weight and renal function
25 – 30 mg/kg (Initial Dose)
Normal renal function: q 12 dosing
Goal trough concentrations:
10 – 15 mcg/mL: skin and soft tissue infections
15 – 20 mcg/mL (or AUC/MIC > 400 mg.h/L) : bacteremia, osteomyelitis, meningitis, pneumonia
Obtain trough levels prior to the 4th dose of a new regimen (prior to the 3rd dose for patients with dosing intervals > 24 hours)
Rybak M. Am J Health Sys Pharm 2009;66:82Lui C Clin Infec Dis 2011;52:18 53
Vancomycin Dosing
DOSAGE ADJUSTMENTCreatinine Clearance
> 60 15 mg/kg Every 12 hrs
IV
40-60 15 mg/kg Every 24 hrs
IV
10-40 15 mg/kg Every 48-96 hrs
IV
< 10 15 mg/kg Every 4-7 days
IV
Hemodialysis: No supplementationTarget trough level is 15-20 mcg/mL.
Vancomycin 15 mg/kg Every 12 hrs
IV
Ohio State Dosing Guidelines 2017 - Pneumonia 54

Pharmacokinetics/Pharmacodynamics of Antibiotics: Refresher Part 2CHSPSC, LLC Antimicrobial Stewardship Education Series
ProCE, Inc.www.ProCE.com 28
55
VancomycinTherapeutic Drug Monitoring
• Monitoring of peak vancomycin concentrations is notrecommended
• Obtain serum troughs at steady state (before 4th or 5th dose)
• For most patients with SSTI with normal renal function and not obese, traditional doses of 1 g Q12 are adequate and trough monitoring is not required
• For serious infections (e.g. bacteremia, endocarditis, osteomyelitis, pneumonia, severe SSTI), target vancomycin trough concentrations of 15-20 g/mL
Moise-Broder Clin Pharmacokinet t2004;43:925-42 Jeffres Chest 2006; 130:947-55 Arbeit R CID 2004;38:1673-81 Stryjewski CID 2008;46:1683-93 Lipsky JAC 2005;55:240-5 Breedt AAC 2005; 49:4658-66
56

Pharmacokinetics/Pharmacodynamics of Antibiotics: Refresher Part 2CHSPSC, LLC Antimicrobial Stewardship Education Series
ProCE, Inc.www.ProCE.com 29
57
58
Related Documents











