Chronic Vesikobulosa Dermatosis Chronic Vesikobulosa Dermatosis • 1. Pemphigus • 2. Bullous Pemphigoid • 3. Dermatitis Herpetiformis • 4. Chronic Bullous Disease of Childhood • 4. Chronic Bullous Disease of Childhood • 5. Cicatrical Pemphigoid • 6. Gestationes Pemphigoid • 7. Bullous Epidermolysis

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Chronic Vesikobulosa DermatosisChronic Vesikobulosa Dermatosis
• 1. Pemphigus
• 2. Bullous Pemphigoid
• 3. Dermatitis Herpetiformis
• 4. Chronic Bullous Disease of Childhood• 4. Chronic Bullous Disease of Childhood
• 5. Cicatrical Pemphigoid
• 6. Gestationes Pemphigoid
• 7. Bullous Epidermolysis
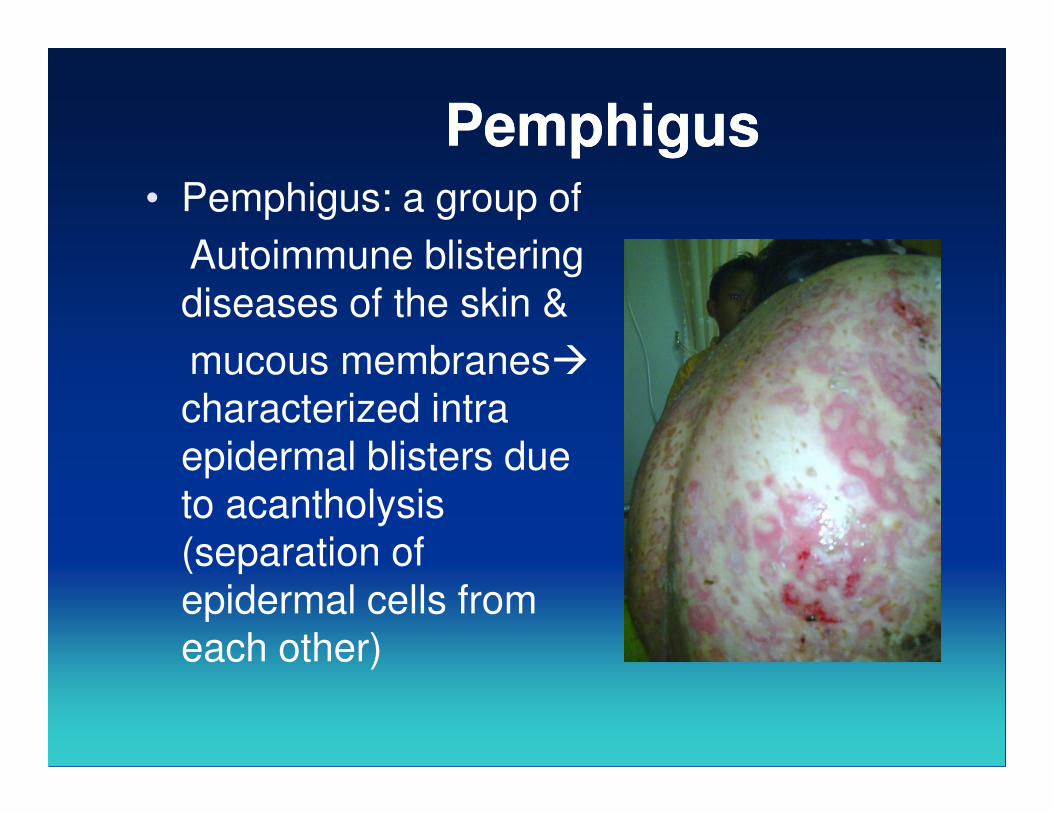
PemphigusPemphigus• Pemphigus: a group of
Autoimmune blistering
diseases of the skin &
mucous membranes�
characterized intra characterized intra
epidermal blisters due
to acantholysis
(separation of
epidermal cells from
each other)
Classification of PemphigusClassification of Pemphigus
Type Form
1. Pemphigus vulgaris P. Vegetans:
Localized
Drug-induce
2. Pemphigus foliaceus P. Erythematosus: localized
Fogo selvagem: Endemic drug
induce
3. Paraneoplastic pemphigus
IgA pemphigus Sub-corneal pustular dermatosis
Intraepidermal neutrophilic IgA
dermatosis
ImmunopathologicallyImmunopathologically
Bound and circulating IgG directed against the
cell surface of keratinocyte
P. Vulgaris (PV): blister in the deeper part of P. Vulgaris (PV): blister in the deeper part of
epidermis� above the basal
layer
P. Foliaceus (PF)= superficial pemphigus
� blister in the granular layer
ImmunofluorescenseImmunofluorescense
• The hallmark: IgG autoantibodies against the cell surface of keratinocyte (in pat’s serum� indirect IF
• Direct IF in PV & PF: IgG on the cell • Direct IF in PV & PF: IgG on the cell surface of KC in perilesional skin
• 80%> : pat. PV� circulating antiepithelial
cell surface IgG
Pemphigus antigenPemphigus antigen
- Desmogleins 3
- Transmembrane glycoproteins of desmosomes
(cell to cell adhesion structure)
� anti desmoglein 3 antibodies
anti desmoglein 1 antibodies
PV � affect predominnantly m. membrane :
only anti desmoglein 3 antibodies
PV mucocutaneus: anti desmg. 1 & 3 antibodies
Clinical ManifestationClinical Manifestation
Skin:
• Rarely pruritic� often painful
• Flaccid blister� arises on normal
appearing skin/ erythematous skin� fragile�
broken blister�erosions� often painfulbroken blister�erosions� often painful
erosions quite large� tendency to spread at
their periphery
Bulla> vesicles
Clinical ManifestationClinical Manifestation
• Nikolsky sign (+): active blister� applying lateral pressure to normal appearing skin
• Erosion� excessive granulation tissue &
crusting� intertrigenous areascrusting� intertrigenous areas
scalp, face
Mucous membrane: painful m. membrane
erosion ( 5 month
before skin lesion
develop)
Nikolsky sign (+)Nikolsky sign (+)
• Pemphigus
• Epidermolysis Bullosa
• Erythema Multiforme
• Toxic Epidermal Necrolysis• Toxic Epidermal Necrolysis
Clinical ManifestationClinical Manifestation• 52 % painful oral lesion� generalized in 5
months -1 year
• Some had oral lesions for > 5 years before generalization
• Intact blister are rare� because fragile &
break easily
Scattered� often extensive erosions (oral
cavity, buccal mocosa� pharynx, other
area)
Histopathology PVHistopathology PV
• Suprabasilar blister with acantholysis�
just above basal cell layer epidermal cells lose their normal cell to cell contact� form blister� KC in the blister cavityblister� KC in the blister cavity
basal layer stay attached to the BMZ�may lose the contact with their neigbors� row of tombstones
Bulla : intra epidermal/ supra basal
Tzanck TestTzanck Test
• To show acantholytic Epidermal cells
ImmunofluorescenceImmunofluorescence
• The hallmark: IgG autoantibodies against the cell surface of keratinocytes
• Indirect immnunofluorescence:• Indirect immnunofluorescence:
80 % pats. � have circulating
antiepithelial surface IgG
TreatmentTreatment
• Prednisone: high dose� disease activity is controlled� tapering pred.� low dose
• If combination immunosuppressive� dose intermediate/ low doseintermediate/ low dose
• Immunosuppressive:
mycophenolate mofetil (cellcept)
azathioprine (imuran)
cyclophoaphamide (cytoxan)
Bullous PemphigoidBullous Pemphigoid
• Usually occurs in elderly pat.
• Mortality 6%-40% in 1 year
• Pruritic urticarial lesions
• Tense large blisters• Tense large blisters
• Oral m. membrane erosions in minority of
pats
Direct Immunfluorescence C3 , IgG at epidermal basement membrane

Bullous pemphigoidBullous pemphigoid
ImmunofluorescenceImmunofluorescence
• Direct: C3 and IgG at epidermal basement membrane
• Indirect: antibasement membrane IgG in • Indirect: antibasement membrane IgG in serum
• Perilesional skin reveals immunoreactants deposited in linear pattern at epid basement membrane
AutoantigensAutoantigens
• Proteins in the Kc hemidesmosome a basal cell-basement membrane adhesion structurestructure
Etiology & pathogenesisEtiology & pathogenesis
• Electron microscopy: early blister formation occurs in the lamina lucida, between the basal cell membrane and the lamina densalamina densa
• Blister formation: there is loss anchoring filaments and hemidesmosome
degranulation of infiltrating leucocytes
ImmunofluorescenceImmunofluorescence
• Indirect IMF antibodies does not usually correlate with disease extent/ activity in contrast in pemphigus)
• C3 and other components classicals and • C3 and other components classicals and alternative complement pathways & complement regulatory protein B 1H� at BMZ
• Activated complement in blister fluid
Pemphigoid antigensPemphigoid antigens
• Immnunoelectron microscope: Ag in the hemidesmosome, an adhesion junction importants in anchoring the basal cell to BMZ
Clinical FindingsClinical Findings
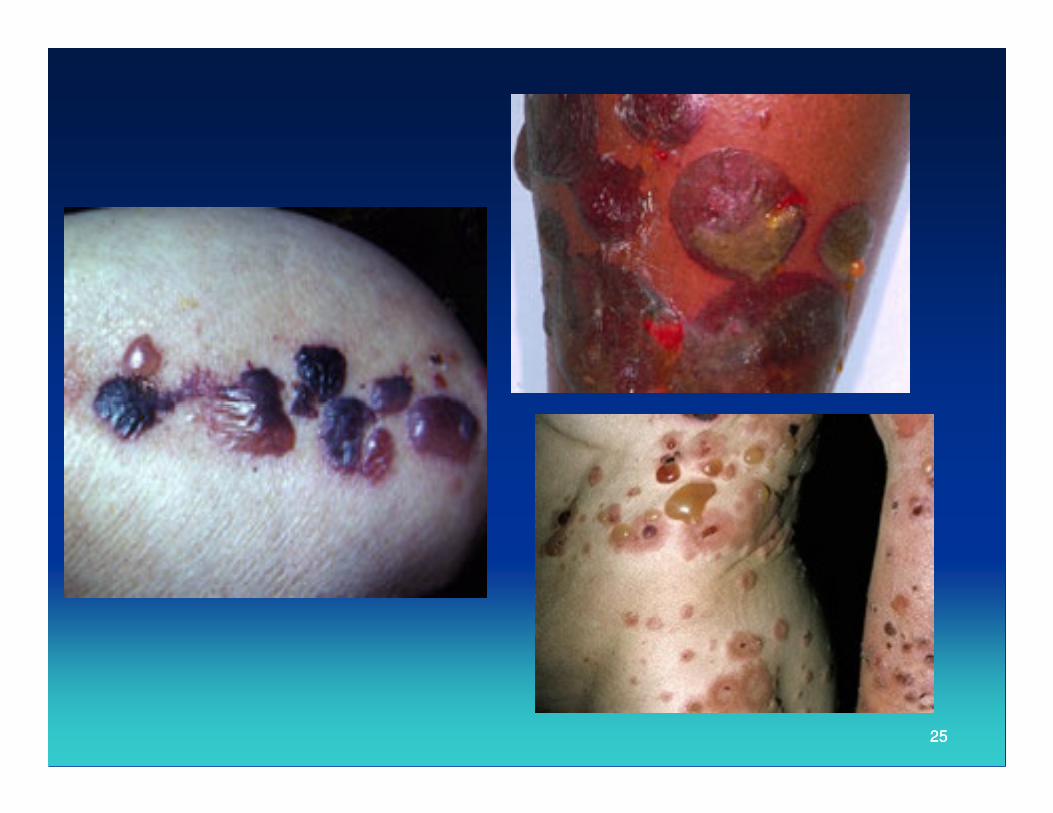
• Bullous: large, tense, arising in normal
skin/ erythematous base
filled : clear fluid/ hemorrhagic
Eroded skin� tendency to reepithelize
The erosion do not tend to expand at the The erosion do not tend to expand at the
periphery
• Localisation: lower abdomen
inner / anterior thights
flexor forarms/ any where
The lesion� do not scar
Clinical FindingClinical Finding
• Usually : pruritus
• Sometimes: erythematous component�pat. with urticarial lesion
• Resolution : from the center, • Resolution : from the center, hyperpigmentation
• M. Membrane : 10-35%� limited oral MM
(buccal mocosa)
TreatmentTreatment
Localized BP: topical steroids
topical tacrolimus
Extensive disease� oral prednisone:
1mg/kg BB/day 1mg/kg BB/day
once a day
�Topical thy 40 gr/day clobetasol propionate cream 0,05%� 2 x/day
Immonosupresive: azathioprine
2525
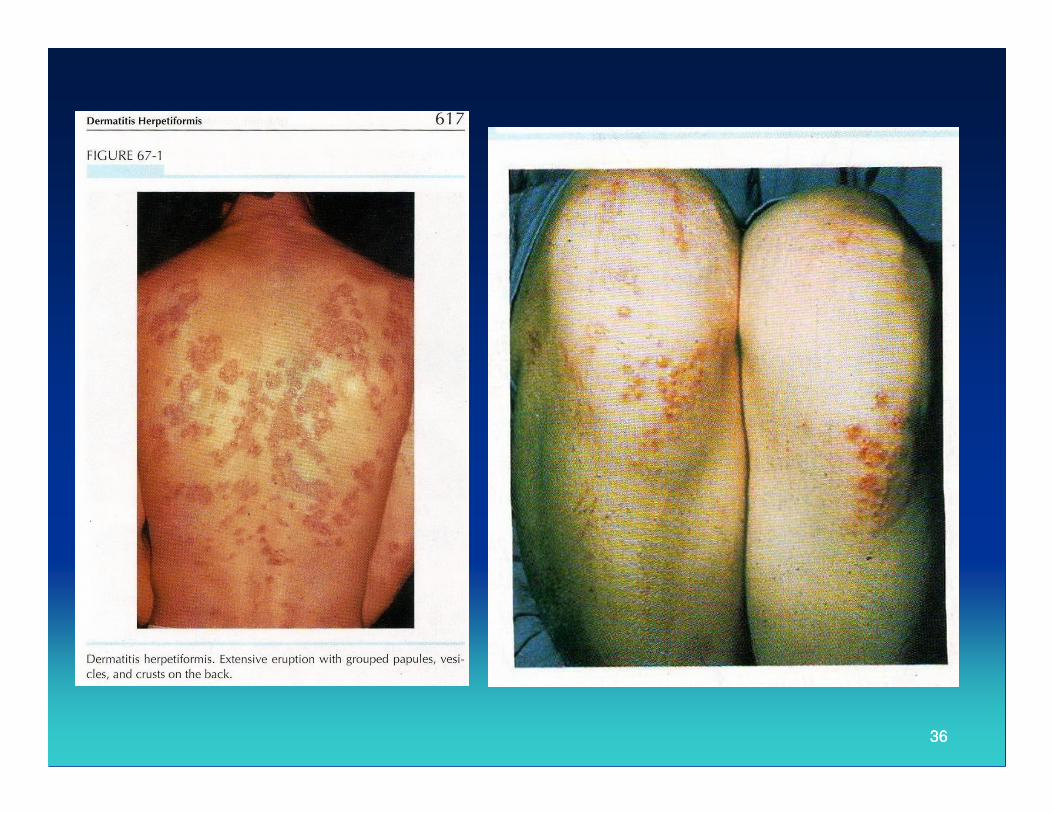
Dermatitis HerpetiformisDermatitis Herpetiformis
• Characterized by an intensely itchy
• Chronic papulovesicular eruption
• Distribution symetrically on extensor surfaces
• Clearly distinguished from other subepidermal • Clearly distinguished from other subepidermal
blistering erup. By histologic, immunologic,
Gastro Intest Criteria
• Any age
• Associated gluten sensitive enteropathy
Etiology and pathogenesisEtiology and pathogenesis
• Antibodies to tissue transglutaminases (Tigases) in sera from DH.
• Epidermal tigase is the dominant autoantigen in DHautoantigen in DH
• Gluten a protein found in wheat, barley, rye
-> play a critical role in pathogenesis in DH
Gastro abnormality in pat. DH (60-75%)
DiagnosticDiagnostic
• Granular immunoglobulin A deposits in nomal appearing skin
• Assocated gluten sensitive enteropathy• Assocated gluten sensitive enteropathy
Clinical ManifestationClinical Manifestation
• Primary lesion: erythematous papule
urticarial like plaque/
vesicles >>
Large bullae occure infrequentlyLarge bullae occure infrequently
Vesicles in palm: hemorrhagic
Disappearance : hyperpigmentation &
hypopigmentation
Herpetiform (herpes like): group of lesions
Clinical ManifestationClinical Manifestation
• Symptoms: severe stinging, burning,
itching
Symetric distribution:
elbows, knees, buttock, shoulders and elbows, knees, buttock, shoulders and sacral areas
Most pat: scalp lesions and/or nuchal posterior, face and facial hairline
M. Memb. : uncommon as in palms & sole
Laboratory TestLaboratory Test
• Perilesional and uninvolved skin pat DH: granular (or fibrillar) Ig deposits located in dermal papilary tips� igA
• IgA deposits are unaffected by treatment • IgA deposits are unaffected by treatment with drugs� may decrease in intensity or disappear after long term adherence to gluten free diet

Laboratory FindingLaboratory Finding
• IgA1 (produce in bone marrow) >
• IgA2 (produced in gut secretion)
• Complement (C3)� the same location as IgA
• C3� is not affected by treatment with dapson, • C3� is not affected by treatment with dapson,
may not detectable after teatment with gluten
free diet
• Immunoelectron Micrc: IgA associated with
bundles of microfibril, anchoring fibrils of the
papillary dermis below the basal lamina
Immunogenetic FindingsImmunogenetic Findings
• 77%-87% : HLA-B8
• Class II major histocompatibility complex : HLA-DR and DQ associated in DHHLA-DR and DQ associated in DH
HistopathologyHistopathology
• Early lesions (non vesicular)� dermal papillary collections of neutrophils (micro absces), neutrophilic fragments, eosinophil, fibrin� sometimes separation eosinophil, fibrin� sometimes separation of the papillary tips from the overlying epidermis
• Upper and middle dermal blood vessels are suurounded by lymphohistiocyte infiltrate
TreatmentTreatment
• Sulphones: diaminodiphenyl sulfone
(dapsone),
sulfoxone (diasone)
Dose: 100 mg-150 mg/day (once a day)Dose: 100 mg-150 mg/day (once a day)
occasional: 300-400 mg/day, 25 mg/week
Sulphapyridine: 1,0-1,5 gr daily
(in pat. intolerant of dapsone)
3636
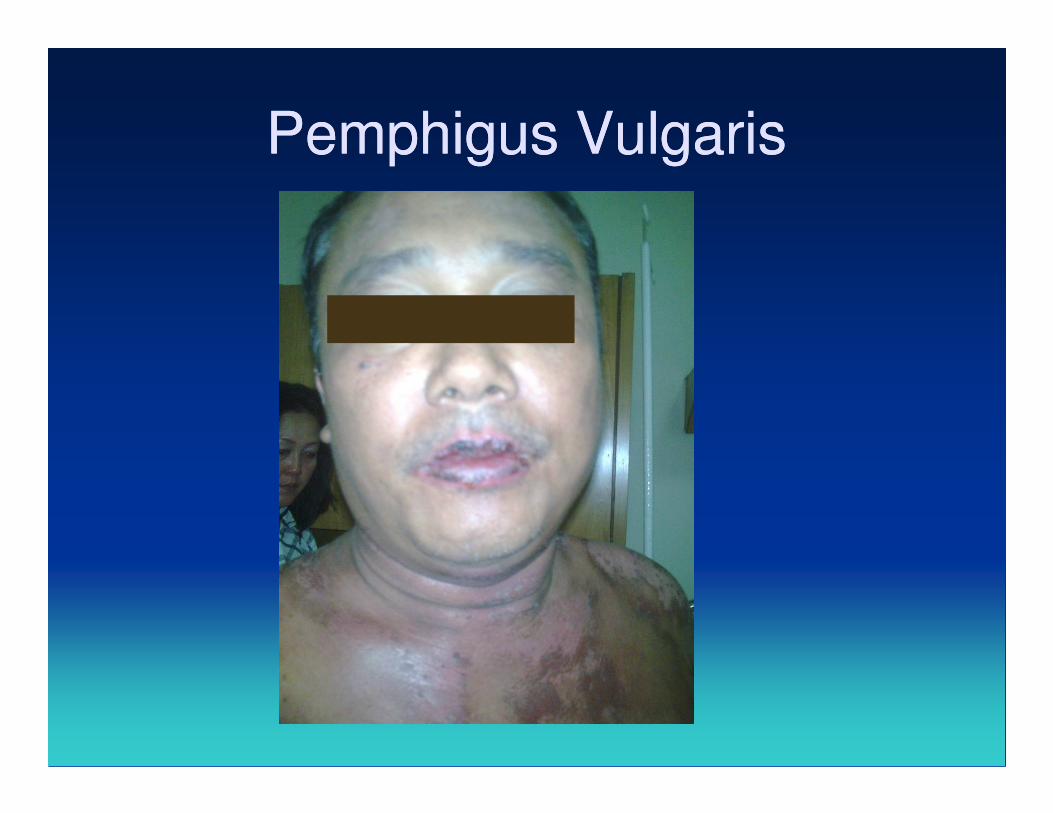
Pemphigus VulgarisPemphigus Vulgaris

Pemphigus VulgarisPemphigus Vulgaris
THANK YOU FOR LISTENINGTHANK YOU FOR LISTENINGTHANK YOU FOR LISTENINGTHANK YOU FOR LISTENING
Related Documents











