DOI 10.1378/chest.106.1.151 1994;106;151-155 Chest and Raúl Acosta Fabiola León-Velarde, Manuel Vargas, Luis Huicho, Alberto Arregui Lower Respiratory Tract Disorders Chronic Mountain Sickness and Chronic http://chestjournal.chestpubs.org/content/106/1/151 services can be found online on the World Wide Web at: The online version of this article, along with updated information and ISSN:0012-3692 ) http://chestjournal.chestpubs.org/site/misc/reprints.xhtml ( prior written permission of the copyright holder. this article or PDF may be reproduced or distributed without the Dundee Road, Northbrook, IL 60062. All rights reserved. No part of Copyright1994by the American College of Chest Physicians, 3300 Physicians. It has been published monthly since 1935. is the official journal of the American College of Chest Chest 1993, by the American College of Chest Physicians by guest on July 12, 2011 chestjournal.chestpubs.org Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

DOI 10.1378/chest.106.1.151 1994;106;151-155Chest
and Raúl AcostaFabiola León-Velarde, Manuel Vargas, Luis Huicho, Alberto Arregui Lower Respiratory Tract DisordersChronic Mountain Sickness and Chronic
http://chestjournal.chestpubs.org/content/106/1/151
services can be found online on the World Wide Web at: The online version of this article, along with updated information and
ISSN:0012-3692)http://chestjournal.chestpubs.org/site/misc/reprints.xhtml(
prior written permission of the copyright holder.this article or PDF may be reproduced or distributed without theDundee Road, Northbrook, IL 60062. All rights reserved. No part of Copyright1994by the American College of Chest Physicians, 3300Physicians. It has been published monthly since 1935.
is the official journal of the American College of ChestChest
1993, by the American College of Chest Physicians by guest on July 12, 2011chestjournal.chestpubs.orgDownloaded from

Chronic Mountain Sickness and ChronicLower Respiratory Tract Disorders*
Fabiola Leon-Velarde, D.Sc.; Alberto Arregui, M.D.;Manuel Vargas, M.D.; Luis Huicho, M.D.; and Raul Acosta, M.D.
To determine whether chronic lower respiratory tractdisorders contributed to the development of chronicmountain sickness (CMS), we compared hemoglobin(Hb), oxygen saturation (SaO2), peak expiratory flow rate(PEFR), and CMS scores (CMSsco) in 97 normal men athigh altitude with those of men at high altitude withacute (ARD; n=12), chronic upper (CURD; n=33), andchronic lower (CLRD; n=34) respiratory diseases. Theclinical diagnosis of the different types of respiratorydisorders was based on the results of a questionnaire andphysical examination performed during an epidemio-logic study. The CLRD group had higher CMSsco andHb concentrations, and lower SaO2 and PEFR valueswhen compared with the other groups. The frequency oflow PEFR and SaO2 and high Hb and CMSsco was sub-stantially higher in men with CLRD when comparedwith normal subjects. The results support the hypothe-
Chronic mountain sickness (CMS) or Monge's dis-ease was described more than six decades ago as
a process of loss of adaptation to life at high altitudes.Affected individuals, mostly adult men, complain ofheadaches, dyspnea, insomnia, dizziness, tinnitus,mental tiredness, confusion, depression, loss of ap-petite, and bone and muscle pains. They usually havedecreased exercise tolerance, intermittent or perma-nent cyanosis, venous dilatation in hands and feetand, in extreme cases, clubbing of the fingers andtoes.1 The disease has been described in differentmountain areas of the world: Peru',1-3 Bolivia,4 UnitedStates,5,6 Tibet, and China.7,8 An outstanding findingin patients with CMS is erythrocytosis that is dispro-portionately high for the altitude of residence.1'9
Hypoventilation has been accepted as a primarycause of CMS when there is no obvious pulmonarydisease;6"10'1' central depression of ventilation bychronic cerebral hypoxia, abnormalities matchingventilation to perfusion, and inefficient ventilationcontribute to hypoventilation.'2 Sime et al'3 havepostulated the sequence of hypoventilation, hypox-emia, excessive erythrocytosis, and CMS as a causal
*From the Departments of Physiological Sciences (Drs. Le6n-Velarde, Vargas, and Huicho), Neurology (Dr. Arregui), andMedicine (Dr. Acosta), Universidad Peruana Cayetano Heredia,Lima, Peru.Supported by grant 3-P-89-0247 from the International Devel-opment Research Centre, IDRC, Canada.
Manuscript received July 20, 1993; revision accepted December27.
sis that there is an association between signs andsymptoms of CMS, as measured by the CMSsco, andCLRD. The chronic hypoxemia, product of chronic lungdiseases, would cause excessive erythrocytosis and in-crease the signs and symptoms of CMS. Studies of Hb,PEFR, pulse oximetry, and CMSsco are recommendedfor early detection of high-altitude natives at risk of de-veloping CMS. (Chest 1994; 106:151-55)
ARD=acute respiratory disorder; CLRD=chronic lowerrespiratory tract disorder; CMS=chronic mountain sick-ness; CMSsco=chronic mountain sickness score; CURD=chronic upper respiratory tract disorder; PEFR=peak ex-piratory flow rate; SaO2=oxygen saturation
Key words: chronic mountain sickness; high altitude; hy-poxia; respiratory disorders
pathophysiologic relationship. These authors haveshown that loss of age-dependent ventilation leads toarterial hypoxemia and subsequent age-dependentpolycythemia. Likewise, the exaggerated hypoxemiaduring sleep has been stipulated to play a role in theaccentuation of hypoventilation and desaturation ofthe arterial blood at high altitude.'4"15A high body weight has been suggested to be an
additional risk factor in the development of CMS; itseems to play a role in lowering arterial oxygen sat-uration, and thus producing excessive erythrocytosis.At sea level, a clear correlation between hypoventi-lation and the syndrome of extreme obesity has beenfound,'6"7 and at high altitude, men with excessiveerythrocytosis have been found to have higher bodyweights when compared with men with physiologicerythrocytosis. 18Some authors have suggested that when CMS ap-
pears in the presence of a respiratory disorder, itshould be called secondary or type 2:3 Other authorshave questioned the existence of CMS as a primarypathologic entity and postulate that it is necessary toestablish its abnormality before it can be accepted asa distinct condition.'9 They suggest that some casesmay represent unrecognized respiratory dysfunctionin persons living at high altitude. Furthermore, notonly alveolar hypoventilation but also chronic ob-structive lung disease in some patients with CMS hasbeen suggested to be responsible for the exaggeratedhypoxemia characteristic of this disorder.20The purpose of this study was to investigate, with
CHEST/ 106/1 /JULY, 1994 151
1993, by the American College of Chest Physicians by guest on July 12, 2011chestjournal.chestpubs.orgDownloaded from

a population survey perspective, how the hypoxemiagenerated by chronic lung diseases was able toincrease both high-altitude polycythemia and theprevalence of other signs and symptoms of CMS(CMSsco) as an indication of the association of com-mon lower respiratory tract disorders with CMS.
METHODSAn epidemiologic survey was conducted among adult men
(46.3 percent of the total male population) with permanent res-idence (born, 87 percent, or living more than 10 years, 13 percent)in the mining town of Cerro de Pasco (4,300 m; total population:70,000). The sampling frame was constructed from updated mapsthat were detailed at the block level. A two-stage cluster samplewas chosen. The first stage was a simple random sampling ofblocks. The second stage was a simple random sampling of onehousehold per block in each of the blocks chosen in the first stage.The sample size was computed so as to obtain 95 percent confi-dence intervals at 5 percent significance for all the estimates andcomparisons of the variables of interest. The head of each familyanswered the survey questions, which had information regard-ing age, occupation, smoking history, and an inquiry about anyhealth-related complaint. Particular emphasis was given onsymptoms and signs of respiratory diseases and of CMS. If thesurveyed men had one or more complaints, a physician askedadditional questions and performed a detailed clinical examina-tion. A total of 345 men answered the survey.We elaborated a CMS score (CMSsco) based on the ten most
frequent symptoms and/or signs found in CMS and assigned avalue of 1 to negative answers and values of 2 and 3 to positiveanswers, "occasional" and "frequently," respectively. The mean+2 SDs deviations, ie, >21, was defined as a high CMSsco. Thesensitivity, specificity, and positive and negative predictive valuesfor each individual question when compared with a "gold stan-dard" (hemoglobin [Hb] >21.3 g/dl), have been reported else-where.21 In brief, the odds ratio for CMSsco was 1.57, the sensi-tivity was 0.17, the specificity was 0.91, the positive predictivevalue was 0.25, and the negative predictive value was 0.86 whencompared with the "gold standard" Hb >21.3 g/dl.2' This indi-cator was defined as the Hb value above 2 SDs of the normal dis-tribution curve of a 20- to 29-year-old high-altitude group at thesame altitude.18The criteria for the presence of acute (ARD), chronic upper
(CURD), and chronic lower respiratory disorder (CLRD) wasbased on currently accepted recommendations.22-24 The ques-tionnaire included a clinical assessment of dyspnea (age of onset,severity, insidious or abrupt onset), cough (productive or non-productive, duration throughout the months and years), wheez-ing (continuous or paroxysmal, age of onset), sputum production,recurrent respiratory infections, hemoptysis, sensation of chest
discomfort, and pleural pain. Physical features included signs oflung hyperinflation, increased respiratory muscle effort, alteredbreathing patterns, and abnormal breath sounds such as wheezesand diminished breath sounds, dry, crackling rales, and clubbingof the fingers or toes.The results of the questionnaire and physical examination al-
lowed us to separate men who were healthy (normal subjects),from those with ARD, CURD, or CLRD. We identified differentclinical syndromes when following current recommendationsproposed by the American Thoracic Society.22 Asthma, chronicbronchitis, and chronic obstructive lung disease were included inthe CLRD group; chronic sinusitis, allergic rhinitis, chronic otitismedia, and chronic pharyngitis were included in the CURDgroup. In 18 men, a definitive diagnosis could not be made. He-moglobin concentration was measured in a finger stick bloodsample using a portable hemoglobinometer ("Hemocue"). Oxy-gen saturation (SaO2) was measured by pulse oximetry using apulse oximeter (Nellcor), and peak expiratory flow rate (PEFR)was measured with a peak flow meter (Assess), recording thehighest of three PEFR readings. The PEFR values were expressedas a function of height and the flow meter readings were correctedfor high altitude by adding 6.6 percent per 100 mm Hg drop inbarometric pressure.25 Laboratory devices were checked beforeand after field studies. Hemoglobin and pulse oximetry wereperformed in all the surveyed subjects. The PEFR values wereavailable only for 176 men of whom 97 were normal, 12 had ARD,33 had CURD, and 34 had CLRD. These 176 subjects were mainlypart of the control group and do not differ from it in age, Hbconcentration, residence history, or any other relevant variable.The results were processed through a microcomputer using a
program (dBase plus 1.1) that was then translated to a statisticalpackage (SPSS Inc, SPSS/PC+ V2) for tabulation and analysis.Mean, median, variance, and standard deviation were deter-mined for continuous variables and comparisons among healthy,ARD, CURD, and CLRD groups were performed by analysis ofvariance. Analysis of covariance was used to compare slopes andintercepts of regression lines, and the Yates'-corrected x2 test wasused for analysis of discrete variables.
RESULTSMen with CLRD had higher Hb values and
CMSsco, and lower PEFRs and SaO2 values whencompared with normal men or men with ARD (Ta-ble 1). We compared the frequencies (percent) ofmen with excessive erythrocytosis (Hb >21.3 g/dl),low SaO2 values (SaO2 <81.5 percent), low PEFRvalues (PEFR <276 L/min), and high CMSsco(CMSsco >21) among the normal, ARD, CURD, andCLRD groups. The low SaO2 value of 81.5 percent
Table 1-Age, Hb, Sat 02, PEFR, and CMSsco in Healthy (Normal) Men at High Altitude Compared With MenWith Acute or Chronic Respiratory (tract) Disorders*
Normal ARD CURD CLRD(n=97) (n=12) (n=33) (n=34)
Age, yr 42.2 (10.5) 44.8 (8.7) 39.0 (10.5)t 44.4 (12.9)Hb, g/dl 18.8 (2.3) 19.3 (2.5) 18.6 (2.2) 20.2 (2.5)1Sat 02, % 84.9 (4.6) 84.0 (3.2) 84.7 (4.1) 83.0 (4.8)tPEFR, L/min/m 324 (52.2) 361 (53.8) 364 (65.7) 286 (61.2)§CMSsco 16.8 (3.2) 17.3 (1.8) 17.2 (2.8) 19.5 (4.3)4*Values are means (SD).tp<0.05.Jp<O.Ol.§p<0.001 when compared with normal subjects, and subjects with ARD, CURD, and CLRD.
Chronic Mountain Sickness (Leon-Velarde et al)152
1993, by the American College of Chest Physicians by guest on July 12, 2011chestjournal.chestpubs.orgDownloaded from
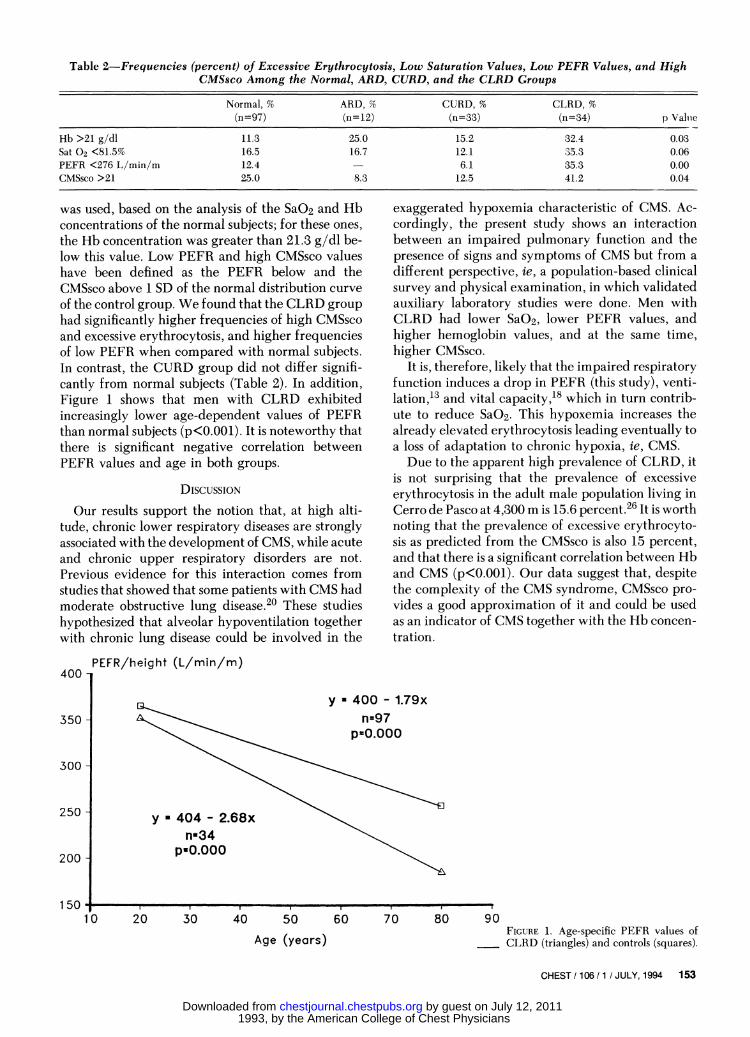
Table 2-Frequencies (percent) of Excessive Erythrocytosis, Low Saturation Values, Low PEFR Values, and HighCMSsco Among the Normal, ARD, CURD, and the CLRD Groups
Normal, % ARD, % CURD, % CLRD, %(n=97) (n=12) (n=33) (n=34) p Valuie
Hb >21 g/dl 11.3 25.0 15.2 32.4 0.03Sat 02 <81.5% 16.5 16.7 12.1 35.3 0.06PEFR <276 L/min/m 12.4 - 6.1 35.3 0.00CMSsco >21 25.0 8.3 12.5 41.2 0.04
was used, based on the analysis of the SaO2 and Hbconcentrations of the normal subjects; for these ones,the Hb concentration was greater than 21.3 g/dl be-low this value. Low PEFR and high CMSsco valueshave been defined as the PEFR below and theCMSsco above 1 SD of the normal distribution curveof the control group. We found that the CLRD grouphad significantly higher frequencies of high CMSscoand excessive erythrocytosis, and higher frequenciesof low PEFR when compared with normal subjects.In contrast, the CURD group did not differ signifi-cantly from normal subjects (Table 2). In addition,Figure 1 shows that men with CLRD exhibitedincreasingly lower age-dependent values of PEFRthan normal subjects (p<0.001). It is noteworthy thatthere is significant negative correlation betweenPEFR values and age in both groups.
DISCUSSION
Our results support the notion that, at high alti-tude, chronic lower respiratory diseases are stronglyassociated with the development of CMS, while acuteand chronic upper respiratory disorders are not.Previous evidence for this interaction comes fromstudies that showed that some patients with CMS hadmoderate obstructive lung disease.20 These studieshypothesized that alveolar hypoventilation togetherwith chronic lung disease could be involved in the
exaggerated hypoxemia characteristic of CMS. Ac-cordingly, the present study shows an interactionbetween an impaired pulmonary function and thepresence of signs and symptoms of CMS but from adifferent perspective, ie, a population-based clinicalsurvey and physical examination, in which validatedauxiliary laboratory studies were done. Men withCLRD had lower SaO2, lower PEFR values, andhigher hemoglobin values, and at the same time,higher CMSsco.
It is, therefore, likely that the impaired respiratoryfunction induces a drop in PEFR (this study), venti-lation,13 and vital capacity,18 which in turn contrib-ute to reduce SaO2. This hypoxemia increases thealready elevated erythrocytosis leading eventually toa loss of adaptation to chronic hypoxia, ie, CMS.Due to the apparent high prevalence of CLRD, it
is not surprising that the prevalence of excessiveerythrocytosis in the adult male population living inCerro de Pasco at 4,300 m is 15.6 percent.26 It is worthnoting that the prevalence of excessive erythrocyto-sis as predicted from the CMSsco is also 15 percent,and that there is a significant correlation between Hband CMS (p<O.OO1). Our data suggest that, despitethe complexity of the CMS syndrome, CMSsco pro-vides a good approximation of it and could be usedas an indicator of CMS together with the Hb concen-tration.
PEFR/height (L/min/m)
y U 400 - 1.79xn=97
p=0.000
y * 404 - 2.68xn334
pU0.000
20 30 40
I. -
50 60 70 80
Age (years)FIGURE 1. Age-specific PEFR values ofCLRD (triangles) and controls (squares).
CHEST / 106/1 / JULY, 1994 153
400 -
350 -
300 -
250 -
200 -
1501lc
l---
1993, by the American College of Chest Physicians by guest on July 12, 2011chestjournal.chestpubs.orgDownloaded from

There have been several contrasting positions tothe exclusive use of a clinical approach when diag-nosing CLRD, such as that used in our work. Badgettet al,24 however, have recently shown that the chanceof having chronic obstructive pulmonary disease wasvery unlikely in the presence of normal findings frommedical history and physical examination. In ourstudy, the diagnostic accuracy could be furtherstrengthened by evaluating pulmonary function withPEFR. This test has a good correlation with standardrespiratory function tests, namely: forced expiratoryvolume in 1 (FEV1), and forced vital capacity(FVC).27,28 Peak expiratory flow rate has been shownto be a useful tool in the clinical assessment of severalconditions such as bronchial asthma and other ob-structive and restrictive respiratory disorders,28,29and has proved to be a good indicator of respiratoryfunction in epidemiologic studies.30-32The hypothesis that age is a contributing factor in
the development of CMS is supported by our findingof a negative correlation between PEFR and age. Inthis regard, a longitudinal study performed in 12adult natives of the Peruvian Andes, and a mathe-matical analysis based on published data favored thesequence of events: aging, hypoventilation, hypox-emia, polycythemia, and development of CMS.13,33,34Our epidemiologic studies showing that the preva-lence of excessive erythrocytosis increases with ageand that there is a significant reduction of vitalcapacities with age are also in agreement with theabove chain of events.18'26
It has been shown that high-altitude natives havediminished ventilatory responses to acute hypoxia"land that chronic hypoxia desensitizes irreversibly thehyperventilation reflex response to acute hypoxiaduring the first 2 years of life.35 Although a "blunt-ed" respiratory response could lead one to proposethat it may act as a contributing factor in CMS, it ispresent in young high-altitude natives who rarelydevelop CMS. Furthermore, Grover and Kryger12have demonstrated that a low hypoxic ventilatoryresponse does not cause the hypoventilation andsubsequent hypoxemia. A "blunted" respiratory re-sponse does not mean diminished basal ventilatoryrates; it is instead a response to acute hypoxic situa-tions and not to the chronic hypoxia of high altitudes.Whereas we recognize that there remain severalquestions to be solved concerning the pathophysio-logic condition of CMS, our results indicate thatwhatever the primary cause of CMS may be, havinga CLRD appears to aggravate CMS by affecting res-piratory function; this, in turn, will decrease SaO2and increase Hb concentration. The high averagedCMSsco and high prevalence of high CMSsco foundin men with CLRD supports this proposition. Allthese laboratory findings seem to be useful instru-
ments in the assessment of the likelihood of devel-oping CMS.
REFERENCES1 Monge-M C, Encinas E, Heraud C, Hurtado A. La enfermedad
de los Andes. Ann Fac Med (Lima) 1928; 23:1-3142 Hurtado A. Chronic mountain sickness. JAMA 1942; 120:
1278-803 Arias-Stella J, Kruger H, Recavarren S. Pathology of chronic
mountain sickness. Thorax 1973; 28:701-084 Ergueta J, Spielvogel H, Cudkowicz L. Cardio-respiratory
studies in chronic mountain sickness (Monge's syndrome).Respiration 1971; 28:485-517
5 Hecht HH, McClement JH. A case of 'chronic mountain sick-ness' in the United States. Am J Med 1958; 25:470-77
6 Kryger MH, Grover RF. Chronic mountain sickness. In: PettyTL, Cherniack RM, eds. Seminars in respiratory medicine (vol5): man at altitude. New York: Thieme-Stratton; 1983; 164-68
7 Wu TY, Zhang Q, Chen QH, Jing BS, Xu FD, Liu H, et al.Twenty-six cases of chronic mountain sickness. Natl Med JChina 1987; 64:167-68
8 Pei SX, Chen XJ, Si Ren BZ, Liu YH, Cheng XS, Harris EM,et al. Chronic mountain sickness in Tibet. Q J Med 1989;266:555-74
9 Monge-M C, Monge-C C. High altitude diseases: mechanismand management. Springfield, Ill: Charles C Thomas Publisher,1966; 91
10 Kryger M, McCullough RE, Doekel R, Collins D, Weil JV,Grover RF. Excessive polycythemia of high altitude: role ofventilatory drive and lung disease. Am Rev Respir Dis 1978;118:659-66
11 Severinghaus JW, Bainton CR, Carcelen A. Respiratory insen-sitivity to hypoxia in chronically hypoxic man. Respir Physiol1966; 1:308-34
12 Grover R, Kryger M. Polycythemia of chronic mountain sick-ness. In: Adjustment to high altitude. Washington, DC: NationalInstitutes of Health, publication No. 83-2496, 1983; 37-42
13 Sime F, Monge CC, Whittembury J. Age as a cause of chronicmountain sickness (Monge's disease). Int J Biometeorol 1975;19:93-8
14 Kryger MH, Glas RD, Jackson RE, McCullough RE, ScogginCH, Grover RF, et al. Impaired oxygenation during sleep inexcessive polycythemia of high altitude: improvement withrespiratory stimulation. Sleep 1978; 1:3-17
15 Normand H, Vargas E, Bordachar J, Benoit 0, Raynaud J. Sleepapneas in high altitude residents (3,800 m). Int J Sports Med1992; 13(suppl 1):S40-S42
16 Hackney JD, Crane MG, Collier CC, Rokaw S, Griggs DE.Syndrome of extreme obesity and hypoventilation: studies ofetiology. Ann Intern Med 1959; 51:541-46
17 Auchincloss H Jr, Gilbert R. The cardiorespiratory syndromerelated to obesity: clinical manifestations and pathologic phys-iology. Prog Cardiovasc Dis 1959; 1:423-27
18 Le6n-Velarde F, Arregui A, Monge CC, Ruiz y Ruiz H. Agingat high altitudes and the risk of chronic mountain sickness. JWild Med 1993; 4:183-88
19 Heath D. Discussion. In: Porter R, Knight J, eds. Cor pulmon-ale in chronic mountain sickness: present concept of Monge'sdisease in high altitude physiology: cardiac and respiratory as-pects: A Ciba Foundation Symposium. Edinburgh: ChurchillLivingstone, 1971; 52
20 Sun SF, Huang SY, Shang JG, Droma TS, Banden G, McCul-lough RE, et al. Decreased ventilation and hypoxic ventilatoryresponsiveness are not reversed by naloxone in Lhasa residentswith chronic mountain sickness. Am Rev Respir Dis 1990;142:1294-1300
Chronic Mountain Sickness (Leon-Velarde et al)154
1993, by the American College of Chest Physicians by guest on July 12, 2011chestjournal.chestpubs.orgDownloaded from

21 Arregui A, Le6n-Velarde F. Puntaje de mal de montania cr6nico(pMMC): sensibilidad y especificidad [abstract]. Rev MedHerediana 1992; 3(suppl 1):5
22 American Thoracic Society. Standards for the diagnosis andcare of patients with chronic obstructive pulmonary disease(COPD) and asthma. Am Rev Respir Dis 1987; 136:225-43
23 Crystal RG. Interstitial lung disorders. In: Braunwald E, Issel-bacher KJ, Petersdorf RG, Wilson JD, Martin JB, Fauci AS, eds.Harrison's principles of internal medicine. New York: Mc-Graw-Hill Inc, 1987; 1095-1102
24 Badgett RG, Tanaka DJ, Hunt DK, Jelley MJ, Feinberg LE,Steiner JF, et al. Can moderate chronic obstructive pulmonarydisease be diagnosed by historical and physical findings alone?Am J Med 1993; 94:188-96
25 Thomas PS, Harding RM, Milledge JS. Peak expiratory flow ataltitude. Thorax 1990; 45:620-22
26 Arregui A, Le6n-Velarde F, Valcarcel M, Salud y Mineria. Elriesgo del mal de montania cronico entre mineros de Cerro dePasco. 1st ed. Lima, Peru: ADEC-ATC/Mosca Azul, 1990; 87-102
27 Kelly CA, Gibson GJ. Relation between FEV1 and peak expi-ratory flow in patients with chronic airflow obstruction. Thorax
1988; 43:335-3628 Morris MJ, Taylor AG. Peak flow measurements as screening
test for restrictive pulmonary disorders. Respir Med 1990;84:27-30
29 Banner AS, Shah RS, Addington WW. Rapid prediction of needfor hospitalization in acute asthma. JAMA 1976; 235:1337-38
30 Malik SK, Jindal SK, Jindal B, Bansal S. Peak expiratory lowrates in healthy adults. Ind J Chest Dis 1975; 17:166-71
31 Gregg I, Nunn AJ. Peak expiratory flow in normal subjects. BMJ1973; 4:282-84
32 Leiner GC, Abramowitz S, Small MJ, Stenby VB, Lewis WA.Expiratory peak flow rate. Am Rev Respir Dis 1963; 88:664-51
33 Whittembury J, Monge-C. High altitude, hematocrit, and age.Nature 1972; 238:278-79
34 Monge CC, Whittembury J. Chronic mountain sickness and thephysiopathology of hypoxemic polycythemia. In: Sutton JR,Houston CS, Jones NL, eds. Hypoxia: man at altitude. NewYork: Thieme-Stratton, 1982; 51-6
35 Sorensen SC, Severinghaus JW. Irreversible respiratory insen-sitivity to acute hypoxia in man born at high altitude. J ApplPhysiol 1971; 25:217-23
CHEST /106/ 1 / JULY, 1994 155
1993, by the American College of Chest Physicians by guest on July 12, 2011chestjournal.chestpubs.orgDownloaded from
DOI 10.1378/chest.106.1.151 1994;106; 151-155ChestRaúl Acosta
Fabiola León-Velarde, Manuel Vargas, Luis Huicho, Alberto Arregui andDisorders
Chronic Mountain Sickness and Chronic Lower Respiratory Tract
July 12, 2011This information is current as of
http://chestjournal.chestpubs.org/content/106/1/151Updated Information and services can be found at:
Updated Information & Services
http://chestjournal.chestpubs.org/content/106/1/151#related-urlsThis article has been cited by 5 HighWire-hosted articles:
Cited Bys
http://www.chestpubs.org/site/misc/reprints.xhtmlfound online at: Information about reproducing this article in parts (figures, tables) or in its entirety can bePermissions & Licensing
http://www.chestpubs.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
Reprints
"Services" link to the right of the online article.Receive free e-mail alerts when new articles cite this article. To sign up, select the
Citation Alerts
PowerPoint slide format. See any online figure for directions. articles can be downloaded for teaching purposes inCHESTFigures that appear in Images in PowerPoint format
1993, by the American College of Chest Physicians by guest on July 12, 2011chestjournal.chestpubs.orgDownloaded from
Related Documents








![Improved Detection of Sleeping Sickness Cases by …Both subspecies are cyclically transmitted by infected tsetse flies of the Glossina genus [1]. The chronic form of sleeping sickness](https://static.cupdf.com/doc/110x72/5f3ebb14546ae86eba7ad8a2/improved-detection-of-sleeping-sickness-cases-by-both-subspecies-are-cyclically.jpg)


