1 Chronic Leukemia

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
1
Chronic Leukemia

2
What Are the Types of Chronic Leukemia?

3
Classification of CL.
There are two types:
1-chronic myeloid leukemia. 2-chronic lymphoid leukemia.
4
Chronic Myeloid Leukemia.

5
Definition of CML:
Is a clonal disorder of a pluripotent stem cell and is classified as one of the myeloproliferative disorder.
Constitute six different types of leukemia.
• See table.
6
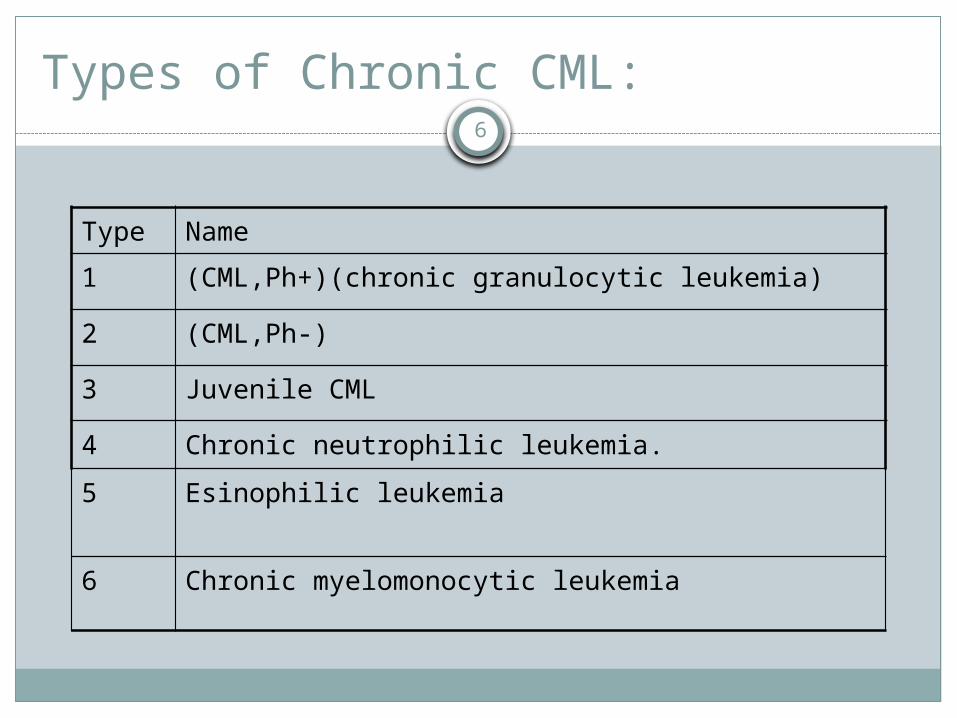
Types of Chronic CML:
Type Name
1 (CML,Ph+)(chronic granulocytic leukemia)
2 (CML,Ph-)
3 Juvenile CML
4 Chronic neutrophilic leukemia.
5 Esinophilic leukemia
6 Chronic myelomonocytic leukemia

7
Cont:
The disease accounts for around 15% of leukemia.
May occur at any age.

8
What Is Philadelphia Chromosome?
9
Philadelphia :
Is the chromosome which result from the t(9;22)(q34;q11)part of the Abelson proto-oncogene ABL is moved to the BCR gene on chromosome 22 & part of chromosome 22 moves to chromosome 9.
The abnormal chromosome 22is the Ph.
See fig.

10
Fig

11
How Would the Patient With CML Present?

12
Clinical Presentation:
It can occur in any age .But the most age presentation is between 40-60.
Symptoms related to hyper metabolism:(weight loss,lassitude,anorexia or night
sweats).(Gout or renal impairment caused by
hyperuriceamia ).Bone marrow failure:Anemia.
13
Cont:
Bruising ,epistaxis,menorrhagia or hemorrhage from any site because of platelet dysfunction.
Organ infiltration:Splenomegally almost always present and is
frequently massive.Rare symptoms include visual disturbance.
14
How Would You Investigate the Patient With Suspected CML?….

15
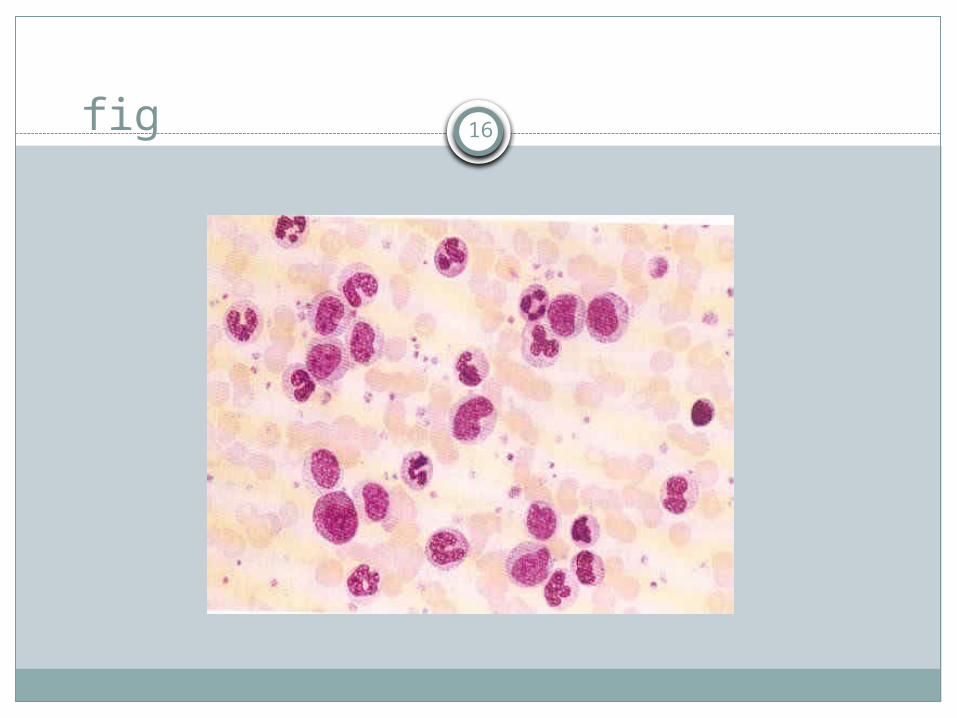
Investigation:
CBC:Wbc is usually >50X10/l & some times
>500X10/l.Normocytic normochromic anemia.Platelets .
peripheral blood film:Ý circulating basophil.
16fig

17
Cont:
Neutrophil alkaline phosphatase score is invariably low.
BM: is hyper cellular with granulopoietic predominance.
Cytogenetics: ph chromosome.Serum vitamin B12 & vitamin b12-binding
capacity are.Serum uric acid is usually.

18
What Are the Phases of CML?…
19
Phases of CML:
Chronic phase :Accelerated phase:Blast phase:

20
How Would You Treat CML?…

21
Treatment:
Chemotherapy:Tyrosine kinase inhibitor:Interferon-.Stem cell transplant.

22
What Is the Course and Prognosis of CML?..
23
Course & prognosis:
Usually shows excellent response to chemtherapy in the chonic phase.
Death usually occur from terminal acute trasformation ,hemorrhage or infection.

24
Chronic lymphocytic Leukemia:
25
Introduction:
CLL is the most common of the chronic lymphoid leukemias.
Peak incidence between 60-80yrs.It is characterize by chronic persistent
lymphocytosis which later infiltrate different organs.

26
What Is the Clinical Presentation?

27
Clinical presentation:
The disease occurs in older subject,rare before 40yrs.
M:F is 2:1.Many cases discover routinely.Symmetrical enlargement of superficial
lymph node is the most frequent clinical sign.Feature of anemia.
28
Fig(1)
29
Cont:
Splenomegaly & hepatomegaly usual in later stage.
Repeated bacterial or fungal infection.
Thrombocytopenia.

30
Fig(2)
31
How would you investigate patient with CLL?..

32
Investigation:
CBC: Wbc:. Diff:lymphocytosis ,the absolute lymphocyte count
is>5x109/l and may be up to 300x109/l or.More.
Anemia:normocytic normochromic anemia is present in later stages,autoimmune haemolysis.
Platelets : thrombocytopenia may occur.

33
Cont:
Blood film:70-99% of white cells mature lymphocyte.
Smudge or smear cells also present.Immunophenotyping:Shows that the lymphocyte are B cells(CD19)expressing
one form of light chain( or only)cells are also CD5&CD23+ve.

34
Fig(3)
35
Cont:
Bone marrow aspiration:Lymphocytic replacement of normal marrow.
Immunoglobulinelectrophoresis:¯ of Ig more marker with advance disease.• Cytogenetic :The 4 most common abnormalities are;
deletion of13q14,trisomy 12,deletion of11q23&structural abnormality of 17p involving the p53 gene.

36
What Is the Staging of CLL?…
37
Staging :
Staging is very important for prognosis and treatment.
There are two staging system(Rai and Binet).
See table.

38
A-Rai Classification:
Stage definition
0 Absolute lymphocytosis >15x109/l.
1 Stage 0+enlarged lymph nodes.
11 Stage 0+liver or/and spleen adenopathy.
111 Stage 0+anemia organomegally or adenopathy.
1V Stage 0+thrombocytopenia organomegally or adenopathy.

39
B-Binet Classification:
Stage . Organomegally.
Hb Platelet.
A(50-60%) 0,1,or2areas
B(30%) 3,4,or 5areas 10 100
C(<20%) Not considered <10 and /or <100

40
How Would You Treat Patient With CLL?…

41
Treatment :
Since cure is rare,the treatment aim is only symptoms control.
Indication for treatment: Troublesome organomegaly. Hemolytic episodes. Bone marrow suppression.

42
Modality of Treatment:
1-chemotherapy:Chlorambucil: 6mg/m2 daily for 10 days monthly for
2-4 month after which remission will be obtain.
Fludarabine:more effective as single agent.
Corticosteroid :indicated in bone marrow failure,also indicated in autoimmune hemolytic anemia and thrombocytopenia.

43
Cont:
2-Radiotherapy:Is useful in reducing the size of lymphnode not
responsive to chemo.3-Monoclonal antibody:Both campath IH(anti CD52)and
Rituximab(anti CD20)produce response in proportion of patient.

44
Cont:
4-Splenectomy :For immune-mediated cytopenia or painful
bulky splenomegally.
5-immunoglobulin replacement:250mg/kg /month by IV for patient with
hypogammaglobulinemia and recurrent infection.

45
Cont:
5- Stem cell transplant:Under clinical trial.

46
Good Luck!……..
Related Documents











