http://lan.sagepub.com/ Laboratory Animals http://lan.sagepub.com/content/38/4/362 The online version of this article can be found at: DOI: 10.1258/0023677041958990 2004 38: 362 Lab Anim Lane Smith, M. Hakam Tiba, Mary Ellen Goldberg and R. Wayne Barbee Chronic implantation of transit-time flow probes on the ascending aorta of rodents Published by: http://www.sagepublications.com On behalf of: Laboratory Animals LtdLaboratory Animals Ltd can be found at: Laboratory Animals Additional services and information for http://lan.sagepub.com/cgi/alerts Email Alerts: http://lan.sagepub.com/subscriptions Subscriptions: http://www.sagepub.com/journalsReprints.nav Reprints: http://www.sagepub.com/journalsPermissions.nav Permissions: What is This? - Oct 1, 2004 Version of Record >> by guest on November 23, 2013 lan.sagepub.com Downloaded from by guest on November 23, 2013 lan.sagepub.com Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

http://lan.sagepub.com/Laboratory Animals
http://lan.sagepub.com/content/38/4/362The online version of this article can be found at:
DOI: 10.1258/0023677041958990
2004 38: 362Lab AnimLane Smith, M. Hakam Tiba, Mary Ellen Goldberg and R. Wayne Barbee
Chronic implantation of transit-time flow probes on the ascending aorta of rodents
Published by:
http://www.sagepublications.com
On behalf of:
Laboratory Animals LtdLaboratory Animals Ltd
can be found at:Laboratory AnimalsAdditional services and information for
http://lan.sagepub.com/cgi/alertsEmail Alerts:
http://lan.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- Oct 1, 2004Version of Record >>
by guest on November 23, 2013lan.sagepub.comDownloaded from by guest on November 23, 2013lan.sagepub.comDownloaded from

Various rodent species continue to gain popularity as experimental models in physio-logical studies due to the availability ofmicrosurgical monitoring devices and therising costs of large-animal research.Increasingly, rat and mouse strains arechronically instrumented for long-termmonitoring of haemodynamic parameterssuch as cardiac output and arterial bloodpressure (Smith et al. 1987, Tsui et al. 1991,Doursout et al. 2001). While the availabilityof small-animal anaesthestic machines has
facilitated the use of rodents for haemody-namic studies, there have been fewbreakthroughs in intubation techniques tofacilitate chronic instrumentation involvingthe thoracic cavity for small-animalresearch.
The implantation of transit-time flowprobes on the ascending aorta of rodents isone example of this chronic instrumenta-tion that requires general anaesthesia, intu-bation, microsurgical probe placement, andclose postoperative monitoring. Proper tech-nique at all stages is vital to insure that theprobe implantation does not adversely affectthe animal’s response to future studies—especially if these studies involve haemody-namic stress such as hypoxia and shock.
Chronic implantation of transit-time flowprobes on the ascending aorta of rodents
Lane Smith1,2, M. Hakam Tiba2, Mary Ellen Goldberg3,4 & R. Wayne Barbee1,2
Departments of 1Physiology, 2Emergency Medicine, 3Physical Therapy and 4Anatomy andNeurobiology, Virginia Commonwealth University Reanimation Engineering and Shock Center,Virginia Commonwealth University Health System, Richmond, Virginia, USA
Summary
This study describes the implantation of transit-time flow probes on the ascending aorta ofrats while minimizing the risk of postoperative complications. Special emphasis is placedon our new method of rat intubation as well as the production of materials necessary forthe implantation procedure such as endotracheal tubes and heparin bonded vessel catheters.The effects of these devices on the response to acute hypoxia were studied in rats followinga 5–7 day recovery from the implantation procedure. Systemic and microvascular measure-ments were made on instrumented rats (n �5) and non-instrumented controls (n �3) thatwere ventilated with 21%, 15%, 10%, 8% and 5% oxygen. Arterial pressure, PO2, lactate,and base deficit were not different between the implanted and control animals at anyinspired oxygen concentration. Microvascular flow in the primary arterioles of the spino-trapezius muscle was also similar between the two groups at all inspired oxygen concentra-tions. We conclude that this novel methodology facilitates the measurement of whole bodyoxygen delivery in resting and haemodynamically-stressed rats.
Keywords Postoperative care; endotracheal intubation; operative surgical procedures;blood flow; red blood cell velocity; rheology; methods
Accepted 15 March 2004 © Laboratory Animals Ltd. Laboratory Animals (2004) 38, 362–370
Correspondence to: Mary Ellen Goldberg, VirginiaCommonwealth University, Departments of PhysicalTherapy, Anatomy and Neurobiology, PO Box 980224,Richmond, VA 23298–0224, USAE-mail: [email protected]
by guest on November 23, 2013lan.sagepub.comDownloaded from

Laboratory Animals (2004) 38
This study describes the implantation ofaortic flow probes in rats and the aftercarethat is necessary to maintain the animalsfor subsequent studies. Included in thedescription is a new method to simplifyrodent intubation and maintain the animalsunder general anaesthesia. We also comparethe systemic and microcirculatory responsesto hypoxia in non-instrumented animals,and animals that are chronically instru-mented with aortic flow probes to helpdetermine the suitability of these devicesfor use in animals subjected to severehaemodynamic stress such as shock.
Materials and methods
AnimalsThis study was approved by the VirginiaCommonwealth University’s InstitutionalAnimal Care and Use Committee protocolnumber 0009-2852. The animals werehoused in the vivarium until the day ofthe procedure. Outbred male Wistar Kyoto(WKY) rats (Harlan Sprague DawleyLaboratories, Indianapolis, IN; n �5),200–300 g, 49–75 days old, were housedin plastic containers (Allentown CagingEquipment Company) containinglaboratory-grade pine shavings (Teklad®)at 20–23�C, 12:12 h light/dark, humidity40–70%, 15 air changes/hour and allowedaccess to food (Teklad® RodentMaintenance Diet) and water (potable,uncontaminated) ad libitum until theexperiment. Postoperatively, the animalswere returned to the vivarium only afterthey were ambulatory and fully recovered.
Intubation and catheter productionOral intubation catheters were producedfrom polyethylene (PE-190) tubing (ClayAdams, Parsippany, NJ), and made to fit ratsweighing 200–300 g. Although the diameterof the tubing can be reduced for smalleranimals, sizes less than PE-120 posedproblems when used in conjunction withpressure-controlled ventilators due toincreased airway resistance.
To achieve a tight airway seal, thecatheters were bonded with self-levellingsilicone rubber sealant (734 RTV, DowCorning, Midland, MI) to form a teardrop-shaped terminus at the tracheal end (Fig 1).This was accomplished by applying a smalldrop of the sealant one centimetre above thetracheal end and gently rotating the catheterat a 45-degree angle to form the neededteardrop shape. The sealant’s surface wascured in approximately 15 min, and com-plete curing occurred after 24 h. Great carewas taken to leave sufficient catheter length(one centimetre for a 250 g rat) at thetracheal end to pass through the glottis.
Rodent intubationThe animals were administered atropine(300 mg/kg, i.p.) to minimize pharyngealsecretions, and underwent anaesthesiainduction with isoflurane (5%, balance O2;Abbott Laboratories, North Chicago, IL)administered in a standard induction cham-ber (Harvard Apparatus, Holliston, MA)with a gas vaporizer (Harvard Apparatus).Once the animals reached stage III anaesthe-sia (shallow respirations with 1–2 s pauses
Chronic flow probe in rats 363
Fig 1 (a) Intubation catheter with teardrop bulbproduced from PE-190 tubing along with a styletproduced from PE-50 tubing. The stylet shouldextend approximately 2 cm from the tracheal end ofthe intubation catheter for easy guidance into theglottis. (b) Vessel catheter produced by fusing PE-60and PE-20 tubing with Superglue. Scale shown byruler in centimetres
by guest on November 23, 2013lan.sagepub.comDownloaded from

Laboratory Animals (2004) 38
between breaths), intubation was accom-plished with the previously describedintubation catheters and a fibreoptic laryn-goscope set with a size 0 Miller blade(Harvard Apparatus). The laryngoscope bladewas narrowed to one centimetre width inorder to accommodate the animals’ oralpharynx. We constructed a Plexiglasintubation platform consisting of a base(15 cm �30 cm) and an appendage(15 cm �40 cm, attached to the base at a60-degree angle) that suspended the animalsby the upper jaw from a copper cord heldby a pair of 3 cm screws (Fig 2). This posi-tion maximized displacement of pharyngealstructures by gravity, and allowed theoperator to comfortably visualize theairway. Directing the large intubationcatheter into the airway was facilitated bythreading an 8 cm length of PE-50 tubingthrough the intubation catheter to form astylet that extended 3 cm past the catheter’stracheal tip as seen in Fig 1. The stylet wasdirected into the trachea, and the intubationcatheter slid over the length of PE-50 untilthe silicone bulb wedged into the glottis to
form a tight airway seal. The animals weremechanically ventilated (inspiratory pres-sure �10 cmH2O, frequency 1.5 Hz) with arodent ventilator (Kent Scientific, Litchfield,CT), and gas anaesthesia titrated to stage IIIanaesthesia. Ophthalmic ointment(Puralube Vet Ointment, Melville, NY)was applied to each animal to preventpost-surgical irritation.
Placement of flow transducers on ascending aortaEach animal was shaved along the chest andnape of the neck using clippers (OsterGolden A5, Sunbeam Products Inc.,McMinnville, TN) with a size 40 blade.Nair™ depilatory cream (Carter-Wallace,Inc., New York, NY) was applied to theshaved surfaces to remove remaining hair.Final preparation of the shaved areasinvolved cleaning the entire surgical fieldwith Betadine® (povidone-iodine 7.5%).
Using sterile techniques, a small skinincision was made at approximately thethird intercostal space along the right mid-axillary line. The skin incision was extendedtoward the midline while taking great careto avoid bleeding from cutaneous vessels.After removing the overlying connectivetissue, the exposed pectoral musclewas transected, and sutures placed in themuscle’s free ends for future repair. Oncethe pectoral muscle was severed, the under-lying rectus muscle was dealt with in thesame way to reveal the ribs and intercostalspace.
The third intercostal space was identifiedas the second space encountered whencounting in a caudal direction from theaxilla. Metzenbaum scissors were used todissect through the third intercostal space atthe mid-axillary line while taking care toavoid damaging the underlying lung.Complications from the thoracotomy wereminimized by momentarily suspendingventilation with the lungs deflated just priorto dissection, or ventilating with lowend-tidal pressures (4–5 cmH2O) and highfrequencies (�2 Hz). In addition, we dissectedjust above the fourth rib to avoid the inter-costal neurovascular bundle positioned
364 Smith et al.
Fig 2 Intubation technique performed with afibreoptic laryngoscope on a specially designedintubation table. Suspending the anaesthetizedanimal by the upper jaw at a 60-degree anglefacilitated anterior displacement of pharyngealstructures
by guest on November 23, 2013lan.sagepub.comDownloaded from

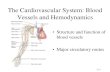
below each rib. The initial thoracotomyincision was extended no closer than 2 mmto the sternum to avoid damaging the adja-cent mammary artery. Adequate visualiza-tion of the thoracic contents was achievedby spreading the incision with an Almretractor as seen in Fig 3. Mechanical venti-lation was then resumed at slightly lowerinspiratory pressures (5–10 cmH2O) andhigher frequencies (1.5–2 Hz) to keep theright lung out of the immediate surgicalfield.
Access to the ascending aorta wasachieved by displacing the overlying thymusgland and thin pericardium as seen in Fig 3.Once the aorta was identified, the surround-ing fascia was cleared by passing curvedforceps between the aorta and the vertebralcolumn. After clearing the fascia, it waspossible to slide the probe (model 2.5SB,Transonic Systems, Inc., Ithaca, NY) underand around the aorta with forceps. Greatcare was taken to insure that no abnormaltension was placed on the probe that mighthamper blood flow.
Prior to closing the animal’s chest, athoracostomy tube was placed for futureevacuation of the pneumothorax producedby the thoracotomy. This was accomplishedby making a 3 mm incision at the level ofthe fourth intercostal space along the rightmid-axillary line. A 10 cm length of silastictubing with multiple holes along its distalend was inserted into the pleural space, andthe incision closed with a purse-stringsuture. Once the chest was closed, thissuture was tightened to create an airtightseal for evacuation of the pneumothorax.
Closure of the thoracotomy proceeded inlayers beginning with the approximation ofthe third and fourth rib with 5-0 silksutures. The free ends of the rectus andpectoral muscles were then approximatedvia the sutures that were placed during theinitial dissection. Once the pectoral musclewas repaired, the probe’s cord was directedunder the right forelimb, and tunnelled to aone centimetre incision at the nape of theneck. This involved attaching a length ofsuture material to the probe’s protectivecover, and pulling the suture-probe assemblythrough the neck incision. The probe wasexteriorized to a silastic saddleback cuff(model AAPC102, Transonic) that wassutured to the skin with 4-0 nylon sutures.Great care was taken to place the probeassembly between the scapular regions ofthe neck and avoid contact with the ears.Additionally, the cutaneous layers of thethoracotomy incision were closed with 4-0nylon sutures.
After closing the chest, the animal’spneumothorax was evacuated by applying avacuum to the thoracostomy tube, whilesimultaneously increasing the peak airwaypressures to 20 cmH2O with a ‘sigh’ (main-tained end-expiratory breath) setting. As thepneumothorax was evacuated, the tube waswithdrawn, and tension increased on thepurse-string suture so that the thoracostomyincision sealed during removal of the tube.
After evacuating the pneumothorax, theanimal was weaned from the ventilator byreducing the gas anaesthesia to 0.5% andlowering the respiratory rate to 40 perminute. This allowed the animal’srespiratory drive to recover in response to
Fig 3 A view of the thoracic contents once theAlm retractor is placed in the third intercostalspace. The middle and upper lobes of the right lung are in the immediate field, can be pushedaside for viewing of the heart and aorta. Retractionof the thymus gland with forceps reveals theascending thoracic aorta
Chronic flow probe in rats 365
Laboratory Animals (2004) 38 by guest on November 23, 2013lan.sagepub.comDownloaded from

Laboratory Animals (2004) 38
the increased arterial PCO2. Once sponta-neous respirations returned, the animal wascompletely removed from the ventilator andextubated.
Postoperative care of the chronicallyinstrumented rodentBecause the probe required a connectivetissue ‘seal’ to prevent absorption of theultrasound signal by air, it was necessaryto wait 5–10 days from the time ofimplantation before further experimenta-tion. Thus, proper postoperative care ofthe instrumented animals was importantfor recovery during this period. Thebroad-spectrum antibiotic Enrofloxacin(2.5 mg/kg, i.p.) was administered immedi-ately before or after implantation to preventpost-surgical infection. Adequate paincontrol was generally achieved with a0.3 mg/kg subcutaneous dose of buprenor-phine that was administered when theanimal achieved ventral recumbence.Tylenol® (acetaminophen) was added to thedrinking water at a concentration of2 mg/ml to achieve a dose of 150 mg/kg/dayif additional pain relief was necessary. Theanimal’s body weight was closely monitoredduring the recovery period, as weight losswas a sign of distress. Any animal that didnot recover to its post-surgical body weightwithin 2 weeks was excluded from furtherstudies.
Vessel catheter productionPlacement of catheters in the blood vesselsof rodent species for acute and chronichaemodynamic monitoring is well describedin the scientific literature (Tsui et al. 1991,Burvine et al. 1998). However, this proce-dure becomes problematic when attemptedon small vessels (e.g. rat femoral artery), orwhen significant blood withdrawal isdesired. Typically, catheters smaller thanPE-60 experience problems with bloodclotting due to slow flow during bloodwithdrawals, small-tip diameters, and aprothrombotic state during haemorrhage(Bit-Alkhas Irani & Cliffton 1970).Unintentional haemodilution is a potential
result when repeated saline flushes are usedto remove catheter clots.
To accommodate small vessels and mini-mize clotting problems, we fused differentsizes of PE tubing to form a catheter that issmall enough at the tip to fit the desiredvessel and maximize flow during bloodwithdrawal. For cannulation of the ratcarotid artery, fused lengths of PE-20 andPE-60 were made. This was accomplishedby applying a thin coat of Superglue to thedistal 2 mm of a 2 cm length of PE-20tubing. Then, the glued end of the PE-20tubing was carefully threaded into thelumen of an 8 cm length of PE-60 tubing asseen in Fig 1. Great care was taken toprevent obstruction of the catheters’lumens, and to insure a complete sealbetween the catheter walls.
Once the Superglue cured, the catheterswere bonded with heparin to further reducethe incidence of catheter clotting. This wasaccomplished by filling and immersing thecatheters in tridodecylmethylammoniumheparinate (TDMAC-heparin; Polysciences,Inc.; Warrington, PA) at a concentration of3500 units/ml for a minimum of 12 h(Chitwood et al. 1978). The TDMAC-heparin was then displaced with air, andthe catheters rinsed with sterile saline aminimum of three times. Because theTDMAC-heparin solution is an inflammableskin and eye irritant, the bonding procedurewas performed under a ventilation hoodwith proper eye and hand protection.
Determination of systemic andmicrovascular haemodynamic parametersFollowing the recovery period, the instru-mented WKY rats (n �5) and a group of non-instrumented WKY controls (Harlan SpragueDawley Laboratories, Indianapolis, IN; n �3)were initially anaesthetized with a mixtureof ketamine/xylazine (70/3 mg/kg, i.p.). Thetrachea was cannulated with PE-240 tubingvia tracheotomy, and the animals weremechanically ventilated with room air(inspiratory pressure �10 cmH2O, frequency1.5 Hz). The carotid and jugular vessels werecannulated with the previously describedheparin-bonded catheters. Red blood cells
366 Smith et al.
by guest on November 23, 2013lan.sagepub.comDownloaded from

(RBCs) labelled with fluorescein isothio-cyanate (FITC) were injected (1% labelledfraction assuming blood volume equal to6% body weight) through the jugularcatheter using the procedure described byLipowsky et al. (1992) for future determina-tion of microvascular RBC velocity andblood flow (Sarelius & Duling 1982,Parthasarathi et al. 1999). The carotidcatheter was used for phasic recording of arterial pressure with a Biopac data acquisition system (model MP150, BiopacSystems, Inc., Santa Barbara, CA), while acontinuous infusion of the anaestheticSaffan (0.2–0.4 mg/kg/min, York, UK) wasadministered through the jugular catheter.In addition, the Biopac was used to recordaortic flow and calculate heart rate in theinstrumented animals.
The spinotrapezius muscle was preparedaccording to the method originallydescribed by Gray (1973). The muscle wasspread to its physiological length on a view-ing platform that was heated to 39�C bywarm water, and the preparation was covered with Saran (Dow Corning, Inc.) to prevent desiccation. The platform wasattached to the stage of a Zeiss Universalmicroscope equipped with a Neofluar40�/0.75 N.A. objective (Carl Zeiss) formicroscopic viewing of the spinotrapeziusmuscle.
Baseline heart rate, phasic arterial pres-sure, and aortic flow (instrumented animalsonly) were determined online while theanimals were ventilated with room air.Video recordings of primary arterioledimensions and FITC labelled RBC velocitywere made for offline analysis of microves-sel blood flow (Sarelius & Duling 1982,Parthasarathi et al. 1999). A 95 µl blood
sample was also obtained from the arterialcatheter for measurement of PO2, PCO2,pH, lactate, and base deficit (model700ABL, Radiometer, Copenhagen). ThePO2 of the inspired air was then dilutedwith nitrogen in a stepwise manner to thefollowing concentrations: 15%, 10%, 8%and 5% O2. At each step, the animals wereallowed a 10 min period to equilibratebefore repeating the systemic andmicrovascular measurements.
StatisticsAll data are expressed as mean �SD, andcomparisons between two independentmeans were made using a one-way ANOVAfollowed by Tukey’s multiple comparisontesting. Significance was taken at theP �0.05 level.
Results
Systemic parametersBaseline phasic blood pressures were thesame (P �0.35) for the instrumented andnon-instrumented animals (Table 1). Bothpopulations experienced a decline in bloodpressure when FiO2 was lowered to below0.15 (Fig 4), and there was no significantdifference between the populations at eachdilution.
Arterial blood gas analysis revealed simi-lar (P �0.52) baseline PO2’s in the instru-mented and non-instrumented populations(Table 1). In addition, the mean lactatelevels for both populations noticeablyincreased at FiO2 �0.1, but were not signifi-cantly different at any inspired oxygenconcentration (Fig 5). Likewise, there was
Table 1 Resting values (mean �SD) for arterial blood pressure (mmHg), arterial PO2 (mmHg), lactate (mmol/l), basedeficit (mmol/l), primary arteriolar flow (nl/min), and aortic flow (ml/min) in instrumented (n �5) rats and non-instrumented (n �3) controls
Arterial Arteriolarpressure Arterial PO2 Lactate Base deficit flow Aortic flow
Instrumented 104 �7.5 119 �11 2.4 �1.5 �5.8 �1.8 22.7 �2.1 61.8 �5.3Non-instrumented 99 �6.3 123 �14 2.2 �1.0 �5.0 �2.0 23.9 �1.5 NA
Chronic flow probe in rats 367
Laboratory Animals (2004) 38 by guest on November 23, 2013lan.sagepub.comDownloaded from

Laboratory Animals (2004) 38
a steady increase in base deficit as FiO2 waslowered, but the values were not significantlydifferent between the instrumented andnon-instrumented populations (Fig 5).
Aortic blood flow did not significantlychange from baseline values in the instru-mented population when the FiO2 wasdecreased to 0.15 (Fig 6). However, furtherreductions in FiO2 resulted in progressivelylower values for aortic flow.
Microvascular parametersBaseline blood flow in the primary arteri-oles of instrumented and non-instrumentedpopulations (Table 1) was not different(P �0.51). For both populations, there was asignificant increase in arteriolar blood flowfrom resting values when the FiO2 waslowered to 0.15 (Fig 7). However, there wasan equivalent decline in arteriolar bloodflow in both populations when FiO2 waslowered to below 0.15, and flow was absentin the arterioles of both populations at FiO20.05.
368 Smith et al.
Fig 4 Phasic arterial blood pressure (mean �SD)versus FiO2 in the instrumented (n �5) and non-instrumented (n �3) populations
Fig 5 Top half: Systemic lactate (mean �SD)versus FiO2 in the instrumented (n �5) andnon-instrumented (n �3) populations. Bottom half:Systemic base deficit (mean �SD) in theinstrumented and non-instrumented populations
Fig 6 Aortic flow (mean �SD) versus FiO2 in theinstrumented (n �5) population
Fig 7 Primary arteriolar blood flow (mean �SD)versus FiO2 in the instrumented (n �5) andnon-instrumented (n �3) populations
by guest on November 23, 2013lan.sagepub.comDownloaded from

Discussion
This study examined the use of chronicallyimplanted transit-time flow probes on theascending aorta of rats as a means of mea-suring systemic blood flow during manipu-lation of oxygen delivery. The implantationprocedure is described as a resource forfuture studies, and we have clarified theeffects of these probes on the systemicresponse to haemodynamic stress.
Complications of the implantationprocedure included intractable pain, infec-tion, persistent pneumothorax, atelectasis,and aortic aneurysm. Severe manifestationof these complications was often evidentby the inability to maintain body weightafter the implantation procedure. In suchcases, the animals were excluded from thestudy and killed. However, these complica-tions rarely occurred after the first fewimplantations, and we found that 95% ofthe instrumented animals recovered theirbody weight within 7 days of implantation.Careful inspection of the thoracic anatomyduring postmortem recovery of the probeswas an effective means to identify lesssevere complications that were not madeevident by the animal’s behaviour. Becausethe presence of an implanted foreign body(i.e. probe and externalized cord) posed aninfection risk that was proportional to theduration of implantation (Corona et al.1990), follow-up experiments were conduct-ed as soon as the animal regained its preop-erative body weight. While complete weightgain was generally achieved in 5–7 days,animals requiring longer recovery time hadtheir cutaneous sutures removed after theseventh postoperative day to help preventcutaneous infections (Hollander & Singer1999). Proper sterile technique and a singledose of Enrofloxacin virtually eliminatedthe occurrence of systemic infection.
We found that successful intubation wasvital to the success of the probe implanta-tion procedure. Animals requiring repeatedattempts at intubation experienced greaterinflammation of the airway and a higherincidence of complications such as anorexiaand atelectasis due to poor respiratory effort.We found that our new intubation technique
resulted in faster intubation times and fewerunsuccessful attempts when compare tomethods that have the animal in a supineposition. The use of a stylet to guide thecatheter through the glottis also helped tominimize pharyngeal trauma. Moreover, theteardrop terminus on our intubationcatheters provided a reliable airway seal thatminimized leakage of the gas anaesthesiainto the environment.
Aside from the known complications ofthe procedure, we wanted to examine thephysiological effects of the implantationprocedure and the presence of the implantedprobes on systemic and microvascularhaemodynamics. Due to the close proximityof the implanted probe to the heart, ascend-ing aorta, and lungs, we were concerned thatthe devices might affect lung expansion,venous return, and aortic flow. However,baseline arterial blood gas analysis (Table 1;unpublished PCO2, HCO3, and pH values)did not suggest an acute or chronic abnor-mality in oxygenation, ventilation, or pH inthe implanted population. Systemic lactateand base deficit values indicate that theinstrumented and non-instrumented popula-tions had similar responses to hypoxia. Inaddition, our values for resting aortic flowin the instrumented population were similarto those obtained by Sweet et al. (1987)using thermodilution (231 �45 ml/min/kg)and radio labelled microspheres(220 �43 ml/min/kg). Of course, theseconclusions must be qualified by the smallsample size and hence limited statisticalpower involved.
Because microvascular blood flow inskeletal muscle is sensitive to sympathetictone during severe hypoxia (Rowell &Blackmon 1987), we measured arteriolarblood flow in the spinotrapezius muscle todetermine the local response to sympatheticstimuli. In both populations there was sig-nificant arteriolar hyperaemia (Fig 7) whenFiO2 was reduced to 0.15 that was attributedto the local production of vasodilatormetabolites (Haddy & Scott 1971, Borgstromet al. 1984,). We expected that this initialvasodilatation would be overwhelmed bythe vasoconstriction associated withincreased sympathetic drive during severe
Chronic flow probe in rats 369
Laboratory Animals (2004) 38 by guest on November 23, 2013lan.sagepub.comDownloaded from

Laboratory Animals (2004) 38
hypoxia (Rowell & Blackmon 1987).Likewise, the reduced arteriolar blood flowseen in both populations with greaterdegrees of hypoxia (Fig 7) was indicative ofequivalent vasoconstriction in the instru-mented and non-instrumented animals.Thus, this study provides no systemic ormicrovascular evidence that the implanta-tion of aortic flow probes results inincreased susceptibility to hypoxia whenobvious complications are excluded.Therefore, we conclude that this novel technology is an accurate method for measuring aortic flow in resting andhaemodynamically-stressed rats. Becausesurgical experience is often the limitingfactor in the success of chronic instrumenta-tion, it is best that first-time operators prac-tise these techniques on animal cadavers, orin an IACUC-approved non-survival study.Such practice will increase the success rateof the implantation procedure, as well asminimize unnecessary animal suffering.
Acknowledgments The authors are grateful toDr Ivo Torres for his technical assistance in perform-ing the implantation procedure. We are also gratefulto Dr Roland N. Pittman for his assistance with themicrovascular measurements. Additional thanks areoffered to the Virginia Commonwealth UniversityInstitutional Animal Care and Use Committee fortheir support and oversight of these techniques.
This work was supported, in part, by grants fromThe National Heart, Lung, and Blood Institute(HL18292), the Department of Defense (DAMD17-01-1-0692) and from the National Institute onDeafness and other Communication Disorders(DC02008).
References
Bit-Alkhas Irani B, Cliffton EE (1970) Coagulationand metabolic changes during hemorrhagic shock.Angiology 21, 161–71
Borgstrom P, Grande PO, Mellander S (1984) Anevaluation of the metabolic interaction withmyogenic vascular reactivity during blood flowautoregulation. Acta Physiologica Scandinavica122, 275–84
Burvine R, Zloczower M, Karnieli E (1998) Double-vein jugular/inferior vena cava clamp techniquefor long-term in vivo studies in rats. Physiology &Behavior 63, 511–15
Chitwood WRJ, Hill RC, Wechsler AS (1978)Maintenance of permanently implanted cardiacpressure catheters in experimental animals.Annals of Thoracic Surgery 26, 485–7
Corona ML, Peters SG, Narr BJ, Thompson RL (1990)Infections related to central venous catheters.Mayo Clinic Proceedings 65, 979–86
Doursout MF, Wouters P, Kashimoto S, Hartley CJ,Rabinovitz R, Chelly JE (2001) Measurement ofcardiac function in conscious rats. Ultrasound inMedicine & Biology 27, 195–202
Gray SD (1973) Rat spinotrapezius muscle prepara-tion for microscopic observation of the terminalvascular bed. Microvascular Research 5, 395–400
Haddy FJ, Scott JB (1971) Bioassay and other evi-dence for participation of chemical factors in localregulation of blood flow. Circulation Research28(Suppl. 1), 86–92
Hollander JE, Singer AJ (1999) Laceration manage-ment. Annals of Emergency Medicine 34, 356–67
Lipowsky HH, Cram LE, Justice W, Eppihimer MJ(1992) Effects of erythrocyte deformability on invivo red cell transit time and hematocrit and theircorrelation with in vitro filterability. Micro-vascular Research 46, 43–64
Parthasarathi AA, Japee SA, Pittman RN (1999)Determination of red blood cell velocity by videoshuttering and image analysis. Annals ofBiomedical Engineering 27, 313–25
Rowell LB, Blackmon JR (1987) Human cardiovascu-lar adjustments to acute hypoxaemia. ClinicalPhysiology 7, 349–76
Sarelius IH, Duling BR (1982) Direct measurement ofmicrovessel hematocrit, red cell flux, velocity, andtransit time. American Journal of Physiology 243,H1018–26
Smith TL, Coleman TG, Stanek KA, Murphy WR(1987) Hemodynamic monitoring for 24 h inunanesthetized rats. American Journal ofPhysiology 253, H1335–41
Sweet CS, Emmert SE, Seymour AA, Stabilito II,Oppenheimer L (1987) Measurement of cardiacoutput in anesthized rats by dye dilution using afiberoptic catheter. Journal of PharmacologicalMethods 17, 189–203
Tsui BC, Mosher SL, Yeung PK (1991) A reliabletechnique for chronic carotid arterial catheteriza-tion in the rat. Journal of PharmacologicalMethods 25, 343–52
370 Smith et al.
by guest on November 23, 2013lan.sagepub.comDownloaded from
Related Documents