Chronic Heart Failure Therapies: Transforming the Landscape Dr. Nadia Giannetti Chief of Cardiology Medical Director, Heart Failure and Heart Transplant Program McGill University Health Center

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Chronic Heart Failure Therapies: Transforming the Landscape
Dr. Nadia GiannettiChief of Cardiology
Medical Director, Heart Failure and Heart Transplant Program
McGill University Health Center

Conflict of Interest
Received grants or honoraria from: Novartis, Servier, Pfizer, Amgen, HeartWare, Astra
2

Agenda
Review the Pathophysiology of Heart Failure and the burden on society
Explore the need to act
Introduce the new data supporting the role of newer drugs therapies
Discuss the Role of family practitioners in the treatment of Heart Failure
3MED/ENT/0149

What is the prevalence of HF in Canada?
4

HF: The Fastest Rising Cardiovascular Condition in Canada
The prevalence of HF has increased over the past few decades1
An estimated 600,000 Canadians are living with HF and 50,000 new patients are diagnosed each year2
• 1.4 million hospital days per year
1. Johansen H, et al. Can J Cardiol. 2003;19(4):430-435 / 2. Ross H, et al. Can J Cardiol. 2006;22(9):749-754. Heart and Stroke Foundation, the Burden of Heart Failure, report on health of Canadians

>750,000 people in Canada will have Heart Failure in 20302
Heart Failure is the Fastest Rising Cardiovascular Condition in Canada
Actual and Projected Incidence of HF in Canada 1
6
1- Management of Heart Failure Patients in Ontario: Recommendations from Best Practice, April 2013, *Ross et al. Treating the right patient at the right time; Access to HF care, CJC 2006. 2- Blais C et all, Assesing HF in Canada CJC 2014; 30: 352-358;
Statistic Canada 2014. 3- Ross H et al. Can J Cardiol 2006: 22(9);749-754 . 4- Cook C, Cole G, Asaria P, Jabbour R, Francis DP. The annual global economic burden of heart failure. Int J Cardiol 2014;171(3):368-376
MED/ENT/0149

Heart Failure Mortality Exceeds that of Most Cancers
Stewart et al. Eur J Heart Fail 2001;3:315-227
All patients with a first administration to any Scottish Hospital in 1991 for HF, MI or the four most common types of cancer specific to men and women were identified, an 5-year survival rates compared
MED/ENT/0149

8
www.heartandstroke.com

The Burden of Heart failure in Canada
9

Canadian Landscape
Large country with large rural population
Mostly family MD provided care with consultative support by specialists
Care is fragmented and variable across the country
Only 15% access HF clinic or Disease management programs These are mostly younger patients
About 2/3 of HF diagnosed in clinics
About 1/3 in ER
50% of HF admissions are de novoGravely S, Can J Cardiol 2012;28:483-9.

Current Challenges Associated With HF Care In Canada
Differential HF clinic access for patients remains a problem
Rural HF care lacks support
Heart and Stroke Foundation’s 2014 Report on the Health of Canadians “More people are surviving heart attacks and strokes, but they face challenges and lack support to thrive to the fullest”
Heart and Stroke Foundation 2014 Report on the Health of Canadians http://www.heartandstroke.com/site/c.ikIQLcMWJtE/b.8968559/k.DE2D/2014_Report_on_health__Creating_Survivors.htm

Four Key Emerging Themes Challenging HF Care in Canada
Hayes et al. BMC Health Services Research (2015) 15:290

• With each acute event, myocardial injury may contribute to progressive LV dysfunction2
• Increasing frequency of acute events with disease progression leads to high rates of hospitalization and increased risk of mortality2
HF is a Progressive Condition with High Morbidity and Mortality
1- Roger VL et al. JAMA 2004;292:344-350. 2- Gheorghiade & Pang. J Am Coll Cardiol 2009;53:557–73.3- Goodlin SJ. J Am Coll Cardiol. 2009 Jul 28;54(5):386-96.
Initial symptoms of HF develop and HF treatment is initiated
Phase 1
Plateau of variable length reached with initial medical management, or following mechanical support or heart transplant
Phase 2
Functional status decline with variable slope; intermittent exacerbations of HF that respond to rescue efforts
Phase 3
Stage D HF, with refractory symptoms and limited function
Phase 4
End of lifePhase 5
Dotted lines represent sudden cardiac death that can occur anytime during the trajectory
Sudden Death Event
Transplant or Ventricular Assist Device
Excellent
Death
Time
Phy
sica
l Fu
nct
ion
1
2
3
4
5
13
3
MED/ENT/0149

Heart Failure: The Abnormality of Cardiac Structure and/or Function
Heart Failure With
Reduced
Ejection Fraction
Weakened heart
muscle
HEART FAILURE Inability for the heart to deliver sufficient
blood/oxygen to meet the demands of the peripheral tissues, or to do so at abnormally high filling pressures, or both
The heart is too weak or too stiff to maintain circulation without running the risk of congestion
Characterized by signs and symptoms of decreased cardiac output and/or volume overload
Heart Failure is a clinical diagnosis and doesn't suggest a cause or underlying pathological state
Normal Heart
CARDIOMYOPATHY
Disease of the heart muscle due to any number of causes
Clinically characterized by heart failure
McMurray et al. Eur Heart J 2012;33:1787–84714MED/ENT/0149

What is the difference between systolic and diastolic HF?
15

Heart Failure with preserved ejectionfraction - EF>40–50%
Heart Failure with reduced ejectionfraction - EF≤ 35–40%
Systolic dysfunction Diastolic dysfunction
Heart Failure with reduced ejection fraction (systolic) and preserved ejection fraction (diastolic)
16
A condition of pressure overload
1. Characterized by concentric
hypertrophic growth
2. Results in normal sized LV cavity
with thickened walls and preserved
systolic function
A condition of volume overload
1. Characterized by eccentric
hypertrophy
2. Results in globular heart with
thinning of LV walls, decreased
systolic function and enlarged LV
volume
1. Aurigemma. Circulation 2006;113;296–304, 2. Paulus et al. Eur Heart J 2007;28:2539–50, 3. Colucci (Ed.). Atlas of Heart Failure, 5th ed. Springer 2008, 4. McMurray et al. Eur Heart J 2012;33:1787–847
MED/ENT/0149

Main causes of Heart Failure
Coronary artery disease
Valvular disease
Cardiomyopathy
Hypertension
Diabetes
17Krum and Gilbert. Lancet 2003;362:147–58; Colucci (Ed.). Atlas of Heart Failure, 5th ed. Springer 2008; Dickstein et al. Eur Heart J 2008;29:2388–442
MED/ENT/0149

Heart Failure triggers the activation of Endogenous Compensatory Mechanisms
Activation of SNS:
Sympathetic tone discharge
Activation of RAAS:
Vasoconstriction necessary to keep enough volume of circulating blood
Natriuretic Peptides:
Natural compensatory system to protect the heart
Risk factors
Myocardial injury to the heart
Initial fall in left ventricle
performance
RAAS: renin-angiotensin-aldosterone system, SNS: sympathetic nervous system Krum H, Abraham WT. Lancet. 2009;373:941-955; Khan MG. Cardiac Drug Therapy. 6th ed. Philadelphia: WB Saunders;
2003.
18
MED/ENT/0149

Fluid retention
Pumping action of the heart grows
weaker
Swelling of feet, ankles, abdomen and lower back area
Coughing
TirednessShortness of breath
Pulmonary edema
Pleural effusion
Symptoms
Breathlessness
Orthopnea
Paroxysmal Nocturnal Dyspnea
Reduced exercise tolerance
Fatigue
Ankle swelling
Signs
Elevated jugular venous pressure
Hepato-jugular reflux
Third heart sound
Laterally displaced apical impulse
Cardiac murmur
Signs and Symptoms of Heart Failure
Early signs of HF:
• Walking less with shortness of breath
• Palpitation
McMurray et al. Eur Heart J 2012;33:1787–84719
MED/ENT/0149

New York Heart Association functional classification Based on severity of symptoms and impact on physical activity
Symptomatic Severity of Heart Failure
NYHA Class
Functional Capacity
I Patients with cardiac disease but resulting in no limitation of physical activity.Ordinary physical activity does not cause undue fatigue, palpitations, or shortness of breath.
II Patients with cardiac disease resulting in slight limitation of physical activity.They are comfortable at rest. Ordinary physical activity results in fatigue, palpitations, or shortness of breath.
III Patients with cardiac disease resulting in marked limitation of physical activity.They are comfortable at rest. Less than ordinary activity causes fatigue, palpitations, or shortness of breath.
IV Patients with cardiac disease resulting in the inability to carry on any physicalactivity without discomfort. Symptoms of HF may be present even at rest. If any physical activity is undertaken, discomfort increases.
Clear relationship between severity of symptoms and survival
Among 411 outpatients total mortality during a follow-up of 1.4 years was: NYHA Class II: 7.1% NYHA Class II: 15% NYHA Class IV: 28%
1- Muntwyler et al. Eur Heart J 2002;23:1861–6; Yeung DF, Boom NK, Guo H, Lee DS, Schultz SE, Tu JV. CMAJ. 2012 Oct 2;184:E765-73 . 2-Levy D, Kenchaiah S, Larson MG et al. N Engl J Med 2002;347(18):1397-1402
20
MED/ENT/0149

What are the goals of therapy?
21

Goals of Therapy
Relieve symptoms and improve QOL
Decrease hospitalizations
Slow disease progression
Prolong life
Is there room for improvement? Definitely!
22

HFrEF until recently
Life-style modificationmo
Devices
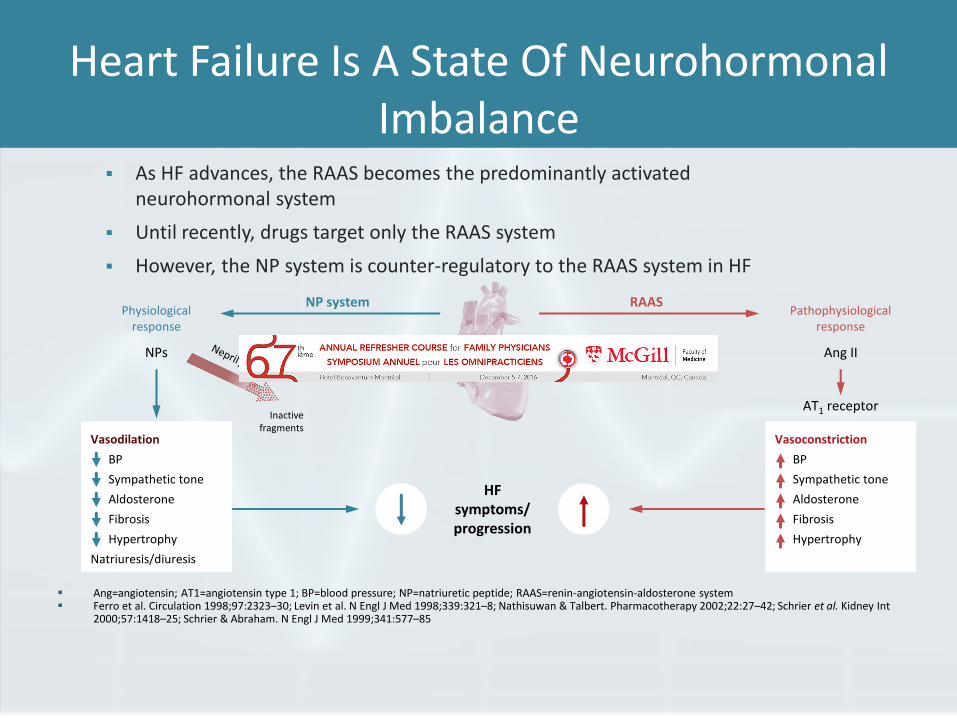
Heart Failure Is A State Of NeurohormonalImbalance
As HF advances, the RAAS becomes the predominantly activated neurohormonal system
Until recently, drugs target only the RAAS system
However, the NP system is counter-regulatory to the RAAS system in HF
Ang=angiotensin; AT1=angiotensin type 1; BP=blood pressure; NP=natriuretic peptide; RAAS=renin-angiotensin-aldosterone system Ferro et al. Circulation 1998;97:2323–30; Levin et al. N Engl J Med 1998;339:321–8; Nathisuwan & Talbert. Pharmacotherapy 2002;22:27–42; Schrier et al. Kidney Int
2000;57:1418–25; Schrier & Abraham. N Engl J Med 1999;341:577–85
HFsymptoms/progression
RAASNP systemPathophysiological
response
Ang II
AT1 receptor
Vasoconstriction
BP
Sympathetic tone
Aldosterone
Fibrosis
Hypertrophy
Physiologicalresponse
NPs
Vasodilation
BP
Sympathetic tone
Aldosterone
Fibrosis
Hypertrophy
Natriuresis/diuresis
Inactive fragments

Evidence Behind ACE Inhibitors
*CONSENSUS Trial . N Engl J Med 1987;316:1429-35. / **SOLVD Investigators. N Engl J Med 1991;325:293-302 / ***Flather MD et al. Lancet 2000;355:1575-81 Arnold JMO, Liu P et al. Can J Cardiol 2006;22(1):23-45.
0.8
0.4
0.2
0
0 2 6 8 12
0.6
4 10
Cu
mu
lati
ve p
rob
abili
ty o
f d
eath
Months
Placebo
Enalapril
p=0.001
CONSENSUS
Cumulative probability
of death*
50
30
10
0
0 24 36 4812
20
40M
ort
alit
y (%
)
Months
Placebo
Enalapril
p=0.0036
SOLVD
Treatment**
40
20
10
0
0 2 3 5
30
1 4
Cu
mu
lati
ve m
ort
alit
y (%
)
Years
Placebo
Enalapril
p=0.0001
SAVE, AIRE
and TRACE
These trials form the basis of ACE inhibitors use in HF with LVEF < 40% and/or post-MI with reduced LVEF and/or HF

New therapy: Sacubitril/Valsartan
Health Canada approved indication:
Oct 2015
Treatment of heart failure with reduced ejection fraction (HFrEF) in patients with NYHA Class II or III, to reduce the incidence of cardiovascular death and heart failure hospitalisation2
Canadian Cardiovascular Society Recommendations For HFrEF:
Jan 2015
We recommend that in patients with mild to moderate HF, an EF < 40%, an elevated NP level or hospitalization for HF in the past 12 months, a serum potassium < 5.2 mmol/L and an eGFR ≥ 30 mL/min and treated with appropriate doses of guideline-directed medical therapy, they should be treated with LCZ696 in place of an ACE inhibitor or an angiotensin receptor blocker, with close surveillance of serum potassium and creatinine (Conditional Recommendation, High-Quality Evidence)1
1- G. Moe, 2014 CCS HF Management Guidelines Focus up-date: CJC 31 (2015): 3-16. 2- J.G. Howlett, The Canadian Cardiovascular Society HF companion; CJC 2015: 1-15
26
MED/ENT/0149
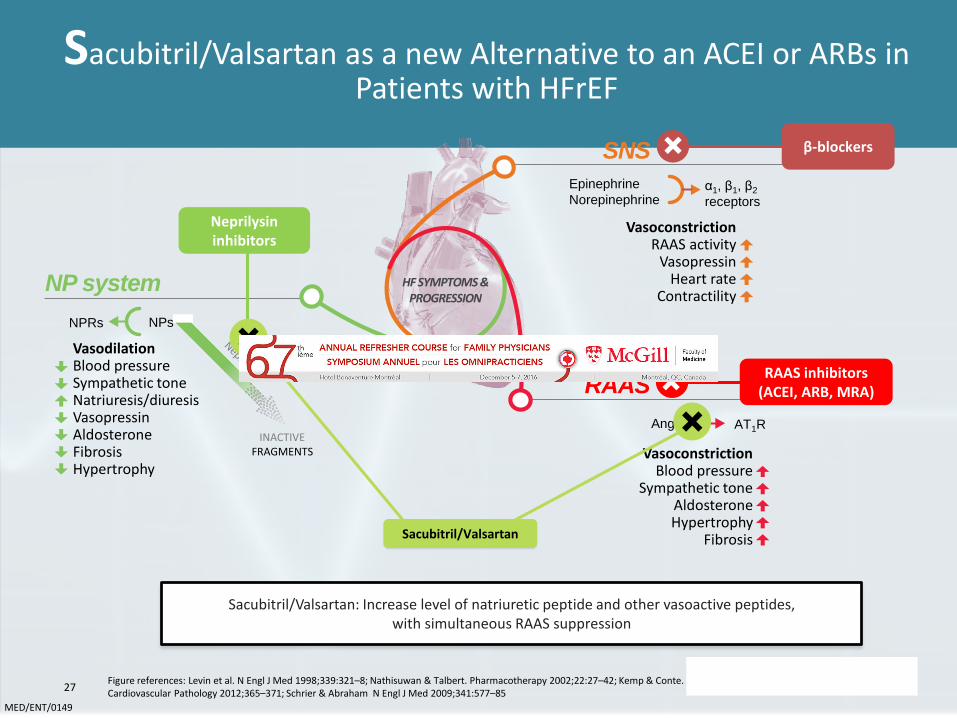
Sacubitril/Valsartan: Increase level of natriuretic peptide and other vasoactive peptides, with simultaneous RAAS suppression
Sacubitril/Valsartan as a new Alternative to an ACEI or ARBs in Patients with HFrEF
SNS
RAAS
VasoconstrictionBlood pressure
Sympathetic toneAldosteroneHypertrophy
Fibrosis
Ang II AT1R
HF SYMPTOMS & PROGRESSION
INACTIVE FRAGMENTS
NP system
VasodilationBlood pressureSympathetic toneNatriuresis/diuresisVasopressinAldosteroneFibrosisHypertrophy
NPRs NPs
Epinephrine
Norepinephrineα1, β1, β2
receptors
VasoconstrictionRAAS activity
VasopressinHeart rate
Contractility
Neprilysininhibitors
RAAS inhibitors (ACEI, ARB, MRA)
β-blockers
Sacubitril/Valsartan
Figure references: Levin et al. N Engl J Med 1998;339:321–8; Nathisuwan & Talbert. Pharmacotherapy 2002;22:27–42; Kemp & Conte. Cardiovascular Pathology 2012;365–371; Schrier & Abraham N Engl J Med 2009;341:577–85
27
MED/ENT/0149

PARADIGM-HF1: The largest mortality-morbidity trialin patients with HFrEF
0
1,000
3,000
4,000
2,000
5,000
6,000
8,000
9,000
10,000
7,000
Nu
mb
er o
f p
atie
nts
N=2569
N=3834
N=1798
N=2548
N=6505
N=2737
N=8442
RAFTHEAALCHARM-AddedSOLVD-T PARADIGM-HFEMPHASIS-HFSHIFT
2003–20092001–20051999–20011986–1989 2009–20132006–20102006–2009Recruitment
CHARM-Added=Candesartan in Heart failure: Assessment of Reduction in Mortality and morbidity-Added trial; EMPHASIS-HF=Eplerenone in Mild Patients Hospitalization And Survival study in Heart Failure; HEAAL=Heart failure Endpoint evaluation of Angiotensin II Antagonist Losartan; HFrEF=heart failure with reduced ejection fraction; PARADIGM-HF=Prospective comparison of ARNI with ACEI to Determine Impact on Global Mortality and morbidity in Heart Failure; RAFT=Resynchronization/Defibrillation for Ambulatory Heart Failure Trial; SHIFT=Systolic Heart Failure Treatment with the If Inhibitor Ivabradine Trial; SOLVD-T=Studies of Left Ventricular Dysfunction Treatment trial
McMurray et al. Eur J Heart Fail 2014;16:817–2528
MED/ENT/0149

PARADIGM-HF: Study Design
*Enalapril 5 mg BID (10 mg TDD) for 1–2 weeks followed by enalapril 10 mg BID (20 mg TDD) as an optional starting run-in dose for those patients who are treated with ARBs or with a low dose of ACEI; †200 mg TDD; ‡400 mg TDD; §20 mg TDD.McMurray et al. Eur J Heart Fail. 2013;15:1062–73; McMurray et al. Eur J Heart Fail. 2014;16:817–25; McMurray et al. N Engl J Med 2014;371 (11):993–1004.
2 Weeks 1–2 Weeks 2–4 Weeks
On top of standard HFrEF therapy (excluding ACEIs and ARBs)
Enalapril10 mg BID*
Sacubitril/Valsartan 97.2/102.8 mg BID‡
Sacubitril/Valsartan 48.6/51.48 mg BID†
Single-blind activerun-in period
Sacubitril/Valsartan 97.2/102.8 mg BID‡
Double-blind Treatment period
Randomizationn=8442
Enalapril 10 mg BID§
Median of 27 months’ follow-up

PARADIGM-HF: Key Inclusion Criteria
Chronic HF NYHA FC II–IV with LVEF ≤40%*
BNP (or NT-proBNP) levels as follows:• ≥150 (or ≥600 pg/mL), or
• ≥100 (or ≥400 pg/mL) and a hospitalization for HFrEFwithin the last 12 months
≥4 weeks’ stable treatment with an ACE inhibitor or an ARB#, and a β-blocker
Aldosterone antagonist should be considered for all patients (with treatment with a stable dose for ≥4 weeks, if given)
*The ejection fraction entry criteria was lowered to ≤35% in a protocol amendment #Dosage equivalent to enalapril ≥10 mg/day McMurray et al. Eur J Heart Fail. 2013;15:1062–73

PARADIGM-HF: Key exclusion criteria
McMurray et al. Eur J Heart Fail. 2013;15:1062–73
History of angioedema
eGFR <30 mL/min/1.73 m2
at screening, end of enalapril run-in or randomization, or a >35% decrease in eGFR between screening and end of enalapril run-in or between screening and randomization
Serum potassium >5.2 mmol/L at screening OR >5.4 mmol/L at the end of the enalapril run-in or end of the LCZ696 run-in
Requirement for treatment with both ACEI and ARBs
Symptomatic hypotension, SBP <100 mmHg at screening, OR SBP <95 mmHg at end of enalapril run-in or at randomization
Current acute decompensated HF
History of severe pulmonary disease
Acute coronary syndrome, stroke, transient ischemic attack, cardiac, carotid, or other major CV surgery, PCI, or carotid angioplasty within the 3 months prior to screening

Characteristic*Sac/Val
(n=4187)Enalapril(n=4212)
Age, years 63.8 ± 11.5 63.8 ± 11.3
Women, n (%) 879 (21.0) 953 (22.6)
Ischemic cardiomyopathy, n (%) 2506 (59.9) 2530 (60.1)
LV ejection fraction, % 29.6 ± 6.1 29.4 ± 6.3
NYHA functional class, n (%)II III
2998 (71.6)969 (23.1)
2921 (69.3)1049 (24.9)
SBP, mmHg 122 ± 15 121 ± 15
Heart rate, beats/min 72 ± 12 73 ± 12
NT pro-BNP, pg/mL (IQR) 1631 (885–3154) 1594 (886–3305)
BNP, pg/mL (IQR) 255 (155–474) 251 (153–465)
History of diabetes, n (%) 1451 (34.7) 1456 (34.6)
Treatments at randomization, n (%)
Diuretics 3363 (80.3) 3375 (80.1)
Digitalis 1223 (29.2) 1316 (31.2)
β-blockers 3899 (93.1) 3912 (92.9
Mineralocorticoid antagonists 2271 (54.2) 2400 (57.0)
ICD 623 (14.9) 620 (14.7)
CRT 292 (7.0) 282 (6.7)
PARADIGM-HF: Summary of Baseline Characteristics: 70% were NYHA Class II
*mean ± standard deviation, unless statedMcMurray, et al. N Engl J Med 2014; ePub ahead of print: DOI: 10.1056/NEJMoa1409077.32
MED/ENT/0149

Sacubitril/Valsartan Reduced Death from CV Causes or First Hospitalization for HF by 20% Compared to Enalapril
1.0
0.6
0.4
0.2
0
0 180 360 540 720 900 1,080 1,260
Enalapril
Sacubitril/ValsartanHazard ratio = 0.80 (95% CI: 0.73–0.87)p<0.001
NNT to prevent one primary event: 21
No. at risk
4187 3922 3663 3018 2257 1544 896 249 Sacubitril/Valsartan
4212 3883 3579 2922 2123 1488 853 236 Enalapril
Outcome, n %Sac/Val
(n=4,187)Enalapril(n=4,212)
Hazard ratio*(95% CI) p value‡
Death from CV causes or first hospitalization for worsening of HF 914 (21.8) 1,117 (26.5) 0.80 (0.73–0.87) <0.001
Death from CV causes 558 (13.3) 693 (16.5) 0.80 (0.71–0.89) <0.001
First hospitalization for worsening of HF 537 (12.8) 658 (15.6) 0.79 (0.71–0.89) <0.001
Cu
mu
lati
ve p
rob
abili
ty
Days since randomization
McMurray et al. Eur J Heart Fail 2014;16:817–2533
MED/ENT/0149

Superiority of Sacubitril/Valsartan was Demonstrated in all Secondary Endpoints
Hazard ratio = 0.80 (95% CI: 0.71–0.89)p<0.001
Days since randomization
Cu
mu
lati
ve
pro
bab
ility
1.0
0.6
0.4
0.2
0
0 180 360 540 720 900 1080 1260
First hospitalization for HF
1.0
0.6
0.4
0.2
0
0 180 360 540 720 900 1080 1260
Hazard ratio = 0.80 (95% CI: 0.71–0.89) p<0.001NNT: 32
Enalapril
Sac/Val
Death from CV causes
Hazard ratio = 0.60 (95% CI: 0.38–0.94)p=0.027
1.5
1.0
0.5
00 10 20 30
Hazard ratio = 0.84 (95% CI: 0.76–0.93)p<0.001
Cu
mu
lati
ve
pro
bab
ility
1.0
0.6
0.4
0.2
0
0 180 360 540 720 900 1080 1260
Death from any cause Heart Failure Hospitalization within 30 days
Days since randomization
McMurray et al. Eur J Heart Fail 2014;16:817–2534
MED/ENT/0149

Resuscitated sudden deaths* occurred in 16 patients receiving LCZ696 versus 28 patients receiving enalapril (HR 0.57, 95% CI: 0.31–1.04, p=0.07). Further, LCZ696 significantly reduced the risk of combined resuscitated and non-resuscitated sudden deaths by 22% when compared with enalapril (HR 0.78, 95% CI: 0.66–0.92, p=0.002)
Sacubitril/valsartan significantly reduced the number of sudden cardiac deaths compared with enalapril
Desai et al. Eur Heart J 2015; epub ahead of print: DOI:10.1093/eurheartj/ehv186;
Data on file. Clinical Study Protocol CLCZ696B2314
Hazard ratio = 0.80 (95% CI: 0.68–0.94) p=0.008
Enalapril
LCZ696
0 180 360 540 720 900 1,080 1,260
0
0.02
0.04
0.06
0.08
0.10
Days since randomizationNo. at riskLCZ696 4,187 3,891 2,478 1,005Enalapril 4,212 3,860 2,410 994
Cu
mu
lati
ve p
rob
abili
ty o
f ev
ent
*Resuscitated sudden deaths were defined as successful resuscitation following cardiac arrest
CI=confidence interval; HR=hazard ratio
15MDL167E

OutcomeSac/Val
(n=4187)Enalapril(n=4212)
Hazard ratio*or difference (95% CI) p-value‡
Death from any cause, n (%) 711 (17.0) 835 19.8) 0.84 (0.76–0.93) <0.001
Change in KCCQ clinical summary score† at 8 months, mean ± SD
-2.99 ± 0.36 -4.63 ± 0.36 1.64 (0.63–2.65) 0.001
New onset atrial fibrillation¶, n (%) 84 (3.1) 83 (3.1) 0.97 (0.72–1.31) 0.83
Decline in renal function§, n (%) 94 (2.2) 108 (2.6) 0.86 (0.65–1.13) 0.28
*Calculated with the use of stratified cox proportional-hazard models‡Two-sided p-values calculated by means of a stratified log-rank test without adjustment for multiple comparisons
†KCCQ scores range from 0 to 100 – higher scores indicate fewer symptoms and physical limitations associated with HF¶2670 patients in the LCZ696 and 2638 in the enalapril group who did not have atrial fibrillation at randomization were evaluated§Defined as: (a) ≥ 50% decline in eGFR from randomization; (b) > 30 mL/min/1.73 m2 decline in eGFR from randomization or to a value of <60 ml/min/1.73 m2, or (c) progression to end-stage renal disease
McMurray et al. Eur J Heart Fail 2014;16:817–2536
Effect of Sacubitril/Valsartan in Secondary Endpoints
MED/ENT/0149

Sacubitril/Valsartan Increase the Effect on CV Death of Current Standard of care (ACEis/ARBs)
10%
20%
30%
40%
ACE
inhibitor
Angiotensin
receptor
blocker10%
% D
ecre
ase in C
V M
ort
alit
y
17%
20%
Angiotensin
neprilysin
inhibition
15%
Effect of ARB vs placebo derived from CHARM-Alternative trial
Effect of ACE inhibitor vs placebo derived from SOLVD-Treatment trial
Effect of Sacubitril/Valsartan vs ACE inhibitor derived from PARADIGM-HF trial
McMurray et al. Eur Heart J 2015;36(7):1434.43937
MED/ENT/0149

Fewer Patients in the Sacubitril/Valsartan Group Stopped Study Medication Because of an Adverse Events
Event, n (%)Sacubitril/Valsartan(n=4,187)
Enalapril(n=4,212)
p value
Hypotension
Symptomatic 588 (14.0) 388 (9.2) <0.001
Symptomatic with SBP <90 mmHg 112 (2.7) 59 (1.4) <0.001
Elevated serum creatinine
≥2.5 mg/dL 139 (3.3) 188 (4.5) 0.007
≥3.0 mg/dL 63 (1.5) 83 (2.0) 0.10
Elevated serum potassium
>5.5 mmol/L 674 (16.1) 727 (17.3) 0.15
>6.0 mmol/L 181 (4.3) 236 (5.6) 0.007
Cough 474 (11.3) 601 (14.3) <0.001
Angioedema (adjudicated by a blinded expert committee)
No treatment or use of antihistamines only 10 (0.2) 5 (0.1) 0.19
Catecholamines or glucocorticoids without hospitalization 6 (0.1) 4 (0.1) 0.52
Hospitalized without airway compromise 3 (0.1) 1 (<0.1) 0.31
Airway compromise 0 0 —
Fewer patients in the sacubitril/valsartan group than in the enalapril group stopped their study medication because of an Adverse Events (10.7 vs. 12.3%, p=0.03)
McMurray et al. N Engl J Med 2014;371:93-100438
MED/ENT/0149

Patients with:• Prior ACE inhibitor or ARB at guidelines-
recommended doses
Initiating and titrating Sacubitril/Valsartan to target dose
Patients with:• Prior ACE inhibitor or ARB at less than
guidelines-recommended doses• Risk for hypotension (≥75 years old, low SBP)• Moderate hepatic impairment (Child-Pugh B)
Sacubitipril/Valsartan should only be initiated in clinically stable patients whose baseline systolic blood pressure, serum potassium and renal function are at acceptable levels.If patients experience tolerability issues, e.g. symptomatic hypotension or hyperkalemia, consideration should be given to temporary down-titration or treatment interruption of Sacubitipril/Valsartan
Stop ACE inhibitor therapy for a 36-hour wash out
Sacubitril/Valsartan must not be started until 36 hours have passed following discontinuation of ACE inhibitor therapy
Entresto TM Product Monograph39
MED/ENT/0149

Conclusion – PARADIGM-HF
40

Ivabradine
41


SHIFT Trial: Design And Follow Up
Swedberg K, et al. SHIFT Investigators. Lancet. 2010;376(9744):875-85.
Median study duration: 22.9 months; maximum: 41.7 months
7,411 screened
6,558 randomized
3,241 analysed2 lost to follow-up
Excluded: 27
3,268 to ivabradine
3,264 analysed1 lost to follow-up
Excluded: 26
3,290 to placebo

SHIFT Trial: Mean Heart Rate Reduction
Böhm M, et al. Lancet. 2010 ;376(9744):886-894.
90
60
50
0 2 weeks 4 12 3220
70
80
1 8 16 24 28
Hea
rt r
ate
(bp
m)
Months
Placebo
Ivabradine
HR = 0.82 (0.75-0.90)
p<0.0001
67
7575
64
Mean ivabradine dose:
6.4 mg bid at 1 month
6.5 mg bid at 1 year

SHIFT Trial: Primary Endpoint CV Death Or Hospital Admission For Worsening CHF
Swedberg K, et al. SHIFT Investigators. Lancet. 2010;376(9744):875-85.
40
20
0
0 6 12 18 3024
30
10Cu
mu
lati
ve f
req
uen
cy (%
)
Months
Placebo
Ivabradine
HR = 0.82 (0.75-0.90)
p<0.0001
18%RRR

PARADIGM-HF: Primary Endpoint: Death From CV Causes Or First Hospitalization For HF
*The numbers of patients who would need to have been treated (NNT) to prevent one primary event was evaluated over the duration of the trialMcMurray et al. N Engl J Med 2014;371 (11):993–1004.
No. at risk
4187 3922 3663 3018 2257 1544 896 249 Sacubitril/Valsartan
4212 3883 3579 2922 2123 1488 853 236 Enalapril
Sacubitril/Valsartan
Enalapril
1.0
0.2
0
0 240 1260900
0.6
0.4
180 360 720 1080
Cu
mu
lati
ve p
rob
abili
ty
Days since randomization
Hazard ratio = 0.80
(95% CI: 0.73–0.87)
p<0.001
HR: 20% difference favoring sacubitril/valsartan
NNT to prevent one primary event: 21

SHIFT Trial: Ivabradine Reduces The Risk Of Death For Heart Failure
Böhm M et al. Clin Res Cardiol. 2012;102(1):11-22. Ivabradine or placebo is given on top of guideline-recommended therapy including ACE inhibitor, β-blocker, mineralocorticoid receptor antagonist
10
5
0
0 6 12 18 3024
Pati
ents
wit
h d
eath
fro
m h
eart
failu
re (%
)
Time (months)
Placebo
Ivabradine
Heart rate 75 bpm
n=4150
p<0.006
39%

AE And Those Leading To Definitive Withdrawal Of Study Drug
Data are number of patients (%). Patients included in this safety analysis are those who had taken at least one dose of study drug. p values are calculated on the basis of number of patients. *Transient enhanced brightness in a restricted area of the visual field.
Patients with an adverse eventPatients with an adverse event
leading to drug withdrawal
Ivabradinegroup
(n=3232)
Placebo group(n=3260)
p valueIvabradine
group(n=3232)
Placebo group(n=3260)
p value
All 2439 (75%) 2423 (74%) 0.303 467 (14%) 416 (13%) 0.051
Heart failure 804 (25%) 937 (29%) 0.0005 70 (2%) 82 (3%) 0.367
Symptomatic bradycardia 150 (5%) 32 (1%) <0.0001 20 (1%) 5 (<1%) 0.002
Asymptomatic bradycardia 184 (6%) 48 (1%) <0.0001 28 (1%) 5 (<1%) <0.0001
Atrial fibrillation 306 (9%) 251 (8%) 0.012 135 (4%) 113 (3%) 0.137
Phosphenes* 89 (3%) 17 (1%) <0.0001 7 (<1%) 3 (<1%) 0.224
Blurred vision 17 (1%) 7 (<1%) 0.042 1 (<1%) 1 (<1%) 1.000

Conclusion SHIFT Trial
49
“findings should be interpreted as the effects of ivabradine in addition to normal clinical practice in the specific population of patients with heart failure and heart rates of 70 bpm or higher, who are unlikely to tolerate the highest dose of β blocker. Our results support the importance of heart-rate reduction with ivabradine for improvement of clinical outcomes in heart failure and confirm the important role of heart rate in the pathophysiology of heart failure”
Swedberg, Lancet Vol 376 September 11, 2010

No
n-p
harm
acolo
gic the
rapies (te
achin
g self care, exercise)
CCS HF Algorithm: Therapeutic Approach To Patients With CHF And Reduced Ejection Fraction
Patient with LVEF <40%
Triple TherapyACEi (or ARB if ACEi intolerant), BB, MRA
Titrate to target doses or maximum tolerated evidence-based dose
NYHA IContinue triple therapy
NYHA II-IVSR, HR ≥70 bpm*ADD Ivabradine† and SWITCH ACEior ARB to LCZ696 for eligible patients**
NYHA II-IVSR with HR ≥70 bpm or AF or pacemakerSWITCH ACEi or ARB to LCZ696 for eligible patients**
NYHA I or LVEF <35%Continue present management
NYHA I-III and LVEF ≤35%refer to ICD/CRT algorithm
NYHA IVConsider:• Hydralazine/nitrates• Referral for advanced HF therapy (mechanical
circulatory support/transplant)• Advance HF referral
Reassess every 1-3 years or with clinical status change‡
Consider LVEF reassessment every 1-5 years
Reassess as needed according to clinical status‡
Diu
reti
cs t
o r
elie
ve c
on
gest
ion
Titr
ated
to
min
imu
m e
ffec
tive
do
se t
o m
ain
tain
eu
vole
mia
Reassess Symptoms
Reassess Symptoms and LVEF
Ad
vance
Care
Plan
and
Do
cum
en
tation
of G
oals o
f Care

Effectiveness Of Multidisciplinary Heart Failure Clinics
HF clinics with greater frequency of visits (>4 contacts of significant duration for 6 months) were associated with lower mortality (hazard ratio, 0.14; p<0.0001) and hospitalization (hazard ratio, 0.69; p=0.039)
More intensive medication management was associated with lower all-cause (hazard ratio, 0.46; p<0.001) and HF readmission (hazard ratio, 0.42; p<0.001).
Wijeysundera HC, et al. Circ Heart Fail. 2013;6(1):68-75.

CCS HF AlgorithmRecommended Initial Referral And Wait Time
He
art
Failu
re C
are
Init
ial R
efer
ral
Situ
atio
nal
wai
t ti
me
ben
chm
arks
See within 12 weeks, ideally within 6
See within 4 weeks, ideally within 2
See within 4 weeks, ideally within 2
See within 24 hours
Routine, Elective Referral• Chronic HF disease management NYHA II• NYHA I – minimal or no symptoms
Semi-Urgent, Intermediate Risk• New diagnosis of HF, stable, compensated• NYHA II/III• Worsening HF on therapy• Mild symptoms with valvular or renal disease or hypotension
Urgent• New diagnosis of HF, not improving on therapy (unstable, decompensated)• Progression to NYHA IV HF• Post-hospitalization or ER visit for HF• Severe HF with valvular or renal disease or hypotension• Post myocardial infarction HF
Emergent• Acute severe myocarditis• Rapidly progressive heart failure/cardiogenic shock• Heart failure with ACS or MI• Transplant and device evaluation of unstable patients• New-onset acute pulmonary edema
Init
ial R
efe
rral
Urg
ency
Howlett JG et al. The Canadian Cardiovascular Society Heart Failure Companion: Bridging Guidelines to Your Practice. CJC 2015;1-15.

CCS HF AlgorithmRecommended Follow-up Frequency
*Visit frequency may increase during medication titration Howlett JG et al. The Canadian Cardiovascular Society Heart Failure Companion: Bridging Guidelines to Your Practice. CJC 2015;1-15.
Follow-up every 6-12 months
Follo
w-u
p F
req
uen
cy*
Follow-up every 1-6 months
Follow-up every 1-4 weeks or as clinically indicated (remote monitoring possible for some titrations)
Make inactive or consider for discharge from HF clinic if a minimum of 2 of the following characteristics are present:
• Stable NYHA I or II for 6-12 months• On optimal therapies• Reversible causes of HF fully controlled• Having access to General Practitioner with expertise
in management of HF
• Stable adherence to optimal HF therapy• No hospitalization for >1 year• LVEF >35%
(consistently shown if more than one recent EF measurement)• Primary care provider has access to urgent specialists reassessment
He
art
Failu
re C
are
High Risk Individual• NYHA IIIb or IV symptoms• Recent HF hospitalization • During titration of HF medications• New onset heart failure• Complications of HF therapy (rising creatinine, hypotension)• Need to down-titrate or discontinue beta-blockers or ACEi/ARB• Severe concomitant and active illness (e.g. COPD, frailty)• Frequent ICD firings (1 month)
Low Risk Individual• NYHA I or II• No hospitalization in past year• No recent changes in medications• Receiving optimal medical/device HF therapies
Intermediate Risk Individual• No clear features of high or low risk.

Heart Failure Patient Stratification And Care Provision
Brand C, et al. Intern Med J 2007; 37(9): 653-659.
Level of Care Patient Status Care Provision
Primary care(Level 1)
Less complexity NYHA I-II Optimal prescription of pharmacological and nonpharmacological therapy, patient and caregiver self-care education and support.
Intermediate care(Level 2)
Intermediate complexityNYHA II-IIIUnable to stabilize at Level 1
Consultation by Level 2 HF team. Patient stabilization, review of therapies and recommendations for changes.Discharge back to Level 1 when stable.
Specialist support(Level 3)
High complexity NYHA III-IVUnable to stabilize at Level 2
Consultation with and involvement of Level 3specialized HF team until patient stabilizes sufficiently for transfer to Level 2 care.
54
MED/ENT/0149

What is the role of the primary care physician in HF management?
55
Primary care physician’s Role in the management of HFrEF patients
Prevalence of patients with HFrEF is rising as population is aging
In many regions of Canada, about 50% of HF patients are being followed by GPs/FPs1
Even patients with mild symptoms have a high risk of heart failure hospitalization and cardiovascular death
NYHA Class II patients are mainly followed and treated by FPs
Sacubiril/valsartan was shown to be superior to ACEi in Class II patients (70% of PARADIGM-HF trial population) on CV mortality and HF hospitalization
Asking the right questions for a better diagnostic of disease progression
Co-management (family practitioners & specialists) of patients with HFrEF has been demonstrated to be the most efficient approach to manage this disease
FPs are the ones who follow most of the HF patients Early identification of signs and symptoms of the patients
Identify early signs and adjust medication before patients decompensate
56 1-Tu K et al. Can J Cardiol. 2004; 20:282-91
MED/ENT/0149

Model For Future Disease Management Of HF
From this To this!
Heart Failure Clinic
Primary Care Provider
Family and community
Other Care Provider HF Patient
Heart Failure Clinic
Patient with Heart Failure
Primary Care Provider

Heart Failure:
50% of patients will die within 5 years1
The leading cause of hospitalization for patients >65 years of age
Approx. 50% of patients with HFrEF are seeing by GPs/FPs in Canada2
HF burden on patients, families and society
1.4 million hospital days per year
The Estimated direct cost of heart Failure in Canada in 2012 was $2.9 billions
New therapies are available to decrease risk of CV death and heart failure hospitalization inheart failure patients with reduced EF:
Sacubitril/Valsartan
Ivabradine
The role of GPs/FPs in HFrEF patients treatment optimization is critical:
Asking the right questions
Increase survival
Reduce hospitalization
Summary
1- Roger VL et al. JAMA 2004;292:344-350. 2- Tu K et al. Can J Cardiol. 2004; 20:282-913- McMurray et al. N Engl J Med 2014;371:993–1004. 4- Packer et al. Circulation 201458
MED/ENT/0149

Summary
Heart failure is on the rise and a growing burden to our society and our health care resources
Evidence-based medical therapy can improve quality of life, morbidity and mortality in our patients
Access to care and optimization of therapy is essential to improve the future of heart failure
59
Related Documents