Investigating (unwarranted) clinical variation in the inpatient setting Chronic Heart Failure / Chronic Obstructive Pulmonary Disease Professor Peter Macdonald Conjoint Professor of Medicine in the University of New South Wales, Medical Director Heart Transplant Unit, St Vincent’s Hospital, Sydney LEADING BETTER VALUE CARE 1 Quality Improvement Collaboration – QuIC February Webinar A QuIC Update on Initial Clinical Assessment & Diagnostic Investigations for an Acute Exacerbation of CHF

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Investigating (unwarranted) clinical variation in the inpatient setting
Chronic Heart Failure / Chronic Obstructive Pulmonary Disease
Professor Peter Macdonald
Conjoint Professor of Medicine in the University of New South Wales,
Medical Director Heart Transplant Unit, St Vincent’s Hospital, Sydney
LEADING BETTER VALUE CARE
1
Quality Improvement Collaboration –
QuIC February Webinar
A QuIC Update on Initial Clinical Assessment &
Diagnostic Investigations for an Acute Exacerbation of CHF

Acute Decompensated Heart Failure Assessment & Treatment
Peter Macdonald Medical Director
Heart Transplant Unit St Vincent’s Hospital, Sydney

Take home messages: Acute Heart Failure (AHF)
• Rapid onset of or increasing severity of symptoms and signs of heart failure – New onset of AHF – Acute decompensation of chronic heart failure
• Key Questions – Is this heart failure? – What is the trigger? – What is the underlying cause?
• Life-threatening condition – Initial triage – Is the patient hypoxaemic? – Is the patient hypotensive ? – Usually require admission to hospital

Newton P, et al. Med J Aust 2016:Feb 15;204(3):113.e1-8

13
25 hospitals
Newton P, et al. Med J Aust 2016:Feb 15;204(3):113.e1-8

Recruitment
0
10
20
30
40
50
60
70
80
90
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25
Nu
mb
er
recr
uit
ed
n = 811
Newton P, et al. Med J Aust 2016:Feb 15;204(3):113.e1-8

Baseline demographics All n = 811
Demographic Profile
Male 465 (58%)
Age (mean ± SD) 77 ± 13
Caucasian 699 (86%)
Residential aged care facility 80 (11%)
Clinical Profile
CHF 540 (68%)
IHD 445 (56%)
Chronic pulmonary disease 251 (32%)
Diabetes 204 (38%)
Charlson Co-morbidity Index 3.6 + 2.6
Newton P, et al. Med J Aust 2016:Feb 15;204(3):113.e1-8

LV Dysfunction (n = 751)
0
5
10
15
20
25
30
35
40
45
50
> 50% 40-49% 30-39% < 30%
318 125 139 169
Pe
rce
nta
ge o
f p
atie
nts
(%
)
LV Ejection Fraction
Newton P, et al. Med J Aust 2016:Feb 15;204(3):113.e1-8

LV Dysfunction (n = 751)
0
5
10
15
20
25
30
35
40
45
50
> 50% 40-49% 30-39% < 30%
318 125 139 169
Pe
rce
nta
ge o
f p
atie
nts
(%
)
LV Ejection Fraction
HFPEF (LVEF > 50%) 42% HFREF (LVEF < 50%) 58%
HFPEF (LVEF > 40%) 59% HFREF (LVEF < 40%) 41%
Newton P, et al. Med J Aust 2016:Feb 15;204(3):113.e1-8

HFPEF vs HFREF (LVEF – 40%)
HFPEF (n = 443)
HFREF (n = 307)
p value
Age (mean + SD)
78 + 12
74 + 14
<0.001
Sex (M:F%)
48:52
76:24
<0.001
De novo: Decomp (%)
36:64
27:73
0.01
Admisson Rhythm Sinus Afl/Fib Paced
41 46 9
43 35 17
0.001
Admission BP (mmHg)
Systolic Diastolic
139 + 34 75 + 21
131 + 30 80 + 52
0.002 0.08
Newton P, et al. Med J Aust 2016:Feb 15;204(3):113.e1-8

HFPEF vs HFREF (LVEF – 40%)
HFPEF (n = 443)
HFREF (n = 307)
p value
Cause of HF (%) IHD Hypertension Cardiomyopathy Other
36 32 10 38
53 15 24 17
<0.001
Charlson Co-morbidity Index (mean + SD) Chronic Lung Mod/Severe Kidney Diabetes
3.7 + 2.8
35 36 40
3.5 + 2.4
28 34 38
ns
Frailty Category (%) Non-frail Pre-frail Frail
7
20 73
9
22 69
ns
Newton P, et al. Med J Aust 2016:Feb 15;204(3):113.e1-8

Frailty
0
10
20
30
40
50
60
70
80
Not frail Pre-frail Frail
Pe
rce
nta
ge (
%)
Newton P, et al. Med J Aust 2016:Feb 15;204(3):113.e1-8

Section 6
Newton P, et al. Med J Aust 2016:Feb 15;204(3):113.e1-8

Jamar
Dynamometer

Clinical Criteria for Congestive Heart Failure
Major Criteria
• Orthopnoea +/- PND
• Bilateral lung crepitations
• Cardiomegaly
• Third heart sound
• Elevated JVP
Minor Criteria
• Dyspnoea on exertion
• Nocturnal cough
• Pleural effusion
• Bilateral ankle oedema
• Hepatomegaly
• Tachycardia (HR > 120/min)

Precipitants AHF
Rapid triggers (mins – hrs)
• Arrhythmias – VT, Severe Bc
• Acute Coronary Syn (ACS)
• Mech complication of ACS – Pap muscle rupture
– Post-MI VSD
• Acute pulmonary embolism
• Acute valve pathology
• Hypertensive crisis
Less rapid triggers (days - weeks)
• Arrhythmias
– Afl/Afib
• Non-adherence to diet/drug Rx
• Iatrogenic eg NSAIDs, BB
• Alcohol or drug abuse
• Infection
• Anaemia/Fe Deficiency
• Thyroid
– is the pt on amiodarone?
• Renal impairment
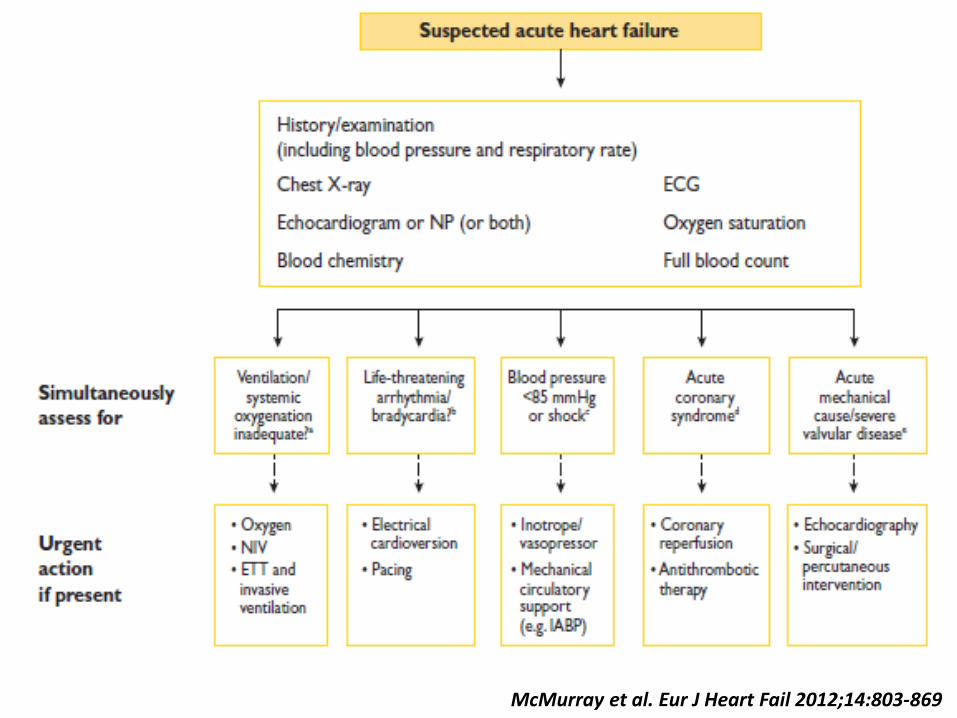
McMurray et al. Eur J Heart Fail 2012;14:803-869

Suspected Acute Heart Failure
• History/examination – incl BP & Respiratory Rate
• O2 saturation • ECG (Rhythm, ACS) • Chest X Ray • Echocardiogram
– HFREF vs HFPEF – Structural Abnormalities
• Bloods – UEC/LFTs/hs TnT – TFTs/Fe Studies – Full blood count
Cardiomegaly Pulmonary Oedema
AF & LVH
HFREF HFPEF

McMurray et al. Eur J Heart Fail 2012;14:803-869
McMurray et al. Eur J Heart Fail 2012;14:803-869

Acute pulmonary oedema/congestion
IV bolus frusemide
O2 Sat < 94% Oxygen
Severe anxiety distress
Consider IV morphine
Measure Systolic BP
SBP < 90 mm Hg or shock SBP > 110 mmHg SBP 90 -110 mmHg
Add inotrope Consider IV GTN Observe response
Yes
Yes
No
No
Adapted from McMurray et al. Eur J Heart Fail 2012;14:803-869

Re-evaluation of patient’s clinical status
SBP < 90 mmHg
O2 sat < 94% Urine output < 20 ml/hr
Stop vasodilator Stop BB, ACEI (if on them)
Consider inotrope then mechanical support
Increase frusemide dose Consider diuretic
combination Consider ultrafiltration
Oxygen CPAP or NIPPV
Invasive Ventilation
No No
Yes Yes Yes
Adapted from McMurray et al. Eur J Heart Fail 2012;14:803-869

Acute Precipitant
Trigger Total HFREF HFPEF
Ischaemia 13% 16% 9%
Infection 22% 21% 25%
Arrhythmia 15% 14% 16%
Non-adherence Rx 5% 5% 7%
Diet/fluid 16% 18% 14%
Other 28% 28% 29%
Newton P, et al. Med J Aust 2016:Feb 15;204(3):113.e1-8

Acute Precipitant – What investigations should I do?
Trigger Total Investigations
Ischaemia 13% ECG, hsTnT
Infection 22% CXR +/- MSU, Viral Swabs etc (depending on Hx & Ex)
Arrhythmia 15% ECG
Non-adherence Rx 5% History
Diet/fluid 16% History
Other 28% FBC (Anaemia/Infection) Fe Studies
UEC/LFTs (Kidney/Liver) TFTS (Thyroid)
BNP or nt-proBNP?*
* If there is doubt re cause of dyspnea – Cardiac versus Respiratory

Acute Precipitant – What other investigations should I do?
New Onset HF
• Echo – HFREF vs HFREF
– LV Hypertrophy
– RWMA/VSD
– Valvular Dis
– Pericardial Disease
• +/- Cardiac MRI
• +/- Coronary Imaging – CT
– Invasive
ADHF in person with CHF
• Echo and more invasive investigations likely to have been performed previously – If no , Echo is essential
– If yes, Consider repeat Echo
• ACS
• ? Mechanical complication
• ? Valvular pathology
– Repeat coronary angio if ACS

Rx- To admit or not to admit?
Rapid trigger
• Does the patient have an advanced care directive (ACD)?
– Immediate transfer to
hospital ED
– Vs
– Palliative/Symptom Management at home
Less rapid trigger
• Home-based Rx vs ED – Re-institution of drug Rx, diet
& fluid management
– Cessation of iatrogenic cause
– Increased oral vs IV diuretic (may depend on Community Heart Failure Service availability)
– Further Rx dept on ACD.

Non-pharmacological Rx
• Monitoring – ECG – Vital signs including HR, BP, RR & O2 satn – Fluid balance – Daily Weight
• Ventilatory support – Oxygen (I/N or by mask) if O2 satn < 94% – Target O2 satn 94-98% – Non-invasive ventilation if inadequate response – ETT & invasive ventilation (ICU)
• Diet – salt & fluid restriction

Aliti et al. JAMA Intern Med. 2013;173(12):1058-1064.
Salt & fluid restriction in acute decompensated heart failure: a word of caution

From: Aggressive Fluid and Sodium Restriction in Acute Decompensated
Heart Failure: A Randomized Clinical Trial
Figure 2. Change in body weight from baseline to 3-day reassessment and from baseline to the end of the study period in the
intervention and control groups. Significance was determined using the Mann-Whitney test. Data points indicate the mean values;
whiskers indicate SD.
Alti et al. JAMA Intern Med. 2013;173(12):1058-1064. doi:10.1001/jamainternmed.2013.552
Increased Thirst in
Intervention Group

From: Aggressive Fluid and Sodium Restriction in Acute Decompensated
Heart Failure: A Randomized Clinical Trial
Alti et al. JAMA Intern Med. 2013;173(12):1058-1064. doi:10.1001/jamainternmed.2013.552

Treatment during admission All n = 811
Oxygen 673 (87%)
CPAP / BiPAP 133 (17%)
Mechanical ventilation 29 (4%)
IV Diuretics 643 (81%)
IV GTN 53 (7%)
IV Inotrope 63 (8%)
Dialysis 16 (2%)
IABP / ECMO 8 (1%)
CPR 21 (3%)
Referred - Heart Tx / LVAD 17 (2%)
Newton P, et al. Med J Aust 2016:Feb 15;204(3):113.e1-8

Treatment of ADHF – ALARM HF
Follath et al Intensive Care Medicine 2011: 37(4); 619-629

Adjusted outcomes for various Rx
Mebazaa et al Intensive Care Medicine 2011: 37(2); 290-301

Baseline demographics The Real
World (Snapshot)
SURVIVE (2007)
REVIVE I & II (2013)
ATOMIC-AHF (2016)
No. of patients
811 1327 600 606
IV Drug frusemide Dobutamine vs levosimendan
Levosimendan Vs placebo
Omecantiv mecarbil vs plac
Male 58% 72% 73% 77%
Age (years) 77 67 64 66
HFREF (LVEF < 40%)
42% 100% (LVEF < 30%)
100% (LVEF < 35%)
100% (LVEF < 40%)
Comorbidities Multiple
Few Few Few
Primary Endpoint
Clinical outcome
Dyspnoea Dyspnoea Dyspnoea

Baseline demographics The Real
World (Snapshot)
ASCEND – HF (2011)
Relax (2013)
No. of patients
811 7141 1161
IV Drug frusemide Nesiritide Vs placebo
Serelaxin Vs placebo
Male 58% 66% 73%
Age (years) 77 67 72
HFREF (LVEF < 40%)
42% 80% 55%
Comorbidities Multiple
Few Few
Comment Mean sBP 136 mmHg
sBP > 100 mmHg sBP > 125 mmHg

CHF Medications (All patients)
0
10
20
30
40
50
60
70
80
90
100
Admission
Discharge
Percentage (%)
Newton P, et al. Med J Aust 2016:Feb 15;204(3):113.e1-8

Medications in HFREF (using LVEF 40% as cut-point
de novo cases excluded at admission)
0
10
20
30
40
50
60
70
80
90
100
Admission
Discharge
Percentage (%)
**
** p = 0.01
Digoxin
Newton P, et al. Med J Aust 2016:Feb 15;204(3):113.e1-8

Other CVS Medications (All patients)
0102030405060708090
100
Admission
Discharge
Percentage (%)
Newton P, et al. Med J Aust 2016:Feb 15;204(3):113.e1-8

Medications in HFREF (using LVEF 40% as the cut-point
de novo cases excluded)
0
10
20
30
40
50
60
70
80
90
100
ACEI/ARB + BB ACEI/ARB + BB + MCA
Admission
Discharge
Newton P, et al. Med J Aust 2016:Feb 15;204(3):113.e1-8

Median Length of Stay (Days)
0
2
4
6
8
10
12
14
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
LOS
Newton P, et al. Med J Aust 2016:Feb 15;204(3):113.e1-8

Post-discharge Follow-Up • Prospective studies and registry data have shown
that the most vulnerable period for readmission is within the first 2 weeks post-discharge.
• Ideally AHF patients should be reviewed within the first 7-14 days of discharge from hospital, regardless of the type of appointment.
• The frequency of their appointments thereafter should be guided by their clinical stability.

Discharge Planning
• Multidisciplinary Heart Failure Service
– Nurse
– Pharmacist
• GP
• Palliative Care

Discharge Medications & Management
• 10 + 4 prescribed medications
• 13 + 7 pills
• 59% referred to HF multi-disciplinary care program
Newton P, et al. Med J Aust 2016:Feb 15;204(3):113.e1-8

Discharge status
0
10
20
30
40
50
60
70
80
Home RACF Transferred toanother facility
Died
Pe
rce
nta
ge (
%)
Newton P, et al. Med J Aust 2016:Feb 15;204(3):113.e1-8

Conclusions
• Patients admitted with ADHF
– Elderly
– Frail
– Multiple co-morbidities
– Limited use of evidence-based HF medications
– Complex medical Rx with high pill burden
– High consumption of complementary medicines
Newton P, et al. Med J Aust 2016:Feb 15;204(3):113.e1-8

Take home messages: Acute Heart Failure (AHF)
• Rapid onset of or increasing severity of symptoms and signs of heart failure – New onset of AHF – Acute decompensation of chronic heart failure
• Key Questions – Is this heart failure? – What is the trigger? – What is the underlying cause?
• Life-threatening condition – Initial triage – Is the patient hypoxaemic? – Is the patient hypotensive ? – Usually require admission to hospital
Related Documents