CHRONIC DIARRHOEA IN DOGS Dave Collins BVSc FANZCVS Registered Specialist in Small Animal Medicine [email protected]

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

CHRONIC DIARRHOEA IN DOGSDave Collins BVSc FANZCVS
Registered Specialist in Small Animal Medicine

www.sashvets.com
Diarrhoea
• Increase frequency, fluidity, or volume of faeces
• Large vs Small
• Acute vs chronic (>14d)

www.sashvets.com
Diarrhoea
• Mechanisms of diarrhoea:
• Osmotic: maldigestion or malabsorption eg EPI
• Secretory: abnormal ion transport due to hormones, toxins, eg enteropath E Coli, IBD
• Increased Mucosal Permeability: eg erosive, ulcerative enteropathies, IBD, neoplasia
• Deranged motility:eg abnormal ileal and colonic motility in IBD
www.sashvets.com
DDx acute* or chronic diarrhoea
• Dietary: diet change *, overeating*, indiscretion*, intolerance, allergy; type I IgE, type IV cell mediated
• Inflammatory: IBD, ARD, AHE*
• Infectious: parasitic – helminths, protozoa; bacteria* – Salmonella, Campylobacter, C. perfringens, C. difficile, E Coli; Viral* –parvovirus; Fungal?; Rickettsial?
www.sashvets.com
DDx acute or chronic diarrhoea
• Extraintestinal:
pancreatitis, EPI, liver, kidney, hypoA
• Toxaemia, Septicaemia
• Neoplasia:
carcinoma, MCT, leiomyosarcomas, GIST, LSA
• Drugs & Toxins: eg NSAIDs, ABs

www.sashvets.com
Chronic Diarrhoea
• Signalment: IBD, PLE breeds, IBD rarely <12 months; GSD, Shar Pei, Irish Setter, SCWT, Basenji, Yorkies, Maltese, Rottweilers
• History: large vs small bowel, severity, weight loss, parasites, diet
• Physical Exam
• Diagnostic tests: Non invasive first!
• CBC/biochem/TLI/ACTH stim

www.sashvets.com
Chronic Diarrhoea
• Faecal Exam: parasitology, bacteriology, Faecal PCR
• Folate/Cobalamin
• Dietary Trial
• Imaging
• Biopsy – endoscopic, laparascopic, surgical

www.sashvets.com
Giardia spp.
• Diagnosis:
• ZnSO4 floatation, SNAP Antigen, PCR
• Treatment:
• Metronidazole
• Fenbendazole
www.sashvets.com
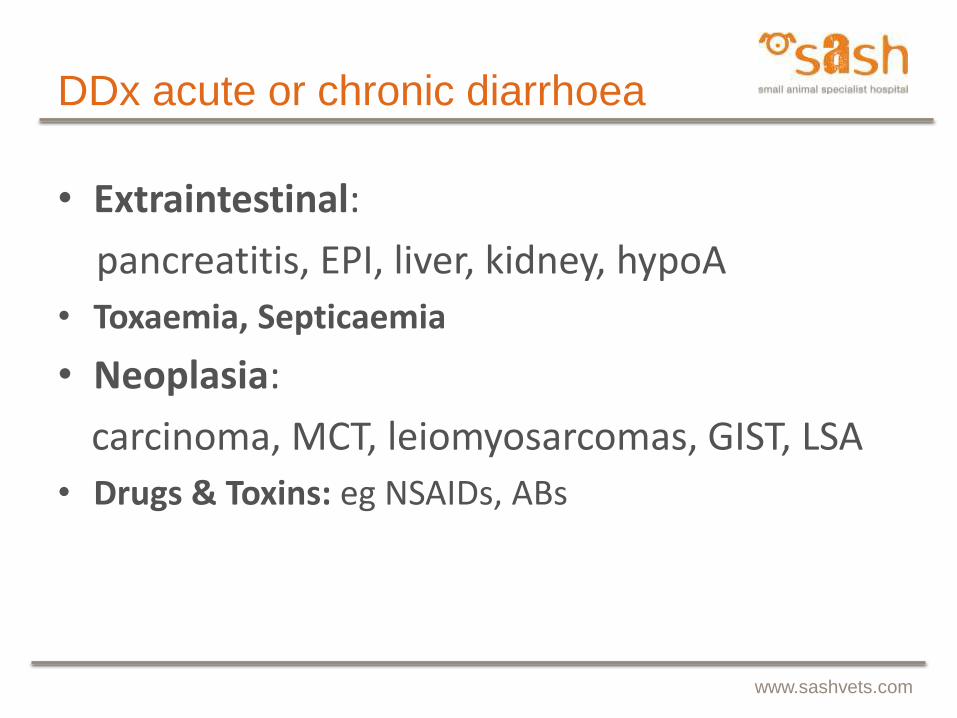
Folate and Cobalamin
www.sashvets.com
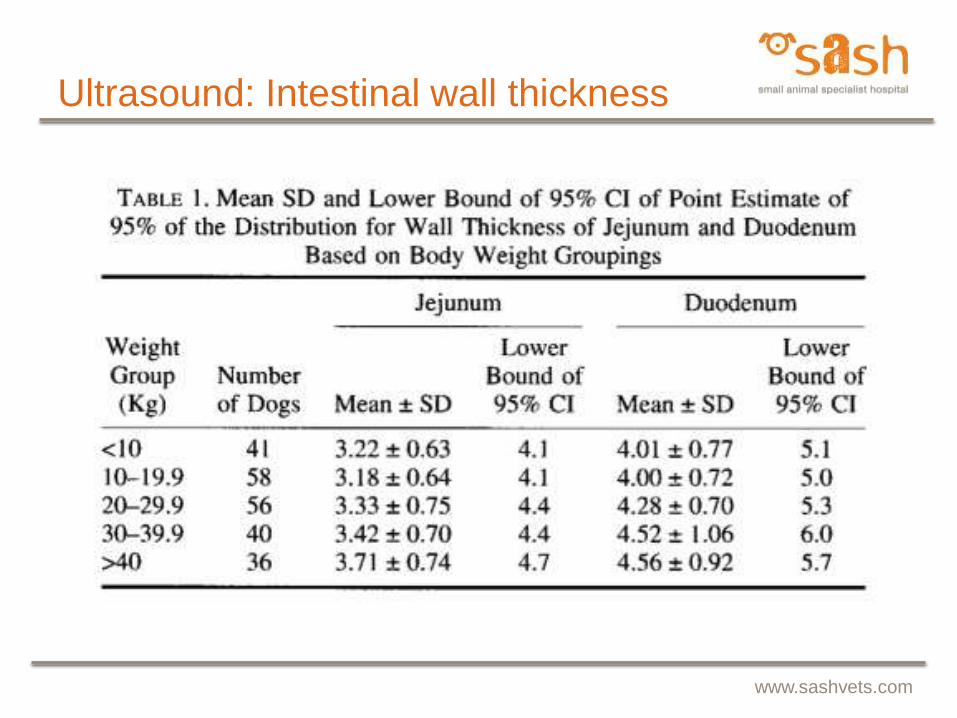
Ultrasound: Intestinal wall thickness
www.sashvets.com
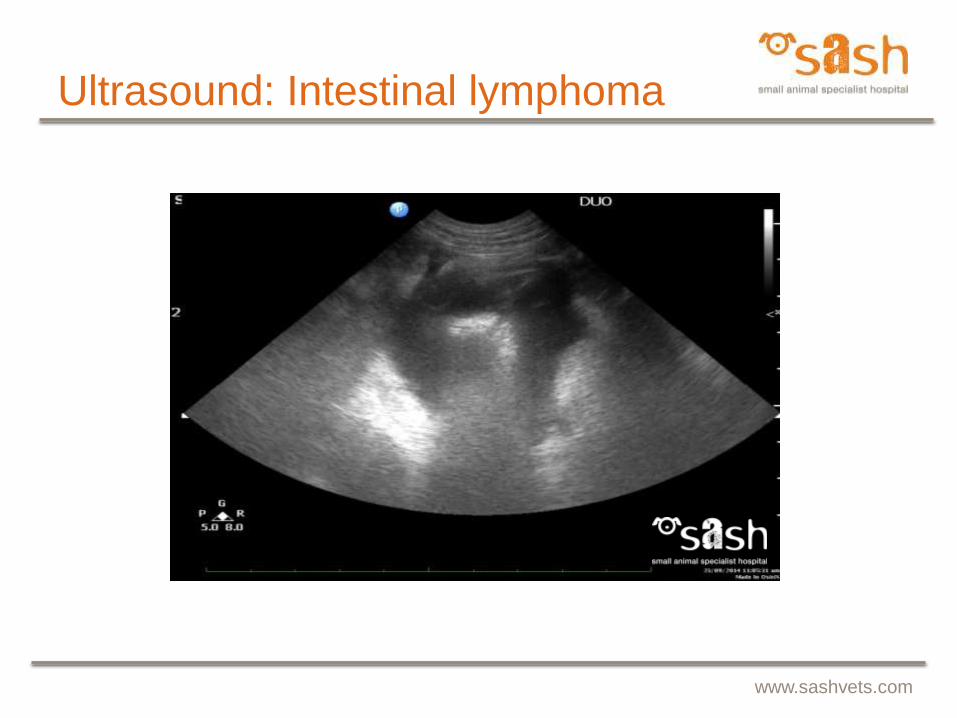
Ultrasound: Intestinal lymphoma

www.sashvets.com
Ultrasound: Intestinal lymphoma

Diarrhea Panel Prevalence Data
Australia US Canada Japan Brazil UK South Korea
Canine Distemper Virus 0.8% 1.1% 0.3% 1.5% 2.3% 1.4% 7.4%
Salmonella spp. 0.2% 0.6% 1.7% 0.7% 0.6% 0.7% 0.9%
Canine Parvovirus 2 4.7% 1.7% 0.3% 2.6% 6.3% 5.5% 1.9%
Cryptosporidium spp. 6.3% 5.6% 6.1% 7.3% 4.0% 6.2% 7.9%
Giardia spp. 7.8% 8.4% 9.3% 11.7% 10.8% 17.2% 21.9%
Canine Enteric Coronavirus 4.4% 11.8% 4.2% 20.7% 12.5% 19.3% 7.4%
C. perfringens alpha toxin (Q) 52.2% 51.6% 38.7% 57.5% 43.8% 7.8% 30.7%
C. perfringens enterotoxin 41.7% 22.7% 12.2% na na 0.0% 0.0%
Campylobacter jejuni 10.7% 4.5% 6.4% 3.1% 12.5% 20.7% 4.7%
Campylobacter coli 1.5% 1.4% 0.5% 1.1% 12.5% 1.4% 0.5%
Overall Infection Rate 78.8% 64.3% 69.7% 71.6% 62.5% 51.7% 47.0%
Coinfection Rate 29.5% 24.9% 47.5% 31.7% 40.0% 41.9% 36.6%
Samples included n=619 n=7829 n=2590 n=486 n=702 n=674 n=215
Canine Diarrhea PanelPrevalence

www.sashvets.com
IBD – WSAVA, ACVIM
1. Chronic persistent or recurrent GI signs
2. Histopath evidence off mucosal inflammation
3. No evidence of other GI disease
4. Inadequate response to dietary, antibiotic and anthelmintic therapy alone
5. Clinical response to anti-inflammatory or immunosuppressive agents
www.sashvets.com
Inflammatory Bowel Disease
• Intestinal mucosa has a barrier function for “immune exclusion”
• Controls exposure of GALT
• Protective immune responses to protect against pathogens
• “tolerance” of harmless environmental antigens such as commensal bacteria and food
• IBD develops when normal decision making process breaks down → inappropriate immune responses and uncontrolled inflammation

www.sashvets.com
Inflammatory Bowel Disease
• Loss of tolerance may result from:
i. Disruption of normal mucosal barrier leading to antigen exposure to submucosal lymphoid tissue
ii. Dysregulation of normal mucosal immune system or both
• Genetics of TLRs, NOD

www.sashvets.com
IBD

www.sashvets.com
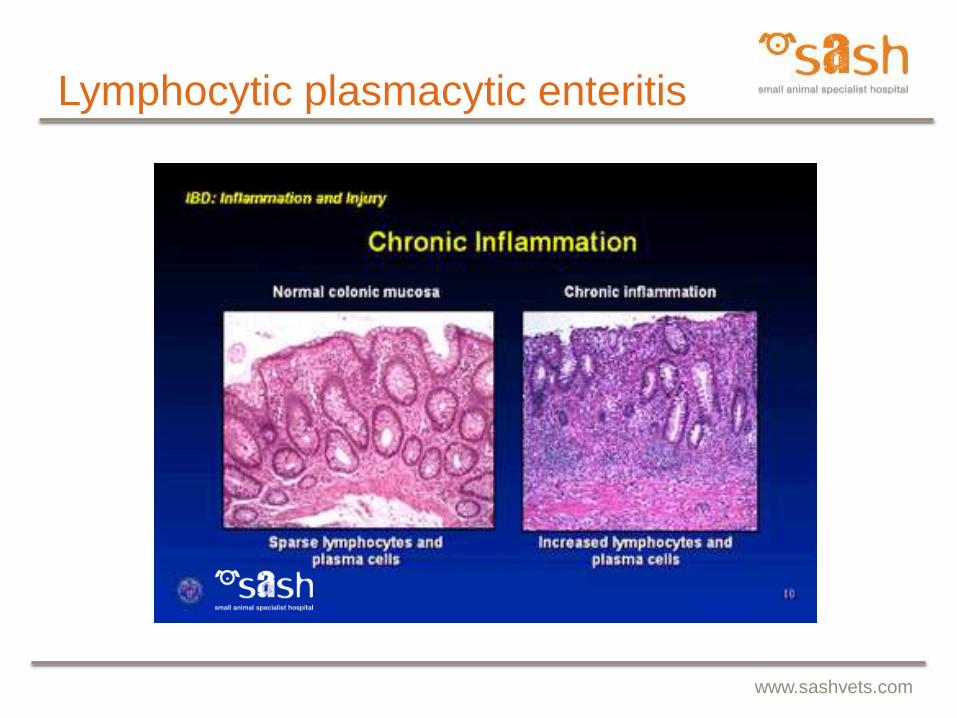
Lymphocytic plasmacytic enteritis
• Most common
• Mucosal infiltrate of lymphocytes and plasma cells, changes in mucosal architecture eg villous atrophy, villous fusion, crypt abscessation
• Other causes of LP infiltration: enteropathogens, Toxoplasma
• GSDs, Shar-Peis, pure bred cats
• Often causes PLE esp Basenjis
www.sashvets.com
Lymphocytic plasmacytic enteritis
www.sashvets.com
Lymphocytic plasmacytic enteritis
www.sashvets.com
Lymphocytic plasmacytic enteritis
• Chronic diarrhoea, weight loss
• Chronic vomiting may predominate
• Histopath: variation in interpretation; subjectivity; localised inflammation - ileal; endoscopic vs full thickness; severe LPE vs LSA –concurrent, pre-neoplastic or misdiagnosis

www.sashvets.com
Eosinophilic Enteritis
• 2nd most common form of IBD
• Frequently involves SI, stomach and/or colon
• Variable changes eg villous atrophy
• Mixed inflammatory infiltrate, predominantly eosinophilic
• Any breed and age, mostly younger adult
• Boxers, Dobermans, German Shepherds

www.sashvets.com
Eosinophilic Enteritis

www.sashvets.com
Eosinophilic Enteritis
• Vomiting, SI diarrhoea, LI diarrhoea
• +/- Mucosal erosion or ulceration
• May be associated with PLE
• DDX: dietary sensitivity, endoparasitism, visceral larva migrans, MCT, idiopathic
• +/- hypereosinophilia (DDX MCT, parasitism, HypoA, allegic cutaneous or respiratory diseases)
www.sashvets.com
Neutrophilic Enteritis
• May be neutrophilic infiltrate or granulomatous inflammation
• Consider underlying bacterial infection
• May be secondary to bacterial invasion of mucosal ulceration/erosion
• Caution: glucocorticoids

www.sashvets.com
Granulomatous Enteritis
• Rare form of IBD
• Mucosal infiltration with macrophages → granuloma formation
• May be similar to human Crohn’s, granulomatous colitis of Boxers
• Enteroadherent and invasive E Coli (EIEC)
• Yersinia, mycobacteria, fb rxn, fungal??

www.sashvets.com
Protein Losing Enteropathy
• Lymphangiectasia - primary (Yorkies, Maltese, Rottweilers, secondary
• Inflammatory : IBD, esp Basenjis, SCWT, gluten enteropathy Irish Setters
• Infectious: viral, bacterial, fungal, parasitic• Neoplasia: LSA, ACA, GIST• Obstructive: chronic fb, intussusception• Haemorrhage: GUE, drugs, hepatic, renal, parasites,
neoplasia• SLE, Hypoadrenocorticism• Right heart failure, pericarditis, portal hypertension
www.sashvets.com
Protein Losing Enteropathy
• Most common:
• Lymphangiectasia – secondary
• Severe IBD
• Neoplasia
• GI haemorrhage
• Treatment considerations: aggressive treatment , dietary – hypoallergenic, low fat, prednisolone , chlorambucil, antithrombotics, +/- diuretics
www.sashvets.com
Treatment Approach
• Diet:
• Novel protein source
• Hydrolysed diets eg Hill’s z/d.
• Protein source? Size of particles too small for crosslinking of IgE but type of immune response unknown; clinical efficacy allergic dermatitis, IBD
• Antibiotic trial
• Immunosuppressives

www.sashvets.com
Antibiotics Trial
• Tylosin 10-15mg/kg PO q8h
• Oxytetracycline 20mg/kg PO q8h
• Metronidazole 10mg/kg PO q12h
• 28 day course
• Long term tylosin 5mg/kg/day

www.sashvets.com
Ciclosporin
• T-lymphocyte effects
• Efficacy in anal furunculosis
• Expensive, variable efficacy and toxicity
• 12 out of 14 steroid resistant enteropathies improved clinical score (CIBDAI), 5mg/kg/day, also reduced T cell numbers in duodenal biopsies (Allenspach JVIM 2006)

www.sashvets.com
Chlorambucil
• Long term use in severe IBD or small cell GI lymphoma in cats
• “Dogs are just big cats?”
• Chlorambucil (4-6 mg/m2/day for first 7 to 21 days)-prednisolone (14 dogs) more efficacious for treatment of chronic enteropathy and concurrent PLE than azathioprine-pred (13 dogs)
Dandrieux JAVMA 2013
www.sashvets.com
Probiotics
• Probiotic strains of human or canine origin (Lactobacillus, Bifidobacterium, and Enterococcus) may affect:
i. Intestinal microbial populations
ii. May reduce specific pathogens in faeces
iii. Immunomodulators
• Two overall positive studies on probiotics in management of dietary sensitivity and food-responsive diarrhea have been published to date
• Level 1 evidence for effectiveness of probiotics in treating lactose intolerance/maldigestion, treating acute infectious or nosocomial diarrhea in children, preventing or treating ARD, maintaining remission of ulcerative colitis in adults

www.sashvets.com
Oscar
• 10MN Labrador
• 2 month history of inappetance, weight loss and diarrhoea
• Mild hypoalbuminaemia 21 (22-39g/L), borderline globulin 26 (26-45g/L)
• AUS: diffusely abnormal SI, thickened jejunum up to 7.0mm, thickened muscularis layer, distended loops, similar changes in ileum
• Laparoscopic intestinal biopsies

www.sashvets.com
Oscar
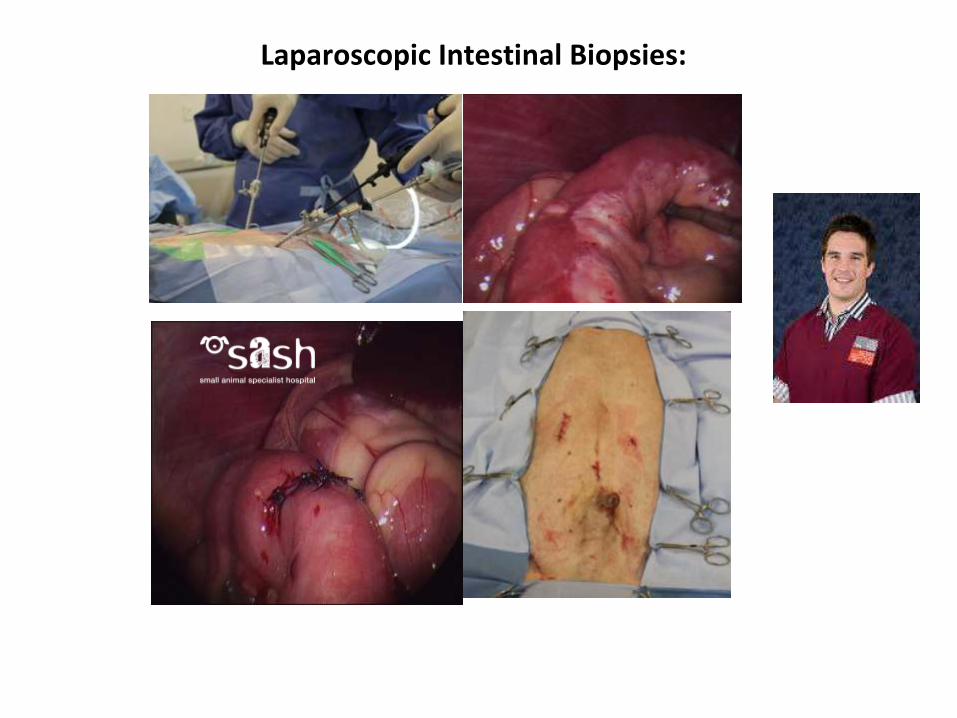
Laparoscopic Intestinal Biopsies:

www.sashvets.com
Oscar
• Histopath:
• Moderate chronic enteritis of jejunum and ileum, with mucosal oedema and lymphatic dilation
• Rx: Hill’s z/d, metronidazole, prednisolone, B12
• 2 weeks post op albumin 24, BAR, still diarrhoea!

www.sashvets.com
Sanka
• 3FS Border Collie
• Week long history of vomiting, lethargy, abdominal pain and pyrexia
• Treated with clavulox, ranitidine
• Now diarrhoea, ropey intestines
www.sashvets.com
Sanka
• Abdominal ultrasound showed marked thickening and lack of wall layering in ileum with grossly enlarge jejunal lymph nodes (image next slide)
• Hypoproteinaemia: albumin 18 g/L
• Exploratory laparotomy with full thickened biopsies

www.sashvets.com
Sanka – Ultrasound Images

www.sashvets.com
Sanka
• Histopathology:
• 55% small lymphocytes, 3% medium lymphoid cells, 2% large lymphoid cells, 2% plasma cells, at least 28% macrophages and 10% neutrophils
• Ileum was abnormal with areas of erythematous thickening
• MARKED CHRONIC MULTIFOCAL TO COALESCING PYOGRANULOMATOUS MURAL ENTERITIS AND LYMPHADENITIS.
• No bacteria, fungal elements or acid-fast organisms seen on Gram, PAS or ZN sections respectively
www.sashvets.com
Sanka
• Culture negative, special stains negative
• No fungal elements or oomycetes seen on methenamine silver sections.
• Fenbendazole
• Enrofloxacin, metronidazole
• Hill’s z/d
• Long term: tylosin

www.sashvets.com
Sanka – Ultrasound Images

www.sashvets.com.au twitter: @SASHvets
Phone - (02) 9889 0289 Fax - (02) 9889 0431
Level 1, 1 Richardson Place, North Ryde 2113, Sydney, NSW
Related Documents