X-Linked Dystonia-Parkinsonism Information for patients and families Christopher Stephen, MD, MRCP (UK) Nutan Sharma, MD, PhD

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

X-Linked Dystonia-Parkinsonism
Information for patients and families
Christopher Stephen, MD, MRCP (UK)Nutan Sharma, MD, PhD

X-Linked Dystonia-Parkinsonism (XDP)- What is it?
Multiple names XDP DYT3 by dystonia classification “Lubag” – local Filipino term describing twisting postures in
early stages
Rare, adult-onset, progressive genetic neurological movement disorder
Almost entirely affects men who descend from the Philippines island of Panay
Can have symptoms of dystonia, Parkinsonism or bothf
First reported in 1975 by Dr. Lillian Lee in the Philippines who established the XDP Study Group in 1980s to focus research towards a cure

Where did XDP originate?
The Philippines –population 98.4 million
Distribution from ancestral migration from Panay
12 million of Filipino descent overseas including USA, UK and Japan
than AZ

How common is XDP?
Information from the XDP registry, Philippines
Registry started by Dr. Lee in the Philippines
508 cases (as of February 2010)
Vast majority male - 500 males and 8 females
Prevalence in the island of Panay is 5.24 per 100,000
Prevalence in the Philippines is 0.34 per 100,000

What is dystonia? Movement disorder
Involuntary, sustained muscle contractions resulting in twisting, repetitive movements and abnormal postures
Can affect any part of the body including limbs, hands, torso, face, neck or vocal cords
Distribution Focal – one body part
involved Segmental or multifocal -
multiple body parts Generalized – many body
parts Breakefield et al. Nat Rev Neurosci 2008

What is Parkinsonism? Movement disorder
Symptoms which are classically associated with Parkinson’s disease but can also be seen in many other conditions
Symptoms include Tremor when at rest Slowness of movement Handwriting smaller Reduced facial expression Shuffling walking Poor balance
Brainmind.com

Course of disease
Very variable
Age of onset ~40 years old (range 12-64)
Presentation
Most present with focal dystonia ▪ More common – legs, jaw, neck and tongue▪ Less common – arms and rarely trunk or tremor
Rarely presents with Parkinsonism (milder course)▪ Rest tremor, slowness, small handwriting, shuffling walking
(sud-sud)

Progression of disease
3 clinical phases
1. Dystonia – focal (e.g. one foot) then often becomes generalized (by normally 5 years of symptoms) Common - twisting/dragging a foot, repeated jaw opening and
closing, abnormal turning or posture of the neck, tongue protrusion, mouth pursing or excessive eye blinking
Rare - bending of the trunk or tremor May have “sensory tricks” - improvement in dystonia by
touching certain areas (particularly neck dystonia)
2. Dystonia and Parkinsonism (7-15 years of symptoms)
3. Parkinsonism predominates (15+ years of symptoms)

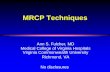
Clinical course of XDP
Lee LV et al. Int J Neurosci 2011
YEARS SINCE INITIAL PRESENTATION
1 2 7 10 15
Focal dystonia
Dystonic phase, dystonia spreads
Dystonia + Parkinsonism
Parkinsonian phase
Pure Parkinsonism with minimal dystonia have a slow, mild, often non-disabling course

Diagnosis and diagnostic considerations
Diagnosis – by clinical picture, family tree and definitive genetic testing
Given variable presentation, XDP may be confused with a number of other conditions Primary dystonic disorder – focal or generalized Parkinson’s disease or other causes of
Parkinsonism
Clues are the adult onset, clinical pattern and ancestral connection to the Philippines particularly the island of Panay
Lee LV et al. Int J Neurosci 2011

What evaluations are needed?
Assessment by a neurologist
Speech and swallowing evaluation
Nutritionist
Physical therapy/Occupational therapy
Genetic counsellingLee LV et al. Int J Neurosci 2011

What are the genetics of XDP?
Inherited by an X-linked (sex-linked) recessive manner
Likely caused by a mutation in the TAF1 gene on the X-chromosome
Clinical genetic testing is available at only a few locations worldwide
Patients should see a genetic counselor before testing
A positive result has implications not only for the patient but also other members of the family and any children

What are the genetics of XDP?
Caused by an abnormality in a gene (mutation) which interferes with the way genes work and affects normal cell processes
Males generally affected as they have only one X chromosome (XY) whereas females have two (XX).
The presence of an additional, healthy X chromosome protects females that have 1 abnormal gene.

What are the genetics of XDP?
Females with 1 copy generally have no symptoms and are called healthy carriers
Females very rarely affected – may occur if inherit 2 copies of the gene – one from a carrier mother and the other from an affected father
Due to carrier females the disease gene may hide in families until there is an affected male

What is the risk of others in the family? Others may find they are at
risk if a person tests positive for XDP
Risk to children If affected male
▪ All daughters carriers▪ No sons affected
If carrier female▪ 50% risk for daughters to be
carriers▪ 50% risk for sons to be
affected
Risk to brothers and sisters of affected male depends on carrier status of mother

Treatment of XDP – Medical therapy
Directed at symptoms – dystonia or Parkinsonism
Medications for dystonia All stages
Anti-cholinergics - Trihexyphenidyl (Artane) Benzodiazepines – clonazepam (Klonopin)
Multi-focal or generalized Tetrabenazine (Xenazine)
Advanced dystonia Zolpidem (Ambien)
Botulinum toxin injections Focal dystonia (particularly neck, eyelids,
tongue and jaw) May worsen swallowing if injected in tongue
or neck

Treatment of XDP – Medical therapy
Directed at symptoms – dystonia or Parkinsonism
Medications for Parkinsonism Levodopa (Sinemet)
Particularly in pure Parkinsonism and become less effective with more dystonia
Dopamine agonists Can be less effective than levodopa and
may worsen dystonia Pramipexole (Mirapex) Ropinirole (Requip)

Treatment of complications of disease
Swallow evaluation Guides diet modifications and other
techniques to reduce the risk of aspiration Physical Therapy and Occupational Therapy
Improvement in mobility and assistive devices
May prevent formation of contractures and delay bed-bound state
Nursing care Observation for pressure sores

Surgical treatment -Deep Brain Stimulation (DBS)
Neurosurgical treatment for XDP
What is it? Delivers electrical stimulation to the
brain in order to alleviate neurological symptoms
Surgically implanted wire (lead or electrode) inserted into the brain
Stimulation target is globus pallidus Powered by an implantable pulse
generator placed under the skin in the chest, similar to a cardiac pacemaker
Stimulation adjusted non-invasively

Surgical treatment –Deep Brain Stimulation (DBS)
What is it used for? Parkinson’s disease Essential tremor Genetic dystonias like XDP
How does it work? Does not damage healthy
brain tissue Blocks electrical signals
from targeted areas in the brain

Surgical treatment –Deep Brain Stimulation (DBS)
What are the benefits? Can improve symptoms by 50-
60% in genetic dystonias but is variable
Limited data regarding use in XDP but appears similarly effective
Lasts at least 10 years
What are the risks? 1-2% risk of bleeding in the brain
or stroke 3-4% risk of surgical infection Generator needs replacement
after 3-9 years depending on type

Why have Filipinos not heard of XDP?
For many years, Filipino families did not have an understanding of what XDP was
Due to the drastic presentation was often a source of family shame
As a result, patients were often confined to their homes or hidden from the community due to the significant social stigma associated with disease.
Through education and outreach, the Collaborative Center for XDP hopes to lift the burden of shame and provide support for XDP patients and their families.

The Collaborative Center for XDP
A consortium of international experts working together to accelerate the pace of discovery in XDP.
2 main sites in collaboration for a cure Dr Sharma’s team at MGH
(coordinating center) Dr Lee’s team in the
Philippines.

The Collaborative Center for XDP
Our goals Accelerate research directed
towards effective treatments, and a cure
Raise awareness of the disease locally and internationally
Expand access to clinical care and treatments in the Philippines and abroad
Offer support to families who are suffering from XDP through outreach and advocacy

The Collaborative Center for XDP
A How will we do this? - TEAMWORK The Center has reached out to
experts all over the world to direct their talents to the problem of XDP:
Geneticists to find the causative mutation
Neuroscientists and cell biologists to determine why neurons in the brain malfunction or die
Clinicians to develop and trial effective treatments
Advocacy, education and interventional programs locally

The Collaborative Center for XDP
What are we doing in the Philippines? Determining the scope of
the disease burden and where needs are greatest in collaboration with the XDP Study Group
Expanding access to treatment Improving clinical infrastructure Empowering patients, care-
givers, advocates and communities
Building tissue banks to provide scientists with the tools they need to advance XDP research

The Collaborative Center for XDP
Our voluntary research involves assessing patients and family members
We are collecting: Medical and family history
information Perform a physical examination Blood sample (DNA genetic analysis) Skin biopsy (fibroblast cell line)
We will then use this information to: Form a bank of XDP patients and
families Allow detailed analysis of the
genetics to find targets for treatments and potential cures

Patient resources
American Dystonia Society www.dystoniasociety.org
Movement Disorders Society of the Philippines
The MGH XDP Center www.massgeneral.org/xdp

Further information regarding the Center and our research
Visit the XDP Center website http://www.massgeneral.org/xdp-center
Contact the XDP Center director, Nutan Sharma, M.D., Ph.D., at (617) 643-208
OR
Contact the genetic counselor and research coordinator, Trisha Multhaupt-Buell, MS at (617) 726-5470 [email protected]
Related Documents