Chris DeFlitch, MD, FACEP Penn State Hershey Medical Center Connected (CIS) Physician Champion Founder, Penn State Partners for Healthcare Engineering Director & Vice-Chair, Dept of Emergency Medicine Healthcare Engineering with Physician Directed Queuing (PDQ) (PDQ) TM TM Success Stories-Triage and Process with EDIS

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Chris DeFlitch, MD, FACEPPenn State Hershey Medical Center
Connected (CIS) Physician ChampionFounder, Penn State Partners for Healthcare Engineering
Director & Vice-Chair, Dept of Emergency Medicine
Healthcare Engineering with Physician Directed
Queuing (PDQ)(PDQ)TMTM
Success Stories-Triage and Process with EDIS

HEALTHCARE TODAYHEALTHCARE TODAY
BOARDERS No Beds for ED Patients HALLWAY Patients Ambulance DIVERSION Dissatisfied Providers Dissatisfied Patients Regulatory Issues
Define Capacity as Bed
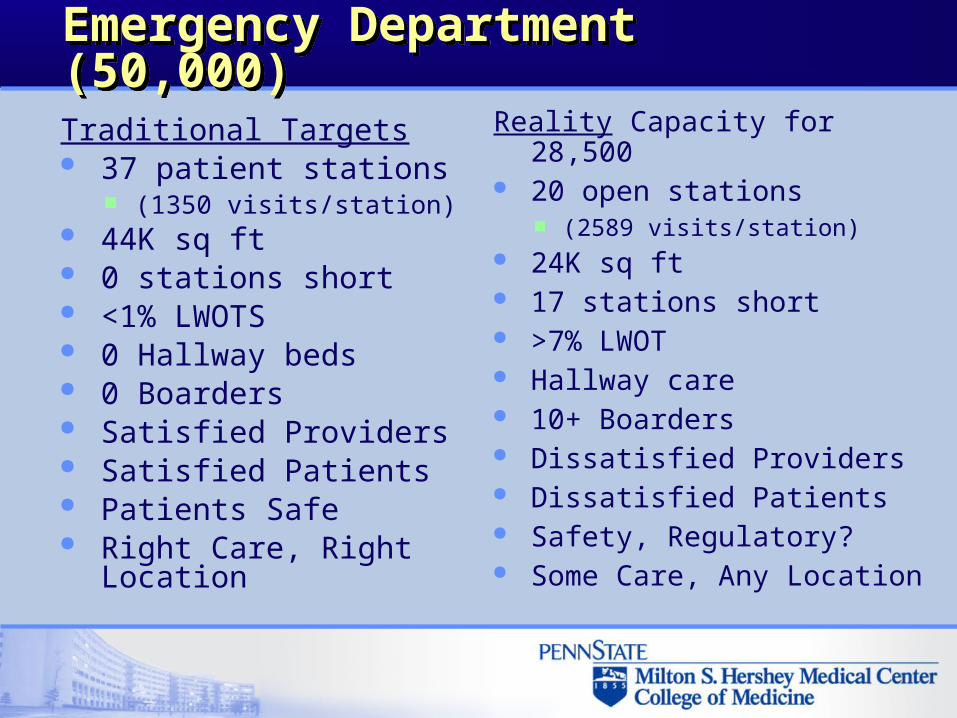
Emergency Department (50,000)Emergency Department (50,000)
Traditional Targets 37 patient stations
(1350 visits/station) 44K sq ft 0 stations short <1% LWOTS 0 Hallway beds 0 Boarders Satisfied Providers Satisfied Patients Patients Safe Right Care, Right
Location
Reality Capacity for 28,500 20 open stations
(2589 visits/station) 24K sq ft 17 stations short >7% LWOT Hallway care 10+ Boarders Dissatisfied Providers Dissatisfied Patients Safety, Regulatory? Some Care, Any Location
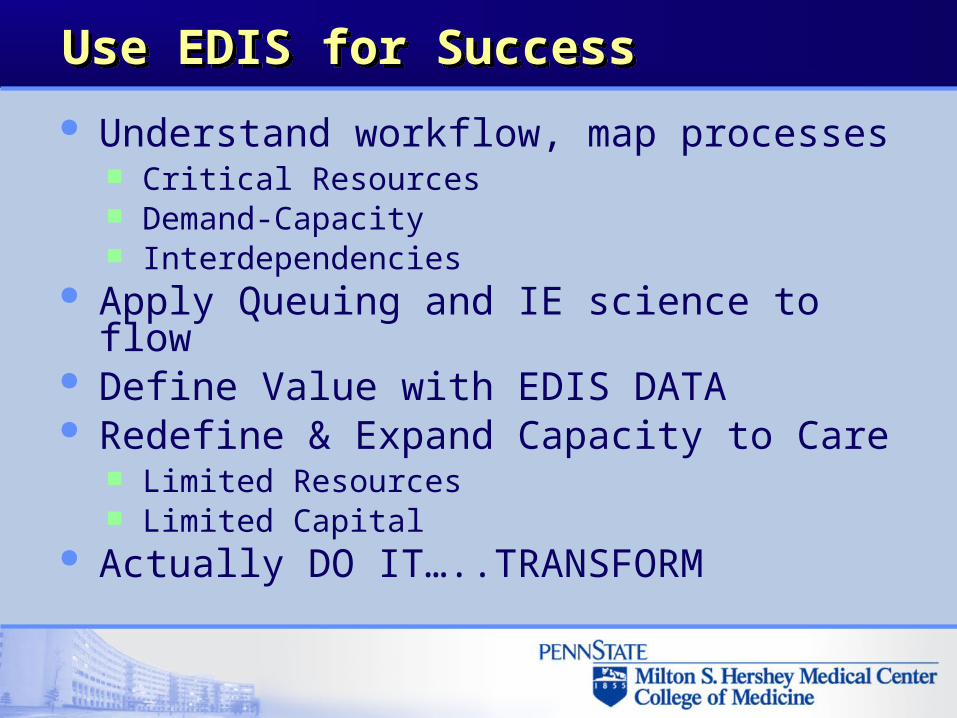
Use EDIS for Success Use EDIS for Success
Understand workflow, map processes Critical Resources Demand-Capacity Interdependencies
Apply Queuing and IE science to flow Define Value with EDIS DATA Redefine & Expand Capacity to Care
Limited Resources Limited Capital
Actually DO IT…..TRANSFORM

Add Operational DATA to WorkflowAdd Operational DATA to Workflow
Arrival distributions Critical Interval Processing Times Resources data, number and type Perspective Flows
Patient Provider Resources

Provider Perspective FlowsProvider Perspective Flows
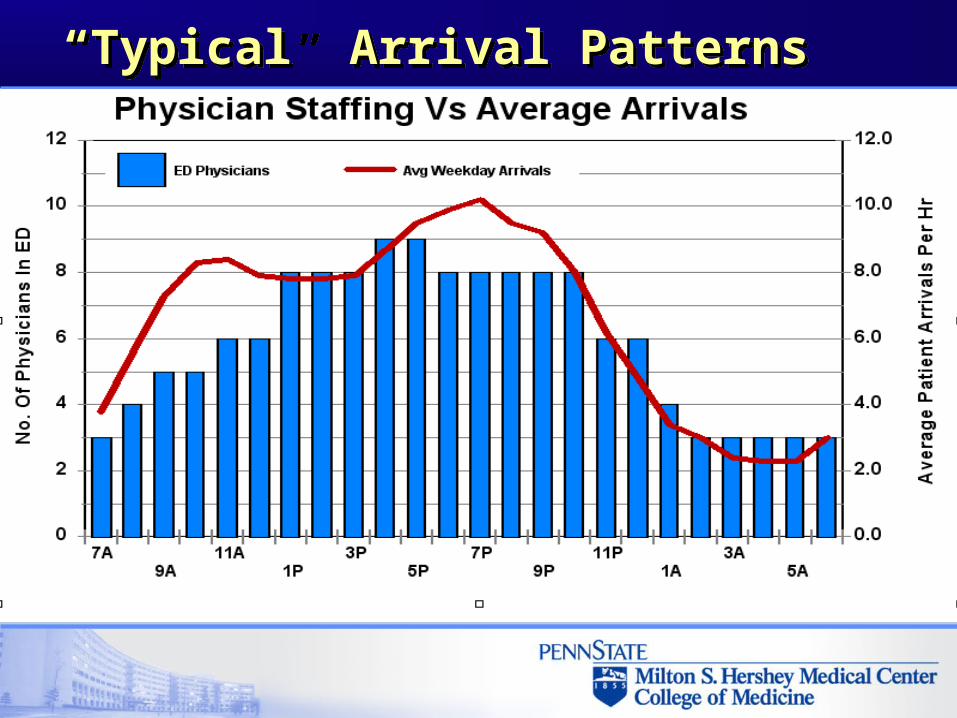
“Typical” Arrival Patterns“Typical” Arrival Patterns
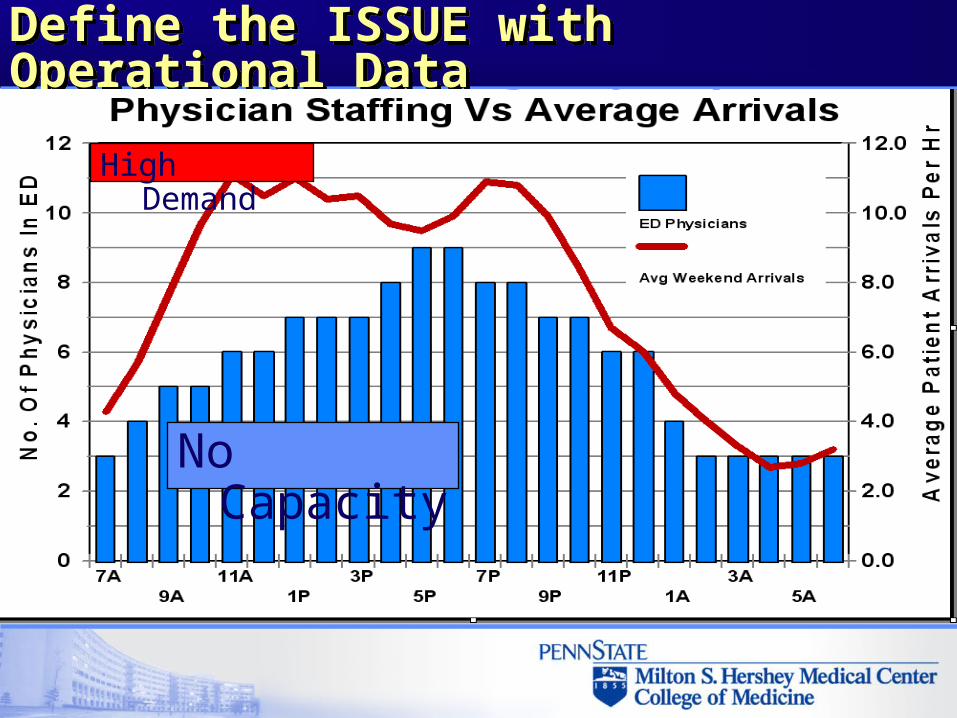
Define the ISSUE with Operational DataDefine the ISSUE with Operational Data
No Capacity
High Demand

Understand Queuing SystemsUnderstand Queuing Systems
Science of WAITING All queuing systems possess the same
basic elements: Customer (Demand) Resources (Capacity) Queues
When analyzed, it is clear that queuing systems are ubiquitous in healthcare.
“One mans WAIT is another mans WORK”

Value-Added Activity Value-Added Activity
Must be performed to meet customer needs
Adds form or feature to service
Enhances service quality
Customers willing to pay for this work
If you STOP the activity, would your customer complain? If yes, then it’s likely Value-Added.
George ML. Lean Six Sigma Pocket Toolbook. 2005
WASTE (non-value added)WASTE (non-value added) Handling beyond what
is minimally required to move work
Rework to fix errors Duplicative work Wait Idle time Delays Unnecessary motion Over processing (too
many steps to complete the job)
If you STOP activity, would any customer know the difference? If not, then it’s probably Non-Value-Added.
George ML. Lean Six Sigma Pocket Toolbook. 2005

Clinical Value AnalysisClinical Value Analysis

Clinical Value Streaming - TRIAGEClinical Value Streaming - TRIAGE

Clinical Value Streaming- CP TriageClinical Value Streaming- CP Triage

“Healthcare is the only industry I have ever heard of that actually has a name for a major category of waste. You have waiting rooms. Most organizations outside of healthcare would go bankrupt if they thought like this”.
“Healthcare is the only industry I have ever heard of that actually has a name for a major category of waste. You have waiting rooms. Most organizations outside of healthcare would go bankrupt if they thought like this”. Page 33 Lean-Six Sigma for Healthcare
Caldwell et al
“Infuse care into the queue (waiting) ….define capacity to CARE not a bed”“Infuse care into the queue (waiting) ….define capacity to CARE not a bed”
Penn State Healthcare Engineering TeamDeFlitch et al
Critical to Healthcare Engineer Critical to Healthcare Engineer
Burning Platform Defined CRITICAL Resource(s) &
interdependencies Boarders Ancillaries Information Providers Minimal Space
WITHOUT Adding Resources
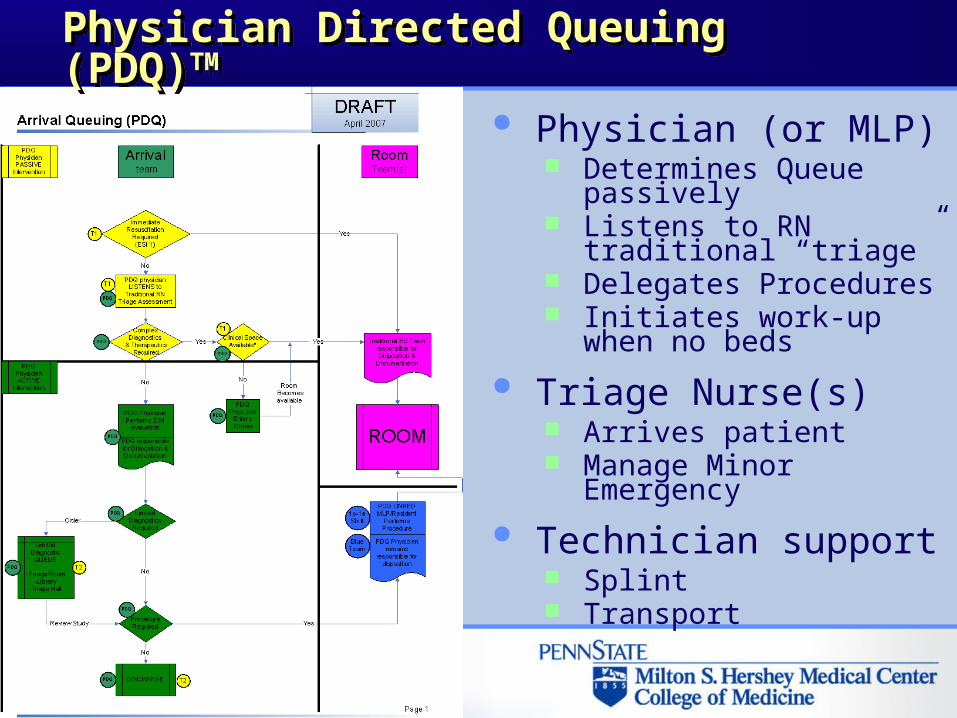
Physician (or MLP) Determines Queue
passively Listens to RN traditional
“triage” Delegates Procedures Initiates work-up when no
beds
Triage Nurse(s) Arrives patient Manage Minor Emergency
Technician support Splint Transport
Physician Directed Queuing (PDQ)TMPhysician Directed Queuing (PDQ)TM

PDQ Year-to-Year Results Comparison PDQ Year-to-Year Results Comparison
Baseline 5.6% 8h 6m
71 min 93 min 5h 34m 5h 51m
Healthcare Engineered 2.7% 6h 16m
45 min 60 min 3h 9m 1h 23m
LWBSLength of
StayDoor-RmDoor-DrESI 4ESI 5
52% 23%
37% 35% 44% 76%
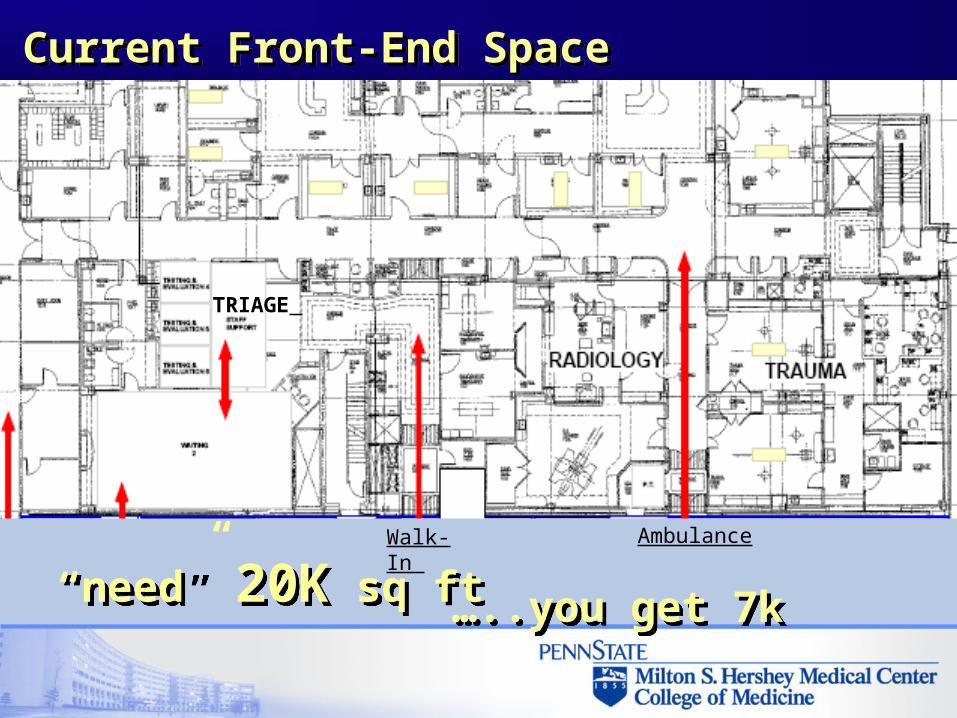
Current Front-End SpaceCurrent Front-End Space
AmbulanceWalk-In
TRIAGE
“need” 20K sq ft “need” 20K sq ft …..you get 7k …..you get 7k
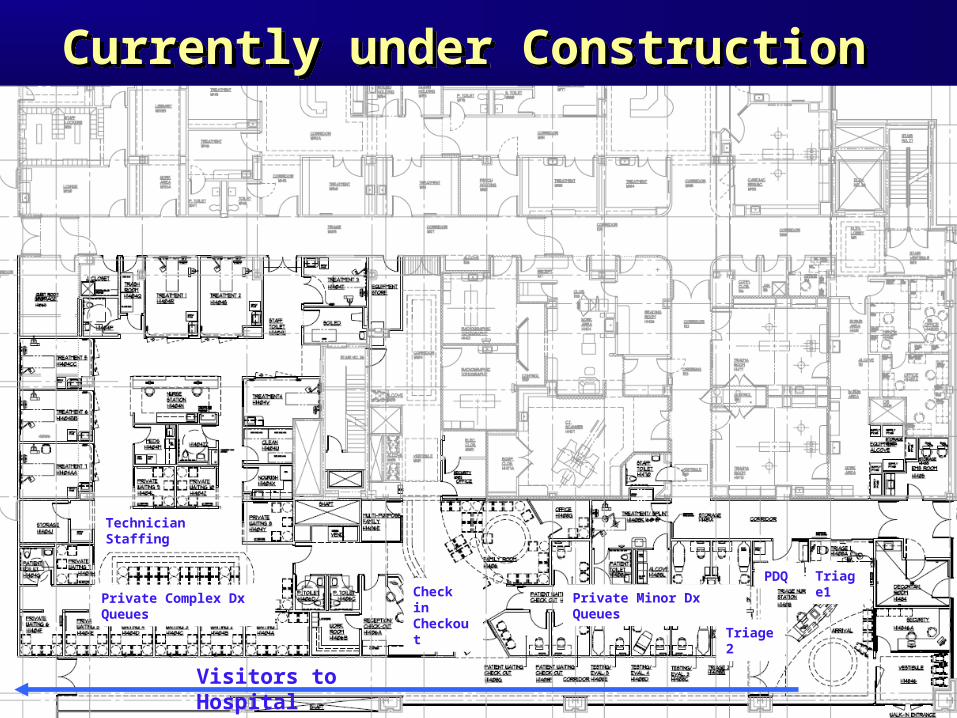
Currently under ConstructionCurrently under Construction
Visitors to Hospital
PDQ Triage1
Triage2
Check in Checkout
Private Complex Dx Queues
Technician Staffing
Private Minor Dx Queues
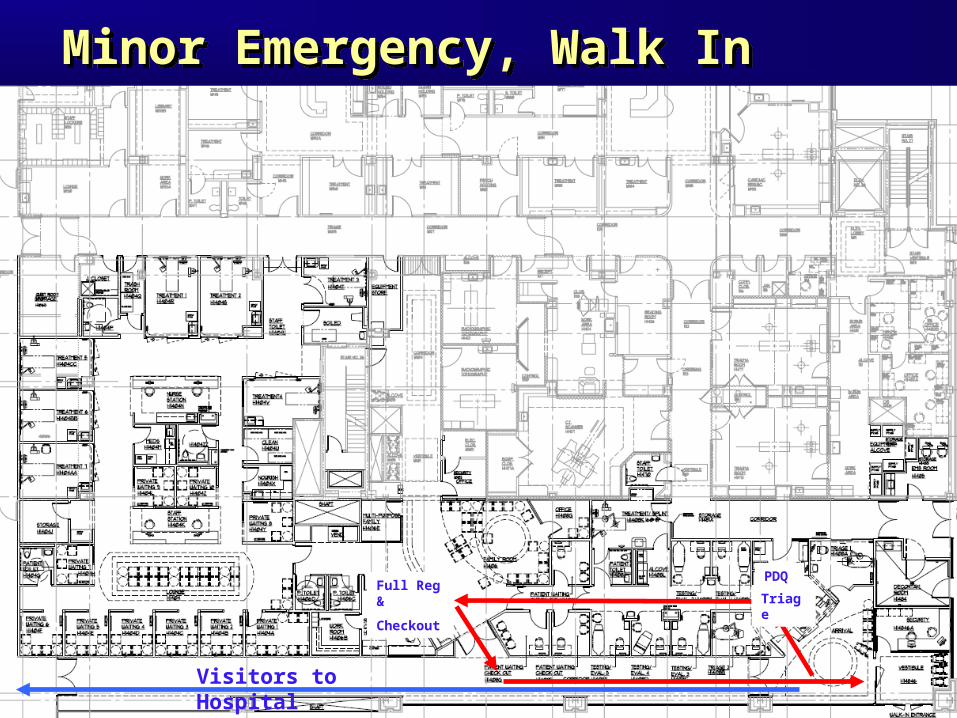
Minor Emergency, Walk InMinor Emergency, Walk In
Visitors to Hospital
Triage
PDQFull Reg &
Checkout
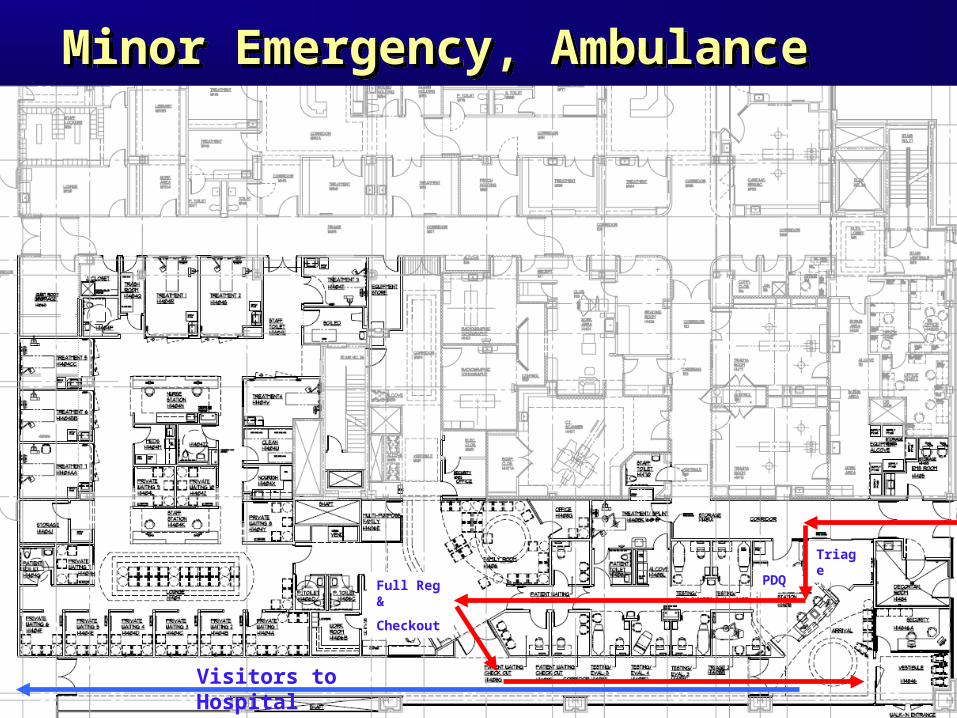
Minor Emergency, AmbulanceMinor Emergency, Ambulance
Visitors to Hospital
Triage
PDQFull Reg &
Checkout

Room Required & Available, Walk In Room Required & Available, Walk In
Visitors to Hospital
Triage

Room Required & Available, Ambulance Room Required & Available, Ambulance
Visitors to Hospital
Triage1Mini Reg
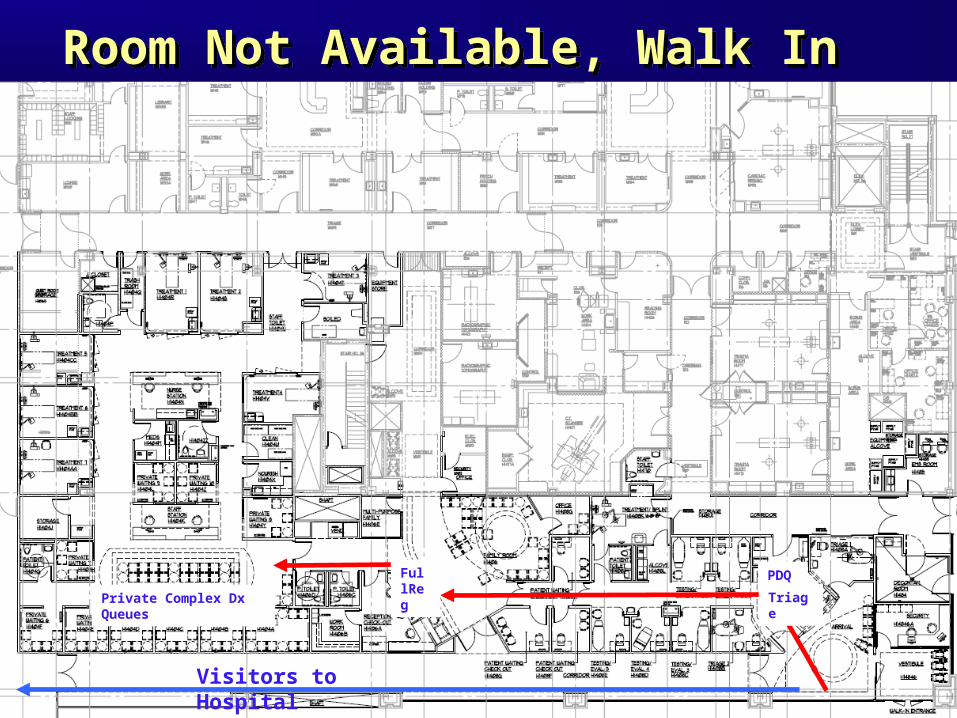
Room Not Available, Walk In Room Not Available, Walk In
Visitors to Hospital
Private Complex Dx Queues
FullReg
Triage
PDQ
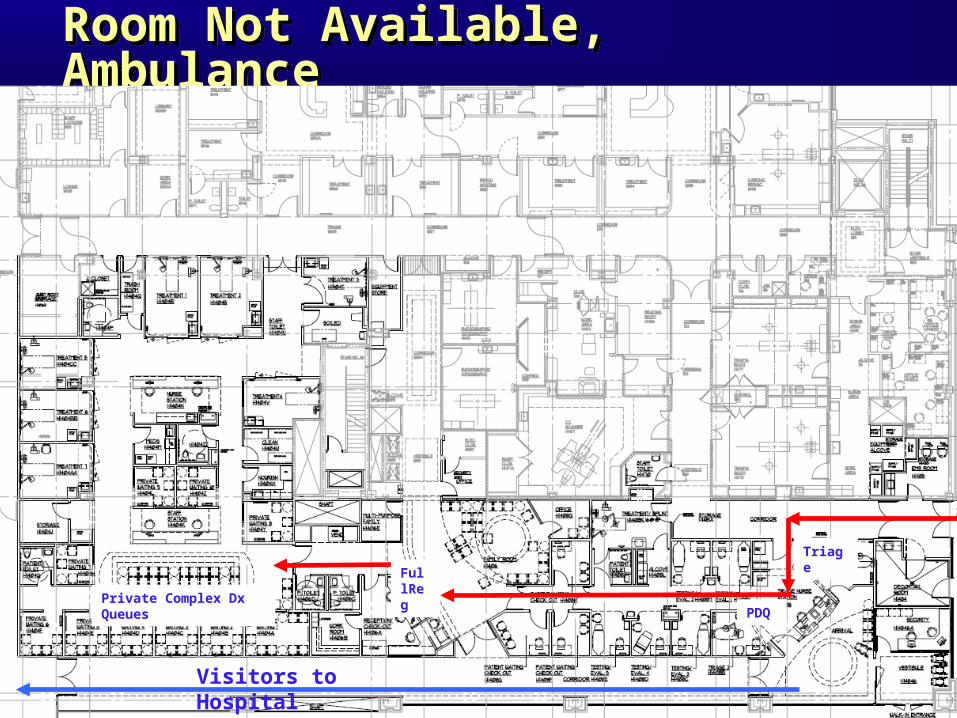
Room Not Available, Ambulance Room Not Available, Ambulance
Visitors to Hospital
Private Complex Dx Queues
FullReg
Triage
PDQ
Next Venues of Healthcare EngineeringNext Venues of Healthcare Engineering
Service Line Flow (Neurosurg) Peri-Op Processing (Operative Suites) Hospital Capacity Management Other Interdependent ED flows Informatics Project Management Quality Outcomes (MRSA, Diabetes) Process Simulation with OSGi

Future of HEALTHCARE ENGINEERINGFuture of HEALTHCARE ENGINEERING
Process simulation models Explicitly represent variability Predict interdependency Manage complex systems in a computer
Predict system performance under varying inputs (loads)
Compare alternative system designs Determine the effects of alternative
policies on system performance
Related Documents











