Choice of antihypertensive Peter von Dadelszen BMedSc, MBChB, DipObst, DPhil, FRANZCOG, FRCSC, FRCOG Associate Professor of Obstetrics & Gynaecology, UBC Consultant in Maternal-Fetal Medicine, BC Women’s Co-Director, CFRI Reproduction & Healthy Pregnancy Cluster PRE -eclampsia E clampsia M onitoring, Prevention & T reatment

Choice of antihypertensive Peter von Dadelszen BMedSc, MBChB, DipObst, DPhil, FRANZCOG, FRCSC, FRCOG Associate Professor of Obstetrics & Gynaecology, UBC.
Dec 17, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Choice of antihypertensive
Peter von DadelszenBMedSc, MBChB, DipObst, DPhil, FRANZCOG, FRCSC, FRCOG
Associate Professor of Obstetrics & Gynaecology, UBCConsultant in Maternal-Fetal Medicine, BC Women’s
Co-Director, CFRI Reproduction & Healthy Pregnancy Cluster
Dr Peter von DadelszenBMedSc, MBChB, DipObst, DPhil, FRANZCOG, FRCSC, FRCOG
Principal Investigator
Department of Obstetrics & Gynaecology, UBCReproduction & Healthy Pregnancy Cluster, CFRI Consultant in Maternal-Fetal Medicine, BC Women’s
2H30-4500 Oak Street, Vancouver, BC V6H 3N1, Canada
PRE-eclampsiaEclampsiaMonitoring,Prevention &Treatment
Phone: +1-604-875-3054 | Fax: +1-604-875-2725 | e-mail: [email protected]

Christchurch

PRE-EMPT(PRE-eclampsia-Eclampsia Monitoring, Prevention &
Treatment)
• Five objective, LMIC community intervention-focussed, pre-eclampsia project
• Funding:– Bill & Melinda Gates Foundation

Why use antihypertensives?
• Maternal stroke risk associated with both severe systolic and/or diastolic hypertension– sBP >160mmHg– dBP >110mmHg CEMACH 2007
• Severe hypertension associated with placental abruption and attendant maternal and perinatal risks
• Severe hypertension is included in most definitions of ‘severe’ pre-eclampsia, although such classification systems are flawed
Menzies et al. Hypertens Pregnancy 2007

Why use antihypertensives?
• In non-severe pregnancy hypertension – No clear evidence of benefit other than to reduce
the frequency of episodes of severe hypertension– May adversely effect fetal growth velocity
von Dadelszen et al. Lancet 2000
• Therefore, my focus will be on the pharmacological management of severe hypertension
The ‘ideal’ agent in rural & remote settings
• Oral administration• Reliable reduction in BP• Smooth reduction in BP• Rapid onset of action• Minimal overshoot
– BP in target range• sBP 130-160mmHg• dBP 80-110mmHg
From what can we choose?
• Hydralazine• Beta-blockers (& alpha-/beta-blockers)
– Atenolol– Labetalol
• Calcium channel blockers– Nifedipine
• Alpha-methyldopa• Angiotensin converting enzyme inhibitors• Angiotensin-II receptor blockers

From what can we choose?
• Hydralazine• Beta-blockers (& alpha-/beta-blockers)
– Atenolol– Labetalol
• Calcium channel blockers– Nifedipine
• Alpha-methyldopa• Angiotensin converting enzyme inhibitors• Angiotensin-II receptor blockers
– Risks of fetal renal toxicity and IUFD
From what can we choose?
•MgSO4 is NOT an antihypertensive

The ‘ideal’ agent in rural & remote settings
• Oral administration• Reliable reduction in BP• Smooth reduction in BP• Rapid onset of action• Minimal overshoot
– BP in target range• sBP 130-160mmHg• dBP 80-110mmHg

Oral administration
• Atenolol– No adverse effects on fetal growth when used acutely
• Labetalol• Methyldopa• Nifedipine capsules• Nifedipine intermediate acting
– PA/Retard• Hydralazine
Modified from: Magee & Abdullah. Expert Opin Drug Saf 2004
The ‘ideal’ agent in rural & remote settings
• Oral administration• Reliable reduction in BP• Smooth reduction in BP• Rapid onset of action• Minimal overshoot
– BP in target range• sBP 130-160mmHg• dBP 80-110mmHg
Reliable reduction in BPsevere hypertension
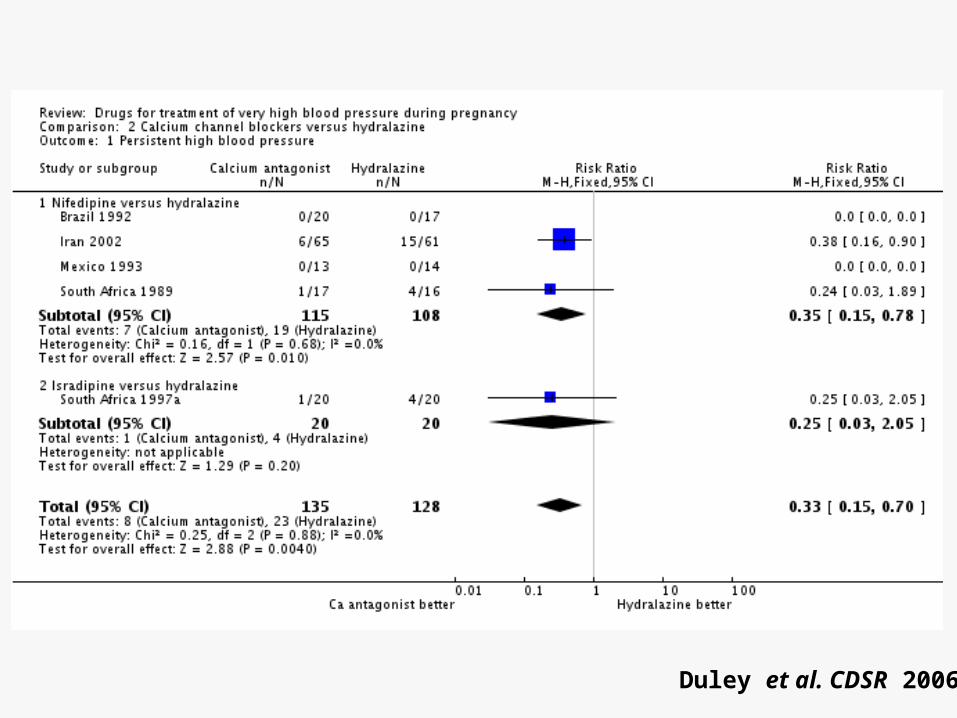
• CCBs are more reliable than hydralazine in lowering BP in pregnant women with severe hypertension
Magee et al. BMJ 2004Duley et al. CDSR 2006
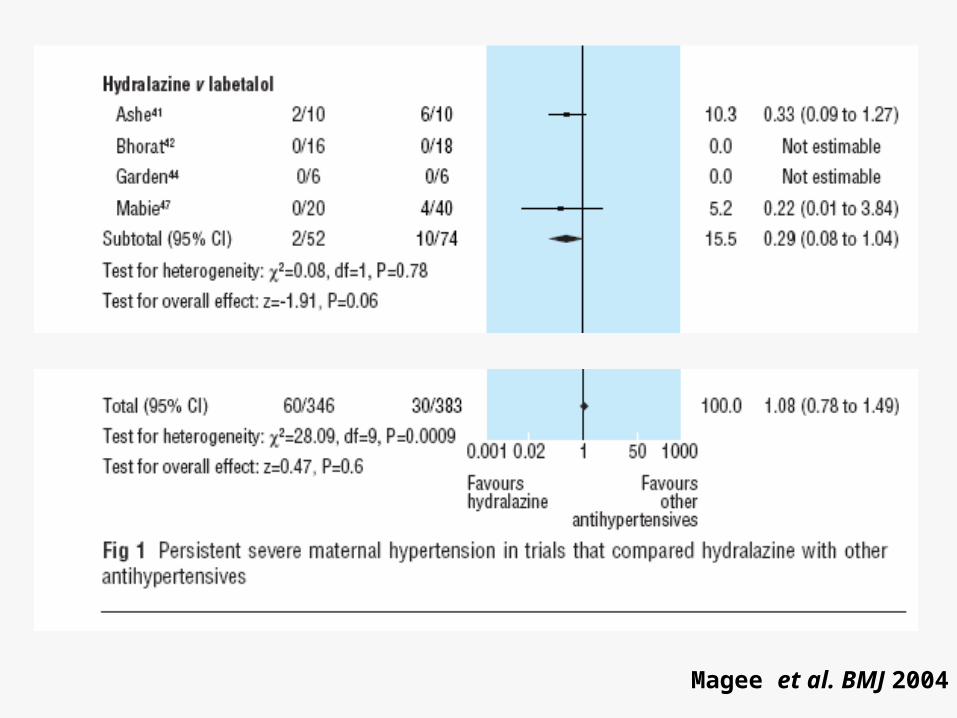
• Hydralazine appears more reliable than labetalolMagee et al. BMJ 2004
• Methyldopa may be an agent of choice for severe hypertension
Duley et al. CDSR 2006
Reliable reduction in BPsevere hypertension
• CCBs are more reliable than hydralazine in lowering BP in pregnant women with severe hypertension
Magee et al. BMJ 2004Duley et al. CDSR 2006
• Hydralazine appears more reliable than labetalolMagee et al. BMJ 2004
• Methyldopa may be an agent of choice for severe hypertension
Magee et al. BMJ 2004
Reliable reduction in BPsevere hypertension
• CCBs are more reliable than hydralazine in lowering BP in pregnant women with severe hypertension
Magee et al. BMJ 2004Duley et al. CDSR 2006
• Hydralazine appears more reliable than labetalolMagee et al. BMJ 2004
• Methyldopa may be an agent of choice for severe hypertension– Widely used – routinely on EMLs

The ‘ideal’ agent in rural & remote settings
• Oral administration• Reliable reduction in BP• Smooth reduction in BP• Rapid onset of action• Minimal overshoot
– BP in target range• sBP 130-160mmHg• dBP 80-110mmHg
Smooth reduction in BP
• The ideal agent will reduce BP effectively and over a relatively short period of time– <60min– Stabilise and reduce MAP by 10% per hour
• BP fall will not be precipitous– Adverse maternal CNS effects– Adverse fetal effects
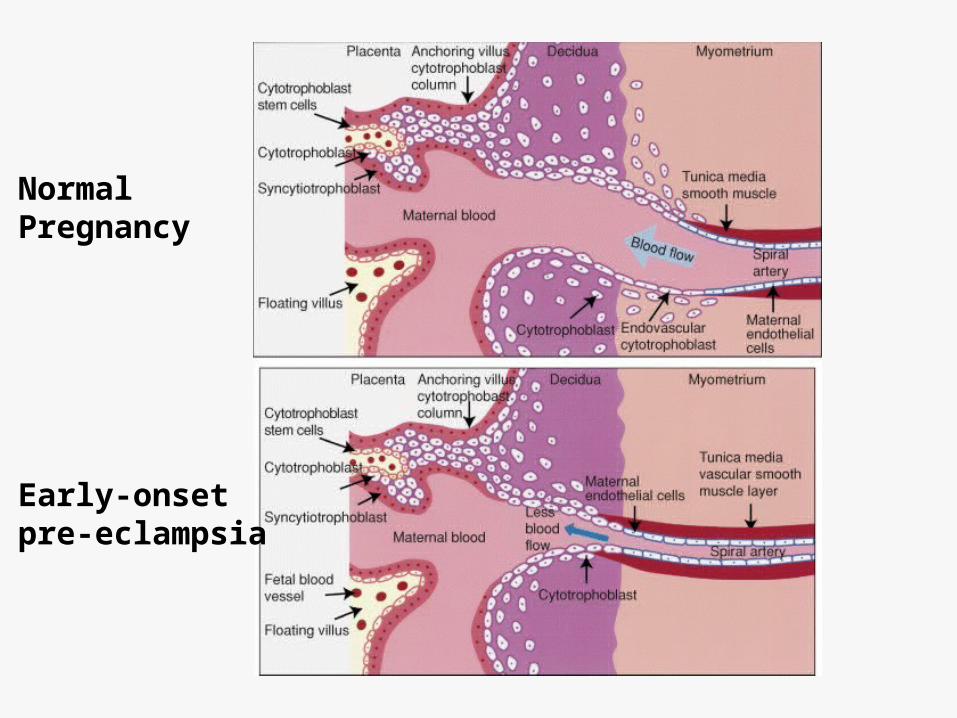
Normal Pregnancy
Early-onsetpre-eclampsia
The ‘ideal’ agent in rural & remote settings
• Oral administration• Reliable reduction in BP• Smooth reduction in BP• Rapid onset of action• Minimal overshoot
– BP in target range• sBP 130-160mmHg• dBP 80-110mmHg

‘Rapid’ onset of action
Modified from: Magee & Abdullah. Expert Opin Drug Saf 2004
Drug Dosage Onset Peak Duration
Atenolol 25 – 50 mg 1hr 2-4hr 24hr
(dose dependent)
Labetalol 200 mg 20min – 2hr 1-4 hr 8-12hr
(dose dependent)
Methyldopa 500 mg – 2 g 40 min 3-6hr 12-24hr
Nifedipine PA (or retard) 10 mg 30min 4hr 12hr
Nifedipine capsule 5 – 10 mg 5-10min 30min 6.5hr

The ‘ideal’ agent in rural & remote settings
• Oral administration• Reliable reduction in BP• Smooth reduction in BP• Rapid onset of action• Minimal overshoot
– BP in target range• sBP 130-160mmHg• dBP 80-110mmHg

Minimal overshoot
• CCBs less likely to cause overshoot than hydralazine Magee et al. BMJ 2004
• Beta-blockers less likely to cause overshoot than hydralazine Magee et al. BMJ 2004
• Nifedipine PA/Retard less likely to cause overshoot than capsules? Brown et al. AJOG 2002
– Small RCT– End-point (‘in range BP’) measured at time PA
approaching maximal effect

On balance• An intervention package should include 1 - 3 oral
antihypertensive agent(s)• The choice for a single antihypertensive lies between
methyldopa, nifedipine, and another beta-blocker, probably atenolol – labetalol is not on EMLs
• Theoretical and practical reasons to have all available– Combined CNS control, beta-blockade and vasodilatation– Second effective agent for women whose BP is resistant to
another agent • Reserve i.v. hydralazine for obtunded/comatose
women

PRE-EMPTObjective 3
• CLIP (Community-Level Interventions for Pre-eclampsia)
– Cluster randomised controlled trial of community level interventions for women with pre-eclampsia
– Aims• Can
– identification, – early risk stratification, and – initiation of life-saving treatment at the community level
• decrease pre-eclampsia-related maternal and perinatal mortality in LMIC?

CLIP• Intervention
– CLIP package of care• Case recognition & triage• Treatment of severe hypertension (sBP ≥160mmHg)
– Oral antihypertensive ? Atenolol; ? Nifedipine, ? Methyldopa– Intramuscular MgSO4 (5g each buttock)
• Treatment of eclampsia– Intramuscular MgSO4 (5g each buttock)
• Transfer into facilities offering evidence-based care – Setting
• Community – community health workers• Primary health units (not repeated)
The ‘ideal’ agent in rural & remote settings
• Oral administration• Reliable reduction in BP• Smooth reduction in BP• Rapid onset of action• Minimal overshoot
– BP in target range• sBP 130-160mmHg• dBP 80-110mmHg
Related Documents











