864 CHAPTER 21 Children’s Health and Education CRAIG T. RAMEY, SHARON LANDESMAN RAMEY, and ROBIN G. LANZI THE CONNECTION BETWEEN HEALTH AND EDUCATION 866 DEFINING BASIC TERMS: HEALTH, EDUCATION, AND DEVELOPMENT 866 APPLIED BIOSOCIAL CONTEXTUAL DEVELOPMENT: A CONCEPTUAL FRAMEWORK FOR UNDERSTANDING, DESIGNING, AND TESTING INTERVENTIONS TO IMPROVE CHILDREN’S HEALTH AND EDUCATION 867 OVERVIEW OF APPLICATION OF THE MODEL TO EARLY INTERVENTION RESEARCH 870 THE NATIONAL HEAD START-PUBLIC SCHOOL EARLY CHILDHOOD TRANSITION DEMONSTRATION PROJECT: A 31-SITE RANDOMIZED TRIAL TO PROVIDE COMPREHENSIVE HEAD START-LIKE SUPPORTS TO CHILDREN AND FAMILIES FROM KINDERGARTEN THROUGH THIRD GRADE 871 Study Purpose and History 871 Application of the Conceptual Framework to the Design and Evaluation of the Intervention 871 Measurement of Inputs, Processes, and Outcomes 874 Selected Findings from the National Transition Demonstration Study about Children’s Health and Education 874 PRINCIPLES OF EFFECTIVE INTERVENTION SUPPORTED BY LONGITUDINAL RESEARCH ON CHILDREN’S HEALTH AND EDUCATION 877 The Principle of Dosage 877 The Principle of Timing 879 The Principle of Direct Receipt of Services 880 The Principle of Differential Benefits 882 The Principle of Continuity of Supports 884 KEY FEATURES OF COLLABORATIVE AND COMMUNITY PARTICIPATORY RESEARCH 885 Universities and Public Policy 886 SUMMARY 888 REFERENCES 890 Children’s health and education can be facilitated by systematic supports that span traditional and innovative health care, health promotion, and disease prevention and that apply scientific principles about how young children learn and develop. Conversely, children’s de- velopment can be impaired by disease and injury, nonoptimal lifestyle, the presence of multiple risk fac- tors, and the failure to receive high-quality experiences to promote cognitive, social-emotional, and physical well-being. During the past half-century, a new field has emerged—prevention developmental science (e.g., Bryant, Windle, & West, 1997; Coie et al., 1993)—that systemati- cally integrates theories and methods from the broad fields of public health, psychology, medicine, sociology, and education to improve developmental outcomes for children at risk for a wide variety of poor outcomes in health and education. Exciting integrative advances in de- velopmental neuroscience have conjoined with prevention science to fuel design and implementation of studies about the fundamental interconnectedness of children’s health and education (e.g., C. T. Ramey & Ramey, 2004a; Teti, 2004). Indeed, many of the health disparities and in- equities in children’s educational attainment are likely the result of this complex interplay between health and educa- tion (e.g., Livingston, 2004). David Satcher, 16th surgeon general of the United States and now director of the National Center for Pri- mary Health Care at Morehouse School of Medicine, has used what is termed a health disparities lens to bring into focus the huge toll taken on the well-being of many individuals from historically marginalized and minority

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

864
CHAPTER 21
Children’s Health and Education
CRAIG T. RAMEY, SHARON LANDESMAN RAMEY, and ROBIN G. LANZI
THE CONNECTION BETWEEN HEALTH ANDEDUCATION 866
DEFINING BASIC TERMS: HEALTH, EDUCATION,AND DEVELOPMENT 866
APPLIED BIOSOCIAL CONTEXTUALDEVELOPMENT: A CONCEPTUAL FRAMEWORKFOR UNDERSTANDING, DESIGNING, ANDTESTING INTERVENTIONS TO IMPROVECHILDREN’S HEALTH AND EDUCATION 867
OVERVIEW OF APPLICATION OF THE MODEL TOEARLY INTERVENTION RESEARCH 870
THE NATIONAL HEAD START-PUBLIC SCHOOLEARLY CHILDHOOD TRANSITIONDEMONSTRATION PROJECT: A 31-SITERANDOMIZED TRIAL TO PROVIDECOMPREHENSIVE HEAD START-LIKESUPPORTS TO CHILDREN AND FAMILIESFROM KINDERGARTEN THROUGHTHIRD GRADE 871
Study Purpose and History 871
Application of the Conceptual Framework to the Designand Evaluation of the Intervention 871
Measurement of Inputs, Processes, and Outcomes 874Selected Findings from the National Transition
Demonstration Study about Children’s Health andEducation 874
PRINCIPLES OF EFFECTIVE INTERVENTIONSUPPORTED BY LONGITUDINAL RESEARCH ONCHILDREN’S HEALTH AND EDUCATION 877
The Principle of Dosage 877The Principle of Timing 879The Principle of Direct Receipt of Services 880The Principle of Differential Benefits 882The Principle of Continuity of Supports 884KEY FEATURES OF COLLABORATIVE AND
COMMUNITY PARTICIPATORY RESEARCH 885Universities and Public Policy 886SUMMARY 888REFERENCES 890
Children’s health and education can be facilitated bysystematic supports that span traditional and innovativehealth care, health promotion, and disease preventionand that apply scientific principles about how youngchildren learn and develop. Conversely, children’s de-velopment can be impaired by disease and injury,nonoptimal lifestyle, the presence of multiple risk fac-tors, and the failure to receive high-quality experiencesto promote cognitive, social-emotional, and physicalwell-being.
During the past half-century, a new field hasemerged—prevention developmental science (e.g., Bryant,Windle, & West, 1997; Coie et al., 1993)—that systemati-cally integrates theories and methods from the broadfields of public health, psychology, medicine, sociology,and education to improve developmental outcomes for
children at risk for a wide variety of poor outcomes inhealth and education. Exciting integrative advances in de-velopmental neuroscience have conjoined with preventionscience to fuel design and implementation of studies aboutthe fundamental interconnectedness of children’s healthand education (e.g., C. T. Ramey & Ramey, 2004a; Teti,2004). Indeed, many of the health disparities and in-equities in children’s educational attainment are likely theresult of this complex interplay between health and educa-tion (e.g., Livingston, 2004).
David Satcher, 16th surgeon general of the UnitedStates and now director of the National Center for Pri-mary Health Care at Morehouse School of Medicine, hasused what is termed a health disparities lens to bringinto focus the huge toll taken on the well-being of manyindividuals from historically marginalized and minority
dam4_c21.qxd 12/20/05 9:39 AM Page 864

Children’s Health and Education 865
groups, especially children of color and children withdisabilities. Satcher (2004, p. xxxi) summarized:
Although major progress has been made in reducing mor-bidity and mortality, as well as increasing the life ex-pectancy among vulnerable and at-risk populations, suchas African Americans, the ethnic divide continues towiden. As a matter of fact, in some cases it has even gottenworse! Because we are essentially dealing with the inher-ent complexities of human behavior on the micro or indi-vidual level, which are inextricably tied to ongoing factorsand conditions at the macro or societal level, the reasonsfor the lack of more substantial improvements over the en-suring years are complex. . . . To suffice, however, it canbe reasoned that increased vulnerability to adverse healthamong [targeted subgroups] is differentially mediated byvarious environmental factors and conditions. All of thesefactors and conditions serve to inf luence individuals’ per-sonal choices concerning health lifestyle choices; avail-ability, accessibility, and acceptability of services; and,ultimately, impact negatively on their physiologic func-tioning, hence the current health disparities dilemma. Atthe risk of oversimplifying a complex situation, what isdesperately needed at the macro level is health-care re-form to guide the nation’s policies and research agenda.
We concur that such health care reform is imperative,and argue further that the need for educational reform isequally compelling. Satcher’s (2004) observations aboutvulnerability apply soundly to educational inequities aswell as to health.
For more than 3 decades, we and many other develop-mental scientists have constructed broad conceptualframeworks that build on biological systems theory(e.g., Bertalanffy, 1975; Miller, 1978) and social ecol-ogy and Gestalt theory (e.g., Binder, 1972; Bronfenbren-ner, 1977, 1979; Lewin, 1936, 1951; Stokols, 1992,1996) and extended it to delineate social transactions(cf. Lewis, 1984; C. T. Ramey & Ramey, 1998a;Sameroff, 1983) that shape the course of individual de-velopment. These conceptual frameworks incorporatefundamental assumptions about the interconnectednessof the individual and the environment, biology and be-havior, and the dynamic nature of changes over time.Similarly, developmental science has acknowledged that“dividing the child” into separate functional strands ofdevelopment—such as perceptual, motor, cognitive, so-cial, emotional, and physical growth—is largely arbi-trary, based on historical disciplinary fields in whichdifferent aspects of human functioning were studied andtreated. Today, the evidence compellingly supports the
strong interdependencies among multiple domains (out-comes) of development; that is, a child’s development ismore aptly depicted as intertwined, overlapping, andcodetermined by influences within and outside the child.
The historical disciplinary isolation in both academiaand clinical and educational practices that serve children(e.g., education, pediatrics, psychiatry, social work, psy-chology, rehabilitation, nutrition, physical education)contributes to the lack of a common language and an ac-knowledged awkwardness in finding words to capturethis more integrated transdisciplinary and biosocialperspective. Many developmental and biological scien-tists have demonstrated the inadequacy of simplisticnature-versus-nurture formulations of development (e.g.,Borkowski, Ramey, & Bristol-Powers, 2002; Moser,Ramey, & Leonard, 1990; Shonkoff & Phillips, 2000);comparably, others have highlighted the flaws of tryingto measure independent contributions of the environmentto the individual, and vice versa (e.g., Landesman-Dwyer& Butterfield, 1983; Lewis, 1984; S. L. Ramey, 2002).We, too, struggle to overcome the dominance of the olderways of thinking. This is reflected in the fact that we stillemphasize that health includes mental health, that cogni-tion also refers to social and emotional cognition, andthat social competence is more than behavioral interac-tions but includes mental representations and problemsolving in the social realm. Indisputably, brain and be-havior are interdependent, perhaps fundamentally insep-arable; but current measurement strategies and analyticframeworks constrain how we formulate the role of chil-dren’s experiences in their biological and psychosocialbehavioral development, and how health impinges on ed-ucation and vice versa.
In this chapter, we describe the broad conceptualframework with which we have been working, known asapplied biosocial contextual development (ABCD), thatconsiders health and education as key outcomes influ-enced by individual, family, and environmental contextsand processes, incorporating biological and behavioralfactors. We then present an example of a multidiscipli-nary, longitudinal, large-scale, randomized trial thatembraced this conceptual framework to inform studyconceptualization, design, measurement, and analyticstrategy. We selectively highlight both health and edu-cational outcomes from these studies. Next, we identifyfive principles of effective early childhood interven-tions, supported by results from a wide array of random-ized controlled trials (RCTs) of early childhood healthand education interventions. We conclude that there is
dam4_c21.qxd 12/20/05 9:39 AM Page 865

866 Children’s Health and Education
great potential to apply theoretical, technological, andpractical advances in innovative ways to improve chil-dren’s well-being, to reduce health disparities, and toensure educational adequacy for all children (S. L.Ramey & Ramey, 2000). We outline key features ofcommunity collaborative and participatory research andrecommend that universities, scientific organizations,advocacy groups, philanthropy, government agencies,and professional practices seek new alliances that tran-scend the historical and political boundaries that con-tributed to unduly complex, inefficient, and oftenineffective systems for the delivery of health and educa-tion supports and for vigorous scientific inquiry.
THE CONNECTION BETWEEN HEALTHAND EDUCATION
Higher levels of educational attainment have long beenassociated with better health status among adults, andpoor health among children is widely recognized as animpediment to full participation in formal education (cf.Waldfogel & Danziger, 2001). That both educational at-tainment and health status are closely linked to socioe-conomic status, residential conditions, and the presenceof major disabilities also is irrefutable. What has notbeen explored carefully—particularly via prospective,longitudinal scientific inquiry with ethnically and eco-nomically diverse populations—are the ways health andeducation mutually and dynamically influence thecourse of a child’s life, and how educational and healthfactors in turn influence subsequent generations.
DEFINING BASIC TERMS: HEALTH,EDUCATION, AND DEVELOPMENT
To help promote a common language for the field ofyoung children’s health and education, we provide ex-plicit definitions of basic terms. We endorse the WorldHealth Organization’s (World Health Organization,2005) definition of “health” as “the state of completephysical, mental and social well-being and not merely theabsence of disease or infirmity.” The WHO definitionwas once considered revolutionary, with its emphasis onhealth as multifaceted, its endorsement of the centralityof mental and social well-being, and its position that
health was fundamentally synonymous with complete,optimal human functioning.
We regret that the term “education” is frequentlyused in a quite narrow way to refer only to the formalsystem of external supports to instruct children academ-ically, often reducing education to a variable measuredas “years of education,” or “most advanced degreeearned.” Alternatively, we advocate a broader definitionof education intended to reflect an individual’s actualattainment and application of knowledge and skills. TheRandom House Dictionary of the English Language,second edition, Webster’s unabridged (1987, p. 621),defines education as “ the active process of imparting oracquiring general knowledge, developing the powers ofreasoning and judgment, and generally of preparing one-self or others intellectually for mature life.” Education,thus defined, encompasses many life experiences out-side of formal schooling and didactic instruction. Unde-niably, one of the major childhood tasks is to do well inschool and to participate in the formal system of educa-tion; yet increasingly, social and life skills are recog-nized by educators and parents as vital to a child’slearning. In this chapter, we use the term education torepresent the child’s own acquisition of intellectual com-petencies, including practical, creative, and logical-deductive thinking. As such, education is a measurable,multifaceted child outcome, just as health is.
We use the term “development” to capture an ongo-ing set of biological, psychological, and social processesthat result in measurable change(s) at the individuallevel that ref lect increasing dif ferentiation and hierar-chical integration of functions. Development is oftendescribed in everyday terms such as increased compe-tencies, greater maturity, and more refined and adapt-able skills, which in turn help a child prepare for a largenumber of diverse and often unexpected encounters andlife challenges. Development progresses in ways thatalter both internal functioning and external behavior.Internal functioning includes sensory and motor percep-tions, feelings, thinking, remembering, and metacogni-tive strategies that help a child to govern his or herplans, reasoning, and actions; external behavior spansbasic actions to complex performance in everyday situa-tions and in formal evaluations or tests of skill, knowl-edge, and problem solving. Development can includeincremental, steady changes as well as major transfor-mations and the emergence of new classes of behaviorsat different times and stages of life. Ultimately, devel-
dam4_c21.qxd 12/20/05 9:39 AM Page 866

Applied Biosocial Contextual Development 867
opment is purposive, such that development contributesto the individual’s increased adaptability and effective-ness of thoughts and behavior, including social transac-tions, which in turn promote the individual’s ability tounderstand the world and successfully contribute in anethically principled and constructive manner to his orher society and its future.
Collectively, these terms characterize important uni-versal goals for children: that children develop in waysthat promote their health and their education and thatchildren’s health and education directly contribute toand are part of their development.
APPLIED BIOSOCIAL CONTEXTUALDEVELOPMENT: A CONCEPTUALFRAMEWORK FOR UNDERSTANDING,DESIGNING, AND TESTINGINTERVENTIONS TO IMPROVECHILDREN’S HEALTH AND EDUCATION
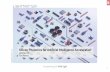
Figure 21.1 presents the conceptual framework withwhich we work, named applied biosocial contextualdevelopment (C. T. Ramey, MacPhee, & Yeates, 1982;C. T. Ramey & Ramey, 1998a; S. L. Ramey & Ramey,1992). ABCD incorporates both health and educationas explicit outcomes, through pathways that representmultiple levels and sources of influence on a child’sdevelopment. ABCD is well-suited for designing, im-plementing, and evaluating early interventions andpreventive programs to improve children’s health andeducation outcomes, because ABCD addresses thewhole child in the child’s natural multiple settings andenvironments.
In the left column of Figure 21.1, the box labeledChild is centered within the Family, because young chil-dren are dependent on the care of others (note: As a con-vention, we capitalize words that denote majorcomponents in the figure). The term Family meansthose caring for the child, regardless of whether they re-side together, and recognizing that roles and legal rela-tionships may fluctuate over time. Family identifiesthose people who assume the ethical, practical, and legalresponsibility for a child. Next, the child and family aresurrounded by eight boxes indicating major domains offunctioning and influence. The status of the child andfamily in each domain is hypothesized to be interre-
lated. A holistic picture of a child and family is a centralfeature of ABCD, such that study of one aspect of devel-opment, such as a child’s health status or a child’s read-ing achievement, is likely to be advanced through morecomprehensive study of what is happening in multipledomains of the child’s and the family’s life. Though thisis cumbersome for research and for those who imple-ment interventions to improve child outcomes, the fail-ure to recognize this reality often becomes a seriousobstacle to realizing desired comprehensive outcomes.The eight domains are Survival Resources to meet thechild’s and family’s basic needs; Health and Nutrition;Safety and Security; Appraisal of Self; Motivation andValues related to child and family functioning; SocialSupport; Communication Skills; and Basic Academic,Social, and Work Skills.
Figure 21.1 shows multiple influences on the eightfunctional domains, deriving from (a) the CommunityContext, with its specific Community Resources; and(b) Biology and Prior Experiences. The CommunityContext can be measured from the closely proximal tomore distal relationships in the young child’s life, andincludes Community Resources, such as Social andChild Care Supports, Supports for Learning, PhysicalSupports, Health Services, and School Systems. Foryoung children, these community resources often di-rectly influence their health and education status, withresources impinging on family supports for the child(e.g., job training and literacy, parenting programs, sub-stance abuse and mental health treatments for familymembers) and sometimes directly affecting the child(e.g., exposure to toxic substances, risk while in childcare, supports from school readiness programs). Ofequal theoretical importance are influences subsumedin the lower box labeled Biology and Prior Experiences.These include Intergenerational Influences, IndividualBiology, and the cumulative experiences of a child andthe child’s family members. We admit that trying to dis-play a dynamic, ever-changing systems theory in a two-dimensional, static, black-and-white format that fitsonto one page is a nearly insurmountable challenge, andwe judge our pictorial representation to be limited inadequately reflecting the complex pathways and feed-back loops that are so eloquently identified by DavidSatcher (2004; see earlier quote). A video representa-tion illustrating how distinctive, time-distributed inputsand processes would be a more suitable format for cap-turing the ABCD framework. For now, the words and
dam4_c21.qxd 12/20/05 9:39 AM Page 867

868 Children’s Health and Education
Figure 21.1 Applied biosocial contextual development (ABCD): a conceptual framework for health and education interventions.
Health • Physical • Mental • Social
Education • Knowledge • Skills • Achievement (Performance)
PersonalConstructs • Ethics/Values • Engagement • Enjoyment
OutcomesProcessesInputs
Health Promotionand Health Care • Health Care - Accessible - Appropriate - Acceptable • Healthy Lifestyle Behaviors
EducationPrograms andSupports • At School • At Home • In the Community
Social Supportand Services • Instrumental • Informational • Emotional • Affiliative
Social-Emotional • Poor Quality Childcare and Education • Poor Parenting Practices • Neglect
Societal • External Threats to Community • Lack of Adequate Information and Education • Economic Turmoil • Racism and Discrimination
Physical Risks • Crime and Violence • Toxins • Unsafe Environments • Abuse
Promotive ProcessesHarmful Factors and Stressors
Family
Child
SocialSupport
Motivationand Values
Appraisalof Self
Safety andSecurity
Health andNutrition
SurvivalResources
BasicAcademic,Social and
Work Skills
Comm-unicaton
Skills
Biology and Prior Experiencese.g., Intergenerational Influences,Individual Biology, Previous Childand Family Experience
Community Contexte.g., Location, Demography/Diversity, Economic and Political Climate, Infrastructure, Neighborhood
Community ResourcesSocial andChild CareSupports
Supportsfor
Learning
PhysicalSupports
HealthServices
SchoolSystems
Stre
ngth
s an
d N
eeds
• C
hild
• F
amily
• S
choo
l •
Hea
lth •
Com
mun
ity
= Inputs
= Processes
= Outcomes
Key to Model
the reader’s own comprehension of the extensive devel-opmental science findings of the past century will haveto suffice.
As a systems theory, a fundamental premise ofABCD is that changes in the child and the family serveto alter both biology and experiences, as well as to pos-sibly alter community context and community resources,particularly when children and families change in waysthat affect the availability, the appropriateness, and/orthe acceptability of prior community resources.
Together, the child’s functioning in all of the majordomains serves to undergird what are defined as out-comes, that is, the formal assessment at a specified timeor a sequential portrayal of a child’s status at multipletime points (i.e., developmental trajectory). We ac-knowledge that there is considerable ambiguity and cir-cularity in separating an outcome from a child’sfunctioning. In fact, we think these are one and thesame, in many cases, because the very processes inextri-cably linked to a child’s development are what become
dam4_c21.qxd 12/20/05 9:39 AM Page 868

Applied Biosocial Contextual Development 869
part of the measurement of an identified outcome. Forexample, a child’s experiences in the realm of languageand how a child functions in terms of everyday commu-nication and academic aspects of language and literacyare actually simultaneously developmental processesand developmental outcomes. In the realm of health, forinstance, how a child’s body handles the metabolism ofcarbohydrates is part of what defines an outcome relatedto hyperglycemia (e.g., risk for or presence of diabetes).Typically, the term “outcome” is one of convenience forclinical, administrative, and research purposes, as acheck on the child’s status at a moment in time. Some-times, an outcome is represented in terms of a moreglobal and personally meaningful or valued outcome,such as “doing well in school,” which is a composite ormultifaceted outcome with many indicators rather thana single measure. Rarely are outcomes amenable to mea-surement in absolute terms, even when the outcome is abiomedical marker. For example, over the past severaldecades, the clinical definitions used to diagnose dia-betes, childhood obesity, and childhood autism havechanged considerably (they are relative definitions, notabsolutes). Similarly, intellectual and education out-comes rely primarily on nationally normed standardizedtests, which means that approximately half of all chil-dren will always be classified as “below national aver-age,” even if all children realized considerable gains inabsolute levels of academic achievement. Accordingly,when selecting outcomes, scientists and practitionersbenefit from seeking a consensus about what are posi-tive, valued, and adaptive health and education out-comes for young children. Outcomes can never bevalue-free, although the measurements can become in-creasingly well specified, standardized, and scored inways that allow valid comparisons of changes over time,cohorts, and contexts.
This values and relativistic perspective is part of thereason the name of our conceptual model includes theterm “contextual.” Applied biosocial contextual devel-opment is basically an inductive framework to promoteincorporating new findings and greater specificity anddirectionality to its components, and eventually to in-form interventions that are designed to be maximally ef-fective and efficient in yielding desired (valued) childhealth and education outcomes.
In the realm of outcomes (depicted as octagons on thefar right of Figure 21.1), we display the well-recognizedareas of Health and Education, as well as a third out-
come to encompass dimensions of a child’s life that donot easily fit within health and education. We hearkenback to the pioneering work of George Kelly (1955),who advanced the concept of “personal constructs.”Kelly’s innovative contribution was to bring a phenome-nological (personal, experiential) perspective to bear onthe major issues in psychology. How an individual un-derstands his or her world, and the personal value as-signed to experiences, is an undeniable filter, one thatperhaps has been overlooked for too long in the field ofdevelopmental science. Similarly, Vygotsky (1978) ad-vanced the theory that consciousness was an end productof socialization, and explicitly identified a cognitive-cultural component that served a central role in creatingthe child’s individual reality. Rarely are these dimen-sions included in the study of young children’s healthand education. By explicitly including this personal con-structs dimension, ABCD advances the idea that chil-dren may respond differently (i.e., in an idiographicway) to the same environments—even environments con-sidered “good” or “bad” for most children—and that thereasons for differential responding transcend variablessuch as age, gender, ethnicity, skill level, and pres-ence/absence of major health conditions. Also, we pro-vide examples of meaningful dimensions of life such asEthics/Values, Engagement, Enjoyment, and PerceivedSocial Support because they capture highly valued as-pects of life that are not included in conventional out-come measures of health and education.
The processes hypothesized to influence outcomes(depicted in circles in the center of Figure 21.1) are rep-resented in terms of two major types: PromotiveProcesses and Harmful Factors and Stressors. Depend-ing on the focus of a study and an intervention, greateror lesser specificity about the particular types ofprocesses is needed. Children’s outcomes, in general,are hypothesized to be supported by Educational Pro-grams and Supports at School, Home, and in the Com-munity; by Social Support and Services that provideInstrumental, Informational, Emotional, and affiliativesupport (e.g., Reid, Ramey, & Burchinal, 1990); and byhealth promotion and health care, including healthylifestyle behaviors. Even when children receive promo-tive supports, their development can be threatened byHarmful Factors and Stressors. These represent actualrisks the child experiences directly, not merely the com-munity or family context that may increase or decreasethe probability that risks will occur. Harm can occur in
dam4_c21.qxd 12/20/05 9:39 AM Page 869

870 Children’s Health and Education
many domains, including the child’s physical, social andemotional, and personal constructs development. In gen-eral, harmful factors and stressors have exerted a strongeffect on children’s outcomes, although there has beenhigh interest in children who appear resilient, invulnera-ble, or successful in overcoming these risk factors (e.g.,Garmezy, 1983; Grotberg, 2003; Rutter, 2000; Werner,Bierman, & French, 1971).
OVERVIEW OF APPLICATION OFTHE MODEL TO EARLYINTERVENTION RESEARCH
The ABCD conceptual framework has been used forseveral multidisciplinary RCTs of prevention and inter-vention programs in early childhood. These include theAbecedarian Project and Project CARE (e.g., Camp-bell, Pungello, Burchinal, & Ramey, 2001; Campbell,Ramey, Pungello, Sparling, & Miller-Johnson, 2002;C. T. Ramey, Bryant, Campbell, Sparling, & Wasik,1988; C. T. Ramey & Ramey, 1998b; Wasik, Ramey,Bryant, & Sparling, 1990), which sought to prevent in-tellectual disabilities and to improve school achieve-ment among extremely low resource families; theeight-site RCT called the Infant Health and Develop-ment Program (IHDP), which adapted the AbecedarianProject and CARE early intervention program foruse in the first 3 years of life with premature, low-birthweight infants (e.g., IHDP, 1990; C. T. Rameyet al., 1992); and the National Head Start-PublicSchool Transition Demonstration Project conducted in31 sites to test the effectiveness of 4 continuous yearsof comprehensive health and education supports (cf.S. L. Ramey, Ramey, & Phillips, 1997; S. L. Rameyet al., 2001; the latter study is described in detail laterin the chapter). All of these studies were grounded intheory and prior research findings and adopted an ex-plicit and broad integrative, multidisciplinary concep-tual framework, derived from ABCD, (a) to inform thedesign of the intervention or prevention strategy; (b) toselect the measurement approach to document inputs,processes, and outcomes; (c) to guide the data analysesthat considered multiple and intersecting influences onthe major health and education outcomes; and (d) to re-fine and further specify the nature and magnitude ofinfluences on child developmental trajectories in spec-ified developmental domains.
In writing this chapter, we would like to acknowl-edge that it has not been “standard science” to endeavorto conduct a rigorous study of both health and educa-tion for young children within a single longitudinalstudy. Although almost all longitudinal research in de-velopmental psychology includes some marker-levelvariables in health and education, research historicallyhas been more focused, studying, for example, chil-dren’s mental illnesses (usually a particular form ofmental illness), children’s cognitive and academic de-velopment, children’s social skills and behavioral prob-lems, or children’s medical illnesses or injuries. Thesestudies have led to a rich scientific literature in thesediscrete but remarkably unlinked fields. The scientificjournals have multiplied and become, in most cases,narrower and more topic-specific, with only a few inte-grative and transdisciplinary in their focus. This re-flects, in large part, the traditional organization ofuniversities into departments and schools, as well asthe scientific review process that favors proposals thatare more narrowly focused. For an argument in favor ofmajor university reform to support multidisciplinaryand transdisciplinary scientific inquiry and practicerelated to children’s health and education, see S. L.Ramey and Ramey (1997b) and C. T. Ramey andRamey (1997b).
There is strong evidence that the National Institutesof Health (NIH) has embraced the need for new, innova-tive, and integrative approaches—with correspondingimplications for university organization and opera-tions—in the evolving NIH road map (described on theNIH Web site), as well as the reorganized National Sci-ence Foundation, the National Academy of Sciences inthe U.S. Department of Education (e.g., see the out-standing summary of early childhood research by Shon-koff & Phillips, 2000), and the Institute of EducationSciences, newly created by the U.S. Congress.
We judge the greatest challenges that derive fromABCD to be the discovery of ways to support the prepa-ration of scientists, practitioners, and policy shapers towork collaboratively and to understand this integrativeworldview of how children develop. An urgent priorityis to align intervention, prevention, and promotion ac-tivities in productive and open ways with research,practice, evaluation, and policies to achieve maximalbenefit for children, their families, their communities,and society at large (S. L. Ramey & Ramey, 2000). Anexceptionally promising line of scientific inquiry di-rectly addresses the dynamic relationship of a child’s
dam4_c21.qxd 12/20/05 9:39 AM Page 870

The National Head Start-Public School Early Childhood Transition Demonstration Project 871
education to his or her health and the ways healthierchildren may be more likely to benefit from opportuni-ties to advance their education. In turn, intergenera-tional effects of increased health and increasededucation may convey particular benefits to the nextgeneration, mediated through interdependent biologicaland social mechanisms.
THE NATIONAL HEAD START-PUBLICSCHOOL EARLY CHILDHOODTRANSITION DEMONSTRATION PROJECT:A 31-SITE RANDOMIZED TRIAL TOPROVIDE COMPREHENSIVE HEAD START-LIKE SUPPORTS TO CHILDREN ANDFAMILIES FROM KINDERGARTENTHROUGH THIRD GRADE
In this section, we provide an overview of a longitudi-nal and experimental study that adopted a preventionscience approach to the design and measurement ofsystematic, multipronged health and education inter-ventions to decrease risk and to increase both the edu-cational competence and the health and well-being ofyoung vulnerable children. We selected this study be-cause it represents a well-supported, multiyear effortto transform the field of early childhood inquiry by en-gaging individuals from multiple disciplines; workingclosely with practitioners, scientists, and policymakersfrom the start and throughout the project; establishinginternal and external oversight mechanisms to promotescientific rigor and integrity; and creating public usedata sets that are amenable to productive secondarydata analyses to advance the field. Within the confinesand intent of this chapter, we do not strive to provide acompendium of all the findings from this research proj-ect. Rather, we selectively describe the project’s pur-poses, delineate the key components of the interventionprogram and its corresponding data collection strate-gies, and report some of the findings to date that haveimplications for practice, policy, and future large-scalestudies of health and education.
Study Purpose and History
In 1991, the U.S. Congress passed legislation titled theHead Start Transition Project Act, authorizing fundingto test the value of extending comprehensive and contin-
uous Head Start-like service and supports to childrenfor the first 4 years of elementary school. Local sitescompeted for funding to do the following: (a) developpromising strategies in which Head Start programs, par-ents, local education agencies (LEA), and other commu-nity agencies joined together to plan and implement acoordinated, continuous program of comprehensive ser-vices for low-income children and their families begin-ning in Head Start and continuing through third grade;(b) to develop ways to support the active involvement ofparents in their education of their children; and (c) toconduct rigorous research at the local and national lev-els, using a randomized design to assign children andschools to the transition demonstration condition or thecomparison group. The 31 funded sites were dispersedacross 30 states and one Indian nation. More than 8,700former Head Start children were enrolled and nearly3,000 additional classmates. A distinctive feature ofthis intervention was that it was provided for the entireclassroom, rather than just singling out former HeadStart children.
Application of the Conceptual Framework tothe Design and Evaluation of the Intervention
Figure 21.2 shows how ABCD was used to help framethe conceptualization of the interventions and to repre-sent, in a general way, how the health and educationcomponents of the intervention were hypothesized toimprove child health and education outcomes. As shownon the lower left side of the figure, the Planning Stage (a1-year period) for the Transition Demonstration Pro-gram involved local adaptation of a national ProgramModel that mandated certain components to achieve the“comprehensive Head Start-like” feature of the pro-gram. The model established a Governing Board (withat least 51% of membership from parents of children tobe served); local decision making regarding ProgramImplementation (the logistics of who would be hired,how local partnerships would be formed and operate,and specific plans to change Community Resources de-signed to improve outcomes); and Program Costs (an es-sential area for ensuring that intervention programs canbe adequately implemented and replicated across sites).
The Planning Stage also involved creating and nurtur-ing a National Consortium of the 31 sites, with each sitehaving a three-way partnership of Head Start, the publicschools, and an evaluation team typically at a universityor research firm. At the national level, the consortium
dam4_c21.qxd 12/20/05 9:39 AM Page 871

872
Fig
ure
21.
2T
he c
once
ptua
l fr
amew
ork
used
for
the
Nat
iona
l T
rans
itio
n D
emon
stra
tion
Pro
gram
. So
urce
:F
rom
“E
valu
atin
g E
duca
tion
al P
rogr
ams:
Str
ateg
ies
toU
nder
stan
d an
d E
nhan
ce E
duca
tion
al E
ffec
tive
ness
” (p
p.27
4–2
92),
by
S.
L.
Ram
ey a
nd C
. T
. R
amey
, in
Con
tinu
ing
Issu
es i
n E
arly
Chi
ldho
od E
duca
tion
,2n
d ed
.,C
. See
feld
t an
d A
. Gal
per
(Eds
.), 1
997b
, Eng
lew
ood
Cli
ffs,
NJ:
Pre
ntic
e-H
all.
Rep
rint
ed w
ith
perm
issi
on.
= I
nput
s
= P
roce
sses
= O
utco
mes
Key
to M
odel
Proc
esse
sIn
puts
Bio
logy
and
Pri
or E
xper
ienc
ese.
g., I
nter
gene
ratio
nal I
nflu
ence
s,In
divi
dual
Bio
logy
, Pre
viou
s C
hild
and
Fam
ily E
xper
ienc
e
Fam
ily
Chi
ld
Soci
alSu
ppor
t
Mot
ivat
ion
and
Val
ues
Self
Con
cept
Safe
ty a
ndSe
curi
ty
Hea
lth a
ndN
utri
tion
Surv
ival
Res
ourc
es
Bas
icA
cade
mic
and
Wor
k Sk
ills
Com
m-
unic
aton
Com
mun
ity C
onte
xte.
g., L
ocat
ion/
Setti
ng, D
emog
raph
y/D
iver
sity
, In
fras
truc
ture
, Eco
nom
ic O
ppor
tuni
ty,
Polit
ical
/Soc
ial C
limat
e, N
eigh
borh
ood
Com
mun
ity R
esou
rces
Soci
al a
ndC
hild
Car
eSu
ppor
ts
Supp
orts
for
Lea
rnin
g
Scho
olSy
stem
sH
ealth
Serv
ices
Phys
ical
Supp
orts
Strengths and Needs• Child • Family • School • Health • Community
Out
com
es
Fam
ilySe
rvic
es
Hea
lthan
dN
utri
tion
Pare
nt
Invo
lvem
ent
• Sc
hool
s•
Gov
erni
ng
Boa
rd•
Com
mun
ity
Edu
catio
n•
Dev
elop
-
men
tally
A
ppro
pria
te
Prac
tices
• In
clus
ion
Con
tinuo
us C
ompr
ehen
sive
Hea
d St
art-
Lik
e Se
rvic
es
Tra
nsiti
on D
emon
stra
tion
Prog
ram
Im
plem
enta
tion
Strengths and Needs Assessment• Individual Family Plans • Individual Child Transition Plans
Goo
d pr
epar
atio
nof
chi
ldre
n, f
amili
es,
and
scho
ol f
orad
just
men
t to
elem
enta
rysc
hool
Com
preh
ensi
vesu
ppor
t for
child
ren,
fam
ilies
,an
d sc
hool
s du
ring
earl
y ye
ars
inel
emen
tary
scho
ol
Posi
tive
expe
ctat
ions
by c
hild
ren,
fam
ilies
,an
d sc
hool
for
fut
ure
oppo
rtun
ities
rel
ated
to le
arni
ng a
ndsc
hool
adj
ustm
ent
Succ
essf
ul T
rans
ition
sT
hrou
ghou
t Sch
oolin
g•
Chi
ldre
n ha
ve g
ood
feel
ings
abou
t sch
ool,
teac
hers
,
pare
nts
and
peer
s
• C
hild
ren
show
goo
d pr
ogre
ss
in
phy
sica
l, so
cial
, em
otio
nal,
an
d in
telle
ctua
l dev
elop
men
t
• Pa
rent
s an
d ke
y ad
ults
exp
ress
posi
tive
attit
udes
tow
ard
scho
ol
an
d ac
tivel
y pr
omot
e ch
ildre
n’s
le
arni
ng
• Te
ache
rs a
nd s
choo
l per
sonn
el
appr
ecia
te a
nd p
rovi
de p
rogr
ams
ad
apte
d to
chi
ldre
n’s
indi
vidu
al
deve
lopm
ent a
nd c
ultu
ral/
lin
guis
tic d
iver
sity
• M
utua
lly s
uppo
rtiv
e re
latio
n-
ship
s oc
cur
amon
g fa
mili
es,
sc
hool
per
sonn
el, s
ervi
ce
pr
ovid
ers,
com
mun
ities
Gro
wth
and
Cha
nge
in C
hild
ren
and
Fam
ilies
Gro
wth
and
Cha
nge
in S
choo
ls a
ndC
omm
uniti
es
Plan
ning
Impl
emen
tatio
nK
inde
rgar
ten
3rd
Gra
de
dam4_c21.qxd 12/20/05 9:39 AM Page 872

The National Head Start-Public School Early Childhood Transition Demonstration Project 873
addressed the eight functional domains (represented byeight boxes surrounding the child and family), endorsingtheir importance for the intervention and the research,and further specifying how these domains would be as-sessed at the beginning of the study (baseline) andthroughout the course of the study (4 years).
As Figure 21.2 displays in the Implementation Phase(identified along the x-axis at the bottom of the figure),each site was to conduct an individualized Strengthsand Needs Assessment for all participating childrenand families. This assessment was referred to as anIndividualized Transition Plan that addressed thestrengths and needs of the child and the family. This as-sessment was designed to maximize early identificationof any special supports and services for a successfultransition to school. As shown to the right of the oval onassessment, the major components of the TransitionDemonstration Program are identified in four majorareas: Family Services, Health and Nutrition, Educa-tion, and Parent Involvement. Collectively, these fourareas constitute the comprehensive Head Start-like ser-vices. The time period for implementation was from theplanning for kindergarten entry (ideally, in the yearchildren were served by traditional Head Start) througheach of the next 4 years in public school, with system-atic efforts to ensure continuity of planning and sup-ports from grade to grade.
For evaluation, the ABCD conceptualization wasused to identify what would be measured, starting withdescriptions of each local site in terms of the Commu-nity Context and Community Supports; comprehensiveassessment of the child and family’s health and educa-tion, including multiple measures designed to tap theconstructs in each of the eight functional domains; andongoing and annual documentation of program imple-mentation, combining program participation data fromthe local site with external multidisciplinary site visitsduring which additional data were collected and thelocal site program documentation was verified. In Fig-ure 21.2, the Transition Demonstration Program ser-vices are shown to contribute to three general areas(processes). That is, the intervention program was hy-pothesized to change children’s health and educationoutcomes through three primary pathways. The first wascreating “good preparation of children, families, andschools for the child’s adjustment to elementary school.”The Individualized Transition Plan and the process ofcreating local partnerships around the topic of positiveschool transitions were central features altering the
community- and family-specific context for schoolreadiness. The second pathway was “comprehensive sup-port for children, families, and schools during the earlyyears in elementary school.” This was hypothesized toresult from the many in-school supports and community-based activities for children and parents, increased pro-fessional development activities for educators, andmultiple parent involvement programs to facilitate chil-dren’s academic progress. Third, “positive expectationsby children, families, and schools for future opportuni-ties related to learning and school adjustment” was in-cluded as a specific pathway. Measures of this wereobtained by in-depth open-ended and structured inter-views with families, teachers, principals, and childrenthemselves.
This project recognized that in many communities,the poor performance of children in the past set thestage for low expectations and concomitant dismal pre-dictions of outcomes for children from low-income fam-ilies. An explicit component of the intervention was tochange these expectations for academic and life suc-cess, that is, to create an expectation that the historicalhealth disparities and educational inequities could besignificantly reduced or eliminated. Collectively, theprocesses of increasing preparation for school success,providing supports for health and education during theearly elementary school years, and increasing expecta-tions for positive outcomes among a large stakeholdergroup surrounding the child are the general pathways—each of which was measured by multiple indicatorsthroughout the study—conceptualized as producingpositive outcomes.
Finally, Figure 21.2 indicates the outcomes (the octagons in the far right column) specified for the Tran-sition Demonstration Project. These agreed-upon out-comes, building on an earlier shared vision and localcommunity partnerships and input to the national evalu-ation, transcend the typical academic indicators of testscores only, and reflect the fact that outcomes for alarge, intensive intervention or community reform effortshould correspond to ways that the stakeholders actuallythink about children and their well-being. Specifically,we note that some subjective measures are identified aslegitimate outcomes, such as “Children have going goodfeelings about school, teachers, parents, and peers”(what most people call “liking school” and “positiveschool attitudes”), as well as their parents and teachershaving positive attitudes and being actively engaged intheir children’s learning. Although outcomes such as
dam4_c21.qxd 12/20/05 9:39 AM Page 873

874 Children’s Health and Education
having “mutually supportive relationships among fami-lies, school personnel, service providers, and communi-ties” can be challenging for researchers to measure,these are important valid outcomes to target. Of course,children’s health and educational status are also mea-sured, but these did not constitute the sole indicators ofeffectiveness for this National Transition Demonstra-tion Program.
By using the ABCD conceptual framework, the prog-ress of the project and the extent to which goals were re-alized could be studied in a prospective way, assessingyear-by-year changes at the level of the child, the family,the school, the health and social service delivery sys-tem, and the community as a whole. More important, thesteps from Planning through Implementation could betracked, so that if intended outcomes did not occur, thesupportive processes could be carefully reviewed to con-sider likely explanations for differential benefits acrossand within the 31 sites.
Measurement of Inputs, Processes, and Outcomes
The ABCD framework facilitated the identification ofconstructs to be measured. Table 21.1 presents anoverview of the measures selected and links these to theABCD model. (For further details and references aboutmethodology, see S. L. Ramey et al., 2001.) Note: thisdata set is now in the public domain, with supportivedata dictionaries and summary variables available.
Selected Findings from the National TransitionDemonstration Study about Children’s Healthand Education
In this chapter, we chose findings about three topicsoften overlooked in conventional studies of children’shealth and education: children’s perceptions about theirschool experiences, the developmental trajectory of aca-demically gifted former Head Start children, and theways families protect children from injuries.
Children’s Feelings about School
Children’s feelings about school, as revealed during a Vygotskian-style dialogue, permitted children asyoung as 5 years of age to tell the child assessors howthey felt about things happening in school. The areasrated by children included how well they got along withtheir teacher and peers; how important they and theirparents (separate queries) thought it was to do well in
school; how much they liked school; how well theythought they were doing in academic areas; and howgood their teacher was at teaching them new things. The dialogue “What I Think of School” (Reid et al.,1990) has good psychometric properties and is sensitiveto individual differences. For example, S. L. Ramey,Lanzi, Phillips, and Ramey (1998) reported that by thespring of kindergarten, about 7% of former Head Startchildren were having multiple negative perceptions ofschool. Especially impressive was the finding that chil-dren’s negative early perceptions were highly predictiveof subsequent academic progress in reading and math, asmeasured by standardized assessments and teacher rat-ings, and that children’s feelings about school con-tributed significant information above and beyond themeasures of their kindergarten-level language, reading,math, and social skills. Children’s impressions of schoolfit within the outcome labeled Personal Constructs inthe ABCD conceptual model (Figure 21.1). We inter-preted this finding to support the recommendation thatchildren’s experiences warrant inclusion in almost allinvestigations of children’s school adjustment and theirmental and physical well-being. Also, this finding exem-plifies a practically useful result well suited for sharingwith educators and program staff. That is, in a collabo-rative style of program research and evaluation, infor-mation such as this can help inform subsequent changesin the intervention—perhaps to encourage the programs,teachers, and parents to consider children’s feelings asimportant early warning signs that are likely to precedeawareness by the adults that things are not going well.
High-Achieving Low-Income Children
Another interesting set of findings from this multisite,multidisciplinary longitudinal study concerns identifyinga subgroup of children with exceptionally positive devel-opment. Analysis sought to understand the supportive andprotective factors in their lives (Robinson, Lanzi, Wein-berg, Ramey, & Ramey, 2002; Robinson, Weinberg,Redden, Ramey, & Ramey, 1998). All too often, studiesgrounded in a commitment to eliminate the health and ed-ucational disparities concentrate disproportionately onthe negative outcomes, or the reduction in negative out-comes. In the process, the presence of highly accom-plished children and families is overlooked, and negativestereotypes are reinforced. Analyses such as these areimportant for both practical and theoretical reasons. Inthe Transition Demonstration Project, for example, thechildren who scored in the upper 3% of this former Head
dam4_c21.qxd 12/20/05 9:39 AM Page 874

875
Peabody Picture Vocabulary Test Communication X X X X X
Woodcock-Johnson:Reading AchievementMath Achievement Academic Skills
XX
XX
XX
XX
XX
What I Think of School Motivation and values, related to school and self-concept X X X X
Writing Sample Academic skills and communication X X
Getting to Know Your Family Motivation, expectations, values, and social support X
Family Background Interview (updatedannually)
Survival resources, health, security, basic skills, andcommunity context /resources X X X X X
Family Resource Scale Survival resources, security, and social support X X
Family Routines Questionnaire Family context X X
Primary Caregiver Health: Depression Screen Health and security X X X
Social Skills Rating System:Social SkillsProblem Behavior Basic skills
X X X XX
XX
Your Child’s Health and Safety Social and health services in the community context andsurvival resources X X
Social Skills Rating System:Social SkillsProblem BehaviorAcademic Competence Basic skills
XXX
XXX
XXX
XXX
School Survey of Early Childhood Programs(Part C: 1–9) School context X X X X
School Climate Survey School context X X X X
Neighborhood Scales School context X X X
Your Child’s Adjustment to School Self-concept, motivation /expectations/values (related toschool), social support , and basic skills X X X X
Family Involvement in Children’s Learning Demonstration program context and school programcontext X X
Child Health Questionnaire for Teachers Health X X X X
School Climate Survey School context X X X X
Parenting Dimensions Inventory Parent-child transactions and mediating processes X X X
FK SK SI S2 S3
TABLE 21.1 Data Collection Schedule for National Transition Development Project
Procedure Functional Domain(s) Addressed
Information from Family
Data Collection Period
Information from Teachers
(continued)
dam4_c21.qxd 12/20/05 9:39 AM Page 875

876 Children’s Health and Education
TABLE 21.1 Continued
School Climate Survey School context X X X X
School Survey of Early Childhood Programs(Part A: 1–6; Part B: 1–5) School context X X X X
Information from Existing Records
School Archival Records Search Basic skills and school program context X X X X
Information from Classroom Observation
Assessment Profile for Early ChildhoodPrograms
Classroom context X X X X
ADAPT (to measure use of developmentallyappropriate practices in the classroom)
Classroom contextX X X X
Procedure Functional Domain(s) Addressed FK SK S1 S2 S3
Information from Principals
Data Collection Period
Start sample on individually administered standardizedtests of vocabulary, reading, and math came from all eth-nic groups and many sites; these children also werehighly accomplished by national norms, not just projectnorms. In addition to their academic achievements, thesechildren were thriving socially and emotionally as well,according to both teacher and parent ratings (although,interestingly, parents did not rate their children as morecooperative). The social ecological factors contributingto the positive outcomes for these children included somepredictable, and some unexpected, factors. For instance,parents reported significantly fewer stressors in theirlives, but they did not report significantly more familystrengths. Residential stability, somewhat higher fatherinvolvement, fewer single-parent households, and higherrates of parent high school graduation were predictablyassociated with higher-achieving children. Unexpectedly,however, rates of maternal depression did not differ forthe highest-achieving versus remaining children (25%versus 23%), and parental Nurturance and Consistency(factor scores from the Parenting Dimensions Inventory;Slater & Power, 1987) were comparable for these groups.What was important were the dimensions of parent Re-sponsiveness and Nonrestrictiveness, such that childrenwhose parents endorsed less restrictive parenting prac-tices and were more responsive to individual child needshad children with higher academic achievement. Further,teachers rated parents of the highest-achieving formerHead Start students as more strongly encouraging of theirchildren to succeed in school, despite the fact that the
parents did not so describe themselves. Parents of thehighest-achieving children did not report discussingschool with their children, being in touch with theteacher, or participating in planned parent activities atschool more than other parents, but they did report volun-teering more often at their child’s school.
Findings such as these bring into focus the impor-tance of differentiating subgroups or clusters of chil-dren and families within a larger at-risk population.Indeed, in this study, we identified and verified sixmajor family types, based on the strengths and needs as-sessments, living in poverty (e.g., C. T. Ramey, Ramey,& Lanzi, 1998). This type of differentiation permitsstudy of the likelihood of differential courses of devel-opment and the importance of different processes tosupport children having more or less positive outcomes.
Unintentional Child Injuries
Schwebel, Brezausek, Ramey, and Ramey (2004) ex-plored children’s unintentional injury risk, the leadingcause of deaths among children 1 to 18 years (NationalSafety Council, 2001). At the time we conducted theseanalyses, available data supported the view that chil-dren’s impulsive, hyperactive behavior patterns servedto increase risk of injury and that poor parenting mightalso independently increase injury risk in the same sam-ples. Remarkably, no analyses had considered whetheractive, positive parenting (supportive processes) couldreduce injury among children at risk because of difficultbehavior patterns. Using a logistic regression approach
dam4_c21.qxd 12/20/05 9:39 AM Page 876

Principles of Effective Intervention Supported by Longitudinal Research on Children’s Health and Education 877
that considered child, parenting, and contextual factorsand their possible interactions, this data set affirmedthat children’s hyperactivity was a strong predictor ofinjuries (odds ratio = 28.4). The ABCD conceptualiza-tion, however, contributed to the important additionalfinding that parents’ report of the adequacy of theirtemporal resources—that is, time available to parentsfor desired activities, including time to be with theirchildren—was a significant protective factor for thisincreased-risk group of children. Thus, the family envi-ronment and parental behavior emerged as key promo-tive processes. (For further findings about the NationalTransition Demonstration Project, see S. L. Ramey,Ramey, & Lanzi, 2004.)
Collectively, these findings provide a window onways to study developmental pathways to alternativehealth and education outcomes and to consider how as-pects of the child’s context, initial status of the child andfamily, and supportive as well as harmful processes canalter the course of development and children’s outcomes.
PRINCIPLES OF EFFECTIVEINTERVENTION SUPPORTED BYLONGITUDINAL RESEARCH ONCHILDREN’S HEALTH AND EDUCATION
For many decades, the single most pressing question inearly childhood education was simply “Do early educa-tion and health interventions work?” There was robustskepticism that early educational interventions couldalter the cumulative negative toll that poverty and otherrisk circumstances take on the development of youngchildren. But by the mid-1980s, a professional consensuswas reached (cf. Guralnick & Bennett, 1987) that earlyeducational interventions can—under certain condi-tions—produce meaningful benefits, as reflected in theacademic achievement and social progress of young chil-dren. Just as important, when early interventions fail toproduce intended benefits, the likely reasons are impor-tant to understand for practice and theory. Given thecross-study consistencies in findings, we summarizefindings about early educational interventions in termsof five major scientific principles (C. T. Ramey &Ramey, 1998a; S. L. Ramey & Ramey, 1992). We postu-late that these principles are likely to hold true forhealth interventions, although there is scant scientificsupport from randomized controlled trials designed toimprove the physical health of at-risk children or to pre-
vent prevalent childhood disorders such as asthma, obe-sity, depression, and chronic dental disease. We have en-deavored to incorporate health examples, however, asmuch as possible, including several dramatic publichealth interventions that have altered the CommunityContext and Community Supports directly. These fivemajor principles are (1) the dosage principle, (2) thetiming principle, (3) the direct receipt of services prin-ciple, (4) the differential benefits principle, and (5) thecontinuity of supports principle.
The Principle of Dosage
Programs that provide higher amounts of intervention(i.e., full dosage) produce greater benefits in health andeducation outcomes. This principle of dosage or inter-vention intensity has considerable scientific support, de-rived from cross-study comparisons of magnitude ofbenefits from multipronged and educational interven-tions that varied in their dosage, as well as some experi-mental studies that directly tested different dosagelevels within the same study, and from post hoc analysesthat analyzed rates of participation using sophisticatedanalytical techniques. Dosage is indexed in differentways, for different types of interventions; we cautionthat for medical interventions, the intensity principlerefers to administering the full dosage, recognizing thatoverdosage could be dangerous.
For educational interventions in the first 8 years oflife, dosage can be indexed by variables such as numberof hours per day, days per week, and weeks per yearthat children receive the educational intervention. Anideal measure—which has never been calculated, to ourknowledge, in educational interventions—would be theactual amount of instructional and learning time childrenhave when they attend, multiplied by the child’s atten-dance. Theoretically, the reason that more intensive pro-grams produce significantly larger positive effects thando less intensive programs is straightforward: Childrenare engaged in more learning, which in turn supportstheir continued growth and development in the domainsin which the learning occurs. For health, the greater theamount of time spent in health promotion activities andthe greater the compliance with recommended healthcare treatments (representing a complex interplay ofavailability, accessibility, and acceptability of appropri-ate services), the healthier the child should be.
Many early interventions do not significantly im-prove children’s intellectual or academic performance
dam4_c21.qxd 12/20/05 9:39 AM Page 877

878 Children’s Health and Education
(see S. L. Ramey & Ramey, 2000, for discussion of somereasons why these likely fail). A key characteristic ofmany of these unsuccessful interventions is that theywere not very intensive. For instance, none of the 16 ran-domized trials of early interventions for young childrenwith disabilities or delays evaluated by the Utah StateEarly Intervention Research Institute (White, 1991)provided full-day 5-day/week programs, and none ofthese programs produced any measurable benefits forchildren in terms of their competencies. Similarly, Scarrand McCartney (1988) provided intervention only onceper week to economically impoverished families inBermuda in an effort to replicate the findings of Leven-stein’s (1970) Verbal Interaction Project. They alsofailed to detect any positive cognitive effects.
In marked contrast, two RCTs conducted in NorthCarolina using the same educational curriculum, theAbecedarian Project and Project CARE, producedmultiple significant benefits to participants in this high-dosage educational intervention. The Abecedarian Proj-ect and Project CARE both provided educationalsupports to children within a full-day, 5 days a week, 50weeks per year program for 5 consecutive years, using astructured and individualized curriculum delivered in ahigh-quality, university-based child development centerthat was continuously monitored and supported for qual-ity of curriculum implementation (C. T. Ramey &Ramey, 2004a, 2004b, 2004c). To our knowledge, thesetwo programs are among the most intensive (highdosage) that have been subjected to rigorous experimen-tal study, and the principle of dosage may account for alarge portion of the increased magnitude of benefit de-tected at ages 8, 12, 15, and 21 years. We particularlynote the benefits for language and literacy, as demon-strated in significant gains at every age on every lan-guage measure and all reading assessments (C. T. Rameyet al., 2000; C. T. Ramey & Ramey, 2004c). Other edu-cationally important outcomes include markedly lowerrates of placement in special education, reduced from48% in the comparison group to 12% in the educationalintervention group (close to the national average of11%), and reduced rates of grade repetition, from 56%in the control group to 30% in the educational group.
The Milwaukee Project was an RCT that producedlarge, immediate benefits in intelligence and language(Garber, 1988) and provided a high-dosage, daily earlyeducational intervention from birth through the transi-tion to school, with a university child development pro-gram offered daily (see review by S. L. Ramey & Ramey,
2000). However, long-term benefits were not sustained tothe same degree as in the North Carolina projects, per-haps because of the influence of the principle of continu-ity of supports and the differences in the enrollmentcriteria across these projects (i.e., the North Carolinaprojects enrolled on a combination of family risk vari-ables; the Milwaukee Project enrolled only children bornto mothers with mental retardation).
Two studies provide experimental evidence that pro-gram intensity matters: An early intervention homevisit program (Powell & Grantham-McGregor, 1989)that systematically tested different levels of intensitydiscovered significant cognitive benefits at a dosagelevel of three visits per week, whereas fewer visits perweek did not produce any significant gains, and theBrookline Early Education Project (Hauser-Cram,Pierson, Walker, & Tivnan, 1991) reported that onlythe most intensive services were sufficient to benefitchildren from less well-educated families, whereas thelowest and intermediate intensities had no measurableconsequences.
The eight-site Infant Health and DevelopmentProgram RCT systematically investigated program in-tensity effects at the level of the individual child’sparticipation. Originally, C. T. Ramey et al. (1992) re-ported that the intensity of educational interventioneach child and family received related significantly tocognitive outcomes at age 3. Dosage was a sum of threeprogram components: total days the child attended thechild development center between 12 and 36 months;number of home visits from birth to age 3; and numberof monthly educational meetings the parents attended.This “participation index” demonstrated a strong, linearrelationship to the child’s intellectual and behavioral de-velopment at 36 months, even after controlling for vari-ables that might have influenced individual rates ofparticipation (such as maternal education, maternal ver-bal competence, family income, child health status, andethnicity). When considering the efficacy of this 3-year,multipronged educational intervention to prevent mentalretardation (IQ less than 70 points) at age 3, the resultsshowed that children in the highest participation grouphad nearly a nine-fold reduction in the percentage oflow-birthweight children who were mentally retarded(under 2%), compared with control children who re-ceived only high-quality pediatric follow-up services(about 18%). Later, Blair, Ramey, and Hardin (1995)demonstrated that year-by-year participation rates pro-duced significant and independent effects on the course
dam4_c21.qxd 12/20/05 9:39 AM Page 878

Principles of Effective Intervention Supported by Longitudinal Research on Children’s Health and Education 879
of the child’s measured cognitive competence at 12, 24,and 36 months of age.
Hill, Brooks-Gunn, and Waldfogel (2003) extendedthese intensity analyses to answer the question “Dolonger-term effects, at ages 5 and 8, relate to participa-tion rates?” When the children were 3, 5, and 8 years ofage, multiple assessments of language and cognition werecompleted, with the 8-year battery including the fullWechsler Intelligence Scale for Children (WISC; Verbal,Performance, and Full-Scale IQ scores), the Woodcock-Johnson Reading and Math assessments, and the PeabodyPicture Vocabulary Test-Revised (PPVT-R). On 12 majoroutcome measures across 3 age periods, all measuresshowed higher performance for children in two higher-participation groups (attending more than 350 days andattending more than 400 days in the child developmentcenter) relative to the randomly assigned follow-upgroup, which received pediatric and social services, butnot the educational component of this multipronged earlyintervention. The first set of analyses confirmed thatchildren who participated at higher rates differed signifi-cantly from the comparison group, with site-specific dif-ferences in which variables (e.g., maternal ethnicity,maternal education, maternal use of drugs, and prenatalcare) correlated with amounts of participation. Accord-ingly, this team applied a sophisticated set of data-analytic techniques that are well-known in medicalRCTs, involving an adaptation of a propensity scorematching procedure coupled with logistic regression toreduce the influence of the natural selection bias whenevaluating treatment effects. The results yielded com-pelling support for the dosage principle, demonstratingdifferences between matched high-dosage and controlchildren, and between higher- and lower-dosage childrenwithin the treatment group. The magnitude of these dif-ferences is impressive at all 3 ages analyzed, and extendsto the reading and math scores at age 8, with sustainedbenefits of the early educational intervention correspon-ding to gains of 6.1 to 11.1 points higher (depending onthe definition used for high dosage) on the Woodcock-Johnson, as well as sustained (although slightly reduced)benefits at ages 5 and 8 for PPVT (4.1 to 6.6 points at age8) and WISC IQ scores (6.5 to 8.4 points at age 8).
The Principle of Timing
Generally, when interventions begin earlier and con-tinue longer, they produce larger and longer-lasting benefits to the participants than do those that begin
much later and do not last as long. The age when chil-dren enter early educational interventions ranges frombirth through 8 years of age. Typically, children fromeconomically disadvantaged families become eligiblefor early educational interventions (e.g., Head Start,public school pre-K for at-risk children) in their homecommunities beginning at 4 years of age, and sometimesat 3 years of age. Many of the well-cited early educa-tional interventions, however, began when children wereyoung infants, such as the Abecedarian Project (C. T.Ramey, Bryant, Campbell, Sparling, & Wasik, 1988;C. T. Ramey, Yeates, & Short, 1984), the BrooklineEarly Education Project (Hauser-Kram et al., 1991), theMilwaukee Project (Garber, 1988), Project CARE(Wasik et al., 1990), and the Infant Health and Develop-ment Program (1990). Two noteworthy exceptions, how-ever, are the Perry Preschool Project, conducted inYpsilanti, Michigan (Schweinhart & Weikart, 1983),and the Early Training Project (Gray, Ramsey, & Klaus,1982), which began when children were 3 years of age.An important difference in these two interventions thatbegan later in life and did produce significant benefits isthat the children were documented to be significantlydelayed in their cognitive development at age 3, whereasthe other studies that enrolled children earlier sought toprevent intellectual decline linked to early and contin-ued impoverished language and learning environments.
The principle of timing has always been one of highinterest and is associated with vigorous debate. Con-cerning neurobiology and education outcomes, the stun-ning technology advances to document brain growth anddevelopment, coupled with research on early brain de-velopment (primarily experimental animal research)and how experiences shape brain activities lend support,in a general way, to the principle that earlier andmore sustained educational interventions are especiallypromising to maximize benefits to children. Even thecarefully controlled animal experiments on early expe-rience, which support the general principle of timing, donot refute the possibility that educational interventionsbegun at later ages can produce measurable gains (S. L.Ramey & Sackett, 2000). One of the most consistentlycited areas that lend support to the principle of timingcomes from the observational research of Kuhl, Tsao,and Liuh (2003) concerning acquisition of speech andlanguage perception, demonstrating that an infant’s ex-posure (naturally) to his or her first language results inthe loss of a generalized discrimination ability thatexisted at earlier ages. This reflects development (see
dam4_c21.qxd 12/20/05 9:39 AM Page 879

880 Children’s Health and Education
earlier definition) in which there is increasing selectivedifferentiation and hierarchical integration, that is hy-pothesized to facilitate (and to reflect) more efficient,higher-order functioning. When young infants are notexposed to certain sensory-perceptual experiences veryearly in life, they seem to lose their initial capacity(such as the universal ability of young babies to recog-nize phonemes in all languages, later narrowing to rec-ognize primarily phonemes in their native language).
Just as we cautioned earlier regarding possible nega-tive effects of overdosage, we recognize that certaintypes of interventions may be infeasible, ineffective, oreven iatrogenic (producing unintended negative conse-quences) if provided too early. There are some historicalexamples of this, often given in textbooks, such as astudy that trained babies to walk earlier than usual bypracticing the walking reflex daily, and efforts to teachcomplex motor skills to nursery school children. Bothstudies found short-term changes, but these seemingbenefits were washed out when the age-typical displayof these motor skills occurred for the control (un-treated) children.
The Abecedarian Project involved a two-phase educa-tional intervention, with 50% of the children whoreceived 5 consecutive years of early educational inter-vention and 50% in the control group (receiving nutri-tional, pediatric, and social services only) who wererandomly selected to participate in an elementaryschool Home-School Resource Program for 3 consecu-tive years. This partially tested the issue of timing, of-fering extra educational supports during the school year(provided by individualized assistance to children andtheir families with schoolwork and school-family com-munication) and a summer educational camp that soughtto increase children’s learning opportunities fromkindergarten through entry into third grade. The resultsdemonstrate two clear sets of findings. First, the ele-mentary school support program (i.e., the later onset ofintervention) did yield measurable benefits to partici-pants, as indexed by higher scores on standardized as-sessments of reading and math achievement at age 8.However, there were not comparable gains on generaltests of intelligence or language, compared to childrenwho received the preschool early education interven-tion. Second, the magnitude of benefits, even for thereading and math achievement scores, was smaller thanfor children who received the earlier-onset education in-tervention (see C. T. Ramey et al., 2000). This study isnot germane, however, in helping to resolve the vital
question about differential timing benefits during thepreschool years. Further, this study tested a reasonablywell-designed and replicable public school enhancementprogram, but did not seek to directly control the overallclassroom curriculum and instruction and thus is not asimple and pure test of timing effects alone.
In summary, the principle of timing has modest sup-port from human studies, but further research is neededfor conclusive evidence about its importance for differ-ent aspects of language, literacy, and other academiccompetencies. For health interventions, examples amongdeaf children such as timing of cochlear implants andage of teaching infants sign language confirm thegreater malleability or recoverability of the brain whensuch corrective procedures are implemented. In general,early detection and treatment are so widely accepted aspositive in health care that they rarely are studied sys-tematically. There are no compelling data, at this time,to support the notion of an absolute critical period, suchthat educational intervention or health supports pro-vided after a certain age cannot be beneficial at all;rather, this is a principle of relative timing effects.
The Principle of Direct Receipt of Services
This principle affirms that early educational and healthinterventions that directly alter children’s daily healthand education produce larger positive and longer-lastingresults than do those interventions that rely primarily onindirect or pass-through routes to change competencies.
Early education and health interventions have beenpresented in many different forms, including those thatare based in child development centers with trainedteaching and health staff, those that are home-based andseek to change parents’ health behavior and provide en-vironmental enrichments (books, learning games, educa-tional videos), and those that combine center- andhome-based components. These different types of earlyeducational and health interventions may be divided intotwo major categories: those that rely primarily on directprovision of academic and health instruction to childrenand those that seek indirect means of enhancing childlearning, such as seeking to change the parents’ behaviorand, through that mechanism, to alter the child’s healthand education.
The empirical findings regarding the differential ef-fects of these two quite different strategies are clear:The indirect interventions that seek to change interme-diary factors are not as powerful in changing children’s
dam4_c21.qxd 12/20/05 9:39 AM Page 880

Principles of Effective Intervention Supported by Longitudinal Research on Children’s Health and Education 881
language, reading, intellectual, or health performance(Lewis, 1984; Madden, Levenstein, & Levenstein, 1976;C. T. Ramey, Ramey, Gaines, & Blair, 1995; Scarr &McCartney, 1988; Wasik et al., 1990). This generaliza-tion holds true for economically disadvantaged children,seriously biologically disadvantaged children, and high-risk children with both environmental and individualrisk conditions.
C.T. Ramey, Bryant, Sparling, and Wasik (1985) con-ducted the first systematic and experimental study withdirect provision of instruction versus intermediaryforms of early educational intervention. In an RCT,high-risk children were randomly assigned just afterbirth to receive one of three interventions: (1) the daily,highly intense child development center program, identi-cal to that provided to children in the Abecedarian Proj-ect, coupled with the home visiting program; (2) a homevisiting (intermediary) program that lasted for 5 years,used the same educational curriculum as the center-based intervention, and sought to have parents deliverthe intervention; and (3) a comparison group that re-ceived enhanced nutritional, pediatric, and social ser-vices only (both intervention groups also received thesehealth and social support services). An importantachievement in this study, the longest-lasting home visit-ing program we know of, is that participants in all threegroups remained highly engaged in the program and theassessments. The home visiting was planned to beweekly during the first 2 years of life and then everyother week for the next 3 years. Further, the home visi-tors received ongoing supervision and continuing sup-port throughout the 5 years and used a structured butadaptable curriculum, and both the home visitors andthe families reported that they perceived the home visit-ing program to very positive. Despite the enthusiasm forthe effort to change parents, who in turn could transmitincreased learning opportunities to their children, theoutcome data demonstrated no measurable gains for thechildren in the home visiting program compared to the control children, and both of these groups fared sig-nificantly worse than the group that received the daily,year-round center-based educational curriculum plushome visiting. Post hoc analyses indicated that magni-tude of benefits associated with the children who re-ceived direct language and academic instruction (in thecenter) plus the 5 years of home visiting was almostidentical to that reported for the Abecedarian Projectparticipants, who did not receive the same intensivehome visiting educational component. On a promising
note, from another home visiting program, Powell andGrantham-McGregor (1989) indicated that three homevisits per week—but not less—produced significantchild improvement through the intermediary or indirectintervention approach.
Just recently, Olds et al. (2004) reported positive butmodest education and health benefits from a nurse homevisiting program detected 2 years after the programended but not during the program. These results wereparticularly noteworthy in the areas of receptive lan-guage and intelligence. These high-risk children werealso more likely to have been enrolled in formal out-of-home care, so it is not clear whether a direct or indirectroute of influences or a combination best accounts forthe results.
There clearly is popular appeal to the idea that in-creasing the skills and knowledge of young children’sfirst teachers—their parents—will be beneficial, be-cause parents are children’s natural support system and,typically, care deeply about their children’s well-being.Also, most programs hope that changing parents and im-proving the home environment will have spillover effectsto the next children born into these families and willhelp to increase the local community’s competence inproviding the right types of education and health experi-ences, at the right times, for many other young children.Increasingly, many of these parent-focused educationaland health interventions consider that some parentsthemselves lacked good educational and health opportu-nities when they were growing up, and some parentslacked positive parenting models in their own lives. Ac-cordingly, the curricula used for the parenting and homevisiting programs often address the parent’s own devel-opmental needs and crucial aspects of culture and localcommunity, along with “how to parent” issues.
What are the likely reasons that center-based pro-grams with more traditional types of language enrich-ment, health care, and teacher-provided instructionrelating to academic skills yield positive results in termsof academic achievement and cognition, whereas the in-direct or intermediary programs do not? We hypothesizethat at least four factors may be contributing to this pat-tern of results. One is that most home visiting programsare not equal in intensity or dosage to the center-basedprograms. Another is that the natural language and aca-demic skills of some parents in at-risk families may not be equal to those of teachers or caregivers in the center-based programs, even when parents are encour-aged to provide more language and academic learning
dam4_c21.qxd 12/20/05 9:39 AM Page 881

882 Children’s Health and Education
experiences to their preschool children. Thus, the chil-dren in the two groups would not receive similar levelsof exposure to a rich language environment on an every-day basis (cf. Hart & Risley, 1995; Huttenlocher, 1990).A third reason is that parents who respond positively tothe home visiting still may not spend enough time withtheir children for the children to have the full benefit oftheir parents’ increased skills. For many parents, theirchildren may be in the care of others for extended peri-ods during the day or night, and these other caregiversmay not be meeting the needs of these at-risk children(National Institute of Child Health and Human Devel-opment [NICHD] Consortium for the Study of EarlyChild Care, 2005). Fourth and finally, the rate at whichparticipating parents acquire and then implement theirenhanced parenting and instructional skills may not berapid enough to achieve the intended benefits for theirchildren. This harkens back to the principles of bothdosage and timing. We note that home visiting programsmay serve other valuable purposes, such as preventingchild neglect and abuse and increasing children’s healthand safety, as demonstrated in research projects suchthose by as Olds and colleagues (2004).
For reasons we do not fully understand, the earlychildhood community has become polarized around is-sues that concern direct or explicit teaching of certainskills to young children. It appears common knowledgethat babies are born without knowing any specific wordsor ideas, and that skills related to reading, writing, andmath require direct exposure; that is, their advancementcannot occur without some introduction, scaffolding,modeling or demonstration, and practice and feedback.We believe that some practitioners in early childhoodprograms mistakenly tried to enact kindergarten-orfirst-grade-level instruction for much younger children,and adopted ineffective methods of repetitive drill, re-stricted young children’s spontaneous play and explo-ration, and tried to force very young children to attendand behave in ways that were counterproductive. Ac-cordingly, the anti-instruction movement could beviewed as a backlash to such inappropriate applicationsof early educational interventions. An alternative expla-nation is that some of the competent caregivers foryoung children, particularly low-income and minoritychildren, in the United States have low levels of formaleducation and lack formal teaching credentials. Theremay be a fear that all of these individuals will be ex-cluded from the future of child care and early educationand judged to be incompetent simply because they can-
not articulate precisely how they instruct children andhelp to prepare them for school. Although there aremany published studies documenting a general relation-ship between an adult’s level of education, languageskills, and intelligence and the adult’s skills in promot-ing children’s cognitive and language development (cf.NICHD Consortium for the Study of Early Child Care,2005), there are many notable exceptions to the general-ization. From our own professional experience, we haveobserved highly competent teachers of young childrenwho come from all types of educational backgroundsand all types of linguistic and cultural backgrounds. Ad-vanced degrees in early childhood education are not aguarantee of high-quality instruction occurring on a re-sponsive and regular basis; neither does the lack of acollege degree prohibit an adult from providing high-quality language and academic learning opportunities.
Currently, the Institute of Educational Sciences iscoordinating an effort to evaluate RCTs that test thebenefits of different published preschool curricula,mostly for 4-year-olds. This effort is designed to yieldmuch needed information about “what works” in pre-Ksettings. There are, however, already recognized limitsthat have surfaced in this new research endeavor, such asdifferences across sites regarding the dosage of the in-tervention (hours per day, weeks per year), the degree ofrisk in the children participating, the quality of and con-trol over curriculum implementation, and the levels ofparticipation from the children and families. What isadmirable about this research initiative is that both edu-cational science and curriculum development are beingadvanced, and the practical importance of this type ofscientific inquiry has become paramount by creating anational network of projects concerned with children’slanguage and literacy outcomes. Content analysis of ex-isting early educational interventions that have alreadyproduced large and lasting benefits through RCTs wouldbe a worthwhile endeavor, as well as efforts to measurethe actual classroom instruction at levels that corre-spond to the particular types of learning and languageexperiences hypothesized to be the most essential foryoung children’s learning (e.g., C. T. Ramey & Ramey,1999; S. L. Ramey & Ramey, 1998).
The Principle of Differential Benefits
This principle asserts that some children show greaterbenefits from participation in early educational andhealth interventions than do other children. These indi-
dam4_c21.qxd 12/20/05 9:39 AM Page 882

Principles of Effective Intervention Supported by Longitudinal Research on Children’s Health and Education 883
Figure 21.3 Differential effects of the Infant Health andDevelopment Program on age 3 IQ outcomes (Stanford-Binet)as a function of maternal educational status.
70
75
80
85
90
95
100
105
110
SomeHigh School
104
85
104
93
110 110
95
105
High SchoolGraduate
SomeCollege
CollegeGraduate
Comparison(Pediatric care and family social work)
IHDP Intervention(Home Visiting andChild Education Programplus pediatric care and family social services)
vidual differences appear to relate to aspects of the chil-dren’s initial risk condition and the degree to which theprogram meets the child’s needs or services to preventthe harmful consequences of those risk conditions overtime (e.g., by providing sufficient amounts of direct pos-itive learning experiences that otherwise would not havebeen present).
A fundamental assumption in the fields of educationand social ecology is that of person × environment (readas “person by environment”) or person × treatmenteffects. This assumption is that different individuals re-spond differently to the same program, and correspond-ingly, different programs may be needed to produce thesame outcome for different participants. These ideashave long prevailed in the clinical and educational liter-ature, but only recently have they been explored system-atically in the early intervention field.
In providing broad-based early intervention for pre-mature, low-birthweight infants, the Infant Health andDevelopment Program (1990) reported that children atgreater presumed biological risk, as indexed by theirlower birthweight ( less than 2,000 gm), at age 3 yearsdid not initially benefit as much from the program as didchildren at lesser presumed risk (with birthweight be-tween 2,000 and 2,499 gm), even though both groupsshowed significant gains. In a longer-term follow-up ofthese children at 5 and 8 years of age, Hill et al. (2003)reported large and significant risk × intervention ef-fects, such that the heavier low-birthweight childrenshowed IQ point benefits of about 14 points, and lighterbabies had effects of about 8 points, compared to theirappropriate-birthweight matched controls who did notreceive the educational component of the intervention.
Another study focused on early educational interven-tion for children with disabilities and considered twoinfluences simultaneously: the degree of the child’s im-pairment and the form of educational intervention pro-vided. Cole, Dale, Mills, and Jenkins (1991) found anaptitude × treatment effect in a randomized design com-paring Feuerstein’s “mediated learning” techniques andmore traditional direct instruction. Contrary to conven-tional wisdom, students who performed relatively better(as measured on the pretest battery of cognitive, lan-guage, and motor tests) gained more from direct instruc-tion, whereas students who performed worse showedgreater benefits from the mediated learning treatment.
From the Abecedarian Project, Martin, Ramey, andRamey (1990) discovered that the children who showedthe greatest relative gains (i.e., compared to controls)
were those whose mothers were the most intellectuallylimited (i.e., maternal IQ scores below 70; in fact, allexperimental children whose mother was mentally re-tarded performed at least 20 points higher and averaged32 points higher than did their own mother; Landesman& Ramey, 1989). These dramatic findings are compara-ble to the large benefits reported in the Milwaukee Proj-ect, which enrolled only economically disadvantagedmothers with IQs below 75 (Garber, 1988).
Some of the programs that have failed to detect anysignificant overall benefits may have enrolled a highlyheterogeneous group of children, some of whom wereat very low or no risk for poor educational outcomes.This could serve to lessen the power to detect real inter-vention effects if, in fact, only the high-risk childrenshowed benefits. As an example, analyses conducted onchildren participating in the Infant Health and Develop-ment Program showed significantly different levels ofbenefit based on the educational level of the children’smother. As Figure 21.3 shows, the degree of benefits,as indexed by children’s IQ scores on the Stanford-Binetat age 3, displayed a highly orderly relationship tomother’s education. The gains were the greatest (com-paring treated and control children) for those childrenwhose mother had less than a high school education, fol-lowed by those whose mother earned a high school
dam4_c21.qxd 12/20/05 9:39 AM Page 883

884 Children’s Health and Education
degree or GED, and then those whose mother had somecollege education. Interestingly, there were neither anybenefits nor any harm related to participating in thiseducational intervention for children whose motherad earned a 4-year college degree or higher (seeS. L. Ramey & Ramey, 2000). These findings of differ-ential benefits are consistent with an interpretation thatthese educational interventions supplement children’sexperiences at home in ways that are essential for the de-velopment of average (or above-average) intelligence;accordingly, for children whose cognitive and linguisticdevelopment is strongly supported by their family andother natural environments, additional educational in-terventions are not needed to prevent subaverage perfor-mance. We also note that in this study, the controlchildren, like those in all of the RCTs we have reviewed,were never prevented from participating in other pro-grams, and many of the college-educated parents in theInfant Health and Development Program sought, ontheir own, additional help and information to supportthe early development of their premature and low-birthweight infants.
The Principle of Continuity of Supports
This principle states that over time, the initial positiveeffects of early interventions will diminish if there areinadequate later supports to maintain children’s positiveoutcomes. This has been demonstrated mostly in the ed-ucational realm, but logically is just as important forchildren’s health. The reason postintervention programscontinue to matter is that children continue to learn athigh rates, with educational and health progress that de-pends not only on a child’s entry-level skills or healthstatus but his or her continued acquisition of the cogni-tive, language, and academic skills—complemented byappropriate physical, social, and emotional skills—tohave a positive transition to school (S. L. Ramey, Ramey,& Lanzi, 2004).
For many early intervention programs for at-risk chil-dren, long-lasting and substantial effects on schoolachievement, grade retention, and special educationplacement have been repeated. In some, but not all, stud-ies (e.g., Garber, 1988), the long-term effects of earlyeducational intervention on IQ scores lessen over time.Two important issues are relevant. First, it is not suffi-cient for disadvantaged children merely to maintain theadvantages from effective early educational interven-tions. Rather, children must continue to develop at nor-mative rates in multiple domains if they are to succeed
in school settings. Second, no currently influential de-velopmental theory is premised on the assumption thatpositive early learning experiences are sufficient bythemselves to ensure that children will perform wellthroughout their lives. A poor school environment, sub-optimal health, a seriously disrupted home environment,and many other conditions influence the behavior ofchildren at all ages. Thus, longitudinal inquiry about thelong-term effects of early intervention must take intoconsideration children’s subsequent environments andexperiences (i.e., after early intervention ceases).
As described earlier, only one RCT early interven-tion study, the Abecedarian Project, has extended earlyintervention into the elementary school years to evaluatethe importance of additional systematic supports duringthe transition to school. As Figure 21.4 shows, at 8 yearsof age, children who had received continuous educa-tional intervention for the first 8 years performed thebest of any group in reading and mathematics, followednext by those who received early intervention for 5years, followed by those who received the elementaryschool treatment only (Horacek, Ramey, Campbell,Hoffman, & Fletcher, 1987). Longitudinal analysis ofIQ scores revealed effects only for the early interven-tion groups; that is, the supplemental program fromkindergarten through age 8 did not result in higher IQscores (C.T. Ramey & Campbell, 1994). Later, at age12, children who had received the early interventioncontinued to show benefits in terms of both academicachievement and IQ scores and a reduction of nearly50% in the rate of repetition of at least one grade in theelementary school years. Overall, however, the group ofchildren who performed best across all measures werethose who had both the preschool and school-age educa-tional interventions.
Currie and Thomas (1995) have conducted importantanalyses of the long-term educational progress of for-mer Head Start children and demonstrated that thosewho go to average or above-average schools continue tokeep up with their age or grade peers, whereas those inthe very lowest performing schools show a decline (rela-tive to their school entry level). Tragically, 50 yearsafter Brown v. Board of Education, it remains true thatAfrican American low-income children disproportion-ately attend very poor quality schools, at rates far higherthan for other ethnic groups even when family income isbelow the poverty line.
Recently, Barnett (2004) has written an excellent andintegrative review that confronts the “myth of fade-out.”Although it is true that IQ scores per se show dimin-
dam4_c21.qxd 12/20/05 9:39 AM Page 884

Key Features of Collaborative and Community Participatory Research 885
Figure 21.4 The Abecedarian Project: selected health and education outcomes from infancy through young adulthood.
80
85
90
95
100
8 Years
94
85
91
85
93
8889
94
12 Years 15 Years 21 Years
Grade Retention Special Education0
10
20
30
40
50
60
30
56
12
48
0
10
20
30
40
50
60
Teen Parent
26
45
39
55
36
14
39
18
Smoking Marijuana Use Attending4-Year College
Comparison Group(Nutrition supplements,regular pediatric care, and family social services)
Abecedarian Treatment(5 years of preschool education plus nutrition supplements, regular pediatric care and family social services)
0
10
20
30
40
50
60
70
80
90
100
6 Months
10093
100
78
95
4549
95
18 Months 36 Months 48 Months
Young Adult (Age 21 Years) Healthy Lifestyle IndicatorsRates of Grade Retention/Repetition andSpecial Education Placement by Age 15
Percent in Normal IQ Range (>84) during Preschool Years;Bayley Scales of Infant Development at 6 and 18 Months;
Stanford-Binet at 36 and 48 Months; (National M = 100, S.D. = 15)Mean Reading Achievement Scores
(National M = 100, S.D. = 15) on Woodcock-Johnson
ished group difference over time, achievements in read-ing, language, math, and overall school adjustment as in-dexed by grade retention and special educationplacement show long-lasting benefits. When these sus-tained effects do not appear, one of the contributing fac-tors—in addition to the principles already detailed inthis chapter—may well be the quality and intensity ofthe educational programs that follow the early educa-tional intervention. The opportunity to conduct morerigorous post hoc analyses about the schools that chil-dren attended across the well-conducted RCTs that havelongitudinal data would be valuable, as well as more de-
scription about the natural variation in the alignmentand educational supports for children transitioning fromearly educational interventions into public school pro-grams (Kagan, 1994).
KEY FEATURES OF COLLABORATIVE ANDCOMMUNITY PARTICIPATORY RESEARCH
Traditionally, scientific inquiry about child developmenthas been guided primarily by scientists with interests inadvancing scientific theory and practical understanding
dam4_c21.qxd 12/20/05 9:39 AM Page 885

886 Children’s Health and Education
of what influences the course of human development.Some research has been fueled by advocacy concerns,such as increased research into Autism, mental retarda-tion, AIDS, and learning and reading disabilities.Rarely, however, is research conducted in a way that ad-equately includes the perspectives of those whose livesare the primary topic of the research. Further, clini-cians, educators, and community members often haveextensive in-depth knowledge of topics germane to lon-gitudinal research on children and families, yet these in-dividuals seldom participate as full partners in thedesign and conduct of longitudinal research. Increas-ingly, scientists recognize the tremendous potentialvalue of conducting research in a way that actively en-gages and respects a much broader range of expertise,from multiple disciplines, practices, and community ex-periences. The challenge is how to efficiently and effec-tively create new types of partnerships in whichmultiple groups of “experts” can be combined to yield amore complete understanding of important influenceson children’s health and education.
We have established and used guidelines for conduct-ing collaborative research to evaluate the effects of in-terventions in education and health settings (S. L.Ramey & Ramey, 1997b). Figure 21.5 summarizes criti-cal activities in planning and conducting responsive,useful research on education and health interventions.Briefly, these include early engagement of key individu-als and groups as participants to create a shared visionand framework to guide decision making and the identi-fication of key questions and plans for gathering and an-alyzing data. Vital to the success of collaborative andcommunity participatory research is the generation oftimely interim reports that provide practical informationabout the progress of program implementation and earlyevidence about program impact and children’s develop-ment. Active maintenance of these partnerships isequally important to ensure continuity in the conduct oflongitudinal intervention research and to understandother changes occurring over time in the community andfamilies’ lives that may affect measured health and edu-cation outcomes. These research partnerships facilitateaccurate identification of changes in the community andfamily context that may independently and interactivelyaffect child health and education. These partnershipsnot only serve to foster scientific integrity in terms ofthe appropriate measurement of relevant multiple influ-ences, but also set the stage for informed interpretation,dissemination, and application of the results of such re-
search. In addition, the partnerships themselves canserve as an ongoing means of timely exchange of rele-vant information, including opportunities for scientiststo provide practitioners and families with valuable find-ings from previous research that could be practically ap-plied in the community (see Figure 21.5).
We would be remiss if we did not state there are seri-ous challenges associated with conducting such com-plex, ambitious, and action-oriented research. Theseinclude the importance of identifying the appropriate in-dividuals who will be engaged in the partnership, recog-nizing that the members in the partnership will changeover time (for many reasons), findings ways the partner-ship can offer tangible benefits and appropriate recogni-tion to all participants throughout the partnership,anticipating and proposing how to resolve likely prob-lems and disagreements, and creating stronger supportswithin most universities for this type of research. Ide-ally, clearly written agreements (e.g., memoranda of un-derstanding) signed by key participants and communityand university leaders, widespread public media aboutthe partnership, and ongoing documented meetings toexchange information in ways that are open and honestserve as important mechanisms for maintaining projectintegrity, acceptability, and productivity.
As an example, when we created a long-term re-search partnership between a geographic communityand a major research university, we developed and en-dorsed a set of guiding operating principles (for moredetails, see C.T. Ramey & Ramey, 1997a, 1997b).These were (a) a pledge that there will be joint univer-sity and community development of all programs; (b) acommitment to research that benefits both the commu-nity and the university; (c) a commitment to programsthat make a difference in people’s everyday lives; (d) apledge from partners to maintain the partnership for anextended period (e.g., a decade); (e) a belief that overtime both the community and the university will be-come better places as a direct result of the quality ofpartnership; and (f ) a commitment to conducting thepartnership in a way that could serve as a model for oth-ers (e.g., to expand the benefits and to facilitate produc-tive university-community partnerships).
Universities and Public Policy
Universities have been the largest incubator for modelresearch programs to enhance young children’s educa-tion and to test health interventions. Unfortunately,
dam4_c21.qxd 12/20/05 9:39 AM Page 886

887
Figure 21.5 Critical activities in planning and conducting responsive, useful health and education evaluations. Adapted from “TheRole of Universities in Child Development” (pp. 13–44), by S. L. Ramey and C. T. Ramey, in Children and Youth: InterdisciplinaryPerspectives, H. J. Walberg, O. Reyes, and R. P. Weissberg (Eds.), 1997b, Thousand Oaks, CA: Sage. Reprinted with permission.
dam4_c21.qxd 12/20/05 9:39 AM Page 887

888 Children’s Health and Education
many of the model programs shown to yield positivebenefits have not been adopted and implemented in com-munity settings to realize comparable benefits on alarge scale. We think this indicates an inherent limita-tion in the old-style research that has been primarilyconducted within one or two major disciplines, led byuniversity scientists, funded by federal agencies withoutrequiring early and sustained engagement of key com-munity stakeholders, and not designed to take into ac-count public policies and practical issues that willdetermine whether new programs can readily be imple-mented in the community.
To a remarkable degree, the historical structure ofuniversities also has guided the structure of the researchfunding and the ways communities are organized to pro-vide supports for children and families (C. T. Ramey &Ramey, 1997b). Specifically, the historical disciplinarytraining that grants degrees in areas such as social work,psychology, pediatrics, pediatric dentistry, pediatric re-habilitation, early childhood education, special educa-tion, educational psychology, child and family nursing,child psychiatry, public health, and urban planning (andmany others) contributed to the creation of paralleltypes of service organizations and community-basedpractices that have hindered the provision of well-coordinated, efficient, and comprehensive supports forchildren and families. This dispersion has created a re-markable fragmentation and duplication of services in atime of limited resources and high need. Similarly,within universities, a highly compartmentalized knowl-edge base about children and families has evolved, withno obvious way to create a unified understanding ofchild development and effective means of enhancing thedevelopment of the most at-risk children.
Potential benefits of reorganization within universi-ties and communities, consistent with the scientific evi-dence about how children learn and how their health ispromoted, are great. Just as the university-led researchand demonstration projects are inherently limited, so,too, are many well-intentioned community-based pro-grams that have not realized their intended benefits,even when they have sought to be comprehensive and co-ordinated. The community initiatives often do not in-clude rigorous research from the beginning, just as manyuniversity-led efforts have not adequately included com-munity input and partners. We think this further sup-ports the need for major policy and organizationalchanges in both universities and communities—changesthat will not be easy or welcomed by all. Genuine reor-
ganization would likely mean the end of some disciplinesand practices as we know them today and the creation ofnew combined or coordinated fields and practices de-signed to better meet the needs of children and familiesin ways that are more holistic, informed by scientificfindings, and responsive to communities and consumers.
This type of research also places universities in a newposition, one in which they are actively supporting rela-tionships to improve well-being in the community, whileat the same time generating new knowledge. Accord-ingly, universities may need to consider how to strategi-cally invest in infrastructure support for this type ofresearch (i.e., on a par with planning for new technologyand laboratory supports), how to recognize and rewardfaculty and staff for productively sustaining these research-service partnerships, and how to operate inmore flexible and accommodating ways to promote thesepartnerships (e.g., creating easy-to-handle subcontracts,joint hiring or supervising of staff, reducing indirectcost rates for certain activities, f lexibility in paying forcommunity consultation, offering access to universitycourses and services to community partners). Finally,universities need to anticipate that the emerging resultsfrom longitudinal research may sometimes be controver-sial and politically charged. Ideally, the partnershipagreements will have anticipated a full range of results,and active partnerships will accept responsibility foragreed-upon ways to share and act on the findings. Sci-entific and academic freedom cannot be compromised;neither should the needs of the community and researchparticipants be ignored in how the findings are inter-preted and disseminated. These complicated and thornyissues need to be openly discussed and considered in anongoing fashion, consistent with the overall goal of pro-moting children’s health and education.
SUMMARY
Both early childhood education programs and community-based prevention and health promotion interventions needto incorporate a transdisciplinary approach that builds onrecent scientific findings and reflects advances in inte-grating the historically separate fields of health and edu-cation. This relatively new and innovative approach can becharacterized as a systematic endeavor to individualizeand integrate the supports provided to treat and educate“the whole child.” Health is defined consistent with the
dam4_c21.qxd 12/20/05 9:39 AM Page 888

Summary 889
WHO definition as including an individual’s psychosocialwell-being, not merely the absence of disease or disability.Similarly, education is defined as more than just intellec-tual ability and performance on standardized measures ofacademic achievement; that is, a child’s progress in theeducational arena includes social-emotional skills, theability to adapt to change, and a wide array of cognitiveand problem-solving skills that support lifelong learningand competence.
There are many well-intentioned federal, state, andlocal multicomponent initiatives under way, includingthe well-known Head Start, Early Head Start, early in-tervention programs for children with developmentaldisabilities and risk conditions, subsidized child carequality enhancement efforts, and school readiness andtransition-to-school programs. This chapter presented asan example the Head Start-Public School Early Child-hood Transition Demonstration Project, a multisite,congressionally mandated intervention to help promotethe educational attainment and health of former HeadStart children and their classmates, based on an ideologyof two-generation, community-based family support.
Children’s health and education are widely recog-nized as vital for their success as contributing mem-bers of society, yet relatively few studies haveendeavored to understand how health and educationmutually influence each other and combine to deter-mine the course of a child’s development. Appliedbiosocial contextual development is a general concep-tual framework that is strongly supported by researchfindings and has proven useful in designing and study-ing interventions to improve children’s health and edu-cation. ABCD identifies multiple and co-occurringtypes of influences on development from a systems theory perspective. Children’s development is dimen-sionalized in terms of biological and social processesthat can be more or less supported or hindered by envi-ronmental conditions, and thus contribute to threemajor classes of interrelated outcomes: children’shealth status and health promotion behaviors (health);children’s behavioral, intellectual, and social develop-ment, and their educational progress (education); andchildren’s own internal representations of themselves,their environments, and their experiences (personalconstructs).
Many carefully planned interventions have yieldedscientific findings about what constitutes effectivechildhood interventions. We reviewed and summarizedthese findings by delineating five major principles of ef-
fective early intervention. The scientific principles sup-ported by research are the following:
1. The principle of dosage, in which more intensive orhigher-dose interventions yield larger and longer-lasting effects, whereas less intensive interventionsoften yield limited or no demonstrable benefits.
2. The principle of timing, supporting the conclusion thatinterventions that are well-timed to take advantage ofchildren’s neuroplasticity in multiple domains, by be-ginning fairly early in life and continuing through pe-riods of rapid growth and learning, produce morepositive outcomes.
3. The principle of direct receipt of supports, indicatingthat, to date, programs that seek to change children onlyby changing their parents and community providershave not produced evidence of significant benefits tochildren themselves, whereas programs that provideservices directly to children (often accompanied byfamily and community supports) can alter the develop-mental trajectories of individual children.
4. The principle of differential benefits, which predictsthat planned interventions are likely to have greateror lesser impact on children, depending on a combi-nation of factors, such as the initial type and magni-tude of a child’s risks and needs and the extent towhich these are specifically addressed in the inter-vention. For example, children whose mother has lim-ited resources to meet her young children’s cognitiveand language learning needs have benefited signifi-cantly more from early educational interventionsthan have children whose mother initially had muchgreater amounts of educational, economic, and healthresources.
5. The principle of continuity of supports, which af-firms the importance of children receiving the righttypes and amounts of environmental supports forhealth and education throughout their development.That is, there is no evidence that early interventionprograms alone can produce large and sustainablebenefits in the absence of children receiving reason-ably good supports from schools, families, and com-munities after the planned intervention.
Much remains to be learned about the ways these fivemajor principles interact across different ages and stagesof development and within and across diverse culturaland regional settings. The future of scientific inquiry
dam4_c21.qxd 12/20/05 9:39 AM Page 889

890 Children’s Health and Education
about children’s health and education research will de-pend largely on the degree to which studies are morecarefully designed, implemented, documented, and sum-marized in ways that can be compared and combinedwithin a practically useful knowledge framework.
To conduct such complex research, especially involv-ing large-scale and sustainable prevention and interven-tion programs, a new style of collaborative research thatengages the community and broader expertise from pro-fessionals, scientists, and citizens is vitally needed. En-gaging individuals and groups in the early stages ofplanning and implementation has great promise for pro-ducing results that are more valid, more sensitive, andmore acceptable and useful to families, practitioners,and communities. Conducting such research necessi-tates an in-depth understanding of the complex andchanging ways that policy, economics, politics, and prac-tice operate in the fields of education and health. Thegoal of such research is undeniably both basic and ap-plied, and potentially may yield insights to move into anera where the large disparities and inequities in healthand education for low-income, historically marginalizedgroups of children are drastically reduced and eventu-ally eliminated.
REFERENCES
Barnett , W. S. (2004). Does Head Start have lasting cognitive ef-fects? The myth of fade out. In E. Zigler & S. J. Styfco (Eds.),Head Start debates (pp. 221–249). Baltimore: Paul H. Brookes.
Bertalanffy, L. V. (1975). Perspectives on general system theory. NewYork: George Braziller.
Binder, A. (1972). A new context for psychology: Social ecology.American Psychologist, 27, 903–908.
Blair, C., Ramey, C. T., & Hardin, M. (1995). Early intervention for lowbirth weight premature infants: Participation and intellectual de-velopment. American Journal on Mental Retardation, 99, 542–554.
Borkowski, J. G., Ramey, S. L., & Bristol-Powers, M. (Eds.). (2002).Parenting and the child’s world: Inf luences on academic, intellec-tual, and social-emotional development. Hillsdale, NJ: Erlbaum.
Bronfenbrenner, U. (1977). Toward an experimental ecology ofhuman development. American Psychologist, 32, 513–530.
Bronfenbrenner, U. (1979). The ecology of human development. Cam-bridge, MA: Harvard University Press.
Bryant, K., Windle, M., & West, S. G. (1997). The science of preven-tion: Methodological advances from alcohol and substance abuseresearch. Washington, DC: American Psychological Association.
Campbell, F. A., Pungello, E., Burchinal, M., & Ramey, C. T. (2001).The development of cognitive and academic abilities: Growthcurves from an early childhood educational experiment. Develop-mental Psychology, 37, 231–242.
Campbell, F. A., Ramey, C. T., Pungello, E., Sparling, J., & Miller-Johnson, S. (2002). Early childhood education: Young adult out-
comes from the Abecedarian Project. Applied Developmental Sci-ence, 6, 42–57.
Coie, J., Watt , N., West, S., Haskins, D., Asarnow, J., Markman, H.,et al. (1993). The science of prevention: A conceptual frameworkand some directions for a national research program. AmericanPsychologist, 48, 1013–1022.
Cole, K. N., Dale, P. S., Mills, P. E., & Jenkins, J. R. (1991). Effectsof preschool integration for children with disabilities. ExceptionalChildren, 58, 36–45.
Currie, J., & Thomas, D. (1995). Does Head Start make a difference?American Economic Review, 83, 241–364.
Garber, H. L. (1988). Milwaukee Project: Preventing mental retarda-tion in children at risk. Washington, DC: American Associationon Mental Retardation.
Garmezy, N. (1983). Stressors of childhood. In N. Garmezy &M. Rutter (Eds.), Stress, coping and development in children(pp. 43–84). New York: McGraw-Hill.
Grantham-McGregor, S., Powell, C., & Fletcher, P. (1989). Stunting,severe malnutrition and mental development in young children.European Journal of Clinical Nutrition, 43, 403–409.
Gray, S. W., Ramsey, B. K., & Klaus, R. A. (1982). From 3 to 20: Theearly training project. Baltimore: University Park Press.
Grotberg, E. H. (2003). Resilience for today. Westport , CT: Praeger.
Guralnick, M. J., & Bennett , F. C. (Eds.). (1987). The ef fectiveness ofearly intervention for at-risk and handicapped children. SanDiego: Academic Press.
Hart , B., & Risley, T. R. (1995). Meaningful dif ferences in theeveryday experience of young American children. Baltimore: PaulH. Brookes.
Hauser-Cram, P., Pierson, D. E., Walker, D. K., & Tivnan, T. (1991).Early education in the public schools. San Francisco: Jossey-Bass.
Hill, J. L., Brooks-Gunn, J., & Waldfogel, J. (2003). Sustained effectsof high participation in an early intervention for low-birth-weightpremature infants. Developmental Psychology, 39, 730–744.
Horacek, H. J., Ramey, C. T., Campbell, F. A., Hoffman, K. P., &Fletcher, R. H. (1987). Predicting school failure and assessingearly interventions with high-risk children. Journal of the Ameri-can Academy of Child Psychiatry, 26, 758–763.
Huttenlocher, P. R. (1990). Morphometric study of human cerebralcortex development. Neuropsychologia, 28(6), 517–527.
Infant Health and Development Program. (1990). Enhancing the out-comes of low birth weight, premature infants: A multisite ran-domized trial. Journal of the American Medical Association, 263,3035–3042.
Kagan, S. L. (1994). Defining and achieving quality in family sup-port. In B. Weissbourd & S. L. Kagan (Eds.), Putting familiesfirst: America’s family support movement and the challenge ofchange (pp. 375–400). San Francisco: Jossey-Bass.
Kelly, G. A. (1955). The psychology of personal constructs. Oxford:Norton.
Kuhl, P. K., Tsao, F. M., & Liu, H. M. (2003). Foreign-language expe-rience in infancy: Effects of short-term exposure and social inter-action on phonetic learning. Proceedings of the National Academyof Science, 100(15), 9096–9101.
Landesman, S., & Ramey, C. T. (1989). Developmental psychologyand mental retardation: Integrating scientific principles withtreatment practices. American Psychologist, 44, 409–415.
Landesman-Dwyer, S., & Butterfield, E. C. (1983). Mental retarda-tion: Developmental issues in c ognitive and social adaptation. In
dam4_c21.qxd 12/20/05 9:39 AM Page 890

References 891
M. Lewis (Ed.), Origins of intelligence: Infancy and early child-hood (2nd ed., pp. 479–519). New York: Plenum Press.
Levenstein, P. (1970). Cognitive growth in preschoolers through ver-bal interaction with mothers. American Journal of Diseases ofChildren, 136, 303–309.
Lewin, K. (1936). Principles of topological psychology. New York:McGraw-Hill.
Lewin, K. (1951). Field theory in social science: Selected theoreticalpapers. New York: Harper & Row.
Lewis, M. (1984). Beyond the dyad. New York: Plenum Press.
Livingston, I. L. (Ed.). (2004). Praeger handbook of Black Americanhealth: Policies and issues behind disparities in health (Vols.1–2). Westport , CT: Praeger.
Madden, J., Levenstein, P., & Levenstein, S. (1976). Longitudinal IQoutcomes of the mother-child home program. Child Development,76, 1015–1025.
Martin, S. L., Ramey, C. T., & Ramey, S. L. (1990). The prevention ofintellectual impairment in children of impoverished families:Findings of a randomized trial of educational day care. AmericanJournal of Public Health, 80, 844–847.
Miller, J. G. (1978). Living systems. New York: McGraw-Hill.
Moser, H. W., Ramey, C., T., & Leonard, C. O. (1990). Mental retar-dation. In A. E. H. Emery & D. L. Rimoin (Eds.), The principlesand practices of medical genetics (Vol. 2, pp. 495–511). NewYork: Churchill Livingstone.
National Institute of Child Health and Human Development EarlyChild Care Research Network. (2005). Child care and child devel-opment: Results from the NICHD Study of Early Child Care andYouth Development. New York: Plenum Press.
National Safety Council. (2001). Injury facts: 2001 edition. Chicago:Author.
Olds, D. L., Kitzman, H., Cole, R., Robinson, J., Sidora, K., Luckey,D. W., et al. (2004). Effects of nurse home-visiting on maternallife course and child development: Age 6 follow-up results of arandomized trial. Pediatrics, 114, 1550–1559.
Ramey, C. T., Bryant, D. M., Campbell, F. A., Sparling, J. J., &Wasik, B. H. (1988). Early intervention for high-risk children:The Carolina Early Intervention Program. In H. R. Price, E. L.Cowen, R. P. Lorion, & J. Ramos-McKay (Eds.), Fourteen ouncesof prevention (pp. 32–43). Washington, DC: American Psycholog-ical Association.
Ramey, C. T., Bryant, D. M., Sparling, J. J., & Wasik, B. H. (1985).Project CARE: A comparison of two early intervention strategiesto prevent retarded development. Topics in Early Childhood Spe-cial Education, 5, 12–25.
Ramey, C. T., Bryant, D. M., Wasik, B. H., Sparling, J. J., Fendt,K. H., & LaVange, L. M. (1992). Infant Health and DevelopmentProgram for low birth weight, premature infants: Program ele-ments, family participation, and child intelligence. Pediatrics, 89,454–465.
Ramey, C. T., Campbell, F. A., Burchinal, M., Skinner, M. L., Gard-ner, D. M., & Ramey, S. L. (2000). Persistent effects of earlychildhood education on high-risk children and their mothers. Ap-plied Developmental Science, 4, 2–14.
Ramey, C. T., MacPhee, D., & Yeates, K. O. (1982). Preventing devel-opmental retardation: A general systems model. In J. M. Joffee &L. A. Bond (Eds.), Facilitating infant and early childhood devel-opment (pp. 343–401). Hanover, NH: University Press of New England.
Ramey, C. T., & Ramey, S. L. (1997a). Evaluating educational pro-grams: Strategies to understand and enhance educational effec-tiveness. In C. Seefeldt & A. Galper (Eds.), Continuing issues inearly childhood education (2nd ed., pp. 274–292). EnglewoodCliffs, NJ: Prentice-Hall.
Ramey, C. T., & Ramey, S. L. (1997b). The development of universi-ties and children: Commissioned paper for the Harvard UniversityProject on Schooling and Children. Cambridge, MA: HarvardUniversity Press.
Ramey, C. T., & Ramey, S. L. (1998a). Early intervention and earlyexperience. American Psychologist , 53, 109–120.
Ramey, C. T., & Ramey, S. L. (1998b). Prevention of intellectual dis-abilities: Early interventions to improve cognitive development.Preventive Medicine, 27, 224–232.
Ramey, C. T., & Ramey, S. L. (1999). Beginning school for children atrisk. In R. C. Pianta & M. J. Cox (Eds.), The transition to kinder-garten (pp. 217–251). Baltimore: Paul H. Brookes.
Ramey, C. T., & Ramey, S. L. (2004a). Early childhood education:The journey from efficacy research to effective practice. In D.Teti (Ed.), Handbook of research methods in developmental sci-ence (pp. 233–248). Malden, MA: Blackwell.
Ramey, C. T., & Ramey, S. L. (2004b). Early educational interven-tions and intelligence: Implications for Head Start. In E. Zigler &S. Styfco (Eds.), Head Start debates (pp. 3–17). Baltimore: PaulH. Brookes.
Ramey, C. T., & Ramey, S. L. (2004c). Early learning and schoolreadiness: Can early intervention make a difference? Merrill-Palmer Quarterly, 50, 471–491.
Ramey, C. T., Ramey, S. L., Gaines, R., & Blair, C. (1995). Two-generation early intervention programs: A child development per-spective. In I. Sigel (Series Ed.) & S. Smith (Vol. Ed.), Two-gen-eration programs for families in poverty—A new interventionstrategy: Vol. 9. Advances in applied developmental psychology(pp. 199–228). Norwood, NJ: Ablex.
Random House Webster’s unabridged dictionary (2nd ed.) (1997).Random House.
Ramey, C. T., Ramey, S. L., & Lanzi, R. G. (1998). Differentiatingdevelopmental risk levels for families in poverty: Creating a fam-ily typology. In M. Lewis & C. Feiring (Eds.), Families, risk, andcompetence (pp. 187–205). Hillsdale, NJ: Erlbaum.
Ramey, C. T., Yeates, K. O., & Short , E. J. (1984). The plasticity ofintellectual development: Insights from preventive intervention.Child Development, 55, 1913–1925.
Ramey, S. L. (2002). The science and art of parenting. In J. G.Borkowski, S. L. Ramey, & M. Bristol-Power (Eds.), Parentingand the child’s world: Inf luences on academic, intellectual, andsocial-emotional development (pp. 47–71). Hillsdale, NJ: Erlbaum.
Ramey, S. L., Lanzi, R., Phillips, M., & Ramey, C. T. (1998). Per-spectives of former Head Start children and their parents onschool and the transition to school. Elementary School Journal,98, 311–328.
Ramey, S. L., & Ramey, C. T. (1992). Early educational interventionwith disadvantaged children: To what effect? Applied and Preven-tive Psychology, 1, 131–140.
Ramey, S. L., & Ramey, C. T. (1997a). Evaluating educational pro-grams: Strategies to understand and enhance educational effec-tiveness. In C. Seefeldt & A. Galper (Eds.), Continuing issues inearly childhood education (2nd ed., pp. 274–292). EnglewoodCliffs, NJ: Prentice-Hall.
dam4_c21.qxd 12/20/05 9:39 AM Page 891

892 Children’s Health and Education
Ramey, S. L., & Ramey, C. T. (1997b). The role of universities inchild development. In H. J. Walberg, O. Reyes, & R. P. Weissberg(Eds.), Children and youth: Interdisciplinary perspectives(pp. 13–44). Thousand Oaks, CA: Sage.
Ramey, S. L., & Ramey, C. T. (1998). The transition to school: Op-portunities and challenges for children, families, educators, andcommunities. Elementary School Journal, 98, 293–296.
Ramey, S. L., & Ramey, C. T. (2000). Early childhood experiencesand developmental competence. In J. Waldfogel & S. Danziger(Eds.), Securing the future: Investing in children from birth to col-lege (pp. 122–150). New York: Russell Sage Foundation.
Ramey, S. L., Ramey, C. T., & Lanzi, R. G. (2004). The transition toschool: Building on preschool foundations and preparing for life-long learning. In E. Zigler & S. J. Styfco (Eds.), Head Start de-bates (pp. 397–413). Baltimore: Paul H. Brookes.
Ramey, S. L., Ramey, C. T., & Phillips, M. M. (1997). Head Startchildren’s entry into public school (Research Report 1997–2002).Washington, DC: U.S. Department of Health and Human Services,Administration for Children and Families.
Ramey, S. L., Ramey, C. T., Phillips, M. M., Lanzi, R. G.,Brezausek, C., Katholi, C. R., et al. (2001). Head Start children’sentry into public schools: A report on the National HeadStart /Public School Early Childhood Transition DemonstrationStudy (Contract No. 105-95-1935). Washington, DC: U.S. De-partment of Health and Human Services, Administration onChildren, Youth, and Families.
Ramey, S. L., & Sackett , G. P. (2000). The early caregiving environ-ment: Expanding views on non-parental care and cumulative lifeexperiences. In A. Sameroff, M. Lewis, & S. Miller (Eds.), Hand-book of developmental psychopathology (2nd ed., pp. 365–380).New York: Plenum Press.
Reid, M., Ramey, S. L., & Burchinal, M. (1990). Dialogues with chil-dren about their families. In I. Bretherton & M. Watson (Eds.),Children’s perspectives on their families: New directions for childdevelopment (pp. 5–28). San Francisco: Jossey-Bass.
Robinson, N. M., Lanzi, R. G., Weinberg, R. A., Ramey, S. L., &Ramey, C. T. (2002). Family factors associated with high aca-demic competence in former Head Start children at third grade.Gifted Child Quarterly, 46, 281–294.
Robinson, N. M., Weinberg, R. A., Redden, D., Ramey, S. L., &Ramey, C. T. (1998). Family factors associated with high aca-demic competence among former Head Start children. GiftedChild Quarterly, 42, 148–156.
Rutter, M. (2000). Resilience reconsidered: Conceptual considera-tions, empirical f indings, and policy implications. In S. J.Meisels & J. P. Shonkoff (Eds.), Handbook of early childhood in-tervention (2nd ed., pp. 651–682). New York: Cambridge Univer-sity Press.
Sameroff, A. J. (1983). Developmental systems: Contexts and evolu-tion. In P. H. Mussen (Ed.), Handbook of child psychology (Vol. 1,pp. 237–394). New York: Wiley.
Satcher, D. (2004). Foreword to Praeger handbook of Black Americanhealth. In I. L. Livingston (Ed.), Praeger handbook of Black Amer-ican health: Policies and issues behind disparities in health(pp. xxxi–xxxiv). Westport , CT: Praeger.
Scarr, S., & McCartney, K. (1988). Far from home: An experimentalevaluation of the mother-child home program in Bermuda. ChildDevelopment, 59, 531–543.
Schwebel, D. C., Brezausek, C. M., Ramey, S. L., & Ramey, C.(2004). Interactions between child behavior patterns and parent-ing: Implications for children’s unintentional injury risk. Journalof Pediatric Psychology, 29, 93–104.
Schweinhart , L. J., & Weikart , D. P. (1983). The effects of the PerryPreschool Program on youths through age 15. In Consortium forLongitudinal Studies (Ed.), As the twig is bent: Lasting ef fectsof preschool programs (pp. 71–101). Hillsdale, NJ: Erlbaum.
Shonkoff, J. P., & Phillips, D. A. (2000). From neurons to neighbor-hoods: The science of early childhood development. Washington,DC: National Academy Press.
Slater, M. A., & Power, T. G. (1987). Multidimensional assessmentof parenting in single-parent families. In J. P. Vincent (Ed.),Advances in family intervention, assessment and theory(pp. 197–228). Greenwich, CT: JAI Press.
Stokols, D. (1992). Establishing and maintaining healthy environ-ments: Toward a social ecology of health promotion. AmericanPsychologist, 47, 6–22.
Stokols, D. (1996). Translating social ecological theory into guide-lines for community health promotion. American Journal ofHealth Promotion, 10, 282–298.
Teti, D. (Ed.). (2004). Handbook of research methods in developmen-tal science. Malden, MA: Blackwell.
Vygotsky, L. S. (1978). Mind in society: The development of higherpsychological processes (M. Cole, V. John-Steiner, S. Scribner, &E. Souberman, Eds. & Trans.). Cambridge, MA: Harvard Univer-sity Press.
Waldfogel, J., & Danziger, S. (Eds.). (2001). Securing the future: In-vesting in children from birth to college. New York: Sage.
Wasik, B. H., Ramey, C. T., Bryant, D. M., & Sparling, J. J. (1990). Alongitudinal study of two early intervention strategies: ProjectCARE. Child Development, 61, 1682–1696.
Werner, E. E., Bierman, J. M., & French, F. E. (1971). The children ofKauai: A longitudinal study from the prenatal to age ten. Hon-olulu: University Press of Hawaii.
White, K. R. (1991). Longitudinal studies of the ef fects of alterna-tive types of early intervention for children with disabilities (An-nual report for project period October 1, 1990–September 30,1991). Logan: Utah State University, Early Intervention Re-search Institute.
World Health Organization. (2005). Retrieved September 15, 2005,from http://www.who.int /en.
dam4_c21.qxd 12/20/05 9:39 AM Page 892
Related Documents