Children with Special Health Care Needs ECSE 641 April 2015

Children with Special Health Care Needs ECSE 641 April 2015.
Dec 26, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Children with Special Health Care Needs
ECSE 641April 2015

CSHCN
Children with Special Health Care Needs:
Those who have or are at increased risk for a chronic physical, developmental, behavioral, or emotional condition and who require health and related services of a type or amount beyond that required by children generally.
Newacheck et al., 1998, p. 117
CSHCNO Development of technology services
to support children with disabilitiesO More children dependent on medical
technologyO More technology in the general and
special education classroomsO May require medical support services
throughout the day
CSHCNO Successful integration of students
who are dependent on medical technology requires:O Educational staffO Primary care physicianO School nurseO Family membersO Student (when appropriate)
Legal IssuesO Education for All Handicapped
Children Act of 1975
O IDEA 1990
O Individuals with Disabilities Education Improvement Act of 2004 (IDEIA)
Legal Issues - FAPEO Free, appropriate, public, education for all
children with disabilities that interfere with their educational process
O Transportation, physical therapy, occupational therapy, counseling, speech therapy, and health services
O Student must qualify for special education
O The service must be necessary for the student to benefit from special education

Legal Issues – Section 504
ORehabilitation Act of 1973 O -an individual with a physical or mental
impairment which substantially limits one or more of the person’s major life activities...(may include) caring for one’s self, performing manual tasks, walking, seeing, hearing, speaking, breathing, learning, and or working
Gelfman & Schwab, 2005, p. 337
Legal Issues – Section 504
O Child need not qualify for special education services.
O Services provided include: physical access, school health services, modified physical education, transportation, and access to field trips and extracurricular activities
O Gelfman & Schwab, 2005, p. 337
Legal Issues - ADA
OAmericans with Disabilities Act of 1990O Access for individuals with disabilities
to all public accommodations, including both public and private schools
O Includes all employees and members of the public
O Physical access and transportation
Special Health Care Procedures
O If possible, encourage full participation or partial participation during health care procedures to encourage independence and self-determination
O For instance: O Encourage student to climb onto nurses cot in
preparation for a routine procedureO Have student hold items in preparation for a
gastrostomy tube feeding

Special Health Care Procedures
O Something as routine as position changes for a student with limited movement abilities may help PREVENT health issues.
O Regular Position Changes may: O Facilitate drainage of lung secretions to help
with breathing O Encourage a BM to avoid constipationO Prevent a sore from prolonged pressure on skin
Special Health Care Procedures
O IHP- Individualized Health Care PlanO Developed and monitored by school nurse,
often in conjunction with the students family and medical doctor(s).
O Ensures that proper plans and safeguards, including emergency care plans, are in place.

General Health and SafetyO Infection Control
O ImmunizationsO Hepatitis B (HepB); Diphtheria, tetanus, acellular petussis
(DTaP); Measles, Mumps, Rubella (MMR); Inactivated Polio Vaccine (IPV); Haemophilus influenza type b (Hib); Pneumococcal (PCV); Chickenpox
O Other protections: Flu shot, Synagis (palivizumab) shot for RSV
O Hand washing/Glove use during certain proceduresO Disinfecting toys
Preventive Procedures – Skin Care
O Skin CareO Monitor the skin of children
O who spend the majority of their day in a wheelchairO who wear braces/splintsO who have decreased sensation (i.e. MMC or SCI)
O Allow for frequent position changes to avoid prolonged periods of pressure on bony prominences.
O Keep skin clean and dry. Skin that is moist for prolonged periods is more vulnerable to injury and the development of sores.

Special Health Care ProceduresO Regular Position Changes:
Tumble Forms Tadpole Positioning System
Tumble Forms Prone Wedge
Rifton Prone Stander

Specialized Procedures - Seizures
O Seizure- “A seizure involves the abnormal, excessive, and concurrent firing of a large population of cortical neurons. This results in the interruption of usual brain-generated electrical signals…”
O Epilepsy- “…a condition involving two unprovoked seizures separated by 24 hours.”
(Definitions from Batshaw, Pellegrino, and Roizen, 2007.)

Specialized Procedures -Seizures
O Optimal control of seizures with medications is often difficult in children with cerebral palsy and developmental problems.
O Medications used to control seizure activity are referred to as AED’s – Antiepileptic DrugsO phenytoin- DilantinO carbamazepine – TegretolO valproate – Depakene, Depakote
Specialized Procedures -Seizures
O AED’s often have side effects and include: O SleepinessO Decreased attentionO Decreased memoryO Difficulty producing speechO Unstable gaitO Double visionO Cognitive impairment at high doses during
treatment (long term effects unknown)
Specialized Procedures -Seizures
O Other treatmentsO Surgery to remove seizure focusO VNS – Vagus Nerve Stimulation
O Poor response to medications O Generalized Seizures (no focal point)
O Hemispherectomy in extreme casesO Special diets (ketogenic diet)O Ensure adequate rest, avoid illness/infection,
avoid “triggers”
Specialized Procedures -Seizures
O A child with a known seizure disorder should have a care plan (IHP) in place with instructions specific to that child. Some children wear lightweight protective helmets.
O Intervention will depend on seizure type and duration.
O Once seizure activity has ended, document length of seizure and what occurred before and during the seizure.
Specialized ProceduresDuring a Seizure
O In general:O Place child on floor and turn to one sideO Do not tightly restrainO Loosen clothing, especially around the neckO Do not insert anything in the mouthO Call EMS if:
O Seizure lasts longer than 5 minutesO There is no history of seizuresO A second seizure quickly occursO Child does not regain consciousness
Specialized Procedures - Seizures
O After the seizure activity has ended: O Monitor breathing-
O if breathing has stopped, activate EMS and begin resuscitation efforts.
O if student is breathing, roll to side and monitor
Specialized Procedures -Medications
O Follow school district policies regarding administration of medications.
O Be aware of medications your students are taking even if they do not receive them at school.
O Be aware of medication side effects and precautions O i.e. Avoidance of sun exposure
Specialized Procedures –Alternative Feeding
O Alternative forms of feeding are necessary for: O children unable to eat or drink anything by
mouth (NPO) because of- O risk of aspiration, O abnormalities of the mouth, jaw, and/or upper GI
tract, O extreme sensitivity issues
O children unable to ingest sufficient amounts of food/fluids for adequate nutrition and hydration
Specialized Procedures – Alternative Feeding
O Naso-gastric tube – NG tube O Gastrostomy tube – G-tubeO Gastrostomy button – i.e Mic Key feeding tubeO Jejunostomy tube – J- tubeO G-J Tube
O These are forms of enteral nutrition

Specialized Procedures – Alternative Feeding
NG Tube
Mic Key Feeding Tube
Gastrostomy Tube

Specialized Procedures – Alternative Feeding
O Formula, blended food, or liquids are administered through the tube.
O The tube empties either into the stomach or the upper intestine.
O Feedings may be continuous or intermittentO Feedings may be driven by gravity, pump, or
syringe.

Specialized Procedures – Alternative Feeding
O If possible, children should receive their feedings during the regular meal times or snack times.
O Typically children are sitting or in an upright position during the tube feeding and remain upright for approximately one hour after the completion of the feeding.

Specialized Procedures- Alternative Feeding
O A plan should be in place in the event of feeding tube failure or dislodgement. Usually an extra tube kit is kept at school or the child care facility.
O If a gastrostomy tube dislodges, cover the stoma with clean gauze. Alert the school nurse or parent (follow the care plan). The tube should be replaced soon- within 2 hours.
O A physician must replace a jejunostomy-tube.
Special Care Procedures- Respiratory Management
O Trachea- air tube extending from the larynx into the lungs
O Tracheotomy/Tracheostomy- the operation of opening into the trachea
O Tracheostomy tube-the tube inserted into the opening in the trachea
O “Artificial Nose”- warms and humidifies the air breathed in.
Special Care Procedures- Respiratory Management
O Reasons a child may have a tracheostomy tube: O Obstruction of respiratory tractO Allows for long term assisted ventilation in
cases of respiratory insufficiency from: O Conditions that affect the lungs O Deregulation of central controls for breathing
(TBI)O Disease/disorder of chest wall/thorax
O Allows for removal of secretions by suctioning

Special Care Procedures- Respiratory Management
O Children with tracheostomy tubes, with or without mechanical ventilation, typically are accompanied to school with a nurse.
O Routine procedures that may occur at school include: suctioning to remove secretions, cleaning the tracheostomy tube, care of the skin around tube, and changing the ties. Changing the tube is typically performed at home, but a spare tube is always kept with the child.
Special Care Procedures- Respiratory Management
O Speaking valve- a special valve placed on the tracheostomy tube that allows the child to breath in, but then closes when the child breathes out, forcing air around the vocal cords and allowing the student to speak.
O The Passy-Muir valve is often used with infants and young children.
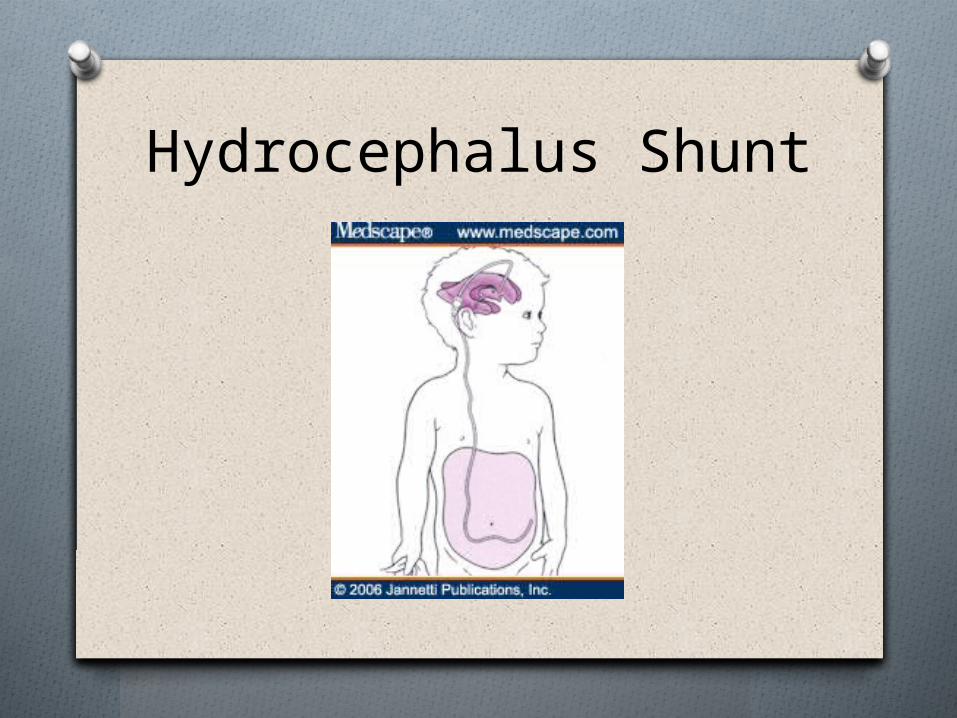
Hydrocephalus Shunt
Signs of Shunt MalfunctionFrom : A Teachers Guide to Hydrocephalus (2002). Hydrocephalus Association: San Francisco, California
www.hydroassoc.org
Vomiting Headache Vision problems Irritability and/or
tirednessPersonality change Loss of coordination or
balance
Swelling along the shunt tract
Difficulty in waking up or staying awake
Decline in academic performance
Fever Redness along the
shunt tract
Signs of shunt malfunctionAdditional signs from Snell, M. & Brown, F. (2006). Instruction of students with severe disabilities (6th ed.) New Jersey: Pearson Publishing.
OChange in appetiteO IrritabilityOSwelling along path
of shuntOOnset of or
increased seizures
ONeck painOOnset of or
increased spasticityOChanges in vision
and eye movements
ReferencesO A Teachers Guide to Hydrocephalus (2002).
Hydrocephalus Association: San Francisco, Californiawww.hydroassoc.org
O Batshaw, M., Pellegrino, L., & Roizen, N. (2007). Children with disabilities (6th ed.) Baltimore: Paul H. Brookes Publishing
O Snell, M. & Brown, F. (2006). Instruction of students with severe disabilities (6th ed.) New Jersey: Pearson Publishing.
Related Documents











