Childhood Caries & Dental Trauma on Primary Teeth Henri Hartman, drg. Sp.KGA

Childhood Caries 1
Sep 29, 2015
asdaf
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Childhood Caries
Childhood Caries&Dental Trauma on Primary Teeth
Henri Hartman, drg. Sp.KGA
4 yrs old
Panoramic x-ray before treatment
Preparation
Post op with zirconia crown
6 mth later
1,5 yrs later
Caries?
progressive dissolution of the inorganic component of dental hard tissues mediated by dental plaque
A biofilm (plaque)-induced acid demineralization of enamel or dentin, mediated by saliva
Dental Plaque
contains bacteria acidogenic and aciduric
Streptococcus mutans
lactobacilli
Acidogenic : produce acid
Aciduric : live on acid environment
S. mutans
initiation of enamel demineralization
Inoculated vertically form mother/caregiver
Inoculated horizontally by peers at childcare centre
Came as teeth erupted
High S.mutans High caries risk
Diet
Host Factor
TEETH
Microbes
Tooth quality, saliva, amount of microbe, sugar contact
13
Subtstrate
Bacteria can use fermentable carbohydrates as a ready source of energy and the end-products of the glycolytic pathway in bacterial metabolism are acids.
Sucrose
Saliva
Saliva Function
antibacterial and antifungal and antiviral activity.
lubrication, which also assists in bolus formation.
inhibition of demineralization and stabilization of calcium and phosphate ions, which assists remineralization.
TIME
acid challenges occur repeatedly,
collapse of enamel crystals
Ca10(PO4)6(OH)2+2H+ 10Ca2+ + 6PO43- + 2H2O
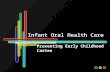
Early Childhood Caries
baby bottle tooth decay,
early childhood dental decay,
Early childhood tooth decay,
comforter caries,
Nursing bottle caries,
maxillary anterior caries,
rampant caries,
ECC
The presence of one or more decayed(non-cavitated or cavitated lesions), missing (due to caries) or filled tooth surfaces in any primary tooth in a preschool-age child between birth and 71 months of age.
ECC
Terminology, aapd
19
affect the primary teeth of infants and pre-school children.
the maxillary primary incisors are hit the hardest, followed by the first primary molars.
The mandibular incisors normally are spared because they are covered by the tongue during suction movements and are thus buffered against cariogenic liquids
ECC
Primary canines and second primary molars,
later eruption
ECC
Tooth usually spared or little affected by ECC.
timing of the tooth eruption,
the time span of the harmful oral habit,
the type of muscle movements the child makes when sucking
Caries develop quickly
ECC factor level
ECC stage
chalky, opaque demineralization lesions on the smooth surfaces of the maxillary primary incisors
whitish line can be distinguished in the cervical region of the vestibular and palatal surfaces of the maxillary incisors.
reversible but are frequently unrecognized
can be diagnosed when teeth thoroughly dried.
Initial stage (ages of 10 and 20 months)
The dentin is affected.
The dentin is exposed and appears soft and yellow.
The maxillary primary molars present initial lesions in the cervical, proximal and occlusal regions
ECC stage
Second stage (ages of 16 and 24 months)
Stage 1 and stage 2
ECC stage
large, deep lesions on the maxillary incisors
pulpal irritation.
pain when chewing or teeth brushed,
spontaneous pain during the night.
At this point, the maxillary primary molars are at stage 2, while stage 1 can be diagnosed on the mandibular primary molars and the maxillary canines.
ECC stage
Third stage (20 and 36 months)
coronal fractures of the anterior maxillaries as a result of amelodentinal destruction
maxillary incisors are usually necrotized,
maxillary primary molars are at stage 3.
The secondary molars and maxillary canines and the first mandibular molars are at stage 2.
Some young children suffer but are unable to express their toothache complaints.
They experience sleep deprivation and refuse to eat.
ECC stage
The fourth stage, (30 and 48 months)
Stage 4
ECC stage
ECC Complications
Complications
pulp necrosis,
infection spreads to the pulpalperiodontal
the acute form (cellulitis, adenopathy and mobility of the affected teeth)
the chronic form (abcesses and interdental septum syndrome).
infection can spread to the buds of the permanent teeth, causing irreversible lesions.
ECC stage
PREVENTION of ECC
Dental Health Promotion
Pregnancy treatment (routine maintanence)
After birth : cleaned erupted tooth with wet cloth / childs toothbrush / fluoride toothpaste
Age One yrs old : brushed twice daily
No candy / sugar / sweet drink
Fluoride therapy if needed
Pit & Fissure Sealant
Caries Arrested
Primary tooth anatomy
Dental Injury/Trauma
Classification of trauma to anterior teeth
Ellis and Davey (1961)
Class 1 : simple fracture of the crown, involving little or no dentin
Class 2 : extensive fracture of the crown involving considerable dentin, but not the pulp
Class 3 : extensive fracture of the crown involving dentin and pulp
Class 4 : the traumatized tooth which becomes non-vital with or without loss of crown structure
Class 5 : Loss of tooth
Class 6 : Root fracture with or without loss of crown structure
Class 7 : displacement of a tooth without fracture of crown or root
Class 8 : Fracture of crown enmass
Class 9 : Traumatic injuries of deciduous teeth
Classification
WHO clasiffication
873.60 : Enamel fracture
873.61 : Crown fracture involving enamel and dentin without pulp exposure
873.62 : Crown fracture with pulp exposyure
873.63 : Root Fracture
873.64 : Crown-root fracture
(uncomplicated/complicated crown- root fracture)
873.66 : Luxation
(Concussion / subluxation / lateral luxation)
873.67 : Intrusion or extrusion
873.68 : Avulsion
873.69 : Other injuries like soft tissue injuries
Enamel Cracking
Fracture involving only enamel
Fracture involving enamel & dentin
Fracture involving enamel & dentin & pulp
uncomplicated crown-root fracture
complicated crown-root fracture
Tooth nonvital with or without fracture
1/3 Apical root fracture
1/3 coronal root fracture
1/3 Middle root fracture
Fracture of crown enmass
I
Intrusion
Extrusion
Lingual/palatal displacement
Concussion & Subluxation
Concussion is an injury to the tooth and ligament without displacement or mobility of the tooth.
Subluxation occurs when the tooth is mobile but is not displaced.
Concussion & Subluxation
Management
Periapical radiographs as baseline.
Soft diet for 1 week.
Advice to the parents of possible sequelae, such as pulp necrosis and infection.
Individualized follow-up.
Intrusion
Management
If the crown is visible and there is only minor alveolar damage leave tooth to re-erupt.
If the whole tooth is intruded extract.
Extrusion and lateral luxation
Treatment is dependent on the mobility and extent of displacement. If there is excessive mobility the tooth should be extracted.
Avultion
No reimplantation for PRIMARY teeth
Root Fracture
No treatment needed unless : necrotic pulp, infection, sinus tract, high mobility
Leave apical fragmen
Extract coronal fragmen
Fracture without pulp involve
GIC restoration
Resin composite
Strip-crown
Zirconia crown
-Auf Wiedersein-
Related Documents