Wisdom of the Land Childhood acute leukemia 4 th August, 2019 Kleebsabai Sanpakit, MD Division of Hematology/Oncology Department of Pediatrics Faculty of Medicine, Siriraj Hospital Mahidol University

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Wisdom of the Land
Childhood acute leukemia
4th August, 2019
Kleebsabai Sanpakit, MD Division of Hematology/Oncology
Department of Pediatrics Faculty of Medicine, Siriraj Hospital
Mahidol University
Topic outline
Conditions Predisposing to childhood leukemia Diagnosis and classification Risk stratification Treatment in pediatric leukemia Indications for HSCT Summary
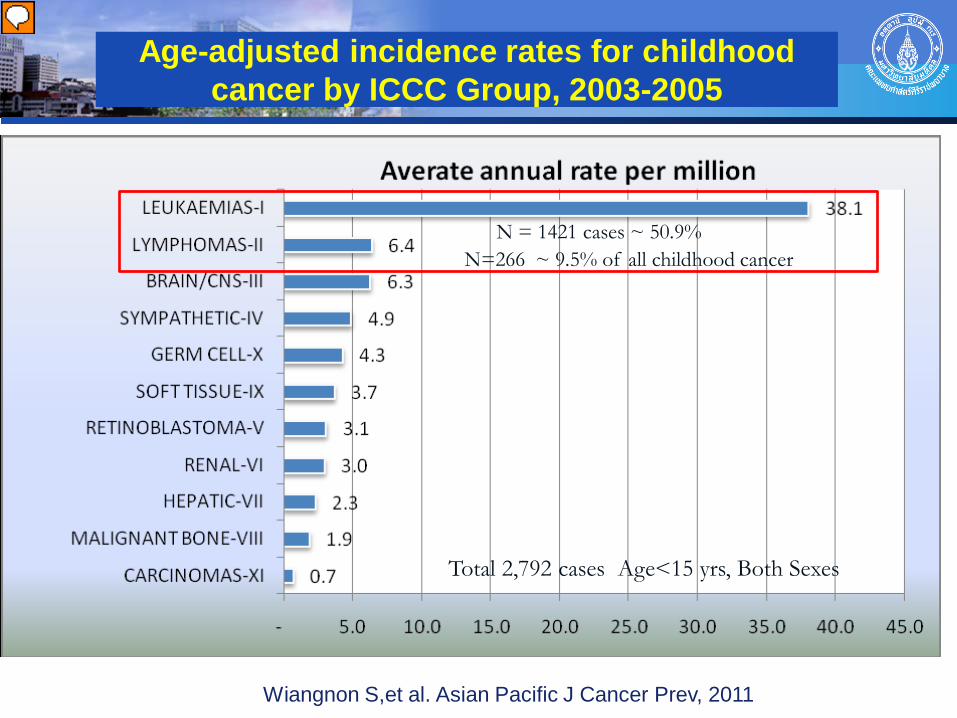
Age-adjusted incidence rates for childhood cancer by ICCC Group, 2003-2005
Wiangnon S,et al. Asian Pacific J Cancer Prev, 2011
Total 2,792 cases Age<15 yrs, Both Sexes
N=266 ~ 9.5% of all childhood cancer
N = 1421 cases ~ 50.9%
Presenter
Presentation Notes
Aged-standardization rate (ASR) 6.4 per million person-years International Classification of Childhood Cancer (ICCC)
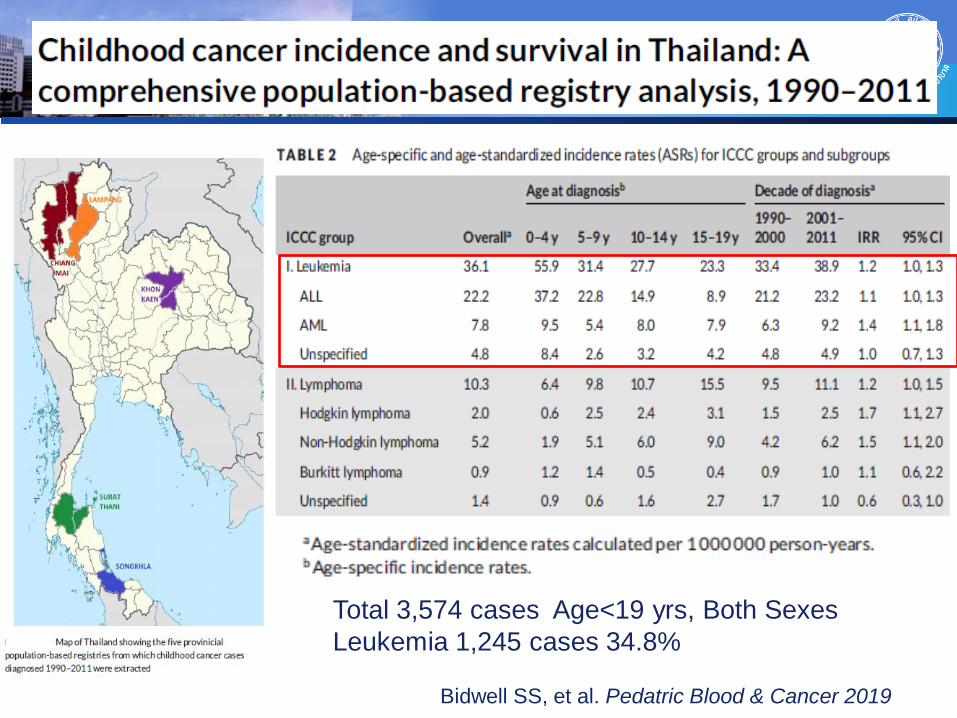
Bidwell SS, et al. Pedatric Blood & Cancer 2019
Total 3,574 cases Age<19 yrs, Both Sexes Leukemia 1,245 cases 34.8%
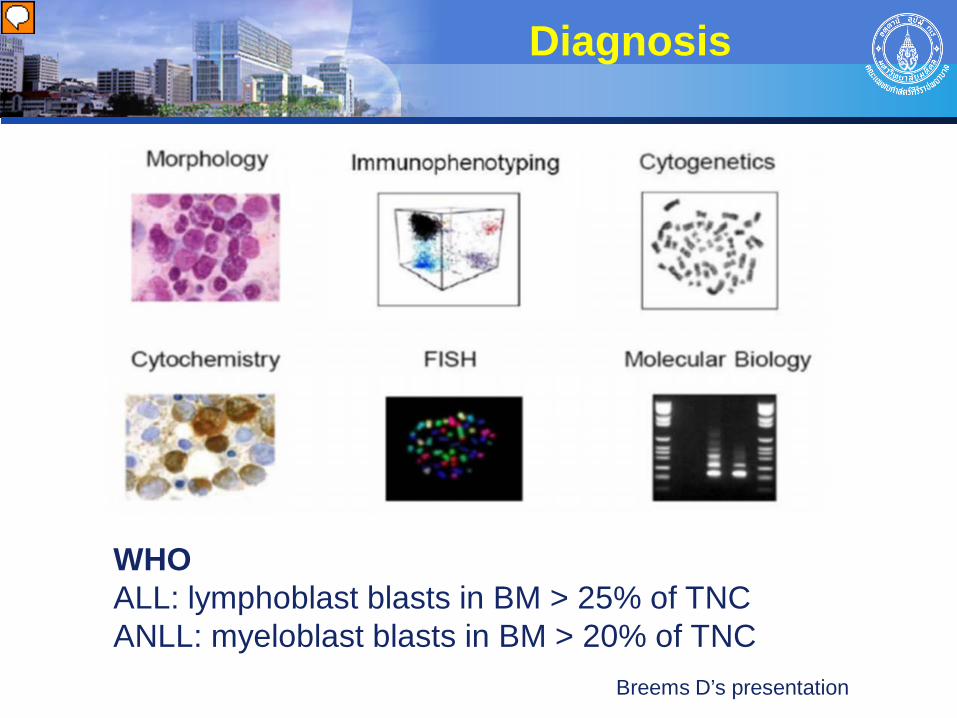
Diagnosis
Breems D’s presentation
WHO ALL: lymphoblast blasts in BM > 25% of TNC ANLL: myeloblast blasts in BM > 20% of TNC
Presenter
Presentation Notes
Breems D’s presentation AML: Heterogeneous disease classified by - Morphology ตาม FAB classification - lineage/ immunophenotyping - genetic: cytogenetic study, molecular genetic analysis
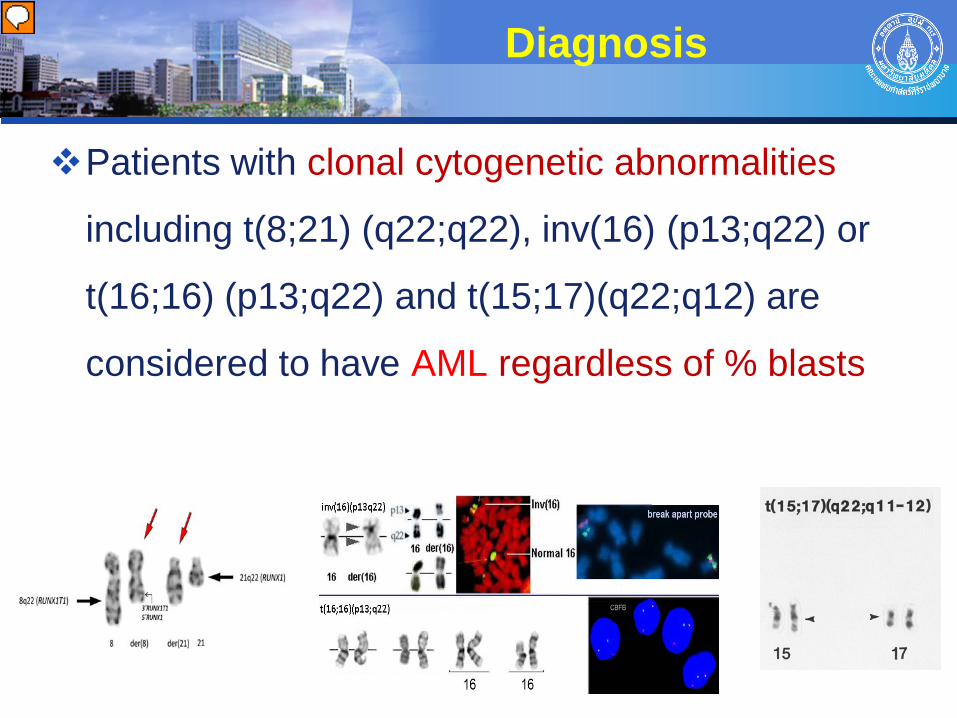
Diagnosis
Patients with clonal cytogenetic abnormalities
including t(8;21) (q22;q22), inv(16) (p13;q22) or
t(16;16) (p13;q22) and t(15;17)(q22;q12) are
considered to have AML regardless of % blasts
Presenter
Presentation Notes
Myeloid leukemia associated with Down syndrome
1. Environmental
- Ionizing radiation
- Chemical exposure: Benzene/Petroleum, Herbicides/Pesticides
- Drugs: Alkylating agents typically present within 3-5 years after
Rx, AML with poor-risk cytogenetics
Epidophyllotoxin typically present 6-36 months after Rx,
FAB M4 or M5, often involves MLL gene rearrangement (11q.23)
- Infections: EBV - Burkitt’s lymphoma
HTLV I - T cell ALL
Risk factors
Presenter
Presentation Notes
Therapy-related AML (t-AML) worse prognosis than de novo AML with identical cytogenetics
Risk factors
2. Predisposing conditions - Noninherited syndrome:
Aplastic anemia, PNH, MDS AML
Immunodificiencies (drug/viral) ALL
Immune suppression: previous organ transplant
- Siblings of children with leukemia, especially among identical twins
Risk factors
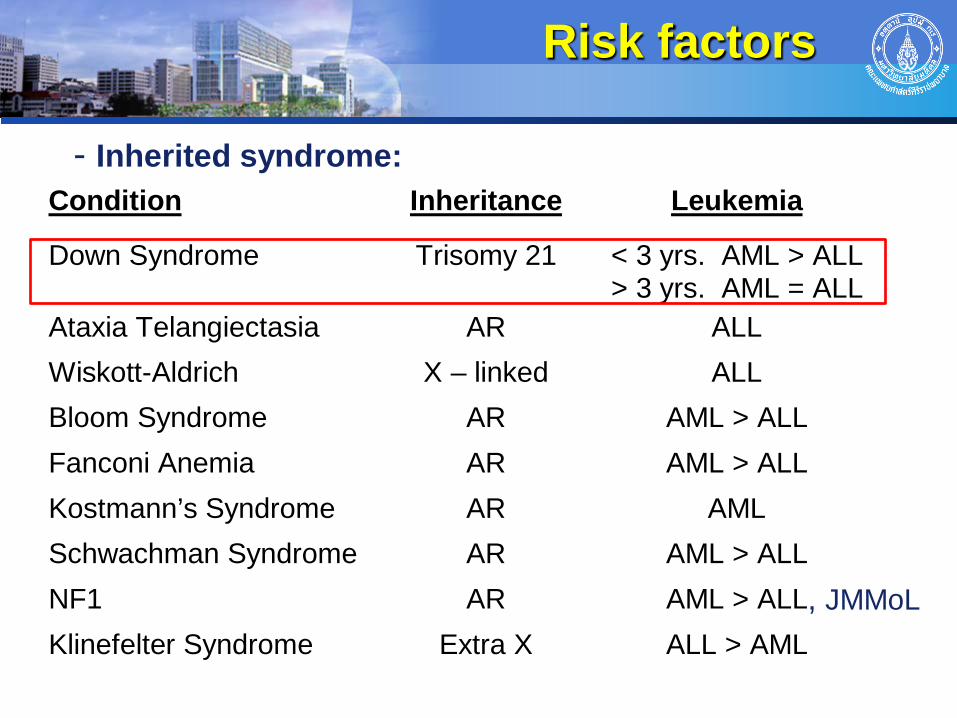
Condition Inheritance Leukemia
Down Syndrome
Trisomy 21
< 3 yrs. AML > ALL > 3 yrs. AML = ALL
Ataxia Telangiectasia AR ALL Wiskott-Aldrich X – linked ALL Bloom Syndrome AR AML > ALL Fanconi Anemia AR AML > ALL Kostmann’s Syndrome AR AML Schwachman Syndrome AR AML > ALL NF1 AR AML > ALL Klinefelter Syndrome Extra X ALL > AML
- Inherited syndrome:
, JMMoL
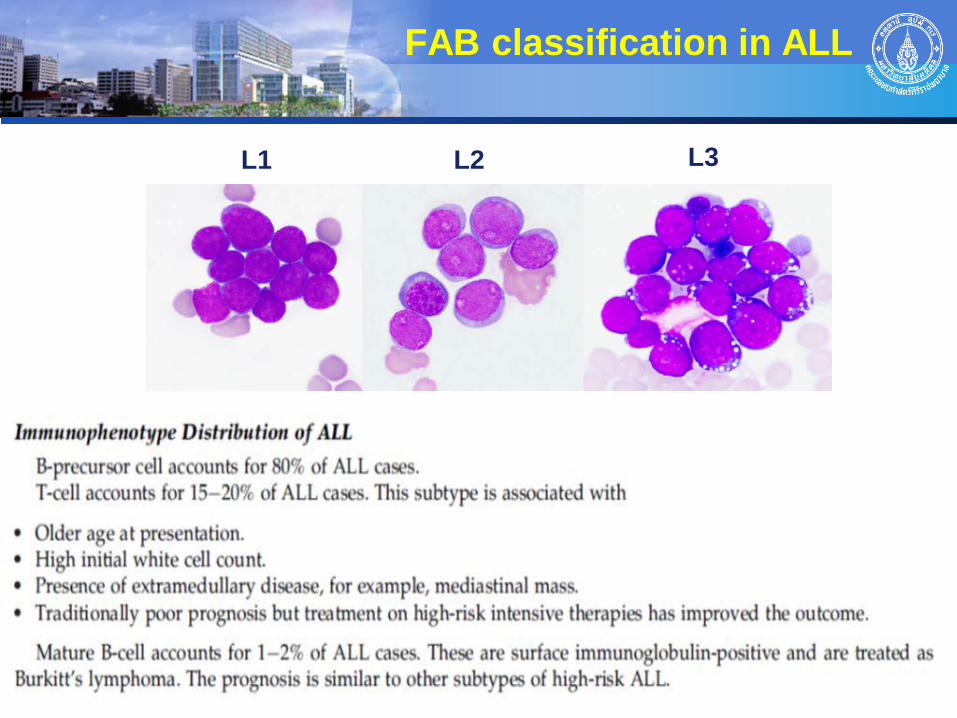
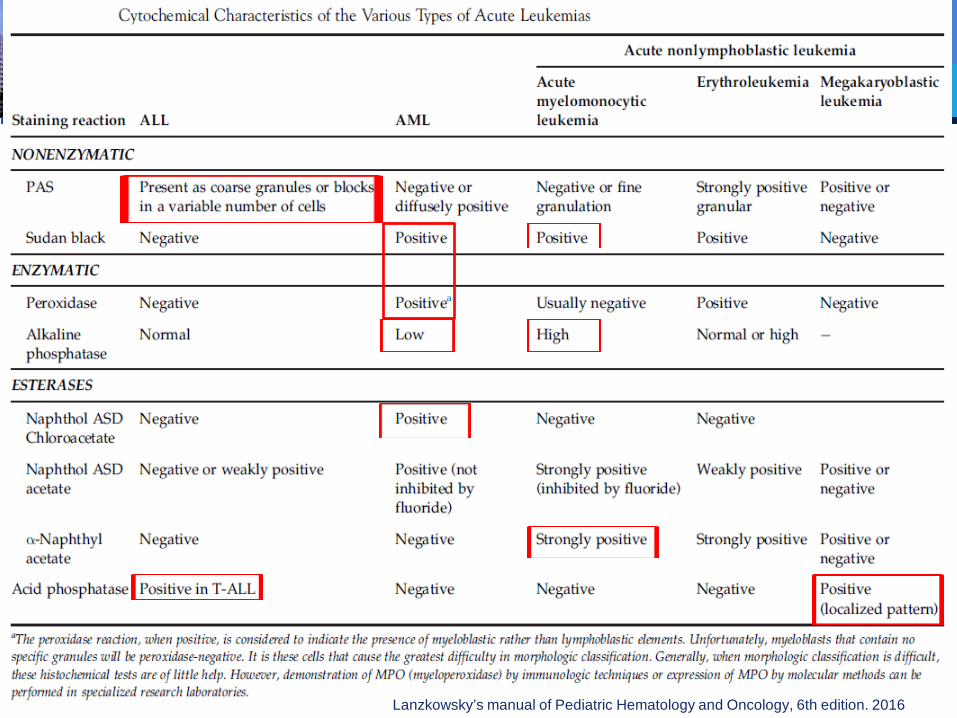
FAB classification in ALL
L1 L2 L3
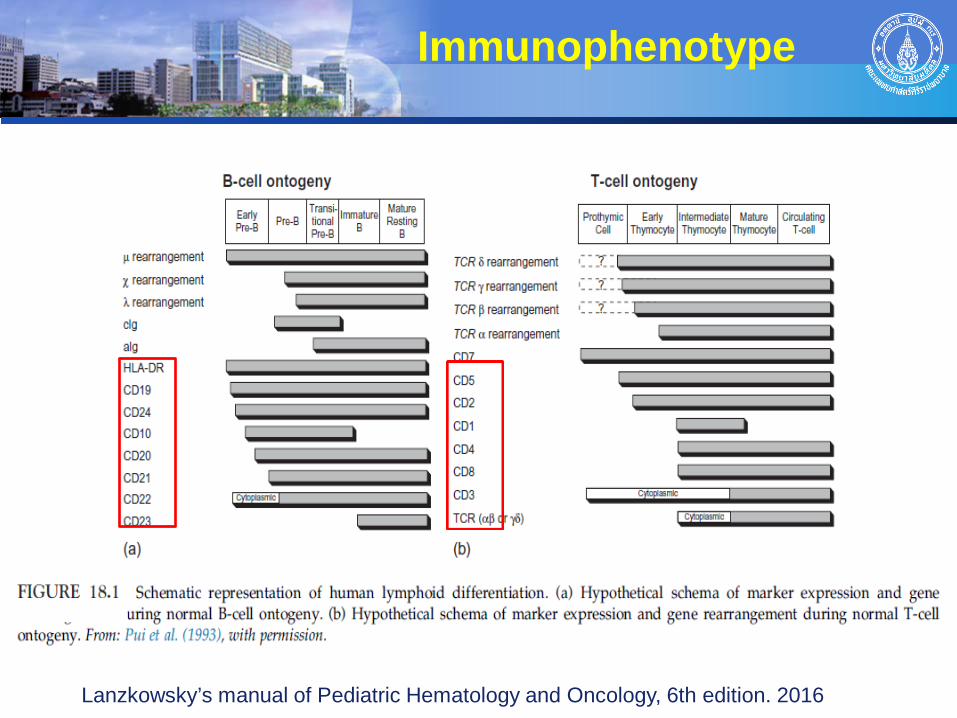
Immunophenotype
Lanzkowsky’s manual of Pediatric Hematology and Oncology, 6th edition. 2016
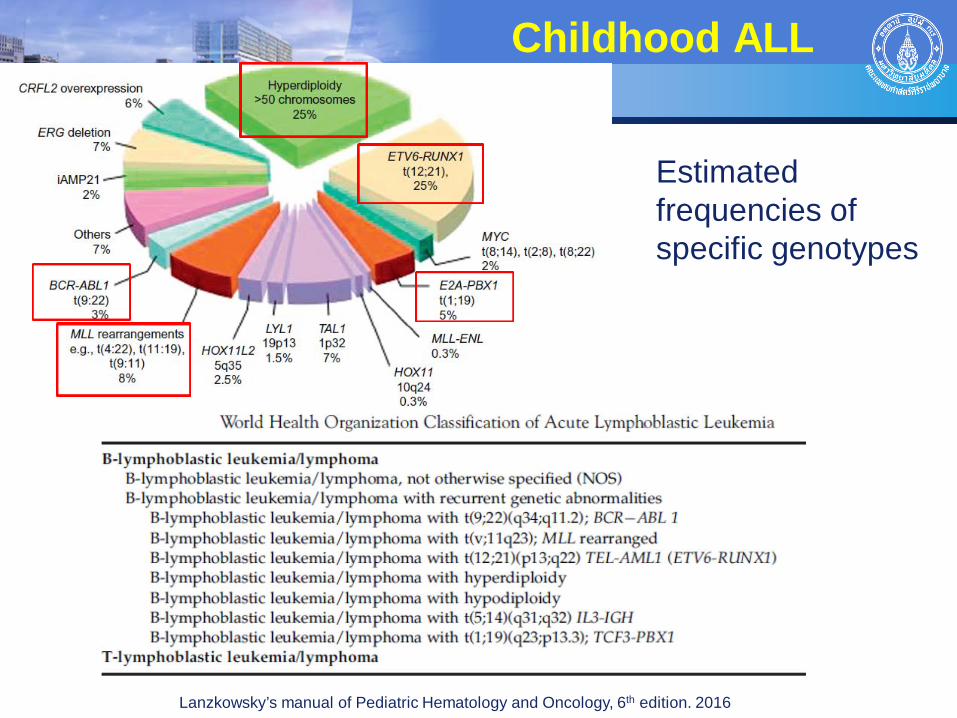
Childhood ALL
Lanzkowsky’s manual of Pediatric Hematology and Oncology, 6th edition. 2016
Estimated frequencies of specific genotypes
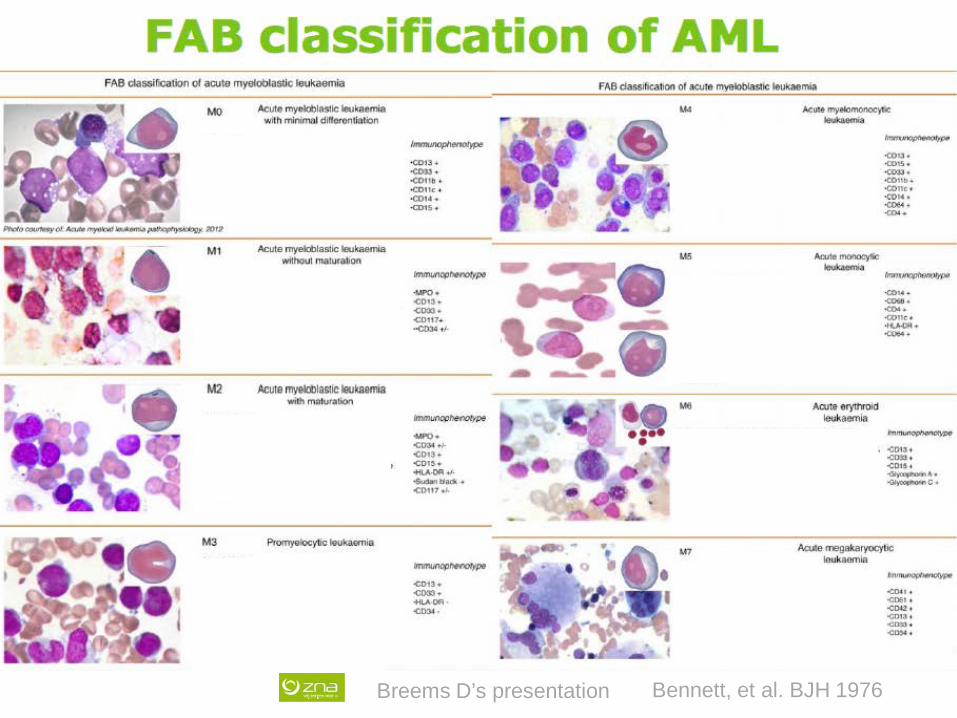
Bennett, et al. BJH 1976 Breems D’s presentation
Breems D’s presentation,
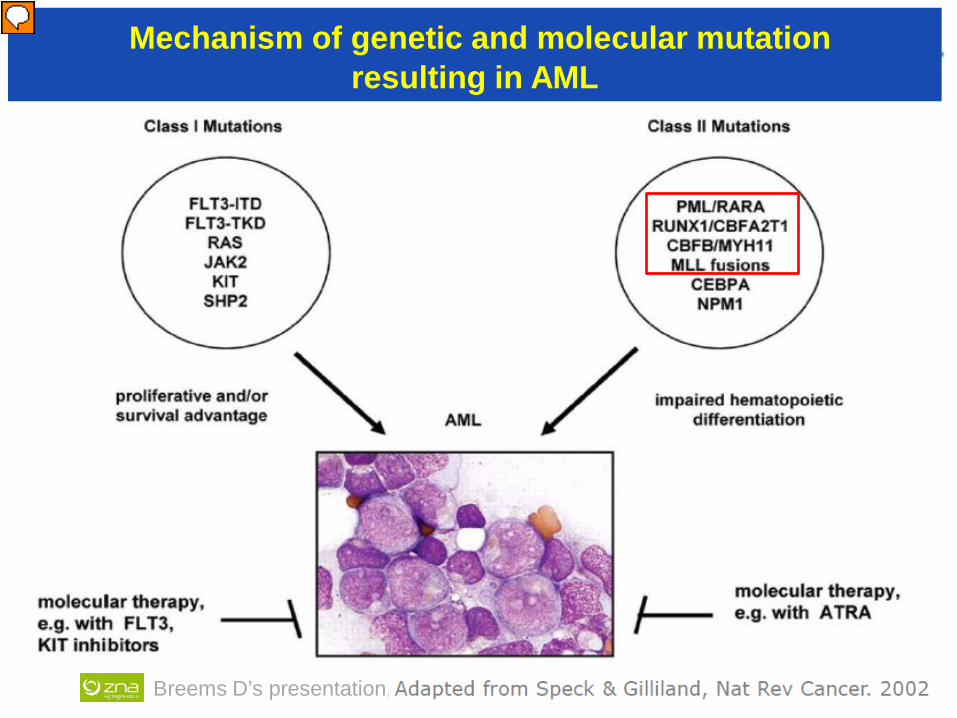
Mechanism of genetic and molecular mutation resulting in AML
Presenter
Presentation Notes
ผู้ป่วยเด็กโรค AML มักจะตรวจพบ recurrent cytogenetic abnormalities ข้อ 1.1-1.4 ประมาณร้อยละ 50 ของจำนวนผู้ป่วยทั้งหมด
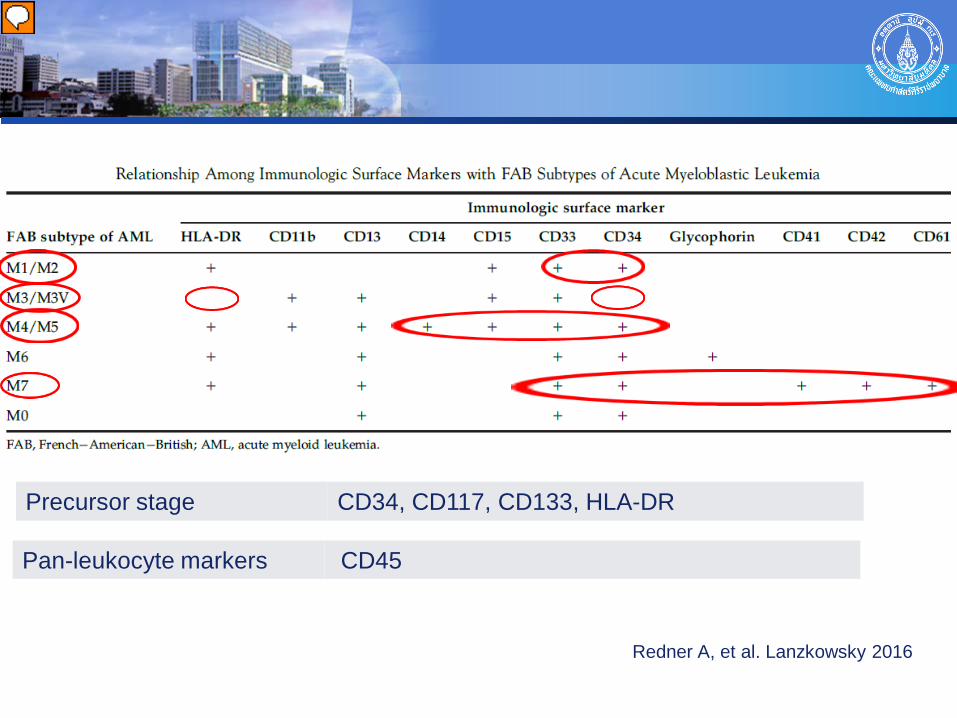
Redner A, et al. Lanzkowsky 2016
Precursor stage CD34, CD117, CD133, HLA-DR
Pan-leukocyte markers CD45
Presenter
Presentation Notes
The predictive value of HLA-DR and CD34 in the diagnosis of four distinct genetic entities of AML patients with t(15;17), t(8;21), inv(16), and abn(11q23).
Lanzkowsky’s manual of Pediatric Hematology and Oncology, 6th edition. 2016
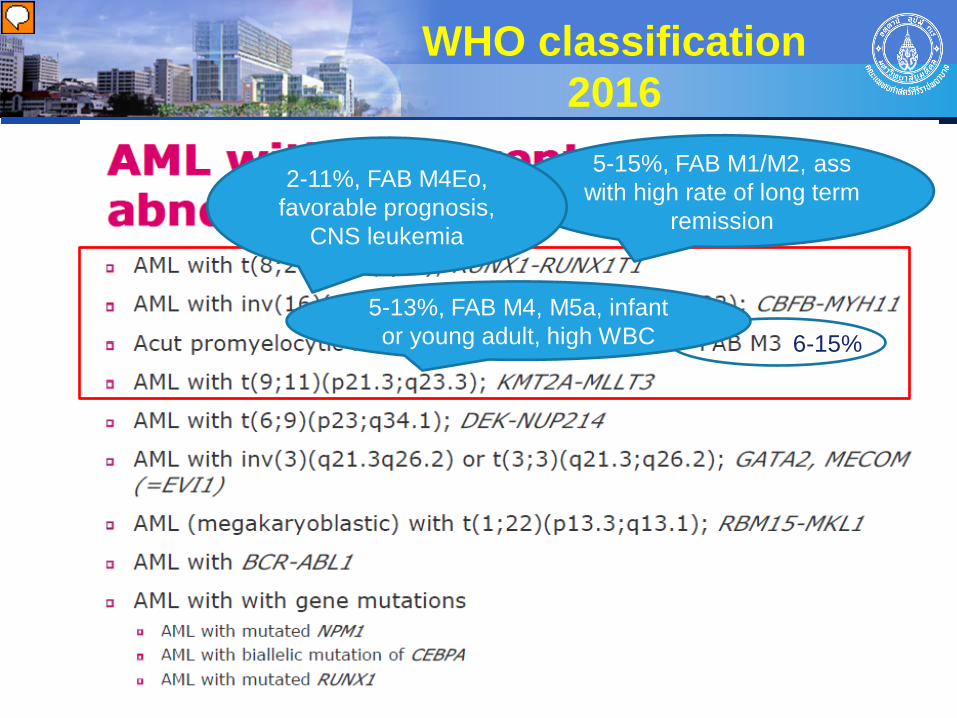
WHO classification 2016
5-15%, FAB M1/M2, ass with high rate of long term
remission
2-11%, FAB M4Eo, favorable prognosis,
CNS leukemia
5-13%, FAB M4, M5a, infant or young adult, high WBC 6-15%
Presenter
Presentation Notes
ผู้ป่วยเด็กโรค AML มักจะตรวจพบ recurrent cytogenetic abnormalities ข้อ 1-4 ประมาณร้อยละ 50 ของจำนวนผู้ป่วยทั้งหมด FAB M3 coagulopathy, ATRA responsiveness CBF-AML = core binding factor AML; t(8;21)(q22;q22), inv(16)(p13.1q22)
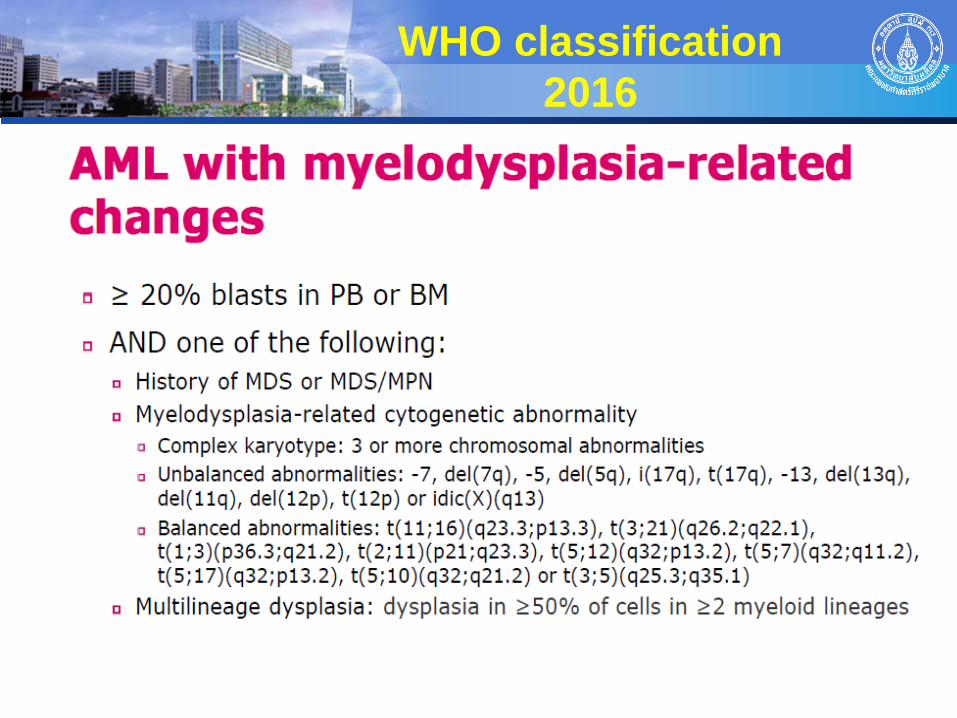
WHO classification 2016
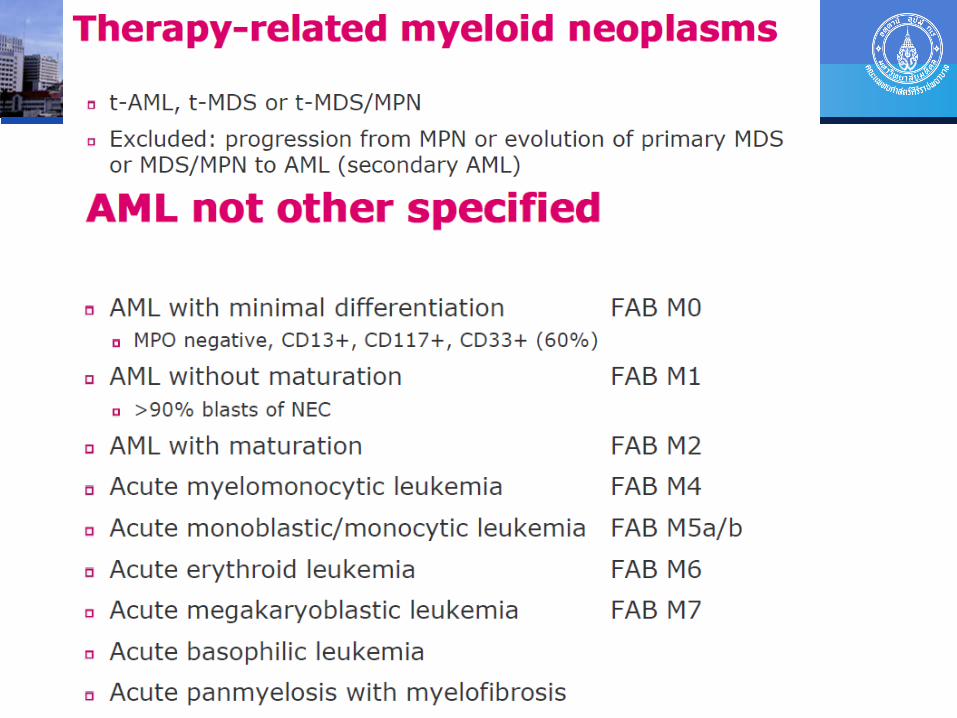
WHO classification 2016
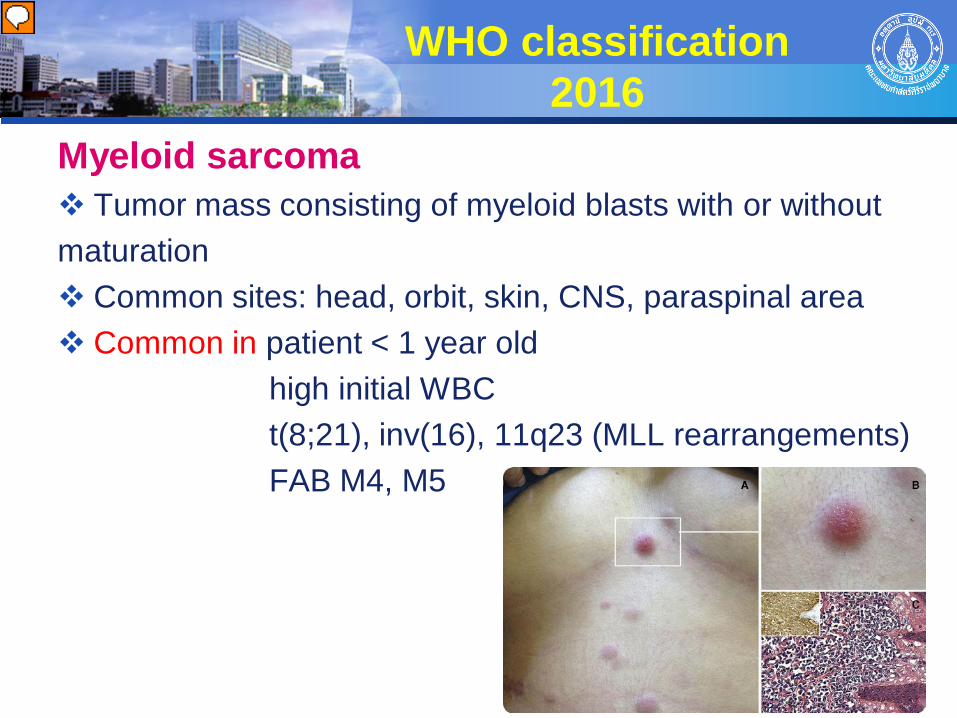
Myeloid sarcoma Tumor mass consisting of myeloid blasts with or without maturation Common sites: head, orbit, skin, CNS, paraspinal area Common in patient < 1 year old high initial WBC t(8;21), inv(16), 11q23 (MLL rearrangements) FAB M4, M5
Presenter
Presentation Notes
extramedullary myeloid tumor หรือ chloroma หรือ myeloid sarcomas) โดยพบบ่อยที่บริเวณศีรษะและเบ้าตา อาจมีก้อนที่กดเบียดไขสันหลัง เหงือกบวม (gingival hypertrophy) หรือ พบก้อนที่ผิวหนัง (leukemia cutis) ได้ โดยพบได้บ่อยในผู้ป่วยเด็กเล็กอายุต่ำกว่า 1 ปี ผู้ป่วยที่มีจำนวนเม็ดเลือดขาวสูงเมื่อแรกวินิจฉัย ผู้ป่วยที่มี t(8;21), inv(16), 11q23 (MLL rearrangements) ผู้ป่วยที่จัดอยู่ใน French-American-British (FAB) classification ชนิด M4 (acute myelomonocytic leukemia) หรือ M5 (acute monoblastic/monocytic leukemia)
Myeloid proliferations related to Down syndrome
Transient abnormal myelopoiesis (TAM)
- Association with Trisomy 21, Mosaicism may be present - Clonal expansion of myeloblasts, Mainly GATA1 gene mutation - Usually occur in first few days of life, 4-10% occur within 1 yr - Indistinguishable from congenital AML - Majority of patients have spontaneous regression in 1-3 months - Some have severe life-threatening symptoms exchange transfusion and/or low-dose cytarabine - 20-30 % of pts develop AML in 2-4 yrs
WHO classification 2016
Presenter
Presentation Notes
ผู้ป่วยที่ใช้เวลานานในการหายได้เองจาก TAM หรือมีการตรวจพบความผิดปกติทาง cytogenetic อื่นๆนอกเหนือ trisomy 21 จะเพิ่มความเสี่ยงในการเกิดโรค AML ตามมา
WHO classification 2016
Myeloid proliferations related to Down syndrome Myeloid leukemia associated with Down syndrome
- 10-20 times more likely to develop leukemia
- For first 3 yrs : AML > ALL
- MDS prodrome frequent
- M7 subtype ~ 500 times more common
- Myelofibrosis is common in M7
- Superior outcome compare to non-DS AML
- Patients > 4 years old had a significantly worse EFS
Presenter
Presentation Notes
- Superior outcome comepare to non-DS AML because increasedsensitivity of DS myeloblasts to cytarabine due to a mutation in GATA1, a hematopoetic transcription factor - patients >4 years had a significantly worse EFS of approximately 33%. A possible explanation is that patients .4 years old with DS-ML often lack GATA1 mutations, with the risk of relapse more similar to sporadic AML.
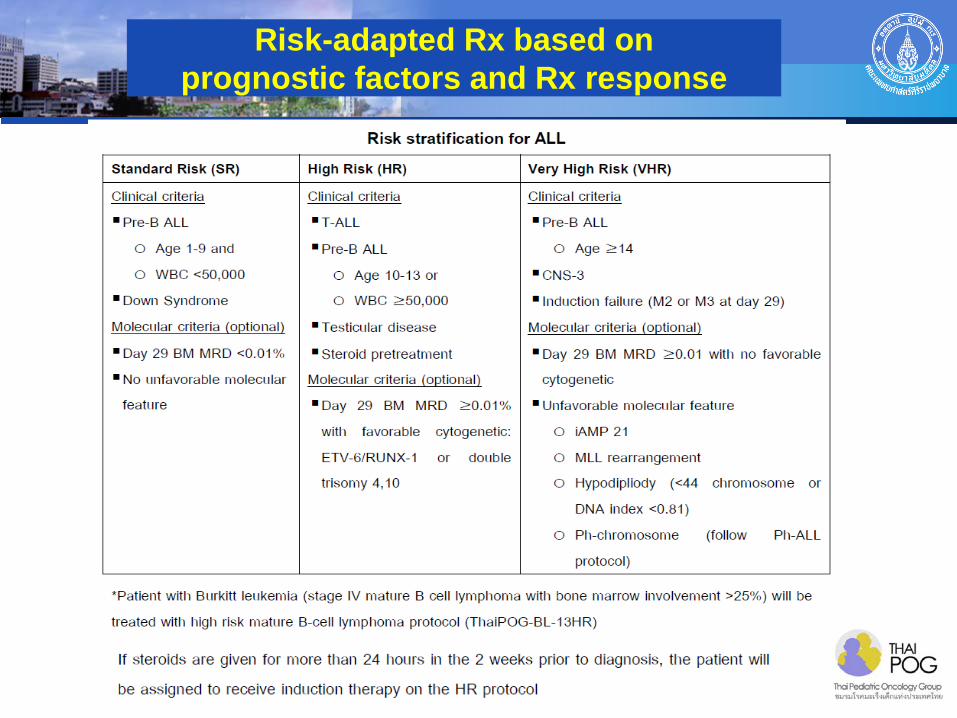
Risk-adapted Rx based on prognostic factors and Rx response
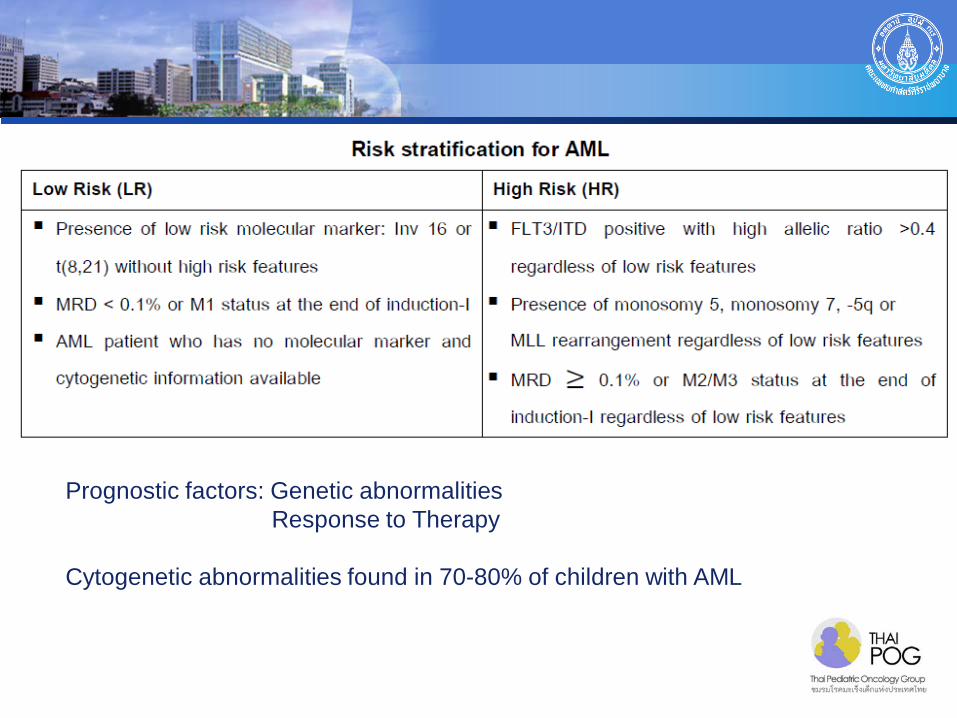
Prognostic factors: Genetic abnormalities Response to Therapy Cytogenetic abnormalities found in 70-80% of children with AML
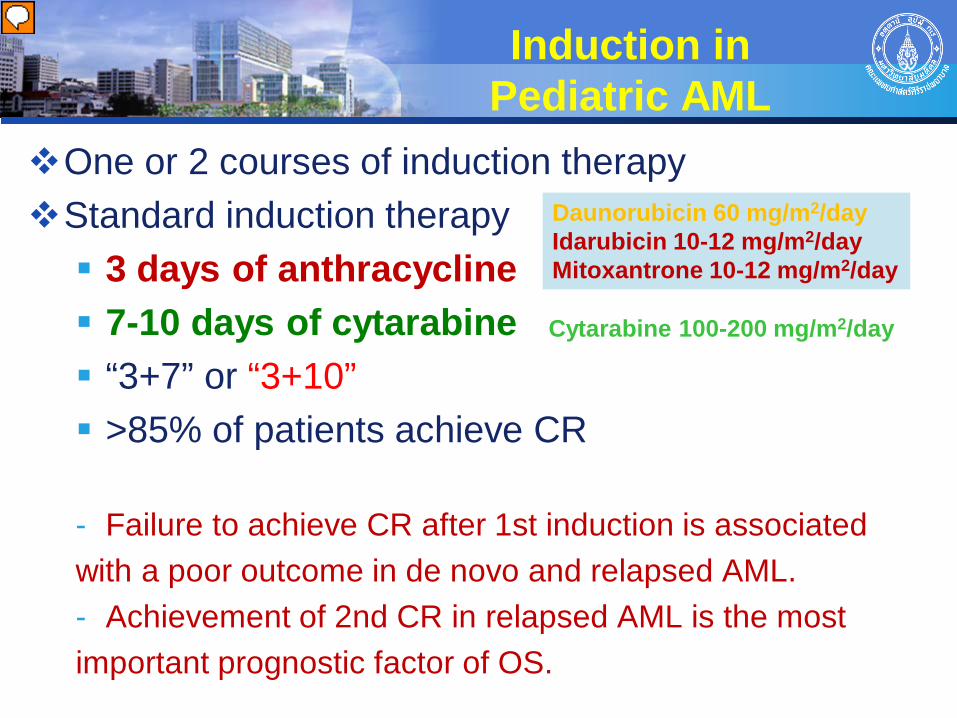
Induction in Pediatric AML
One or 2 courses of induction therapy Standard induction therapy 3 days of anthracycline 7-10 days of cytarabine “3+7” or “3+10” >85% of patients achieve CR - Failure to achieve CR after 1st induction is associated with a poor outcome in de novo and relapsed AML. - Achievement of 2nd CR in relapsed AML is the most important prognostic factor of OS.
Daunorubicin 60 mg/m2/day Idarubicin 10-12 mg/m2/day Mitoxantrone 10-12 mg/m2/day
Cytarabine 100-200 mg/m2/day
Presenter
Presentation Notes
ThaiPOG: Ara-C + Ida
CNS leukemia
5-10% of pediatric AML: CNS involvement at diagnosis and at relapse
Factors Associated with CNS disease - Younger age < 2 years - Hyperleukocytosis (>100,000/cumm) - Monocytic leukemia (FAB M4 or M5) - APL with PML/RARA in relapse - Certain molecular/cytogenetic findings (eg, FLT3-ITD; AML with inv(16) or chrom 11 abnormalities; complex karyotypes) - Expression of CD56 on the surface of blast cells - Elevated LDH Not affect OS, although increased incidence of isolated
CNS relapse
CNS Therapy
No prospective studies comparing the use of IT chemotherapy and cranial radiation in patients with CNS involvement
In general, triple IT chemotherapy is preferred in patients with CNS involvement without neurological deficits
Radiation therapy may be considered in CNS involvement with focal neurological deficits Tumor mass impinges on important structure such as
spinal cord Failure to respond to IT chemotherapy (CNS +ve after 4 x IT-chemotherapy)
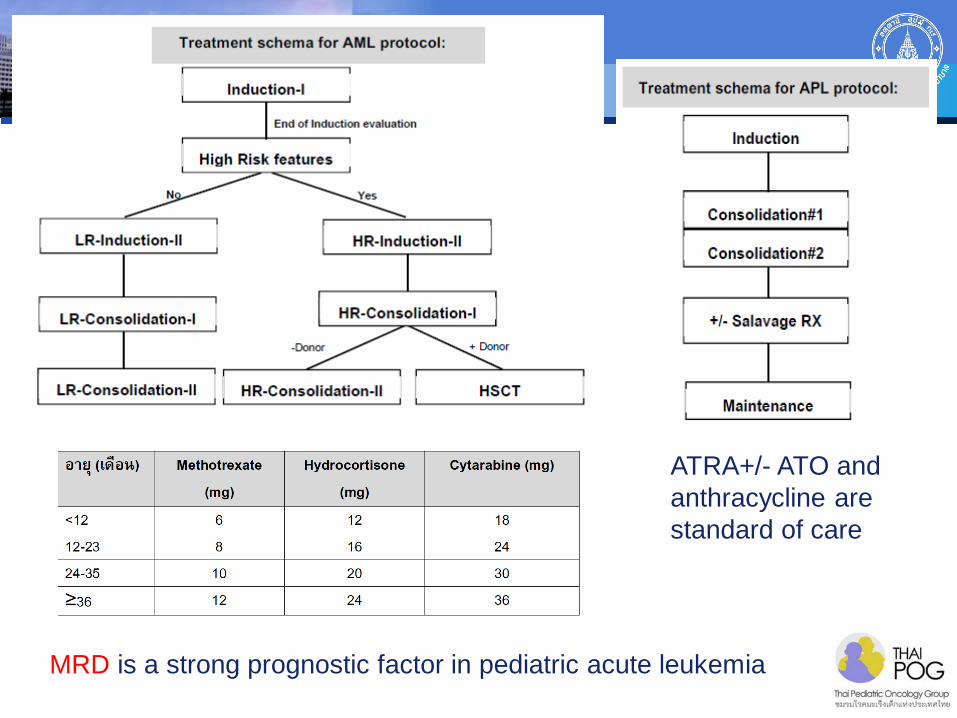
MRD is a strong prognostic factor in pediatric acute leukemia
ATRA+/- ATO and anthracycline are standard of care
Prognosis of APL
Poor prognosis if initial white count ( > 10,000 cumm) platelet count ( < 40,000 cumm) PLZF-RARa (not respond to ATO and ATRA)
FLT3-ITD or additional cytogenetic not significantly related to adverse outcome.
De Botton S, et al. British journal of haematology. 2000;111(3):801-6.
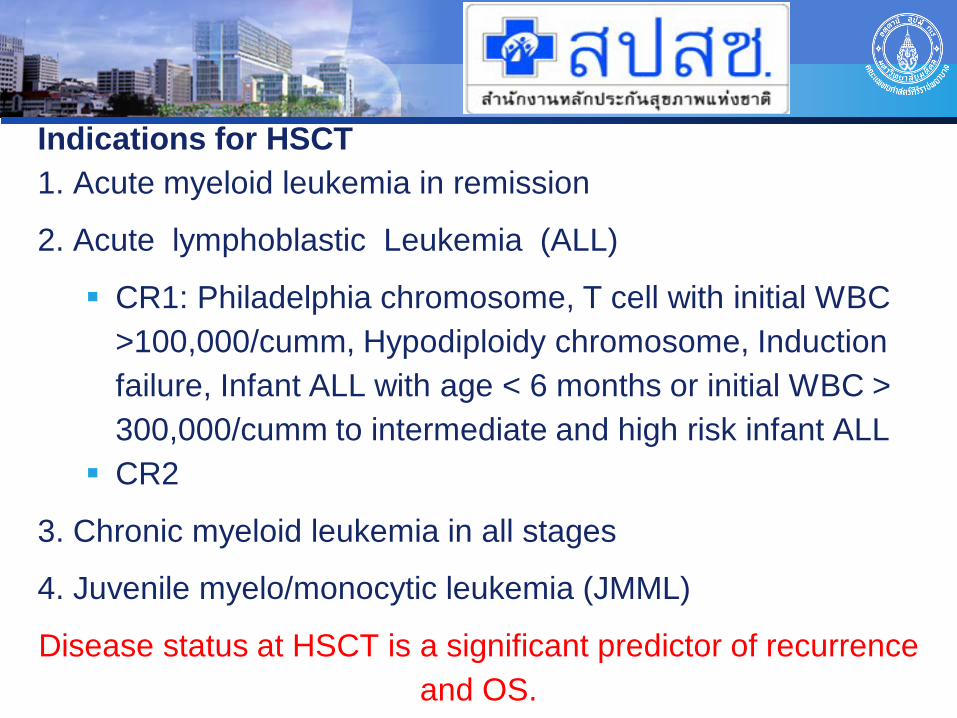
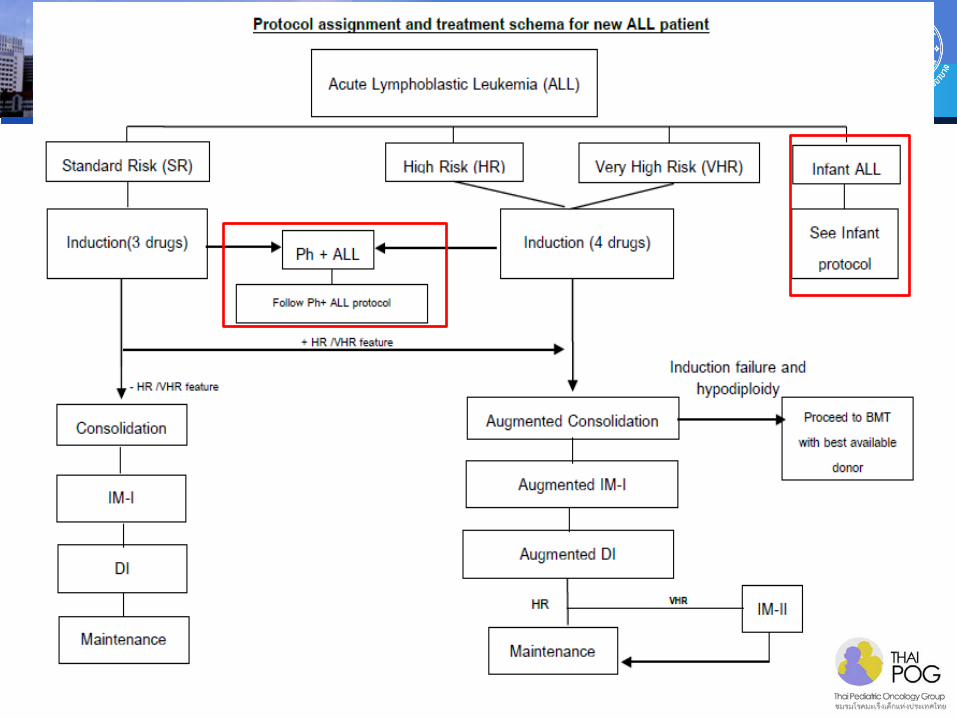
Indications for HSCT 1. Acute myeloid leukemia in remission
2. Acute lymphoblastic Leukemia (ALL)
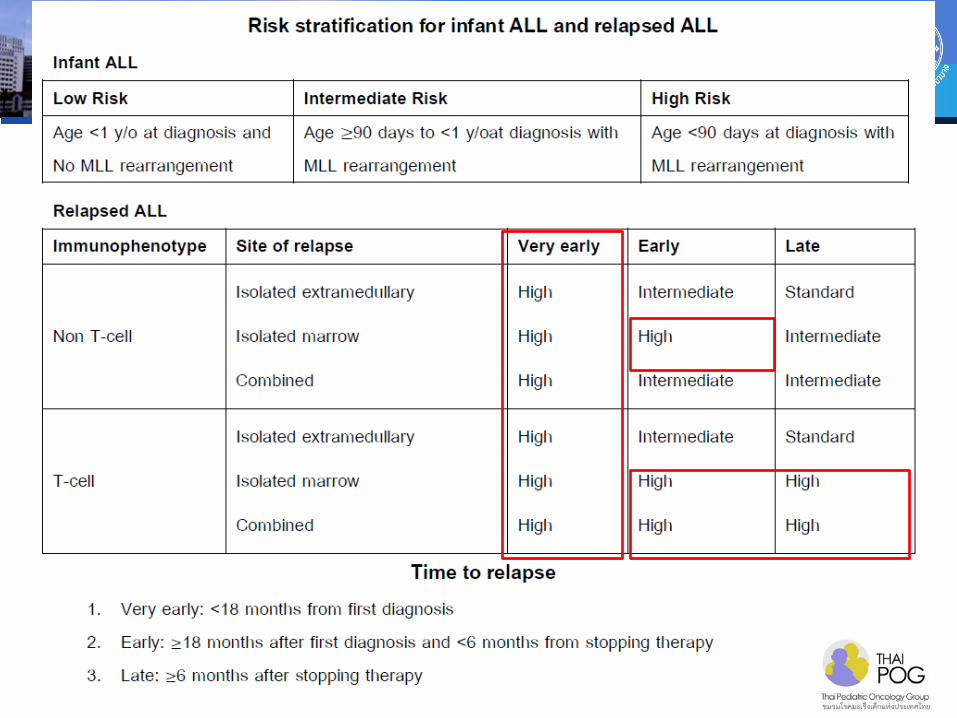
CR1: Philadelphia chromosome, T cell with initial WBC >100,000/cumm, Hypodiploidy chromosome, Induction failure, Infant ALL with age < 6 months or initial WBC > 300,000/cumm to intermediate and high risk infant ALL
CR2
3. Chronic myeloid leukemia in all stages
4. Juvenile myelo/monocytic leukemia (JMML)
Disease status at HSCT is a significant predictor of recurrence and OS.
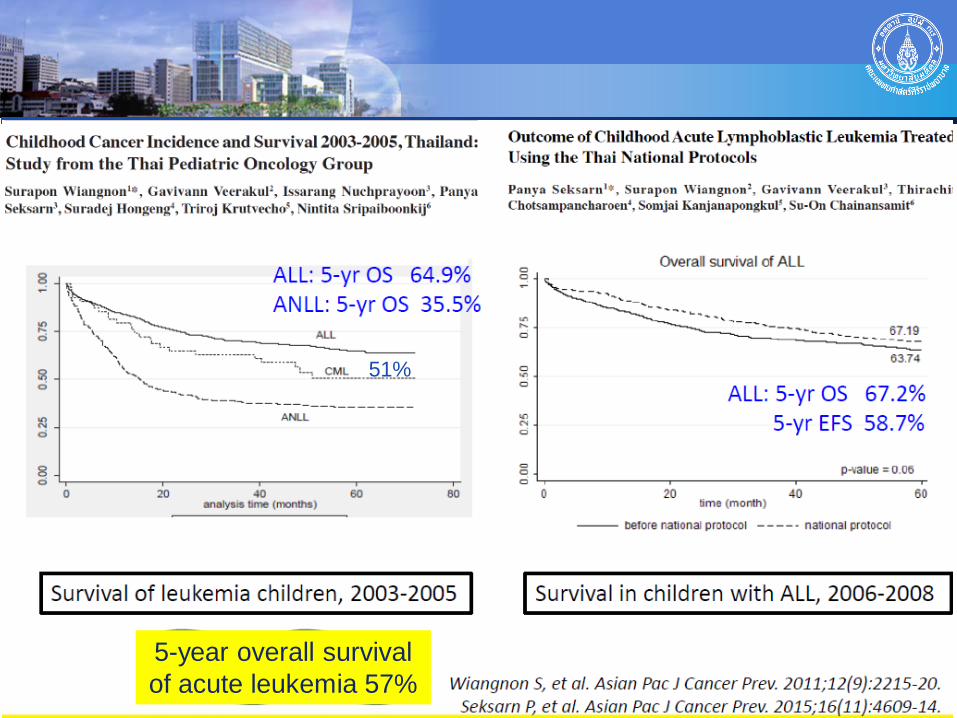
5-year overall survival of acute leukemia 57%
51%
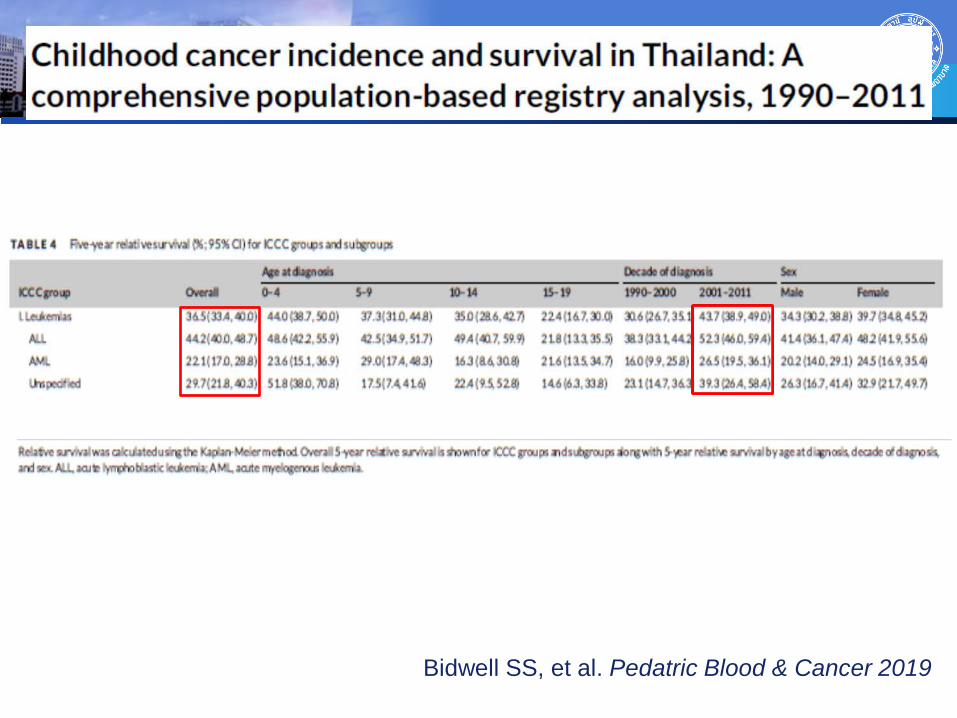
Bidwell SS, et al. Pedatric Blood & Cancer 2019
Summary
Improvements in survival rates of pediatric leukemia
- Defining risk stratification based on cytogenetic and
molecular markers and response to therapy
- Optimizing of chemotherapy regimens to reduce toxicity for
patients who can be cured with less intensity and intensify
therapy for patients who remain at high risk of relapse
- Monitoring response to therapy using MRD
- Better salvage options including HSCT
- Good supportive care
Thank you for your attention
Related Documents