Child ps y chiatry and DSM-5 Dr. Natalie Grizenko Associate Professor, McGill University Medical Director – Child and Adolescent Psychiatry at the Douglas Mental Health University Institute

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Child psychiatry and DSM-5
Dr. Natalie Grizenko Associate Professor, McGill University
Medical Director – Child and Adolescent Psychiatry at the Douglas Mental Health University Institute

Child psychiatry and DSM-5
Diagnostic criteria are intended to summarize signs and symptoms that point to an underlying disorder with characteristic:
– developmental history
– biological and environmental risk factors
– neuropsychological and physiological correlates
– clinical course

Child psychiatry and DSM-5
Interesting that DSM-V looks at pathology developmentally, across age groups
e.g.
Reactive Attachment Disorder – under Trauma and Stress-Related Disorder Separation Anxiety – under Anxiety Disorders

Child psychiatry and DSM-5
DSM-IV Disorders first diagnosed in infancy, childhood and adolescence 1) Mental Retardation 2) Learning Disorders 3) Motor Skills Disorders 4) Communication Disorders 5) PDD 6) ADHD 7) Tourette’s and Tics 8) Conduct Disorder 9) ODD
DSM-5
Neurodevelopmental Disorders Disruptive, Impulse-Control and Conduct Disorders

Child psychiatry and DSM-5 DSM-IV
Disorders first diagnosed in infancy, childhood and adolescence 10) Elimination Disorders (enuresis, encopresis) 11) Separation anxiety disorder 12) Selective mutism 13) Reactive Attachment Disorder
DSMDSM-5
Elimination Disorders
Anxiety Disorders Trauma and Stressor Related Disorder
New under Depressive Disorders
- Disruptive Mood Dysregulation Disorder

Intellectual Disability in DSM-5
• Term « mental retardation » replaced by « intellectual disabilities »;
• defined by functioning in conceptual domain, (reasoning, problem solving, etc.), social domain and practical (self-care) domain and not IQ numbers;
• 4 levels: mild, moderate, severe, profound.
Intellectual Disability in DSM-5
DSM-IV: mild MR: IQ 50-55 to 70
DSM-5: . difficulties in learning (reading, math, writing) . immature in social interactions, poor social judgement and assessment of risk
. language more concrete
. difficulty regulating emotions and behaviour
. need support in complex daily living tasks (i.e. grocery shopping, child-care, banking)

Intellectual Disability in DSM-5
DSM-IV: moderate MR: 35-40 to 50-55.
DSM-5: moderate: understanding time occurs slowly, training needed for hygiene, dressing and household tasks, simple spoken language, poor interpretation of social cues.
Problems with DSM-5 – probably reliability will decrease.

Communication Disorder in DSM-5
DSM-IV: Distinction between expressive and receptive language disorder.
DSM-5: Language Disorder encompasses expressive and receptive dysfunction.
Learning Disorders in DSM-5 DSM-IV - Reading Disorder
- Mathematics Disorder
- Disorder of Written Expression
DSM-5 - Specific Learning Disorders with impairment in:
• Reading
• Mathematics
• Written expression
- min 6m despite provision of intervention
- Impairing at school or work
- not due to intellectual disability or other psychopathology

ADHD in DSM-5
DSM-IV DSMDSM-5
• 6/9 inattention and/or hyperactivity-impulsivity symptoms
• All child examples e.g.
on the go as if driven by a motor
• 6/9 inattention and/or hyperactivity-impulsivity symptoms
• 5/9 if > 17
• Adolescent/adult examples added
e.g. uncomfortable being still for extended periods as in a restaurant or meeting
ADHD in DSM-5 DSM-IV
• On s
• Onset < 7
• Symptoms do not occur exclusively during course of schizophrenia, PDD or other psychotic disorders or better explained by another mental disorder (e.g. mood, anxiety, dissociative, substance abuse, personality disorders)
• Min 2 settings, interfers with functioning
DSM-5 • Onset < 12
• ASD not excluded
• Same

ADHD in DSM-5
DSM-IV
• 3 types - combined - predominantly
inattentive - predominantly
hyperactive-impulsive
DSM-5
• Deletion of types (not
stable over time) instead «current presentation»
• Severity: mild, moderate,
severe

ADHD in DSM-5 - Inattention DSM-IV
1. Doesn’t pay close attention to
details, careless mistakes in homeworks
2. Difficulty sustaining attention
3. Doesn’t seem to listen when spoken to directly
4. Doesn’t follow instructions 5. Difficulty organizing activities
6. Avoid tasks that require sustained
attention (e.g. homework) 7. Often loses things (e.g. pencils) 8. Easily distracted 9. Forgetful 10.1.1.1
DSM-5 1. E.g. misses details, work is
inaccurate
2. E.g. difficulty staying focused during lectures
3. E.g. mind seems elsewhere
4. Easily side-tracked 5. E.g. Messy disorganized work, fails
to meet deadlines 6. E.g. dislikes completing forms,
reviewing lengthy papers 7. E.g. loses keys, mobile phones 8. E.g. may have unrelated thoughts 9. E.G. forgets to pay bills, keep
appointments
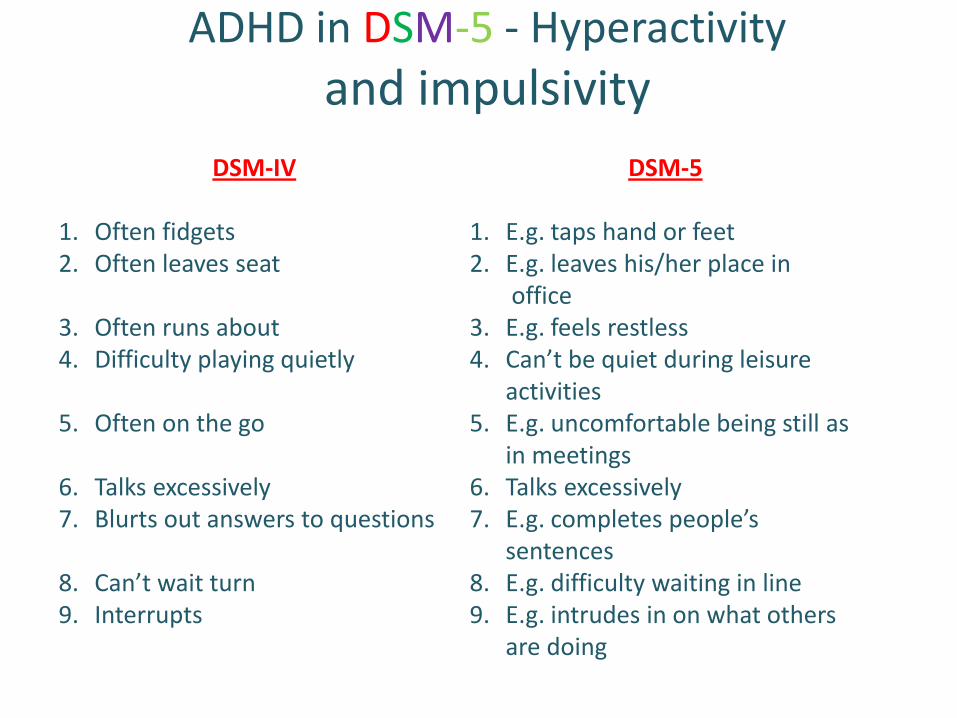
ADHD in DSM-5 - Hyperactivity
and impulsivity
DSM-IV
1. Often fidgets 2. Often leaves seat
3. Often runs about 4. Difficulty playing quietly
5. Often on the go
6. Talks excessively 7. Blurts out answers to questions
8. Can’t wait turn 9. Interrupts
DSM-5
1. E.g. taps hand or feet 2. E.g. leaves his/her place in office 3. E.g. feels restless 4. Can’t be quiet during leisure
activities 5. E.g. uncomfortable being still as
in meetings 6. Talks excessively 7. E.g. completes people’s
sentences 8. E.g. difficulty waiting in line 9. E.g. intrudes in on what others
are doing

ADHD in DSM-5
Intent: maintain core diagnostic criteria while improving applicability across life span (onset < 12 to avoid recall difficulties in adults, out of 5 vs 6 symptoms for > 17)
Potential consequences:
- Increase in diagnosis, especially for high school, college and university students and adults
Problem: Adults with ADHD have numerous comorbidities - Important to understand primary
diagnosis and not diagnose everyone with ADHD

Autism Spectrum Disorders in DSM-5
DSM-IV PDD
1. Autism Disorder
2. Rett’s Disorder
- N dev until 5m, then head circonference and deterioration - F
3. Childhood Disintegrative Disorder - N dev for first 2 years followed by deterioration
4. Asperger’s - N cognition and language development
DSM-5 ASD

Autism Spectrum Disorders in DSM-5
DSM-IV
Autistic Disorder
Total 6 items (min 2 from A + 1 from B+C)
A) Impaired social interaction 1. non verbal behaviour e.g. lack eye contact/facial expression
2. lack of social emotional reciprocity
3. lack of interest sharing 4. deficits in peer relations B) Impaired communication
1. delayed/no language 2. poor conversation 3. stereotyped language 4. lack of imaginative play
DSM-5 AAutism Spectrum Disorder
A) Deficits in social communication and interactions 1. deficits in non verbal
communication and behaviour 2. deficits in social emotional
reciprocity - includes interest sharing, abnormal social approach
3. deficits in peer relations - includes poor imaginative play and lack of interest in peers

Autism Spectrum Disorders in DSM-5
DSM-IV Autistic Disorder
C) Restricted repetitive stereotypic
behaviour and interests 1. stereotypic movement (e.g. flapping
2. inflexible routines 3. fixed interests 4. persistent preoccupations with
parts of objects D) Present before age 3
DSM-5 Autism Spectrum Disorder
B) Restrictive repetitive pattern of
behaviour, interests or activities (min 2) 1. stereotypic/repetitive
movements or speech 2. insistance on sameness 3. fixated interests 4. hyper or hypo sensory reactivity C) Present in early development
D) Symptoms impairing Not 20 to - intellectual disability C) (ASD + ID can coexist) D)(ASD(A(ASDS(ASDDSDASD (ASD + ID ca

Autism Spectrum Disorders in DSM-5
General comments :
1. Aspergers no longer a separate diagnosis - it was more acceptable to patients than autism;
2. Grouping together very different patients:
- different entities
- difficult for research
- different prognostic implications

Oppositional Defiant Disorder in DSM-5
• Grouped under disruptive, impulse-control and conduct disorders with APS, pyromania, kleptomania and intermittent explosive disorder
• Same criteria as in DSM-IV, but grouped in:
• Anger/Irritable Mood;
• Argumentative/Defiant Behaviour;
• Vindictiveness.
• Can occur with CD (no longer exclusion criteria)
• Cannot occur with disruptive mood dysregulation

Conduct Disorder in DSM-5
• Similar 15 criteria: (3/15 in past 12m and 1/15 in past 6m)
• Symptoms grouped in
A) aggression to people and animals
B) destruction of property
C) deceitfulness or theft
D) serious violations of rules (e.g. staying out at night without permission before age 13, running away from home O/N, truant from school before age 13)
• Childhood onset before age 10, adolescent onset after age 10

Conduct Disorder in DSM-5
New specifier: with limited prosocial emotions
- need min. 2/3 characteristics over 12m
• lack of remorse or guilt
• callous – lack of empathy
• unconcerned about performance (also blame others for their poor performance)
• shallow or deficient affect (insincere, superficial)
Current severity: mild, moderate, severe
Comment: Specifier is imporant because it predicts outcome
- back to DSM-III where they had undersocialized subtypes

Separation Anxiety Disorder in DSM-5
Goal: to facilitate the application of the diagnosis to adults • Moved from disorders usually arising in childhood to
Anxiety Disorders
• Text was modified to be more applicable to adults e.g. refusal to go to school or work because of fear of separation
• Lasts at least 4w. (DSM-IV and DSM-5) in children and 6m and adults (DSM-5)

Selective Mutism in DSM-5
- Same criteria, but also moved under Anxiety Disorders to facilitate application of the diagnosis to adults.
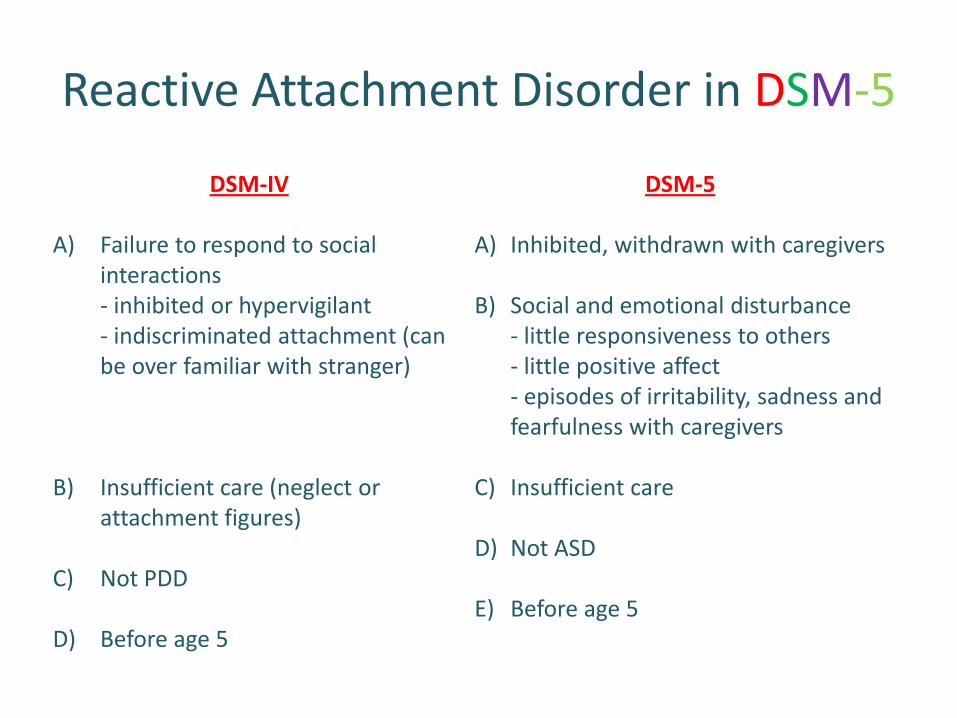
Reactive Attachment Disorder in DSM-5
DSM-IV
A) Failure to respond to social interactions - inhibited or hypervigilant - indiscriminated attachment (can be over familiar with stranger)
B) Insufficient care (neglect or attachment figures)
C) Not PDD
D) Before age 5
DSM-5
A) Inhibited, withdrawn with caregivers
B) Social and emotional disturbance - little responsiveness to others - little positive affect - episodes of irritability, sadness and fearfulness with caregivers
C) Insufficient care
D) Not ASD
E) Before age 5

Reactive Attachment Disorder in DSM-5
• Moved to trauma and stress related disorders
• Contrary to DSM-IV, there is no discussion of indiscriminated sociability with excessive familiarity with strangers
• More emphasis on inhibited, withdrawn behaviour and episodes of irritability, sadness and fearfulness
• Specifier – persistent if duration > 12m

Disruptive Mood Dysregulation Disorder in DSM-5
• New disorder
• US phenomenon: a 40 fold increase in the diagnosis of bipolar disorder in children (as young as 2 yrs of age)
• Bipolar disorder in children was argued erroneously to be chronic rather than episodic
• DMDD was introduced to change diagnostic practice by providing a diagnosis for chronically irritable children

Disruptive Mood Dysregulation Disorder in DSM-5
A) Severe recurrent temper outbursts out of proportion in intensity and duration to situation
B) Outburst inconsistent with developmental level
C) At least 3x/w
D) Mood between outbursts is irritable or angry
E) Duration 12m (with no symptom free period of >3m)
F) In 2/3 settings (home, school and with peers)
G) First diagnosis between ages 6-18
H) Symptoms start before age 10 (by history or observation)
I) No mania or hypomania
J) Not 20 to Depression, ASD, PTSD, separation anxiety, dysthymic
Can be comorbid with ADHD, CD. If ODD + DMDD give only Dx of DMDD.
Disruptive Mood Dysregulation Disorder in DSM-5
Potential issues
• Poor reliability in field trials
• Rarely occurs on its own. Almost always with ADHD, ODD or ASD
• Interesting to explore longitudinally the course of DMDD.

31
Thank you for your attention
Related Documents