NEW RESEARCH Child- and Family-Focused Cognitive- Behavioral Therapy for Pediatric Bipolar Disorder: A Randomized Clinical Trial Amy E. West, PhD, Sally M. Weinstein, PhD, Amy T. Peters, MA, Andrea C. Katz, MA, David B. Henry, PhD, Rick A. Cruz, MA, Mani N. Pavuluri, MD, PhD Objective: Previous studies have found that family-based psychosocial treatments are effective adjuncts to pharmacotherapy among adults and adolescents with bipolar disorder (BD). The objective of this study was to compare the efficacy of adjunctive child- and family-focused cognitive-behavioral therapy (CFF-CBT) to psychotherapy as usual (control) for mood symp- tom severity and global functioning in children with BD. Method: Sixty-nine youth, aged 7 to 13 years (mean ¼ 9.19, SD ¼ 1.61) with DSM-IV-TR bipolar I, II, or not otherwise specified (NOS) disorder were randomly assigned to CFF-CBT or control groups. Both treatments con- sisted of 12 weekly sessions followed by 6 monthly booster sessions delivered over a total of 9 months. Independent evaluators assessed participants at baseline, week 4, week 8, week 12 (posttreatment), and week 39 (6-month follow-up). Results: Participants in CFF-CBT atten- ded more sessions, were less likely to drop out, and reported greater satisfaction with treatment than controls. CFF-CBT demonstrated efficacy compared to the control treatment in reducing parent-reported mania at posttreatment and depression symptoms at posttreatment and follow-up. Global functioning did not differ at posttreatment but was higher among CFF-CBT participants at follow-up. Conclusion: CFF-CBT may be efficacious in reducing acute mood symptoms and improving long-term psychosocial functioning among children with BD. J. Am. Acad. Child Adolesc. Psychiatry, 2014;-(-):-–-. Key Words: pediatric bipolar disorder, cognitive-behavioral therapy, family-focused intervention, randomized clinical trial P ediatric bipolar disorder (PBD) describes bipolar spectrum illness among children and preadolescents. Affecting approxi- mately 1% to 2% of the population, 1 PBD is characterized by extreme episodic mood dys- regulation accompanied by symptoms (e.g., decreased need for sleep, hypersexuality, impul- sivity) that significantly impair multiple domains of functioning. PBD is differentiated from adult- onset bipolar disorder (BD) by increased rates of rapid cycling, mixed mood states, psychi- atric comorbidity, and developmentally-specific psychosocial impairment. 2,3 Compared to healthy peers, children with PBD demonstrate neurocognitive deficits, poor academic perfor- mance, 4,5 and disruptive school behavior. 6 Peer relationships are characterized by limited peer networks, peer victimization, and poor social skills. 7,8 Compared to families that are not affected by PBD, family functioning is often characterized by strained relationships, 8,9 low levels of cohesion, and increased conflict; 10-12 in addition, family stress and dysfunction in- crease with symptom levels. 13,14 The accumu- lation of psychosocial risk renders PBD a significant public health concern as evidenced by high rates of repeated hospitalization and suicide attempts. 15 In adulthood, people with BD demonstrate greater mental health care use, elevated rates of other health conditions, lower rates of graduation, and decreased career pro- ductivity. 15-17 Recent data from the World Health Organization indicate that BD is the fourth lead- ing cause of disability in youth ages 10 to 24 years worldwide. 18 Clinical guidance is available at the end of this article. Supplemental material cited in this article is available online. JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY VOLUME - NUMBER - - 2014 www.jaacap.org 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
NEW RESEARCH
JOURNAL
VOLUM
Child- and Family-Focused Cognitive-Behavioral Therapy for Pediatric BipolarDisorder: A Randomized Clinical Trial
Amy E. West, PhD, Sally M. Weinstein, PhD, Amy T. Peters, MA, Andrea C. Katz, MA,David B. Henry, PhD, Rick A. Cruz, MA, Mani N. Pavuluri, MD, PhD
Objective: Previous studies have found that family-based psychosocial treatments are effectiveadjuncts to pharmacotherapy among adults and adolescents with bipolar disorder (BD). Theobjective of this study was to compare the efficacy of adjunctive child- and family-focusedcognitive-behavioral therapy (CFF-CBT) to psychotherapy as usual (control) for mood symp-tom severity and global functioning in children with BD. Method: Sixty-nine youth, aged 7 to13 years (mean ¼ 9.19, SD ¼ 1.61) with DSM-IV-TR bipolar I, II, or not otherwise specified(NOS) disorder were randomly assigned to CFF-CBT or control groups. Both treatments con-sisted of 12 weekly sessions followed by 6 monthly booster sessions delivered over a total of9 months. Independent evaluators assessed participants at baseline, week 4, week 8, week 12(posttreatment), and week 39 (6-month follow-up). Results: Participants in CFF-CBT atten-ded more sessions, were less likely to drop out, and reported greater satisfaction with treatmentthan controls. CFF-CBT demonstrated efficacy compared to the control treatment in reducingparent-reported mania at posttreatment and depression symptoms at posttreatment andfollow-up. Global functioning did not differ at posttreatment but was higher among CFF-CBTparticipants at follow-up. Conclusion: CFF-CBT may be efficacious in reducing acute moodsymptoms and improving long-term psychosocial functioning among children with BD. J. Am.Acad. Child Adolesc. Psychiatry, 2014;-(-):-–-. Key Words: pediatric bipolar disorder,cognitive-behavioral therapy, family-focused intervention, randomized clinical trial
ediatric bipolar disorder (PBD) describesbipolar spectrum illness among children
P and preadolescents. Affecting approxi-mately 1% to 2% of the population,1 PBD ischaracterized by extreme episodic mood dys-regulation accompanied by symptoms (e.g.,decreased need for sleep, hypersexuality, impul-sivity) that significantly impair multiple domainsof functioning. PBD is differentiated from adult-onset bipolar disorder (BD) by increased ratesof rapid cycling, mixed mood states, psychi-atric comorbidity, and developmentally-specificpsychosocial impairment.2,3 Compared tohealthy peers, children with PBD demonstrate
Clinical guidance is available at the end of this article.
Supplemental material cited in this article is available online.
OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATR
E - NUMBER - - 2014
neurocognitive deficits, poor academic perfor-mance,4,5 and disruptive school behavior.6 Peerrelationships are characterized by limited peernetworks, peer victimization, and poor socialskills.7,8 Compared to families that are notaffected by PBD, family functioning is oftencharacterized by strained relationships,8,9 lowlevels of cohesion, and increased conflict;10-12
in addition, family stress and dysfunction in-crease with symptom levels.13,14 The accumu-lation of psychosocial risk renders PBD asignificant public health concern as evidencedby high rates of repeated hospitalization andsuicide attempts.15 In adulthood, people withBD demonstrate greater mental health care use,elevated rates of other health conditions, lowerrates of graduation, and decreased career pro-ductivity.15-17 Recent data from the World HealthOrganization indicate that BD is the fourth lead-ing cause of disability in youth ages 10 to 24 yearsworldwide.18
Y
www.jaacap.org 1
WEST et al.
Pharmacotherapy is the first-line treatment forPBD but is complicated by low response rates,poor tolerability,19 and inability to address thefull range of impairments associated with PBD.Thus, adjunctive psychosocial intervention isconsidered essential for effective treatment.20
Despite this, few psychosocial treatments foryouth with BD have been studied systematically.Adaptations of dialectical behavior therapy(DBT)21 and interpersonal and social rhythmtherapy (IPSRT)22 for adolescents with BD havebeen tested in pilot studies. However, only 2interventions have demonstrated efficacy inrandomized controlled trials (RCT): multi-familypsycho-education group psychotherapy (MF-PEP) for youth with BD or unipolar depressionin children aged 8 to 12 years,23 and family-focused treatment (FFT) for adolescents aged13 to 18 years.24 These treatments demonstratedeffects on mood severity in children23 anddepression relapse in adolescents,24 respectively.It is not yet known whether a treatment modelsuch as child- and family-focused cognitive-behavioral therapy (CFF-CBT), which morespecifically targets the unique symptoms andimpairments in childhood BD, will improveoutcomes compared to these other treatments.
CFF-CBT was developed to target the uniquedevelopmental needs of the PBD population ina comprehensive family-focused format. CFF-CBT integrates CBT with psychoeducation andcomplementary mindfulness-based and inter-personal/family therapy techniques tailored toaddress the range of therapeutic needs in fam-ilies affected by PBD. The components ofCFF-CBT are driven by 3 areas of research:developmentally specific symptoms of PBD (e.g.,rapid cycling, mixed mood states, comorbiddisorders); affective circuitry brain dysfunctionin PBD (e.g., poor problem-solving duringaffective stimulation via ventral frontostriataland dorsolateral prefrontal circuitry dysfunctionand deficits in superior temporal and visualcortices)25-27; and the impact of PBD on inter-personal/family functioning. CFF-CBT is deliv-ered via 12 manualized weekly 60- to 90-minutesessions with the child, parent, and/or family.It includes 7 components that comprise the treat-ment acronym “RAINBOW”: Routine (develop-ing consistent daily routines); Affect Regulation(psychoeducation about feelings; mood moni-toring; coping strategies to improve mood re-gulation); I Can Do It! (improving child self-esteem and parent self-efficacy); No Negative
JOURN
2 www.jaacap.org
Thoughts/Live in the Now (cognitive restruc-turing and mindfulness techniques to reducenegative thoughts); Be a Good Friend/BalancedLifestyle (social skill-building and improving par-ent self-care); Oh How Do We Solve this Problem?(family problem-solving and communicationtraining); and Ways to Find Support (enhancingsupport networks; detailed in Pavuluri et al.28).
This was the first RCT testing the efficacy ofCFF-CBT in treating PBD. Open trials haveestablished the feasibility, acceptability, and pre-liminary efficacy of CFF-CBT with promisingoutcomes.28-30 The goal of this trial was to testthe efficacy of the individual family format ofCFF-CBT compared to that in patients receivingpsychotherapy as usual (control) on outcomesof symptom control and global functioning. Wehypothesized that CFF-CBT would improve thesymptoms and global functioning of children atposttreatment compared to the control condition.We also hypothesized that treatment effectswould be maintained at follow-up, evidenced bydifferences in longitudinal trajectories of symp-toms and functioning from baseline through thefollow-up assessment point.
METHODStudy ParticipantsParticipants were children (N ¼ 69) diagnosed withPBD recruited from a specialty pediatric mood disor-ders clinic (PMDC) in an urban academic medicalcenter between 2010 and 2013. Children meeting DSM-IV-TR criteria for bipolar spectrum disorders (BD-I, II,and not otherwise specified [BP-NOS]) aged 7 to 13years were eligible to participate. Inclusion criteriaencompassed the following: stabilization on medica-tion, parental consent, and youth assent. Stabilizationon medication was defined by a Young Mania RatingScale (YMRS)31 score �20 and Children’s DepressionRating Scale–Revised (CDRS-R)32 score <80 (indicatingno severe symptoms requiring immediate more inten-sive care). These criteria were intended to excludechildren who needed acute stabilization before beingable to participate in psychotherapy but to still includechildren who were actively symptomatic. Thus, chil-dren scoring above threshold on these measures (n ¼ 4)were included if their psychiatrist determined theywere stable enough to engage in treatment. Exclusioncriteria for the study included: youth IQ <70, asmeasured by the Kaufman Brief Intelligence Scale–2(KBIT-233), active psychosis, active substance abuse/dependence, neurological or other medical problemsthat significantly complicate child’s psychiatric symp-toms as assessed via the Washington UniversitySchedule for Affective Disorders and Schizophrenia(WASH-U-KSADS34), and active suicidality requiring
AL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME - NUMBER - - 2014
CHILD AND FAMILY CBT FOR PEDIATRIC BIPOLAR DISORDER
hospitalization as measured by the Columbia SuicideSeverity Rating Scale (C-SSRS)35. In addition, youthwhose primary caretakers were experiencing currentdepressive or manic episodes, indicated by a BeckDepression Inventory (BDI36) score �28 and an Alt-man’s Self-Report of Mania (ASRM)37 score >6, wereexcluded. Youth with comorbid disorders, includinghigh-functioning autism, were included to ensure aclinically relevant sample.
ProceduresDiagnosis and Randomization. All study procedureswere approved by the Institutional Review Board atthe University of Illinois at Chicago. Eligibility wasassessed by trained study personnel. Potential partic-ipants were educated about the demands of thetreatment protocol and the importance of adher-ence, regardless of treatment assignment. Afterproviding informed consent and completinginclusion/exclusion measures, parents were inter-viewed using the WASH-U-KSADS34 and portions ofthe Kiddie-SADS–Present and Lifetime Version (K-SADS-PL)38 to define mood episodes, with corrobo-rating information coming from child-report. Trainedclinical interviewers (n ¼ 6) included licensed clinical
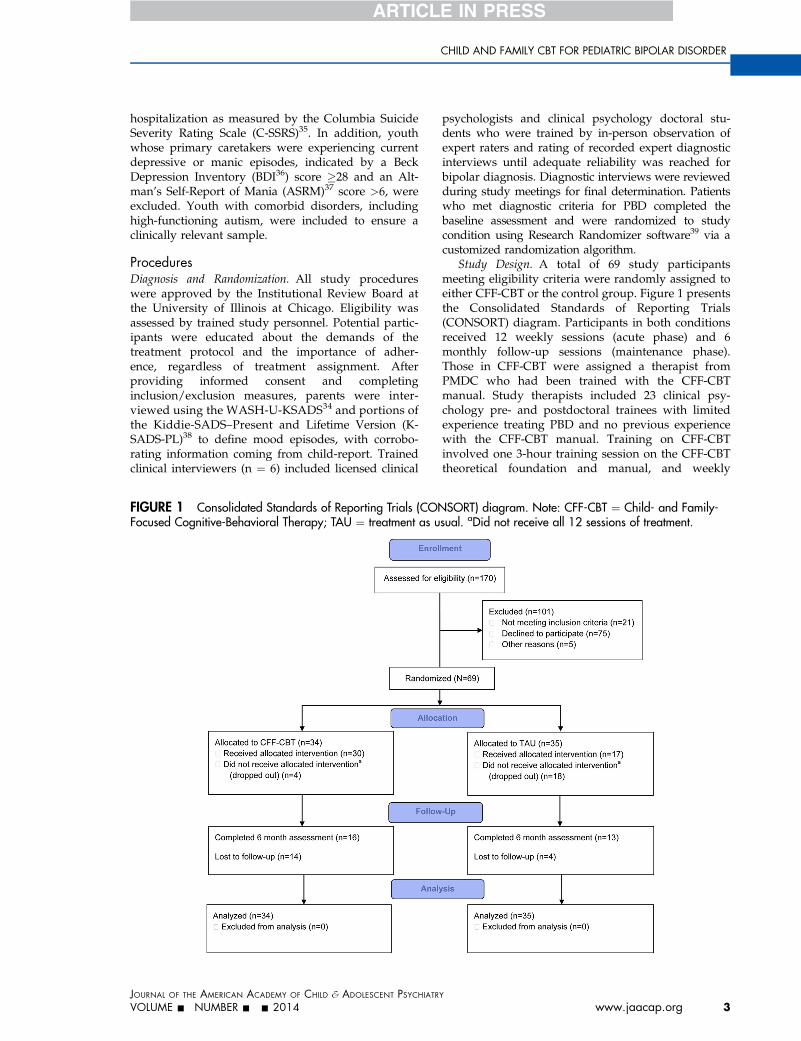
FIGURE 1 Consolidated Standards of Reporting Trials (CONFocused Cognitive-Behavioral Therapy; TAU ¼ treatment as u
JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATR
VOLUME - NUMBER - - 2014
psychologists and clinical psychology doctoral stu-dents who were trained by in-person observation ofexpert raters and rating of recorded expert diagnosticinterviews until adequate reliability was reached forbipolar diagnosis. Diagnostic interviews were reviewedduring study meetings for final determination. Patientswho met diagnostic criteria for PBD completed thebaseline assessment and were randomized to studycondition using Research Randomizer software39 via acustomized randomization algorithm.
Study Design. A total of 69 study participantsmeeting eligibility criteria were randomly assigned toeither CFF-CBT or the control group. Figure 1 presentsthe Consolidated Standards of Reporting Trials(CONSORT) diagram. Participants in both conditionsreceived 12 weekly sessions (acute phase) and 6monthly follow-up sessions (maintenance phase).Those in CFF-CBT were assigned a therapist fromPMDC who had been trained with the CFF-CBTmanual. Study therapists included 23 clinical psy-chology pre- and postdoctoral trainees with limitedexperience treating PBD and no previous experiencewith the CFF-CBT manual. Training on CFF-CBTinvolved one 3-hour training session on the CFF-CBTtheoretical foundation and manual, and weekly
SORT) diagram. Note: CFF-CBT ¼ Child- and Family-sual. aDid not receive all 12 sessions of treatment.
Y
www.jaacap.org 3

WEST et al.
supervision from the CFF-CBT developer and first(A.E.W) or second (S.M.W) author.
Participants randomized to the control group wereassigned a therapist in the General Psychiatry Clinic.These sessions were otherwise unstructured by thestudy design. Control therapists were clinical psy-chology doctoral students, postdoctoral fellows, psy-chiatry fellows, and social work interns who had notbeen trained in CFF-CBT but were given a 1-hourtraining on PBD. All sessions in both conditions wereaudiotaped to assess treatment content (see below).
All participants were treated in the same outpatientpsychiatry program, and thus logistics associated withtreatment that might affect access or engagement (e.g.,clinic times, location, parking, scheduling) did notdiffer by condition. Participants in both conditionsreceived medication management by a psychiatrist inthe PMDC following an evidence-based algorithm.40
Although patients were required to be stabilized ontheir medication (stable dosages for 4þ weeks) beforebaseline and randomization, medication managementwas delivered as it would be in regular practice andwas not manipulated as part of the study design.Medication changes over the course of the study werecarefully tracked at all assessments. Assessmentsoccurred at the following: baseline (pre-randomiza-tion); 4 and 8 weeks (during treatment); 12 weeks(posttreatment); and 39 weeks (follow-up assessment at6-months posttreatment).
MeasuresDiagnosis. The WASH-U-KSADS34, a semistructuredinterview specifically designed to assess for PBD, wasused to make a DSM-IV diagnosis.41 Research assis-tants were trained to administer the interview anddemonstrated adequate interrater reliability (k > 0.74).
Symptom Severity. The Child Mania Rating Scale(CMRS),42 a parent-rated measure to assess DSM-IV-TR mania symptoms, was our primary outcome mea-sure of mania symptoms. Scores are calculated bysumming across 21 items, each rated on a Likert scaleranging from 0 (never) to 3 (very often). Scores �20 areconsidered clinically significant. Reliability in thissample was strong (Cronbach’s a ¼ 0.90). The CMRSwas chosen as the method for assessing maniasymptoms because of its ability to capture symptomchanges over time by reporters (parents) that havemore comprehensive access to the child’s behaviorthroughout the course of treatment and across manydifferent contexts. Research suggests that parent reportmay result in more accurate assessment of mania,43 andthe CMRS demonstrates strong psychometric proper-ties, concurrent validity with the YMRS, and sensi-tivity to symptom change across treatment.42,44
The Child Bipolar Depression Rating Scale (CBDRS;unpublished data, August 2003) is a companion mea-sure to the Child Mania Rating scale. This parent reportincludes 22 items that assess for DSM-IV-TR depressive
JOURN
4 www.jaacap.org
symptoms. The scale has face validity, demonstratedstrong reliability (a ¼0.88), and was significantlycorrelated with clinician-reported depression (CDRS-R26) in this sample at baseline (r ¼ 0.32, p ¼ .008).
The Children’s Depression Rating Scale–Revised(CDRS-R)32 is a clinician-rated instrument for measuringdepression in children. Scores are summed across 17items rated on a 5-point Likert scale. Internal reliabilityand rater reliability across assessments in this samplewere strong (a ¼ 0.84; intraclass correlation[ICC] ¼ 0.78).
Global Functioning. The Children’s Global Assess-ment Scale (C-GAS)45 is a clinician-rated measure ofchild functioning based on impairment in family, so-cial, school, and work areas due to psychiatric symp-toms. Scores range from 1 to 100, with higher scoresindicating better functioning. Rater reliability acrossassessments was moderate in this sample (ICC ¼ 0.76).
The Children’s Global Impressions Scales forBipolar Disorder (CGI-BP)46 is a clinician report of achild’s overall psychiatric illness severity. Scores aresummed across the subscales (mania, depression,attention-deficit/hyperactivity, psychosis, and ag-gression). Rater reliability across assessments in thissample was strong (ICC ¼ 0.81).
Treatment Measures. The Treatment SatisfactionScale is a 21-item scale that was completed posttreat-ment to assess caregiver satisfaction with treatment. Atotal score is calculated by averaging item responses;responses range from 1 (not true) to 3 (very true). Thismeasure was developed and piloted for the pre-liminary study28 and demonstrated strong reliability inthis sample (a ¼ 0.94).
Therapist Fidelity to CFF-CBT was assessed via afidelity checklist developed and piloted in the pre-liminary study,28 which asked raters to record the keyCFF-CBT elements delivered in each treatment session(defined as number of elements delivered/total ele-ments to be delivered � 100). Ten CFF-CBT partici-pants were randomly selected, and a trained ratercompleted the fidelity checklist for audio recordings ofall 12 CFF-CBT sessions for that participant. In addi-tion, 10 control participants were randomly selected,and a trained rater completed the CFF-CBT fidelitychecklist for all 12 control sessions to assess for po-tential overlap with CFF-CBT ingredients.
Analytic ApproachMixed-effects regression (growth curve) models(MRMs)47 were conducted via SPSS MIXED to examineyouth response to treatment on key outcomes. MRMsare well-suited for longitudinal data analysis; they arerobust to the data dependency that occurs withrepeated assessments of individuals over time. Inaddition, MRMs are efficient in handling missing databy using all available data for a given participant toestimate group trends at each time point. SeparateMRMs were evaluated for each outcome measure and
AL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME - NUMBER - - 2014
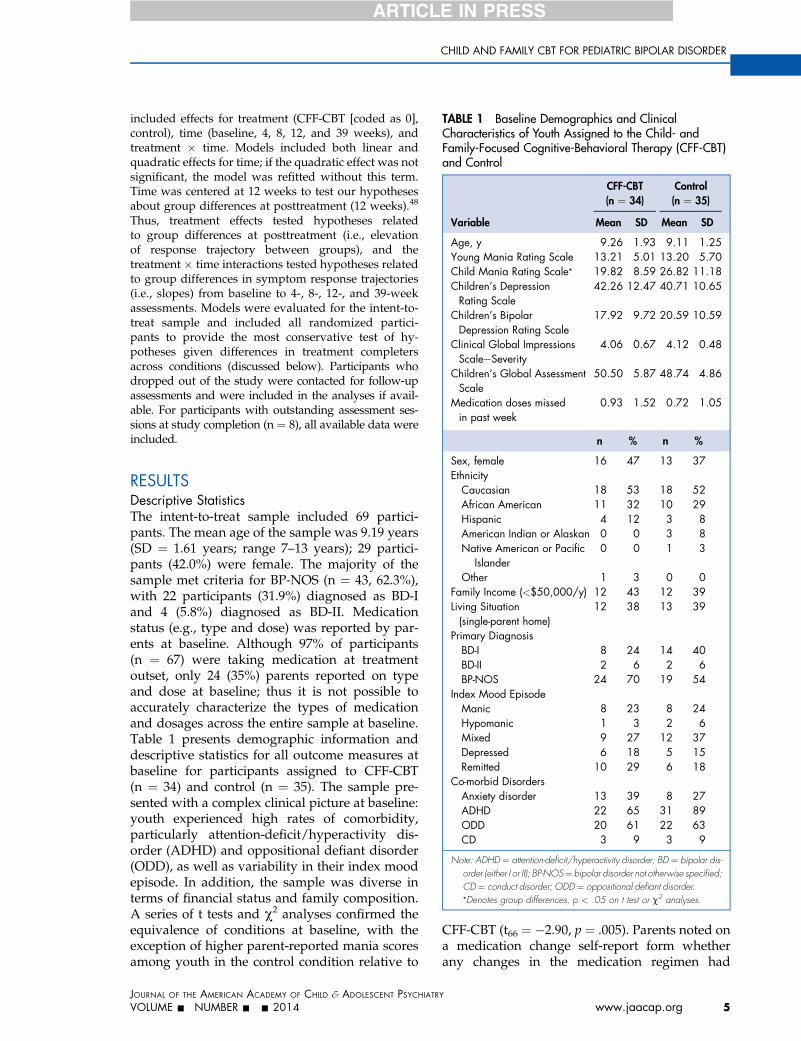
TABLE 1 Baseline Demographics and ClinicalCharacteristics of Youth Assigned to the Child- andFamily-Focused Cognitive-Behavioral Therapy (CFF-CBT)and Control
Variable
CFF-CBT(n ¼ 34)
Control(n ¼ 35)
Mean SD Mean SD
Age, y 9.26 1.93 9.11 1.25Young Mania Rating Scale 13.21 5.01 13.20 5.70Child Mania Rating Scale* 19.82 8.59 26.82 11.18Children’s DepressionRating Scale
42.26 12.47 40.71 10.65
Children’s BipolarDepression Rating Scale
17.92 9.72 20.59 10.59
Clinical Global ImpressionsScaleeSeverity
4.06 0.67 4.12 0.48
Children’s Global AssessmentScale
50.50 5.87 48.74 4.86
Medication doses missedin past week
0.93 1.52 0.72 1.05
n % n %
CHILD AND FAMILY CBT FOR PEDIATRIC BIPOLAR DISORDER
included effects for treatment (CFF-CBT [coded as 0],control), time (baseline, 4, 8, 12, and 39 weeks), andtreatment � time. Models included both linear andquadratic effects for time; if the quadratic effect was notsignificant, the model was refitted without this term.Time was centered at 12 weeks to test our hypothesesabout group differences at posttreatment (12 weeks).48
Thus, treatment effects tested hypotheses relatedto group differences at posttreatment (i.e., elevationof response trajectory between groups), and thetreatment � time interactions tested hypotheses relatedto group differences in symptom response trajectories(i.e., slopes) from baseline to 4-, 8-, 12-, and 39-weekassessments. Models were evaluated for the intent-to-treat sample and included all randomized partici-pants to provide the most conservative test of hy-potheses given differences in treatment completersacross conditions (discussed below). Participants whodropped out of the study were contacted for follow-upassessments and were included in the analyses if avail-able. For participants with outstanding assessment ses-sions at study completion (n ¼ 8), all available data wereincluded.
Sex, female 16 47 13 37Ethnicity
Caucasian 18 53 18 52African American 11 32 10 29Hispanic 4 12 3 8American Indian or Alaskan 0 0 3 8Native American or Pacific
Islander0 0 1 3
Other 1 3 0 0Family Income (<$50,000/y) 12 43 12 39Living Situation(single-parent home)
12 38 13 39
Primary DiagnosisBD-I 8 24 14 40BD-II 2 6 2 6BP-NOS 24 70 19 54
Index Mood EpisodeManic 8 23 8 24Hypomanic 1 3 2 6Mixed 9 27 12 37Depressed 6 18 5 15Remitted 10 29 6 18
Co-morbid DisordersAnxiety disorder 13 39 8 27ADHD 22 65 31 89ODD 20 61 22 63CD 3 9 3 9
Note: ADHD ¼ attention-deficit/hyperactivity disorder; BD ¼ bipolar dis-order (either I or II); BP-NOS¼ bipolar disorder not otherwise specified;CD¼ conduct disorder; ODD¼ oppositional defiant disorder.*Denotes group differences, p < .05 on t test or c2 analyses.
RESULTSDescriptive StatisticsThe intent-to-treat sample included 69 partici-pants. The mean age of the sample was 9.19 years(SD ¼ 1.61 years; range 7–13 years); 29 partici-pants (42.0%) were female. The majority of thesample met criteria for BP-NOS (n ¼ 43, 62.3%),with 22 participants (31.9%) diagnosed as BD-Iand 4 (5.8%) diagnosed as BD-II. Medicationstatus (e.g., type and dose) was reported by par-ents at baseline. Although 97% of participants(n ¼ 67) were taking medication at treatmentoutset, only 24 (35%) parents reported on typeand dose at baseline; thus it is not possible toaccurately characterize the types of medicationand dosages across the entire sample at baseline.Table 1 presents demographic information anddescriptive statistics for all outcome measures atbaseline for participants assigned to CFF-CBT(n ¼ 34) and control (n ¼ 35). The sample pre-sented with a complex clinical picture at baseline:youth experienced high rates of comorbidity,particularly attention-deficit/hyperactivity dis-order (ADHD) and oppositional defiant disorder(ODD), as well as variability in their index moodepisode. In addition, the sample was diverse interms of financial status and family composition.A series of t tests and c2 analyses confirmed theequivalence of conditions at baseline, with theexception of higher parent-reported mania scoresamong youth in the control condition relative to
JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATR
VOLUME - NUMBER - - 2014
CFF-CBT (t66 ¼ �2.90, p ¼ .005). Parents noted ona medication change self-report form whetherany changes in the medication regimen had
Y
www.jaacap.org 5
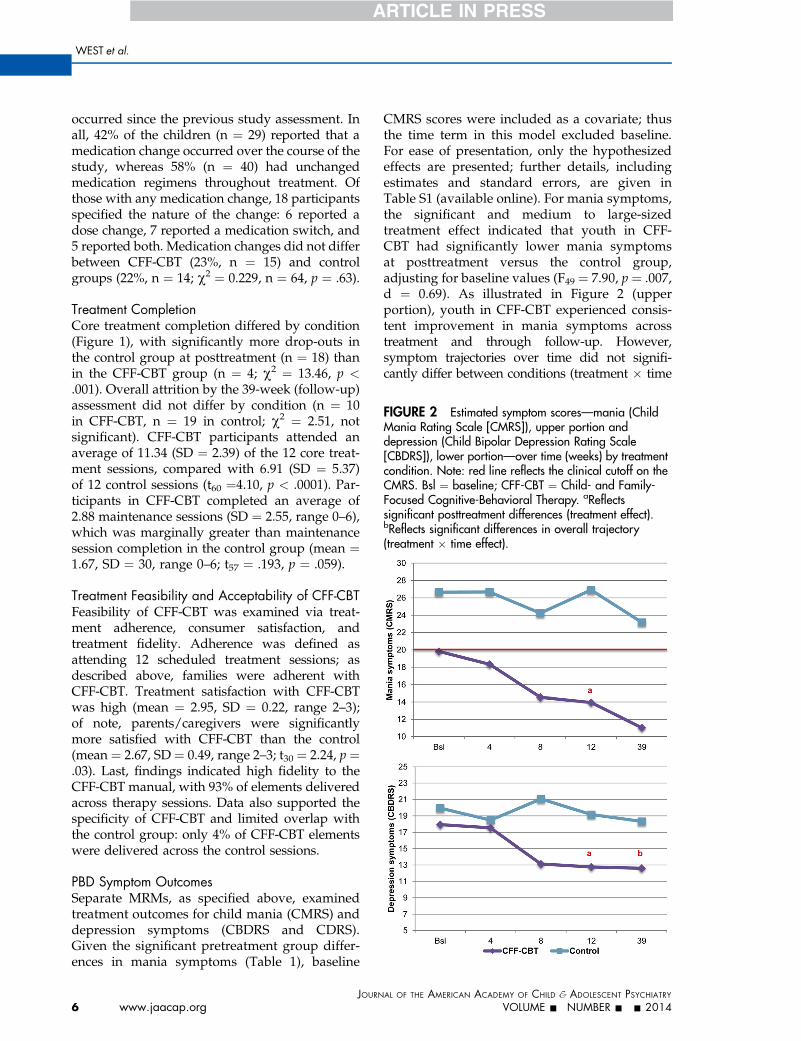
FIGURE 2 Estimated symptom scores—mania (ChildMania Rating Scale [CMRS]), upper portion anddepression (Child Bipolar Depression Rating Scale[CBDRS]), lower portion—over time (weeks) by treatmentcondition. Note: red line reflects the clinical cutoff on theCMRS. Bsl ¼ baseline; CFF-CBT ¼ Child- and Family-Focused Cognitive-Behavioral Therapy. aReflectssignificant posttreatment differences (treatment effect).bReflects significant differences in overall trajectory(treatment � time effect).
WEST et al.
occurred since the previous study assessment. Inall, 42% of the children (n ¼ 29) reported that amedication change occurred over the course of thestudy, whereas 58% (n ¼ 40) had unchangedmedication regimens throughout treatment. Ofthose with any medication change, 18 participantsspecified the nature of the change: 6 reported adose change, 7 reported a medication switch, and5 reported both. Medication changes did not differbetween CFF-CBT (23%, n ¼ 15) and controlgroups (22%, n ¼ 14; c2 ¼ 0.229, n ¼ 64, p ¼ .63).
Treatment CompletionCore treatment completion differed by condition(Figure 1), with significantly more drop-outs inthe control group at posttreatment (n ¼ 18) thanin the CFF-CBT group (n ¼ 4; c2 ¼ 13.46, p <.001). Overall attrition by the 39-week (follow-up)assessment did not differ by condition (n ¼ 10in CFF-CBT, n ¼ 19 in control; c2 ¼ 2.51, notsignificant). CFF-CBT participants attended anaverage of 11.34 (SD ¼ 2.39) of the 12 core treat-ment sessions, compared with 6.91 (SD ¼ 5.37)of 12 control sessions (t60 ¼4.10, p < .0001). Par-ticipants in CFF-CBT completed an average of2.88 maintenance sessions (SD ¼ 2.55, range 0–6),which was marginally greater than maintenancesession completion in the control group (mean ¼1.67, SD ¼ 30, range 0–6; t57 ¼ .193, p ¼ .059).
Treatment Feasibility and Acceptability of CFF-CBTFeasibility of CFF-CBT was examined via treat-ment adherence, consumer satisfaction, andtreatment fidelity. Adherence was defined asattending 12 scheduled treatment sessions; asdescribed above, families were adherent withCFF-CBT. Treatment satisfaction with CFF-CBTwas high (mean ¼ 2.95, SD ¼ 0.22, range 2–3);of note, parents/caregivers were significantlymore satisfied with CFF-CBT than the control(mean ¼ 2.67, SD ¼ 0.49, range 2–3; t30 ¼ 2.24, p ¼.03). Last, findings indicated high fidelity to theCFF-CBT manual, with 93% of elements deliveredacross therapy sessions. Data also supported thespecificity of CFF-CBT and limited overlap withthe control group: only 4% of CFF-CBT elementswere delivered across the control sessions.
PBD Symptom OutcomesSeparate MRMs, as specified above, examinedtreatment outcomes for child mania (CMRS) anddepression symptoms (CBDRS and CDRS).Given the significant pretreatment group differ-ences in mania symptoms (Table 1), baseline
JOURN
6 www.jaacap.org
CMRS scores were included as a covariate; thusthe time term in this model excluded baseline.For ease of presentation, only the hypothesizedeffects are presented; further details, includingestimates and standard errors, are given inTable S1 (available online). For mania symptoms,the significant and medium to large-sizedtreatment effect indicated that youth in CFF-CBT had significantly lower mania symptomsat posttreatment versus the control group,adjusting for baseline values (F49 ¼ 7.90, p ¼ .007,d ¼ 0.69). As illustrated in Figure 2 (upperportion), youth in CFF-CBT experienced consis-tent improvement in mania symptoms acrosstreatment and through follow-up. However,symptom trajectories over time did not signifi-cantly differ between conditions (treatment � time
AL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME - NUMBER - - 2014
CHILD AND FAMILY CBT FOR PEDIATRIC BIPOLAR DISORDER
F120 ¼ 0.95, p > .05, d ¼ 0.24). Notably, all youthexperienced mania symptoms at (CFF-CBT) orabove (control) clinical threshold at baseline(Table 1), but only youth in CFF-CBT achievedmean subthreshold mania symptoms by post-treatment and follow-up. Specifically, 88% (n ¼22) of youth in CFF-CBT scored below thresholdat posttreatment and 93% (n ¼ 14) were belowthreshold by follow-up, versus 21% (n ¼ 3)posttreatment and 46% (n ¼ 5) at follow-up inthe control group. In addition, youth in CFF-CBTalso experienced significantly reduced parent-reported depression at posttreatment and asteeper symptom response trajectory across theentire study period (Figure 2, lower portion;F67 ¼ 4.92, p ¼ .03, d ¼ 0.55 and F162 ¼ 3.82,p <.05, d ¼ 0.48); both effects were medium-sized. For clinician-reported depression symp-toms, however, neither the treatment nortreatment � time effect was significant (F62 ¼0.06, d ¼ 0.06 and F170 ¼ 2.5, d ¼ 0.39, respec-tively; p > .05).
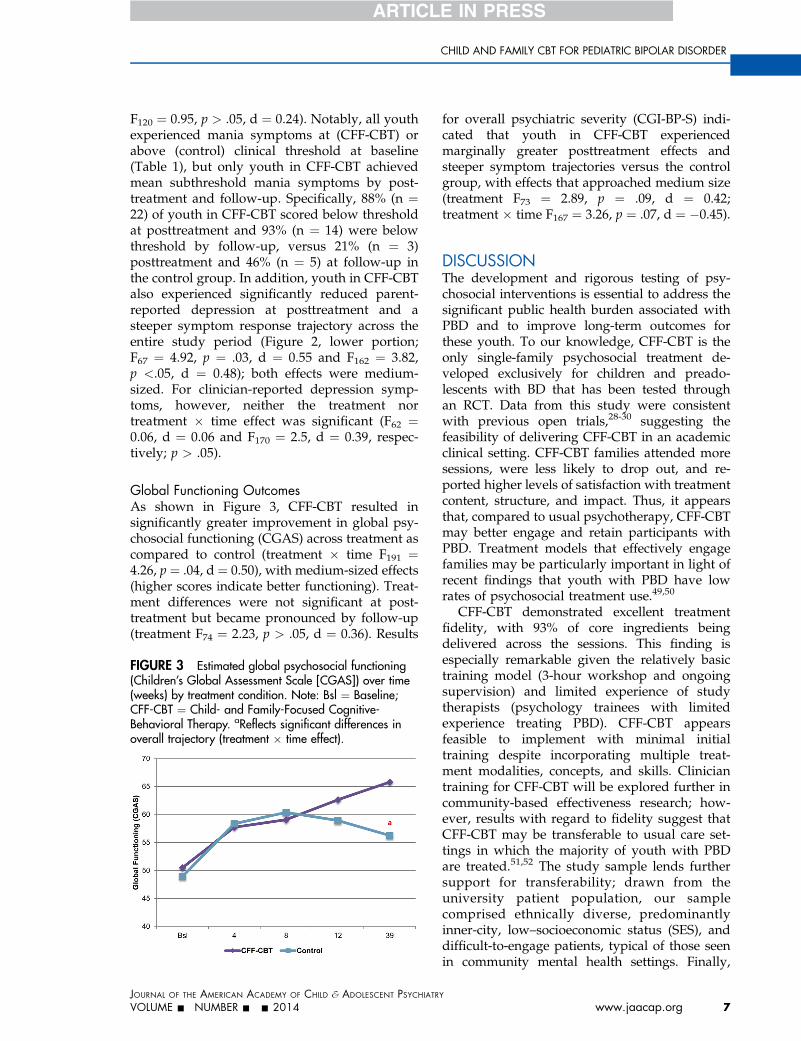
Global Functioning OutcomesAs shown in Figure 3, CFF-CBT resulted insignificantly greater improvement in global psy-chosocial functioning (CGAS) across treatment ascompared to control (treatment � time F191 ¼4.26, p ¼ .04, d ¼ 0.50), with medium-sized effects(higher scores indicate better functioning). Treat-ment differences were not significant at post-treatment but became pronounced by follow-up(treatment F74 ¼ 2.23, p > .05, d ¼ 0.36). Results
FIGURE 3 Estimated global psychosocial functioning(Children’s Global Assessment Scale [CGAS]) over time(weeks) by treatment condition. Note: Bsl ¼ Baseline;CFF-CBT ¼ Child- and Family-Focused Cognitive-Behavioral Therapy. aReflects significant differences inoverall trajectory (treatment � time effect).
JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATR
VOLUME - NUMBER - - 2014
for overall psychiatric severity (CGI-BP-S) indi-cated that youth in CFF-CBT experiencedmarginally greater posttreatment effects andsteeper symptom trajectories versus the controlgroup, with effects that approached medium size(treatment F73 ¼ 2.89, p ¼ .09, d ¼ 0.42;treatment � time F167 ¼ 3.26, p ¼ .07, d ¼ �0.45).
DISCUSSIONThe development and rigorous testing of psy-chosocial interventions is essential to address thesignificant public health burden associated withPBD and to improve long-term outcomes forthese youth. To our knowledge, CFF-CBT is theonly single-family psychosocial treatment de-veloped exclusively for children and preado-lescents with BD that has been tested throughan RCT. Data from this study were consistentwith previous open trials,28-30 suggesting thefeasibility of delivering CFF-CBT in an academicclinical setting. CFF-CBT families attended moresessions, were less likely to drop out, and re-ported higher levels of satisfaction with treatmentcontent, structure, and impact. Thus, it appearsthat, compared to usual psychotherapy, CFF-CBTmay better engage and retain participants withPBD. Treatment models that effectively engagefamilies may be particularly important in light ofrecent findings that youth with PBD have lowrates of psychosocial treatment use.49,50
CFF-CBT demonstrated excellent treatmentfidelity, with 93% of core ingredients beingdelivered across the sessions. This finding isespecially remarkable given the relatively basictraining model (3-hour workshop and ongoingsupervision) and limited experience of studytherapists (psychology trainees with limitedexperience treating PBD). CFF-CBT appearsfeasible to implement with minimal initialtraining despite incorporating multiple treat-ment modalities, concepts, and skills. Cliniciantraining for CFF-CBT will be explored further incommunity-based effectiveness research; how-ever, results with regard to fidelity suggest thatCFF-CBT may be transferable to usual care set-tings in which the majority of youth with PBDare treated.51,52 The study sample lends furthersupport for transferability; drawn from theuniversity patient population, our samplecomprised ethnically diverse, predominantlyinner-city, low–socioeconomic status (SES), anddifficult-to-engage patients, typical of those seenin community mental health settings. Finally,
Y
www.jaacap.org 7
WEST et al.
the limited overlap between the content of CFF-CBT and the control group suggests that thecore components of specialized treatment forPBD are not typically delivered in usual treat-ment, even in a university-based clinic with well-trained and supervised clinicians.
CFF-CBT demonstrated efficacy compared tothe control group in reducing parent-reportedmania symptoms. Youth in CFF-CBT exhibitedsignificantly lower mania symptoms after treat-ment. By follow-up, groups did not differ signifi-cantly in mania symptoms, but only those youthin CFF-CBT achieved below-threshold clinicalsymptoms. Thus, although the groups’ maniasymptom trajectories did not significantly differover the course of the study, there appears to be astrong treatment effect for CFF-CBT, as groupdifferences were significant at posttreatment, andonly participants in CFF-CBT had subclinicalmania symptoms at follow-up. It is important tonote that the youth in CFF-CBT began treatmentwith significantly lower mania symptoms, whichmay have influenced their positive outcomesrelative to the control group by posttreatment andfollow-up.
Youth in CFF-CBT also experienced signifi-cantly reduced parent-reported depressionsymptoms at posttreatment and a steeper symp-tom response trajectory across the entire studyperiod. For clinician-rated depression symptoms,however, groups did not differ at posttreatmentor across the follow-up period. The lack of find-ings for clinician-reported depressive symptomsrelative to parent-report is interesting. It is likelythat parents are more sensitive to smaller changesin depressive symptoms over time as comparedto a blinded rater with limited data to contextu-alize the child’s current symptom experience. Inaddition, findings may reflect rater “noise” due tomultiple blind raters rating each case over time;unfortunately, we did not have a sufficientlypowered sample to add a rater term to analyticmodels to further investigate these effects. Alter-natively, because parents were involved in thetreatment and not blind to condition, their reportsmay have been biased towards an overestimate ofchange in the CFF-CBT condition.
Youth in CFF-CBT also demonstratedimproved global functioning compared to youthin the control condition across treatment, withpronounced differences in psychosocial func-tioning by follow-up. This suggests that psy-chosocial functioning may improve graduallyyet steadily as treatment effects are internalized
JOURN
8 www.jaacap.org
and consolidated, in contrast to the acute im-provement observed in symptoms. Importantly,youth in CFF-CBT achieved a rating level by thefollow-up that suggested these youth werefunctioning well at home and school, hadmeaningful social relationships, and any behav-ioral problems were sporadic or isolated. Thisfinding was in contrast to youth in the controlcondition, whose levels of global functioningindicated moderate impairment in most socialdomains. In addition, findings indicated asteeper trajectory of improvement for overallbipolar symptom severity in the CFF-CBT groupversus control that approached significance.Marginally significant effects may be driven, inpart, by measurement issues given the con-stricted range on the CGI-BP (i.e., a 7-point rat-ing scale); thus, statistical models that betteraccount for this scaling may be considered with alarger sample.
Overall, findings suggest that CFF-CBT issuperior to psychotherapy as usual (even whenenhanced via brief PBD training) in addressingsymptoms and functional impairment in PBD.Results are consistent with extant studiesinvolving youth with mood disorders morebroadly and adolescents with BD, indicatingthat targeted evidence-based treatment for PBDmay optimize outcomes for these families.53
These results are also consistent with findingsfrom randomized trials of adults with BD,which have found that adaptations of CBT,family-focused therapy (FFT), group psycho-education, IPSRT, and systematic care manage-ment programs can be effective in hasteningstabilization, delaying relapses, reducingsymptom severity over time, and enhancingpsychosocial and family functioning.54 Interest-ingly, findings from the largest RCT of psycho-social treatment for adult BD55 to date, whichsupport the efficacy of intensive psychotherapy(CBT, FFT, or IPSRT) relative to a 3-sessioncontrol intervention (collaborative care), corre-spond to only a small effect size estimate forintensive psychotherapy over control in recov-ery rates. In the current study, we found me-dium to large-size effect sizes for CFF-CBTcompared to a more intensive dose-matched,psychotherapy-as-usual control, suggestingthat CFF-CBT may contribute unique andpowerful content relative to usual care.
Strengths of this study include a novel treat-ment model, rigorous RCT design, a sample sizeadequately powered for primary analyses, well-
AL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME - NUMBER - - 2014

CHILD AND FAMILY CBT FOR PEDIATRIC BIPOLAR DISORDER
validated assessment instruments and outcomemeasures, and a diverse and clinically represen-tative sample of youth with PBD. One of themost significant strengths of the study is the useof an active, dose-matched, psychotherapy con-trol condition delivered in the same competitiveacademic medical setting, thus delivering apowerful test of our manual-based treatmentmodel for PBD. However, findings from thisstudy must be interpreted in the context of studylimitations. First, there was greater core treat-ment completion in CFF-CBT participants versusthe control group. Although this finding isimportant for feasibility and acceptability, itlimited the ability for equivalent measurementacross conditions. The drop-out rate in the con-trol group was consistent with that of our uni-versity psychiatry clinic, which serves an inner-city, low-SES patient population; potential fac-tors specifically related to treatment assignmentmay include logistical and emotional barriers notaddressed well in treatment, and disappointmentin receiving the control condition. Second, andrelated, participants were not blinded to treat-ment condition. Although the study protocolenhanced perceived equipoise by emphasizingCFF-CBT as experimental, presenting the controlcondition as standard-of-care child and familytreatment, using language and tone thatexpressed equivalency, and communicating theimportance of engagement and participation toall participants during the consent process,treatment expectancy may have affectedengagement and outcomes. This weakness wasminimized by the use of clinician raters blindedto treatment condition. Third, although the useof blinded clinician raters is considered a designstrength, their accuracy may have been hinderedby the fact that they had no other interactionwith the patients and were unable to assessthe overall context of the participants’ symptomexperiences over time. Fourth, youth in the con-trol condition exhibited significantly highermania symptoms at baseline than youth in CFF-CBT. Although we controlled for this differencein analyses, it still indicates that the 2 groupswere not entirely equivalent in terms of clinicalcharacteristics at baseline. Fifth, the primaryoutcome of mania symptoms was measured byparent report only. This decision was madebased on the fact that the CMRS has demon-strated excellent psychometric properties,42,44
and parent reports of mania are considered
JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATR
VOLUME - NUMBER - - 2014
most accurate.56 In addition, our own clinicalexperience with the CMRS versus the clinician-rated YMRS is that the CMRS contributes morecomprehensive, nuanced, and contextualizeddata on mania symptoms, whereas the YMRSdemonstrates limited range and restricted var-iability in our patient population. However,a multiple-informant approach would havestrengthened outcome measurement for mania.Sixth, although medication changes were cap-tured in the measurement plan and did notdiffer by condition, it is possible that unmea-sured medication effects might explain symp-tom improvement for some study participants.Finally, the interpretation of findings from theoverall treatment trajectory (core treatment phaseand follow-up together) is hindered by the largeamount of attrition during the follow-up phase(29 participants dropped out before the 6-monthfollow-up). For this reason, posttreatment (treat-ment effect) was our primary outcome point,and results for the full 9-month trajectory (i.e.,treatment � time effect) are regarded asexploratory.
Despite these limitations, this study makes animportant contribution to the literature inproviding rigorous evidence for a novel family-based psychosocial treatment model for chil-dren with PBD, a difficult-to-treat population forwhom there are few, if any, effective evidence-based treatments. CFF-CBT proved efficaciouscompared to psychotherapy-as-usual in thisstudy. Additional strengths with regard to futuredissemination may include its short duration(12 weeks), efficient training model (3-hourworkshop plus initial supervision), and the abil-ity to engage difficult-to-treat families (e.g., se-vere symptoms; urban, low-SES clinic populationwith significant barriers to treatment). Futurestudies may establish whether CFF-CBT can betransported successfully to community settingsand factors (e.g., training, organizational context)related to its successful implementation. Inaddition, we hope to examine potential moder-ators of treatment response, such as baselinefamily functioning, that can inform more indi-vidualized treatment approaches. Finally, weplan to explore potential treatment mechanisms,such as improved parental well-being and effi-cacy, and to incorporate novel neurobiologicalmeasures of treatment response that approximatethese changes at the brain level (e.g., changesin neural circuitry related to arousal and
Y
www.jaacap.org 9

WEST et al.
emotional processing) to inform specific treat-ment targets. &
Clinical Guidance
� The psychosocial impairments and morbidconsequences associated with PBD, along withlimited efficacy of medication to address broaddomains of functioning, has led to consensus thatpsychosocial intervention is a necessary componentof treatment for PBD.
� Children with BD may benefit from structuredmanual-based treatment specialized for PBD. In thistrial, CFF-CBT demonstrated efficacy versus dose-matched control treatment for improving symptoms ofPBD as well as global psychosocial functioning.CFF-CBT is a 12-session manualized therapy thatfocuses on improving the key domains of difficultyassociated with PBD, including affect regulation,self-efficacy, social/family functioning, and youth/parent coping with the disorder.
� CFF-CBT was feasible to implement even withminimal initial training and nonexpert clinicians, thusdemonstrating promise for dissemination intocommunity practice settings.
� Future studies may be able to determine the specificfactors associated with positive treatment outcomesin PBD.
10
Accepted September 4, 2014.
Drs. West, Weinstein, Henry, and Pavuluri, and Mss. Peters and Katzare with the University of Illinois at Chicago. Dr. Henry is also with theUniversity of Alaska, Center for Alaska Native Health Research. Mr.Cruz is with Utah State University, but was with the University of Illinoisat Chicago at the time the study was performed.
JOURNAL
www.jaacap.org
This research was supported by the National Institutes of Mental Health(NIMH) K23 grant MH079935 (A.E.W.).
Dr. Henry served as the statistical expert for this research.
The authors thank Patrick Tolan, PhD, of the University of Virginia, andDavid Miklowitz, PhD, of the University of California at Los Angeles, formentorship and consultation; Christine Celio, PhD, and Jackie Doxie,MA, of the University of Illinois at Chicago, for serving as study co-ordinators. The authors thank all of the psychology, psychiatry, andsocial work trainees and staff at the University of Illinois at Chicago thatserved as study therapists and/or supervisors. The authors also thankall of the undergraduate and graduate psychology trainees from theUniversity of Illinois at Chicago who served as study raters andresearch assistants. Finally, the authors thank the University of IllinoisCenter for Clinical and Translational Science (CCTS) for resources tosupport this study. The CCTS is supported by the National Center forAdvancing Translational Sciences, National Institutes of Health (NIH),through grant UL1TR000050. The work of the Center is solely the re-sponsibility of the authors and does not necessarily represent the officialviews of NIH.
Disclosures: Dr. West has received honoraria from the NIH (grant re-view), Northwestern University (Grand Rounds), and University of Lund(academic talk). Dr. Weinstein has received funding from the AmericanFoundation for Suicide Prevention (AFSP) and honoraria from the Uni-versity of Lund (academic talk). Dr. Henry has received funding from theNational Institute of Justice, National Institute of Drug Abuse, NIMH,Center for Disease Control and Prevention, and the McCormickFoundation. He has received honoraria and consultancies from RushUniversity, the Center for Alaska Native Health Research, and theUniversity of Virginia Curry School of Education. Dr. Pavuluri hasreceived grant support from the following sources: NIH, NIMH, theNational Alliance for Research on Schizophrenia and Depression(NARSAD), the American Foundation for Suicide Prevention, and theMarshall Reynolds Foundation. She is the recipient of the Berger-Col-beth Term Chair in Child Psychiatry and participated in the OtsukaPharmaceuticals National Advisory Board meeting once. Mr. Cruz hasreceived grant support from the National Institute of Drug Abuse. Hehas consulted for Mental Health Data Services, Inc. Ms. Peters andMs. Katz report no biomedical financial interests or potential conflictsof interest.
Correspondence to Amy E. West, PhD, Department of Psychiatry,1747 W. Roosevelt Road, Chicago, IL 60608; e-mail: [email protected]
0890-8567/$36.00/ª2014 American Academy of Child andAdolescent Psychiatry
http://dx.doi.org/10.1016/j.jaac.2014.08.013
REFERENCES
1. Van Meter AR, Moreira AL, Youngstrom EA. Meta-analysis ofepidemiologic studies of pediatric bipolar disorder. J Clin Psy-chiatry. 2011;72:1250-1256.
2. Geller B, Sun K, Zimerman B, Luby J, Frazier J, Williams M.Complex and rapid-cycling in bipolar children and adolescents: apreliminary study. J Affect Disord. 1995;34:259-268.
3. Pavuluri MN, Birmaher B, Naylor MW. Pediatric bipolar disorder:a review of the past 10 years. J Am Acad Child Adolesc Psychiatry.2005;44:846-871.
4. Henin A, Mick E, Biederman J, et al. Can bipolar disorder-specificneuropsychological impairments in children be identified?J Consult Clin Psychol. 2007;75:210-220.
5. Pavuluri MN, O’Connor MM, Harral EM, Moss M, Sweeney JA.Impact of neurocognitive function on academic difficulties in pe-diatric bipolar disorder: a clinical translation. Biol Psychiatry.2006;60:951-956.
6. Geller B, Zimerman B, Williams M, Delbello MP, Frazier J,Beringer L. Phenomenology of prepubertal and early adolescentbipolar disorder: examples of elated mood, grandiose behaviors,decreased need for sleep, racing thoughts and hypersexuality.J Child Adolesc Psychopharmacol. 2002;12:3-9.
7. Geller B, Craney JL, Bolhofner K, Nickelsburg MJ, Williams M,Zimerman B. Two-year prospective follow-up of children with aprepubertal and early adolescent bipolar disorder phenotype. AmJ Psychiatry. 2002;159:927-933.
8. Wilens TE, Biederman J, Forkner P, et al. Patterns of comorbidityand dysfunction in clinically referred preschool and school-agechildren with bipolar disorder. J Child Adolesc Psychopharma-col. 2003;13:495-505.
9. Geller B, Bolhofner K, Craney JL, Williams M, DelBello MP,Gundersen K. Psychosocial functioning in a prepubertal and earlyadolescent bipolar disorder phenotype. J Am Acad Child AdolescPsychiatry. 2000;39:1543-1548.
10. Rucklidge JJ. Psychosocial functioning of adolescents with andwithout paediatric bipolar disorder. J Affect Disord. 2006;91:181-188.
11. Schenkel LS, West AE, Harral EM, Patel NB, Pavuluri MN. Parent-child interactions in pediatric bipolar disorder. J Clin Psychol.2008;64:422-437.
12. Goldstein TR, Miklowitz DJ, Mullen KL. Social skills knowledgeand performance among adolescents with bipolar disorder. Bi-polar Disord. 2006;8:350-361.
OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME - NUMBER - - 2014

CHILD AND FAMILY CBT FOR PEDIATRIC BIPOLAR DISORDER
13. Keenan-Miller D, Peris T, Axelson D, Kowatch RA, Miklowitz DJ.Family functioning, social impairment, and symptoms amongadolescents with bipolar disorder. J Am Acad Child AdolescPsychiatry. 2012;51:1085-1094.
14. Kim EY, Miklowitz DJ, Biuckians A, Mullen K. Life stress and thecourse of early-onset bipolar disorder. J Affect Disord. 2007;99:37-44.
15. Lewinsohn PM, Seeley JR, Klein DN. Bipolar Disorder in Ado-lescents: Epidemiology and Suicidal Behavior. New York: Guil-ford Press; 2003.
16. Kessler RC, Akiskal HS, Ames M, et al. Prevalence and effects ofmood disorders on work performance in a nationally representa-tive sample of U.S. workers. Am J Psychiatry. 2006;163:1561-1568.
17. Kupfer DJ. The increasing medical burden in bipolar disorder.JAMA. 2005;293:2528-2530.
18. Gore FM, Bloem PJ, Patton GC, et al. Global burden of disease inyoung people aged 10-24 years: a systematic analysis. Lancet.2011;377:2093-2102.
19. Goldstein BI, Sassi R, Diler RS. Pharmacologic treatment of bipolardisorder in children and adolescents. Child Adolesc PsychiatrClinics N Am. 2012;21:911-939.
20. McClellan J, Kowatch R, Findling RL. Work Group on Quality I.Practice parameter for the assessment and treatment of childrenand adolescents with bipolar disorder. J Am Acad Child AdolescPsychiatry. 2007;46:107-125.
21. Goldstein TR, Fersch-Podrat RK, Rivera M, et al. DialecticalBehavior Therapy (DBT) for adolescents with bipolar disorder:results from a pilot randomized trial. J Child Adolesc Psycho-pharmacol. 2014 Jul 10 [Epub ahead of print].
22. Hlastala SA, Kotler JS, McClellan JM, McCauley EA. Interpersonaland social rhythm therapy for adolescents with bipolar disorder:treatment development and results from an open trial. DepressAnxiety. 2010;27:457-464.
23. Fristad MA, Verducci JS, Walters K, Young ME. Impact of multi-family psychoeducational psychotherapy in treating children aged8 to 12 years with mood disorders. Arch Gen Psychiatry. 2009;66:1013-1021.
24. Miklowitz DJ, Axelson DA, Birmaher B, et al. Family-focusedtreatment for adolescents with bipolar disorder: results of a 2-yearrandomized trial. Arch Gen Psychiatry. 2008;65:1053-1061.
25. Garrett AS, Reiss AL, Howe ME, et al. Abnormal amygdala andprefrontal cortex activation to facial expressions in pediatric bi-polar disorder. J Am Acad Child Adolesc Psychiatry. 2012;51:821-831.
26. Rich BA, Carver FW, Holroyd T, et al. Different neural path-ways to negative affect in youth with pediatric bipolar disor-der and severe mood dysregulation. J Psychiatr Res. 2011;45:1283-1294.
27. Passarotti AM, Pavuluri MN. Brain functional domains informtherapeutic interventions in attention-deficit/hyperactivity disor-der and pediatric bipolar disorder. Expert Rev Neurotherapeut.2011;11:897-914.
28. Pavuluri MN, Graczyk PA, Henry DB, Carbray JA, Heidenreich J,Miklowitz DJ. Child- and family-focused cognitive-behavioraltherapy for pediatric bipolar disorder: development and pre-liminary results. J Am Acad Child Adolesc Psychiatry. 2004;43:528-537.
29. West AE, Henry DB, Pavuluri MN. Maintenance model of inte-grated psychosocial treatment in pediatric bipolar disorder: a pilotfeasibility study. J Am Acad Child Adolesc Psychiatry. 2007;46:205-212.
30. West AE, Jacobs RH, Westerholm R, et al. Child and family-focused cognitive-behavioral therapy for pediatric bipolar disor-der: pilot study of group treatment format. J Can Acad ChildAdolesc Psychiatry. 2009;18:239-246.
31. Young RC, Biggs JT, Ziegler VE, Meyer DA. A rating scale formania: reliability, validity and sensitivity. Br J Psychiatry. 1978;133:429-435.
32. Poznanski EO, Grossman JA, Buchsbaum Y, Banegas M,Freeman L, Gibbons R. Preliminary studies of the reliability andvalidity of the Children’s Depression Rating Scale. J Am AcadChild Psychiatry. 1984;23:191-197.
33. Kaufman AS, Kaufman NL. Kaufman Brief Intelligence Test–Second Edition (KBIT-2). Circle Pines, MN: American GuidanceService; 2004.
JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATR
VOLUME - NUMBER - - 2014
34. Geller B, Williams M, Zimerman B, Frazier J. Washington Uni-versity in St. Louis Kiddie Schedule for Affective Disorders andSchizophrenia (WASH-U-KSADS). St Louis: Washington Univer-sity; 1996.
35. Posner K, Brown GK, Stanley B, et al. The Columbia–SuicideSeverity Rating Scale: initial validity and internal consistencyfindings from three multisite studies with adolescents and adults.Am J Psychiatry. 2011;168:1266-1277.
36. Beck AT, Steer RA, Brown GK. Manual for the Beck DepressionInventory–II. San Antonio, TX: Psychological Corporation; 1996.
37. Altman E, Hedeker D, Peterson JL, Davis JM. A comparativeevaluation of three self-rating scales for acute mania. Biol Psy-chiatry. 2001;50:468-471.
38. Primakoff L, Epstein N, Covi L. Homework compliance: an un-controlled variable in cognitive therapy outcome research. BehavTherapy. 1986;17:433-446.
39. Urbaniak, G. C., & Plous, S. Research randomizer, version 3.0.Available at: http://www.randomizer.org/about.htm. AccessedSeptember 24, 2014.
40. Pavuluri MN, Henry DB, Devineni B, Carbray JA, Naylor MW,Janicak PG. A pharmacotherapy algorithm for stabilization andmaintenance of pediatric bipolar disorder. J Am Acad ChildAdolesc Psychiatry. 2004;43:859-867.
41. American Psychiatric Association. Diagnostic and StatisticalManual of Mental Health Disorders (4th ed). Washington, DC:American Psychiatric Association; 1994.
42. Pavuluri MN, Henry DB, Devineni B, Carbray JA, Birmaher B.Child Mania Rating Scale: development, reliability, and validity.J Am Acad Child Adolesc Psychiatry. 2006;45:550-560.
43. Youngstrom E, Meyers O, Demeter C, et al. Comparing diagnosticchecklists for pediatric bipolar disorder in academic and com-munity mental health settings. Bipolar Disord. 2005;7:507-517.
44. West AE, Celio CI, Henry DB, Pavuluri MN. Child Mania RatingScale–Parent Version: a valid measure of symptom change due topharmacotherapy. J Affect Disord. 2011;128:112-119.
45. Shaffer D, Gould MS, Brasic J, et al. A Children’s Global Assess-ment Scale (CGAS). Arch Gen Psychiatry. 1983;40:1228-1231.
46. Spearing MK, Post RM, Leverich GS, Brandt D, Nolen W. Modi-fication of the Clinical Global Impressions (CGI) Scale for Use inBipolar Illness (BP): the CGI-BP. Psychiatry research. 1997;73:159-171.
47. Laird NM, Ware JH. Random-effects models for longitudinal data.Biometrics. 1982;38:963-974.
48. JDaW Singer. J.B, Applied longitudinal data analysis: modelingchange and event occurrence. Oxford: Oxford UniversityPress; 2003.
49. Merikangas KR, He J-p, Burstein M, et al. Lifetime prevalenceof mental disorders in US adolescents: results from theNational Comorbidity Survey Replication–Adolescent Supple-ment (NCS-A). J Am Acad Child Adolesc Psychiatry. 2010;49:980-989.
50. Rizzo CJ, Esposito-Smythers C, Swenson L, et al. Factors associ-ated with mental health service utilization among bipolar youth.Bipolar Disord. 2007;9:839-850.
51. Youngstrom E, Meyers O, Demeter C, et al. Comparing diag-nostic checklists for pediatric bipolar disorder in academic andcommunity mental health settings. Bipolar Disorders. 2005;7:507-517.
52. Case BG, Olfson M, Marcus SC, Siegel C. Trends in the inpatientmental health treatment of children and adolescents in US com-munity hospitals between 1990 and 2000. Arch Gen Psychiatry.2007;64:89.
53. Weinstein SM, West AE, Pavuluri M. Psychosocial intervention forpediatric bipolar disorder: current and future directions. ExpertRev Neurotherapeut. 2013;13:843-850.
54. Cakir S, Ozerdem A. [Psychotherapeutic and psychosocial ap-proaches in bipolar disorder: a systematic literature review]. TurkPsikiyatri Dergisi [Turkish J Psychiatry]. 2010;21:143-154.
55. Miklowitz DJ, Otto MW, Frank E, et al. Psychosocial treatments forbipolar depression: a 1-year randomized trial from the SystematicTreatment Enhancement Program. Arch Gen Psychiatry. 2007;64:419-426.
56. Youngstrom EA, Birmaher B, Findling RL. Pediatric bipolar dis-order: validity, phenomenology, and recommendations for diag-nosis. Bipolar Disorders. 2008;10:194-214.
Y
www.jaacap.org 11
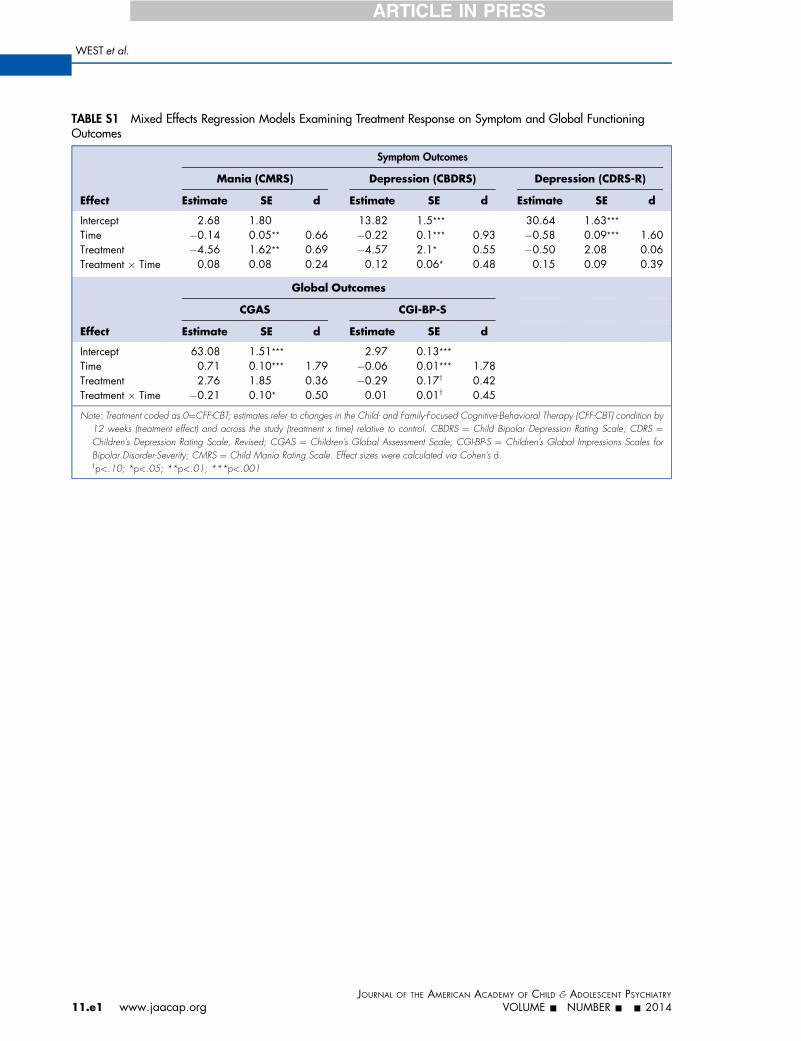
TABLE S1 Mixed Effects Regression Models Examining Treatment Response on Symptom and Global FunctioningOutcomes
Effect
Symptom Outcomes
Mania (CMRS) Depression (CBDRS) Depression (CDRS-R)
Estimate SE d Estimate SE d Estimate SE d
Intercept 2.68 1.80 13.82 1.5*** 30.64 1.63***Time �0.14 0.05** 0.66 �0.22 0.1*** 0.93 �0.58 0.09*** 1.60Treatment �4.56 1.62** 0.69 �4.57 2.1* 0.55 �0.50 2.08 0.06Treatment � Time 0.08 0.08 0.24 0.12 0.06* 0.48 0.15 0.09 0.39
Effect
Global Outcomes
CGAS CGI-BP-S
Estimate SE d Estimate SE d
Intercept 63.08 1.51*** 2.97 0.13***Time 0.71 0.10*** 1.79 �0.06 0.01*** 1.78Treatment 2.76 1.85 0.36 �0.29 0.17y 0.42Treatment � Time �0.21 0.10* 0.50 0.01 0.01y 0.45
Note: Treatment coded as 0¼CFF-CBT; estimates refer to changes in the Child- and Family-Focused Cognitive-Behavioral Therapy (CFF-CBT) condition by12 weeks (treatment effect) and across the study (treatment x time) relative to control. CBDRS ¼ Child Bipolar Depression Rating Scale; CDRS ¼Children’s Depression Rating Scale, Revised; CGAS ¼ Children’s Global Assessment Scale; CGI-BP-S ¼ Children’s Global Impressions Scales forBipolar Disorder-Severity; CMRS ¼ Child Mania Rating Scale. Effect sizes were calculated via Cohen’s d.yp<.10; *p<.05; **p<.01; ***p<.001
WEST et al.
JOURN
11.e1 www.jaacap.org
AL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRYVOLUME - NUMBER - - 2014
Related Documents