Chest Exam / Lung Topography

Chest Exam / Lung Topography
Jan 02, 2016
Chest Exam / Lung Topography. Physical examination employs the use of inspection, palpation, percussion, and auscultation to determine patients’ clinical status and their response to therapy Each examination is modified according to the purpose of the examination - PowerPoint PPT Presentation
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Chest Exam / Lung Topography
Physical examination employs the use of inspection, palpation, percussion, and auscultation to determine patients’ clinical status and their response to therapy
Each examination is modified according to the purpose of the examination
Physical examination skills develop over time with practice
Examination of the Head and Neck
Identify the patient’s facial expression, looking for evidence of pain or acute distress
Look for evidence of cyanosis around the lips and oral mucosa
Patients may use pursed-lip breathing when COPD is present
Eyes
The eyes are inspected for pupillary response to light when neurologic defects are suspected
Dilated and fixed pupils suggest brain death in some patients
The eyelids may droop (ptosis), indicating damage to the third cranial nerve

Neck
The trachea should be midline If it is deviated to one side, a unilateral lung
problem is probably present Atelectasis pneumothorax
The status of the jugular veins in the neck is important Patients with cor pulmonale have JVD
Use of accessory muscles in the neck suggests obstructive lung disease
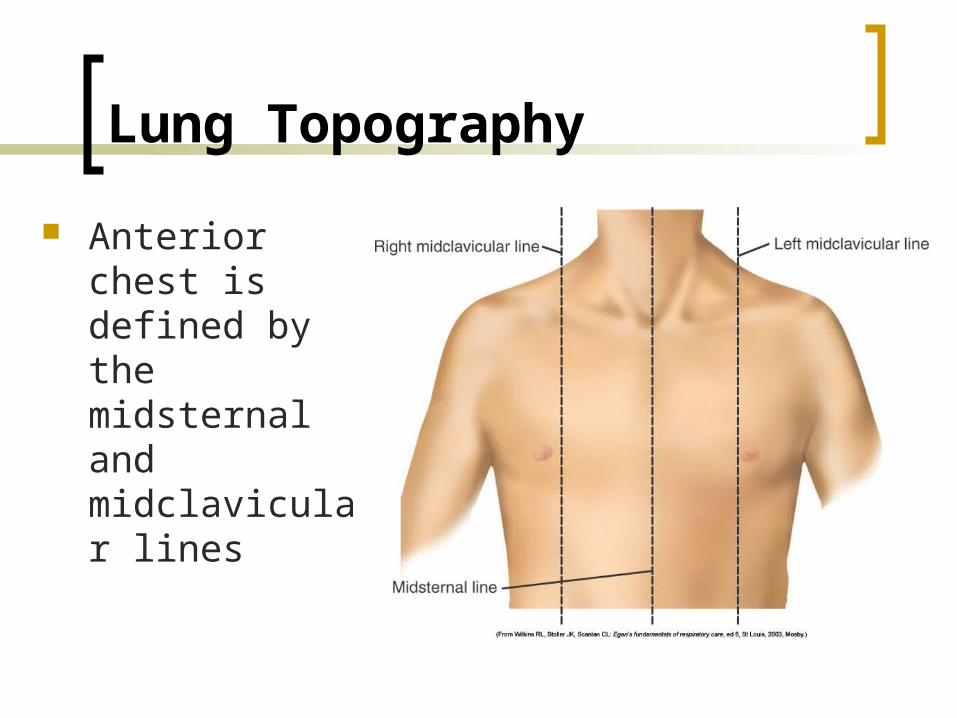
Lung Topography
Anterior chest is defined by the midsternal and midclavicular lines
Lung Topography
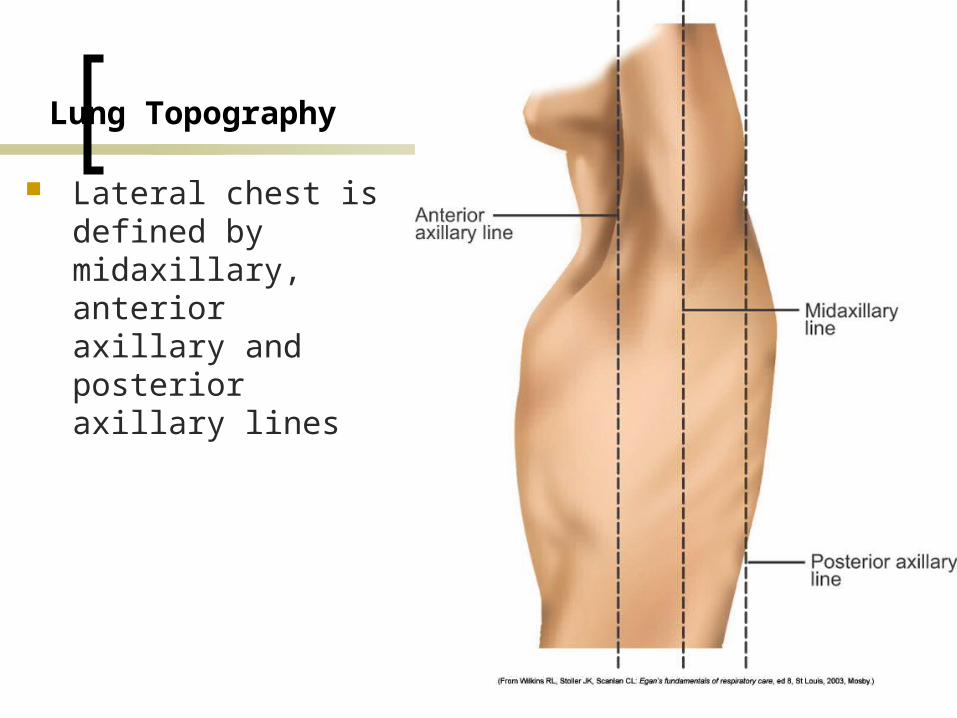
Lateral chest is defined by midaxillary, anterior axillary and posterior axillary lines
Lung Topography
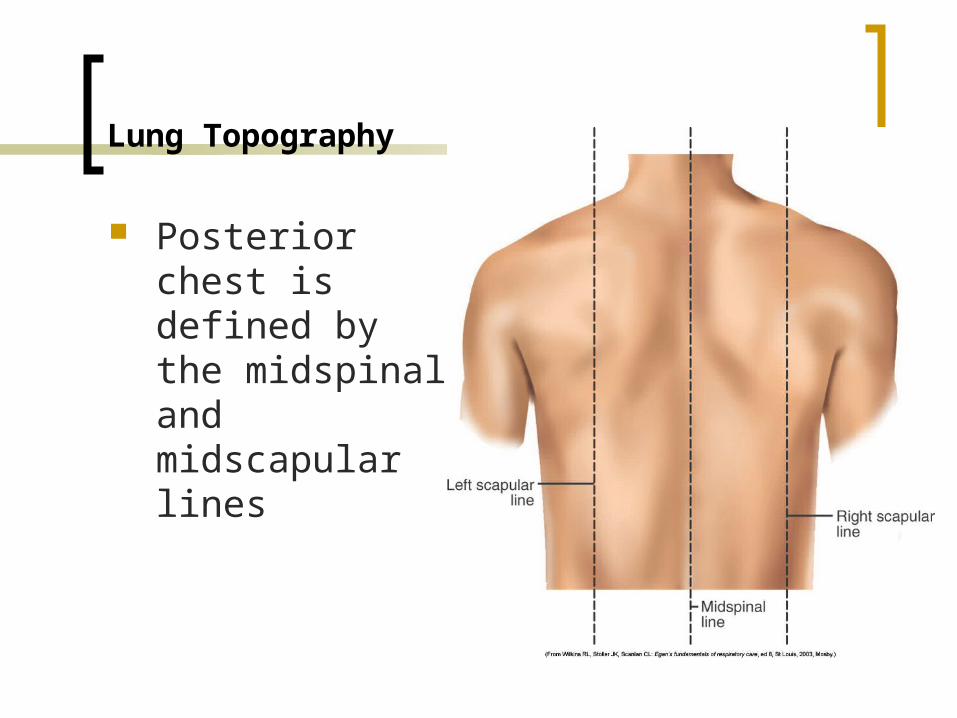
Posterior chest is defined by the midspinal and midscapular lines
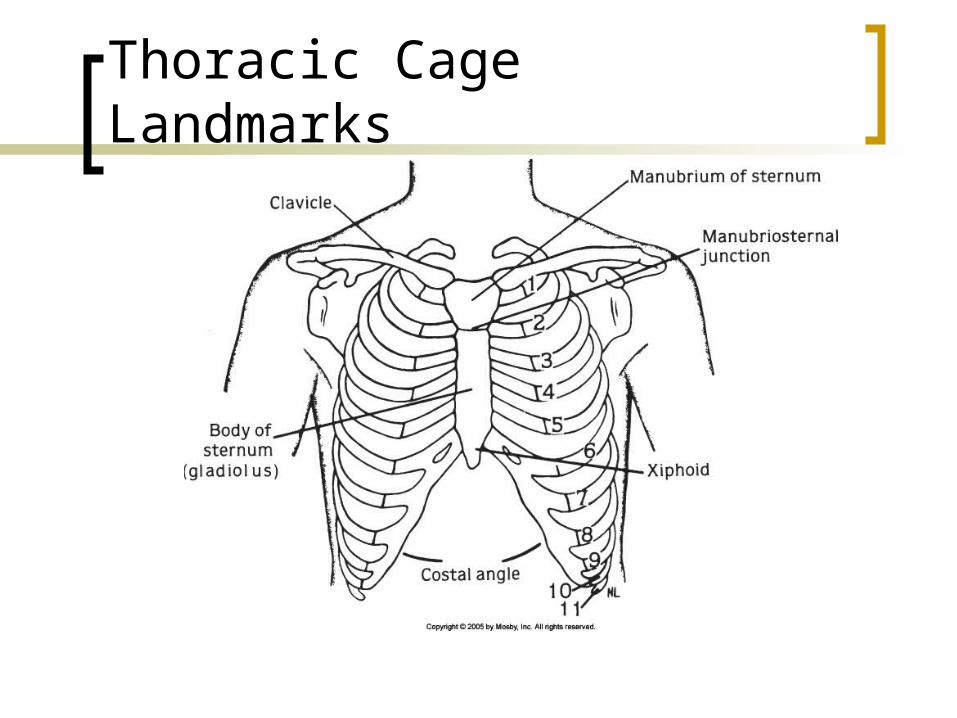
Thoracic Cage Landmarks
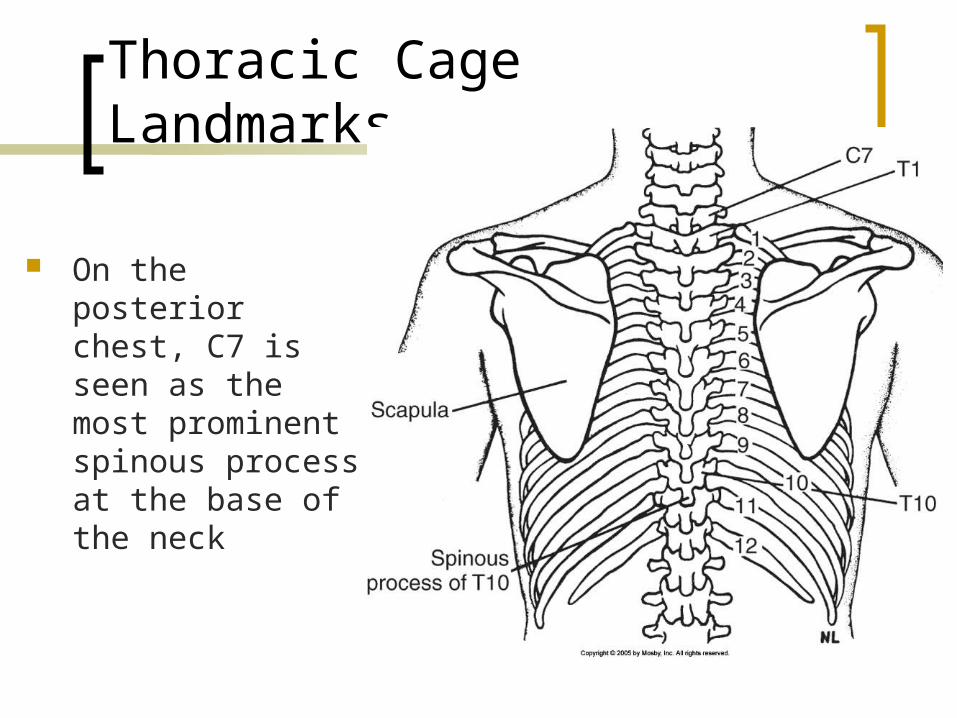
Thoracic Cage Landmarks
On the posterior chest, C7 is seen as the most prominent spinous process at the base of the neck
Thoracic Cage Landmarks
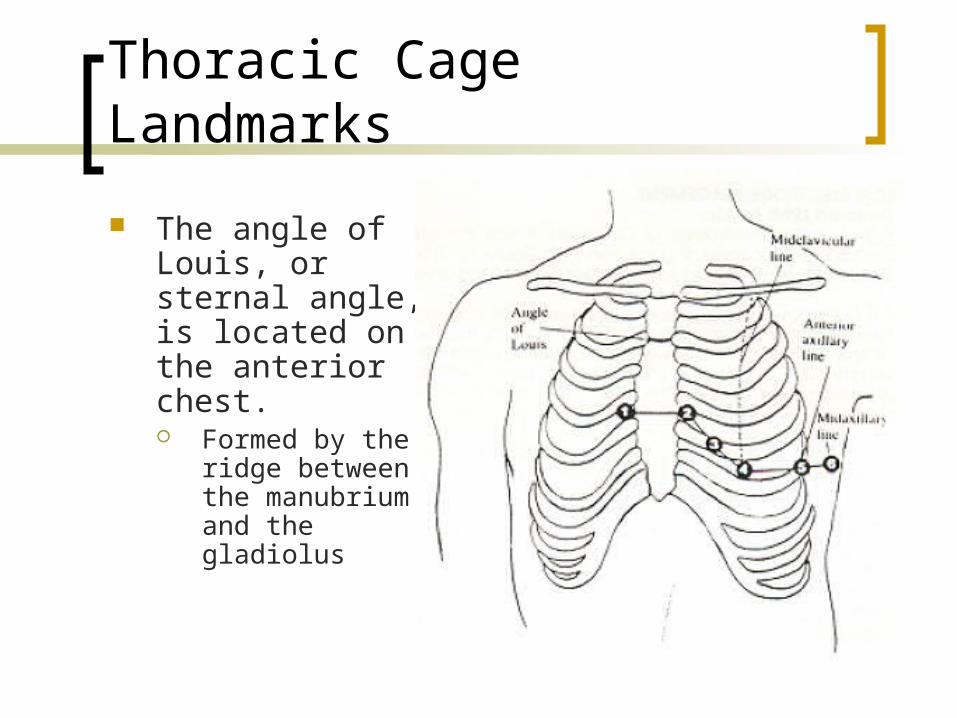
The angle of Louis, or sternal angle, is located on the anterior chest. Formed by the
ridge between the manubrium and the gladiolus
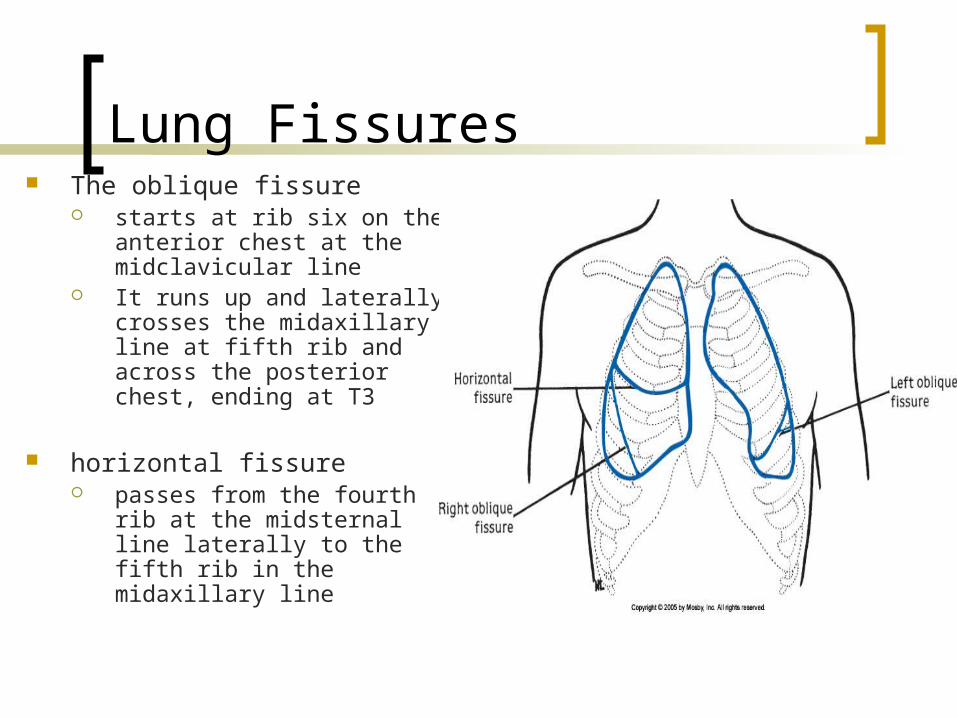
Lung Fissures The oblique fissure
starts at rib six on the anterior chest at the midclavicular line
It runs up and laterally crosses the midaxillary line at fifth rib and across the posterior chest, ending at T3
horizontal fissure passes from the fourth rib at
the midsternal line laterally to the fifth rib in the midaxillary line

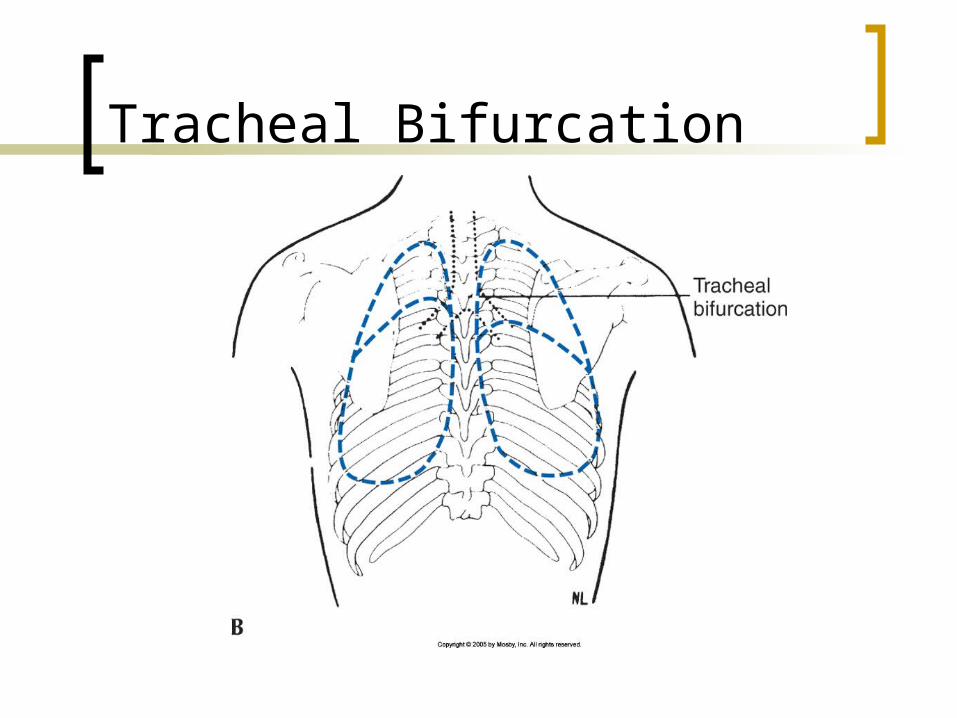
Tracheal Bifurcation
At T4 on posterior chest
At sternal angle on anterior chest
Tracheal Bifurcation

Diaphragm
The diaphragm is a dome-shaped muscle
The top of the dome rests at about the fifth rib anteriorly and at T9 on the posterior chest normally

Lung Borders
On the anterior chest the upper border of the lung extends 2 to 4 cm above the medial third of the clavicles. The inferior border of the lung is at rib six normally

Lung Borders
On the lateral chest the lower margin of the lung is at rib eight

Lung Borders
On the posterior chest the superior border of the lung extends to T1. The inferior border varies with breathing but is usually at about T10
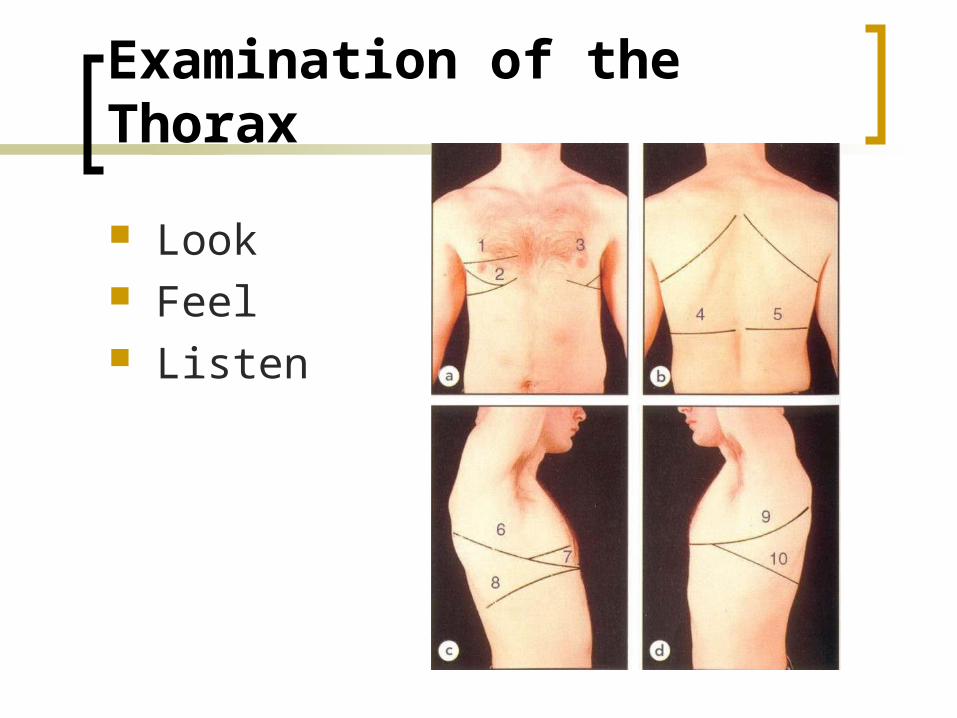
Examination of the Thorax
Look Feel Listen
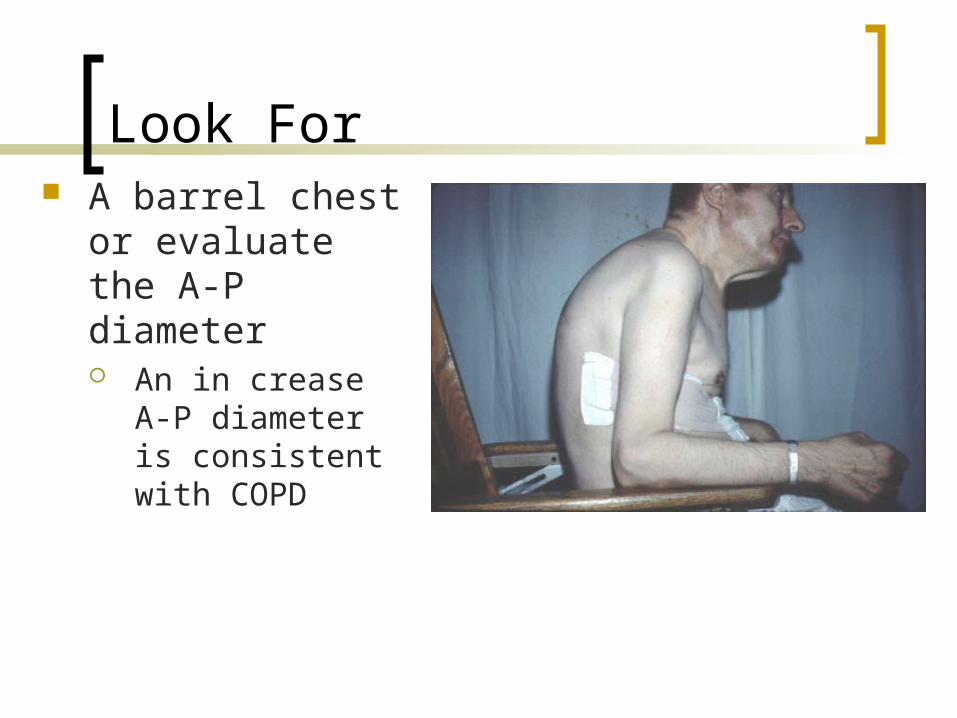
Look For A barrel chest or
evaluate the A-P diameter An in crease A-P
diameter is consistent with COPD
Look For
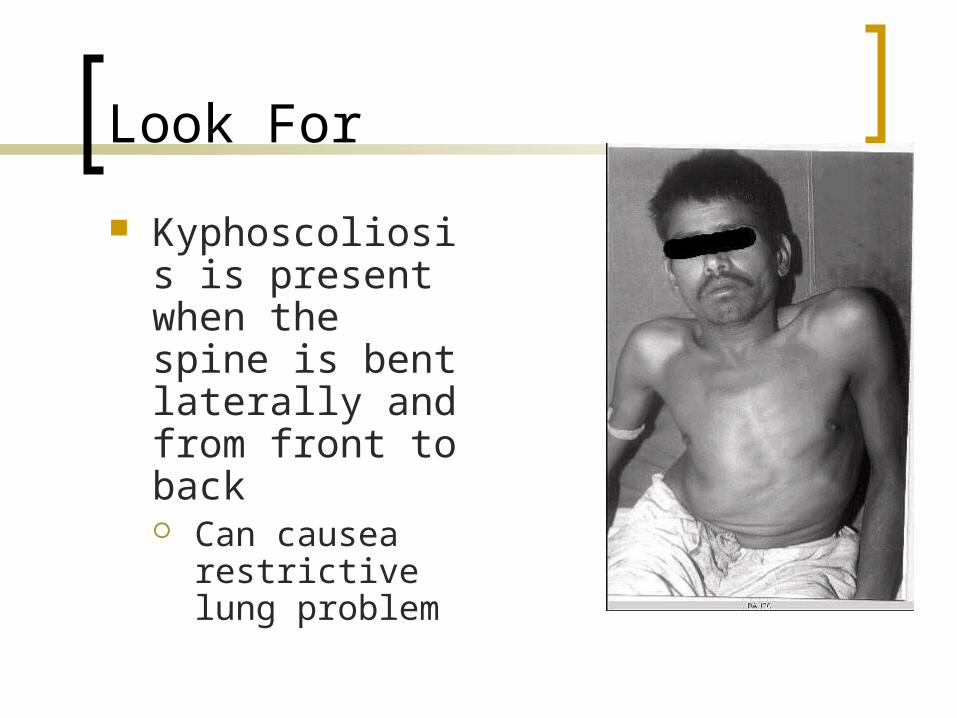
Kyphoscoliosis is present when the spine is bent laterally and from front to back Can causea
restrictive lung problem

Look For
Pectus carinatum is seen as an abnormal sternal protrusion
Look For
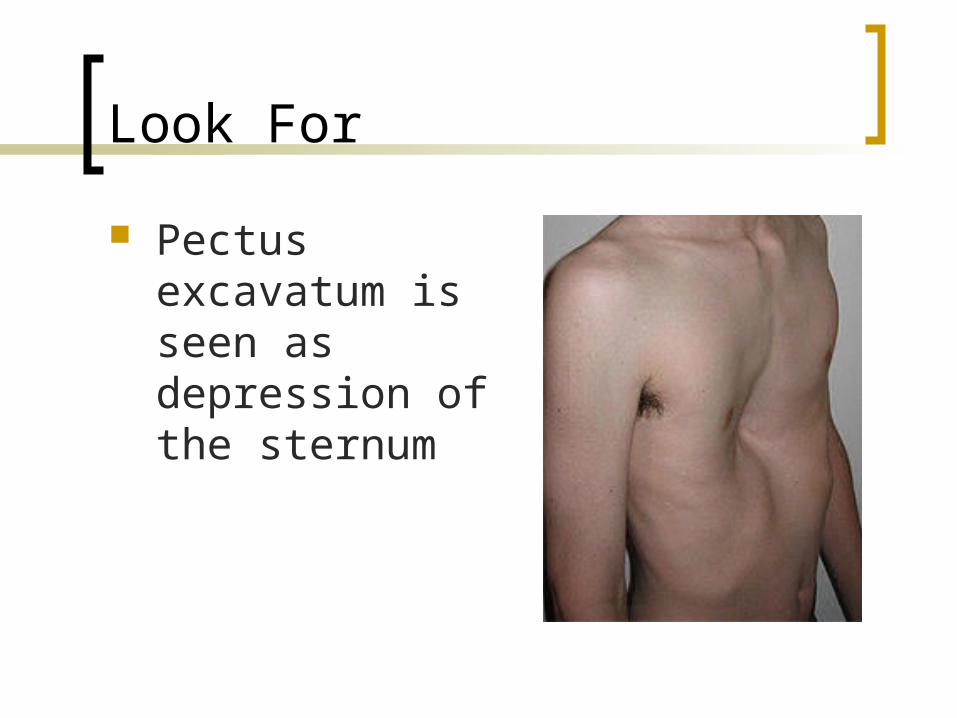
Pectus excavatum is seen as depression of the sternum
Look For
Breathing pattern is important to identify when lung disease is present
Rapid and shallow breathing is consistent with restrictive disease
A prolonged expiratory time is consistent with obstructive lung disease
Retractions are seen as inward depression of the skin around the rib cage with inspiration This suggests a high work of breathing (WOB)
Abdominal paradox is seen as inward movement of the abdomen with inspiration This suggests diaphragm paralysis or fatigue
Hoover’s sign is seen as inward movement of the lateral chest with inspiration. It is a sign of severe COPD.
Feel For (Palpation)
Vocal fremitus is assessed to identify pathologic changes in the lung.
Increased vocal fremitus is consistent with pneumonia and atelectasis.
Decreased vocal fremitus is consistent with lung hyperinflation, pleural disorders, and obesity.
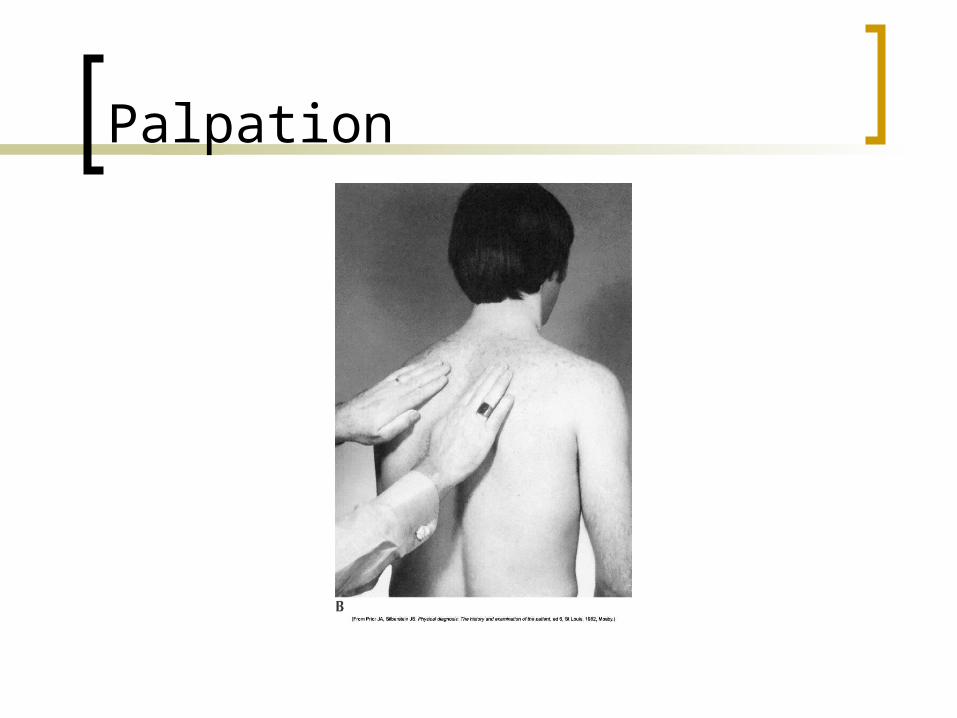
Palpation
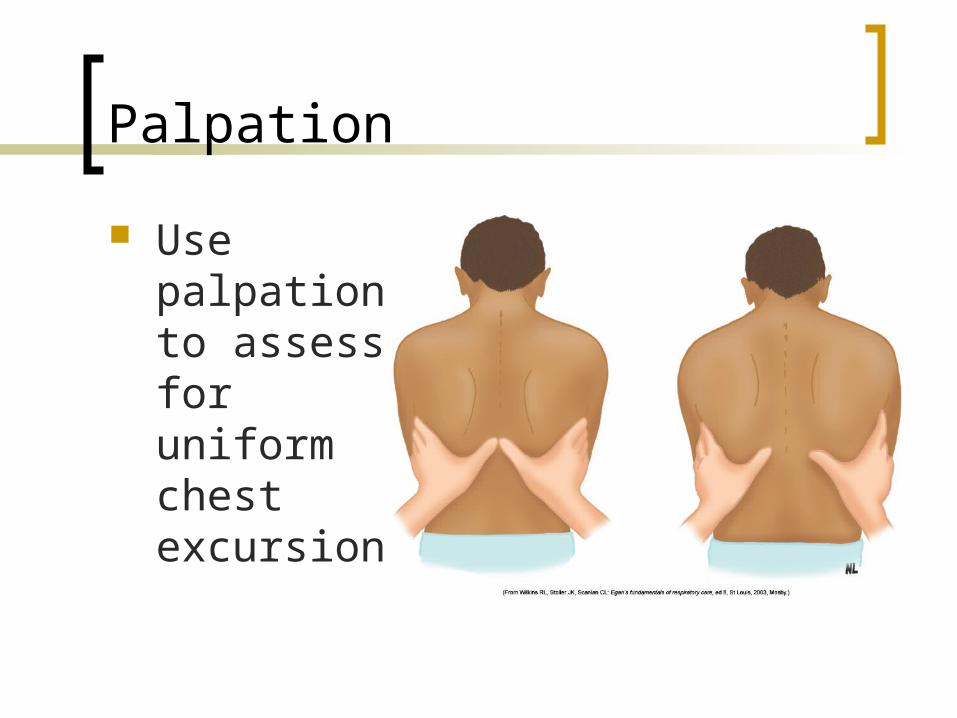
Palpation
Use palpation to assess for uniform chest excursion

Percussion
Percussion is done to determine the condition of the underlying lung.
Increased resonance is heard with pneumothorax and lung hyperinflation.
Decreased resonance is heard with pneumonia and atelectasis.
Related Documents











![Raad - Effects of waterpipe tobacco smoking on lung function [CHEST]](https://static.cupdf.com/doc/110x72/543de436afaf9fb00a8b4c68/raad-effects-of-waterpipe-tobacco-smoking-on-lung-function-chest.jpg)