Online Supplement Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data. © 2016 AMERICAN COLLEGE OF CHEST PHYSICIANS. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians. See online for more details. DOI: 10.1016/j.chest.2015.11.026 Antithrombotic Therapy for VTE Disease CHEST Guideline and Expert Panel Report Clive Kearon, MD, PhD; Elie A. Akl, MD, MPH, PhD; Joseph Ornelas, PhD; Allen Blaivas, DO, FCCP; David Jimenez, MD, PhD, FCCP; Henri Bounameaux, MD; Menno Huisman, MD, PhD; Christopher S. King, MD, FCCP; Timothy A. Morris, MD, FCCP; Namita Sood, MD, FCCP; Scott M. Stevens, MD; Janine R. E. Vintch, MD, FCCP; Philip Wells, MD; Scott C. Woller, MD; and COL Lisa Moores, MD, FCCP CHEST 2016; 149(2):315-352

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Online Supplement
Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
© 2016 AMERICAN COLLEGE OF CHEST PHYSICIANS. Reproduction of this article is prohibited without writtenpermission from the American College of Chest Physicians. See online for more details. DOI: 10.1016/j.chest.2015.11.026
Antithrombotic Therapy for VTE Disease
CHEST Guideline and Expert Panel Report
Clive Kearon, MD, PhD; Elie A. Akl, MD, MPH, PhD; Joseph Ornelas, PhD; Allen Blaivas, DO, FCCP; David Jimenez, MD, PhD, FCCP; Henri Bounameaux, MD; Menno Huisman, MD, PhD; Christopher S. King, MD, FCCP; Timothy A. Morris, MD, FCCP; Namita Sood, MD, FCCP; Scott M. Stevens, MD; Janine R. E. Vintch, MD, FCCP; Philip Wells, MD; Scott C. Woller, MD; and COL Lisa Moores, MD, FCCP
CHEST 2016; 149(2):315-352

Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
Online Supplement

Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
Online Supplement

Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
Online Supplement

Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
Online Supplement

Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
Online Supplement

Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
Online Supplement

Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
Online Supplement

Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
Online Supplement

Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
Online Supplement

Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
Online Supplement
Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
Online Supplement

Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
Online Supplement
151469

Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
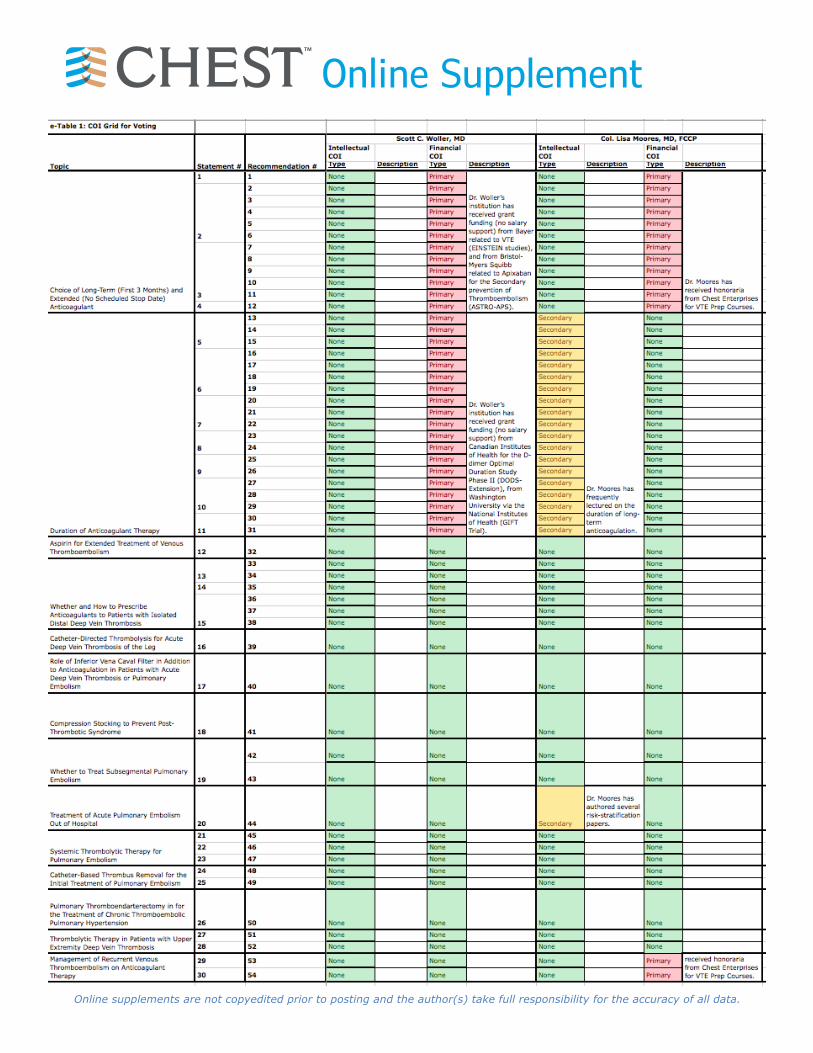
Online Supplemente-Table 2: Structured Clinical Questions
Topic Population Intervention(s) Comparator(s) Outcome(s) Methodology
Choice of Long-Term (First 3 Months) and Extended (No Scheduled Stop Date) Anticoagulant
Patients with acute DVT of the leg or PE.
LMWH, dabigatran, rivaroxaban, apixaban, edoxaban
VKA Recurrent VTE, major bleeding, mortality, QOL and PTS RCTs
Duration of Anticoagulant Therapy Patients with an acute DVT of the leg or PE Longer duration Shorter duration Recurrent VTE, major bleeding,
mortality, QOL and PTS RCTs
Aspirin for Extended Treatment of Venous Thromboembolism
Patients with DVT of the leg or PE who have completed at last 3 month of initial anticoagulation.
Aspirin No antithrombotic, an anticoagulant
Recurrent VTE, major bleeding, mortality, QOL and PTS RCTs
Whether and How to Prescribe Anticoagulants to Patients with Isolated Distal Deep Vein Thrombosis
Patient with acute isolated distal DVT of the leg Anticoagulation No anticoagulation
DVT extension, PE, major bleeding, mortality, QOL and PTS
RCTs
Catheter-Directed Thrombolysis for Acute Deep Vein Thrombosis of the Leg
Patients with acute proximal DVT of the leg Catheter directed thrombolysis
No active thrombus removal or another method of thrombus removal
Recurrent VTE, major bleeding, mortality, QOL and PTS , shorter ICU and hospital stays, and acute complications
RCTs
Role of Inferior Vena Caval Filter in Addition to Anticoagulation in Patients with Acute Deep Vein Thrombosis or Pulmonary Embolism
Patients with acute DVT of the leg or PE started on anticoagulation
IVC filter No IVC filter Recurrent DVT and PE, major bleeding, mortality, QOL, PTS, and acute complications
RCTs and Cohort Studies
Compression Stocking to Prevent Post-Thrombotic Syndrome
Patients with acute DVT of the leg started on anticoagulant treatment
Compression stocking No compression stocking QOL, PTS and recurrent VTE RCTs
Whether to Treat Subsegmental Pulmonary Embolism
Patient with acute isolated subsegmental PE Anticoagulation No anticoagulation Recurrent VTE, major bleeding,
mortality, QOL and PTS RCTs and Cohort Studies
Treatment of Acute Pulmonary Embolism Out of Hospital Patients with acute PE In hospital treatment At home treatment
Recurrent DVT and PE, major bleeding, mortality, QOL and PTS
RCTs
Systemic Thrombolytic Therapy for Pulmonary Embolism Patients with acute PE Thrombolytic therapy No thrombolytic therapy
Recurrent DVT and PE, major bleeding, mortality, QOL and PTS
RCTs
Catheter-Based Thrombus Removal for the Initial Treatment of Pulmonary Embolism Patients with acute PE Use of catheter-assisted
thrombus removal No use of catheter-assisted thrombus removal
Recurrent DVT and PE, major bleeding, mortality, QOL, and acute complications
RCTs and Cohort Studies
Pulmonary Thromboendarterectomy in for the Treatment of Chronic Thromboembolic Pulmonary Hypertension
Patients with chronic thromboembolic pulmonary hypertension
Pulmonary thromboendarterectomy
No pulmonary thromboendarterectomy
Recurrent VTE, major bleeding, mortality, QOL and PTS
RCTs and Cohort Studies
Thrombolytic Therapy in Patients with Upper Extremity Deep Vein Thrombosis
Patients with upper extremity DVT Systemic thrombolytic therapy No systemic thrombolytic
therapy
Recurrent VTE, major bleeding, mortality, QOL and PTS , shorter ICU and hospital stays, and acute complications
RCTs and Cohort Studies
Management of Recurrent Venous Thromboembolism on Anticoagulant Therapy
Patients with recurrent VTE while on anticoagulant therapy
Higher intensity therapy, alternative anticoagulant, use of IVC filter
No change in anticoagulant therapy
Recurrent VTE, major bleeding, mortality, QOL and PTS
RCTs and Cohort Studies

Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
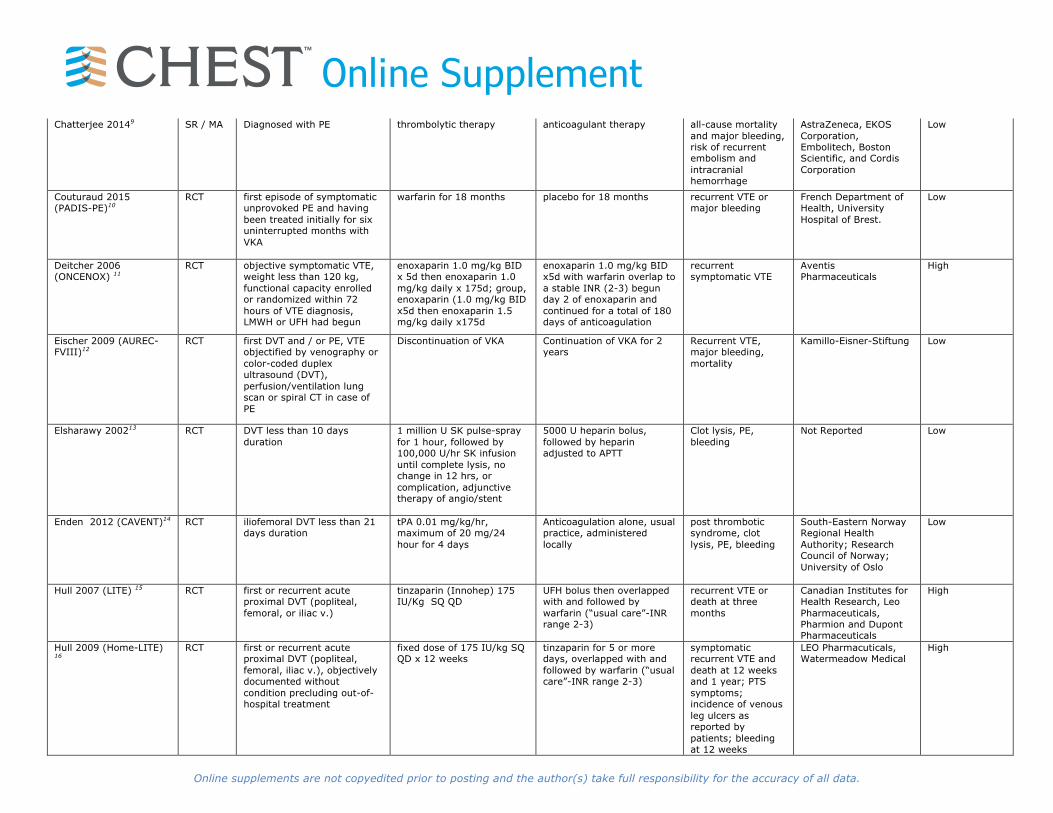
Online Supplemente-Table 3: Evidence Table of Individual Studies and Meta-Analyses Used for Estimates
Study Name Study Design Participants Description Intervention Description Control Description
Outcomes Assessed
Funding and Conflicts of Interest
Risk of Bias Assessment
Agnelli 2001 (WODIT-DVT)1
RCT first episode of symptomatic idiopathic proximal DVT, completed three uninterrupted months of oral anticoagulant therapy without having a recurrence of thromboembolism or bleeding
continuation of oral anticoagulant therapy for nine additional months, dose of warfarin or other oral anticoagulant was adjusted to achieve a target international normalized ratio (INR) between 2.0 and 3.0.
baseline was three months of therapy with warfarin (in 97 percent of the cases) or acenocoumarol; discontinuation of oral anticoagulant therapy was the control
recurrent VTE, major bleeding and death at two years
None Disclosed Low
Agnelli 2003 (WODIT-PE)2
RCT first episode of symptomatic idiopathic proximal DVT, completed three uninterrupted months of oral anticoagulant therapy without having a recurrence of thromboembolism or bleeding
continuation for 3 additional months (PE associated with transient risk factors) or 9 additional months (idiopathic PE), INR between 2.0 and 3.0
baseline was three months of warfarin or acenocoumarol therapy, then discontinuation
recurrent VTE, major bleeding at three months
None Disclosed Low
Agnelli 2013 (AMPLIFY)3 RCT objectively confirmed, symptomatic proximal DVT or PE (with or without DVT)
apixaban 10 mg BID x7 d then 5 mg BID x 6 mo
conventional enoxaparin, followed by warfarin
recurrent VTE, major bleeding and death
Pfizer and Bristol-Myers Squibb
Low
Agnelli 2013 (AMPLIFY-EXT)4
RCT objectively confirmed, symptomatic proximal DVT or PE (with or without DVT)
2.5 mg of apixaban, 5 mg of apixaban, twice daily for was 12 months.
placebo twice daily for 12 months.
recurrent VTE, major bleeding and death
Pfizer and Bristol-Myers Squibb
High
Bauersachs 2010 (EINSTEIN) 5
RCT acute, symptomatic, objectively confirmed proximal DVT, without symptomatic PE
oral rivaroxaban 15 mg twice daily for the first 3 weeks, followed by 20 mg once daily for the intended 3, 6, or 12 months of treatment
subcutaneous enoxaparin, 1.0 mg/kg twice daily, and either warfarin or acenocoumarol
recurrent VTE, major bleeding
Bayer Schering Pharma and Ortho-McNeil
High
Buller 2012 (EINSTEIN–PE) 6
RCT acute, symptomatic pulmonary embolism with objective confirmation, with or without symptomatic DVT
rivaroxaban 15 mg twice daily for the first 3 weeks, followed by 20 mg once daily
enoxaparin 1.0 mg/kg of body weight twice daily and either warfarin or acenocoumarol
recurrent VTE, major bleeding
Bayer Health- Care and Janssen Pharmaceuticals
Low
Buller 2013 (Hokusai) 7 RCT objectively diagnosed, acute, symptomatic deep-vein thrombosis involving the popliteal, femoral, or iliac veins or acute, symptomatic pulmonary embolism (with or without DVT)
heparin or LMWH followed by edoxaban 60 mg orally once daily, (30 mg once daily in patients with a CC 30-50 ml/min or <=60 kg or potent P-glycoprotein inhibitors)
heparin or LMWH followed by warfarin
recurrent VTE, major bleeding
Daiichi-Sankyo Low
Campbell 20078 RCT DVT and/or PE six months of anticoagulation with heparin for five days accompanied and followed by warfarin, with a target international normalised ratio of 2.0-3.5.
three months of anticoagulation with heparin for five days accompanied and followed by warfarin, with a target international normalised ratio of 2.0-3.5.
Recurrent VTE, major bleeding and death
Pfizer
Low
Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
Online SupplementChatterjee 20149 SR / MA Diagnosed with PE thrombolytic therapy anticoagulant therapy all-cause mortality
and major bleeding, risk of recurrent embolism and intracranial hemorrhage
AstraZeneca, EKOS Corporation, Embolitech, Boston Scientific, and Cordis Corporation
Low
Couturaud 2015 (PADIS-PE)10
RCT first episode of symptomatic unprovoked PE and having been treated initially for six uninterrupted months with VKA
warfarin for 18 months placebo for 18 months recurrent VTE or major bleeding
French Department of Health, University Hospital of Brest.
Low
Deitcher 2006 (ONCENOX) 11
RCT objective symptomatic VTE, weight less than 120 kg, functional capacity enrolled or randomized within 72 hours of VTE diagnosis, LMWH or UFH had begun
enoxaparin 1.0 mg/kg BID x 5d then enoxaparin 1.0 mg/kg daily x 175d; group, enoxaparin (1.0 mg/kg BID x5d then enoxaparin 1.5 mg/kg daily x175d
enoxaparin 1.0 mg/kg BID x5d with warfarin overlap to a stable INR (2-3) begun day 2 of enoxaparin and continued for a total of 180 days of anticoagulation
recurrent symptomatic VTE
Aventis Pharmaceuticals
High
Eischer 2009 (AUREC-FVIII)12
RCT first DVT and / or PE, VTE objectified by venography or color-coded duplex ultrasound (DVT), perfusion/ventilation lung scan or spiral CT in case of PE
Discontinuation of VKA Continuation of VKA for 2 years
Recurrent VTE, major bleeding, mortality
Kamillo-Eisner-Stiftung Low
Elsharawy 200213 RCT DVT less than 10 days duration
1 million U SK pulse-spray for 1 hour, followed by 100,000 U/hr SK infusion until complete lysis, no change in 12 hrs, or complication, adjunctive therapy of angio/stent
5000 U heparin bolus, followed by heparin adjusted to APTT
Clot lysis, PE, bleeding
Not Reported Low
Enden 2012 (CAVENT)14 RCT iliofemoral DVT less than 21 days duration
tPA 0.01 mg/kg/hr, maximum of 20 mg/24 hour for 4 days
Anticoagulation alone, usual practice, administered locally
post thrombotic syndrome, clot lysis, PE, bleeding
South-Eastern Norway Regional Health Authority; Research Council of Norway; University of Oslo
Low
Hull 2007 (LITE) 15 RCT first or recurrent acute proximal DVT (popliteal, femoral, or iliac v.)
tinzaparin (Innohep) 175 IU/Kg SQ QD
UFH bolus then overlapped with and followed by warfarin (“usual care”-INR range 2-3)
recurrent VTE or death at three months
Canadian Institutes for Health Research, Leo Pharmaceuticals, Pharmion and Dupont Pharmaceuticals
High
Hull 2009 (Home-LITE) 16
RCT first or recurrent acute proximal DVT (popliteal, femoral, iliac v.), objectively documented without condition precluding out-of-hospital treatment
fixed dose of 175 IU/kg SQ QD x 12 weeks
tinzaparin for 5 or more days, overlapped with and followed by warfarin (“usual care”-INR range 2-3)
symptomatic recurrent VTE and death at 12 weeks and 1 year; PTS symptoms; incidence of venous leg ulcers as reported by patients; bleeding at 12 weeks
LEO Pharmacuticals, Watermeadow Medical
High

Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
Online SupplementKahn 2014 (SOX) 17 RCT first symptomatic proximal
DVT compression stockings: below knee 30-40 mm Hg
placebo stockings PTS at 6 -24 months (Ginsberg's criteria); PTS score (Villalta)
Canadian Institutes of Health Research, Sigvaris.
Low
Kahn 2014 (SOX 2) 18 RCT first symptomatic proximal DVT
compression stockings: below knee 30-40 mm Hg
placebo stockings acute leg pain Canadian Institutes of Health Research, Sigvaris.
Low
Lee 2003 (CLOT) 19 RCT active cancer and newly diagnosed, symptomatic proximal DVT and/or PE
200 IU of dalteparin per kilogram (max daily dose, 18,000 IU) daily for the first month. Then 75-83% of the full dose (~150 IU/kg) x 5mo.
dalteparin initially for 5-7d and a VKA for 6 mo. dose adjusted to target IN 2.5 (range 2-3), dalteparin was d/ced after a >/= 5d and once the INR had remained above 2.0 for two consecutive days
objective symptomatic recurrent VTE, major bleeding and death at six months
Pharmacia High
Lee 2015 (CATCH)20
RCT active cancer and newly diagnosed, symptomatic proximal DVT and/or PE
tinzaparin 175 IU/kg once daily for 6 months
initial tinzaparin 175 IU/kg once daily for 5-10 days overlapped and followed by dose-adjusted warfarin (target INR 2.0-3.0) for 6 months
recurrent VTE and major bleeding
Bayer, Bristol-Myers Low
Lopaciuk 199921 RCT phlebographically proven acute proximal DVT
nadroparin fixed dose 85 anti-Xa IU/kg s.c. BID x 10d then 85 anti-Xa IU/kg sq daily
initial nadroparin fixed dose 85 anti-Xa IU/kg BIX x 10 d then w/ acenocoumarol adjusted to INR 2-3
clinical overt radiographically confirmed DVT
Not Reported High
Lopez-Beret 200122 RCT consecutive symptomatic DVT referred to the vascular laboratory in one hospital in whom lower limb DVT was objectively documented with duplex scan examination
nadroparin adjusted to body weight (0.1 mL/10kg)
acenocoumarol administered daily starting on the 3rd day with an initial dose of 4 mg then adjusted to INR 2-3
recurrent VTE and major bleeding
Not Reported High
Meyer 200223 RCT cancer of any type and PE and/or DVT
enoxaparin 1.5mg/kg SQ daily x 3 mo. w/out dose adjustment
enoxaparin 1.5mg/kg SQ daily + warfarin until INR >2 on 2 consecutive days after at least 4 injections. Target INR 2-3
recurrent VTE, major hemorrhage and death at three months
Aventis Pharmaceuticals
High
Mismetti 2015 (PREPIC 2)24
RCT hospitalized with acute, symptomatic pulmonary embolism associated with lower-limb vein thrombosis and at least one criterion for severity, scheduled to receive anticoagulant therapy for at least six months
insertion and later withdrawal of a retrievable inferior vena cava filter
no filter symptomatic recurrent PE at three months, recurrent PE at six months, symptomatic DVTs, major bleeding and death at three and six months, and filter complications
University Hospital of Saint-Etienne
Low

Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
Online SupplementPinede 2001 (DOTAVK)25
RCT written informed consent, and symptomatic C-DVT, P-DVT, or PE that was confirmed by positive Doppler ultrasonography or venography
6 weeks for isolated C-DVT with a long course of therapy, 6 months for P-DVT/PE; 12 weeks for C-DVT
short oral anticoagulant course (3 months for proximal DVT and/or PE
recurrences and major, minor, or fatal bleeding complications
French Ministry of Health, Hospices Civils de Lyon, Conseil Régional Rhône-Alpes, and the Association pour la recherche et l’évaluation thérapeutique (APRET)
Low
Piran 201326 SR / MA diagnosed with a PE outpatient antithrombotic treatment
inpatient recurrent VTE, rate of recurrent VTE, major bleeding
American Society of Hematology, Heart and Stroke Foundation of Canada, Heart and Stroke Foundation of Ontario
High
Prins 201327 SR / MA symptomatic DVT and/or PE rivaroxaban 15mg BID x 21d then 20mg daily
enoxaparin plus VKA (INR 2-3)
symptomatic recurrent VTE (composite of fatal or nonfatal PE or DVT), clinically relevant bleeding ( composite of major and non-major clinically relevant bleeding)
Bayer HealthCare and Janssen Pharmaceuticals
Low
Romera 200928 RCT referred to the vascular surgery department with first episode acute proximal leg DVT
tinzaparin SQ in a fixed dose of 175 IU anti-Xa per kg of body weight once daily x 6 mo.
3 mg of acenocoumarol adjusted to (INR 2-3) x 6 mo
first symptomatic DVT or PE at six months and one year, major bleeding at 6-mo
Leo Pharmaceutical Products
High
Schulman 2013 (REMEDY and RESONATE) 29
RCT objectively confirmed, symptomatic, proximal DVT or PE that had already been treated with an approved anticoagulant or if they had received dabigatran in the RE-COVER or RE-COVER II studies
dabigatran at a fixed dose of 150 mg twice daily and warfarin-like placebo
active warfarin titrated to INR 2-3 with a POC device that that provided an encrypted. INR and a dabigatran-like placebo
recurrent symptomatic and objective VTE or death associated with VTE
Boehringer-Ingelheim Low
Schulman 2009 (RECOVER 1)30
RCT acute VTE treated with LMWH or UFH for median of 9 days, objectively diagnosed proximal DVT or PE
dabigatran 150 mg twice daily
warfarin. recurrent symptomatic, objectively confirmed VTE and related deaths at 6 months
Boehringer-Ingelheim Low
Schulman 2014 (RECOVER 2) (Joint Analysis with RECOVER 1) 31
RCT acute VTE treated with LMWH or UFH for 5 to 11 days, objectively diagnosed proximal DVT or PE
dabigatran 150 mg twice daily
warfarin. recurrent symptomatic, objectively confirmed VTE and related deaths at 6 months
Boehringer-Ingelheim Low

Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
Online SupplementSimes 201432 SR / MA first unprovoked VTE aspirin placebo recurrent VTE,
major vascular events (recurrent VTE, MI, stroke and CVD death) and bleeding
National Health and Medical Research Council, New Zealand Health Research Council, New South Wales Health, and Australian Society of Thrombosis and Haemostasis. University of Perugia, Bayer HealthCare
Low
Siragusa 2008 (DACUS)33
RCT With residual vein thrombosis and documented idiopathic and provoked proximal DVT
Oral anticoagulant treatment for 12 months
Oral anticoagulant treatment for 3 months
Recurrence and major bleeding
None Low
Watson 201434 SR / MA acute DVT of lower limb thrombolytic therapy and anticoagulation
anticoagulation alone PE recurrent VTE, major bleeding, post-thrombotic complications, venous patency and venous function
None Low

Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
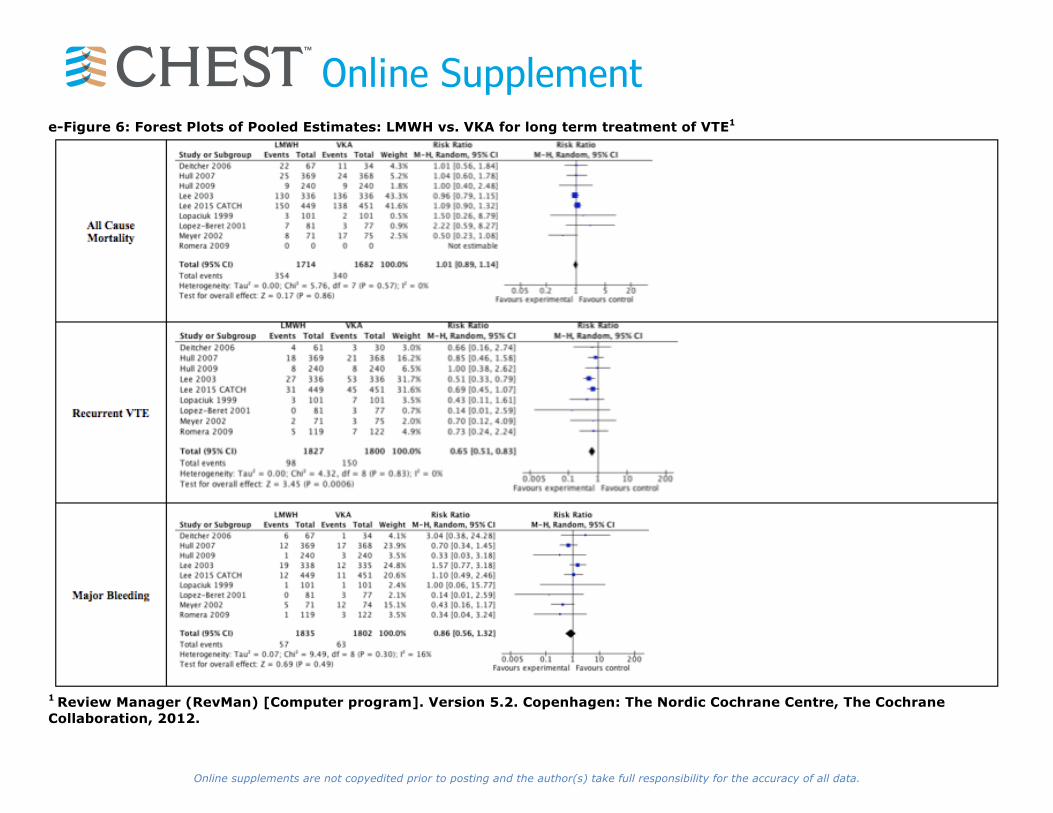
Online Supplemente-Table 4: Evidence Profile - LMWH vs VKA for long term treatment of VTE 1
Bibliography: Deitcher et al. (ONCENOX)11, Hull et al. (LITE)15, Hull et al. (LITE Home)16, Lee et al. (CLOT)19, Lopaciuk et al.21, Lopez-Beret et al.22, Meyer et al.23, Romera et al.28, Lee et al. (CATCH)20 Quality assessment Summary of Findings Participants (studies) Follow up
Risk of bias
Inconsistency Indirectness Imprecision Publication bias
Overall quality of evidence
Study event rates (%)
Relative effect (95% CI)2
Anticipated absolute effects
With VKA
With LMWH
Risk with VKA
Risk difference with LMWH (95% CI)
All Cause Mortality (IMPORTANT OUTCOME) 3396 (9 studies) 6 months
Serious3 no serious inconsistency
no serious indirectness
no serious imprecision
undetected ⊕⊕⊕⊝ MODERATE3 due to risk of bias
340/1682 (20.2%)
354/1714 (20.7%)
RR 1.01 (0.89 to 1.14)
Non-Cancer4 17 per 1000
0 more per 1000 (from 2 fewer to 2 more)
Non-Metastatic Cancer4 42 per 1000
0 more per 1000 (from 5 fewer to 6 more)
Metastatic Cancer4 253 per 1000
3 more per 1000 (from 28 fewer to 35 more)
Recurrent VTE (CRITICAL OUTCOME) 3627 (9 studies) 6 months
Serious5 no serious inconsistency
no serious indirectness
no serious imprecision
undetected ⊕⊕⊕⊝ MODERATE5 due to risk of bias
150/1800 (8.3%)
98/1827 (5.4%)
RR 0.65 (0.51 to 0.83)
Low6 30 per 1000
11 fewer per 1000 (from 5 fewer to 15 fewer)
Moderate6 80 per 1000
28 fewer per 1000 (from 14 fewer to 39 fewer)
High6 200 per 1000
70 fewer per 1000 (from 34 fewer to 98 fewer)
Major bleeding (CRITICAL OUTCOME) 3637 (9 studies) 6 months
no serious risk of bias
no serious inconsistency
no serious indirectness
Serious7,8 undetected ⊕⊕⊕⊝ MODERATE7,8 due to imprecision
63/1802 (3.5%)
57/1835 (3.1%)
RR 0.86 (0.56 to 1.32)
Low9 20 per 1000
3 fewer per 1000 (from 9 fewer to 6 more)
High9 80 per 1000
11 fewer per 1000 (from 35 fewer to 26 more)
1 The initial parenteral anticoagulation was similar in both arms for all except one study (Hull et al.15) in which patients randomized to LMWH received initially the same LWMH whereas patients randomized to VKA received initially UFH 2 The relative effect (RR; 95% CI) of LMWH versus VKA was assessed, and compared, in the subgroup of trials that enrolled patients without (Hull et al. (LITE)15, Lopez-Beret et al..22) and with (Deitcher et al. (ONCENOX)11, Hull et al. (LITE)15, Lee et al. (CLOT)19, Lee et al. (CATCH)20, Lopez-Beret et al.22, Meyer et al.23) cancer: Recurrent VTE: cancer RR 0.59 (0.44 to 0.78) vs. no cancer RR 0.99 (0.46 to 2.13); P=0.21 for subgroup difference. Major Bleeding: cancer RR 0.96 (0.65 to 1.42) vs. no cancer RR 0.43 (0.17 to 1.17); P=0.14 for subgroup difference. All Cause Mortality: cancer RR 1.00 (0.88 to 1.33) vs. no cancer RR 1.85 (0.59 to 5.77); P=0.29 for subgroup difference. 3 One study did not report deaths, which is unusual and could reflect selective reporting of outcomes.

Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
Online Supplement4 Low corresponds to patients without cancer and patients with non-metastatic cancer. High corresponds to patients with metastatic cancer. These control event rates were derived from the RIETE registry (an ongoing prospective registry of consecutive patients with acute VTE) (Prandoni et al.35) 5 None of the studies was blinded while the diagnosis of recurrent VTE has a subjective component and there could be a lower threshold for diagnosis of recurrent VTE in VKA-treated patients as switching the treatment of such patients to LMWH is widely practiced. At the same time, there is reluctance to diagnose recurrent VTE in patients who are already on LMWH as there is no attractive alternative treatment option. 6 Risk of recurrent VTE: Low corresponds to patients without cancer (3% estimate taken from recent large RCTs of acute treatment), intermediate to patients with local or recently resected cancer (appears to be consistent with Prandoni [particularly if low risk is increased to 4%]), and high to patients with locally advanced or distant metastatic cancer. (Prandoni et al.36) 7 Confidence interval includes both no effect and harm with LMWH
8 95% confidence intervals for the risk ratio for major bleeding includes a potentially clinically important increase or decrease with LMWH, and may also vary with the dose of LMWH used during the extended phase of therapy 9 Risk of bleeding: Low corresponds to patients without risk factor for bleeding (i.e., > 75 years, cancer, metastatic disease; chronic renal or hepatic failure; platelet count <80,0000; requires antiplatelet therapy; history of bleeding without a reversible cause). (Prandoni et al.35, Byeth et al.37)

Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
Online Supplemente-Table 5: Evidence Profile - Dabigatran vs VKA for long-term treatment of VTE 1,2
Bibliography: Schulman et al. (RE-COVER I & II)31 Quality assessment Summary of Findings Participants (studies) Follow up
Risk of bias
Inconsistency Indirectness Imprecision Publication bias
Overall quality of evidence
Study event rates (%) Relative effect (95% CI)
Anticipated absolute effects With VKA
With Dabigatran
Risk with VKA
Risk difference with Dabigatran (95% CI)
All Cause Mortality (CRITICAL OUTCOME) 5107 (2 studies)
no serious risk of bias
no serious inconsistency
no serious indirectness
serious3 undetected ⊕⊕⊕⊝ MODERATE3 due to imprecision
46/2554 (1.8%)4
46/2553 (1.8%)
RR 1.0 (0.67 to 1.5)4
18 per 10004
0 fewer per 1000 (from 6 fewer to 9 more)
Recurrent VTE (CRITICAL OUTCOME) 5107 (2 studies)
no serious risk of bias
no serious inconsistency
no serious indirectness
serious3 undetected ⊕⊕⊕⊝ MODERATE3 due to imprecision
55/2554 (2.2%)4
60/2553 (2.4%)
RR 1.12 (0.77 to 1.62)4
22 per 10004
3 more per 1000 (from 5 fewer to 13 more)
Major Bleeding (CRITICAL OUTCOME) 5107 (2 studies)
no serious risk of bias
no serious inconsistency
no serious indirectness
serious3 undetected ⊕⊕⊕⊝ MODERATE3 due to imprecision
51/2554 (2%)4
37/2553 (1.4%)
RR 0.73 (0.48 to 1.1)4
20 per 10004
5 fewer per 1000 (from 10 fewer to 2 more)
1 Dabigatran 150 mg twice daily vs. warfarin 2 Patients with acute VTE treated initially with low-molecular-weight or unfractionated heparin 3 CI includes values suggesting no effect and values suggesting either benefit or harm
4 Pooled analysis of Schulman et al. (Re-Cover I)30 and Schulman et al. (Re-Cover II)31 performed by Schulman et al.31

Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
Online Supplemente-Table 6: Evidence Profile - Rivaroxaban vs LMWH and VKA for acute and long-term treatment of VTE1,2
Bibliography: Prins et al.27 Quality assessment Summary of Findings Participants (studies) Follow up
Risk of bias
Inconsistency Indirectness Imprecision Publication bias
Overall quality of evidence
Study event rates (%) Relative effect (95% CI)
Anticipated absolute effects With LMWH and VKA
With Rivaroxaban
Risk with LMWH and VKA
Risk difference with Rivaroxaban (95% CI)
All Cause Mortality (CRITICAL OUTCOME) 8281 (2 studies) 3 months
no serious risk of bias
no serious inconsistency
no serious indirectness
serious4 undetected ⊕⊕⊕⊝ MODERATE3 due to imprecision
99/4131 (2.4%)4
96/4150 (2.3%)
RR 0.97 (0.73 to 1.27)
24 per 10004
1 fewer per 1000 (from 6 fewer to 6 more)
Recurrent VTE (CRITICAL OUTCOME) 8281 (2 studies) 3 months
no serious risk of bias
no serious inconsistency
no serious indirectness
serious4 undetected ⊕⊕⊕⊝ MODERATE3 due to imprecision
95/4131 (2.3%)4
86/4150 (2.1%)
RR 0.90 (0.68 to 1.2)
23 per 10004
2 fewer per 1000 (from 7 fewer to 5 more)
Major Bleeding (CRITICAL OUTCOME) 8246 (2 studies) 3 months
no serious risk of bias
no serious inconsistency
no serious indirectness
no serious imprecision
undetected ⊕⊕⊕⊕ HIGH
72/4116 (1.7%)4
40/4130 (0.97%)
RR 0.55 (0.38 to 0.81)
17 per 10004
8 fewer per 1000 (from 3 fewer to 11 fewer)
1 Rivaroxaban 20 mg daily for 6 or 12 month after initial long-term therapy 2 Included patients had acute, symptomatic, objectively verified proximal deep-vein thrombosis of the legs or PE (unprovoked 73%; cancer 5%; previous VTE 19%) 3 CI includes values suggesting no effect and values suggesting either benefit or harm 4 Pooled analysis of Bauersachs et al. (EINSTEIN-DVT)5 and Buller et al. (EINSTEIN-PE)6 performed by Prins et al.27
Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
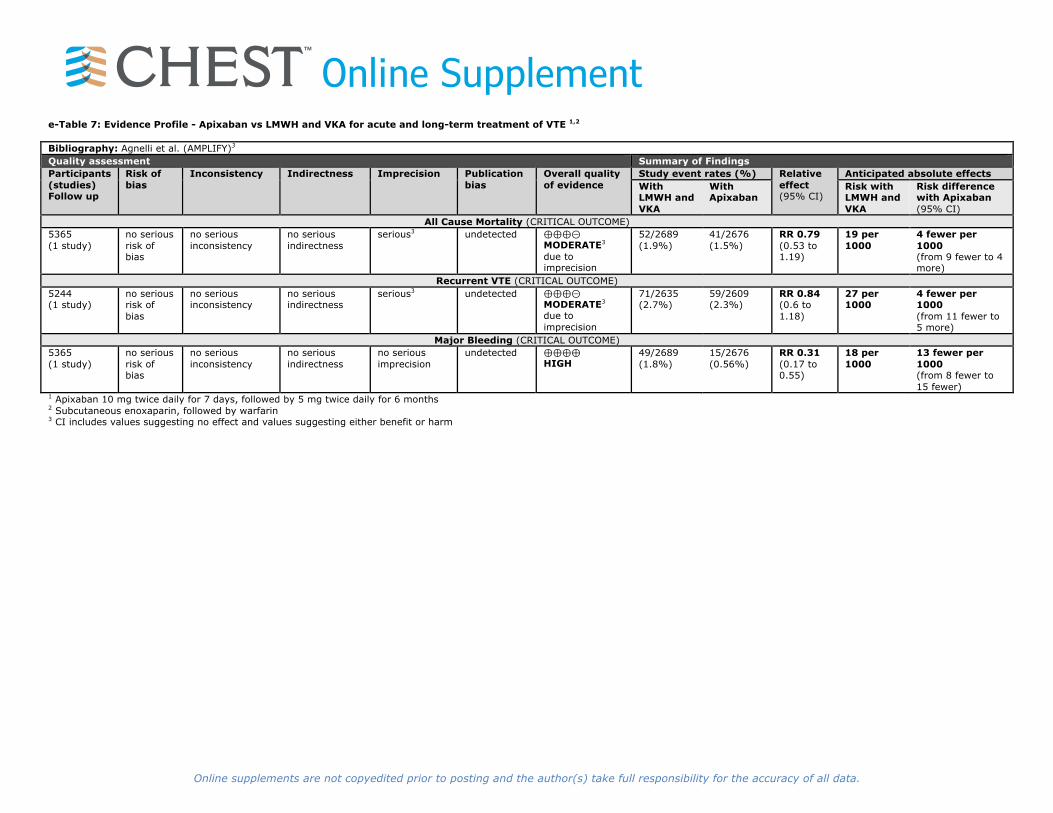
Online Supplemente-Table 7: Evidence Profile - Apixaban vs LMWH and VKA for acute and long-term treatment of VTE 1,2
Bibliography: Agnelli et al. (AMPLIFY)3 Quality assessment Summary of Findings Participants (studies) Follow up
Risk of bias
Inconsistency Indirectness Imprecision Publication bias
Overall quality of evidence
Study event rates (%) Relative effect (95% CI)
Anticipated absolute effects With LMWH and VKA
With Apixaban
Risk with LMWH and VKA
Risk difference with Apixaban (95% CI)
All Cause Mortality (CRITICAL OUTCOME) 5365 (1 study)
no serious risk of bias
no serious inconsistency
no serious indirectness
serious3 undetected ⊕⊕⊕⊝ MODERATE3 due to imprecision
52/2689 (1.9%)
41/2676 (1.5%)
RR 0.79 (0.53 to 1.19)
19 per 1000
4 fewer per 1000 (from 9 fewer to 4 more)
Recurrent VTE (CRITICAL OUTCOME) 5244 (1 study)
no serious risk of bias
no serious inconsistency
no serious indirectness
serious3 undetected ⊕⊕⊕⊝ MODERATE3 due to imprecision
71/2635 (2.7%)
59/2609 (2.3%)
RR 0.84 (0.6 to 1.18)
27 per 1000
4 fewer per 1000 (from 11 fewer to 5 more)
Major Bleeding (CRITICAL OUTCOME) 5365 (1 study)
no serious risk of bias
no serious inconsistency
no serious indirectness
no serious imprecision
undetected ⊕⊕⊕⊕ HIGH
49/2689 (1.8%)
15/2676 (0.56%)
RR 0.31 (0.17 to 0.55)
18 per 1000
13 fewer per 1000 (from 8 fewer to 15 fewer)
1 Apixaban 10 mg twice daily for 7 days, followed by 5 mg twice daily for 6 months 2 Subcutaneous enoxaparin, followed by warfarin 3 CI includes values suggesting no effect and values suggesting either benefit or harm

Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
Online Supplemente-Table 8: Evidence Profile - Edoxaban vs VKA for acute and long-term treatment of VTE 1,2
Bibliography: Buller et al. (Hokusai)7 Quality assessment Summary of Findings Participants (studies) Follow up
Risk of bias
Inconsistency Indirectness Imprecision Publication bias
Overall quality of evidence
Study event rates (%) Relative effect (95% CI)
Anticipated absolute effects With VKA
With Edoxaban
Risk with VKA
Risk difference with Edoxaban (95% CI)
All Cause Mortality (CRITICAL OUTCOME) 8240 (1 study)
no serious risk of bias
no serious inconsistency
no serious indirectness
serious3 undetected ⊕⊕⊕⊝ MODERATE3 due to imprecision
126/4122 (3.1%)4
132/4118 (3.2%)
RR 1.05 (0.82 to 1.33)
31 per 10004
2 more per 1000 (from 6 fewer to 10 more)
Recurrent VTE (CRITICAL OUTCOME) 8240 (1 study)
no serious risk of bias
no serious inconsistency
no serious indirectness4
serious3 undetected ⊕⊕⊕⊝ MODERATE3,4 due to imprecision
146/4122 (3.5%)
130/4118 (3.2%)
RR 0.83 (0.57 to 1.21)
35 per 1000
6 fewer per 1000 (from 15 fewer to 7 more)
Major Bleeding (CRITICAL OUTCOME) 8240 (1 study)
no serious risk of bias
no serious inconsistency
no serious indirectness
serious3 undetected ⊕⊕⊕⊝ MODERATE3 due to imprecision
66/4122 (1.6%)
56/4118 (1.4%)
RR 0.85 (0.6 to 1.21)
16 per 1000
2 fewer per 1000 (from 6 fewer to 3 more)
1 Edoxaban 60 mg once daily, or 30 mg once daily if patients with creatinine clearance of 30 to 50 ml per minute or a body weight below 60 kg
2 Patients with acute VTE who had initially received heparin 3 CI includes values suggesting no effect and values suggesting either benefit or harm 4 Death, with PE not ruled out

Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
Online Supplemente-Table 9: Evidence Profile - Dabigatran vs VKA for extended treatment of VTE 1,2,3,4
Bibliography: Schulman et al. (REMEDY)29 Quality assessment Summary of Findings Participants (studies) Follow up
Risk of bias
Inconsistency Indirectness Imprecision Publication bias
Overall quality of evidence
Study event rates (%) Relative effect (95% CI)
Anticipated absolute effects With VKA
With Dabigatran
Risk with VKA
Risk difference with Dabigatran (95% CI)
All Cause Mortality (CRITICAL OUTCOME) 2856 (1 study)
no serious risk of bias5
no serious inconsistency
no serious indirectness
serious6 undetected ⊕⊕⊕⊝ MODERATE 5,6 due to imprecision
19/1426 (1.3%)
17/1430 (1.2%)
RR 0.89 (0.47 to 1.71)
13 per 1000
1 fewer per 1000 (from 7 fewer to 9 more)
Recurrent VTE (CRITICAL OUTCOME) 2856 (1 study)
no serious risk of bias5
no serious inconsistency
no serious indirectness7
serious6 undetected ⊕⊕⊕⊝ MODERATE5,6,7 due to imprecision
18/1426 (1.3%)
26/1430 (1.8%)
RR 1.44 (0.79 to 2.62)
13 per 1000
6 more per 1000 (from 3 fewer to 20 more)
Major Bleeding (CRITICAL OUTCOME) 2856 (1 study)
no serious risk of bias5
no serious inconsistency
no serious indirectness
serious6 undetected ⊕⊕⊕⊝ MODERATE5,6 due to imprecision
25/1426 (1.8%)
13/1430 (0.91%)
RR 0.52 (0.27 to 1.01)
18 per 1000
8 fewer per 1000 (from 13 fewer to 0 more)
1 Included patients had acute, symptomatic, objectively verified proximal DVT of the legs or PE 2 Dabigatran 150 mg twice daily taken orally for 6 months after an initial treatment with LMWH or IV UFH 3 Warfarin adjusted to achieve an INR of 2.0 to 3.0 for 6 months after an initial treatment with LMWH or IV UFH 4 Active-Control study outcomes used from Schulman et al. (REMEDY)29 5 Allocation was concealed. Patients, providers, data collectors and outcome adjudicators were blinded. Modified ITT analysis. 1.1% loss to follow-up. Not stopped early for benefit. 6 CI includes values suggesting no effect and values suggesting either benefit or harm 7 Primary end point was composite of recurrent or fatal VTE or unexplained death

Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
Online Supplement e-Table 10: Evidence Profile - Dabigatran vs Placebo for extended treatment of VTE 1,2,3
Bibliography: Schulman et al. (RESONATE)29 Quality assessment Summary of Findings Participants (studies) Follow up
Risk of bias
Inconsistency Indirectness Imprecision Publication bias
Overall quality of evidence
Study event rates (%) Relative effect (95% CI)
Anticipated absolute effects With Placebo
With Dabigatran
Risk with Placebo
Risk difference with Dabigatran (95% CI)
All Cause Mortality (CRITICAL OUTCOME) 1343 (1 study)
no serious risk of bias
no serious inconsistency
no serious indirectness
serious4 undetected ⊕⊕⊕⊝ MODERATE4 due to imprecision
2/662 (0.3%)
0/681 (0%)
- - 3 fewer per 1000 (from 11 fewer to 3 more)
Recurrent VTE (CRITICAL OUTCOME) 1343 (1 study)
no serious risk of bias
no serious inconsistency
no serious indirectness
no serious imprecision
undetected ⊕⊕⊕⊕ HIGH
37/662 (5.6%)
3/681 (0.44%)
RR 0.08 (0.02 to 0.25)
56 per 1000
51 fewer per 1000 (from 42 fewer to 55 fewer)
Major Bleeding (CRITICAL OUTCOME) 1343 (1 study)
no serious risk of bias
no serious inconsistency
no serious indirectness
serious4 undetected ⊕⊕⊕⊝ MODERATE4 due to imprecision
0/662 (0%)
2/681 (0.29%)
- - 3 more per 1000 (from 3 fewer to 11 more)
1 Dabigatran 150 mg twice daily 2 Placebo-Control study outcomes used from Schulman et al. (RESONATE)29 3 Patients with VTE who had completed at least 3 initial months of therapy
4 Event rate low in a large sample size.

Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
Online Supplemente-Table 11: Evidence Profile - Rivaroxaban vs Placebo for extended treatment of VTE 1, 2
Bibliography: Bauersachs et al. (EINSTEIN-Extension)5 Quality assessment Summary of Findings Participants (studies) Follow up
Risk of bias
Inconsistency Indirectness Imprecision Publication bias
Overall quality of evidence
Study event rates (%) Relative effect (95% CI)
Anticipated absolute effects With Placebo
With Rivaroxaban
Risk with Placebo
Risk difference with Rivaroxaban (95% CI)
All Cause Mortality (CRITICAL OUTCOME) 1196 (1 study)
no serious risk of bias
no serious inconsistency
no serious indirectness
serious3 undetected ⊕⊕⊕⊝ MODERATE3 due to imprecision
2/594 (0.34%)
1/602 (0.17%)
RR 0.49 (0.04 to 5.43)
3 per 1000
2 fewer per 1000 (from 3 fewer to 15 more)
Recurrent VTE (CRITICAL OUTCOME) 1196 (1 study)
no serious risk of bias
no serious inconsistency
no serious indirectness
no serious imprecision
undetected ⊕⊕⊕⊕ HIGH
42/594 (7.1%)
8/602 (1.3%)
RR 0.19 (0.09 to 0.4)
71 per 1000
57 fewer per 1000 (from 42 fewer to 64 fewer)
Major Bleeding (CRITICAL OUTCOME) 1188 (1 study)
serious no serious inconsistency
no serious indirectness
no serious imprecision
undetected ⊕⊕⊕⊝ MODERATE due to risk of bias
0/590 (0%)
4/598 (0.67%)
- - 4 more per 1000 (from 1 less to 17 more)
1 Rivaroxaban 20mg daily or placebo, specific to the continued treatment study 2 Patients who had completed 6 to 12 months of treatment for VTE 3 CI includes values suggesting no effect and values suggesting either benefit or harm

Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
Online Supplemente-Table 12: Evidence Profile - Apixaban vs Placebo for extended treatment of VTE 1,2
Bibliography: Agnelli et al. (AMPLIFY-EXT)4 Quality assessment Summary of Findings Participants (studies) Follow up
Risk of bias
Inconsistency Indirectness Imprecision Publication bias
Overall quality of evidence
Study event rates (%) Relative effect (95% CI)
Anticipated absolute effects With Placebo
With Apixaban
Risk with Placebo
Risk difference with Apixaban (95% CI)
All Cause Mortality (CRITICAL OUTCOME) 1669 (1 study) 12 months
no serious risk of bias
no serious inconsistency
no serious indirectness
serious3,4 undetected ⊕⊕⊕⊝ MODERATE3,4 due to imprecision
14/829 (1.7%)
7/840 (0.83%)
RR 0.49 (0.2 to 1.22)
17 per 1000
9 fewer per 1000 (from 14 fewer to 4 more)
Recurrent VTE (CRITICAL OUTCOME) 1669 (1 study) 12 months
no serious risk of bias
no serious inconsistency
no serious indirectness
no serious imprecision
undetected ⊕⊕⊕⊕ HIGH
73/829 (8.8%)
14/840 (1.7%)
RR 0.19 (0.11 to 0.33)
88 per 1000
71 fewer per 1000 (from 59 fewer to 78 fewer)
Major Bleeding (CRITICAL OUTCOME) 1669 (1 study) 12 months
no serious risk of bias
no serious inconsistency
no serious indirectness
serious3,4 undetected ⊕⊕⊕⊝ MODERATE3,4 due to imprecision
4/829 (0.48%)
2/840 (0.24%)
RR 0.49 (0.09 to 2.64)
5 per 1000
2 fewer per 1000 (from 4 fewer to 8 more)
1 Apixaban 2.5 mg twice-daily dose vs. placebo 2 Patients with VTE who had completed 6 to 12 months of anticoagulation therapy 3 Significantly wide CIs, including appreciable benefit / harm and no effect line 4 Low number of events

Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
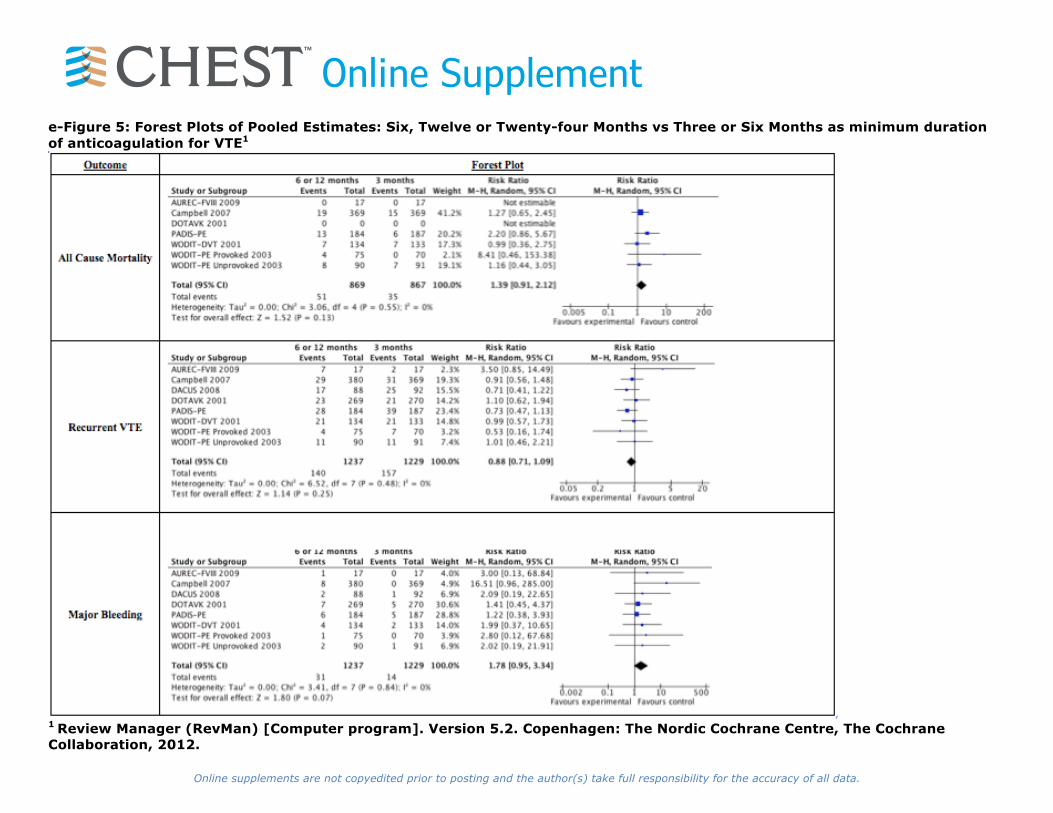
Online Supplemente-Table 13: Evidence Profile - Six, Twelve or Twenty-four Months vs Three or Six Months as minimum duration of anticoagulation for VTE 1,2 Bibliography: Campbell et al.8, Pinede et al. (DOTAVK)25, Agnelli et al. (WODIT-PE Provoked and Unprovoked)2, Agnelli et al. (WODIT-DVT)1, Couturand et al. (PADIS-PE)10, Siragusa et al. (DACUS)33, Eischer et al.(AUREC-FVIII)12 Quality assessment Summary of Findings Participants (studies) Follow up
Risk of bias
Inconsistency Indirectness Imprecision Publication bias
Overall quality of evidence
Study event rates (%) Relative effect (95% CI)
Anticipated absolute effects With No extended
With Extended
Risk with No extended
Risk difference with Extended (95% CI)
Mortality (IMPORTANT OUTCOME) 1736 (7 studies) 1-3 years
no serious risk of bias3
no serious inconsistency
no serious indirectness4
serious5 undetected ⊕⊕⊕⊝ MODERATE3,4,5 due to imprecision
51/869 (5.8%)
35/867 (4.0%)
RR 1.39 (0.91 to 2.12)
41 per 1000 16 more per 1000 (from 4 fewer to 46 more)
Recurrent VTE (CRITICAL OUTCOME) 2466 (8 studies) 1-3 years
no serious risk of bias3
no serious inconsistency
no serious indirectness4
serious5 undetected ⊕⊕⊕⊝ MODERATE3,4,5 due to imprecision
140/1237 (11.3%)
157/1229 (12.7%)
RR 0.88 (0.71 to 1.09)
128 per 1000
18 fewer per 1000 (from 40 fewer to 8 more)
Major Bleeding (CRITICAL OUTCOME) 2466 (8 studies) 1-3 years
no serious risk of bias3
no serious inconsistency
no serious indirectness4
serious5 undetected ⊕⊕⊕⊝ MODERATE3,4,5 due to imprecision
31/1237 (2.5%)
14/1229 (1.4%)6
RR 1.78 (0.95 to 3.34)
12 per 1000 9 more per 1000 (from 1 fewer to 27 more)
1 Studies vary in follow-up duration (10 months to 3 years) and in duration of time-limited VKA (3 to 6 months). 2 VKA as NOACs are not included 3 Timing of randomization relative to the start of treatment and length of treatment varied across studies: Pinede et al.25 and Campbell et al.8 randomized at diagnosis; and Agnelli et al.2, Eischer et al.12 and Couturaud et al.10 randomized after the initial 3 mo (Agnelli et al.2) or 6 mo (Eischer et al.12 Couturaud et al.10) of treatment to stop or continued treatment. The longer duration of treatment was 6 mo in Agnelli et al. (provoked PE)2 and Pinede et al.25, 12 months in Agnelli et al. (unprovoked DVT; unprovoked PE)1,2, 24 months in Couturaud et al.10, and 30 months in Eischer et al.12 Generally, study design was strong. No study stopped early for benefit; three stopped early because of slow recruitment (Campbell et al.8, Pinede et al.25, Eischer et al.12) and one because of lack of benefit (Agnelli et al.2). In one study (Campbell et al.8), 20% of VTE outcomes were not objectively confirmed. Patients and caregivers were blinded in Couturaud et al.10, but none of the other studies. Adjudicators of outcomes were blinded in all but one study (Campbell et al.8). All studies used effective randomization concealment, intention-to-treat analysis, and a low unexplained drop-out frequency. 4 Study populations varied across studies: Pinede et al.25 enrolled provoked and unprovoked proximal DVT and PE; Campbell et al.8, enrolled provoked and unprovoked isolated distal DVT, proximal DVT, and PE; Agnelli et al.2 had separate randomizations for provoked PE (3 vs 6 mo) and unprovoked (3 vs 12 mo); Agnelli et al.1 enrolled unprovoked proximal DVT; Eischer et al.12 enrolled unprovoked isolated DVT, proximal DVT and PE with high levels of factor VIII; and Couturaud et al.10 enrolled unprovoked PE. 5 CIs include both values suggesting no effect and values suggesting either benefit or harm.

Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
Online Supplemente-Table 14: Evidence Profile - Aspirin vs Placebo for extended treatment of VTE
Bibliography: Simes et al. (INSPIRE)32 Quality assessment Summary of Findings Participants (studies) Follow up
Risk of bias
Inconsistency Indirectness Imprecision Publication bias
Overall quality of evidence
Study event rates (%)
Relative effect (95% CI)
Anticipated absolute effects
With Control
With Aspirin
Risk with Control
Risk difference with Aspirin (95% CI)
All Cause Mortality (CRITICAL OUTCOME) 1224 (2 studies) up to 4 years
no serious risk of bias1
no serious inconsistency
no serious indirectness
very serious2,3
undetected ⊕⊕⊝⊝ LOW1,2,3 due to imprecision
23/608 (3.8%)
20/616 (3.2%)
HR 0.82 (0.45 to 1.52)4
Moderate risk population5 5 per 1000
1 fewer per 1000 (from 3 fewer to 3 more)
Recurrent VTE (CRITICAL OUTCOME) 1224 (2 studies) up to 4 years
no serious risk of bias1
no serious inconsistency
no serious indirectness
serious3 undetected ⊕⊕⊕⊝ MODERATE1,3 due to imprecision
112/608 (18.4%)
81/616 (13.1%)
HR 0.65 (0.49 to 0.86)4
184 per 1000
60 fewer per 1000 (from 24 fewer to 89 fewer)
Major Bleeding (CRITICAL OUTCOME) 1224 (2 studies) up to 4 years
no serious risk of bias1
no serious inconsistency
no serious indirectness
serious2 undetected ⊕⊕⊕⊝ MODERATE1,2 due to imprecision
7/608 (1.2%)
9/616 (1.5%)
HR 1.31 (0.48 to 3.53)4
12 per 1000
4 more per 1000 (from 6 fewer to 29 more)
1 Both of the included studies were stopped early with knowledge of overall rates of VTE. Decision to stop was not made with unblinded data. Only 1/3 of the intended patients in the study 2 CI includes values suggesting no effect and values suggesting either benefit or harm 3 Greater than 50% change in risk reduction 4 Estimate based on Simes et al. (INSPIRE)32 of synthesis of Brighton et al. (ASPIRE)38 and Becattini et al. (WARFASA)39 5 Estimate taken from Douketis et al.40

Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
Online Supplement e-Table 15: Evidence Profile - Catheter assisted thrombus removal vs anticoagulation alone for acute leg DVT
Bibliography: Watson et al.34 used for all outcomes except Patency and QoL. Enden et al.14 used for Patency estimates. Enden et al.41 used for QoL estimates. Quality assessment Summary of Findings Participants (studies) Follow up
Risk of bias
Inconsistency Indirectness Imprecision Publication bias
Overall quality of evidence
Study event rates (%) Relative effect (95% CI)
Anticipated absolute effects With Anticoagulation alone
With Catheter assisted thrombus removal
Risk with Anticoagulation alone
Risk difference with Catheter assisted thrombus removal (95% CI)
All Cause Mortality (CRITICAL OUTCOME) 209 (1 study) 3 months
no serious risk of bias
no serious inconsistency
no serious indirectness
very serious1,2
undetected ⊕⊕⊝⊝ LOW1,2 due to imprecision
5/108 (4.6%)3
2/101 (2%)
RR 0.43 (0.08 to 2.16)
46 per 10003 26 fewer per 1000 (from 43 fewer to 54 more)
Recurrent VTE (IMPORTANT OUTCOME) 189 (1 study) 3 months
no serious risk of bias
no serious inconsistency
no serious indirectness
very serious1,2
undetected ⊕⊕⊝⊝ LOW1,2 due to imprecision
18/99 (18.2%)
10/90 (11.1%)
RR 0.61 (0.3 to 1.25)4
Moderate risk population5 48 per 1000 19 fewer per
1000 (from 34 fewer to 12 more)
Major bleeding (CRITICAL OUTCOME) 224 (2 studies) 3 months
no serious risk of bias
no serious inconsistency
no serious indirectness
very serious1,2
undetected ⊕⊕⊝⊝ LOW1,2 due to imprecision
0/116 (0%)
3/108 (2.8%)
RR 7.69 (0.4 to 146.9)4
Moderate risk population5,7 29 per 1000 194 more per
1000 (from 17 fewer to 1000 more)
Postthrombotic syndrome (CRITICAL OUTCOME) 189 (1 study) 2 years
no serious risk of bias
no serious inconsistency
no serious indirectness
serious1 undetected ⊕⊕⊕⊝ MODERATE1 due to imprecision
55/99 (55.6%)
37/90 (41.1%)
RR 0.74 (0.55 to 1)6
Moderate risk population9 588 per 1000 153 fewer
per 1000 (from 265 fewer to 0 more)8
Patency (IMPORTANT OUTCOME) 189 (1 study) 6 months
no serious risk of bias
no serious inconsistency
no serious indirectness
serious2 undetected ⊕⊕⊕⊝ MODERATE2 due to imprecision
45/99 (45.5%)10
58/90 (64.4%)
RR 1.42 (1.09 to 1.85)
455 per 100010 191 more per 1000 (from 41 more to 386 more)
Quality of Life (CRITICAL OUTCOME; Better indicated by higher values) 189 (1 study) 24 months
serious12 no serious inconsistency
no serious indirectness
no serious imprecision
undetected ⊕⊕⊕⊝ MODERATE11 due to risk of bias
99 90 - The mean quality of life in the intervention groups was 0.2 higher (2.8 lower to 3 higher)12, 13
1 Confidence interval includes values suggesting both benefit and harm 2 Low number of events 3 Reported deaths from Enden et al. (CAVENT)14

Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
Online Supplement4 Estimate taken from Watson et al.34. The one study included for this outcome was Enden et al. (CAVENT)14 5 Baseline risks for non-fatal recurrent VTE and for major bleeding derived from Douketis et al.42 6 This estimate is based on the Watson et al.34. The one study included for this outcome was Enden et al. (CAVENT).14 For PTS at 6 months, published data from Enden et al. (CAVENT)14 provides an estimate RR of 0.93 (0.61, 1.42) via Watson et al.34 7 Most of bleeding events occur during the first 7 days 8 For severe PTS, assuming the same RR of 0.46 and a baseline risk of 13.8%43, the absolute reduction is 75 fewer severe PTS per 1000 (from 29 fewer to 138 fewer) over 2 years 9 This estimate is based on the findings of the VETO study.43 10 Reported patency from Enden et al. (CAVENT)14 11 Open-label 12 Disease-specific QOL (VEINES-QOL) estimate used at 24 months according to treatment allocation 13 Generic QoL (EQ-5D) at 24 months according to treatment allocation estimate is MD 0.04 (-0.01 to 0.17)
Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
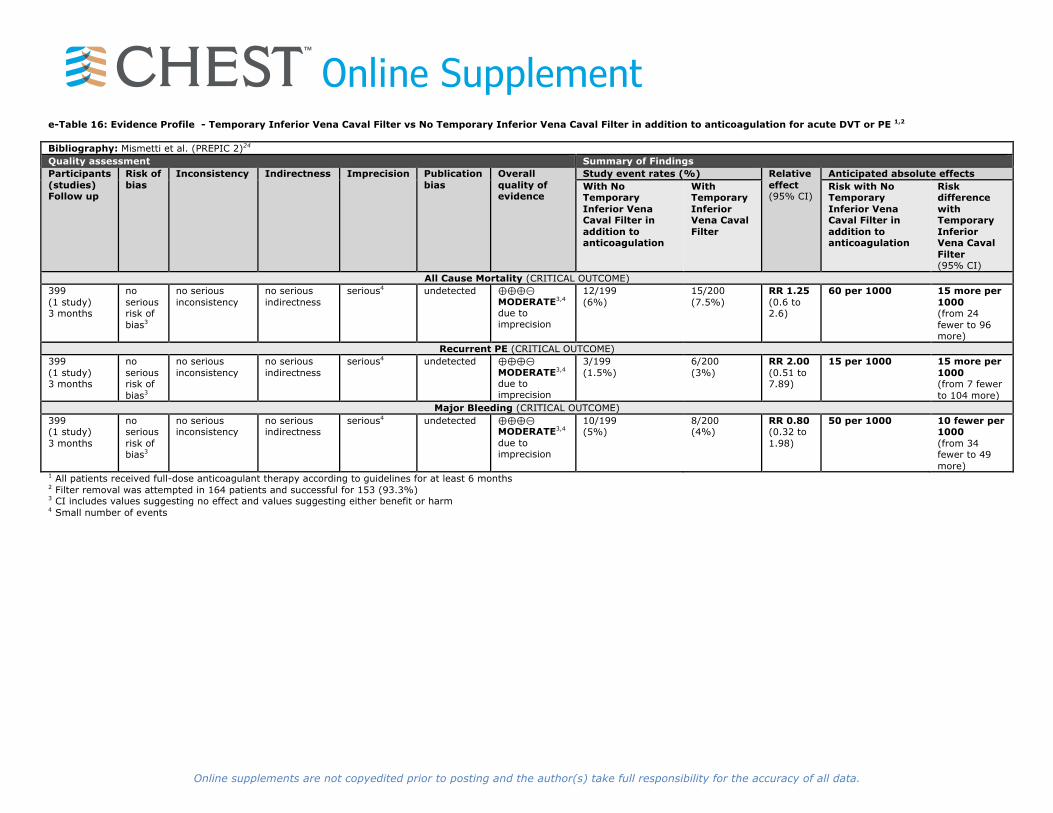
Online Supplemente-Table 16: Evidence Profile - Temporary Inferior Vena Caval Filter vs No Temporary Inferior Vena Caval Filter in addition to anticoagulation for acute DVT or PE 1,2
Bibliography: Mismetti et al. (PREPIC 2)24 Quality assessment Summary of Findings Participants (studies) Follow up
Risk of bias
Inconsistency Indirectness Imprecision Publication bias
Overall quality of evidence
Study event rates (%) Relative effect (95% CI)
Anticipated absolute effects With No Temporary Inferior Vena Caval Filter in addition to anticoagulation
With Temporary Inferior Vena Caval Filter
Risk with No Temporary Inferior Vena Caval Filter in addition to anticoagulation
Risk difference with Temporary Inferior Vena Caval Filter (95% CI)
All Cause Mortality (CRITICAL OUTCOME) 399 (1 study) 3 months
no serious risk of bias3
no serious inconsistency
no serious indirectness
serious4 undetected ⊕⊕⊕⊝ MODERATE3,4 due to imprecision
12/199 (6%)
15/200 (7.5%)
RR 1.25 (0.6 to 2.6)
60 per 1000 15 more per 1000 (from 24 fewer to 96 more)
Recurrent PE (CRITICAL OUTCOME) 399 (1 study) 3 months
no serious risk of bias3
no serious inconsistency
no serious indirectness
serious4 undetected ⊕⊕⊕⊝ MODERATE3,4 due to imprecision
3/199 (1.5%)
6/200 (3%)
RR 2.00 (0.51 to 7.89)
15 per 1000 15 more per 1000 (from 7 fewer to 104 more)
Major Bleeding (CRITICAL OUTCOME) 399 (1 study) 3 months
no serious risk of bias3
no serious inconsistency
no serious indirectness
serious4 undetected ⊕⊕⊕⊝ MODERATE3,4 due to imprecision
10/199 (5%)
8/200 (4%)
RR 0.80 (0.32 to 1.98)
50 per 1000 10 fewer per 1000 (from 34 fewer to 49 more)
1 All patients received full-dose anticoagulant therapy according to guidelines for at least 6 months 2 Filter removal was attempted in 164 patients and successful for 153 (93.3%) 3 CI includes values suggesting no effect and values suggesting either benefit or harm 4 Small number of events

Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
Online Supplemente-Table 17: Evidence Profile - Elastic Compression Stockings vs No Elastic Compression Stockings to Prevent PTS of the leg
Bibliography: Kahn et al. (SOX)17 for PTS and recurrent VTE; Kahn et al.18 for acute leg pain Quality assessment Summary of Findings Participants (studies) Follow up
Risk of bias
Inconsistency Indirectness Imprecision Publication bias
Overall quality of evidence
Study event rates (%) Relative effect (95% CI)
Anticipated absolute effects With No elastic compression stockings
With Elastic compression stockings
Risk with No elastic compression stockings
Risk difference with Elastic compression stockings (95% CI)
PTS (CRITICAL OUTCOME; assessed with: Villalta Score1) 803 (1 study) 6 months
no serious risk of bias
no serious inconsistency
no serious indirectness
serious2 undetected ⊕⊕⊕⊝ MODERATE2 due to imprecision
168/394 (42.6%)
176/409 (43%)
RR 1.01 (0.86 to 1.18)3
Moderate risk population4 479 per 1000 5 more per
1000 (from 67 fewer to 86 more)
Recurrent VTE (CRITICAL OUTCOME) 803 (1 study) 6 months
no serious risk of bias
no serious inconsistency
no serious indirectness
serious2,5 undetected ⊕⊕⊕⊝ MODERATE2,5 due to imprecision
38/394 (9.6%)
33/409 (8.1%)
RR 0.84 (0.54 to 1.31)6
Moderate risk population7 210 per 1000 34 fewer per
1000 (from 97 fewer to 65 more)
Acute Leg Pain (IMPORTANT OUTCOME; Better indicated by lower values) 742 (1 study) 60 days
no serious risk of bias
no serious inconsistency
no serious indirectness
serious5,8 undetected ⊕⊕⊕⊝ MODERATE5,8 due to imprecision
365 377 - The mean acute leg pain in the control groups was 1.13 leg pain severity assessed on an 11-point numerical pain rating scale9
The mean acute leg pain in the intervention groups was 0.26 higher (0.03 lower to 0.55 higher)9
Quality of Life (CRITICAL OUTCOME; Better indicated by higher values) 803 (1 study)
no serious risk of bias
no serious inconsistency
no serious indirectness
no serious imprecision
undetected ⊕⊕⊕⊕ HIGH
394 409 - The mean quality of life in the intervention groups was 0.12 lower (1.11 lower to 0.86 higher)10,11
1 For included studies, number of post-thrombotic syndrome events as assessed by Villalta’s criteria 2 Low number of events 3 There were three studies originally included for this outcome (Brandjes et al.44, Prandoni et al.45 and Kahn et al. (SOX).17) There was very high heterogeneity between the three studies, I2 =92% (p<0.01). The pooled effect of the three studies was RR 0.63 (0.35 to 1.13). Yet, because of the high risk of bias associated with Brandjes et al.44 and Prandoni et al.45, it was decided to focus on the estimate of the low risk trial, Kahn et al. (SOX)17, which is used here 4 This estimate is based on the findings of the VETO study43 5 CI includes values suggesting no effect and values suggesting either benefit or harm 6 There were three studies originally included for this outcome (Brandjes et al.44, Prandoni et al.45 and Kahn et al. (SOX).17). The pooled effect of the three studies was RR 0.91 (0.65 to 1.27). Yet, because of the high risk of bias associated with Brandjes et al.44 and Prandoni et al.45, it was decided to focus on the estimate of the low risk trial, Kahn et al. (SOX)17, which is used here 7 This estimate is the mean of two estimates derived from two studies: 12.4% probable/definite VTE46 and 29.1% confirmed VTE.47 8 Wide CI that includes no effect 9 Estimate derived from Kahn et al.18 10 Estimate based on VEINES-QOL score improvement of 5.8 points (SD 7.5) for active ECS versus 5.9 (SD 7.1) for placebo ECS 11 SF-36 physical component score improved by 8.4 points (SD 13.6) for active ECS versus 9.9 (SD 13.2) for placebo ECS (difference between groups of -1.53 points, 95% CI -3.44 to 0.39; p=0.12)

Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
Online Supplemente-Table 18: Evidence Profile - Systemic thrombolytic therapy vs. anticoagulation alone for acute PE Bibliography: Chatterjee et al.9 Quality assessment Summary of Findings Participants (studies) Follow up
Risk of bias Inconsistency Indirectness Imprecision Publication bias
Overall quality of evidence
Study event rates (%) Relative effect (95% CI)
Anticipated absolute effects With Anticoagulation alone
With Systemic thrombolytic therapy
Risk with Anticoagulation alone
Risk difference with Systemic thrombolytic therapy (95% CI)
All Cause Mortality (CRITICAL OUTCOME) 2115 (17 studies)
no serious risk of bias
no serious inconsistency
no serious indirectness
serious1 undetected ⊕⊕⊕⊝ MODERATE1 due to imprecision
41/1054 (3.9%)2
23/1061 (2.2%)2
OR 0.53 (0.32 to 0.88)3
39 per 10002 18 fewer per 1000 (from 5 fewer to 26 fewer)
Recurrent PE (CRITICAL OUTCOME) 2043 (15 studies)
no serious risk of bias
no serious inconsistency
no serious indirectness
serious1 undetected ⊕⊕⊕⊝ MODERATE1 due to imprecision
31/1019 (3%)2
12/1024 (1.2%)2
OR 0.40 (0.22 to 0.74)4
30 per 10002 18 fewer per 1000 (from 8 fewer to 24 fewer)
Major bleeding (CRITICAL OUTCOME) 2115 (16 studies)
no serious risk of bias
no serious inconsistency
no serious indirectness
no serious imprecision
undetected ⊕⊕⊕⊕ HIGH
36/1054 (3.4%)2
98/1061 (9.2%)2
OR 2.73 (1.91 to 3.91)5
34 per 10002 54 more per 1000 (from 29 more to 87 more)
Intracranial Hemorrhage (CRITICAL OUTCOME) 2043 (15 studies)
no serious risk of bias
no serious inconsistency
no serious indirectness
serious1 undetected ⊕⊕⊕⊝ MODERATE1 due to imprecision
2/1019 (0.2%)2
15/1024 (1.5%)2
OR 4.63 (1.78 to 12.04)6
2 per 10002 7 more per 1000 (from 2 more to 21 more)
1 Low number of events 2 Majority (83%) of participants in Chatterjee et al.9 were "moderate" risk. 3 Estimate from Chatterjee et al.9. Other estimates from meta-analyses on this topic include: Dong et al.48 - OR 0.89 (0.45, 1.78) Cao et al.49 - RR 0.64 (0.29, 1.40) Marti et al.50 - OR 0.59 (0.36 - 0.96) Nakamura et al.51 - RR 0.72 (0.39, 1.31) Chatterjee et al. (Intermediate-Risk PE Only)9 - OR 0.46 (0.25 - 0.92) Marti et al. (Intermediate-Risk PE Only)50 - OR 0.42 (0.17 - 1.03) 4 Estimate from Chatterjee et al.9. Other estimates from meta-analyses on this topic include: Dong et al.48- OR 0.63 (0.33, 1.20) Cao et al.49 - RR 0.44 (0.19, 1.05) Marti et al.50 - OR 0.50 (0.27 - 0.94) Nakamura et al.51 - RR 0.60 (0.21, 1.69) 5 Estimate from Chatterjee et al.9. Other estimates from meta-analyses on this topic include: Dong et al.48 - OR 1.61 (0.91, 2.86) Cao et al.49 - RR 1.16 (0.51, 2.60) Marti et al.50 - OR 2.91 (1.95 - 4.36) Nakamura et al.51 - RR 2.07 (0.58, 7.35) 6 Estimate from Chatterjee et al.9
Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
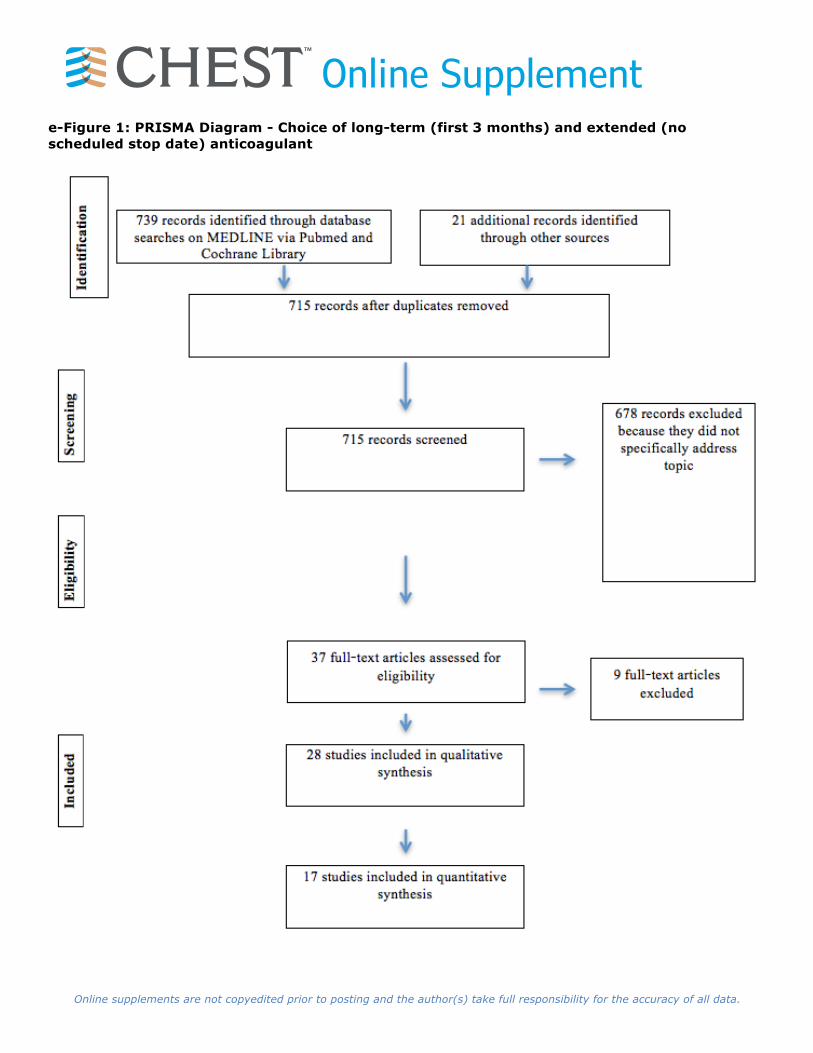
Online Supplemente-Figure 1: PRISMA Diagram - Choice of long-term (first 3 months) and extended (no scheduled stop date) anticoagulant

Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
Online Supplemente-Figure 2: PRISMA Diagram - Duration of anticoagulant therapy

Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
Online Supplemente-Figure 3: PRISMA Flow Diagram - Role of inferior vena caval (IVC) filter in addition to anticoagulation in patients with acute DVT or PE

Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
Online Supplemente-Figure 4: PRISMA Flow Diagram - Compression stocking to prevent post thrombotic syndrome (PTS)
Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
Online Supplemente-Figure 5: Forest Plots of Pooled Estimates: Six, Twelve or Twenty-four Months vs Three or Six Months as minimum duration of anticoagulation for VTE1
1 Review Manager (RevMan) [Computer program]. Version 5.2. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2012.
Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
Online Supplemente-Figure 6: Forest Plots of Pooled Estimates: LMWH vs. VKA for long term treatment of VTE1
1 Review Manager (RevMan) [Computer program]. Version 5.2. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2012.

Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
Online Supplement
References 1. Agnelli G, Prandoni P, Santamaria MG, et al. Three months versus one year of oral anticoagulant
therapy for idiopathic deep venous thrombosis. Warfarin Optimal Duration Italian Trial Investigators. The New England journal of medicine. 2001;345(3):165-169.
2. Agnelli G, Prandoni P, Becattini C, et al. Extended oral anticoagulant therapy after a first episode of pulmonary embolism. Ann Intern Med. 2003;139(1):19-25.
3. Agnelli G, Buller HR, Cohen A, et al. Oral apixaban for the treatment of acute venous thromboembolism. The New England journal of medicine. 2013;369(9):799-808.
4. Agnelli G, Buller HR, Cohen A, et al. Apixaban for extended treatment of venous thromboembolism. The New England journal of medicine. 2013;368(8):699-708.
5. Bauersachs R, Berkowitz SD, Brenner B, et al. Oral rivaroxaban for symptomatic venous thromboembolism. The New England journal of medicine. 2010;363(26):2499-2510.
6. Investigators E-P, Buller HR, Prins MH, et al. Oral rivaroxaban for the treatment of symptomatic pulmonary embolism. The New England journal of medicine. 2012;366(14):1287-1297.
7. Hokusai VTEI, Buller HR, Decousus H, et al. Edoxaban versus warfarin for the treatment of symptomatic venous thromboembolism. The New England journal of medicine. 2013;369(15):1406-1415.
8. Campbell IA, Bentley DP, Prescott RJ, Routledge PA, Shetty HG, Williamson IJ. Anticoagulation for three versus six months in patients with deep vein thrombosis or pulmonary embolism, or both: randomised trial. Bmj. 2007;334(7595):674.
9. Chatterjee S, Chakraborty A, Weinberg I, et al. Thrombolysis for pulmonary embolism and risk of all-cause mortality, major bleeding, and intracranial hemorrhage: a meta-analysis. Jama. 2014;311(23):2414-2421.
10. Couturand F SO, Pernod G, Mismetti P, Jego P, Duhamel E, Provost K, Bal dit Sollier C, Presles E, Castellant P, Parent F, Salaun P, Bressollette L, Nonent M, Lorillon P, Girard P, Lacut K, Guégan M, Bosson J, Laporte S, Leroyer C, Décousus H, Meyer G, Mottier D, for the PADIS-PE Investigators. Two years versus six months of oral anticoagulation after a first episode of unprovoked pulmonary embolism. The PADIS-PE multicenter, double-blind, randomized, trial. 2015.
11. Deitcher SR, Kessler CM, Merli G, et al. Secondary prevention of venous thromboembolic events in patients with active cancer: enoxaparin alone versus initial enoxaparin followed by warfarin for a 180-day period. Clinical and applied thrombosis/hemostasis : official journal of the International Academy of Clinical and Applied Thrombosis/Hemostasis. 2006;12(4):389-396.
12. Eischer L, Gartner V, Schulman S, Kyrle PA, Eichinger S, investigators A-F. 6 versus 30 months anticoagulation for recurrent venous thrombosis in patients with high factor VIII. Annals of hematology. 2009;88(5):485-490.
13. Elsharawy M, Elzayat E. Early results of thrombolysis vs anticoagulation in iliofemoral venous thrombosis. A randomised clinical trial. Eur.J Vasc Endovasc.Surg. 2002;24(3):209-214.
14. Enden T, Haig Y, Klow NE, et al. Long-term outcome after additional catheter-directed thrombolysis versus standard treatment for acute iliofemoral deep vein thrombosis (the CaVenT study): a randomised controlled trial. Lancet. 2012;379(9810):31-38.
15. Hull RD, Pineo GF, Brant RF, et al. Self-managed long-term low-molecular-weight heparin therapy: the balance of benefits and harms. The American journal of medicine. 2007;120(1):72-82.
16. Hull RD, Pineo GF, Brant R, et al. Home therapy of venous thrombosis with long-term LMWH versus usual care: patient satisfaction and post-thrombotic syndrome. The American journal of medicine. 2009;122(8):762-769 e763.
17. Kahn SR, Shapiro S, Wells PS, et al. Compression stockings to prevent post-thrombotic syndrome: a randomised placebo-controlled trial. Lancet. 2014;383(9920):880-888.
18. Kahn SR, Shapiro S, Ducruet T, et al. Graduated compression stockings to treat acute leg pain associated with proximal DVT. A randomised controlled trial. Thromb Haemost. 2014;112(6):1137-1141.

Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
Online Supplement19. Lee AY, Levine MN, Baker RI, et al. Low-molecular-weight heparin versus a coumarin for the
prevention of recurrent venous thromboembolism in patients with cancer. N.Engl.J Med. 2003;349(2):146-153.
20. Lee AY, Kamphuisen PW, Meyer G, et al. Tinzaparin vsWarfarin for Treatment of Acute Venous Thromboembolism in Patients With Active Cancer: A Randomized Clinical Trial. Journal of the American Medical Association. 2015;314:677-686.
21. Lopaciuk S, Bielska-Falda H, Noszczyk W, et al. Low molecular weight heparin versus acenocoumarol in the secondary prophylaxis of deep vein thrombosis. Thromb Haemost. 1999;81(1):26-31.
22. Lopez-Beret P, Orgaz A, Fontcuberta J, et al. Low molecular weight heparin versus oral anticoagulants in the long-term treatment of deep venous thrombosis. J Vasc Surg. 2001;33(1):77-90.
23. Meyer G, Marjanovic Z, Valcke J, et al. Comparison of low-molecular-weight heparin and warfarin for the secondary prevention of venous thromboembolism in patients with cancer: a randomized controlled study. Arch Intern Med. 2002;162(15):1729-1735.
24. Mesmetti, PREPIC 2 Study Group. Retrievable vena cava filter for patients with acute pulmonary embolism: A randomized clinical trial. 2015.
25. Pinede L, Ninet J, Duhaut P, et al. Comparison of 3 and 6 months of oral anticoagulant therapy after a first episode of proximal deep vein thrombosis or pulmonary embolism and comparison of 6 and 12 weeks of therapy after isolated calf deep vein thrombosis. Circulation. 2001;103(20):2453-2460.
26. Piran S, Le Gal G, Wells PS, et al. Outpatient treatment of symptomatic pulmonary embolism: a systematic review and meta-analysis. Thrombosis research. 2013;132(5):515-519.
27. Prins MH, Lensing AW, Bauersachs R, et al. Oral rivaroxaban versus standard therapy for the treatment of symptomatic venous thromboembolism: a pooled analysis of the EINSTEIN-DVT and PE randomized studies. Thrombosis journal. 2013;11(1):21.
28. Romera A, Cairols MA, Vila-Coll R, et al. A randomised open-label trial comparing long-term sub-cutaneous low-molecular-weight heparin compared with oral-anticoagulant therapy in the treatment of deep venous thrombosis. European journal of vascular and endovascular surgery : the official journal of the European Society for Vascular Surgery. 2009;37(3):349-356.
29. Schulman S, Kearon C, Kakkar AK, et al. Extended use of dabigatran, warfarin, or placebo in venous thromboembolism. The New England journal of medicine. 2013;368(8):709-718.
30. Schulman S, Kearon C, Kakkar AK, et al. Dabigatran versus warfarin in the treatment of acute venous thromboembolism. The New England journal of medicine. 2009;361(24):2342-2352.
31. Schulman S, Kakkar AK, Goldhaber SZ, et al. Treatment of acute venous thromboembolism with dabigatran or warfarin and pooled analysis. Circulation. 2014;129(7):764-772.
32. Simes J, Becattini C, Agnelli G, et al. Aspirin for the prevention of recurrent venous thromboembolism: the INSPIRE collaboration. Circulation. 2014;130(13):1062-1071.
33. Siragusa S, Malato A, Anastasio R, et al. Residual vein thrombosis to establish duration of anticoagulation after a first episode of deep vein thrombosis: the Duration of Anticoagulation based on Compression UltraSonography (DACUS) study. Blood. 2008;112(3):511-515.
34. Watson L, Broderick C, Armon MP. Thrombolysis for acute deep vein thrombosis. The Cochrane database of systematic reviews. 2014;1:CD002783.
35. Prandoni P, Trujillo-Santos J, Surico T, et al. Recurrent thromboembolism and major bleeding during oral anticoagulant therapy in patients with solid cancer: findings from the RIETE registry. Haematologica. 2008;93(9):1432-1434.
36. Prandoni P, Lensing AW, Piccioli A, et al. Recurrent venous thromboembolism and bleeding complications during anticoagulant treatment in patients with cancer and venous thrombosis. Blood. 2002;100(10):3484-3488.
37. Beyth RJ, Milligan PE, Gage BF. Risk factors for bleeding in patients taking coumarins. Current hematology reports. 2002;1(1):41-49.
38. Brighton TA, Eikelboom JW, Mann K, et al. Low-dose aspirin for preventing recurrent venous thromboembolism. The New England journal of medicine. 2012;367(21):1979-1987.
Online supplements are not copyedited prior to posting and the author(s) take full responsibility for the accuracy of all data.
Online Supplement39. Becattini C, Agnelli G, Schenone A, et al. Aspirin for preventing the recurrence of venous
thromboembolism. The New England journal of medicine. 2012;366(21):1959-1967. 40. Douketis JD, Gu CS, Schulman S, Ghirarduzzi A, Pengo V, Prandoni P. The risk for fatal pulmonary
embolism after discontinuing anticoagulant therapy for venous thromboembolism. Ann Intern Med. 2007;147(11):766-774.
41. Enden T, Wik HS, Kvam AK, Haig Y, Klow NE, Sandset PM. Health-related quality of life after catheter-directed thrombolysis for deep vein thrombosis: secondary outcomes of the randomised, non-blinded, parallel-group CaVenT study. BMJ open. 2013;3(8):e002984.
42. Douketis JD, Foster GA, Crowther MA, Prins MH, Ginsberg JS. Clinical risk factors and timing of recurrent venous thromboembolism during the initial 3 months of anticoagulant therapy. Arch Intern Med. 2000;160(22):3431-3436.
43. Kahn SR, Shrier I, Julian JA, et al. Determinants and time course of the postthrombotic syndrome after acute deep venous thrombosis. Ann Intern Med. 2008;149(10):698-707.
44. Brandjes DP, Buller HR, Heijboer H, et al. Randomised trial of effect of compression stockings in patients with symptomatic proximal-vein thrombosis. Lancet. 1997;349(9054):759-762.
45. Prandoni P, Lensing AW, Prins MH, et al. Below-knee elastic compression stockings to prevent the post-thrombotic syndrome: a randomized, controlled trial. Ann.Intern.Med. 2004;141(4):249-256.
46. Heit JA, Mohr DN, Silverstein MD, Petterson TM, O'Fallon WM, Melton LJ, 3rd. Predictors of recurrence after deep vein thrombosis and pulmonary embolism: a population-based cohort study. Arch Intern Med. 2000;160(6):761-768.
47. Prandoni P, Noventa F, Ghirarduzzi A, et al. The risk of recurrent venous thromboembolism after discontinuing anticoagulation in patients with acute proximal deep vein thrombosis or pulmonary embolism. A prospective cohort study in 1,626 patients. Haematologica. 2007;92(2):199-205.
48. Dong BR, Hao Q, Yue J, Wu T, Liu GJ. Thrombolytic therapy for pulmonary embolism. The Cochrane database of systematic reviews. 2009(3):CD004437.
49. Cao Y, Zhao H, Gao W, Wang Y, Cao J. Systematic review and meta-analysis for thrombolysis treatment in patients with acute submassive pulmonary embolism. Patient preference and adherence. 2014;8:275-282.
50. Marti C, John G, Konstantinides S, et al. Systemic thrombolytic therapy for acute pulmonary embolism: a systematic review and meta-analysis. 2014.
51. Nakamura S, Takano H, Kubota Y, Asai K, Shimizu W. Impact of the efficacy of thrombolytic therapy on the mortality of patients with acute submassive pulmonary embolism: a meta-analysis. Journal of thrombosis and haemostasis : JTH. 2014;12(7):1086-1095.
151469
Related Documents

![Single Dose Bioequivalence Study of Two Rivaroxaban Tablet ...€¦ · drug [3], rivaroxaban did not fulfil the waiver criteria for crushed bioequivalence testing. Therefore, after](https://static.cupdf.com/doc/110x72/5f024c737e708231d403933a/single-dose-bioequivalence-study-of-two-rivaroxaban-tablet-drug-3-rivaroxaban.jpg)









