CHD Newer Risk Factors An over view on Homocystinemia Dr. R.V.S.N.Sarma M.D., M.Sc., (Canada)

CHD Newer Risk Factors An over view on Homocystinemia Dr. R.V.S.N.Sarma M.D., M.Sc., (Canada)
Dec 19, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

CHDNewer Risk Factors
An over view on
Homocystinemia
Dr. R.V.S.N.Sarma M.D., M.Sc., (Canada)
All are One
• This not about the GOD
• There is only one disease – Over nutrition• Its faces are many such as
– Over weight / Obesity
– Diabetes mellitus, IR, Syndrome X
– Atherosclerosis – HT- CHD – CVD – RVD – PVD
– Hyper lipidemias – endothelial dysfunction
– Wear and tear of joints …. So on
• What are we to do ? - Avoid over-indulgence
Weight in kgs
Height2 in mtsBMI =
How much is much ?
70
1.65 x 1.65BMI = = 25.71
Underweight < 20 Over weight > 25 to 30
Normal 20 to 25 Obesity >30
Waist / Hip ratio = 35” /38” = 0.92
Normal for Males < 0.90, Females <0.80

Macro-vascular Disease
Sedentary Life Style
Less perfect Genetic make-up
Diets rich in Saturated Fat, Chol
Excess body weight/ Obesity
Lipid abnormalities
Atherosclerotic vascular disease
CHD, CVD, PVD
tHcy
ROS

AVD – Clinical Manifestations
Organ Condition Impairment Clinical Presentation
Heart Coronary Heart
Disease (CHD)
Ischemia
Infarction
Angina Pectoris
Myocardial Infarction
Brain Cerebro vascular
Disease (CVD)
Ischemia
Infarction
Transient Ischemia attack
Stroke
Kidney Reno vascular
Disease (RVD)
Ischemia
Infarction
Reno vascular hypertension
Renal impairment
Renal Failure
Leg Muscles
Peripheral Vascular Disease (PVD)
Ischemia
Infarction
Intermittent Claudication
Gangrene
For every thing the common denominator is ED
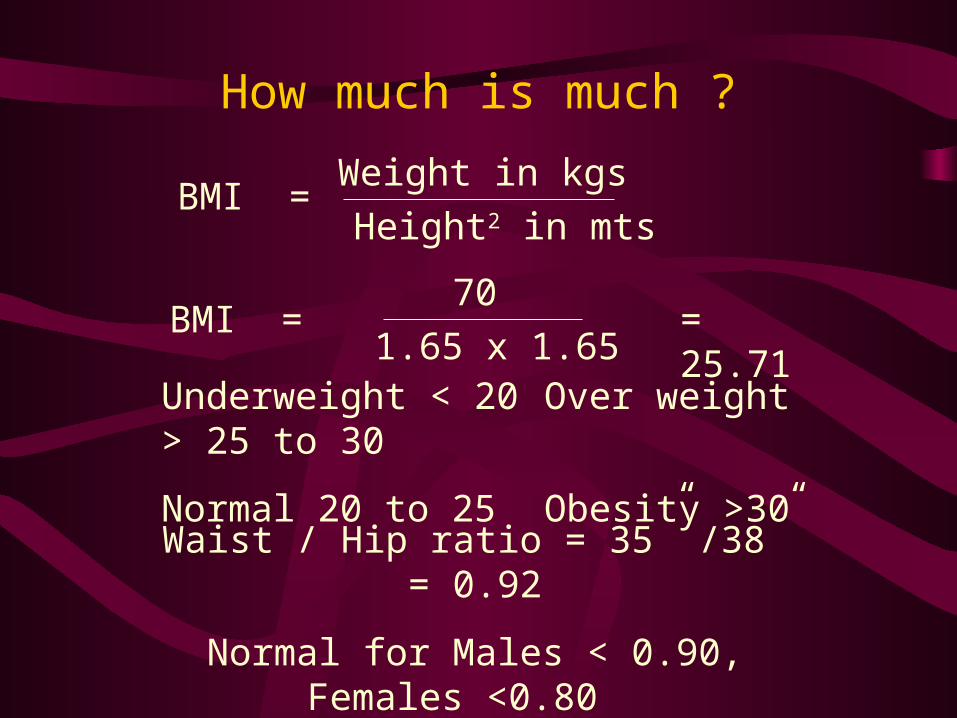
Lipid Peroxidation
LDL, IDL Not normally taken up by the vessel wall
ROS – Free radicals and Pro-oxidants
Oxidized LDL, IDL
Freely enters the vessel wall
Scavenger pathway
Endothelium Macrophages
Foam Cells Cytokines, GF
Atherosclerosis

Risk Factors for AVD
• Hyperhomocyst(e)inemia• Diabetes mellitus• Hypertension• Dyslipidemia• Positive family history,
Smoking, obesity and
physical inactivity
Oxidative Stress
AVD

Free Radical Formation
Homolytic fission of a covalent bond
A B
BAA B
Single covalent bond
Homolytic fission Heterolytic fission
Free radicals Ions

ROS damage biological tissues- membranes
Reactive Oxygen Species
Lipid peroxidation Protein denaturation DNA Damage
Cell Dysfunction and death
Free radicals released

Classification
• Preventive antioxidants-Ceruloplasmin, transferrin, lactoferrin
• Enzyme antioxidants-Superoxide dismutase, catalase, glutathione peroxidase
• Scavenging or ‘chain-breaking’ or ‘sacrificial’antioxidants-Vitamins A,C, and E

ROS and their Antioxidants
ROS Antioxidants
O2 Superoxide
free radical
Superoxide dismutase Vitamin E, -carotene
OH Hydroxyl free radical
Vitamin C
H2O2 Hydrogen peroxide
Glutathione peroxidase
O2 Singlet Oxygen Vitamin A, E

Reactive Oxygen Species (ROS)
Free Radicals Non Radicals
Superoxide O2 Hydrogen peroxide H2O2
Hydroxyl OH Singlet oxygen O2
ROS are highly reactive….and can damage biological tissues and membranes

What is Homocysteine ?
Protein diet Methionine 1)Homocysteine
2)Homocystine
3) Homocysteine thiolactone
Generation of ROS
Homocysteine • 1+2+3= homocyst(e)ine
•homocyst(e)ine = tHcy
•Homocyst(e)inemia=hyper - tHcy
Digestion Metabolism
Auto-oxidationProtein synthesis
HS-CH2-CH2-CH-COOH
NH2
• Sulfur-containing amino acid
•By product of methionine metabolism

Homocysteine : Metabolic Pathways
Remethylation Cycle
Demethylation Cycle
Transsulfuration
Pathway
Diet
Methionine
Homocysteine
Tetra hydrofolate
Methyl tetrahydrofolate
Cystathionine
Cysteine
GlutathioneSulphate
Vitamin B6 (C beta S)
Folic acid MTHFR
Vitamin B6 (MS)
MS – Methionine synthaseMTHFR – Methyl tetrahydro folate reductaseC beta S – Cystathionine beta synthase

Hyperhomocyst(e)inemia
Blood Homocyst(e)ine Levels
Classification Values in mol/L
Normal
Moderate
Intermediate
Severe
05 – 15
16 – 30
31 – 100
> 100
• Moderate to severe hyper – tHcy : established risk factor for AVD 1-4
• Hyper – tHcy
- 5-7 % of the general population
- 12-47 % of patients with AVD
Causes of Hyperhomocyst(e)inemia
A. Nutritional : Vitamin deficiency
Folic Acid
Vitamin B12
Vitamin B6
B. Genetic : Enzyme Abnormality
C. Drugs :
Methotrexate, Phenytoin, Theophylline

Homocysteine & Pathogenesis of AVD
Homocysteine
Auto-oxidation
Generation of ROS
Lipid peroxidationDamages endothelium
H2O2 OH/O2
Oxidizes LDL
Foam cells (chol)Nitric Oxide formation
Vasodilation
Hypertension
Exposure of smooth muscle, subendothelium
Proliferation of SM cells, Chemotaxis
ATHEROSCLEROSIS

Physicians Health Study
• 271 male physicians who had MI and matched controls were studied
• Various risk factors were analyzed• Plasma tHcy is significantly higher in those
with MI compared to controls• The R.R for tHcy levels above 13 is 3.4 after
adjusting for all other risk factors• 482 hyperlipedemic subjects – 72 % with
↑tHcy had atheroscleoris v/s 44 % without

Treatment of Hyperhomocyst(e)inemia
A. Nutritional : Vitamin Supplimentation Folic Acid – 5 mg daily (Folvite)
Supplementation of Vitamin B12
Supplementation of Vitamin B6
B. Drugs : Care while using drugs likeMethotrexate, Phenytoin, Theophylline
C. Role of anti-oxidants – no RCTs

Lp (a) or Little a
• Similar to LDL molecule• a single apo-A is attached by a disulfide bond to
apo-B 100• Primary determinant is genetic• Normal value 20 mg %, > 30 high risk• It may compete with plasminogen because of
structural similarity and so interfere with plasmin synthesis and thrombolytic pathway
• Nicotinic acid, ? Benzafibrate, estrogens lower it
True !
Eat but not over-eat
Drink but not alcohol
Indulge but not in junk food
Think but not worry
Be quiet but with exercise
Have high Chol but only HDL Cholesterol
Be high spirited but not be on ‘spirits’
Smoke any brand of incense stick, but not cigarettes
Related Documents