1 CHAPTER I INTRODUCTION Glucagon is a 29-amino acid peptide hormone secreted by the alpha cells of the pancreas, which was originally identified as a hyperglycemic hormone in pancreatic extracts in 1923 by Kimball and Murlin. The regulation of glucagon secretion is complex; it involves the effects of several metabolic substrates, hormones and neurotransmitters. The main physiological role of glucagon is the maintenance of hepatic glucose production during fasting, hypoglycemia, exercise and infection/trauma. The goal of this dissertation is to describe the acute in vivo regulation of hepatic glucose production by glucagon during insulin-induced hypoglycemia in the overnight- fasted conscious dog. This chapter will provide an introduction to the following: 1) Counterregulatory response to hypoglycemia, 2) Glucagon action and signaling, 3) Insulin action and signaling, 4) Insulin and glucagon interaction. Counterregulatory response to hypoglycemia Under physiological conditions glucose is metabolized by all tissues throughout the body, but is a critical metabolic fuel for the nervous system. The reason for this is that the brain can not synthesize glucose or store more than a small amount of glycogen; it relies mainly on the continuous uptake of glucose from the circulation to supply its metabolic needs (1). As a result, hypoglycemia is a dangerous condition that can lead to brain damage, coma and even death. Therefore, maintenance of the plasma glucose concentration is critical for survival and it is normally tightly regulated by various control

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
CHAPTER I
INTRODUCTION
Glucagon is a 29-amino acid peptide hormone secreted by the alpha cells of the
pancreas, which was originally identified as a hyperglycemic hormone in pancreatic
extracts in 1923 by Kimball and Murlin. The regulation of glucagon secretion is
complex; it involves the effects of several metabolic substrates, hormones and
neurotransmitters. The main physiological role of glucagon is the maintenance of hepatic
glucose production during fasting, hypoglycemia, exercise and infection/trauma.
The goal of this dissertation is to describe the acute in vivo regulation of hepatic
glucose production by glucagon during insulin-induced hypoglycemia in the overnight-
fasted conscious dog. This chapter will provide an introduction to the following: 1)
Counterregulatory response to hypoglycemia, 2) Glucagon action and signaling, 3)
Insulin action and signaling, 4) Insulin and glucagon interaction.
Counterregulatory response to hypoglycemia Under physiological conditions glucose is metabolized by all tissues throughout
the body, but is a critical metabolic fuel for the nervous system. The reason for this is
that the brain can not synthesize glucose or store more than a small amount of glycogen;
it relies mainly on the continuous uptake of glucose from the circulation to supply its
metabolic needs (1). As a result, hypoglycemia is a dangerous condition that can lead to
brain damage, coma and even death. Therefore, maintenance of the plasma glucose
concentration is critical for survival and it is normally tightly regulated by various control

2
mechanisms. These counterregulatory signals are so efficient that hypoglycemia is a rare
clinical condition in normal individuals. Clinical conditions most commonly associated
with hypoglycemia are: ethanol-consumption, certain drugs, insulin-secreting islet cell
tumors, pituitary or adrenal insufficiency, hepatic and renal failure, sepsis and ectopic
production of an insulin-like growth factor (2). However, hypoglycemia is the most
frequent complication experienced by insulin-requiring individuals with diabetes. It is
also the principal factor limiting the glycemic control in people with type 1 diabetes and
late stage type 2 diabetes (1).
For many years investigators performed studies to understand hypoglycemia by
using an acute intravenous bolus of insulin, which resulted in a rapid increase in insulin
concentration followed by a short term hypoglycemia. Garber et al. (3) conducted studies
in healthy humans using insulin injections (0.15 U/kg). The insulin injection resulted in a
rapid fall in glucose production (~30%) followed by a doubling of glucose production by
40 minutes due to an increase in glucagon secretion. The increase in glucose production
was attributable mainly to glucagon’s effects on glycogenolysis (3). This model doesn’t
represent a common clinical condition seen in patients with Type 1 Diabetes in which
hypoglycemia develops gradually and can be present for several hours (4). To
understand better the mechanisms involved in the increase in glucose production during
prolonged hypoglycemia, Lecavalier et al. (5) and Caprio et al. (6) in the human and
Frizzell et al. (7) in the dog, studied the contribution of glycogenolysis and
gluconeogenesis to the regulation of hepatic production during prolonged hypoglycemia.
Frizzell infused a high dose of insulin (5mU/kg/min) intraportally for 3 hours into
overnight fasted conscious dogs. Glucose production fell initially and then doubled by 60

3
minutes. They found that glycogenolysis accounted for ~79% of glucose production
during the first hour of hypoglycemia and gluconeogenesis played a major role by the
third hour of hypoglycemia (~68%). Studies in humans have also concluded that
glycogenolysis accounted for the increase in glucose production in the first hour
following establishment of hypoglycemia while gluconeogenesis played a mayor role
during the subsequent hours of prolonged hypoglycemia (5; 6).
Defense against hypoglycemia
The fall in arterial plasma glucose is sensed in widespread regions of the brain,
portal vein, carotid body and pancreas. When arterial plasma glucose decreases (~80-85
mg/dl) in response to an increase in insulin, there is a reduction of insulin secretion and
enhancement of hepatic glucose production (8; 9). It has been suggested that
glucokinase-mediated sensing in the pancreatic beta cells is involved in this response
(10). As the arterial plasma glucose concentration decreases to ~65-70 mg/dl the
secretion of glucagon and epinephrine increases (8; 9). Under physiological conditions
this response can restore euglycemia without the development of hypoglycemic
symptoms. Glucagon secretion from α cells is regulated by many factors, including
plasma insulin levels, blood substrate concentrations and the autonomic nervous system
(10). Under the control of the CNS, epinephrine is secreted from the adrenal medullae
during hypoglycemia (1). In patients with type 1 diabetes the counterregulatory
mechanisms mentioned above are impaired (8). When plasma glucose decreases to ~60
mg/dl it results in the secretion of norepinephrine, cortisol and growth hormone and to
the development of symptoms (8; 9). Like the epinephrine response, increases in

4
circulating levels of norepinephrine, cortisol and growth hormone are mediated through
the CNS (1).
The glycemic thresholds for the counterregulatory responses described above
apply to insulin induced hypoglycemia. Most studies in vivo used insulin as a
pharmacologic agent to induce hypoglycemia. A study conducted by Flattem et al. (11)
used a glycogen phosphorylase inhibitor to induce hypoglycemia in conscious dogs.
They found that during non insulin-induced hypoglycemia the glycemic threshold for the
increase in glucagon secretion was ~94 mg/dl, which is much higher than the threshold
during insulin-induced hypoglycemia. Therefore, there seems to be a difference in the
glycemic threshold required for the counterregulatory response of the α cell when
hypoglycemia is accompanied by hyperinsulinemia. The mechanism for this increase in
the sensitivity of the α cell to insulin remains unclear but recent studies have shown that
perhaps is attributable to a loss of the fall in intraislet insulin that normally triggers an
increase in glucagon secretion as glucose levels fall (12). For the purpose of our studies
we are going to focus on insulin-induced hypoglycemia.
Hormone Action
The counterregulatory response to hypoglycemia involves the release of glucagon,
epinephrine, norepinephrine, cortisol and growth hormone (1; 4; 13). Studies in humans
and dogs have demonstrated the primary role of glucagon during insulin induced
hypoglycemia (14-17). Studies performed by Gerich et al. (15) in normal and
adrenalectomized humans showed the primary role of glucagon and the secondary role of
epinephrine during insulin-induced hypoglycemia. Dobbins et al. (18) performed studies

5
in overnight fasted conscious dogs to characterize the role of the hormone during insulin-
induced hypoglycemia. A 6 fold rise in glucagon (Δ140 pg/ml) significantly increased
glucose production (Δ 4.5 mg/kg/min) in the presence of hypoglycemia despite an arterial
insulin level that was increased 20 fold (Δ328 µU/ml). The effect of the increment of
glucagon on hepatic glucose production was primarily due to a rapid, time dependent
effect on glycogenolysis and a modest, prolonged effect on gluconeogenesis.
Epinephrine, like glucagon, has been shown to increase production in a rapid,
time-and dose-dependent manner in response to a fall in glucose (19; 20). Studies
performed by Cherrington et al. (21) in overnight fasted conscious dogs showed that an
acute physiological rise in plasma epinephrine was associated with a initial increase in
glucose production due to a glycogenolytic response followed later by a gluconeogenic
response. The effect of epinephrine on glycogenolysis wanes with time like glucagon
(21; 22). This similarity may be explained by the fact that epinephrine exerts its effect by
binding to the β-adrenergic receptors on the liver (23; 24). In addition, Chu et al. (25)
demonstrated that effects of epinephrine on glycogenolysis are the result of a direct effect
of the hormone on the liver. On the other hand, the effects of epinephrine on
gluconeogenesis are the result of its action on peripheral tissues (22; 26-28), specifically
an increase in muscle glycogenolysis and adipose tissue lipolysis.
Norepinephrine is also involved in the counterregulatory response. Circulating
norepinephrine reflects release of the catecholamine from the adrenal medullae but more
importantly its release from sympathetic postganglionic neurons (1; 29). The ability of
norepinephrine to restrain a fall in plasma glucose, while not as potent as epinephrine’s,

6
involves a stimulatory effect on gluconeogenesis which results from a glycogenolytic
effect in muscle and a lipolytic effect in fat (30-32).
Cortisol and growth hormone are referred as “slow acting” hormones because
their effects are seen a few hours after their increase in plasma. Boyle et al. (33)
conducted studies in humans that provide evidence that cortisol and growth hormone are
involved in the defense against hypoglycemia but they are not critical for recovery from a
low blood sugar. Additionally, the authors suggested that the roles of these hormones in
the defense of hypoglycemia are permissive rather than direct. Further, De Feo et al.
(34) have reported that growth hormone effects were evident after 3 hours of insulin-
induced hypoglycemia at which time it enhanced glucose production and decreased
glucose utilization. Goldstein et al. (35; 36) also showed that acute increases in cortisol
have minimal effects on hepatic glucose production whereas chronic infusion of cortisol
(5 days) increased glucose production by maintaining substrate availability to support
gluconeogenesis and by maintaining hepatic glycogen availability. It also had effects in
peripheral tissues where it decreased glucose utilization in muscle and enhanced lipolysis
in adipose tissue.
Autoregulation and other factors
It has been suggested that the liver is capable of adjusting its glucose output in
response to changes in the plasma glucose concentration per se, independent of changes
in the hormones that normally control glucose homeostasis (37; 38). In vitro studies in
perfused rat liver have reported that hepatic glucose production can vary inversely with
the perfusate glucose levels (39). In vivo studies have shown that the hormonal changes

7
are not the only means by which counterrregulation is brought about. Frizzell et al. (40)
performed studies in overnight-fasted conscious dogs to assess the role of the
counterregulatory hormones per se in the response to insulin-induced hypoglycemia. In
one group the counterregulatory hormone response was simulated in the presence of
euglycemia to separate the effects of hypoglycemia per se from those associated with the
counterregulatory hormones. The other groups included a control for the previous group
(insulin + euglycemia) and a group in which insulin was infused alone. They concluded
that the counterregulatory hormones alone accounted for 50% of the response, while the
other 50% resulted from some aspect of hypoglycemia per se. In addition, Bolli et al.
(41) demonstrated the contribution of hepatic autoregulation to hypoglycemic
counterregulation in humans. They assessed the role of hepatic autoregulation during
moderate (~50mg/dl) and severe (~30 mg/dl) hypoglycemia by using somatostatin and
pharmacologic agents to inhibit the secretion of glucagon, growth hormone, cortisol and
to block the action of epinephrine and norepinephrine. Glucagon and growth hormone
were fixed at basal levels while insulin was infused. During moderate hypoglycemia
insulin infusion resulted in complete inhibition of glucose production whereas during
severe hypoglycemia there was an initial suppression of glucose production followed by
an increased in glucose production two times higher than the moderate hypoglycemic
group. Therefore, the authors concluded that hepatic autoregulation is a component of
the counterregulatory response during severe hypoglycemia. Further, Connolly et al. (42)
conducted studies in adrenalectomized overnight-fasted conscious dogs to control for
epinephrine and cortisol release and used somatostatin to clamp insulin and glucagon.
During the euglycemic-hyperinsulinemic control period the liver displayed net hepatic

8
glucose uptake, but as the plasma glucose levels dropped there was a stepwise increase in
net hepatic glucose output despite the absence of counterregulatory hormones. The
authors, therefore, concluded that non-hormonal mechanisms including autoregulation
and direct neural input to the liver can stimulate glucose production in response to
insulin-induced hypoglycemia.
The brain is known to be responsible for most of the rise in the counterregulatory
hormones during hypoglycemia but it also affects glucose production directly (43). It
has been reported that stimulation of the VMH results in an increase in hepatic glucose
production (44) and that electrical stimulation of hepatic nerves results in hyperglycemia
(45). Furthermore, Borg et al. (46) have reported that the VMH stimulates the
counterregulatory response during hypoglycemia in rats. In addition, Connolly et al.
(47) conducted studies to determine if the increase in glucose production seen in the
absence of the counterregulatory hormones is either initiated by liver (autoregulation) or
the brain (neural input) in overnight-fasted conscious dogs. They observed that in the
absence of counterregulatory hormones, hypoglycemia sensed at the liver results in an
increase of hepatic glucose production whereas hypoglycemia sensed at the brain
stimulates the lipolytic and ketogenic responses. Taken together, these studies clearly
indicate that non hormonal mechanisms (autoregulation and neural input to the liver) also
play a role in the metabolic response to hypoglycemia.
Although much about the counterregulatory response during hypoglycemia is
known a controversy still remains regarding the site at which the change in the plasma
glucose level is sensed. The brain and the hepato-portal region have both been postulated
to contain glucose sensing neurons that are responsible for triggering the

9
counterregulatory response. Biggers et al. (43) performed studies in which euglycemia
was maintained in the brain but hypoglycemia was allowed to occur elsewhere. Under
these circumstances, the plasma glucagon levels decreased, the sympathetic nervous
system response to hypoglycemia was blunted and a rise in glucose production was
attenuated by 75%. On the other hand, Donovan et al. (48) has shown that when
glucose was infused into the hepato-portal region during insulin-induced hypoglycemia
there was an inhibition of the sympathetic response to hypoglycemia. Therefore, the
authors suggested that glucose sensing neurons in the hepato-portal region are important
in the response of the sympathetic nervous system to hypoglycemia, supporting the view
that hypoglycemic sensing occurs at peripheral sites. On the other hand, Jackson et al.
(49; 50) have conducted vagal blockade and liver denervation studies resulting in no
prevention of the counterregulatory response to hypoglycemia. More recently, Saberi et
al. (51) conducted studies in chronically cannulated rats that underwent afferent ablation
of spinal afferent nerve endings in the portal vein (PV) or portal and superior mesenteric
veins (PMV) nerve endings to determine if the rate by which glucose falls determines the
primacy of the hypoglycemic sensing. Their data showed that when PV and PMV were
ablated using capsaicin, the sympathetic response was suppressed when hypoglycemia
developed slowly (~80 min). However, when hypoglycemia was reached quickly (~ 20
min) the responses were minimally decreased (15-30 %). Therefore, it seems that low
blood glucose levels are sensed by central and peripheral mechanisms and the
predominance between them is rate sensitive. It should be noted however that glucagon
secretion is solely under the control of central rather than peripheral glucose sensors.

10
Glucagon action and signaling The main physiological role of glucagon is to stimulate hepatic glucose
production. Studies in humans and dogs have established the dose response relationship
between plasma glucagon levels and hepatic glucose production (52; 53). Stevenson at
al. (20) showed using overnight fasted conscious dogs that a selective rise in glucagon (2-
,4-,8-, and 12-fold) for 3 hours resulted in a sensitive dose-dependent increase in glucose
production. In addition, studies in our laboratory have demonstrated that in the presence
of basal insulin a fourfold rise of the hormone produces a half-maximal activation of
hepatic glucose production (~Δ 5.0 mg/kg/min) despite mild hyperglycemia (52).
Additionally, a small change (<10 pg/ml) in arterial plasma glucagon results in an
increase in glucose production of ~ 0.5 mg/kg/min (52; 53). Not only are glucagon’s
effects on hepatic glucose production potent, they also have been shown to be rapid since
it takes ~4.5 minutes for the hormone to half-maximally activate the liver (54). All
together glucagon is a potent and rapid stimulator of hepatic glucose production, and a
small change of the hormone can result in significant changes in hepatic glucose output.
Glucose production by the liver is the result of either glycogen breakdown
(glycogenolysis) or de novo synthesis of glucose from gluconeogenic precursors
(gluconeogenesis). In the dog and the human, the effect of an increment in glucagon on
hepatic glucose production has been shown to be primarily due to a rapid, time dependent
stimulation of glycogenolysis and a modest more prolonged effect on gluconeogenesis
(55-57). The time dependence of glucagon’s effect on glycogenolysis is in part related to
the progressive inhibitory effect of hyperglycemia that occurs in response to the hormone
and in part to factors endogenous to the liver that limit the action of the hormone (58; 59).

11
Glucagon’s effects on gluconeogenesis are more modest. Studies have shown that the
hormone regulates amino acid transport into liver via the transcriptional expression of the
hepatic Na+-dependent amino acid transport system A (60). In addition the hormone is
known to stimulate transcription of gluconeogenic enzymes like PEPCK and G-6-Pase
(61-65). It also enhances the phosphorylation of pyruvate kinase, and
phosphofructokinase and decreases intracellular levels of fructose-2, 6-P2, resulting in
inhibition of glycolysis and stimulation of gluconeogenesis (61). The reason for the
limited effect of glucagon on gluconeogenesis, despite its hepatic effects, lies in its
inability to increase gluconeogenic substrate mobilization from the peripheral tissues
such as muscle and fat (66). In fact there are no glucagon receptors in muscle and there
are very few in adipose tissue (67). As one would predict from this observation
glucagon does not have effects on glucose utilization by adipose tissue or skeletal muscle
(20; 68; 69). Likewise it has minimal effects on lipolysis and protein metabolism.
Glucagon exerts its effects by binding to the glucagon receptor (Figure 1.1). The
glucagon receptor belongs to the superfamily of heptahelical transmembrane G protein-
coupled receptors, which is divided into subfamilies based on amino acid sequence. A
large number of G proteins have been identified: Gs, Gi and Gq and subsets of these
proteins. Each G protein consists of three subunits, α, β and γ (70-74). The binding of
glucagon to the receptor results in conformational changes of the latter, leading to
subsequent activation of the coupled G proteins. Upon G protein-coupled receptor
activation, guanosine diphosphate (GDP) is exchanged for guanosine triphosphate (GTP),
which dissociates the G protein complex into 2 units: the Gα and Gβγ subunits. These
subunits in turn activate or inhibit enzymes. Activation of Gq results in the activation of

12
phospholipase C (PLC) which causes the production of inositol 1,4,5-triphosphate and
subsequent release of intracellular calcium (70; 75). The extent to which this pathway
contributes to glucose production remains unclear. There are in fact inconsistencies in
the data; some investigators have found that in the presence of a physiological increment
of glucagon there is an increase in intracellular calcium (76), while others have found that
calcium only increases in response to a supra-physiological increment in glucagon (77).
A study performed by Yamatani et al. (78) showed that glucagon increased glucose
production mainly through the cAMP pathway and that Ca2+ dependency was only
observed when the cAMP pathway was inhibited and when supra-physiological levels of
glucagon were present (78).
On the other hand, activation of Gs leads to the activation of adenyl cyclase, and
elevation of cAMP (61; 67; 70; 79). The rise in cAMP causes the activation of c-AMP-
dependent protein kinase or PKA (80), leading to the phosphorylation of a number of
cellular proteins involved in glycogenolysis, gluconeogenesis, glycolysis and glycogen
synthesis (67; 70; 79).
Glucagon stimulates glycogenolysis through the activation of PKA. PKA
catalyzes the phosphorylation of a single serine residue in each subunit of glycogen
phosphorylase. The phosphorylation of the serine-14 residue leads to major changes in
the catalytic and physical properties of the enzyme (81). This in turn increases glycogen
breakdown and net hepatic glucose output. Another effect of glucagon is inhibition of
glycogenesis. Glucagon controls glycogenesis by inducing the phosphorylation and
inactivation of glycogen synthase. Studies have shown that the enzyme is subject to
multi-site phosphorylation, some of which results in the inactivation of the enzyme.

13
Recent studies have suggested that PKA activation by cAMP leads to the
phosphorylation of cAMP response element-binding protein (CREB). PKA
phosphorylates CREB at serine 133 leading to its activation (82). CREB is a
transcription factor that induces the expression of key genes involved in the
gluconeogenic pathway such as PEPCK and G-6-Pase (83). PGC-1 (Peroxisome
proliferator-activated receptor- coactivator) is a transcriptional target of CREB and its
expression is triggered by elevated cAMP levels (84). Studies performed by Yoon et al.
(85) showed that overexpression of PGC-1 in liver increased glucose production and the
transcription of genes encoding gluconeogenic enzymes. In addition Heizig et al. (86)
provided evidence that the metabolic effects of cAMP in the liver may be mediated
through PGC-1. Furthermore studies have shown that the nuclear transcription factor
hepatocyte nuclear factor-4 (HNF-4) acts together with PGC-1 to increase the
transcription of PEPCK (85). Transcription factors function through the docking of
specific coactivitors or corepressors proteins. Recently Koo et al. (87) identified the
transcriptional regulator TORC2 (Transducer of regulated CREB activity 2) as an
important component of the gluconeogenic gene regulation (87; 88). Furthermore,
glucagon has been shown to activate glucose-6-phosphatase activity (89). Hornbuckle et
al. (90) have shown that glucagon increased the G-6-Pase activity by selectively
stimulating the transcription of the G-6-Pase catalytic subunit but not the G-6-Pase
transporter and they found that the effect is cAMP dependent (90).
In addition glucagon via cAMP and PKA enhances the phosphorylation of
pyruvate kinase and phosphofructokinase and decreases intracellular levels of fructose-2,
6-P2, resulting in the inhibition of glycolysis (61; 91). Fructose-1, 6-P2ase catalyzes the

14
hydrolysis of the C-1 phosphate in fructose 1, 6-P2 into fructose 6-P. Fructose-1, 6-P2ase
is allosterically inhibited by fructose 2, 6-P2. The levels of fructose 2, 6-P2 are regulated
by the hepatic bifunctional enzyme, 6PF-2-K/Fru-2, 6-P2ase. Studies have shown that
upon glucagon stimulation, activated PKA phosphorylates, 6PF-2-K/Fru-2, 6-P2ase in the
liver at serine-32, leading to the inhibition of the kinase and activation of the
phosphatase. This in turn reduces the intracellular levels of the fructose-2, 6-P2, thereby
relieving the inhibition of fructose-1, 6-P2ase and stimulating gluconeogenesis (91-93).
Phosphofructokinase is allosterically activated by fru-2,6-P2ase therefore the
activated PKA by reducing the levels of the biphosphate also causes the inhibition of the
phosphofructokinase (92; 94). In addition, glucagon inhibits pyruvate kinase due to the
PKA phosphorylation and it also inhibits transcription of the pyruvate kinase gene and
increases the degradation of pyruvate kinase mRNA (92; 95).

15
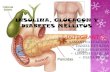
Figure 1.1: Glucagon receptor-signaling pathway
(cAMP) Adenosine 3’,5’-cyclic monophosphate; (PKA) protein kinase A; (GS) Glycogen Synthase; (GPK) Glycogen Phosphorylase Kinase; (GP) Glycogen Phosphorylase; (I-1) Inhibitor 1; (PP1) Protein Phosphatase 1; (PGC-1) Peroxisome Proliferator-Activated Receptor-γcoactivator; (PEPCK) Phosphoenolpyruvate Carboxykinase; (G-6-Pase) Glucose-6-Phosphatase; (PFK-2/F2,6P2ase) 6-phosphofructo-2-kinase/fructose-2,6-bisphosphatase; (PK) L-type pyruvate kinase; (PLC) Phospholipase C; (PIP2) Phosphatidylinositol 4,5-biphosphate; (PIP3) Posphatidylinositol 3,4,5 trisphosphate; (CREB) cAMP Responsive element binding protein; (TORC2) Transducer of regulated CREB activity 2. From reference (70).
CREB TORC2CREB TORC2CREB TORC2

16
Insulin action and signaling
Insulin has a wide variety of physiologic effects in different tissues. Insulin
stimulates cell growth and differentiation and promotes the storage of substrates in fat,
liver and muscle by stimulating lipogenesis, glycogen synthesis and protein synthesis and
by inhibiting lipolysis, glycogenolysis, gluconeogenesis and protein breakdown (96). It
has been known for many years that increasing plasma insulin levels results in an
inhibition of glucose production. In addition, there was a dose-dependent relationship
between hepatic sinusoidal insulin levels and glucose production (52; 53).
Insulin rapidly inhibits hepatic glucose production, but it requires several hours
(~3 hours) to reach its steady state effect (97). A number of investigators have studied
the ability of insulin to inhibit glycogenolysis and gluconeogenesis. In vitro studies have
shown that insulin represses gluconeogenesis by inhibiting PEPCK and G-6-Pase gene
transcription (61; 98) More recently Hall et al. (99) found that addition of insulin to
dexamethasone-treated cells results in a rapid dissociation of the glucocorticoid receptor,
polymerase II, and other transcriptional regulators from the PEPCK and G-6-Pase gene
promoter. They suggested that insulin caused the demethylation of arginine-17 on
histone H3 of both genes, leading to the reduction in gene transcription of both genes.
On the other hand in vivo studies performed in humans and dogs have shown that the
effect of insulin in gluconeogenesis is minimal and that its main effect comes about
through an inhibition of glycogenolysis (100; 101). Edgerton et al. (101) conducted
studies in overnight fasted conscious dogs in which they used three different methods to
determine gluconeogenesis and glycogenolysis. They found that the liver glycogenolysis
is markedly sensitive to small changes in insulin whereas the gluconeogenic flux is not.

17
For many years insulin was thought to decrease hepatic glucose production by a
direct interaction with its hepatic receptor. That was until in 1987 when Prager et al.
(102) suggested that the hormone can suppress glucose production through indirect
actions. In these studies carried out using insulin-resistant obese subjects insulin was
infused peripherally in the presence of euglycemia and hepatic glucose production was
suppressed by 82%. There was a decrease in endogenous insulin secretion in response to
peripheral insulin infusion such that portal insulin levels were calculated to have changed
minimally. Thus the authors concluded that indirect effects of the hormone caused the
inhibition of glucose production since the insulin level at the liver did not change
appreciably (102). This concept has subsequently been supported by others (103; 104)
but the indirect mechanisms by which insulin suppresses hepatic glucose production was
probably best demonstrated in a study performed by Sindelar et al (105). The authors
used overnight fasted conscious dogs to investigate the mechanism of a selective increase
in either peripheral or portal insulin in changing hepatic glucose production. A selective
rise of 14µU/ml in either the arterial insulin or portal insulin was associated with a
decrease in NHGO of ~ 50%. Even though the extent to which insulin inhibited hepatic
glucose production was similar in both groups, the time required for the inhibition and
the mechanism for the inhibition was markedly different. The response of the liver to a
selective increase in portal insulin (direct action) was observed at 15 minutes and it was
attributable to an inhibition in glycogenolysis. On the other hand, the response of the
liver to a selective rise in arterial insulin (indirect action) occured slowly (~ 1 hour) and
resulted from the suppression of hepatic gluconeogenic precursor uptake secondary to a
reduction in gluconeogenic amino acid flux from muscle and glycerol from adipose tissue

18
and from the redirection of glycogenolytic carbon to lactate due to a decrease in NEFA
levels (105; 106). Therefore, insulin inhibits hepatic glucose production by directly
inhibiting glycogenolysis and indirectly by inhibiting net gluconeogenic flux and
lipolysis.
In addition to insulin’s indirect effects in the muscle and fat, it has been reported
that insulin can inhibit the alpha cell leading to inhibition of glucagon secretion. In
unpublished data from our laboratory a rise of insulin of ~ 20µU/ml resulted in a decrease
in glucagon to ~15pg/ml. In addition, in perfused pancreas from rats a retrograde
infusion of ~0.3mU/ml of insulin significantly inhibit glucagon secretion (107). Recent
investigations have provided some insight into the possible mechanisms by which insulin
inhibits glucagon secretion. It appears that insulin increases α-cell KATP channel activity
in PI-3K dependent manner thus resulting in hyperpolarization of the membrane and
inhibition of α-cell electrical activity and glucagon secretion (108; 109). Another
mechanism proposed recently, involves the GABA-GABAA receptor system. Insulin has
been reported to activate GABAA receptors in the α-cells through receptor translocation
via an AKT kinase-dependent pathway, leading to hyperpolarization and ultimately
inhibition of glucagon secretion (110). In any event any insulin induced decrease in
glucagon levels would reduce glucose production by the liver.
Furthermore, it has been suggested that insulin’s action in the brain may explain
part of insulin’s indirect actions in the liver. Studies performed by Davis et al. have
shown that the brain can sense circulating insulin levels (111). It is also known that the
brain provides neural drive to the liver (112). Most recently, Obici et al. (113) showed
that infusion of insulin into the third ventricle in six hour fasted conscious rats resulted in

19
suppression of glucose production. They also showed that blockade of the insulin
receptor using an antisense oligonucleotide injection into the hypothalamus impaired the
ability of a rise in plasma insulin to inhibit hepatic glucose production. Thus they
concluded that hypothalamic insulin signaling could be important to the action of insulin
on the liver. On the other hand, Edgerton et al. (114) carried out a study to determine the
effect of a 4-fold rise in the head insulin on hepatic glucose production during peripheral
hyperinsulinemia and hepatic insulin deficiency in overnight fasted conscious dogs.
They found that an acute 4-fold rise of insulin in the head did not reduce hepatic glucose
production. Furthermore, they demonstrated that the direct effects of insulin on hepatic
glucose production are dominant. The different results obtained in these studies might be
explained by the differences between the animal model used (rodents and dogs) and acute
effects vs. chronic effects of insulin. The glucose production rate is much greater in the
rodents compared to the dog or human. The hepatic glucose production rate of a rat or
mouse is ~12 and 20 mg/kg/min, respectively, whereas in the dog or human it is ~2-
3mg/kg/min. . It is conceivable that this might result in the existence of higher neural
drive to the liver in the rodent than in the dog or human (115; 116). Furthermore, it is
possible that an acute increment in insulin is not able to acutely regulate hepatic glucose
production via an action on the brain whereas a chronic rise in insulin might be able to
(115; 116).
Insulin exerts its effect by binding to the insulin receptor. The insulin receptor
(IR) is a tetrameric protein that consists of two extracellular α-subunits and two
intracellular β-subunits linked together by disulfide bonds. It belongs to a subfamily of
receptor tyrosine kinases which also includes the insulin growth factor-1 receptor

20
(IGF1R) and IR-related receptor (IRR) (117). Binding of insulin to the α-subunit induces
a conformational change resulting in the autophosphorylation of several tyrosine residues
present in the β-subunit (96; 118). These residues are recognized by phosphotyrosine-
binding (PTB) domains of adaptor proteins such as members of the insulin receptor
substrate family (IRS), Gab-1, Shc and Cbl. (96; 118; 119). Upon tyrosine
phosphorylation, these proteins interact with signaling molecules through their SH2
domains. This results in the activation of PI 3-Kinase and downstream PtdIns(3,4,5)P3,
ras, MAP kinase cascade, Cbl/CAP and TC10 (96). Cbl/CAP and TC 10 are involved in
stimulation of glucose uptake and GLUT4 translocation. The MAPK pathway regulates
the expression of some genes and cooperates with the PI3K pathway to control cell
growth and differentiation. The PI 3-kinase pathway is responsible for the metabolic
aspects of insulin action. For the purpose of this thesis we will focus on the PI-3K
pathway.
The metabolic effects of insulin are mediated through downstream effectors of
Phosphoinositide 3-kinase (PI3K), atypical protein kinase (aPKC) and Protein Kinase B
(PKB) or Akt. Previous studies have reported that the increase in plasma insulin that
follows a carbohydrate meal results in a decreased transcription and translation of
PEPCK in vitro (61; 120). In addition, studies have shown that insulin represses G-6-
Pase gene expression in vitro and in vivo (121; 122). Furthermore, overexpression of the
catalytic subunit of PI 3-kinase is sufficient to markedly inhibit PEPCK and G-6-Pase
gene expression (123). In addition more recently studies conducted by Dentin et al. (124)
have reported that insulin inhibits the gluconeogenic gene expression during re-feeding
by promoting the phosphorylation and degradation of TORC2, a cAMP-responsive

21
CREB coactivator. All together these effects of insulin on gluconeogenic gene
expression contribute to the reduction in gluconeogenesis seen after the ingestion of a
carbohydrate meal.
After a carbohydrate meal, insulin stimulates glycogen synthesis and inhibits
glycogen breakdown. Glycogen synthase, an enzyme that catalyzes the rate-determining
step in glycogen synthase, is regulated by insulin through changes in phosphorylation.
Insulin activates glycogen synthase by promoting its dephosphorylation via the inhibition
of GSK-3 (96). This results in the inactivation of GSK-3 and in the disinhibition of
glycogen synthase, leading to an increase in glycogen synthesis. In addition, PP1 also
reduces GSK-3 activity and inhibits glycogen phosphorylase, a key enzyme in glycogen
breakdown (96). In addition, insulin stimulates PDE3B which promotes the degradation
of cAMP in the liver. The reduction in cAMP results in decreased activation of PKA and
a subsequent decrease in glycogenolysis in the liver (91; 125-127).
In addition, PI3K is an upstream regulator of mTOR (mammalian target of
rapamysin) which is a central regulator of ribosome biogenesis, protein synthesis, cell
growth. mTOR controls the translation machinery, in response to aminos acids and
growth factors via activation of p70 ribosomal S6 Kinase and inhibition of eIF-4E
binding protein (128). Therefore, insulin effects on GSK-3, PP1, mTOR and PDE inhibit
glucose production, promote glycogen, FFA, protein and triglycerides synthesis, all
together, opposing glucagon’s action.

22
Figure 1.2. Insulin-receptor signaling pathway Insulin receptor substrate family (IRS), Gab-1, Shc and Cbl. Phosphoinositide 3-kinase (PI3K); atypical protein kinase (aPKC); Protein Kinase B (PKB) or Akt; mammalian target of rapamysin (mTOR); Protein Phosphatase 1 (PP1); Glycogen Synthase Kinase 3 (GSK-3). From reference (96).
cAMP5’-AMP PDE3
mTORcAMP5’-AMP PDE3
mTOR

23
Insulin and glucagon interaction
Insulin and glucagon are potent regulators of carbohydrate metabolism and their
interaction is usually the main determinant of gluconeogenic and glycogenolytic flux in
the liver. After an overnight fast, glucagon plays a major role in stimulating hepatic
glucose production while insulin acts as a potent inhibitor of the process. Glucagon can
be considered to provide the positive drive to the liver which allows insulin to exert its
controlling effects on glucose production.
In response to carbohydrate ingestion, insulin secretion increases whereas
glucagon secretion decreases (52; 53). These changes in hormone secretion, along with
the hyperglycemia that results from the glucose load and the portal glucose signal, inhibit
hepatic glucose production and convert the liver to net glucose consumtion (53; 129).
Insulin is an anabolic hormone that promotes storage of substrates in fat, liver and
skeletal muscle by stimulating triglyceride, glycogen and protein synthesis, and inhibiting
lipolysis, and glycogen and protein breakdown (130)
Furthermore, Steiner at al. (131) has previously examined the interaction between
insulin and glucagon in controlling glucose production using a pancreatic clamp in the
conscious dog. A constant replacement of basal amounts of insulin and glucagon did not
change glucose production. A selective four-fold rise in glucagon resulted in an
increment in glucose production of ~4.5 mg/kg/min at 30 minutes. In contrast, a
selective four-fold rise in insulin resulted in a decrement in glucose production of ~1.3
mg/kg/min at 30 minutes. When both hormones were simultaneously increased fourfold,
the decrement in glucose production at 30 minutes was only ~0.6 mg/kg/min. Therefore,
glucagon’s effect was 4.5 mg/kg/min in the presence of basal insulin despite a developing

24
hyperglycemia and only 0.7 mg/kg/min in the presence of high insulin, a reduction of
almost 85%. Consequently, insulin dominates glucagon’s action on the liver even if the
increments are equimolar (131). This was not the case in the presence of hypoglycemia
as seen in another previous study (18). A 6 fold rise in glucagon (Δ140 pg/ml)
significantly increased glucose production (Δ 4.5 mg/kg/min) in the presence of
hypoglycemia despite an arterial insulin level that was increased 20 fold (Δ328 µU/ml).
Therefore, glucagon appears to be more effective during hypoglycemia than during
euglycemia, despite dramatically increased insulin levels.
Despite the fact that previous studies have suggested that the liver is more
sensitive to glucagon during hypoglycemia, a direct comparison of the effects of a
controlled rise in glucagon on glucose production in the presence of euglycemia versus
hypoglycemia has never been carried out. Therefore, the aim of this work was to
examine the interaction of a selective rise in insulin and glucagon in controlling hepatic
glucose production under euglycemic and hypoglycemic conditions.

25
CHAPTER II
MATERIALS AND METHODS
Animal Care
Studies were conducted on twenty-four 18 h fasted conscious mongrel dogs (18-
25 kg) of either sex that had been fed a standard diet of meat (Kal Kan, Vernon, CA) and
chow (Purina Lab Canine Diet No. 5006; Purina Mills, St. Louis, MO) composed of 34%
protein, 14.5% fat, 46% carbohydrate, and 5.5% fiber based on dry weight (1500
kilocalories). Water was available at all times. Only dogs that had good appetite, a
leukocyte count < 18,000/mm3, a hematocrit >35%, and normal stools were used for
studies. The animals were housed in a facility which met the American Association for
Accreditation of Laboratory Animal Care guidelines, and the protocol was approved by
the Vanderbilt University Medical Center Animal Care Committee.
Surgical Procedures
Approximately 16 days prior to the metabolic study, surgery was performed on
each dog while it was under general anesthesia. Anesthesia was induced with propofol
(given until induction) preceded by buprenorphine HCl (0.02 mg/kg, presurgery) 30 min
earlier. Anesthesia was maintained by isoflurane (1.5-2.0% with oxygen) inhalation. The
dog was placed in a supine position on a surgical table with an 8.5 mm inner diameter
(ID) endotracheal tube (Concord/Protex, Kenee, NH), and ventilated with a tidal volume
of 400 ml at 14 breaths per minute.

26
A laparotomy was performed by making a midline incision 1.5 cm caudal to the
xyphoid process through the skin, subcutaneous layers and linea alba, and extending
caudally 15-20 cm. Silastic catheters (0.03 in ID; HelixMedical, Carpintera, CA) were
placed in the following manner: A portion of the jejunum was exposed and a branch of a
jejunal vein was selected for cannulation. A small section of the vessel was exposed by
blunt dissection and ligated with 4-0 silk (Ethicon, Inc, Sommerville, NJ). A silastic
infusion catheter was inserted into the vessel through a small incision and passed
antegrade until the tip of the catheter lay approximately 1 cm proximal to the coalescence
of two jejunal veins. Another silastic catheter was inserted into a distal branch of the
splenic vein and advanced until the tip of the catheter lay 1 cm beyond the bifurcation of
the main splenic vein. The catheters were secured in place with 4-0 silk.
For blood sampling, silastic catheters (0.04 in ID) were placed into the left hepatic
vein, the hepatic portal vein and left femoral artery. The central and left lateral lobes of
the liver were retracted cephalically and caudally, respectively. The left common hepatic
vein and the left branch of the portal vein were exposed. A 14-gauge angiocath (Benton
Dickinson Vascular Access, Sandy, UT) was inserted in the left branch of the portal vein
2 cm from the central liver lobe. A silastic catheter (0.04 in ID) was inserted into the hole
created by the angiocath, advanced retrograde about 4 cm into the portal vein so that the
tip of the catheter lay 1 cm beyond the bifurcation of the main portal vein. It was then
secured with three ties of 4-0 silk through the adventitia of the vessel and around the
catheter. An angiocath was inserted into the left common hepatic vein 2 cm from its exit
from the left lateral lobe. A silastic sampling catheter was inserted into the hole and
passed antegrade 2 cm and secured into place with three ties of 4-0 silk suture.

27
For sampling of arterial blood, a catheter was inserted into the left femoral artery
following a cut-down in the left inguinal region. A 2 cm incision was made parallel to
the vessel. The femoral artery was isolated and ligated distally. A silastic catheter (0.04
in ID) was inserted and advanced 16 cm in order to place the tip of the catheter in the
abdominal aorta. It was then secured into place with 4-0 silk suture.
All catheters were filled with normal saline (Baxter Healthcare Corp, Deerfield,
IL) containing 200 U/ml heparin (Abbott Laboratories, North Chicago, IL) and knotted.
Abdominal catheters were secured to the abdominal wall and placed in a subcutaneous
pocket prior to closure of the skin. The arterial sampling catheter was also placed in a
subcutaneous pocket prior to closure of the skin.
Ultrasonic flow probes (Transonic System Inc, Ithaca, NY) were positioned
around the hepatic artery and portal vein, to determine liver blood flow during
experiments. The duodenum was retracted laterally to expose a section of the hepatic
artery and portal vein. A small section of the portal vein was exposed by blunt dissection,
taking care not to disturb the nerve bundle located on the vessel. A 6 or 8 mm ID
ultrasonic flow probe (Transonic Systems Inc, Ithaca, NY) was placed around the vessel.
A small portion of the common hepatic artery was also carefully exposed and a 3 mm ID
ultrasonic flow probe was secured around the vessel. To prevent blood from entering the
portal vein beyond the site of the flow probe, the gastroduodenal vein was isolated and
ligated. Blood that would normally flow through the gastroduodenal vein was shunted
through the caudal pancreatoduodenal vein draining the tail of the pancreas. The
ultrasonic flow probe leads were positioned in the abdominal cavity and secured with the
ends of the catheters to the abdominal wall.

28
After all abdominal surgeries, the subcutaneous layer was closed with a
continuous suture of 2-0 chromic gut (Ethicon, Inc.). The skin was closed with
horizontal mattress sutures of 3-0 Dermalon (Ethicon, Inc.). Immediately following
surgery, the dogs received an intramuscular injection of penicillin G (106 U, Procaine;
Anthony Products, Irwindale, CA) to minimize the possibility of infection. In addition,
Flunixin (Meglumine 50mg/ml; Phoenix Scientific, Inc., St. Joseph, MO) was injected
intramuscularly (1 mg/kg body weight) after wound closure for acute pain relief.
Animals awoke from surgery within 2 h, were active, and ate normally approximately 8 h
after surgery. Post-operatively, each dog also received 500 mg ampicillin (Principen;
Bristol-Myers Squibb, Princeton, NJ) orally twice a day for 3 days.
Experimental Procedure
On the day of the experiment following an 18h fast, the free ends of the catheters
and ultrasonic leads were removed from their subcutaneous pockets under local
anesthesia (2% lidocaine; Abbott Laboratories, North Chicago, IL). The contents of each
catheter were aspirated, and they were flushed with saline. Blunt needles (18 gauge;
Monoject, St. Louis, MO) were inserted into the catheter ends and stopcocks (Medex,
Inc, Hilliard, OH) were attached to prevent the backflow of blood between sampling
times.
Twenty gauge Angiocaths (Beckton Dickson) were inserted percutaneously into
the left and right cephalic veins and into a saphenous vein for the infusion of
somatostatin, tracers, dye and glucose. A continuous infusion of heparinized (1U/ml;
Abbott Laboratories, North Chicago,IL) normal saline was started via the femoral artery

29
at a rate to prevent any clotting in the line. Animals were allowed to rest quietly in a
Pavlov harness for at least 100 min before the start of the experiment.
Experimental Design
The study included four groups of animals: saline-euglycemia (SE), saline-
hypoglycemia (SH), glucagon-euglycemia (GE) and glucagon-hypoglycemia (GH). Each
experiment consisted of equilibration (-140 to -40 min), basal (-40 to 0 min) and
experimental (0 to 180 min) periods (Figure 2.1). At -140 min a priming dose of [3-3H]
glucose (33 µCi) was given, followed by a constant infusion of [3-3H] glucose
(0.35µCi/min) and indocyanine green (0.08 mg/min). The equilibration period was
followed by a control period and an experimental period which was divided into period 1
(0-60 min) and period 2 (60-180 min). In period 1, somatostatin (0.8µg/kg/min) and
intraportal insulin (5.0 mU/kg/min) were infused and glucose was monitored every five
minutes in order to maintain euglycemia using glucose infusion through the saphenous
vein as required (20% Dextrose). In period 2, the somatostatin and insulin infusions were
continued and in addition either glucagon (2.3ng/kg/min) or saline were infused
intraportally. Glucose was infused as required to bring about euglycemia (~100 mg/dl) or
hypoglycemia (~50 mg/dl).

30
Figure 2.1: Experimental Design
Po Glucagon (2.3 ng/kg/min) or Saline
Euglycemia
Hypoglycemia
Po Glucagon (2.3 ng/kg/min) or Saline
180-40 min 0 60CP P2P1
Pe Somatostatin (0.8 g/kg/min) + Po Insulin (5.0 mU/kg/min)
Pe Glucose(Euglycemia)
[3-3H]-Glucose (0.35µCi/min) + Indocyanine Green (0.08 mg/min)
SAL + EU (n=6)
GGN + EU (n=6)
SAL + HYPO (n=6)
GGN + HYPO (n=6)
Pe - Peripheral; Po - PortalCP - Control Period P1 - Period 1; P2 - Period 2
Po Glucagon (2.3 ng/kg/min) or Saline
Euglycemia
Hypoglycemia
Po Glucagon (2.3 ng/kg/min) or Saline
180-40 min 0 60CP P2P1
Pe Somatostatin (0.8 g/kg/min) + Po Insulin (5.0 mU/kg/min)
Pe Glucose(Euglycemia)
[3-3H]-Glucose (0.35µCi/min) + Indocyanine Green (0.08 mg/min)
SAL + EU (n=6)
GGN + EU (n=6)
SAL + HYPO (n=6)
GGN + HYPO (n=6)
Pe - Peripheral; Po - PortalCP - Control Period P1 - Period 1; P2 - Period 2 Pe - Peripheral; Po - PortalCP - Control Period P1 - Period 1; P2 - Period 2

31
Collection and Processing of Samples
Blood samples were drawn from the femoral artery and portal and hepatic veins at
the predetermined time points. Additionally, whenever the experimental design required
a glucose clamp, small (~0.5 ml) arterial samples were drawn every 5 min to facilitate
maintenance of the plasma glucose concentration. Before samples were taken, the
sampling catheter was cleared by withdrawing 5 ml of blood into a syringe. After
sampling, this blood was re-infused and the catheter was flushed with heparinized saline
(1 U/ml; Abbott Laboratories, North Chicago, IL). The total volume of blood withdrawn
did not exceed 20% of the animal’s blood volume, and two volumes of normal saline
(0.9% sodium chloride; Baxter Healthcare Co., Deerfield, Il) were given for each volume
of blood withdrawn. No significant decrease in hematocrit occurred throughout duration
of study.
Before the experiment started, an arterial blood sample was drawn and
centrifuged (3000 rpm for 7 min). The plasma from this blood sample was used to
prepare hormone infusates and the indocyanine green standard curve. When samples
were taken from all vessels, the arterial and portal blood samples were collected
simultaneously ~30 s before the collection of the hepatic vein samples in an attempt to
compensate for the transit time through the liver, and thus allow for the most accurate
estimates of net hepatic substrate balance (132).
Immediately following each sample collection, the blood was processed. A 20 l
aliquot of arterial whole blood was used for the immediate duplicate measurement of
hematocrit using capillary tubes (0.4 mm ID; Drummond Scientific Co., Broomall, PA).
One ml of the collected blood was placed in a tube containing 20µl of 0.2M glutathione

32
(Sigma Chemical Co.) and 1.8mg EGTA (Sigma Chemical Co.) for catecholamine
measurements. This tube was vortexed, centrifuged at 3000 rpm for 7 minutes, and the
supernatant was stored in a separate tube for later analysis. The remaining blood was
placed into tubes containing potassium ethylenediaminetetraacetate (EDTA, 1.6 mg/ml;
Sarsdedt, Newton, NC), inverted and gently mixed. One ml aliquot of whole blood was
lysed with 3 ml of 4% perchloric acid (PCA; Fisher Scientific, Fair Lawn, New Jersey),
centrifuged and the supernatant was stored for later analysis of metabolites levels (lactate,
alanine, -hydroxybutyrate and glycerol). The remainder of the whole blood was
centrifuged at 3000 rpm at 4º C to obtain plasma.
The plasma samples were used for all other measurements. Glucose
concentrations were immediately determined from four 10 l aliquots of plasma using the
glucose oxidase method with a glucose analyzer (Beckman Instruments, Fullerton, CA).
A 1 ml aliquot of plasma received 50 l of 10,000 KIU/ml Trasylol (FBA
Pharmaceuticals, New York, NY) and was stored for analysis of glucagon. Insulin, [3H]-
glucose, free fatty acids and cortisol were measured from aliquots of plasma (1.0, 1.0, 0.5
and 0.5 ml respectively) The arterial and hepatic insulin samples were used for
measurement of indocyanine green, as will be described later, and then frozen at -70ºC
until insulin was measured. After each sample was processed, it remained on wet ice for
the remainder of the experiment and was then stored at -70º C until analysis was
performed.
Following the study, the plasma samples for [3H]-glucose measurement were
deproteinized by stepwise addition of 5 ml of 0.067 N Ba(OH)2 and 5 ml 0.067 N ZnSO4

33
(Sigma Chemical Co.). These samples were then stored at 4ºC for 1-3 days and then
processed.
Sample Analysis
Plasma Glucose
Plasma glucose concentrations were determined during the experiment using the
glucose oxidase method (133) with a Beckman glucose analyzer (Beckman Instruments,
Fullerton, CA). The reaction sequence was as follows:
Glucose Oxidase ß-D-glucose + O2 ---------------------------► gluconic acid and H2O2 (1) Catalase H2O2 + ethanol ---------------------------► acetaldehyde + H2O (2) Molybdate H2O2 + 2H+ +2I- ---------------------------► I2 + H2O (3)
The glucose concentration is proportional to the rate of oxygen consumption. The
plasma glucose concentration in a sample (10 l) is determined by comparison of the
oxygen consumption in the samples with the rate of oxygen consumption by a standard
solution (150 mg/dl). There is no end-product inhibition of the process, as reactions 2 &
3 remove all of the hydrogen peroxide. Thus virtually all of the glucose in the sample is
consumed. Glucose was measured 4 times at each sampling time point for each vessel
and a minimum of 2 times for samples drawn to clamp glucose. The glucose analyzer is
accurate to 450 mg/dl.

34
Plasma [3-3H] glucose
Plasma [3-3H] glucose was measured from the samples deproteinized according to
the method of Somogyi-Nelson (134-136) involving addition of Ba(OH)2 and ZnSO4 as
described under Collection and Processing of Samples. After incubation of 1-3 days, the
samples were centrifuged at 3000 rpm for 20 min. A 5 ml aliquot of the supernatant was
pipetted into a glass scintillation vial and placed in a heated vacuum oven to evaporate all
water (hence removing 3H2O). The residue was reconstituted in 1 ml of deionized water
and 10 ml liquid scintillation fluid (EcoLite (+); Research Product Division, Costa Mesa,
CA), and placed in Beckman LS 9000 Liquid Scintillation Counter (Beckman
Instruments Inc, Irvine, CA) for counting. The scintillation counter was programmed so
that the processor corrected the counts per minute (cpm) for quenching of the
radioactivity in the sample and presented the results as disintegrations per minute (dpm).
To assess the loss of radioactive glucose during the deproteinization process, a
recovery standard was prepared. The [3-3H]glucose infusate was diluted 1:250 (vol:vol)
with saturated benzoic acid containing 1 mg/ml cold glucose. Six 1 ml aliquots of this
diluted 3H infusate were placed into 2 sets of glass scintillation vials labeled as chemical
standard evaporated (CSE) or chemical standard (CS); therefore CSE and CS were
measured in triplicate. The diluted infusate aliquots in the CSE vials were evaporated to
dryness (with plasma samples) in a heated vacuum oven and reconstituted with 1 ml
deionized water. The diluted infusate aliquots in the CS were not evaporated.
Scintillation fluid (10 ml) was added to all standard vials and the standards were counted.
Three additional 1 ml aliquots of diluted 3H infusate were treated identical to the plasma
samples and labeled chemical recovery standard (CRS). Comparison of the CS and CSE

35
provided an evaluation of the loss of 3H counts in the evaporation process. The final
amount of radioactivity per sample was determined by generating a recovery factor (ratio
of radioactivity in the CSE compared to CRS) which accounted for the radioactivity lost
during sample processing.
Plasma Fatty Acids (FFAs)
Plasma fatty acids were determined spectrophotometrically using the Packard Multi
Probe Robotic Liquid Handling system (Perkin Elmer;Shelton, CT) and a kit from Wako
Chemicals (Richmond, VA). In the presence of acyl-Coenzyme A (CoA) synthase, CoA
is acylated by the fatty acids within the plasma sample. The acyl-CoA produced is
oxidized by acyl CoA oxidase, resulting in the production of H2O2. The addition of
peroxidase, in the presence of H2O2, subsequently allows for oxidative condensation of 3-
methyl-N-ethyl-N-(β-hydroxyethyl)-aniline with 4-aminoantipyrine (4-AAP) to form a
purple colored adduct. The purple color adduct was measured at an optical density of
550 nm and is proportional to the plasma FFA concentration in the sample. The FFA
concentrations were calculated using a calibration curve of known amounts of oleic acid.
The assay was run at 37ºC. The specific reactions were as follows:
Acyl-CoA Synthetase FFA + ATP + CoA ---------------------------►Acyl-CoA + AMP + Ppi (4)
Acyl-CoA Oxidase Acyl-CoA + O2 ---------------------------► 2,3-trans-enoyl-CoA + H2O2 (5)
2 H2O2 + 3-methyl-N-ethyl-N-(β-hydroxyethyl)-aniline + 4-AAP Peroxidase ---------------------------► Purple colored adduct (6)

36
Metabolites
Whole blood concentrations of lactate, alanine, β-hydroxybutyrate (BOHB) and
glycerol were determined using the methods developed by Lloyd et al. (137) for the
Technicon Autoanalyzer (Tarrytown, NY) and were modified for the Packard Multi
Probe Robotic Liquid Handling System (Perkin Elmer; Shelton, CT). Enzymes and
coenzymes for metabolic analyses were obtained from Boehringer-Mannheim
Biochemicals (Germany) and Sigma Chemicals. The reduced form (NADH) has a native
fluorescence, which is not exhibited in the oxidized form. Excess amounts of NAD and
enzyme/coenzyme are added to the metabolite samples. NAD is reduced to NADH upon
oxidation of the metabolite. A fluorometer incorporated in the system detects changes in
fluorescence resulting from changes in NADH concentration; therefore, the concentration
of the metabolite present is proportional to the NADH produced.
Metabolites were measured in the PCA-treated blood samples as described above.
A standard curve was constructed for each metabolite using known concentrations of the
analyte prepared in 3% PCA. The Packard Multi Probe Robotic Liquid Handling System
pipettes the sample into one well of the 96-well plate. After an initial absorbance is read,
the Packard Multi Probe Robotic Liquid Handling System pipettes enzyme solution into
each well and shakes the plate to mix sample and enzyme. The reaction proceeds and
after an allotted time, the change in absorbance is determined. All assay reactions are
reversible, with the exception of glycerol kinase. The NAD and enzyme are in excess
compared to the substrate, thus the reactions are essentially taken to completion and the
rate-limiting component is the substrate; therefore, all reactions below are written with a
single direction arrow. All reactions are carried out at 23°C.

37
Lactate
The lactate assay involved the following reaction:
Lactate Dehydrogenase Lactate + NAD+ ---------------------------► Pyruvate + NADH + H+
(7)
The enzyme buffer used was 0.24 M glycine and 0.25 M hydrazine dihydrochloride and 7
mM disodium EDTA, pH 9.6. To 10 ml of enzyme buffer, 4.6 mg NAD and 0.1 U lactate
dehydrogenase were added.
Alanine
The alanine assay involved the reaction:
Alanine Dehydrogenase L-alanine + NAD+ + H2O ---------------------------► Pyruvate + NADH + NH4
+ (8)
The enzyme buffer used was 0.05 M trizma base, 2 mM EDTA and 1 mM hydrazine
hydrate, pH 10. To 10 ml of enzyme buffer, 4.6 mg of NAD and 3.4 Units (U) of alanine
dehydrogenase were added.
ß-hydroxybutyrate
The ß-hydroxybutyrate analysis involved the following reaction:
3-hydroxybutyrate dehydrogenase
ß-hydroxybutyrate + NAD+ ---------------------------► Acetoacteate + NADH + H+ (9)

38
The enzyme buffer was 0.2 M monopotassium phosphate, 3 mM EDTA and 1 mM
hydrazine hydrate, pH 8.5. To 10 ml of enzyme buffer, 12 mg NAD and 2.1 U ß-
hydroxybutyrate dehydrogenase were added.
Glycerol
The glycerol assay involved the following reactions:
Glycerokinase Glycerol + ATP ---------------------------► Glycerol-l-phosphate + ADP (10)
Glycerol-3-phosphate dehydrogenase
L-glycerol-l-phosphate + NAD+ ------------------------------------------------► dihydroxyacetone phosphate + NADH + H+
(11)
The enzyme buffer was 0.09 M glycine, 1 mM hydrazine, and 0.01 M MgC12, pH 9.5. To
10 ml of the enzyme buffer, 15.4 g NAD, 15.4 mg ATP, 0.3 U glycerokinase, and 0.6 U
glycerol-3-phosphate dehydrogenase were added.
Hormones
The plasma levels of insulin, glucagon, and C-peptide were measured using
radioimmunoassay (RIA) techniques (138). In general, a sample containing an unknown
amount of hormone was incubated with an antibody specific for that hormone. A known
amount of radiolabeled hormone was added to the mixture to compete with the antibody
binding sites. A double antibody procedure which caused precipitation of the bound
complex was used to separate unbound hormone from the antibody-hormone complexes.
The radioactivity of the precipitate was measured via a Cobra II Gamma Counter

39
(Packard Instrument Co., Meriden, CT). Binding of the radiolabeled hormone is
inversely proportional to the amount of unlabeled hormone present, and a standard curve
was constructed using known concentrations of unlabelled hormone.
Insulin
Immunoreactive plasma insulin was measured using a double-antibody RIA
procedure (139). A 100 µl aliquot of the plasma sample, 200 l of 125I-labeled insulin,
and 100 ml of guinea pig specific antibody to insulin (both from Linco Research, Inc., St.
Charles, MO.) were mixed and incubated for 18 h at 4°C. The sample was then treated
with 100 µl goat anti-guinea pig IgG (2nd antibody) and 100 µl IgG carrier and incubated
for 30 min at 4°C. One ml of a wash buffer was added and the tubes were centrifuged at
3000 rpm. The samples were decanted and the portion of total radioactivity bound to the
antibody (pellet) was counted in a Cobra II Gamma Counter (Packard Instrument Co,
Meriden, CT).
The log of the amount of hormone in the sample was inversely proportional to the
log of bound 125I-labeled insulin to free 125I-labeled insulin. The insulin concentration in
each sample was determined by comparison to a standard curve constructed using known
amounts of unlabeled hormone. The samples were corrected for non-specific binding.
The sample detection range was 1-150 µU/ml. The specificity of the antibody is 100% to
porcine, canine, and human insulin, 90% with bovine insulin, 38% with human
proinsulin, 47 and 72% with the split proinsulin products Des 31,32 and Des 64,65,
respectively. In general, less than 15% of the basal insulin level is due to non-insulin
cross reactivity (mainly the split proinsulin products Des 31,32 and Des 64,65). There is

40
no cross reactivity to glucagon, pancreatic polypeptide, C-peptide, or somatostatin. The
recovery in the assay was between 90-100% based on spiking the sample with known
amounts of insulin, and the interassay CV was approximately 7-8% for the entire range of
the dose response curve.
Glucagon
Immunoreactive plasma glucagon was also measured using a double antibody
RIA (Linco Research, Inc., St. Charles, MO) (140). The protocol utilized primary and
secondary antibodies specific for glucagon (kit with glucagon antibodies and 125I tracers
from Linco). A 100 µl aliquot of the plasma sample and 100 µl of guinea pig specific
antibody to glucagon were mixed and incubated for 24 hours at 4oC. Next, 100 µl of 125I-
labeled glucagon was added and the solution was incubated for an additional 24 h at 4°C.
Samples were then treated with 100 µl goat anti-guinea pig IgG (2nd antibody) and 100
µl IgG carrier and incubated for 2 hours at 4°C. One ml of a wash buffer was added and
the tubes were centrifuged at 3000 rpm. The samples were decanted and the portion of
total radioactivity bound to the antibody (pellet) was counted in a Cobra II Gamma
Counter.
The log of the amount of hormone in the sample was inversely proportional to the
log of bound 125I-labeled glucagon to free 125I-labeled glucagon. Glucagon concentration
in each sample was determined by comparison to a standard curve constructed using
known amounts of unlabeled hormone. The samples were corrected for non-specific
binding, and the sample detection range was 20-400 pg/ml. The antibody is 100%
specific to glucagon with only slight (0.01 %) cross reactivity to oxyntomodulin, and no

41
cross reactivity with human insulin, human proinsulin, human C-peptide, glucagon-like
petide-1, somatostatin, or pancreatic polypeptide. A cross-reacting protein in plasma
reads in this assay and results in a glucagon stripped sample reading 15-20 pg/ml. This
represents a stable, constant background in all samples. The recovery for the assay was
between 80-109% based on spiking the sample with known amounts of glucagon, and the
interassay CV was approximately 6-10% for the entire dose response curve.
Cortisol
Immunoreactive plasma cortisol was measured with a single antibody technique
(141) using a gamma coat RIA from Diagnostics Products Corporation (Los Angeles,
CA). Twenty-five µl aliquot of plasma and 1 ml of 125I-labeled cortisol were pipetted
into a cortisol specific antibody-coated tube with an antibody immobilized on the lower
inner wall of the tube. They were incubated for 2 hours in a 31ºC water bath. Later, the
tubes were decanted and rinsed with dionized water. The tubes were allowed to dry, and
then counted in a Cobra II Gamma Counter for 4 minutes.
The log of the amount of hormone in the sample was inversely proportional to the
log of of bound 125I-labeled cortisol to free 125I-labeled cortisol. The cortisol
concentration in each sample was determined by comparison to a standard curve using
known amounts of unlabeled hormone. The sample detection range was 0.5-50 µg/dl.
The antibody is 100% specific for cortisol with only slight cross-reactivity of 6% with
11-deoxycortisol and 1% with 17-hydroxyprogesterone. In contrast, it has no cross-
reactivity with corticosterone, aldosterone, progesterone, deoxycorticosterone and

42
tetrahydrocortisone. The recovery for the assay was > 90% and the interassay CV was
approximately 8-10% for the entire range of the dose response curve.
Catecholamines
A high performance liquid chromatography (HPLC) method was used to determine
plasma epinephrine and norepinephrine levels as previously described by Goldstein et al.
(142). 400 µl of the plasma samples were partially purified by absorption to 10 mg of
acid-washed alumina (Bioanalytical Systems, West Lafayette, IN) in 600 µl of
Tris/EDTA (ph 8.6) and 50 µl of an internal standard, dihydroxybenzylamine (DHBA,
500pg/ml, Sigma Chemical Co.). Samples were then shaken for 15 minutes, centrifuged
for 4 minutes and aspirated. The alumina pellet was rinsed with 2ml of water, and then
the solution was vortexed, centrifuged and aspirated. This process was repeated 3 times.
Next, the catecholamines were eluted with 200 µl 0.1 M perchloric acid (PCA) according
to Anton and Sayre (143).
Samples were next injected onto a HR-80, reverse phase, 3µm octadecylsilane
column. The mobile phase was composed of 43 ml of methanol, 440 mg of sodium octyl
sulfate, 37 mg of sodium EDTA (ph 3.4) and 14.2 g of disodium phosphate. The system
utilized a Coulochem II Detector, Conditioning Cell (Model 5021) and Analytical Cell
(Model 5011; all obtained from ESA, Bedford, MA). Epinephrine and norepinephrine
concentrations were calculated using a linear calibration curve consisting of 5 standards
(ranging from 50-1000 pg/ml). The standards were prepared from epinephrine bitartrate
and (-)-arterenol bitartrate (norepinephrine) salts (Sigma Chemical Co.). In addition, a
known amount of epinephrine and norepinephrine were added to the sample taken at the

43
start and at the end of each experiment to evaluate recovery and to ensure precise
identification of the peaks.
In order to identify the peaks, data reduction was performed using ESA 500
Chromatograph and data station software. The ratio of the peak height of the internal
standard to the catecholamine was calculated and the concentration of catecholamine was
determined by comparison with the standard curve. The limit of detection of the assay
for epinephrine was 20 pg/ml and for norepinephrine was 5 pg/ml. Recovery of the
hormones was between 80-100%. The interassay CV for epinephrine was 3-11% and 4-
6% for norepinephrine.
Pancreatic Polypeptide
Immunoreactive plasma pancreatic polypeptide was measured using a double antibody
RIA (Linco) (140). The protocol was adapted by using primary and secondary antibodies
specific for pancreatic polypeptide (kit with pancreatic polypeptide antibodies and 125I
tracers from Linco) A 100µl aliquot of the sample was incubated for 72 h at 4ºC with
100µl of rabbit antiserum raised against bovine pancreatic polypeptide. Subsequently,
100µl 125I-labeled pancreatic polypeptide was added and the solution was incubated for
24 h at 4ºC. After 24 h, the sample was incubated with 100µl goat anti-guinea pig IgG
(2nd antibody) and 100µl IgG carrier for 6 h at 4ºC. One ml of wash buffer was added
and the tubes were centrifuged at 3000 rpm. The samples were decanted and the portion
of total radioactivity bound to the antibody (pellet) was counted in a Cobra II Gamma
Counter.

44
The log of the amount of hormone in the sample was inversely proportional to the
log of of bound 125I-labeled pancreatic polypeptide to free 125I-labeled pancreatic
polypeptide. The pancreatic polypeptide concentration in each sample was determined
by comparison to a standard curve using known amounts of unlabeled hormone. Samples
were corrected for non-specific binding, and the sample detection range was 20-1200
pg/ml. The antibody is 100% specific for human and dog pancreatic polypeptide and
there is no detectable cross-reactivity with insulin, glucagon and somatostatin. The
recovery of the assay was between 80-110%, and the interassay CV was approximately
10-15% for the entire range of the dose response curve.
Blood Flow
Blood flow in the hepatic artery and hepatic portal vein were determined using
ultrasonic flow probes implanted during surgery (as described in Surgical Procedures).
Total hepatic blood flow which is defined as the sum of blood flow in the hepatic artery
and the hepatic portal vein was also assessed using the indocyanine green (ICG) dye
method described by Leevy et al. (144). The results presented in this document were
calculated using ultrasonic determined flow. This method allows for the direct
measurement of blood flow in the hepatic artery and hepatic portal vein whereas the ICG
dye method requires an assumption of the percent contribution of each vessel to total
hepatic blood flow. ICG-determined flow was used as a backup measurement in the case
of ultrasonic flow probe failure.
Ultrasonic flow measurements represented instantaneous variations in velocity
and, therefore, provided blood flow in individual vessels of interest. Each probe

45
determined the mean transit time of an ultrasonic signal passed back and forth between
two transducers within a probe which were located upstream and downstream of the
direction of blood flow in the vessel. The transducers are made of piezoelectric material
which is capable of both receiving and transmitting the ultrasonic signal. The
downstream transducer first emits an ultrasonic pulse into the blood vessel that is
received upstream by a second transducer. After the upstream transducer receives the
ultrasonic signal, it re-emits the ultrasonic pulse signal back to the downstream
transducer. The transit time of each ultrasonic beam, as measured by the upstream and
downstream transducers (ΔTup and ΔTdown, respectively), is defined by the following
relationships:
ΔTup = D / (vo - vx ) (12)
ΔTdown = D / (vo + vx ) (13)
where D is the distance traveled by the ultrasonic beam within the acoustic window of the
probe, vo is the phase velocity, or the speed of sound, in blood, and vx is the component
of fluid velocity that is parallel or antiparallel to the phase velocity. The parallel
component augments the phase velocity when the signal is traveling in the same direction
of blood flow, while the antiparallel component is subtracted from phase velocity if the
ultrasonic signal moves against the flow of blood in the vessel. Combining the two
expressions for transit time yields the following equation:
ΔTup - ΔTdown = [D / (vo - vx )] – [D / (vo + vx )] (14)

46
Since the transit times measured by both transducers, the distance traveled by the beam,
and the speed of sound in blood are all known quantities; therefore, this equation can be
used to calculate vx. Once vx is obtained, the transit velocity (V) of blood traveling
through the vessel can be determined according to the following equation:
V cos θ = vx (15)
where θ is the angle between the centerline of the vessel and the ultrasonic beam axis.
Finally, blood flow is the product of the transit velocity and the cross-sectional area of the
vessel. The cross-sectional area of the vessel is pre-determined by the size of the acoustic
window according the probe model. Since transit time is sampled at all points across the
diameter of the vessel, volume flow is independent of the flow velocity profile.
If a flow probe failed during the experiment, the missing values were estimated by
subtracting the values from the functional flow probe from the ICG values.
The ICG method is based on the Fick principle, according to which the net
balance of a substrate across an organ is equal to the concentration difference of the
substrate across the organ multiplied by the blood flow through the organ. The equation
can be rearranged to calculate hepatic blood flow by dividing hepatic ICG balance by the
arteriovenous difference of ICG across the liver. Because the liver is assumed to be the
only site of ICG clearance, hepatic ICG uptake is equal to ICG infusion rate under steady
state conditions. The extraction of ICG across the liver remains constant for brief
infusions. However, if ICG is infused for a longer time (> 4 h), the dye level in plasma
gradually increases, resulting in a 5-10 % overestimation of hepatic blood flow (145).

47
The arterial and the corresponding hepatic vein plasma samples were centrifuged
at 3000 rpm for 30 min without the brake to pellet the residue. The absorbance was then
measured on a Spectronic spectrophotometer at 810 nm. The procedure was then
repeated, and the values obtained for each sample were averaged. A standard curve was
constructed by adding successive 5 µl aliquots of diluted dye (1:10 dilution) to 1 ml of
plasma drawn from the animal before the dye infusion was started. The standard curve
mean difference per incremental changes was then used to calculate hepatic plasma flow
(HPF) as follows:
HPF = [IR x 10 x SCMD] / [dog weight in kg x (0.005) x (A-H)] (16)
where IR is ICG infusion rate (ml/min), SCMD is the standard curve mean difference per
5 µl increments, and A-H is the difference in absorbance between the arterial and the
hepatic venous sample. The value of 10 was used to correct for the dilution of the ICG
used in the standard curve, and 0.005 was the volume in ml used as increments in the
standard curve. Hepatic blood flow (HBF) was derived from HPF:
HBF=HPF/(1-hematocrit) (17)
Hematocrit was measured at every time point of each in which samples were taken from
the hepatic artery and portal and hepatic veins. This technique only determines total
blood flow; therefore, an assumption was made regarding the contribution of blood flow
in the vessels supplying the liver. The normal distribution of flow was assumed to be
28% artery and 72% hepatic portal vein at baseline.

48
Tissue Analysis
Real time PCR and Western blot analysis
Within 2 min of the final sampling time point, each animal was anesthetized with
pentobarbital (390mg/ml Fatal-Plus; vortech Pharmaceutical Inc., Dearborn,MI) at
1ml/kg. The animal was then removed from the Pavlov harness while the tracers and
hormones continued to infuse. A midline laparotomy incision was made, the liver
exposed and clamps cooled in liquid nitrogen were used to simultaneously freeze sections
of the hepatic lobes 2, 3 and 7 in situ. The frozen liver samples (~5g liver lobes) were
stored at -70°C until subsequent analysis of test proteins (via Western blotting) and
mRNA levels (via Real Time PCR).
Real Time PCR analysis of mRNA levels was performed using the BioRad iQ
iCycler Detection System, iQ Supermix, and canine liver cDNA preparations as template.
Test genes were normalized to the housekeeping gene hypoxanthine phosphoribosyl
transferase 1 (HPRT1), using the Livak method (146). Total RNA was extracted by
homogenizing 50 mg of frozen canine liver in Tri-reagent (Sigma, St. Louis, MO)
following the manufacturer’s instructions and RNA was further purified using the Qiagen
RNEasy kit (Qiagen, Valencia, CA). First strand cDNA was synthesized from total RNA
using the High Capacity reverse transcription kit (Applied Biosystems, Foster City, CA)
as per manufacturer’s directions. Primers were designed using the Primer3 program and
possible primer secondary structure was analyzed using the Mfold program, according to
parameters outlined in the BioRad iCycler manual. Primer pairs were as follows: PEPCK
5'-AGCTTTCAATGCCCGATTTCCAGG and 5'-
TCAGCTCGATGCCGATCTTTGACA; G6Pase 5'-TGAAACTTTCAGCCACATCCG

49
and 5'-GCAGGTAAAATCCAAGTGCGAA; HPRT1 5'-
AGCTTGCTGGTGAAAAGGAC and 5'-TTATAGTCAAGGGCATATCC. Primer
efficiencies were validated to be between 91 and 95% for each primer pair using a
dilution series of cDNA, and primer specificity was confirmed by both melt curve
analysis and 1% agarose gel electrophoresis (each of which revealed one product), and
optimal annealing temperature was determined to be 55oC for each primer set. Samples
were run in duplicate, and a negative control (no cDNA template) was included for every
primer pair.
For Western blotting, sample preparation, electrophoretic separation, blotting, and
immunodetection of proteins was performed essentially as described previously
(Ramnanan and Storey, 2006). Antibodies specific for total and phosphorylated Akt,
GSK3β, FOXO1, and CREB proteins were purchased from Cell Signaling (Danvers,
MA), while the PGC1α antibody was purchased from Santa Cruz Biotechnology (Santa
Cruz, CA). The PEPCK antibody was a generous gift from Dr. D.K. Granner. Briefly,
frozen canine liver was homogenized 1:10 w:v in cold (4oC) buffer that was designed to
inhibit endogenous protein phosphatase, protein kinase and protease activities: 50 mM
Tris-HCl pH 7.0, 100 mM sucrose, 10% v:v glycerol, 2 mM EDTA, 2 mM EGTA, and 25
mM NaF; 10 µL/mL homogenization buffer of Sigma Phosphatase Inhibitor Cocktail 1,
Phosphatase Inhibitor Cocktail 2, and Sigma Protease Inhibitor Cocktail were added at
the time of homogenization. Homogenates were centrifuged at 10,000 x g for 20 min,
supernatants were removed and soluble protein concentration was determined using the
Biorad protein assay. Aliquots of supernatant were mixed 1:1 v:v with freshly prepared
2X SDS-PAGE loading buffer (100 mM Tris-HCl, pH. 6.8, 4% w:v SDS, 20% v:v

50
glycerol, 0.2% w:v bromophenol blue, 10% v:v 2-mercaptoethanol) and boiled for 5 min.
Samples were immediately frozen with liquid nitrogen and stored at –20oC. Aliquots
containing 20 µg soluble protein were subjected to SDS-PAGE (12% resolving gel) and
proteins were subsequently wet-transferred to nitrocellulose membranes using the
Invitrogen XCell Blot II apparatus. Blocking conditions and antibody incubation
conditions were optimized for specific proteins. Generally, membranes were blocked
with 5% (wt/v) bovine serum albumin in Tris-buffered saline containing Tween-20
(TBST: 10 mM Tris-base, pH 7.0, 150 mM NaCl, 0.5% v:v Tween 20) for 1 h at room
temperature and then probed with primary antibodies diluted 1:1000 v:v in TBST for 2 h.
After 3 x 5 min washes with TBST, membranes were then incubated with the appropriate
HRP-conjugated secondary antibody (Promega; Madison, WI) diluted 1:2000 v:v in
TBST for 1 h at room temperature, followed by 3 x 5 min washes in TBST. Proteins were
visualized using ECL Plus Western detection reagents (GE Healthcare, Piscataway, NJ)
following manufacturer’s protocols and the ECL signal was detected after exposure to
BioMax Light X-ray film (Kodak, Chalon-sur-Saone, France).
Test protein bands were quantified using ImageJ software
(http://rsb.info.nih.gov/ij/). After immunodetection, blots were normalized for loading as
previously described (147). Bio-Rad Kaleidoscope pre-stained markers were run in one
lane of each gel to verify the subunit molecular mass of target proteins. Membranes were
stripped using Restore reagent from Pierce (Rockford, IL) and reprobed according to
manufacturer’s directions.

51
Calculations
Net Hepatic Substrate Balance and Fractional Extraction
The net hepatic balances and net hepatic fractional extractions of blood glucose,
lactate, alanine, glycerol, BOHB and plasma FFA were calculated using both ultrasonic-
determined and ICG-determined flow. As previously mentioned, the data shown are
those calculated using ultrasonic-determined flow because this flow does not require an
assumption about the distribution of arterial versus portal flow. ICG-determined flows
were used to calculate the data only to verify that conclusions drawn using the flow probe
data were independent of the method used to determine flow.
The net balance of a substrate across an organ was determined using the
arteriovenous (A-V) difference technique. This employed the Fick principle as described
for the ICG-determination of blood flow (as described in Sample Analysis under Blood
Flow)
The net balance of a substrate (NSB) was calculated as:
NHSB = Loadout - Loadin (19)
The Loadout was calculated according to the equation:
Loadout = [S]HV x HBF (20)

52
where [S]HV is the substrate concentration in the hepatic vein blood, and HBF is the total
hepatic blood flow.
The Loadin was calculated according to the equation:
Loadin = ([S]A x HABF) + ([S]PV x PVBF) (21)
where [S]A and [S]PV are the arterial and portal venous blood substrate concentrations,
respectively, and HABD, PVBF are the hepatic artery and the portal vein blood flows,
respectively. For all glucose balance calculations, plasma glucose concentrations were
converted to whole blood values using a previously determined correction factor (148)
which assumes blood glucose to be 73 % of the plasma glucose values. Blood flows
were used for all substrate balance calculations with the exception of FFA balances. FFa
balances were calculated by using plasma flow and plasma substrate concentrations.
Plasma flow was determined by multiplying blood flow by (1-hematocrit). A positive
value for NHSB indicates net substrate production by the liver, whereas a negative value
represents net hepatic substrate uptake. When the data were plotted as net hepatic uptake,
positive values were used.
Net fractional extraction (FE) was also calculated using ultrasonic-determined
blood flow according to the following equation:
FE = NHSU/Loadin (22)

53
where NHSU is net hepatic substrate uptake.
The arterio-venous difference technique has some limitations that must be
taken into account such as: 1) variability of vascular anatomy and heterogeneity of tissue
structure and function, 2) imprecision in measurement of local blood flow, 3)
measurement of net rather than absolute flux across the organ, and 4) access to the portal
vein is required, making this procedure only useful in animals. Furthermore, transit time
through the organ must be taken into account. Glucose transit time through the liver it is
very short (<1 min) making the measurement robust nevertheless the arterio-venous
difference represents net flux across an organ, it is most valid during steady-state
conditions.
Glucose Turnover
Glucose turnover is the rate at which old glucose is replaced with new glucose.
Glucose production (Ra) and glucose utilization (Rd) were determined using an isotope
dilution method described by Wall (149), as simplified by DeBodo (150) and using a
two-compartmental model (151) with canine parameters (152). The glucose pool was
initially primed with an injection of [3-3H]glucose followed by a constant infusion of the
tracer. By the beginning of the control period, the tracer ([3-3H]glucose) and tracee (cold
glucose) were in equilibrium so that the specific activity of glucose (SA = dpm
glucose/mg glucose) was in a steady state. Ra and Rd were calculated according to the
following equations:
Ra = [I - N (dSA/dt)]/SA, and (23)

54
Rd = Ra – (dN/dt) (24)
where I is infusion rate of tracer (dpm/min), N is the size of the glucose pool (mg) and t is
time (min) (153). In a steady state, when dSA/dt = 0, the Ra equation is simplified to:
Ra = I/SA (25)
This method utilizes a one-compartment model of glucose kinetics as described
by Steele (154). Assumptions of the model are that one compartment of glucose consists
of both rapidly mixing and slowly mixing glucose pools; therefore, when a rapid change
in the cold glucose concentration is induced in the system, the consequent changes in
glucose specific activity would be unevenly distributed throughout the entire glucose
compartment. To compensate for this problem, the pool size is calculated as:
N = pVC (26)
where p is the pool fraction, V is the volume of distribution of glucose (ml) and C is
concentration of cold glucose (mg/dl). The pool fraction (the rapidly mixing component
of the glucose compartment) was estimated to be 0.65, or 65 % of the total system (155),
while V was assumed to be the extracellular volume, which is approximately 22% of the
dog weight (156).
The major limitation of the one-compartment model is that a rapid change in SA
invalidates the method, so that a fall in SA, which occurs either by endogenous glucose

55
production or exogenous glucose infusion in the presence of a constant [3-3H] glucose
infusion, the change in SA would cause an error in the estimation of Ra (underestimation
if SA drops, overestimation if SA increases) (157). In order to overcome this problem, in
the present studies, the data were calculated using a two-compartment model (151). This
model describes the glucose system more accurately under non-steady-state conditions.
Ra was calculated as the sum of three terms: a steady-state term, a term for the first
compartment, and the term for the second compartment. The principle equations are as
follows, where the expression of Ra, calculated at the equally spaced time instants t0,
t1,…, tk, tk+1, is determined from the following formulas:
Ra(tk) = (R*inf)(tk)/SA(tk) – V1[C(tk)dSA(tk)/dt] / SA(tk) – V2k22[SA(tk)G(tk) –
G*(tk)]/SA(tk) (27)
G(tk+1) = b1G(tk) + b2C(tk) + b3C(tk+l) (28)
G*(tk+l) = blG*(tk) + b2C*(tk) + b3C*(tk+l) (29)
V2= V1k12k21/k222 (30)
where tk and tk+l are time parameters, respectively; Ra(tk) and R*inf(tk) are the rate of
appearance calculated with a two-compartment model (mg/kg/min) and tracer infusion
rate (dpm/kg/min), respectively; SA(tk) and dSA(tk) are specific activity (dpm/mg) and
derivative of specific activity (dpm/mg/min), respectively. V1 and V2 (ml/kg) are the
volumes of the first and second compartments, respectively; C*(tk) and C(tk) are tracer
and tracee concentrations, respectively; k12, k21, and k22 are constant rate parameters of
the first and second compartments, respectively; G(tk) and G*(tk) are variables calculated

56
recursively from tracee and tracer concentrations, respectively; bl, b2, and b3 are
coefficients of recursive equations for calculating G(tk) and G*(tk). Canine parameters
used for Vl, V2, and k22 in the present studies were those determined by Dobbins et al.
(152). It has been reported (152) that under non-steady state conditions where specific
activity changes dramatically, glucose appearance determined using the two-
compartment model is more accurate than the Steele equation (one-compartment model.)
When glucose was infused, endogenous glucose production (endo Ra) was
determined by subtracting the glucose infusion rate (GIR), from total glucose production
(Ra).
Of note, there are two major assumptions that are made when using the particular
isotope dilution method to determine glucose kinetics. First, the labeled and unlabeled
glucose molecules are assumed to be metabolized in the same manner. Secondly, the
label is assumed to be irreversibly lost (158).
It should also be noted, however, that since both the liver and the kidneys produce
glucose, whole body tracer-determined glucose production is slightly higher than the rate
of hepatic glucose production. Although net kidney glucose balance in the postabsorptive
state is near zero, the kidneys have been estimated to contribute 5-15% to whole body
glucose production. Metanalysis suggests that the kidneys are only a minor contributor to
total glucose production (159).
Hepatic Gluconeogenesis and Glycogenolysis
Gluconeogenesis is the synthesis and release of glucose formed from non-
carbohydrate precursors. Glucose-6-phosphate produced from flux through the

57
gluconeogenic pathway is not only released as glucose; it can also be stored as glycogen,
oxidized or released as lactate. Therefore, there is a distinction between gluconeogenic
flux to glucose-6-phosphate, which is the conversion of precursors to glucose-6-
phosphate, and gluconeogenesis per se, which is the release of glucose derived from
gluconeogenic flux into the blood. In the present studies, we estimated hepatic
gluconeogenic (GNG) flux to glucose-6-phosphate and net hepatic glycogenolytic
(NHGLY) flux.
The net hepatic uptakes of the gluconeogenic precursors alanine, lactate and
glycerol were measured using the arterio-venous difference method (as described in
Calculations under Net Hepatic Substrate Balance and Fractional Extraction). This
method assumes that there is 100% conversion of gluconeogenic precursors taken up by
the liver into G-6-P and that intrahepatic GNG precursors do not contribute significantly
to GNG flux. The net hepatic balance of pyruvate was assumed to be 10% of the net
hepatic lactate balance (160). In these studies certain gluconeogenic precursors were not
measured (e.g. pyruvate, glycine, threonine, serine, glutamine, glutamate). To the extent
that they contributed to gluconeogenic flux, it will be underestimated. To correct for this
error and assuming, based on previous studies (161) that net hepatic alanine uptake
represents a reasonable approximation of the uptake of the unmeasured gluconeogenic
precursors, net hepatic alanine uptake was multiplied by 2. Hepatic gluconeogenic flux
to glucose-6-phosphate was estimated by summing gluconeogenic precursor uptake and
dividing by two to account for the incorporation of the three-carbon precursors into the
six-carbon glucose molecule (to convert the data into glucose equivalents). When net

58
hepatic output of any precursor occurred, rather than uptake, the precursor was
considered to be a product of the liver, and thus uptake was set to zero.
Net hepatic gluconeogenic flux was determined by subtracting the sum of net
hepatic output rates (when such occurred) of gluconeogenic precursors (in glucose
equivalents) and hepatic glucose oxidation from the gluconeogenic flux to G-6-P. A
positive number represents net gluconeogenic flux to G-6-P whereas a negative number
indicates net glycolytic flux from G-6-P or net flux to pyruvate. In the present studies,
glucose oxidation was assumed to be 0.2 mg/kg/min in all groups (162). This parameter
was not directly measured because it is difficult to differentiate between the small signal
and the high inherent noise in the measurement. On the other hand, our laboratory has
reported that glucose oxidation after an overnight fast ranges from 0.1 to 0.2 mg/kg/min.
Although by using this value may slightly overestimate or underestimate the absolute rate
of glucose oxidation; it is unlikely to differ by more than 0.1 mg/kg/min from the true
value. In addition, previous studies have shown that in the presence
euglycemic/hyperinsulinemic states hepatic glucose oxidation did not change
significantly (162). Glucagon has been reported to inhibit pyruvate dehydrogenase and
as a result pyruvate oxidation (163; 164) but the basal oxidation rate is so low that the
noise of the measurement would be greater than the magnitude of the potential fall.
Net hepatic glycogenolytic flux was estimated by subtracting net hepatic
gluconeogenic flux from net hepatic glucose balance. A positive value indicates net
glycogen breakdown whereas a negative value represents net glycogen synthesis.
It is necessary to consider the limitations of the arterio-venous difference
technique to estimate the net hepatic gluconeogenic and glycogenolytic fluxes. There is

59
little or no hepatic production of gluconeogenic amino acids or glycerol whereas that is
not the case for lactate. Our estimate of the rate of gluconeogenic flux to G-6-P will be
quantitatively accurate only if we assume that lactate flux is unidirectional at a given
moment (i.e. either in or out of the liver). Jungermann and Katz (165; 166) have reported
that there is a spatial separation of metabolic pathways, such that gluconeogenic
periportal hepatocytes synthesize glucose and glycogen primarily from lactate and other
non-carbohydrate precursors whereas glycolytic perivenous hepatocytes consume glucose
which is mainly oxidized or released as lactate. Therefore, in a net sense it is possible
that hepatic gluconeogenic and glycolytic flux occur simultaneously, with lactate output
and uptake occurring in different cells. To the extent that flux occurs in both directions
simultaneously the net hepatic balance method will result in an underestimation of the
absolute rate of gluconeogenic flux to G-6-P. Of note, net hepatic gluconeogenic and net
hepatic glycogenolytic fluxes can be calculated accurately without concern for the
assumptions related to whether or not simultaneous gluconeogenic and glycolytic
substrate flux occur. Ideally the gluconeogenic flux rate would be calculated using
unidirectional hepatic uptake and output rates for each substrate, but this would be
difficult, as it would require the simultaneous use of multiple stable isotopes which could
themselves induce a mild perturbation of the metabolic state.
Statistical Analysis
Data are expressed as means ± standard error (SE). The data were analyzed for
differences between saline-euglycemic vs. glucagon-euglycemic and saline-
hypoglycemic vs. glucagon-hypoglycemic. Statistical comparisons were carried out using

60
two-way repeated measures ANOVA and two-way ANOVA with post hoc data analysis
determined by Student-Newman-Kuels Method (Sigma Stat, SPSS Inc.). Significance
was established when P < 0.05.

61
CHAPTER III
THE SENSITIVITY OF THE LIVER TO GLUCAGON IS INCREASED DURING INSULIN-INDUCED HYPOGLYCEMIA
Aim
In the presence of insulin-induced hypoglycemia glucagon is the most important
stimulator of glucose production. In contrast under euglycemic conditions insulin is a
potent inhibitor of glucagon’s effect on the liver. The results of previous studies suggest
that the liver is more sensitive to glucagon during hypoglycemia. A comparison of the
effects of a controlled rise in glucagon on hepatic glucose production in the presence of
euglycemia or hypoglycemia has never been made. For this reason, the aim of the
present study was to examine the ability of a physiologic increase in glucagon to
overcome the inhibitory effect of insulin on glucose production under euglycemic or
hypoglycemic conditions.
Results
Hormone Concentrations
Arterial plasma insulin rose from baseline to between 230 and 300 U/ml in
response to insulin infusion (Figure 3.1A). Arterial plasma glucagon levels were similar
in all groups during the control period (39±1 pg/ml) and they fell during the first
experimental period to between 25±2 and 30±2 pg/ml. They remained low in
experimental period two in the SE and SH groups (26±5 and 23±6 pg/ml respectively)
but rose to ~ 100 pg/ml in response to intraportal glucagon infusion in the GE and GH
groups (Figure 3.1B). Arterial plasma cortisol was ~3.5±0.3 µg/dl in all groups

62
respectively during the control period and experimental period one (Figure 3.2A). It
remained unchanged in the SE and GE groups (3.7±0.8 and 4.8±2.0 µg/dl respectively)
during experimental period two. On the other hand, in response to insulin-induced
hypoglycemia it increased markedly (15±1 and 17±3 µg/dl, in SH and GH respectively;
P<0.05 vs. euglycemic groups). Arterial plasma epinephrine was basal (~130±2 pg/ml)
during the control period and experimental period one in all groups (Figure 3.2B).
During experimental period two, it was ~137±62 and 126±53 pg/ml in the SE and GE
groups respectively, but rose to 1917±376 and 1755±326 pg/ml, in the SH and GH
groups respectively (P<0.05 vs. euglycemic groups). Arterial plasma norepinephrine
levels remained basal and similar between the groups (161±15 pg/ml) during the control
period and experimental period one (Figure 3.2C). During experimental period two it
remained unchanged in the SE and GE groups (209±33 and 162±30 pg/ml), but increased
to 403±83 and 350±86 pg/ml (P<0.05) in the SH and GH groups. The arterial plasma
polypeptide level averaged ~ 181±37 pg/ml in all groups during the control period. It fell
during experimental period one to 101±19, 82±18, 149±44 and 173±59 pg/ml in the SE,
GE, SH and GH, respectively, in response to the intraportal somatostatin infusion and
remained low in period two in all groups (98±21, 129±65, 162±40 and 174±52 pg/ml in
the SE, GE, SH and GH groups, respectively) (Table 3.1)
Blood glucose levels and hepatic glucose balance
Euglycemia was maintained during experimental period one in each group and
during experimental period two in the SE and GE groups (Figure 3.3A). In the latter
groups glucose infusion rates were 14.7±2.6 and 13.1±2.4 mg/kg/min, respectively

63
(Figure 3.3B). On the other hand, hypoglycemia was allowed to occur in the SH and GH
groups (49±1 mg/dl). The glucose infusion rates required to maintain hypoglycemia of
50 mg/dl were 5.9±1.4 and 4.6±1.7 mg/kg/min respectively. NHGO was ~1.6±0.1
mg/kg/min in all groups in the control period. In response to intraportal insulin infusion
in the presence of euglycemia the liver switched to slight net hepatic glucose uptake in all
groups (~ 0.4±1.2 mg/kg/min; Figure 3.4A). During the second experimental period,
NHGU increased slightly over time (to ~1.5±0.4 mg/kg/min) in the SE group while in the
GE group the liver temporarily switched to net output (~0.4±0.6 mg/kg/min) after which
it switched back to net uptake (~0.9±0.7 mg/kg/min). In the SH and GH groups the liver
quickly switched to net glucose output and remained in a production mode until the end
of the study (1.3±0.2 and 3.1±0.5 mg/kg/min, respectively; P<0.05). The increase in net
hepatic glucose balance (60 to 180 minutes) caused by glucagon was significantly greater
in the presence of hypoglycemia (239 mg/kg/120 min; difference in NHGB between SH-
GH) than in the presence of euglycemia (106 mg/kg/120 min; difference in NHGB
between SE-GE) (Figure 3.4B). Changes in tracer-determined endogenous glucose
production (Ra) paralleled the changes in NHGO (Table 3.2)
Tracer determined glucose utilization (Rd) was between 2.2 and 2.8 mg/kg/min
during the control period. Intraportal infusion of insulin increased Rd in all groups (to
11.9±1.8, 10.6±1.3, 11.6±1.7 and 9.2±1.7 mg/kg/min; Table 3.2) during experimental
period one. Rd continued to increase over time in the SE and GE groups (reaching
19.6±2.2 and 18.6±1.3 mg/kg/min, respectively by the end of the study) but it decreased
in the SH and GH groups (6.2±0.9 and 5.3±0.7 mg/kg/min, respectively; P<0.05).
Glucose clearance increased in all groups during experimental period one (Table 3.2) and

64
it rose to a greater extent during experimental period two in the euglycemic groups than
in the hypoglycemic groups.
Metabolites
Arterial blood alanine had decreased in response to the rise in insulin in all groups
by the end of the study. There was no significant change in net hepatic alanine balance
over time and no difference between groups (Table 3.3). On the other hand, the
fractional extraction of alanine by the liver doubled in all groups although this change
was not significant in any individual group. Arterial blood lactate levels were basal
during control period and rose minimally in experimental period one in all groups (Table
3.3). During experimental period two they remained unchanged in both euglycemic
groups but increased markedly in the hypoglycemic groups (Table 3.3). The liver was
producing lactate in all groups during period one. By the end of the study all groups had
switched to net hepatic lactate uptake but the hypoglycemic groups were taking up almost
6 times as much lactate as the euglycemic groups. The presence of glucagon had no
effect in lactate metabolism in the euglycemic or hypoglycemic settings.
Arterial plasma glycerol levels fell in all groups when insulin rose (Table 3.4).
They remained suppressed during experimental period two in both euglycemic groups but
increased markedly in response to hypoglycemia. Net hepatic glycerol uptake followed
the changes in glycerol levels and was more than 10 fold greater in the presence of
hypoglycemia than in the presence of euglycemia. The addition of glucagon in the
presence of euglycemia or hypoglycemia had no effect in glycerol metabolism.

65
Arterial Plasma Free Fatty Acids and BOHB
Arterial plasma free fatty acid levels were basal in all groups during the control
period and fell markedly in response to insulin in experimental period one (Table 3.5).
They fell to less than 50 µmol/L during experimental period two in both euglycemic
groups whereas they increased markedly in the SH and GH groups (to 547±76 and
376±115 µmol/L, respectively). Net hepatic free fatty acid uptake paralleled the changes
in plasma free fatty acid levels (Table 3.5). Arterial blood BOHB levels and net hepatic
BOHB output tended to fall in response to elevated insulin. The decline was slightly less
in the presence of hypoglycemia. The presence of glucagon had no discernable effect in
FFA or BOHB metabolism (Table 3.4).
Net hepatic glycogenolytic and gluconeogenic flux
Net hepatic gluconeogenic(NHGNG) flux was ~ 0.1±0.1 mg/kg/min during the
control period (Figure 3.5A) and decreased to ~ -0.5±0.1 mg/kg/min in all groups during
experimental period one. It remained close to zero in the SE and GE groups during
experimental period two but increased significantly (~1.8 mg/kg/min) in the SH and GH
groups in response to hypoglycemia. Since the increase was virtually identical (1.7±0.4
and 1.8±0.4 mg/kg/min, respectively (P<0.05). it is clear that the drive for
gluconeogenesis was not attributable to glucagon. Net hepatic glycogenolytic (NHGLY)
flux was ~1.5±0.1 mg/kg/min in all groups at the end of the control period (Figure 3.5B)
and it decreased during experimental period one (to -0.5±0.6, -0.5±0.2, 0.0±0.4 and -
0.6±0.3 mg/kg/min in the SE, SH,GE and GH groups, respectively). During
experimental period two the SE group continued to exhibit net glycogen synthesis (-

66
1.3±0.7 mg/kg/min). Addition of glucagon (GE) caused a small glycogenolytic response
followed by a return to net glycogen synthesis. In the SH group net glycogen synthesis
remained near zero during experimental period two. On the other hand, in the GH group
NHGLY flux increased to ~2.9±1 mg/kg/min at 75 minutes and remained elevated
throughout the study. The increase in NHGLY flux between 60 to 180 minutes caused
by glucagon was much greater in the presence of hypoglycemia (279 mg/kg/120 min)
than in the presence of euglycemia (106 mg/kg/120 min) (P<0.05). Hypoglycemia thus
caused a 2.7 fold increase in the glycogenolytic response to glucagon (Figure 3.5C).
Molecular changes
Molecular indices from the last two dogs studied in each group were analyzed and
compared to control values in liver taken from 18 h, fasted dogs in which basal levels of
insulin, glucagon and glucose were maintained. These animals were part of another
study and were included for references purposes. Levels of phosphorylated (Ser473) Akt
were assayed as an index of activation of the insulin signaling pathway, as were the levels
of phosphorylated (Ser256) FOXO1 and (Ser9) GSK3-β, two downstream targets of Akt
that are relevant to hepatic glucose metabolism. Total protein levels of Akt, FOXO1, and
GSK3-β did not change with treatment, and were used to normalize quantification of the
respective phospho-proteins. (Figure 3.6A). Animals in the euglycemic (SE and GE)
groups featured similar 4.8-fold increases in P-Ser473 Akt relative to the control animals.
However, animals in both hypoglycemic groups had partially blunted Akt activation, with
only 2.1- and 1.5-fold increases in P-Ser473 Akt being observed in the SH and GH
groups, respectively. Relative to control animals, P-Ser9 GSK3-β was increased

67
substantially (7.0-fold increase) in SE animals, while progressively smaller increases
(5.7-, 4.4-, and 1.4-fold) were observed in the GE, SH, and GH groups, respectively.
FOXO1 (Ser256) phosphorylation was markedly increased (5.5-fold) in the SE group
relative to control animals, but only a 1.9-fold rise was observed in the GE group and
there was no increase apparent in either hypoglycemic test condition.
To assess glucagon signaling, we assayed levels of phosphorylated (Ser133)
cAMP-response element-binding protein (CREB), PPAR gamma coactivator-1α (PGC1α)
and PEPCK protein levels. Total levels of CREB protein did not vary between groups,
while P-Ser133 CREB was strongly suppressed in the SE group relative to control
animals, but this suppression was equivalently blocked by the presence of hypoglycemia
and/or glucagon in the other groups. Levels of PGC1α were depressed in the SE group to
~60% of that observed in control animals, but the presence of glucagon and/or
hypoglycemia (GE, SH, GH) led to 2.5-fold increases in PGC1α in these groups.
Likewise, the PEPCK protein level in the SE animals was reduced to ~60% of that in
control animals, but were unchanged from basal in the other three groups. Analysis of
gene transcription revealed that PEPCK mRNA levels were decreased by 89% in the SE
group relative to that in the control animals and this strong repression was decreased by
hypoglycemia and/or glucagon, leading to a doubling of PEPCK mRNA relative to that
evident in the SE animals (Figure 3.6B). Similarly, G6Pase mRNA expression was
reduced in the SE group by 87%. Both GE and SH groups exhibited a doubling in
G6Pase mRNA relative to the SE group, and the combination of glucagon and
hypoglycemia (GH) led to an even more substantial (3-fold) increase.

68
Art
eria
lPl
asm
a In
sulin
( U
/ml)
0
150
300
450
SAL + EUGGN + EUSAL + HYPOGGN + HYPO
Time (min)
-40 0 60 120 180
Art
eria
lPl
asm
a G
luca
gon
(pg/
ml)
0
50
100
150
A
B
Figure 3.1 - (A) Arterial plasma insulin (U/ml) and (B) glucagon (pg/ml) during basal(-40 to 0 min) and experimental periods (0 to 180 min) in 18h fasted conscious dogs exposed to a controlled rise of glucagon in the presence of euglycemia and hypoglycemia. Values are means ± SEM; n=6 groups. *P<0.05 vs. euglycemic group; †P<0.05 vs. saline group.
Pe SRIF + Po INS (5.0 mU/kg/min)EU EU or HYPO
Po GGN (2.3 ng/kg/min)

69
A
B
C
Art
eria
l Pl
asm
aEp
inep
hrin
e(p
g/m
l)
0
1000
2000
3000
4000 SAL + EUGGN + EUSAL + HYPOGGN + HYPO
Time (min)
-40 0 60 120 180
Art
eria
l Pl
asm
aN
orep
inep
hrin
e(p
g/m
l)
0
200
400
600
Figure 3.2 - (A) Arterial plasma cortisol, (B) epinephrine and (C) norepinephrine (pg/ml) during basal (-40 to 0 min) and experimental periods (0 to 180 min) in 18h fasted conscious dogs exposed to a controlled rise of glucagon in the presence of euglycemia and hypoglycemia. Values are means ± SEM; n=6 groups. *P<0.05 vs. euglycemic group; †P<0.05 vs. saline group.
**
** *
**
** *
*
**
**
*
**
**
*
** *
***
*
*
Pe SRIF + Po INS (5.0 mU/kg/min)EU EU or HYPO
Po GGN (2.3 ng/kg/min)
Art
eria
lPl
asm
a C
ortis
ol(
g/dl
)
0
5
10
15
20
25

70
Art
eria
lPl
asm
a G
luco
se(m
g/dl
)
0
406080
100120A
B
Time (min)
-40 0 60 120 180
Glu
cose
Infu
sion
Rat
e(m
g/kg
/min
)
0
5
10
15
20
SAL + EUGGN + EUSAL + HYPOGGN + HYPO
Pe SRIF + Po INS (5.0 mU/kg/min)EU EU or HYPO
Po GGN (2.3 ng/kg/min)
Figure 3.3 - (A) Arterial plasma glucose (mg/kg/min) and glucose infusion rate (mg/kg/min) between 60 to 180 caused by glucagon (mg/kg/min2) during basal (-40 to 0 min) and experimental periods (0 to 180 min) in 18h fastedconscious dogs exposed to a controlled rise of glucagon in the presence of euglycemia and hypoglycemia. Values are means ± SEM; n=6 groups. *P<0.05 vs. euglycemic group; †P<0.05 vs. saline group.

71
GGN-SALHYPO
GGN-SALEU
Time (min)-40 0 60 120 180
-2
0
2
4
SAL+EUGGN+EU SAL+HYPO GGN+HYPO
Net
Hep
atic
G
luco
se B
alan
ce(m
g/kg
/min
)A
B
NHGU
NHGO
** *
*†*† *†*†
*† *†
Figure 3.4 - (A) Net Hepatic Glucose Balance (mg/kg/min) and the Delta AUC: for the increase in NHGO between 60 to 180 caused by glucagon (mg/kg/min2) during basal (-40 to 0 min) and experimental periods (0 to 180 min) in 18h fasted conscious dogs exposed to a controlled rise of glucagon in the presence of euglycemia and hypoglycemia. Values are means ± SEM; n=6 groups. *P<0.05 vs. euglycemic group; †P<0.05 vs. saline group.
***
Pe SRIF + Po INS (5.0 mU/kg/min)EU EU or HYPO
Po GGN (2.3 ng/kg/min)
Del
ta A
UC
: Fo
r the
incr
ease
in N
HG
O
from
the
last
2 h
ours
ca
used
by
gluc
agon
(mg/
kg/1
20m
in)
0
50
100
150
200
250
300

72
Del
ta A
UC
: Fo
r the
incr
ease
in G
LY fr
om th
e la
st 2
hou
rs
caus
ed b
y gl
ucag
on(m
g/kg
bw
/120
min
)
0
100
200
300
Pe SRIF + Po INS (5.0 mU/kg/min)EU EU or HYPO
Po GGN (2.3 ng/kg/min)
Figure 3.5 - (A) Net hepatic gluconeogenic and (B) glycogenolytic flux (mg/kg/min) during basal (-40 to 0 min)and experimental periods (0 to 180 min) in 18h fasted conscious dogs exposed to a controlled rise of glucagon in the presence of euglycemia and hypoglycemia. Values are means ± SEM; n=6 groups. *P<0.05 vs. euglycemic group; †P<0.05 vs. saline group.
A
Net GLY syn
Net GLY prod
Time (min)-40 0 60 120 180
Net
Hep
atic
G
lyco
geno
lytic
Flu
x(m
g/kg
/min
)
-2
0
2
4
SAL + EUGGN + EUSAL + HYPOGGN + HYPO
B*†
*†
*†*†
*†*†
GGN-SALHYPO
Net GNG
Net Gycolysis-1
0
1
2N
et H
epat
icG
NG
Flu
x(m
g/kg
/min
)
* * * *
* **
C
GGN-SALEU

73
A
B
Figure 3.6 - (A) Phosphorylation of Akt (Ser 473), GSK3- (Ser 9), FOXO1 (Ser 256), CREB(Ser 133) and PGC-1 and (B) relative gene expression of PEPCK and G-6-Pase of liver samples taken from 18h fasted conscious dogs exposed to a controlled rise of glucagon in the presence of euglycemia and hypoglycemia.

74
TABLE 3.1Pancreatic Polypeptide (pg/ml) during control (-40 to 0 min) and experimental periods (0-180 min) of studies conductedon 18h fasted conscious dogs exposed to a controlled rise in glucagon in the presence of euglycemia and hypoglycemia.
Pancreatic PolypeptideArterial plasma levels (pg/ml)
SAL-EU 148 ± 36 101 ± 19 82 ± 23 103 ± 20 101 ± 23 101 ± 25 103 ± 22GGN-EU 115 ± 33 82 ± 18 97 ± 27 130 ± 62 140 ± 84 118 ± 55 153 ± 96
SAL-HYPO 197 ± 64 149 ± 44 144 ± 40 155 ± 37 161 ± 48 169 ± 47 161 ± 43GGN-HYPO 227 ± 75 172 ± 59 175 ± 62 170 ± 53 190 ± 59 170 ± 54 170 ± 55
Mean ± SEM; n=6; *P < 0.05 vs. euglycemic group; †P<0.05 vs saline group.
P1 P2Experimental Period
180ControlPeriod 30-60 75 90 120 150

75
TABLE 3.2Tracer determined endogenous glucose production, utilization (mg/kg/min) and glucose clearance (ml/kg/min) during control (-40 to 0 min) and experimental periods (0-180 min) of studies conducted on 18h fasted conscious dogs exposed to a controlled rise in glucagon in the presence of euglycemia and hypoglycemia.
Tracer Determined Glucose Production Ra, mg/kg/min
SAL-EU 2.9 ± 0.3 0.7 ± 0.5 -0.7 ± 0.9 -0.1 ± 0.7 0.4 ± 0.6 0.1 ± 0.9 1.0 ± 0.3GGN-EU 2.2 ± 0.2 0.6 ± 0.9 0.6 ± 0.8 -1.1 ± 0.6 0.1 ± 1.0 -0.5 ± 1.1 0.8 ± 1.0
SAL-HYPO 2.5 ± 0.2 0.9 ± 0.8 -0.6 ± 1.4 -0.1 ± 0.9 1.9 ± 0.6 * 1.8 ± 0.6 * 1.8 ± 0.6GGN-HYPO 2.4 ± 0.1 0.6 ± 0.9 2.3 ± 0.4 2.0 ± 0.5* † 3.5 ± 0.6 * 3.3 ± 0.5 * 3.3 ± 0.5
Rd, mg/kg/minSAL-EU 2.8 ± 0.3 11.9 ± 1.8 15.0 ± 1.8 16.5 ± 1.9 18.2 ± 2.0 18.6 ± 2.1 19.6 ± 2.2GGN-EU 2.2 ± 0.2 11.6 ± 1.7 13.2 ± 0.5 14.2 ± 0.6 15.8 ± 0.8 16.9 ± 0.9 18.6 ± 1.3
SAL-HYPO 2.5 ± 0.2 10.6 ± 1.3 8.2 ± 1.5 7.3 ± 1.1 * 6.3 ± 0.8 * 6.1 ± 0.8 * 6.2 ± 0.9 *GGN-HYPO 2.4 ± 0.2 9.2 ± 1.7 8.1 ± 1.1 * 7.0 ± 1.0 * 5.8 ± 0.9 * 5.4 ± 0.7 * 5.3 ± 0.7 *
Glucose Clearance (ml/kg/min)SAL-EU 2.5 ± 0.3 11.4 ± 1.7 14.2 ± 1.8 15.4 ± 1.7 16.8 ± 1.8 17.2 ± 2.0 18.3 ± 2.3GGN-EU 2.0 ± 0.2 11.1 ± 1.6 12.7 ± 0.7 13.9 ± 0.9 15.7 ± 1.3 16.6 ± 1.2 18.2 ± 1.2
SAL-HYPO 2.2 ± 0.2 11.0 ± 1.4 12.7 ± 2.0 13.1 ± 1.9 13.4 ± 1.6 13.3 ± 1.6 13.6 ± 1.8 *GGN-HYPO 2.2 ± 0.1 9.3 ± 1.8 13.1 ± 2.0 13.2 ± 2.0 12.6 ± 2.0 12.0 ± 1.7 * 11.8 ± 1.6 *
Mean ± SEM; n=6; *P < 0.05 vs. euglycemic group; †P<0.05 vs saline group.
Experimental Period
30-60 75 90 120 150PeriodP1 P2Control
180

76
TABLE 3.3Lactate and alanine arterial blood levels and net hepatic balance during control (-40 to 0 min) and experimental periods (0-180 min) of studies conducted on 18h fasted conscious dogs exposed to a controlled rise in glucagon in the presence of euglycemia and hypoglycemia.
LACTATEArterial Blood Levels (µmol/ml)
SAL-EU 694 ± 130 836 ± 74 795 ± 118 796 ± 107 731 ± 103 633 ± 86 671 ± 102GGN-EU 486 ± 116 660 ± 71 728 ± 100 790 ± 92 769 ± 96 759 ± 122 793 ± 90
SAL-HYPO 758 ± 161 850 ± 92 603 ± 98 553 ± 108 1326 ± 369 1721 ± 416 * 1707 ± 380 *GGN-HYPO 563 ± 117 637 ± 105 659 ± 117 830 ± 251 1384 ± 394 1499 ± 351 * 1670 ± 340 *
Net Hepatic Lactate Balance (µmol/kg/min)SAL-EU 3.8 ± 4.8 8.0 ± 1.9 3.4 ± 2.4 0.7 ± 2.0 -1.8 ± 2.3 -1.9 ± 1.9 -2.9 ± 1.2GGN-EU 0.2 ± 3.1 6.1 ± 2.2 6.1 ± 2.1 4.7 ± 2.0 1.5 ± 1.3 0.7 ± 1.7 -2.1 ± 3.2
SAL-HYPO 4.5 ± 2.7 9.1 ± 2.7 -0.8 ± 1.7 -5.2 ± 1.3 -11.1 ± 2.1 * -12.4 ± 2.5 * -13.4 ± 2.5 *GGN-HYPO 2.2 ± 3.6 8.3 ± 2.2 5.7 ± 2.8 3.1 ± 3.6 † -6.1 ± 1.6 -9.2 ± 2.3 * -14.1 ± 3.3 *
Lactate Fractional ExtractionSAL-EU 0.1 ± 0.22 0.5 ± 0.12 0.2 ± 0.10 0.1 ± 0.12 -0.1 ± 0.11 -0.1 ± 0.11 -0.2 ± 0.09GGN-EU -0.1 ± 0.17 0.4 ± 0.17 0.3 ± 0.10 0.2 ± 0.06 0.1 ± 0.07 0.0 ± 0.08 -0.1 ± 0.11
SAL-HYPO 0.2 ± 0.08 0.5 ± 0.10 -0.1 ± 0.10 -0.4 ± 0.10* -0.4 ± 0.11 -0.3 ± 0.08 -0.2 ± 0.04GGN-HYPO 0.0 ± 0.16 0.5 ± 0.10 0.4 ± 0.20 0.2 ± 0.19 † -0.2 ± 0.05 -0.2 ± 0.03 -0.2 ± 0.04
ALANINEArterial Blood Levels (µmol/ml)
SAL-EU 385 ± 33 326 ± 33 255 ± 17 221 ± 17 190 ± 15 161 ± 16 151 ± 15GGN-EU 314 ± 41 255 ± 27 207 ± 21 192 ± 22 176 ± 21 159 ± 20 148 ± 18
SAL-HYPO 356 ± 30 298 ± 31 223 ± 21 192 ± 11 184 ± 17 180 ± 18 171 ± 14GGN-HYPO 331 ± 56 324 ± 42 226 ± 25 198 ± 20 190 ± 24 172 ± 20 167 ± 21
Net Hepatic Alanine Uptake (µmol/kg/min)SAL-EU 2.4 ± 0.4 2.6 ± 0.2 2.8 ± 0.6 2.5 ± 0.4 2.7 ± 0.2 2.4 ± 0.2 2.4 ± 0.2GGN-EU 2.3 ± 0.4 2.1 ± 0.4 2.4 ± 0.4 2.1 ± 0.4 2.3 ± 0.4 2.3 ± 0.5 2.6 ± 0.5
SAL-HYPO 2.5 ± 0.4 2.5 ± 0.6 2.2 ± 0.5 2.2 ± 0.3 2.4 ± 0.3 2.7 ± 0.2 3.1 ± 0.2GGN-HYPO 2.5 ± 0.6 2.1 ± 0.3 2.7 ± 0.5 2.1 ± 0.4 2.2 ± 0.4 2.6 ± 0.5 3.1 ± 0.5
Alanine Fractional ExtractionSAL-EU 1.2 ± 0.02 0.3 ± 0.02 0.4 ± 0.05 0.4 ± 0.04 0.4 ± 0.03 0.5 ± 0.01 0.5 ± 0.01GGN-EU 0.2 ± 0.03 0.3 ± 0.03 0.3 ± 0.02 0.3 ± 0.02 0.4 ± 0.03 0.4 ± 0.04 0.4 ± 0.04
SAL-HYPO 0.2 ± 0.03 0.3 ± 0.10 0.3 ± 0.10 0.3 ± 0.03 0.4 ± 0.04 0.4 ± 0.03 0.4 ± 0.03GGN-HYPO 0.2 ± 0.06 0.3 ± 0.10 0.4 ± 0.10 0.3 ± 0.06 0.3 ± 0.05 0.4 ± 0.05 0.4 ± 0.05
Mean ± SEM; n=6; *P < 0.05 vs. euglycemic group; †P<0.05 vs saline group.
PeriodP1 P2Control
180
Experimental Period
30-60 75 90 120 150

77
TABLE 3.4Glycerol and BOHB arterial blood levels and net hepatic balance during control (-40 to 0 min) and experimental periods (0-180 min) of studies conducted on 18h fasted conscious dogs exposed to a controlled rise in glucagon in the presence of euglycemia and hypoglycemia.
GLYCEROLArterial Blood Levels (µmol/ml)
SAL-EU 86 ± 18 38 ± 13 29 ± 7 25 ± 9 25 ± 9 27 ± 9 26 ± 5GGN-EU 77 ± 14 36 ± 12 24 ± 7 24 ± 6 21 ± 4 30 ± 11 27 ± 7
SAL-HYPO 78 ± 12 34 ± 8 68 ± 34 163 ± 31 * 253 ± 34 * 265 ± 43 * 269 ± 41 *GGN-HYPO 84 ± 17 42 ± 15 107 ± 54 139 ± 27 * 223 ± 29 * 212 ± 31 * 212 ± 27* †
Net Hepatic Glycerol Balance (µmol/kg/min)SAL-EU -1.7 ± 0.4 -0.6 ± 0.2 -0.5 ± 0.1 -0.5 ± 0.1 -0.5 ± 0.1 -0.4 ± 0.1 -0.5 ± 0.2GGN-EU -1.5 ± 0.3 -0.8 ± 0.3 -0.8 ± 0.4 -0.5 ± 0.2 -0.4 ± 0.1 -0.7 ± 0.3 -0.7 ± 0.2
SAL-HYPO -1.8 ± 0.3 -0.8 ± 0.3 -2.1 ± 1.2 -4.1 ± 0.9 * -6.0 ± 1.3 * -6.9 ± 1.5 * -7.9 ± 1.5 *GGN-HYPO -2.2 ± 0.6 -1.1 ± 0.4 -2.9 ± 1.3 -3.4 ± 0.5 * -5.2 ± 0.8 * -5.7 ± 0.9 * -5.9 ± 0.6* †
Glycerol Fractional ExtractionSAL-EU -0.7 ± 0.1 -0.5 ± 0.1 -0.6 ± 0.1 -0.7 ± 0.1 -0.6 ± 0.1 -0.5 ± 0.1 -0.7 ± 0.1GGN-EU -0.6 ± 0.1 -0.7 ± 0.1 -0.6 ± 0.2 -0.6 ± 0.1 -0.6 ± 0.1 -0.6 ± 0.1 -0.7 ± 0.1
SAL-HYPO -0.7 ± 0.0 -0.7 ± 0.1 -0.7 ± 0.0 -0.7 ± 0.0 -0.7 ± 0.0 -0.7 ± 0.0 -0.7 ± 0.0GGN-HYPO -0.7 ± 0.0 -0.7 ± 0.1 -0.7 ± 0.1 -0.7 ± 0.0 -0.7 ± 0.0 -0.7 ± 0.0 -0.7 ± 0.0
BOHBArterial Blood Levels (µmol/ml)
SAL-EU 30 ± 6 22 ± 5 22 ± 7 18 ± 5 18 ± 6 20 ± 6 20 ± 6GGN-EU 40 ± 11 12 ± 2 10 ± 1 10 ± 2 9 ± 1 10 ± 1 10 ± 2
SAL-HYPO 27 ± 3 20 ± 7 16 ± 6 31 ± 6 35 ± 11 37 ± 15 * 32 ± 15GGN-HYPO 32 ± 7 13 ± 1 13 ± 3 14 ± 1 19 ± 3 15 ± 1 † 18 ± 1
Net Hepatic BOHB Balance (µmol/kg/min)SAL-EU 0.5 ± 0.1 0.2 ± 0.1 0.1 ± 0.0 0.1 ± 0.0 0.0 ± 0.1 0.0 ± 0.1 0.0 ± 0.0GGN-EU 1.1 ± 0.4 0.1 ± 0.0 0.1 ± 0.0 0.1 ± 0.1 0.1 ± 0.0 0.1 ± 0.0 0.1 ± 0.0
SAL-HYPO 0.5 ± 0.2 0.3 ± 0.1 0.3 ± 0.1 0.9 ± 0.4 0.3 ± 0.2 0.2 ± 0.2 0.3 ± 0.2GGN-HYPO 0.9 ± 0.3 0.2 ± 0.1 0.3 ± 0.1 0.3 ± 0.1 † 0.3 ± 0.1 0.2 ± 0.1 0.3 ± 0.1
Mean ± SEM; n=6; *P < 0.05 vs. euglycemic group; †P<0.05 vs saline group.
Experimental PeriodP1 P2
180ControlPeriod 30-60 75 90 120 150

78
TABLE 3.5Arterial plasma free fatty acids levels and net hepatic FFA balance during control (-40 to 0 min) and experimental periods (0-180 min) of studies conducted on 18h fasted conscious dogs exposed to a controlled rise in glucagon in the presence of euglycemia and hypoglycemia.
Free Fatty AcidsArterial plasma levels (µmol/l)
SAL-EU 819 ± 126 136 ± 23 83 ± 9 68 ± 7 57 ± 6 47 ± 4 43 ± 2GGN-EU 835 ± 129 105 ± 26 91 ± 25 68 ± 19 52 ± 15 53 ± 15 45 ± 13
SAL-HYPO 838 ± 87 122 ± 17 249 ± 157 * 617 ± 190 * 676 ± 101 * 600 ± 103 * 547 ± 76 *GGN-HYPO 849 ± 131 96 ± 33 163 ± 51 303 ± 37* † 593 ± 147 * 416 ± 101 * 376 ± 115 *
Net Hepatic FFA Balance (µmol/kg/min)SAL-EU -2.9 ± 0.7 -0.1 ± 0.2 0.0 ± 0.1 0.0 ± 0.1 -0.1 ± 0.1 -0.1 ± 0.2 0.0 ± 0.1GGN-EU -2.7 ± 0.5 -0.3 ± 0.1 -0.2 ± 0.1 -0.2 ± 0.1 0.0 ± 0.1 -0.1 ± 0.1 -0.2 ± 0.1
SAL-HYPO -2.7 ± 0.5 0.1 ± 0.1 -0.6 ± 0.6 -2.4 ± 0.9* -2.9 ± 0.4 * -3.0 ± 1.2 * -2.2 ± 0.6 *GGN-HYPO -3.0 ± 0.7 0.0 ± 0.1 -0.1 ± 0.2 -0.7 ± 0.2 † -2.0 ± 0.8 * -1.4 ± 0.7 † -1.5 ± 0.6 *
Mean ± SEM; n=6; *P < 0.05 vs. euglycemic group; †P<0.05 vs saline group.
Experimental Period
180ControlPeriod 30-60 75 90 120 150
P1 P2

79
Discussion
Previous studies have shown that the response of the alpha cell is critical for a
normal counterregulatory response to insulin-induced hypoglycemia (15; 18; 167-169).
In fact glucagon is widely thought to provide the primary defense against a low blood
glucose level. On the other hand, insulin is known to exert a powerful restraining effect
on glucagon’s action (131). This raises the question of how glucagon can have such a
prominent role in counterregulation if it is so easily subject to insulin’s inhibitory action.
The aim of the present study therefore was to determine the extent to which
hypoglycemia enhances glucagon’s ability to overcome insulin’s inhibitory effect on the
liver, and to shed some light on the mechanism by which this comes about. The present
results indicate that hypoglycemia increases glucagon’s ability to increase glucose
production by 2.3 fold even in the presence of extremely high insulin levels. Further,
they also show that this reflects a marked 2.7 fold increase in glycogenolysis which was
associated with a reduction in insulin’s phosphorylation of Akt and enhanced ability of
glucagon to activate GSK-3β.
In the current study, in the presence of hyperinsulinemia and euglycemia a
physiologic rise in glucagon mimicking that seen in response to insulin induced
hypoglycemia caused an increase in net hepatic glucose output that had an AUC of 106
mg/kg bw/120min. On the other hand, when the same rise in glucagon was brought
about under hypoglycemic conditions it produced a 2.3 fold greater increase (239
mg/kg/120min) in NHGO. The rise of glucagon had no effect on net hepatic
gluconeogenic flux under euglycemic or hypoglycemic conditions. In contrast, it had an
almost 3 fold greater effect on glycogenolysis in the presence of hypoglycemia than it did

80
in the presence of euglycemia. It should be noted that the changes in plasma epinephrine,
norepinephrine and cortisol which occurs in response to hypoglycemia were the same
whether glucagon was increased or not and thus a differential response in their secretion
cannot explain any of the differences in glucose production in the two hypoglycemic
groups.
It is possible to estimate how much of glucagon’s full effect is restored in the
presence of hypoglycemia. To do this one needs to determine the effect of an increment
in glucagon of the magnitude used in the present study in the presence of basal insulin
levels. In addition, because under such conditions glucagon would result in
hyperglycemia, one has to take into account the suppression of net hepatic glucose output
that would occur in response to the accompanying increase in glucose. We were able to
do this by analyzing data from earlier studies carried out in our laboratory (26; 131). It
was evident that the full response to a four fold rise in glucagon had an AUC of 423
mg/kg bw/120min. Therefore under euglycemic conditions the rise in insulin which we
employed resulted in a 75% inhibition of glucagon’s action. In the presence of
hypoglycemia, on the other hand, the rise in insulin was only able to reduce glucagon’s
action by slightly more than 40%.
The question then arises as to the mechanism by which the liver’s responsiveness
to glucagon is enhanced by hypoglycemia. It is unclear which physiologic signal,
increased cortisol, increased epinephrine, increased norepinephrine, increased neural
input to the liver, hypoglycemia per se or some combination of these, explains this
important adaptive response. It is certainly possible that hypoglycemia per se brings
about the effect. Previous studies have shown that hyperglycemia per se can inhibit

81
hepatic glucose production (170). The biochemical explanation for this effect is that
glucose binds to phosphorylase in the allosteric site of the phosphorylated form of the
enzyme, causing a conformational change that makes phosphorylase a better substrate for
dephosphorylation by protein phosphatase 1 (PP1) (170). This leads to an inactivation of
the enzyme (170). The fact changes in glycogen metabolism provided the explanation for
the augmented response of the liver to glucagon supports this possibility. On the other
hand, Shiota et al. (171) have performed studies using the perfused rat liver to determine
the ability of hyperglycemia to inhibit the response of the liver to glucagon. In their
study they found that the hyperglycemia reduced basal net hepatic glucose output but not
the response of the liver to glucagon.
Another possibility is that the enhanced response to glucagon during insulin-
induced hypoglycemia is related to the interaction of glucagon with one or other of the
counterregulatory hormones. The effects of these hormones in a hypoglycemic setting by
themselves are well established. Epinephrine restrains the fall in glucose by stimulating
hepatic glucose production, limiting glucose utilization and augmenting muscle
glycogenolysis and adipose tissue lipolysis (19; 26; 28; 31). The ability of
norepinephrine to restrain the fall in glucose, while not as potent as epinephrine’s,
involves a stimulatory effect on gluconeogenesis which results from a glycogenolytic
effect in muscle and lipolytic effect in fat (26; 30; 32). Cortisol restrains the fall in
glucose by maintaining substrate availability to support gluconeogenesis (35; 36; 172).
Several studies have looked at the acute interaction of the counterregulatory
hormones. Eigler et al. (173) in the dog and Shamoon et al. (174) in the human studied
the interaction of epinephrine, glucagon and cortisol. In their studies the infusion of the

82
hormones individually resulted in a transient increase in glucose production, but the
effect of glucagon and epinephrine together resulted in additive effects on glucose
production whereas addition of cortisol resulted in a synergistic effect on glucose
production. However, since neither the insulin and/or glucose levels were controlled in
these studies any interpretation of the data is difficult. Lecavalier et al. (175) performed
studies in humans to assess the interaction between glucagon and cortisol on
gluconeogenesis from 14C lactate in a more controlled way. In these studies, glucose was
clamped and they used a pancreatic pituitary clamp to control for changes in insulin,
glucagon and growth hormone. They found that cortisol enhanced glucagon-stimulated
gluconeogenesis in an additive manner. However, the increment in glucagon used in
these studies was very high so it is conceivable that a synergistic effect of the hormones
could have been missed. Gustavson et al. (176) studied the interaction of epinephrine
and glucagon in the regulation of hepatic glucose production at a time when plasma
insulin and hyperglycemia were fixed in overnight fasted conscious dogs. In their studies
the area under the curve for the increase in net hepatic glucose output in the groups was
661±185, 424±158 and 1,178±57 mg/kg in the glucagon, epinephrine and glucagon +
epinephrine groups respectively. This led to the conclusion that the effects of glucagon
and epinephrine on hepatic glucose production are additive but not synergistic.
Therefore, it seems unlikely that the interaction of glucagon with the other
counterregulatory hormones contributes to the increased sensitivity of the liver to the
hormone during insulin-induced hypoglycemia.
It is also interesting to consider the enhancement of glucagon action in the
presence of hypoglycemia at a cellular level. To do so we analyzed key markers in both

83
the insulin and glucagon signaling pathways. Insulin exerts its effect by phosphorylating
Akt, which in turn phosphorylates and inactivates GSK-3β, preventing the
phosphorylation and inactivation of glycogen synthase (177). Thus, phosphorylated
GSK-3β is an indirect marker of increased glycogen synthesis, it can also be indicative of
decreased glycogenolysis, since glycogen synthesis and breakdown are tightly
coordinated. In addition, Akt phosphorylates the transcription factor FOXO1.
Phosphorylated FOXO1 accumulates in the cytosol, decreasing the expression of the
gluconeogenic genes PEPCK and G6Pase, thereby potentially decreasing hepatic glucose
production(178; 179). Conversely, glucagon action leads to the phosphorylation of
CREB which enhances PGC1α transcription (86); PGC1α synergistically acts with
FOXO1 to promote the transcription of both PEPCK and G6Pase, increasing
gluconeogenesis and as a result hepatic glucose production (180-182)
In the present studies the insulin signaling pathway was strongly activated in the
SE group, as evidenced by marked increases in phosphorylated Akt, GSK-3β, and
FOXO1. The addition of glucagon in the presence of euglycemia (GE) did not alter Akt
activation, but led to a partial blunting of GSK-3β, and FOXO1 phosphorylation,
indicating that part of glucagon’s ability to overcome insulin’s inhibition of hepatic
glucose production was related to an impairment in insulin signaling downstream of Akt.
Phosphorylation of Akt was blunted during both hypoglycemic conditions (SH and GH)
suggesting that hypoglycemia or some change associated with it, blunts that ability of
insulin to activate its signaling cascade. Hypoglycemia (in the absence of glucagon; SH)
decreased phosphorylated GSK-3β but the combination of hypoglycemia and glucagon
produced an even more substantial (95%) decrease in GSK-3β phosphorylation relative to

84
that seen in the SE group. In fact the ability of the increase in glucagon to decrease
phosphorylated GSK-3β (SE vs. GE relative to SH vs. GH) was increased 2.3 fold by
hypoglycemia. This correlates well with the 3 fold increase in glycogenolysis caused by
the hormone in the presence of hypoglycemia.
At the same time markers of glucagon signaling indicated that phosphorylated
CREB, as well as PGC1α and PEPCK protein levels were decreased when insulin was
increased (SE). It should be remembered that basal glucagon secretion was inhibited by
somatostatin with the resulting hypoglucagonemia in the SE and SH groups. As such
changes in the SE protocol can be a function of the rise of insulin and/or the fall in
glucagon. Phosphorylated CREB and PEPCK levels were restored to control values by
glucagon (GE). PGC1α, on the other hand, was increased above the control value by
glucagon. Hypoglycemia (in the absence of glucagon; SH) caused similar changes. The
addition of glucagon to hypoglycemia did little to magnify these changes.
Gene expression data confirmed that PEPCK and G6Pase mRNA levels were
substantially reduced by the rise in insulin (SE) and the fall in glucagon. Addition of the
increase in glucagon or hypoglycemia (in the absence of glucagon) doubled the mRNA
expression of both enzymes. Addition of an increase in glucagon to hypoglycemia did
not increase the expression of PEPCK mRNA further but it did increase the expression of
G-6-Pase mRNA by twofold over what it did under euglycemic conditions. Taken
together the molecular data support a reduction in insulin signaling in the presence of
hypoglycemia combined with an enhanced ability of the increase in glucagon to decrease
the phosphorylation of GSK-3β and to increase G-6-Pase gene expression.

85
It is worth noting that 90% fall in mRNA for PEPCK was associated with only a
40% fall in PEPCK protein and little or no change in net hepatic gluconeogenic flux (SE).
These data are consistent with those from Burgess et al. (183) in which isolated perfused
livers with a 90% reduction of PEPCK content showed only a 40% reduction in
gluconeogenic flux, indicating that PEPCK content has limited control strength over the
gluconeogenic process. Hypoglycemia markedly increased NHGNG flux despite PEPCK
mRNA still being reduced by almost 80% and PEPCK protein being unchanged from
control values. The question thus arises as to how the increase in gluconeogenesis comes
about. The answer lies in the large increases in the delivery of gluconeogenic precursors
to the liver during hypoglycemia.
In muscle, in the presence of hyperinsulinemic hypoglycemia (SH, GH) there
was a marked increase in the arterial blood lactate level and as a resulting in net hepatic
lactate uptake. This indicates that production of lactate by muscle increased dramatically
as a result of the rise in catecholamines (31; 32), neural input to muscle and/or
hypoglycemia per se. The increase in glucagon had no impact on the rise in blood lactate
or net hepatic lactate uptake.
Lipolysis is best estimated from the glycerol data since glycerol must be released
from the fat cell and can not be used for re-esterification. In the presence of
hyperinsulinemic euglycemia (SE) there was a marked inhibition of lipolysis as indicated
by a fall in blood glycerol levels. In the presence of the same conditions a physiologic
rise in glucagon had no effect on lipolysis. During insulin-induced hypoglycemia (SH,
GH), there was a marked increase in arterial blood glycerol and net hepatic glycerol
uptake indicating a dramatic rise in lipolysis. This was the result of the lipolytic effect of

86
catecholamines, hypoglycemia per se and/or neural input to fat (31; 32) Once again the
rise in glucagon had no effect on the response. Thus the marked increase in the net
hepatic gluconeogenesis in response to hypoglycemia was a function of increased
substrate delivery to the liver rather than a stimulation of the hepatic gluconeogenic
pathway per se. Addition of a physiologic rise in glucagon to hypoglycemia and its
various effects doubled the magnitude of the increase in glucose production which
occurred. This underscores the importance of glucagon to the increase in hepatic glucose
production seen during insulin-induced hypoglycemia. For this to be relevant to the
normal response to insulin-induced hypoglycemia it is important to point out that the
magnitude of the increment in glucagon which we used in the study represents the normal
physiologic response of glucagon to hypoglycemia of 50 mg/dl caused by insulin infusion
at 5.0 mU/kg/min and plasma glucose decrease to 50 mg/dl. Frizzell et al. (7) showed
that when insulin was infused at 5mU/kg/min, the increment in glucagon levels over 2
hours was Δ 9510 pg/kg bw/120 min. The increment in glucagon in our studies was Δ
8276 pg/kg bw/120 min. Therefore, the rise in glucagon which we used in our studies
represents a normal response of the hormone to hypoglycemia. It should be noted,
however, that we used a square wave elevation of glucagon to simplify the experimental
design whereas under normal circumstances the response would have had a spike decline
pattern.
In summary, hypoglycemia increased glucagon’s ability to overcome insulin’s
inhibitory effect on hepatic glucose production. This effect was attributable to a marked
(almost 3-fold) enhancement of net glycogen breakdown. It paralleled an increase in the
ability of glucagon to reduce the phosphorylation of GSK-3β in the presence of

87
hypoglycemia as opposed to euglycemia. At the same time hypoglycemia decreased
insulin’s activation of its signaling cascade. Proof that it is hypoglycemia per se, rather
than an increase neural input to the liver, or increases in some other component of the
counterregulatory response remains to be obtained.
Summary and Conclusions
In the United States, approximately 23.2 million people have diabetes (~8% of
population). Of those 18.6 million have been diagnosed and 4.6 million do not yet know
they have the disease. There are three types of diabetes: type1 diabetes, type 2 diabetes
and gestational diabetes. Type 1 diabetes is an autoimmune disease in which the immune
system destroys the insulin-producing β cells in the pancreas. Type 1 diabetes accounts
for about 5 to 10 percent of diagnosed diabetes. On the other hand, Type 2 diabetes
which is the most common form of diabetes accounts for ~ 90-95% of people with the
disease. Type 2 diabetes is characterized by insulin resistance and hyperglycemia.
Gestational diabetes is a type of diabetes that occurs only during pregnancy. Although
this form of diabetes usually disappears after birth of the baby, women who have had
gestational diabetes have a 20% to 50% chance of developing Type 2 diabetes within 5-
10 years.
Glycemic control is fundamental for the management of the disease. Reduction
of glucose levels prevents macrovascular and microvascular complications such as heart
disease, retinopathy, nephropathy and neuropathy in both type 1 and type 2 diabetes.
Another complication that is a limiting factor in the management of diabetes is
hypoglycemia. Hypoglycemia is the most frequent complication of insulin-requiring
diabetes and the principal factor limiting optimization of glycemic control. Is typically

88
the result of the interplay of insulin excess and compromised glucose counterregulation in
individuals with type 1 diabetes. In addition, it may contribute to recurrent morbidity in
patients with type 1 diabetes and may sometimes be fatal in patients with advanced,
insulin-requiring type 2 diabetes.
Hypoglycemia triggers the activation of a counterregulatory response to increase
glucose production. The counterregulatory response to hypoglycemia involves the
release of glucagon, epinephrine, norepinephrine and cortisol. Glucagon increases
glucose production by activating glycogenolysis and gluconeogenesis; however, its effect
on gluconeogenesis is limited by its inability to increase gluconeogenic substrate delivery
to the liver. Epinephrine stimulates hepatic glucose production through activation of
gluconeogenesis and glycogenolysis. Norepinephrine increases hepatic glucose
production by increasing gluconeogenesis which results from a glycogenolytic effect in
muscle and a lipolytic effect in fat. Cortisol stimulates hepatic glucose production by
maintaining substrate availability to support gluconeogenesis and limits glucose
utilization.
Glucagon is the primary hormone involved in the regulation of glucose
production. In addition, previous studies have shown glucagon remains the most
important regulator of glucose production even in the presence of very high insulin levels
(18). In contrast, under euglycemic conditions Steiner et al. (131) have shown that
insulin is a potent inhibitor of glucagon’s effect on the liver. Therefore, our aim was to
determine the extent to which hypoglycemia augments glucagon’s ability to increase
glucose production and at a molecular level, how it does so.

89
In the studies described in this dissertation, hypoglycemia increased glucagon’s
ability to overcome insulin’s inhibitory effect on hepatic glucose production 2.3 fold.
This effect was attributable to a marked (almost 3-fold) enhancement of net glycogen
breakdown which was associated with a 2.3 fold increase in the ability of glucagon to
reduce the phosphorylation of GSK3β caused by insulin.
It remains unclear which physiologic signal (increased cortisol, epinephrine,
norepinephrine, neural input to the liver or hypoglycemia per se) explains this adaptive
response. Therefore future studies should be conducted to determine which of these
physiological signals is responsible for the enhancement of glucagon action. It would be
of interest therefore to determine the effects of these other counterregulatory hormones
on glucagon’s action. One could conduct studies to assess the physiologic effects of
elevated cortisol, epinephrine and norepinephrine with or without a rise in glucagon in
the presence of euglycemia and hyperinsulinemia. The counterregulatory hormones
would be selectively increased to the levels seen during hypoglycemia and euglycemia
would be maintained in order discriminate between the effects of the counterregulatory
hormones and hypoglycemia per se. To assess the role of hypoglycemia per se in
overriding insulin’s inhibitory effect on glucagon action one could conduct studies in
adrenalectomized dogs. Using this approach we could eliminate the effects of
epinephrine and cortisol by removing the adrenal glands and because most of the
norepinephrine involve in the counterregulation process is released from sympathetic
postganglionic neurons one could use a α1-adrenergic blocker to inhibit norepinephrine
effects on the liver (24). Glucagon would be selectively increased and its physiologic
effect in overriding insulin’s inhibitory effect would be determined in the presence of

90
hyperinsulinemic-euglycemic or hyperinsulinemic-hypoglycemic conditions. These
studies would therefore determine if hypoglycemia itself is making glucagon more
effective during insulin-induced hypoglycemia.

91
REFERENCES
1. Cryer PE: The prevention and correction of hypoglycemia. In Handbook of Physiology: The Endocrine Pancreas and Regulation of Metabolism Jefferson L CA, Ed. New York, Oxford University Press, 2001, p. 1057-1092
2. Cryer PE: Hypoglycemia-associated autonomic failure in diabetes. Am J Physiol Endocrinol Metab 281:E1115-1121, 2001
3. Garber AJ, Cryer PE, Santiago JV, Haymond MW, Pagliara AS, Kipnis DM: The role of adrenergic mechanisms in the substrate and hormonal response to insulin-induced hypoglycemia in man. J Clin Invest 58:7-15, 1976
4. Davis SN, Cherrington AD: The hormonal and metabolic responses to prolonged hypoglycemia. J Lab Clin Med 121:21-31, 1993
5. Lecavalier L, Bolli G, Cryer P, Gerich J: Contributions of gluconeogenesis and glycogenolysis during glucose counterregulation in normal humans. Am J Physiol 256:E844-851, 1989
6. Caprio S, Sacca L, Tamborlane WV, Sherwin RS: Relationship between changes in glucose production and gluconeogenesis during mild hypoglycemia in humans. Metabolism 37:707-710, 1988
7. Frizzell RT, Hendrick GK, Biggers DW, Lacy DB, Donahue DP, Green DR, Carr RK, Williams PE, Stevenson RW, Cherrington AD: Role of gluconeogenesis in sustaining glucose production during hypoglycemia caused by continuous insulin infusion in conscious dogs. Diabetes 37:749-759, 1988
8. Cryer PE, Davis SN, Shamoon H: Hypoglycemia in diabetes. Diabetes Care 26:1902-1912, 2003
9. Mitrakou A, Ryan C, Veneman T, Mokan M, Jenssen T, Kiss I, Durrant J, Cryer P, Gerich J: Hierarchy of glycemic thresholds for counterregulatory hormone secretion, symptoms, and cerebral dysfunction. Am J Physiol 260:E67-74, 1991
10. Gromada J, Franklin I, Wollheim CB: Alpha-cells of the endocrine pancreas: 35 years of research but the enigma remains. Endocr Rev 28:84-116, 2007
11. Flattem N, Igawa K, Shiota M, Emshwiller MG, Neal DW, Cherrington AD: Alpha- and beta-cell responses to small changes in plasma glucose in the conscious dog. Diabetes 50:367-375, 2001

92
12. Raju B, Cryer PE: Loss of the decrement in intraislet insulin plausibly explains loss of the glucagon response to hypoglycemia in insulin-deficient diabetes: documentation of the intraislet insulin hypothesis in humans. Diabetes 54:757-764, 2005
13. Bolli GB, Fanelli CG: Physiology of glucose counterregulation to hypoglycemia. Endocrinol Metab Clin North Am 28:467-493, v, 1999
14. Gerich J, Cryer P, Rizza R: Hormonal mechanisms in acute glucose counterregulation: the relative roles of glucagon, epinephrine, norepinephrine, growth hormone, and cortisol. Metabolism 29:1164-1175, 1980
15. Gerich J, Davis J, Lorenzi M, Rizza R, Bohannon N, Karam J, Lewis S, Kaplan R, Schultz T, Cryer P: Hormonal mechanisms of recovery from insulin-induced hypoglycemia in man. Am J Physiol 236:E380-385, 1979
16. Rizza RA, Cryer PE, Gerich JE: Role of glucagon, catecholamines, and growth hormone in human glucose counterregulation. Effects of somatostatin and combined alpha- and beta-adrenergic blockade on plasma glucose recovery and glucose flux rates after insulin-induced hypoglycemia. J Clin Invest 64:62-71, 1979
17. De Feo P, Perriello G, Torlone E, Fanelli C, Ventura MM, Santeusanio F, Brunetti P, Gerich JE, Bolli GB: Evidence against important catecholamine compensation for absent glucagon counterregulation. Am J Physiol 260:E203-212, 1991
18. Dobbins RL, Connolly CC, Neal DW, Palladino LJ, Parlow AF, Cherrington AD: Role of glucagon in countering hypoglycemia induced by insulin infusion in dogs. Am J Physiol 261:E773-781, 1991
19. Stevenson RW, Steiner KE, Connolly CC, Fuchs H, Alberti KG, Williams PE, Cherrington AD: Dose-related effects of epinephrine on glucose production in conscious dogs. Am J Physiol 260:E363-370, 1991
20. Stevenson RW, Steiner KE, Davis MA, Hendrick GK, Williams PE, Lacy WW, Brown L, Donahue P, Lacy DB, Cherrington AD: Similar dose responsiveness of hepatic glycogenolysis and gluconeogenesis to glucagon in vivo. Diabetes 36:382-389, 1987
21. Cherrington AD, Fuchs H, Stevenson RW, Williams PE, Alberti KG, Steiner KE: Effect of epinephrine on glycogenolysis and gluconeogenesis in conscious overnight-fasted dogs. Am J Physiol 247:E137-144, 1984
22. Sacca L, Vigorito C, Cicala M, Corso G, Sherwin RS: Role of gluconeogenesis in epinephrine-stimulated hepatic glucose production in humans. Am J Physiol 245:E294-302, 1983

93
23. Steiner KE, Stevenson RW, Green DR, Cherrington AD: Mechanism of epinephrine's glycogenolytic effect in isolated canine hepatocytes. Metabolism 34:1020-1023, 1985
24. Chu CA, Sindelar DK, Igawa K, Sherck S, Neal DW, Emshwiller M, Cherrington AD: The direct effects of catecholamines on hepatic glucose production occur via alpha(1)- and beta(2)-receptors in the dog. Am J Physiol Endocrinol Metab 279:E463-473, 2000
25. Chu CA, Sindelar DK, Neal DW, Cherrington AD: Direct effects of catecholamines on hepatic glucose production in conscious dog are due to glycogenolysis. Am J Physiol 271:E127-137, 1996
26. Chu CA, Sindelar DK, Neal DW, Allen EJ, Donahue EP, Cherrington AD: Comparison of the direct and indirect effects of epinephrine on hepatic glucose production. J Clin Invest 99:1044-1056, 1997
27. Rizza R, Haymond M, Cryer P, Gerich J: Differential effects of epinephrine on glucose production and disposal in man. Am J Physiol 237:E356-362, 1979
28. Winder WW, MacLean PS, Chandler SL, Huang W, Mills RH: Role of epinephrine during insulin-induced hypoglycemia in fasted rats. J Appl Physiol 77:270-276, 1994
29. Silverberg AB, Shah SD, Haymond MW, Cryer PE: Norepinephrine: hormone and neurotransmitter in man. Am J Physiol 234:E252-256, 1978
30. Connolly CC, Steiner KE, Stevenson RW, Neal DW, Williams PE, Alberti KG, Cherrington AD: Regulation of glucose metabolism by norepinephrine in conscious dogs. Am J Physiol 261:E764-772, 1991
31. Steiner KE, Fuchs H, Williams PE, Stevenson RW, Cherrington AD, Alberti KG: Regulation of ketogenesis by epinephrine and norepinephrine in the overnight-fasted, conscious dog. Diabetes 34:425-432, 1985
32. Connolly CC, Steiner KE, Stevenson RW, Neal DW, Williams PE, Alberti KG, Cherrington AD: Regulation of lipolysis and ketogenesis by norepinephrine in conscious dogs. Am J Physiol 261:E466-472, 1991
33. Boyle PJ, Cryer PE: Growth hormone, cortisol, or both are involved in defense against, but are not critical to recovery from, hypoglycemia. Am J Physiol 260:E395-402, 1991

94
34. De Feo P, Perriello G, Torlone E, Ventura MM, Santeusanio F, Brunetti P, Gerich JE, Bolli GB: Demonstration of a role for growth hormone in glucose counterregulation. Am J Physiol 256:E835-843, 1989
35. Goldstein RE, Reed GW, Wasserman DH, Williams PE, Lacy DB, Buckspan R, Abumrad NN, Cherrington AD: The effects of acute elevations in plasma cortisol levels on alanine metabolism in the conscious dog. Metabolism 41:1295-1303, 1992
36. Goldstein RE, Wasserman DH, McGuinness OP, Lacy DB, Cherrington AD, Abumrad NN: Effects of chronic elevation in plasma cortisol on hepatic carbohydrate metabolism. Am J Physiol 264:E119-127, 1993
37. Moore MC, Connolly CC, Cherrington AD: Autoregulation of hepatic glucose production. Eur J Endocrinol 138:240-248, 1998
38. Cherrington AD, Connolly CC, Chu CA, Moore MC: The role of neural signalling and hypoglycaemia per se in the counterregulatory response. Diabetes Nutr Metab 15:303-307; discussion 307-308, 2002
39. Glinsmann WH, Hern EP, Lynch A: Intrinsic regulation of glucose output by rat liver. Am J Physiol 216:698-703, 1969
40. Frizzell RT, Hendrick GK, Brown LL, Lacy DB, Donahue EP, Carr RK, Williams PE, Parlow AF, Stevenson RW, Cherrington AD: Stimulation of glucose production through hormone secretion and other mechanisms during insulin-induced hypoglycemia. Diabetes 37:1531-1541, 1988
41. Bolli G, De Feo P, Perriello G, De Cosmo S, Ventura M, Campbell P, Brunetti P, Gerich JE: Role of hepatic autoregulation in defense against hypoglycemia in humans. J Clin Invest 75:1623-1631, 1985
42. Connolly CC, Adkins-Marshall BA, Neal DW, Pugh W, Jaspan JB, Cherrington AD: Relationship between decrements in glucose level and metabolic response to hypoglycemia in absence of counterregulatory hormones in the conscious dog. Diabetes 41:1308-1319, 1992
43. Biggers DW, Myers SR, Neal D, Stinson R, Cooper NB, Jaspan JB, Williams PE, Cherrington AD, Frizzell RT: Role of brain in counterregulation of insulin-induced hypoglycemia in dogs. Diabetes 38:7-16, 1989
44. Edwards AV: The hyperglycaemic response to stimulation of the hepatic sympathetic innervation in adrenalectomized cats and dogs. J Physiol 220:697-710, 1972

95
45. Shimazu T, Fukuda A, Ban T: Reciprocal influences of the ventromedial and lateral hypothalamic nuclei on blood glucose level and liver glycogen content. Nature 210:1178-1179, 1966
46. Borg MA, Sherwin RS, Borg WP, Tamborlane WV, Shulman GI: Local ventromedial hypothalamus glucose perfusion blocks counterregulation during systemic hypoglycemia in awake rats. J Clin Invest 99:361-365, 1997
47. Connolly CC, Myers SR, Neal DW, Hastings JR, Cherrington AD: In the absence of counterregulatory hormones, the increase in hepatic glucose production during insulin-induced hypoglycemia in the dog is initiated in the liver rather than the brain. Diabetes 45:1805-1813, 1996
48. Hamilton-Wessler M, Bergman RN, Halter JB, Watanabe RM, Donovan CM: The role of liver glucosensors in the integrated sympathetic response induced by deep hypoglycemia in dogs. Diabetes 43:1052-1060, 1994
49. Jackson PA, Pagliassotti MJ, Shiota M, Neal DW, Cardin S, Cherrington AD: Effects of vagal blockade on the counterregulatory response to insulin-induced hypoglycemia in the dog. Am J Physiol 273:E1178-1188, 1997
50. Jackson PA, Cardin S, Coffey CS, Neal DW, Allen EJ, Penaloza AR, Snead WL, Cherrington AD: Effect of hepatic denervation on the counterregulatory response to insulin-induced hypoglycemia in the dog. Am J Physiol Endocrinol Metab 279:E1249-1257, 2000
51. Saberi M, Bohland M, Donovan CM: The locus for hypoglycemic detection shifts with the rate of fall in glycemia: the role of portal-superior mesenteric vein glucose sensing. Diabetes 57:1380-1386, 2008
52. Cherrington AD: Control of glucose production in vivo by insulin and glucagon. In Handbook of Physiology: The Endocrine Pancreas and Regulation of Metabolism Jefferson L CA, Ed. New York, Oxford University Press, 2001, p. 759-785
53. Cherrington AD: Banting Lecture 1997. Control of glucose uptake and release by the liver in vivo. Diabetes 48:1198-1214, 1999
54. Dobbins RL, Davis SN, Neal D, Caumo A, Cobelli C, Cherrington AD: Rates of glucagon activation and deactivation of hepatic glucose production in conscious dogs. Metabolism 47:135-142, 1998

96
55. Cherrington AD, Williams PE, Shulman GI, Lacy WW: Differential time course of glucagon's effect on glycogenolysis and gluconeogenesis in the conscious dog. Diabetes 30:180-187, 1981
56. Chhibber VL, Soriano C, Tayek JA: Effects of low-dose and high-dose glucagon on glucose production and gluconeogenesis in humans. Metabolism 49:39-46, 2000
57. Magnusson I, Rothman DL, Gerard DP, Katz LD, Shulman GI: Contribution of hepatic glycogenolysis to glucose production in humans in response to a physiological increase in plasma glucagon concentration. Diabetes 44:185-189, 1995
58. Cherrington AD, Diamond MP, Green DR, Williams PE: Evidence for an intrahepatic contribution to the waning effect of glucagon on glucose production in the conscious dog. Diabetes 31:917-922, 1982
59. Ferrannini E, DeFronzo RA, Sherwin RS: Transient hepatic response to glucagon in man: role of insulin and hyperglycemia. Am J Physiol 242:E73-81, 1982
60. Kilberg MS, Stevens BR, Novak DA: Recent advances in mammalian amino acid transport. Annu Rev Nutr 13:137-165, 1993
61. Pilkis SJ, Granner DK: Molecular physiology of the regulation of hepatic gluconeogenesis and glycolysis. Annu Rev Physiol 54:885-909, 1992
62. Pilkis SJ, Park CR, Claus TH: Hormonal control of hepatic gluconeogenesis. Vitam Horm 36:383-460, 1978
63. Christ B, Nath A, Bastian H, Jungermann K: Regulation of the expression of the phosphoenolpyruvate carboxykinase gene in cultured rat hepatocytes by glucagon and insulin. Eur J Biochem 178:373-379, 1988
64. Iynedjian PB, Auberger P, Guigoz Y, Le Cam A: Pretranslational regulation of tyrosine aminotransferase and phosphoenolpyruvate carboxykinase (GTP) synthesis by glucagon and dexamethasone in adult rat hepatocytes. Biochem J 225:77-84, 1985
65. Hanson RW, Reshef L: Regulation of phosphoenolpyruvate carboxykinase (GTP) gene expression. Annu Rev Biochem 66:581-611, 1997
66. Davis MA, Williams PE, Cherrington AD: Effect of glucagon on hepatic lactate metabolism in the conscious dog. Am J Physiol 248:E463-470, 1985
67. Burcelin R, Katz EB, Charron MJ: Molecular and cellular aspects of the glucagon receptor: role in diabetes and metabolism. Diabetes Metab 22:373-396, 1996

97
68. Fradkin J, Shamoon H, Felig P, Sherwin RS: Evidence for an important role of changes in rather than absolute concentrations of glucagon in the regulation of glucose production in humans. J Clin Endocrinol Metab 50:698-703, 1980
69. Cherrington AD, Liljenquist JE, Shulman GI, Williams PE, Lacy WW: Importance of hypoglycemia-induced glucose production during isolated glucagon deficiency. Am J Physiol 236:E263-271, 1979
70. Jiang G, Zhang BB: Glucagon and regulation of glucose metabolism. Am J Physiol Endocrinol Metab 284:E671-678, 2003
71. Summers RJ, McMartin LR: Adrenoceptors and their second messenger systems. J Neurochem 60:10-23, 1993
72. Winzell MS, Ahren B: G-protein-coupled receptors and islet function-implications for treatment of type 2 diabetes. Pharmacol Ther 116:437-448, 2007
73. Neves SR, Ram PT, Iyengar R: G protein pathways. Science 296:1636-1639, 2002
74. Mayo KE, Miller LJ, Bataille D, Dalle S, Goke B, Thorens B, Drucker DJ: International Union of Pharmacology. XXXV. The glucagon receptor family. Pharmacol Rev 55:167-194, 2003
75. Kraus-Friedmann N, Feng L: The role of intracellular Ca2+ in the regulation of gluconeogenesis. Metabolism 45:389-403, 1996
76. Kraus-Friedmann N: Effects of glucagon and vasopressin on hepatic Ca2+ release. Proc Natl Acad Sci U S A 83:8943-8946, 1986
77. Studer RK, Snowdowne KW, Borle AB: Regulation of hepatic glycogenolysis by glucagon in male and female rats. Role of cAMP and Ca2+ and interactions between epinephrine and glucagon. J Biol Chem 259:3596-3604, 1984
78. Yamatani K, Saito K, Ikezawa Y, Ohnuma H, Sugiyama K, Manaka H, Takahashi K, Sasaki H: Relative contribution of Ca2+-dependent mechanism in glucagon-induced glucose output from the liver. Arch Biochem Biophys 355:175-180, 1998
79. Exton JH: Mechanisms of hormonal regulation of hepatic glucose metabolism. Diabetes Metab Rev 3:163-183, 1987
80. Chrisman TD, Jordan JE, Exton JH: Purification of rat liver phosphorylase kinase. J Biol Chem 257:10798-10804, 1982

98
81. Krebs EG: Phosphorylation and dephosphorylation of glycogen phosphorylase: a prototype for reversible covalent enzyme modification. Curr Top Cell Regul 18:401-419, 1981
82. Gonzalez GA, Montminy MR: Cyclic AMP stimulates somatostatin gene transcription by phosphorylation of CREB at serine 133. Cell 59:675-680, 1989
83. Desvergne B, Michalik L, Wahli W: Transcriptional regulation of metabolism. Physiol Rev 86:465-514, 2006
84. Lin J, Handschin C, Spiegelman BM: Metabolic control through the PGC-1 family of transcription coactivators. Cell Metab 1:361-370, 2005
85. Yoon JC, Puigserver P, Chen G, Donovan J, Wu Z, Rhee J, Adelmant G, Stafford J, Kahn CR, Granner DK, Newgard CB, Spiegelman BM: Control of hepatic gluconeogenesis through the transcriptional coactivator PGC-1. Nature 413:131-138, 2001
86. Herzig S, Long F, Jhala US, Hedrick S, Quinn R, Bauer A, Rudolph D, Schutz G, Yoon C, Puigserver P, Spiegelman B, Montminy M: CREB regulates hepatic gluconeogenesis through the coactivator PGC-1. Nature 413:179-183, 2001
87. Koo SH, Flechner L, Qi L, Zhang X, Screaton RA, Jeffries S, Hedrick S, Xu W, Boussouar F, Brindle P, Takemori H, Montminy M: The CREB coactivator TORC2 is a key regulator of fasting glucose metabolism. Nature 437:1109-1111, 2005
88. Cheng A, Saltiel AR: More TORC for the gluconeogenic engine. Bioessays 28:231-234, 2006
89. Band GC, Jones CT: Functional activation by glucagon of glucose 6-phosphatase and gluconeogenesis in the perfused liver of the fetal guinea pig. FEBS Lett 119:190-194, 1980
90. Hornbuckle LA, Everett CA, Martin CC, Gustavson SS, Svitek CA, Oeser JK, Neal DW, Cherrington AD, O'Brien RM: Selective stimulation of G-6-Pase catalytic subunit but not G-6-P transporter gene expression by glucagon in vivo and cAMP in situ. Am J Physiol Endocrinol Metab 286:E795-808, 2004
91. Pilkis SJ, Claus TH, el-Maghrabi MR: The role of cyclic AMP in rapid and long-term regulation of gluconeogenesis and glycolysis. Adv Second Messenger Phosphoprotein Res 22:175-191, 1988

99
92. Pilkis SJ, Claus TH: Hepatic gluconeogenesis/glycolysis: regulation and structure/function relationships of substrate cycle enzymes. Annu Rev Nutr 11:465-515, 1991
93. Kurland IJ, Pilkis SJ: Covalent control of 6-phosphofructo-2-kinase/fructose-2,6-bisphosphatase: insights into autoregulation of a bifunctional enzyme. Protein Sci 4:1023-1037, 1995
94. Castano JG, Nieto A, Feliu JE: Inactivation of phosphofructokinase by glucagon in rat hepatocytes. J Biol Chem 254:5576-5579, 1979
95. Pilkis SJ, El-Maghrabi MR, McGrane M, Pilkis J, Claus TH: Regulation by glucagon of hepatic pyruvate kinase, 6-phosphofructo 1-kinase, and fructose-1,6-bisphosphatase. Fed Proc 41:2623-2628, 1982
96. Saltiel AR, Kahn CR: Insulin signalling and the regulation of glucose and lipid metabolism. Nature 414:799-806, 2001
97. Hother-Nielsen O, Henriksen JE, Holst JJ, Beck-Nielsen H: Effects of insulin on glucose turnover rates in vivo: isotope dilution versus constant specific activity technique. Metabolism 45:82-91, 1996
98. Granner DK, Sasaki K, Chu D: Multihormonal regulation of phosphoenolpyruvate carboxykinase gene transcription. The dominant role of insulin. Ann N Y Acad Sci 478:175-190, 1986
99. Hall RK, Wang XL, George L, Koch SR, Granner DK: Insulin represses phosphoenolpyruvate carboxykinase gene transcription by causing the rapid disruption of an active transcription complex: a potential epigenetic effect. Mol Endocrinol 21:550-563, 2007
100. Gastaldelli A, Toschi E, Pettiti M, Frascerra S, Quinones-Galvan A, Sironi AM, Natali A, Ferrannini E: Effect of physiological hyperinsulinemia on gluconeogenesis in nondiabetic subjects and in type 2 diabetic patients. Diabetes 50:1807-1812, 2001
101. Edgerton DS, Cardin S, Emshwiller M, Neal D, Chandramouli V, Schumann WC, Landau BR, Rossetti L, Cherrington AD: Small increases in insulin inhibit hepatic glucose production solely caused by an effect on glycogen metabolism. Diabetes 50:1872-1882, 2001
102. Prager R, Wallace P, Olefsky JM: Direct and indirect effects of insulin to inhibit hepatic glucose output in obese subjects. Diabetes 36:607-611, 1987

100
103. Ader M, Bergman RN: Peripheral effects of insulin dominate suppression of fasting hepatic glucose production. Am J Physiol 258:E1020-1032, 1990
104. Giacca A, Fisher SJ, Shi ZQ, Gupta R, Lickley HL, Vranic M: Importance of peripheral insulin levels for insulin-induced suppression of glucose production in depancreatized dogs. J Clin Invest 90:1769-1777, 1992
105. Sindelar DK, Balcom JH, Chu CA, Neal DW, Cherrington AD: A comparison of the effects of selective increases in peripheral or portal insulin on hepatic glucose production in the conscious dog. Diabetes 45:1594-1604, 1996
106. Sindelar DK, Chu CA, Rohlie M, Neal DW, Swift LL, Cherrington AD: The role of fatty acids in mediating the effects of peripheral insulin on hepatic glucose production in the conscious dog. Diabetes 46:187-196, 1997
107. Stagner JI, Samols E: Retrograde perfusion as a model for testing the relative effects of glucose versus insulin on the A cell. J Clin Invest 77:1034-1037, 1986
108. Franklin I, Gromada J, Gjinovci A, Theander S, Wollheim CB: Beta-cell secretory products activate alpha-cell ATP-dependent potassium channels to inhibit glucagon release. Diabetes 54:1808-1815, 2005
109. Khan FA, Goforth PB, Zhang M, Satin LS: Insulin activates ATP-sensitive K(+) channels in pancreatic beta-cells through a phosphatidylinositol 3-kinase-dependent pathway. Diabetes 50:2192-2198, 2001
110. Xu E, Kumar M, Zhang Y, Ju W, Obata T, Zhang N, Liu S, Wendt A, Deng S, Ebina Y, Wheeler MB, Braun M, Wang Q: Intra-islet insulin suppresses glucagon release via GABA-GABAA receptor system. Cell Metab 3:47-58, 2006
111. Davis SN, Colburn C, Dobbins R, Nadeau S, Neal D, Williams P, Cherrington AD: Evidence that the brain of the conscious dog is insulin sensitive. J Clin Invest 95:593-602, 1995
112. la Fleur SE, Kalsbeek A, Wortel J, Buijs RM: Polysynaptic neural pathways between the hypothalamus, including the suprachiasmatic nucleus, and the liver. Brain Res 871:50-56, 2000
113. Obici S, Zhang BB, Karkanias G, Rossetti L: Hypothalamic insulin signaling is required for inhibition of glucose production. Nat Med 8:1376-1382, 2002

101
114. Edgerton DS, Lautz M, Scott M, Everett CA, Stettler KM, Neal DW, Chu CA, Cherrington AD: Insulin's direct effects on the liver dominate the control of hepatic glucose production. J Clin Invest 116:521-527, 2006
115. Girard J: Insulin's effect on the liver: "direct or indirect?" continues to be the question. J Clin Invest 116:302-304, 2006
116. Cherrington AD, Moore MC, Sindelar DK, Edgerton DS: Insulin action on the liver in vivo. Biochem Soc Trans 35:1171-1174, 2007
117. Renne Emkey RCK: Molecular aspects of insulin signaling. In Handbook of Physiology L. Jefferson AC, Ed. New York, Oxford University Press, 2001, p. 413-433
118. Taniguchi CM, Emanuelli B, Kahn CR: Critical nodes in signalling pathways: insights into insulin action. Nat Rev Mol Cell Biol 7:85-96, 2006
119. Lizcano JM, Alessi DR: The insulin signalling pathway. Curr Biol 12:R236-238, 2002
120. Granner D, Andreone T, Sasaki K, Beale E: Inhibition of transcription of the phosphoenolpyruvate carboxykinase gene by insulin. Nature 305:549-551, 1983
121. Argaud D, Zhang Q, Pan W, Maitra S, Pilkis SJ, Lange AJ: Regulation of rat liver glucose-6-phosphatase gene expression in different nutritional and hormonal states: gene structure and 5'-flanking sequence. Diabetes 45:1563-1571, 1996
122. Schmoll D, Allan BB, Burchell A: Cloning and sequencing of the 5' region of the human glucose-6-phosphatase gene: transcriptional regulation by cAMP, insulin and glucocorticoids in H4IIE hepatoma cells. FEBS Lett 383:63-66, 1996
123. Barthel A, Schmoll D: Novel concepts in insulin regulation of hepatic gluconeogenesis. Am J Physiol Endocrinol Metab 285:E685-692, 2003
124. Dentin R, Liu Y, Koo SH, Hedrick S, Vargas T, Heredia J, Yates J, 3rd, Montminy M: Insulin modulates gluconeogenesis by inhibition of the coactivator TORC2. Nature 449:366-369, 2007
125. Conti M, Jin SL, Monaco L, Repaske DR, Swinnen JV: Hormonal regulation of cyclic nucleotide phosphodiesterases. Endocr Rev 12:218-234, 1991
126. Hermsdorf T, Dettmer D: Combined effects of insulin and dexamethasone on cyclic AMP phosphodiesterase 3 and glycogen metabolism in cultured rat hepatocytes. Cell Signal 10:629-635, 1998

102
127. Tang Y, Osawa H, Onuma H, Nishimiya T, Ochi M, Sugita A, Makino H: Phosphodiesterase 3B gene expression is enhanced in the liver but reduced in the adipose tissue of obese insulin resistant db/db mouse. Diabetes Res Clin Pract 54:145-155, 2001
128. Asnaghi L, Bruno P, Priulla M, Nicolin A: mTOR: a protein kinase switching between life and death. Pharmacol Res 50:545-549, 2004
129. Abumrad NN, Cherrington AD, Williams PE, Lacy WW, Rabin D: Absorption and disposition of a glucose load in the conscious dog. Am J Physiol 242:E398-406, 1982
130. Flakoll P JM, Cherrington AD: Physiological Action of Insulin. In Diabetes Mellitus D Leroith ST, J Olefsky, Ed., Lippencott Publishing Co, 2004, p. 165-181
131. Steiner KE, Williams PE, Lacy WW, Cherrington AD: Effects of insulin on glucagon-stimulated glucose production in the conscious dog. Metabolism 39:1325-1333, 1990
132. Goresky CA, Bach GG, Nadeau BE: Red cell carriage of label: its limiting effect on the exchange of materials in the liver. Circ Res 36:328-351, 1975
133. Kadish AH, Hall DA: A new method for the continuous monitoring of blood glucose by measurement of dissolved oxygen. Clin Chem 11:869-875, 1965
134. Smogyi M: Notes on sugar determination. J Biol Chem 195:19-23, 1952
135. Smogyi M: Determination of blood sugar. J Biol Chem 160:69-73, 1945
136. Nelson: A photometric adaptation of the Somogyi method for determination of glucose. J Biol Chem 153:375-380, 1944
137. Lloyd B, Burrin J, Smythe P, Alberti KG: Enzymic fluorometric continuous-flow assays for blood glucose, lactate, pyruvate, alanine, glycerol, and 3-hydroxybutyrate. Clin Chem 24:1724-1729, 1978
138. Wide L, Porath J.: Radioimmunoassay of proteins with the use of Sephadex-coupled antibodies. Biochim Biophys Acta 130:257-260, 1966
139. Morgan CR, Lazarow A: Immunoassay of insulin using a two-antibody system. Proc Soc Exp Biol Med 110:29-32, 1962
140. Ensinck JW: Immunoassays for glucagon. Handbook of Experimental Pharmacology:203-221, 1983

103
141. Foster LB, Dunn RT: Single-antibody technique for radioimmunoassay of cortisol in unextracted serum or plasma. Clin Chem 20:365-368, 1974
142. Goldstein DS, Feuerstein G, Izzo JL, Jr., Kopin IJ, Keiser HR: Validity and reliability of liquid chromatography with electrochemical detection for measuring plasma levels of norepinephrine and epinephrine in man. Life Sci 28:467-475, 1981
143. Anton AH, Sayre DF: A study of the factors affecting the aluminum oxide-trihydroxyindole procedure for the analysis of catecholamines. J Pharmacol Exp Ther 138:360-375, 1962
144. Leevy CM, Mendenhall CL, Lesko W, Howard MM: Estimation of hepatic blood flow with indocyanine green. J Clin Invest 41:1169-1179, 1962
145. Hendrick GK: Dissertation Nashville, 1986
146. Livak KJ, Schmittgen TD: Analysis of relative gene expression data using real-time quantitative PCR and the 2(-Delta Delta C(T)) Method. Methods 25:402-408, 2001
147. Ramnanan CJ, Storey KB: Glucose-6-phosphate dehydrogenase regulation during hypometabolism. Biochem Biophys Res Commun 339:7-16, 2006
148. Adkins-Marshall BA, Myers SR, Hendrick GK, Williams PE, Triebwasser K, Floyd B, Cherrington AD: Interaction between insulin and glucose-delivery route in regulation of net hepatic glucose uptake in conscious dogs. Diabetes 39:87-95, 1990
149. Wall JS, Steele R, De Bodo RC, Altszuler N: Effect of insulin on utilization and production of circulating glucose. Am J Physiol 189:43-50, 1957
150. Debodo RC, Steele R, Altszuler N, Dunn A, Bishop JS: On the Hormonal Regulation of Carbohydrate Metabolism; Studies with C14 Glucose. Recent Prog Horm Res 19:445-488, 1963
151. Mari A: Estimation of the rate of appearance in the non-steady state with a two-compartment model. Am J Physiol 263:E400-415, 1992
152. Dobbins RL, Davis SN, Neal DW, Cobelli C, Cherrington AD: Pulsatility does not alter the response to a physiological increment in glucagon in the conscious dog. Am J Physiol 266:E467-478, 1994
153. Mari A: On the calculation of glucose rate of disappearance in nonsteady state. Am J Physiol 266:E825-828, 1994

104
154. Steele R, Wall JS, De Bodo RC, Altszuler N: Measurement of size and turnover rate of body glucose pool by the isotope dilution method. Am J Physiol 187:15-24, 1956
155. Radziuk J, Norwich KH, Vranic M: Experimental validation of measurements of glucose turnover in nonsteady state. Am J Physiol 234:E84-93, 1978
156. Cowan JS, Hetenyi G, Jr.: Glucoregulatory responses in normal and diabetic dogs recorded by a new tracer method. Metabolism 20:360-372, 1971
157. Cobelli C, Mari A, Ferrannini E: Non-steady state: error analysis of Steele's model and developments for glucose kinetics. Am J Physiol 252:E679-689, 1987
158. Wolfe R: Radioactive and stable isotope trcaers in biomedicine. Wiley-Liss, 1992
159. Ekberg K, Landau BR, Wajngot A, Chandramouli V, Efendic S, Brunengraber H, Wahren J: Contributions by kidney and liver to glucose production in the postabsorptive state and after 60 h of fasting. Diabetes 48:292-298, 1999
160. Wahren J, Felig P, Ahlborg G, Jorfeldt L: Glucose metabolism during leg exercise in man. J Clin Invest 50:2715-2725, 1971
161. Edgerton DS, Cardin S, Neal D, Farmer B, Lautz M, Pan C, Cherrington AD: Effects of hyperglycemia on hepatic gluconeogenic flux during glycogen phosphorylase inhibition in the conscious dog. Am J Physiol Endocrinol Metab 286:E510-522, 2004
162. Moore MC, Pagliassotti MJ, Swift LL, Asher J, Murrell J, Neal D, Cherrington AD: Disposition of a mixed meal by the conscious dog. Am J Physiol 266:E666-675, 1994
163. Gerich JE: Control of glycaemia. Baillieres Clin Endocrinol Metab 7:551-586, 1993
164. Randle PJ: Regulatory interactions between lipids and carbohydrates: the glucose fatty acid cycle after 35 years. Diabetes Metab Rev 14:263-283, 1998
165. Jungermann K, Katz N: Functional specialization of different hepatocyte populations. Physiol Rev 69:708-764, 1989
166. Radziuk J, Pye S: Hepatic glucose uptake, gluconeogenesis and the regulation of glycogen synthesis. Diabetes Metab Res Rev 17:250-272, 2001
167. Cryer PE, Tse TF, Clutter WE, Shah SD: Roles of glucagon and epinephrine in hypoglycemic and nonhypoglycemic glucose counterregulation in humans. Am J Physiol 247:E198-205, 1984

105
168. Taborsky GJ, Jr., Ahren B, Havel PJ: Autonomic mediation of glucagon secretion during hypoglycemia: implications for impaired alpha-cell responses in type 1 diabetes. Diabetes 47:995-1005, 1998
169. Havel PJ, Parry SJ, Stern JS, Akpan JO, Gingerich RL, Taborsky GJ, Jr., Curry DL: Redundant parasympathetic and sympathoadrenal mediation of increased glucagon secretion during insulin-induced hypoglycemia in conscious rats. Metabolism 43:860-866, 1994
170. Roach PJ SA, Harris RA: Regulation of glycogen metabolism. In Handbook of Physiology: The Endocrine Pancreas and Regulation of Metabolism Jefferson L CA, Ed. New York, Oxford University, 2001, p. 735-757
171. Shiota M, Green R, Colburn CA, Mitchell G, Cherrington AD: Inability of hyperglycemia to counter the ability of glucagon to increase net glucose output and activate glycogen phosphorylase in the perfused rat liver. Metabolism 45:481-485, 1996
172. De Feo P, Perriello G, Torlone E, Ventura MM, Fanelli C, Santeusanio F, Brunetti P, Gerich JE, Bolli GB: Contribution of cortisol to glucose counterregulation in humans. Am J Physiol 257:E35-42, 1989
173. Eigler N, Sacca L, Sherwin RS: Synergistic interactions of physiologic increments of glucagon, epinephrine, and cortisol in the dog: a model for stress-induced hyperglycemia. J Clin Invest 63:114-123, 1979
174. Shamoon H, Hendler R, Sherwin RS: Synergistic interactions among antiinsulin hormones in the pathogenesis of stress hyperglycemia in humans. J Clin Endocrinol Metab 52:1235-1241, 1981
175. Lecavalier L, Bolli G, Gerich J: Glucagon-cortisol interactions on glucose turnover and lactate gluconeogenesis in normal humans. Am J Physiol 258:E569-575, 1990
176. Gustavson SM, Chu CA, Nishizawa M, Farmer B, Neal D, Yang Y, Donahue EP, Flakoll P, Cherrington AD: Interaction of glucagon and epinephrine in the control of hepatic glucose production in the conscious dog. Am J Physiol Endocrinol Metab 284:E695-707, 2003
177. Cross DA, Alessi DR, Cohen P, Andjelkovich M, Hemmings BA: Inhibition of glycogen synthase kinase-3 by insulin mediated by protein kinase B. Nature 378:785-789, 1995
178. Hall RK, Yamasaki T, Kucera T, Waltner-Law M, O'Brien R, Granner DK: Regulation of phosphoenolpyruvate carboxykinase and insulin-like growth factor-binding

106
protein-1 gene expression by insulin. The role of winged helix/forkhead proteins. J Biol Chem 275:30169-30175, 2000
179. Nakae J, Kitamura T, Silver DL, Accili D: The forkhead transcription factor Foxo1 (Fkhr) confers insulin sensitivity onto glucose-6-phosphatase expression. J Clin Invest 108:1359-1367, 2001
180. Puigserver P, Rhee J, Donovan J, Walkey CJ, Yoon JC, Oriente F, Kitamura Y, Altomonte J, Dong H, Accili D, Spiegelman BM: Insulin-regulated hepatic gluconeogenesis through FOXO1-PGC-1alpha interaction. Nature 423:550-555, 2003
181. Schilling MM, Oeser JK, Boustead JN, Flemming BP, O'Brien RM: Gluconeogenesis: re-evaluating the FOXO1-PGC-1alpha connection. Nature 443:E10-11, 2006
182. Matsumoto M, Pocai A, Rossetti L, Depinho RA, Accili D: Impaired regulation of hepatic glucose production in mice lacking the forkhead transcription factor Foxo1 in liver. Cell Metab 6:208-216, 2007
183. Burgess SC, He T, Yan Z, Lindner J, Sherry AD, Malloy CR, Browning JD, Magnuson MA: Cytosolic phosphoenolpyruvate carboxykinase does not solely control the rate of hepatic gluconeogenesis in the intact mouse liver. Cell Metab 5:313-320, 2007
Related Documents