Chapter 28 Chapter 28 Nursing Management Nursing Management Lower Respiratory Problems Lower Respiratory Problems Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.

Chapter 28 Nursing Management Lower Respiratory Problems Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
Dec 25, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Chapter 28Chapter 28
Nursing ManagementNursing ManagementLower Respiratory ProblemsLower Respiratory Problems
Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.

Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
Chapter 28Chapter 28 1. Describe the pathophysiology, types, clinical manifestations, and collaborative care of 1. Describe the pathophysiology, types, clinical manifestations, and collaborative care of
pneumonia. pneumonia. 2. Explain the nursing management of the patient with pneumonia. 2. Explain the nursing management of the patient with pneumonia. 3. Describe the pathogenesis, classification, clinical manifestations, complications, 3. Describe the pathogenesis, classification, clinical manifestations, complications, diagnostic abnormalities, and nursing and collaborative management of tuberculosis. diagnostic abnormalities, and nursing and collaborative management of tuberculosis. 4. Identify the causes, clinical manifestations, and nursing and collaborative management 4. Identify the causes, clinical manifestations, and nursing and collaborative management of pulmonary fungal infections. (PC 1, 2, 3, 5, 6; MC 1, MP 3)of pulmonary fungal infections. (PC 1, 2, 3, 5, 6; MC 1, MP 3) 5. Explain the pathophysiology, clinical manifestations, and nursing and collaborative 5. Explain the pathophysiology, clinical manifestations, and nursing and collaborative management of lung abscesses. management of lung abscesses. 6. Identify the causative factors, clinical features, and management of environmental lung 6. Identify the causative factors, clinical features, and management of environmental lung diseases. diseases. 7. Describe the causes, risk factors, pathogenesis, clinical manifestations, and nursing and 7. Describe the causes, risk factors, pathogenesis, clinical manifestations, and nursing and collaborative management of lung cancer. collaborative management of lung cancer. 8. Identify the mechanisms involved and the clinical manifestations of pneumothorax, 8. Identify the mechanisms involved and the clinical manifestations of pneumothorax, fractured ribs, and flail chest. fractured ribs, and flail chest. 9. Describe the purpose, methods, and nursing responsibilities related to chest tubes. 9. Describe the purpose, methods, and nursing responsibilities related to chest tubes. 10. Explain the types of chest surgery and appropriate preoperative and postoperative care. 10. Explain the types of chest surgery and appropriate preoperative and postoperative care. 11. Compare and contrast extrapulmonary and intrapulmonary restrictive lung disorders in 11. Compare and contrast extrapulmonary and intrapulmonary restrictive lung disorders in terms of causes, clinical manifestations, and collaborative management. terms of causes, clinical manifestations, and collaborative management. 12. Describe the pathophysiology, clinical manifestations, and management of pulmonary 12. Describe the pathophysiology, clinical manifestations, and management of pulmonary embolism, pulmonary hypertension, and cor pulmonale. embolism, pulmonary hypertension, and cor pulmonale.
13. Discuss the use of lung transplantation as a treatment for pulmonary disorders. 13. Discuss the use of lung transplantation as a treatment for pulmonary disorders.
Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
Acute BronchitisAcute Bronchitis
Inflammation of the BronchiInflammation of the Bronchi Most commonly viral infectionsMost commonly viral infections
Can be bacterialCan be bacterial Most commonly bacterial with smokersMost commonly bacterial with smokers
Symptoms include:Symptoms include: Cough, low grade fever, tachypnea, tachycardiaCough, low grade fever, tachypnea, tachycardia Some wheezing or rhonchiSome wheezing or rhonchi
Nursing management:Nursing management: Medications, testing, supportive careMedications, testing, supportive care
Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
PneumoniaPneumonia
EtiologyEtiology Normal defense mechanismsNormal defense mechanisms Factors predisposing to pneumoniaFactors predisposing to pneumonia Acquisition of organismsAcquisition of organisms
Types of pneumoniaTypes of pneumonia Community-acquired pneumoniaCommunity-acquired pneumonia Hospital-acquired, ventilator-associated, and health care–Hospital-acquired, ventilator-associated, and health care–
associated pneumoniaassociated pneumonia Fungal pneumoniaFungal pneumonia Aspiration pneumoniaAspiration pneumonia Opportunistic pneumoniaOpportunistic pneumonia
Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
Pneumonia (cont'd)Pneumonia (cont'd)
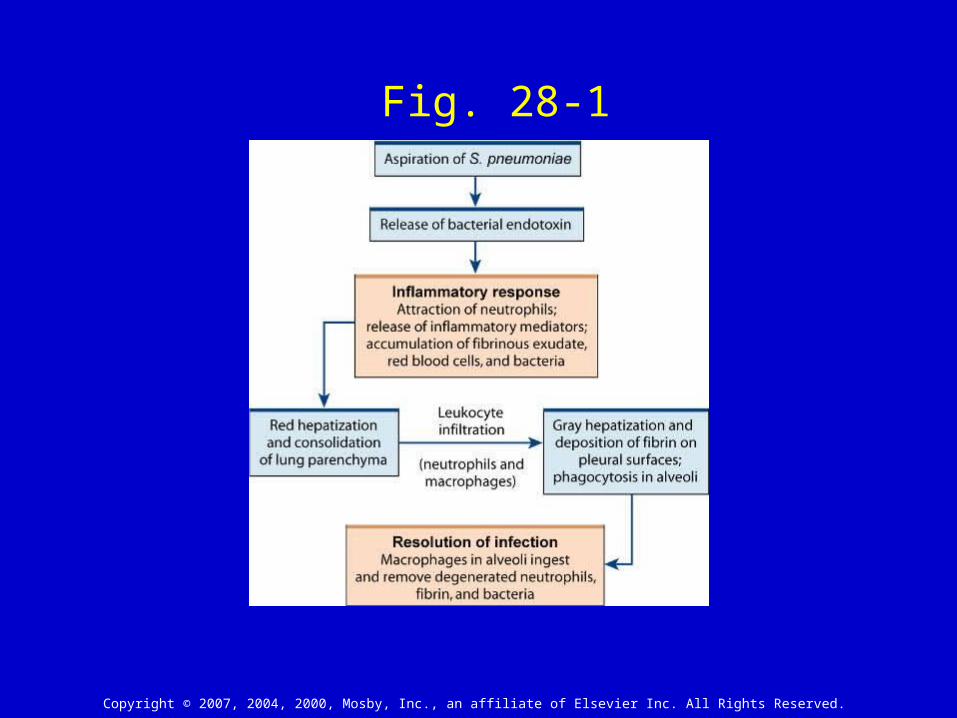
PathophysiologyPathophysiology Pulmonary congestion- bacterial Pulmonary congestion- bacterial
invasioninvasion Immune responseImmune response ResolutionResolution
Clinical manifestationsClinical manifestations Often rapid onsetOften rapid onset Fever, chills, shakingFever, chills, shaking Shortness of breath, cough, chest painShortness of breath, cough, chest pain Breath soundsBreath sounds
Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
Fig. 28-1
Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
Pneumonia (cont'd)Pneumonia (cont'd) ComplicationsComplications
Pleurisy, pleural effusion, atalectasis, lung abscess, Pleurisy, pleural effusion, atalectasis, lung abscess, empyemaempyema
Bacteremia, pericarditis, meningitis, endocarditisBacteremia, pericarditis, meningitis, endocarditis Diagnostic studiesDiagnostic studies
CXR, Sputum culture, Blood culturesCXR, Sputum culture, Blood cultures Collaborative careCollaborative care
Pneumococcal vaccine- high risk should receive every 5 Pneumococcal vaccine- high risk should receive every 5 yearsyears
Drug therapy- Must initiate antibiotic therapy within 4 hours Drug therapy- Must initiate antibiotic therapy within 4 hours of arrival to the hospital, oxygen, bronchodilatorsof arrival to the hospital, oxygen, bronchodilators
Nutritional therapy- Increase fluid intake, small frequent Nutritional therapy- Increase fluid intake, small frequent mealsmeals
Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
Nursing Management PneumoniaNursing Management Pneumonia
Nursing assessment-color, resp. Nursing assessment-color, resp. rate, work of breathing, lung rate, work of breathing, lung soundssounds
Nursing diagnoses- see figure 28-Nursing diagnoses- see figure 28-1 (pg 568)1 (pg 568)
PlanningPlanning
Nursing implementationNursing implementation
Health promotionHealth promotion
Acute interventionAcute intervention
Ambulatory and home careAmbulatory and home care
EvaluationEvaluation
Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
TuberculosisTuberculosis Infectious disease caused by Infectious disease caused by
Mycobacterium TuberculosisMycobacterium Tuberculosis 2 million die worldwide annually (14,000 2 million die worldwide annually (14,000
cases in the U.S. diagnosed)cases in the U.S. diagnosed) Lungs most common infection site but also Lungs most common infection site but also
may infect:may infect: Nervous systemNervous system KidneysKidneys AdrenalsAdrenals Lymph nodesLymph nodes Genital tractGenital tract
People @ riskPeople @ risk PoorPoor HomelessHomeless Foreign bornForeign born InstitutionalizedInstitutionalized ImmunosuppressedImmunosuppressed HIVHIV
Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
Tuberculosis (cont'd)Tuberculosis (cont'd)
Diagnostic studiesDiagnostic studies TB skin testTB skin test Chest x-rayChest x-ray Bacteriologic and other studiesBacteriologic and other studies
Collaborative careCollaborative care Drug therapyDrug therapy
• Active diseaseActive disease• Latent tuberculosis infectionLatent tuberculosis infection• VaccineVaccine
Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
Nursing ManagementNursing ManagementTuberculosisTuberculosis
Nursing assessmentNursing assessment
Nursing diagnosesNursing diagnoses
PlanningPlanning
Nursing implementationNursing implementation
Health promotionHealth promotion
Acute interventionAcute intervention
Ambulatory and home careAmbulatory and home care
EvaluationEvaluation
Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
Atypical MycobacteriaAtypical Mycobacteria
Similar to TB in clinical presentationSimilar to TB in clinical presentation
Only differentiated by CultureOnly differentiated by Culture
Treatment with similar drugsTreatment with similar drugs
Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
Pulmonary Fungal InfectionsPulmonary Fungal Infections
immunocompromised patientsimmunocompromised patients
Cultures/biopsy to identify Cultures/biopsy to identify
s/sx similar to bacterial pneumonias/sx similar to bacterial pneumonia
Antifungal medications: monitor for Antifungal medications: monitor for side effects including renal/hepatic side effects including renal/hepatic
toxicitytoxicity
Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
Lung AbscessLung Abscess
Most commonly associated with aspirationMost commonly associated with aspiration
Cavity is formedCavity is formed
Diagnosed with CXR or CTDiagnosed with CXR or CT
Requires long term antibiotic therapyRequires long term antibiotic therapy
May require surgery or chest tube drainageMay require surgery or chest tube drainage
Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
Environmental Lung DiseasesEnvironmental Lung Diseases
Pneumoconiosis, chemical Pneumoconiosis, chemical pneumonitis, pneumonitis, hypersensitivity hypersensitivity pneumonitispneumonitis
Clinical manifestationsClinical manifestations Symptoms may not develop Symptoms may not develop
for >10 yearsfor >10 years FibrosisFibrosis
Collaborative careCollaborative care
Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
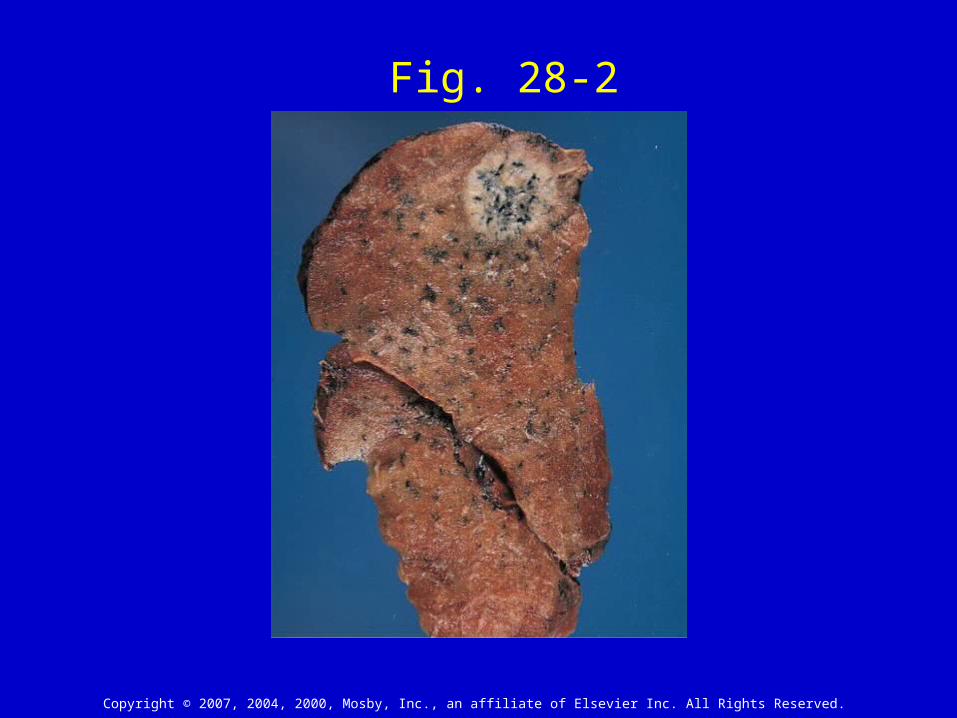
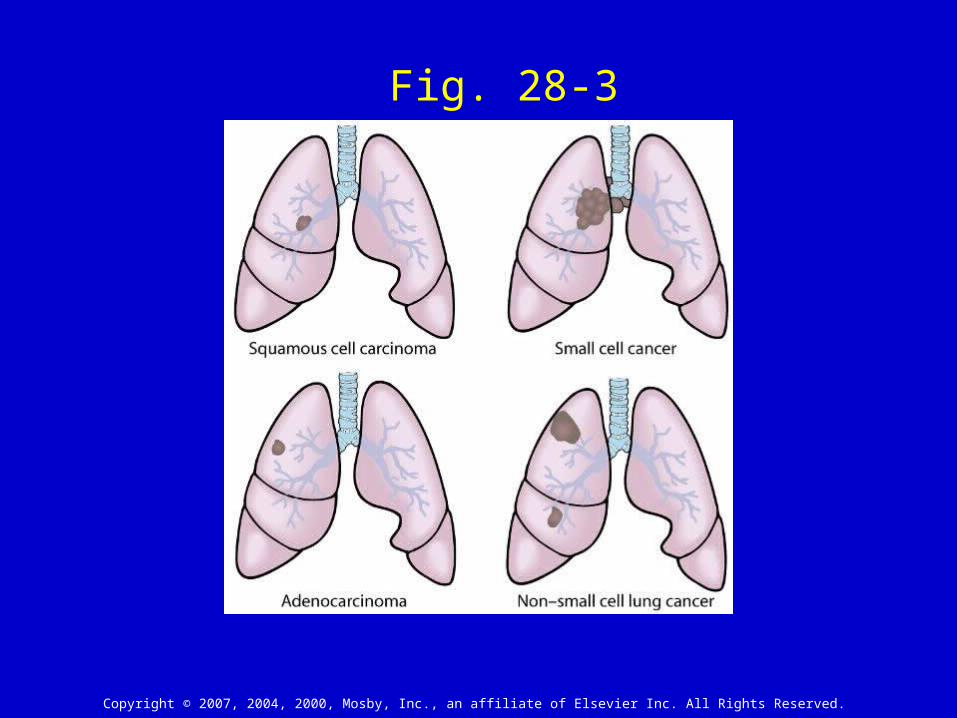
Lung CancerLung Cancer
SmokingSmoking 80-90% of all cancers80-90% of all cancers Risk declines gradually Risk declines gradually
after cessationafter cessation 22ndnd Hand smoke Hand smoke
increases risk by 35%increases risk by 35% Pipe and cigar smoke still Pipe and cigar smoke still
increase riskincrease risk
Clinical ManifestationsClinical Manifestations Tumor may grow for 8-10 Tumor may grow for 8-10
years before visible on years before visible on CXR (1cm mass is CXR (1cm mass is smallest that is seen on smallest that is seen on CXR)CXR)
Persistent cough, Persistent cough, hoarsenesshoarseness
May have fever chillsMay have fever chills Weight loss, fatigue, Weight loss, fatigue,
nausea, vomiting nausea, vomiting
Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
Fig. 28-2
Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
Fig. 28-3
Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
Lung Cancer (cont'd)Lung Cancer (cont'd)
Collaborative careCollaborative care Surgical therapy- treatment of Surgical therapy- treatment of
choice for stage I & IIchoice for stage I & II Radiation therapy- curative as Radiation therapy- curative as
well as adjunct therapy, palliative well as adjunct therapy, palliative carecare
Chemotherapy- usually adjunct Chemotherapy- usually adjunct therapytherapy
Biologic and targeted therapyBiologic and targeted therapy

Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
Lung Cancer (cont'd)Lung Cancer (cont'd)
Collaborative care (cont'd)Collaborative care (cont'd) Other therapiesOther therapies
• Prophylactic cranial radiationProphylactic cranial radiation
• Bronchoscopic laser therapyBronchoscopic laser therapy
• Photodynamic therapyPhotodynamic therapy
• Airway stentingAirway stenting
• CryotherapyCryotherapy
Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
Nursing Management Nursing Management Lung CancerLung Cancer
Nursing assessment (pg. 583)Nursing assessment (pg. 583)
Nursing diagnoses (pg. 583)Nursing diagnoses (pg. 583)
PlanningPlanning
Nursing implementationNursing implementation
Health promotionHealth promotion
Acute interventionAcute intervention
Ambulatory and home careAmbulatory and home care
EvaluationEvaluation
Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
Chest Trauma Chest Trauma and Thoracic Injuriesand Thoracic Injuries
Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
PneumothoraxPneumothorax
Types of pneumothoraxTypes of pneumothorax Closed pneumothoraxClosed pneumothorax Open pneumothoraxOpen pneumothorax Tension pneumothoraxTension pneumothorax HemothoraxHemothorax ChylothoraxChylothorax
Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
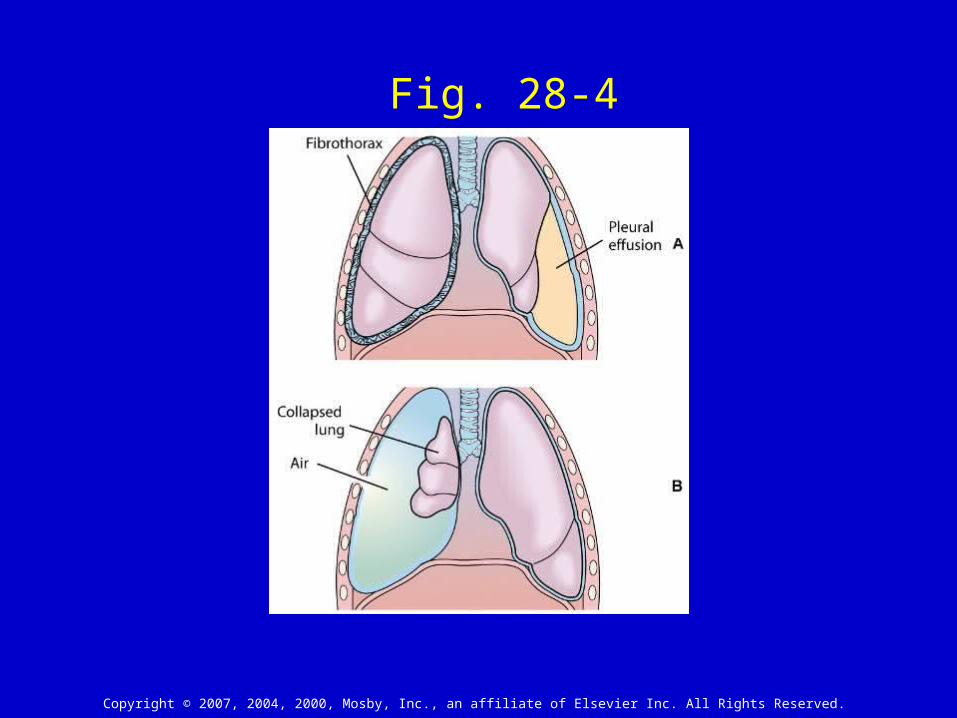
Fig. 28-4
Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
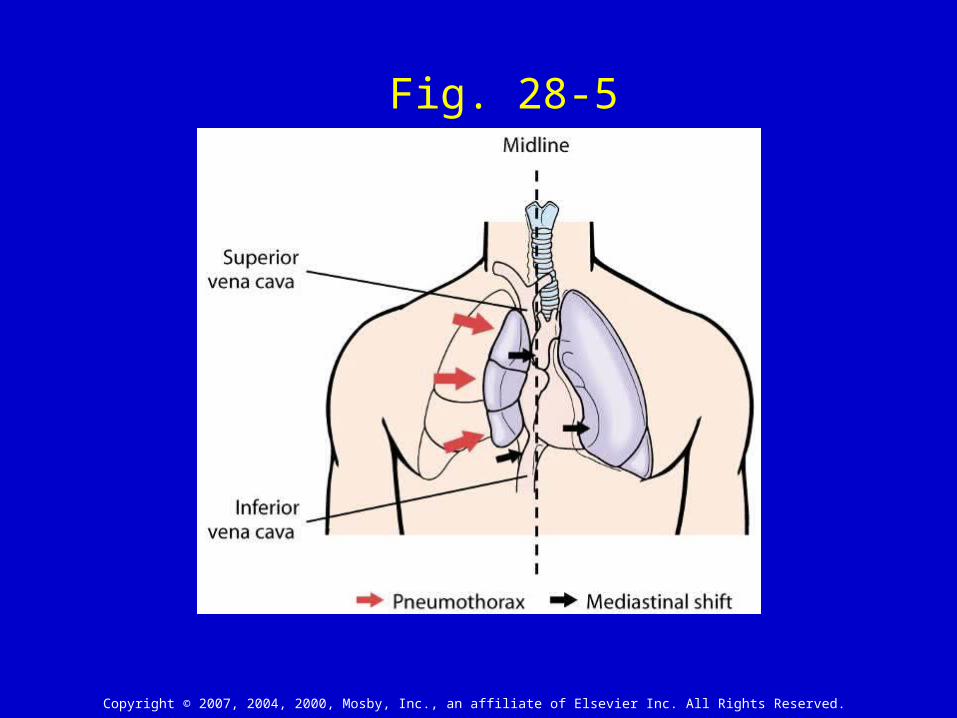
Fig. 28-5

Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
Fractured RibsFractured Ribsand Flail Chestand Flail Chest
Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
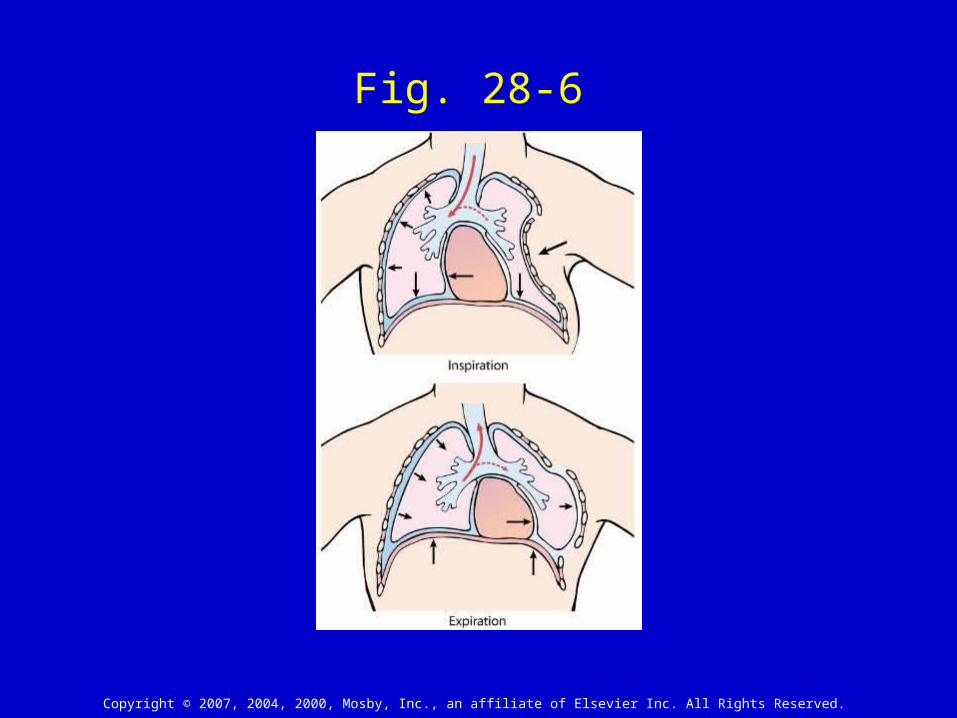
Fig. 28-6
Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
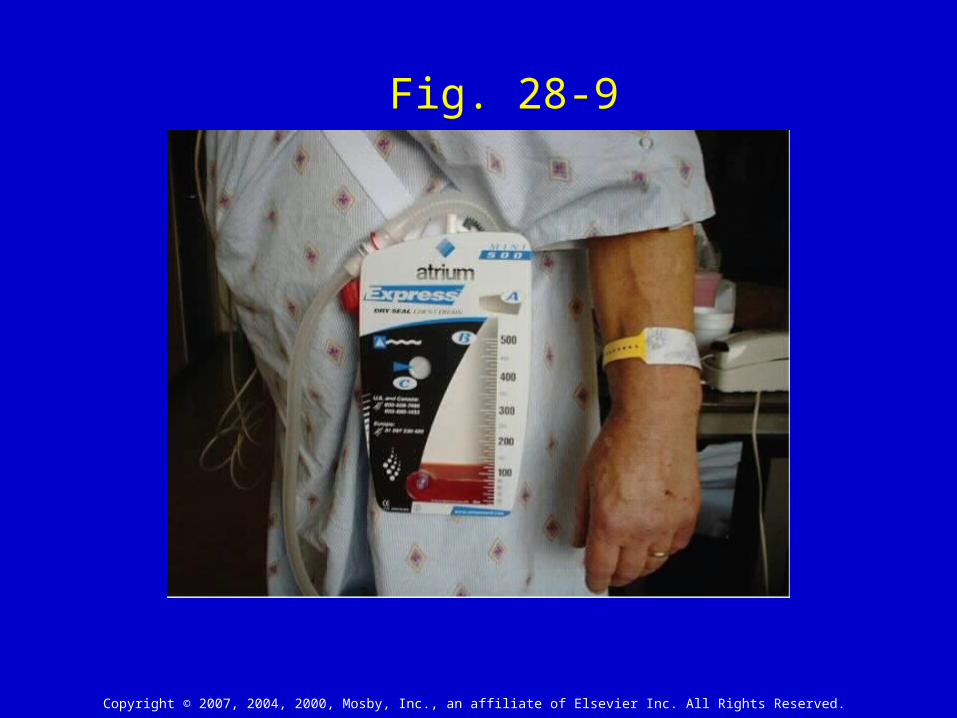
Chest Tubes and Pleural DrainageChest Tubes and Pleural Drainage
Chest tube insertionChest tube insertion
Pleural drainagePleural drainage Heimlich valvesHeimlich valves Small chest tubesSmall chest tubes
Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
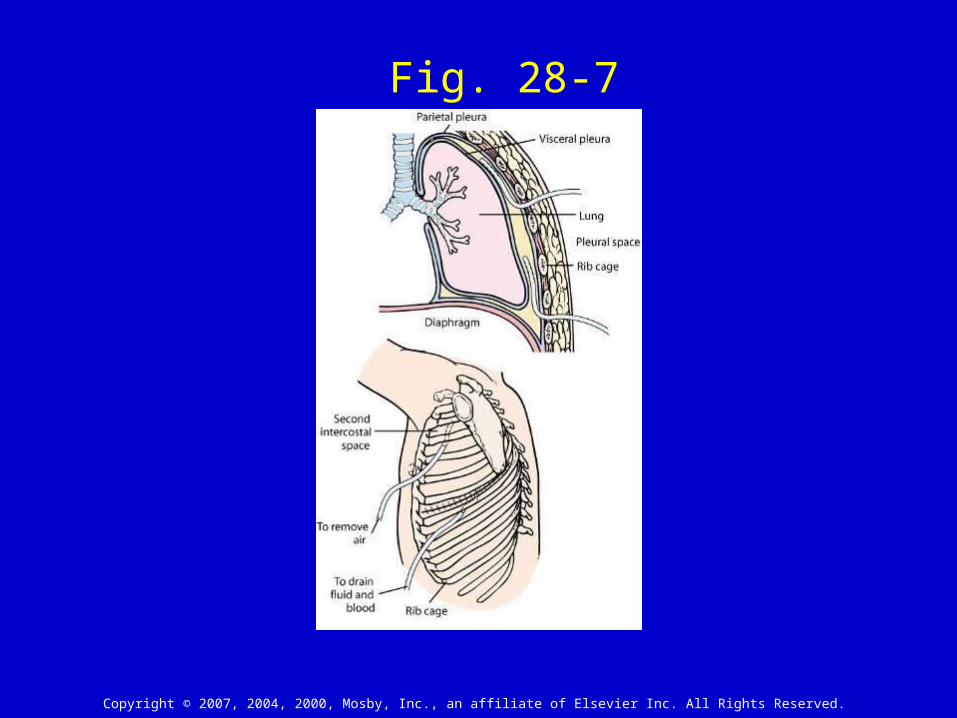
Fig. 28-7
Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
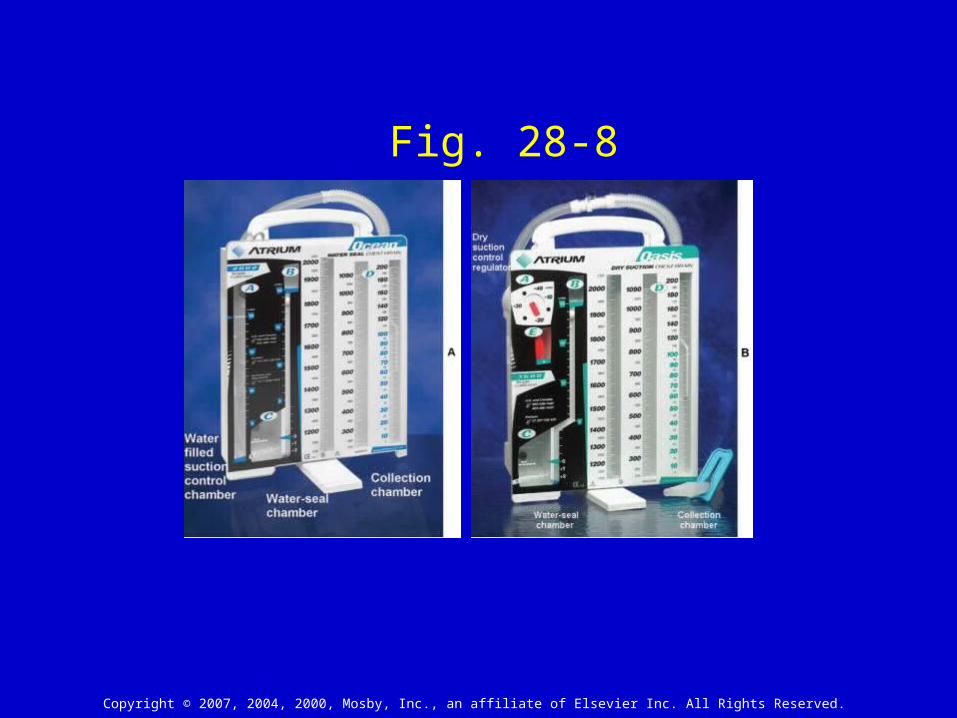
Fig. 28-8
Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
Fig. 28-9
Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
Nursing Management Chest DrainageNursing Management Chest Drainage
ComplicationsComplications
Chest tube removalChest tube removal
Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
Chest SurgeryChest Surgery
Preoperative carePreoperative care Surgical therapySurgical therapy
Video-assisted thoracic surgery (VATS)Video-assisted thoracic surgery (VATS) Postoperative carePostoperative care
Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
Restrictive Respiratory DisordersRestrictive Respiratory Disorders
Pleural effusionPleural effusion PleurisyPleurisy AtelectasisAtelectasis Interstitial Lung DiseaseInterstitial Lung Disease Idiopathic Pulmonary FibrosisIdiopathic Pulmonary Fibrosis SarcoidosisSarcoidosis
Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
Vascular Lung DisordersVascular Lung Disorders
Pulmonary EdemaPulmonary Edema Pulmonary EmbolismPulmonary Embolism Pulmonary HypertensionPulmonary Hypertension Cor PulmonaleCor Pulmonale
Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
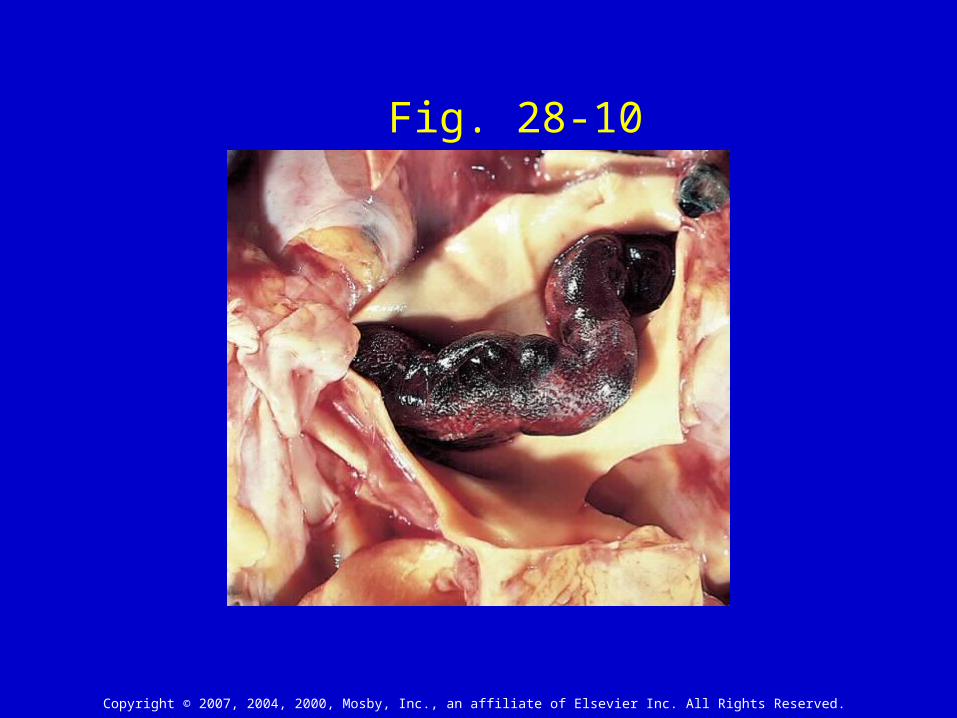
Fig. 28-10
Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
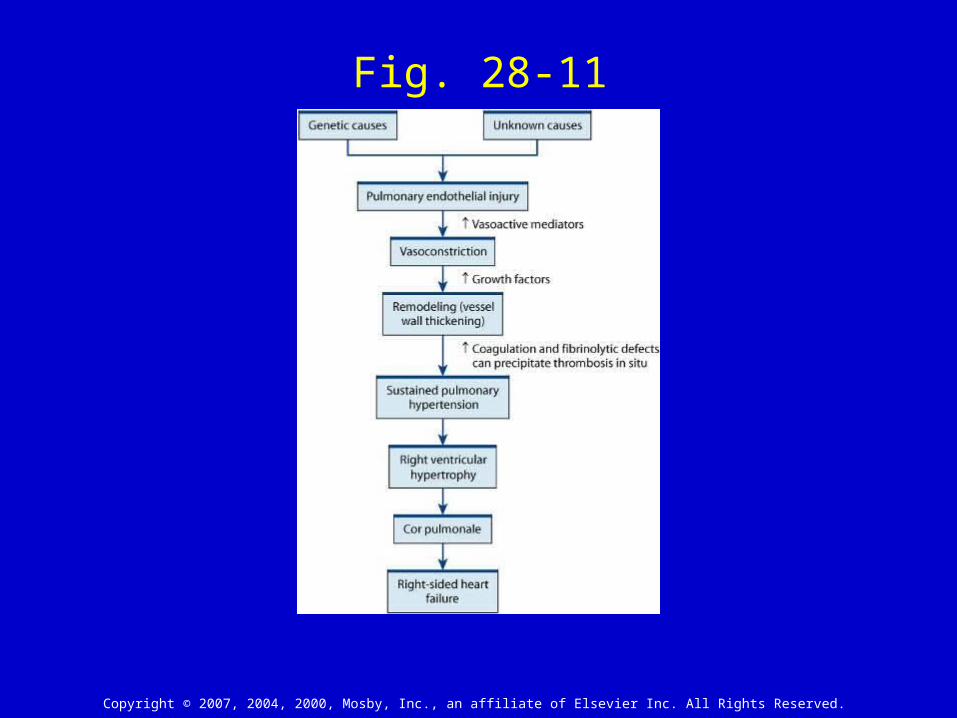
Fig. 28-11

Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
Fig. 28-12
Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
Lung TransplantationLung Transplantation
Patient must pass extensive evaluation Patient must pass extensive evaluation including psychological evaluationincluding psychological evaluation
Lifelong immunosuppressive therapyLifelong immunosuppressive therapy High risk for infectionsHigh risk for infections Acute rejection usually occurs 5-7 days after Acute rejection usually occurs 5-7 days after
transplanttransplant
Related Documents