1 Human Anatomy, Second Edition McKinley & O'Loughlin Chapter 22 Lecture Outline: Heart

Chapter 22, sp 10
May 11, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
Human Anatomy, Second Edition
McKinley & O'Loughlin
Chapter 22 Lecture Outline: Heart

22-2
Overview of the Cardiovascular System The pump, the heart, connects to blood vessels that
transport blood between the heart and other body tissues. arteries carry blood away from the
heart high in oxygen except for the pulmonary
arteries veins carry blood back to the heart
low in oxygen (except for the pulmonary veins)
The arteries and veins entering and leaving the heart are called the great vessels.

22-3
Overview of the Cardiovascular System
There is a unidirectional flow of blood through both the heart and the blood vessels.
Acts like two independent, side-by-side pumps that work independently but at the same rate.
one directs blood to the lungs for gas exchange the other directs blood to body tissues for
nutrient delivery Alternate cycles of heart wall contraction (systole)
and relaxation (diastole) develop blood pressure. Minimum blood pressure is essential to push blood
through blood vessels to the body tissues for nutrient and waste exchange.

22-4
Pulmonary and Systemic Circuits The pulmonary circuit consists of the chambers on
the right side of the heart (right atrium and ventricle) as well as the pulmonary arteries and veins.
conveys blood to the lungs via pulmonary arteries to reduce carbon dioxide and replenish oxygen levels in the blood before returning to the heart in pulmonary veins
Blood returns to the left side of the heart, where it then enters the systemic circuit.
The systemic circuit consists of the chambers on the left side of the heart (left atrium and ventricle), along with all the other named blood vessels.
carries blood to all the peripheral organs and tissues of the body

22-5
Pulmonary and Systemic Circuits Oxygenated blood from the left side of the heart is
pumped into the aorta, the largest systemic artery in the body, and then into smaller systemic arteries.
Gas exchange in tissues occurs in capillaries. Systemic veins then carry deoxygenated blood
(high in carbon dioxide) and waste products. Most veins merge and drain into the superior
and inferior venae cavae, which drain blood into the right atrium.
There, the blood enters the pulmonary circuit, and the cycle repeats.

6

22-7
Postition of the Heart Approximately the size of a fist (about 250 to
350 g) Located left of the midline posterior to the
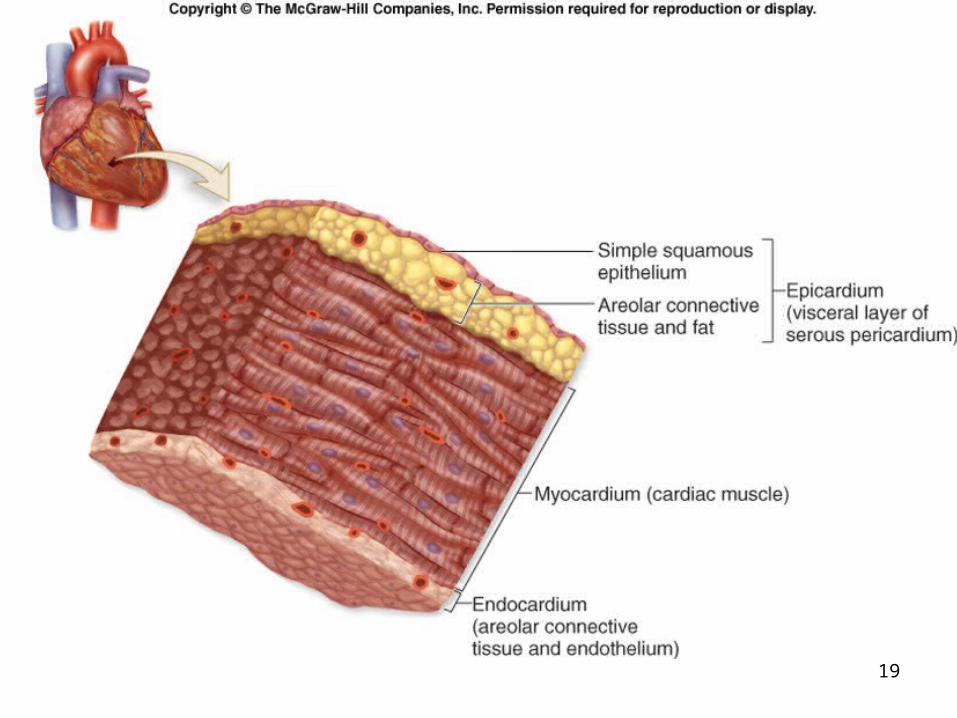
sternum in the middle mediastinum. Rotated such that the right atrium and
ventricle are located more anteriorly, while the left atrium and ventricle are located more posteriorly.
CPR - heart between the sternum and the vertebrae - allows compression
22-8
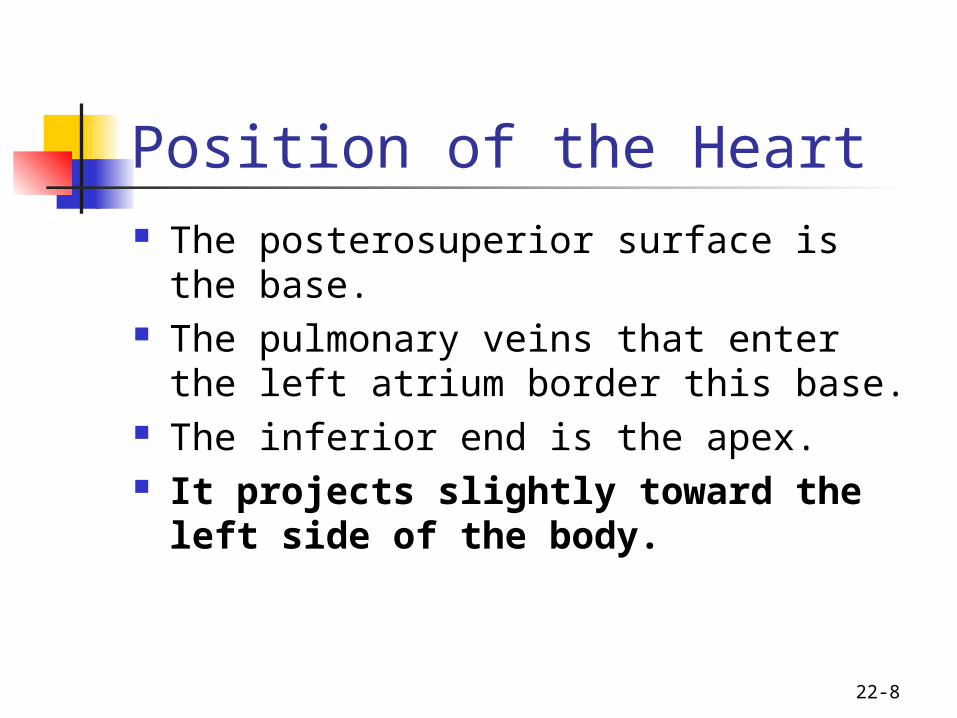
Position of the Heart The posterosuperior surface is the base. The pulmonary veins that enter the left
atrium border this base. The inferior end is the apex. It projects slightly toward the left
side of the body.

9
10

11

12

22-13
Characteristics of the Pericardium The heart is in a fibrous, serous sac held in place within
the mediastinum by connective tissue that supports the great vessels’ external walls superior to the heart and the diaphragm inferior to it.
Restricts heart movements and prevents the heart from overfilling with blood.
Outer portion is a tough, dense connective tissue layer called the fibrous pericardium.
attached to both the sternum and the diaphragm Inner portion is a thin, double-layered serous membrane
called the serous pericardium. parietal layer (fused to fibrous pericardium) visceral layer (epicardium) produces serous fluid

14

22-15
Pericarditis Inflammation of the pericardium Possible causes: viruses, bacteria, or fungi Blood vessels become leaky and blood
accumulates in the pericardial cavity Severe case: cardiac tamponade can
lead to heart failure (drain with a needle) Piercing pain-not crushing pain of heart
attack Also friction rub in pericarditis helps to
distinguish the two

22-16
Anatomy of the Heart

22-17
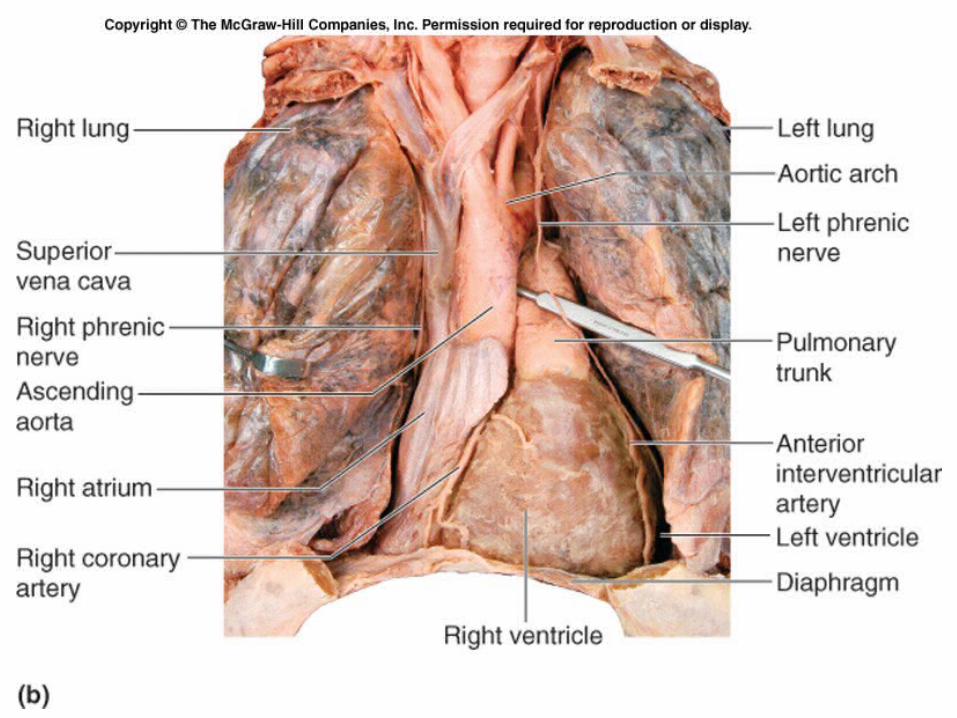
Heart Wall Structure Three distinctive layers:
external epicardium middle myocardium internal endocardium
Epicardium, the outermost heart layer, is also known as the visceral layer of serous pericardium.
As we age, the epicardium becomes thicker and more fatty.

22-18
Heart Wall Structure Myocardium, the middle layer, is
composed chiefly of cardiac muscle tissue and is the thickest layer.
Internal surface of the heart and the external surfaces of the heart valves are covered by a thin endothelium called the endocardium.
19

22-20
External Heart Anatomy Four hollow chambers: two smaller atria and two
larger ventricles. Atria are thin-walled chambers that are located
superiorly. anterior part of each atrium is a wrinkled,
flaplike extension called an auricle Atria receive blood returning to the heart
through both circulatory circuits. right atrium receives blood from the systemic
circuit left atrium receives blood from the pulmonary
circuit

22-21
External Heart Anatomy Blood that enters an atrium is passed to the
ventricle on the same side of the heart. Ventricles are the inferior chambers. Two large arteries, the pulmonary
trunk and the aorta exit the heart at the basal surface.
The pulmonary trunk carries blood from the right ventricle into the pulmonary circuit.
The aorta conducts blood from the left ventricle into the systemic circuit.

22-22
External Heart Anatomy Atria are separated from the ventricles
externally by a relatively deep coronary sulcus (or atrioventricular sulcus) around the circumference of the heart.
The anterior interventricular sulcus and the posterior interventricular sulcus are located between the left and right ventricles on the surfaces of the heart.
These sulci extend toward the heart apex.

23

24

25

26

22-27
Internal Heart Anatomy: Chambers and Valves There are four heart chambers: each plays
a role in the continuous process of blood circulation.
Valves permit the passage of blood in one direction and prevent its backflow.

28

29
22-30
Fibrous Skeleton Dense irregular connective tissue.
separates the atria and ventricles anchors heart valves by forming supportive
rings (like handcuffs) at their attachment points and prevents overdilation of valve openings
provides electrical insulation between atria and ventricles
and thus prevents all of the heart chambers from beating at the same time
Provides a rigid framework for the attachment of cardiac muscle tissue.

31

22-32
Right Atrium Receives venous blood from the systemic circuit
and the heart muscle itself. Three major vessels empty into the right atrium.
superior vena cava drains blood from the head, upper limbs, and superior regions of the trunk
inferior vena cava drains blood from the lower limbs and trunk
coronary sinus drains blood from the heart wall The interatrial septum forms a wall between the
right and left atria. Fossa ovalis in the wall was the foramen ovale
before birth Has pectinate muscles

22-33
Separates the right atrium from the right ventricle.
Also called the tricuspid valve. has three triangular flaps
Venous blood flows from the right atrium, through the valve into the right ventricle.
It is forced closed when the right ventricle begins to contract, preventing blood backflow into the right atrium.
Right A-V Valve
22-34
Right Ventricle Receives deoxygenated venous blood from the right
atrium. An interventricular septum separates the right and
left ventricles. The internal wall surface of each ventricle has cone-
shaped, muscular projections called papillary muscles, which: anchor chordae tendineae
attach to the cusp of the right AV valve and prevent everting and flipping into the atrium when contracting
Trabeculae carneae are muscular ridges in both ventricles

22-35
Right Ventricle The pulmonary semilunar valve marks the
end of the right ventricle and the entrance into the pulmonary trunk.
Pulmonary trunk divides shortly into right and left pulmonary arteries. carry deoxygenated blood to the lungs
Between the pulmonary trunk and the aorta is the ligamentum arteriosum. Before birth, it was the ductus arteriosus, a bypass of the lungs and the left side of the heart.

22-36
Right Ventricle: Pulmonary Semilunar Valve Within the walls of the ventricles immediately
before the connection of the ventricle to the pulmonary trunk and aorta.
Composed of three thin, pocketlike semilunar cusps. As blood is pumped into the arterial trunks, it
pushes against the cusps, forcing the valves open. When ventricular contraction ceases, blood enters
the pockets of the semilunar valves between the cusp and the chamber wall. causes the cusps to “inflate” and meet at the
artery center, effectively blocking blood backflow

22-37
Left Atrium Once gas exchange occurs in the lungs,
the oxygenated blood travels through the pulmonary veins to the left atrium.
Smooth posterior wall of the left atrium contains openings for four pulmonary veins.

22-38
Left A-V Valve Separates the left atrium from the left
ventricle. Also called the bicuspid valve or the mitral
valve. Left AV valve has chordae tendineae similar to
those of the right AV valve. Oxygenated blood flows from the left atrium
into the left ventricle. It is forced closed when the left ventricle
begins to contract prevents blood backflow into the left atrium

22-39
Left Ventricle Largest of the four heart chambers. Wall is typically three times thicker than
the right ventricular wall. Requires thick walls in order to
generate enough pressure to force the oxygenated blood from the lungs into the aorta and then through the entire systemic circuit. right ventricle only has to pump blood
to the nearby lungs

22-40
Left Ventricle Trabeculae carneae in the left ventricle
are more prominent. Two large papillary muscles attach to
the chordae tendineae that help support the left AV valve.
At the superior end of the ventricular cavity, the aortic semilunar valve marks the end of the left ventricle and the entrance into the aorta.

41

22-42
Valve Defects and Their Effects on Circulation Valvular insufficiency or valvular incompetence
Leaky valves from inflammation or disease can lead to regurgitation
Heart working hard to overcome may lead to further heart enlargement with possible bad consequences
A primary cause is rheumatic heart disease Valvular stenosis
Narrowing of valve resists flow and output of affected chamber decreases and may hypertrophy and dilate
Rheumatic heart disease When antibodies against strep cross-react with connective
tissue Most effected are the endocardium, the valve leaflets, and
the left AV valve

22-43
Heart Sounds Four normal heart sounds: lubb-dupp Lubb due to turbulance of blood from
closing of AV valves (long, booming sound)
Pause Dupp due to turbulance of blood from
closing of semilunar valves (short, sharp sound)
Longer pause Sounds are not heard exactly over valves
(surface projection)

22-44
Heart Murmurs Abnormal sounds usually from turbulance
from faulty valves May be innocent or often a valve disorder Serious valve problems reduce the pumping
efficiency of the heart Common cause: carditis, esp., rheumatic fever
from streptococcal infection. 10-20 years later may lead to rheumatic heart disorder
Examples Mitral stenosis Mitral valve prolapse

22-45
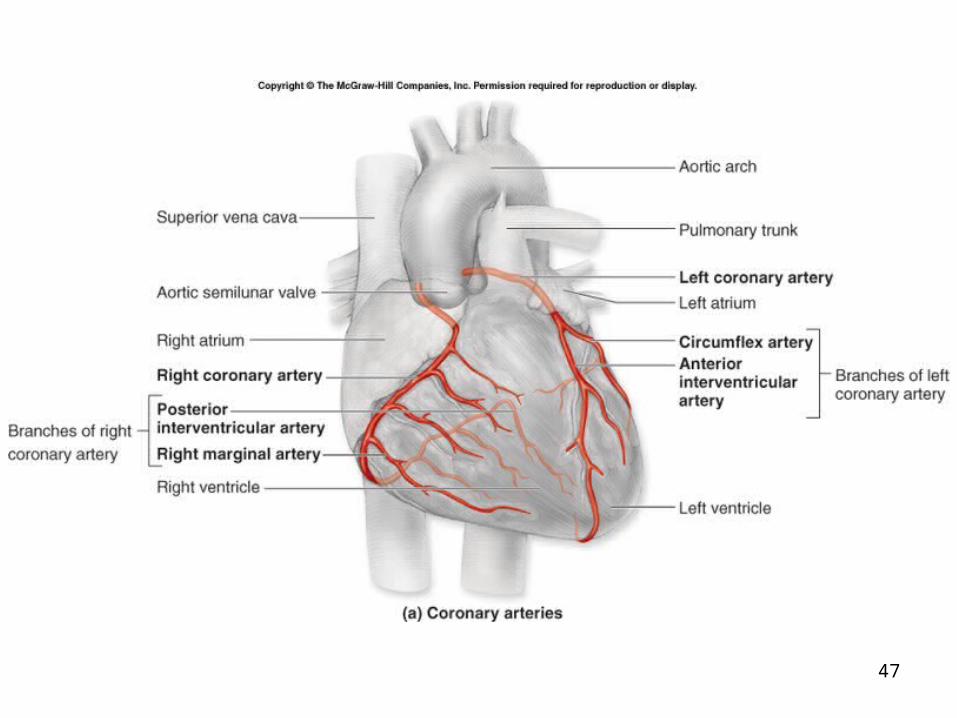
Coronary Circulation Left and right coronary arteries travel in the
coronary sulcus to supply the heart wall. the only branches of the ascending aorta
Openings for these arteries are located immediately superior to the aortic semilunar valve.
The right coronary artery typically branches into the
marginal artery supplies the right border of the heart
posterior interventricular artery supplies both the left and right ventricles

22-46
Coronary Circulation Left coronary artery typically branches into the
anterior interventricular artery. also called the left anterior descending artery (or “widow
maker”) supplies the anterior surface of both ventricles and most
of the interventricular septum Circumflex artery.
supplies the left atrium and ventricle Arterial pattern can vary greatly among
individuals. Anastomoses are small so these arteries are
functional end arteries. Heart muscle can survive with 10-15% of normal supply.
47

22-48
Coronary Circulation Veins parallel arteries generally. Great cardiac vein is beside the anterior
interventricular artery The middle cardiac vein is beside the
posterior interventricular artery The small cardiac vein is beside the right
marginal artery All these cardiac veins drain into the
coronary sinus, a large vein with no smooth muscle in the posterior coronary sulcus, that drains into the right atrium.

49
22-50
Angina Pectoris and Myocardial Infarction Coronary atherosclerosis or coronary
heart disease is the most common cause of death in the US - narrows coronary blood vessels and decreases blood flow and causes chest pain
Angina pectoris Pain with exertion - follows sympathetic
pathways Nitroglycerin may temporarily dilate vessels Prognosis and long-term therapy depend upon
severity of narrowing

22-51
Angina Pectoris and Myocardial Infarction Myocardial infarction (MI) or heart attack
May be from a thrombus (blood clot) or an embolus (a traveling blood clot).
Sudden blockage, infarct, of a coronary artery leads to a dead area. The result is a scar and/or conduction problems.
Deprivation of oxygen may lead to necrosis Symptoms: excruciating, crushing pain; weakness;
shortness or breath; sweating. Some have little pain. May have sudden death if ventricular fibrillation. If
person survives, then scar tissue because little or no regeneration. May weaken heart and lead to death. If person survives, heart muscle may get stronger due to hypertrophy.

22-52
Treatment of Myocardial Infarction Clot busting drugs
Streptokinase tPA Aspirin
May help during an attack Also decreases MI risk but has risks:
cerebral bleeding and GI bleeding (consult doctor)

22-53
Congestive Heart Failure Progressive usually from atherosclerosis,
high blood pressure, multiple infarcts Right sided failure causes
peripheral edema Left sided failure caused pulmonary
edema Eventually leads to right sided failure as well Cor pulmonale
Right ventricular hypertrophy from hypertension in pulmonary circulation

22-54
Risk Factors in Heart Disease 1/5 of those who reach 60 yrs. have a MI 1/4 30-60 yrs. have the potential for MI Major risk factors
High blood cholesterol level High blood pressure Cigarette smoking Obesity Lack of regular exercise Diabetes mellitus Genetic predisposition Male up to 70 yrs.
22-55
Help for Failing Hearts Coronary artery bypass grafting Angioplasty and stents Latissimus dorsi muscle HeartMate LVAD (left ventricular
assist device) Heart transplant

22-56
Prevention
Aerobic exercise, diet, and drugs

22-57
How the Heart Beats: Electrical Properites of Cardiac Tissue The efficient pumping of blood through
the heart and blood vessels requires coordinated contractions of the heart chambers made possible by the properties of cardiac muscle tissue and by specialized cells in the heart, the conducting system.

22-58
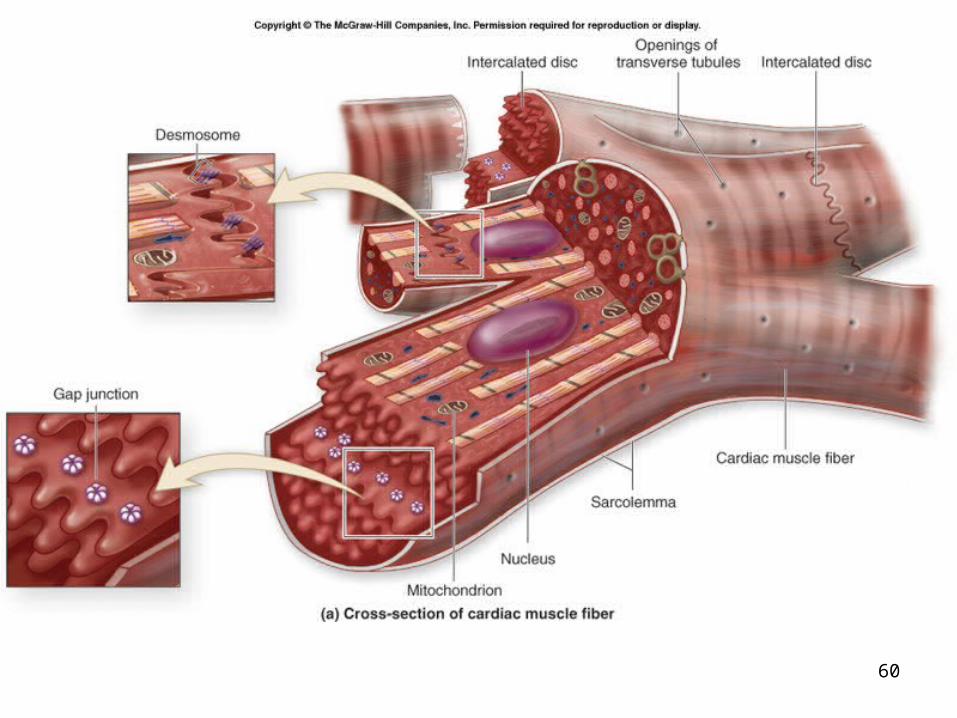
Characteristics of Cardiac Muscle Tissue Fibers are relatively short, branched fibers with one
or two central nuclei and numerous mitochondria for ATP supply.
Fibers are arranged in spiral bundles and wrapped around and between the heart chambers.
Resembles skeletal muscle: fibers are striated, with extensive capillary networks that supply needed nutrients and oxygen.
Cardiac muscle differs from skeletal muscle in certain ways
The sarcoplasmic reticulum is less extensive and organized
No terminal cisternae

22-59
Contraction of Heart Muscle Fibers contract as a single unit because
muscle impulses are distributed immediately and simultaneously throughout all fibers either of the atria or of the ventricles.
Specialized cell–cell contacts called intercalated discs electrically and mechanically link the fibers together and permit the immediate passage of nerve impulses.
60

61

22-62
The Heart’s Conducting System Autorhythmicity. Some of the cells
spontaneously depolarize. Certain cardiac muscle fibers (1%) are
specialized to conduct muscle impulses to the contractile muscle cells of the myocardium.
Specialized cells are part of the heart’s conduction system.
22-63
The Heart’s Conducting System Heartbeat is initiated by the cardiac
muscle fibers of the sinoatrial (SA) node. near the entrance of the superior vena cava
Act as the pacemaker (fastest part of the heart).
Initiates impulses 70 - 80 times per minute.

22-64
The Heart’s Conducting System Impulse travels to both atria,
stimulating atrial systole. And via an internodal conduction
pathway through an opening in the fibrous skeleton to the atrioventricular (AV) node between the right AV valve and the coronary sinus Delay at the AV node

22-65
The Heart’s Conducting System From the AV node to the atrioventricular (AV)
bundle (bundle of His). into the interventricular septum and then divides
into one right and two left bundle branches. To conduction fibers called Purkinje fibers in the
heart apex. Purkinje fibers are larger than other cardiac muscle
fibers. Muscle impulse conduction along the Purkinje fibers is
extremely rapid, consistent with the large size of the cells.
The impulse spreads immediately throughout the ventricular myocardium and the ventricles contract.

22-66
The Heart’s Conducting System Fastest part of the heart sets the
rhythm If the SA node is damaged, then the
rhythm is set by the atria, the next fastest part of the heart
If the AV node is blocked, then the ventricles will beat at a slow rate (about 40 beats/min) and independently of the atria

67

68

22-69
Summary of Blood Flow During the Cardiac Cycle Blood flows continuously into both atria
under low pressure. Blood flows into the ventricles if the AV
valves are open. Most of the ventricular filling is passive (70%). Atrial systole pushes in the final 30%.
During ventricular systole, the AV valves close, and the semilunar valves open to allow blood to enter the large arterial trunks.

22-70
The Electrocardiogram (ECG or EKG) Composite tracing of all muscle
impulses generated by myocardial cells 3 principle deflections
P wave corresponds to atrial depolarization QRS complex corresponds to the beginning
of depolarization of the ventricles (and repolarization of the atria)
T wave corresponds to repolarization of the ventricles

22-71
Atrial flutter 200-400 beats/min - stimulates atria and AV node
repeatedly May last for years and may degenerate to
fibrillation Atrial fibrillation
Chaotic and leads to an irregular heart rate Ventricles respond by increasing and decreasing
contraction activities and may lead to serious dysrhythmia
May increase likelihood of blood clots Decreased efficiency of the heart (20-30%)
Cardiac Arrhythmia (Dysrhythmia)

22-72
Premature ventricular contractions (PVCs) Often from stress, stimulants such as caffeine,
or sleep deprivation May be single or in bursts Common and not a problem unless in great
numbers Ventricular fibrillation
Uncoordinated contractions, life-threatening - leads to cardiac arrest
Paddle electrodes depolarize the heart and puts it in refractory period (stops it), hope that normal sinus rhythm will start up
Cardiac Arrhythmia (Dysrhythmia)

22-73
Innervation of the Heart Innervated by the autonomic nervous
system, the coronary plexus Autonomic innervation by autonomic
centers in the brainstem don’t initiate heartbeat.
Sympathetic innervation increases the rate and the force of heart contractions.
Parasympathetic innervation decreases heart rate, but tends to have no effect on the force of contractions, except in special circumstances.

22-74
Tying It All Together: The Cardiac Cycle The time of one complete heartbeat. Contraction phase is called systole
forces blood either into another chamber or into a blood vessel
Relaxation phase is termed diastole. the chamber fills with blood

22-75
Steps in the Cardiac Cycle

76
22-77
Decreased flexibility and elasticity of the connective tissue can cause the valves to become slightly inflexible and a murmur may develop and blood flow through the heart may be altered.
Decreased conduction system efficiency reduces the ability to pump the extra blood needed during stress and exercise.
Aging and the Heart

22-78
The muscular wall of the ventricle increases in thickness when high blood pressure causes the ventricles to work harder.
That leads to hypertrophy and, therefore, thickening of the cardiac muscle fibers and a change in the normal arrangement of formed fiber bundles. The heart is enlarged, but it works less efficiently.
Aging and the Heart

22-79
Starts to develop in the third week when diffusion is not enough.
During weeks 5-8, the single heart tube becomes partitioned into four chambers and the main vessels entering the leaving the heart form. This partitioning is complex, and errors in development lead to many of the more common congenital heart malformations.
Development of the Heart
22-80
Congenital Heart Defects Ventricular septal defect Transposition of the great vessels Coarctation of the aorta Tetralogy of Fallot Pulmonary stenosis Patent foramen ovale Patent ductus arteriosus
Related Documents